Back to Journals » Journal of Blood Medicine » Volume 16
Effectiveness of PK-Guided Personalized Recombinant FVIII Treatment in Patients with Hemophilia A: Clinical Case Experiences Based on an Observational Study
Authors Mizoguchi Y, Hino M ![]() , Ueda H
, Ueda H ![]() , Miyaguchi Y
, Miyaguchi Y ![]() , Kobayashi M
, Kobayashi M
Received 23 May 2024
Accepted for publication 13 December 2024
Published 10 January 2025 Volume 2025:16 Pages 27—39
DOI https://doi.org/10.2147/JBM.S479564
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Yoko Mizoguchi,1 Moeko Hino,2 Hitoshi Ueda,3 Yasuo Miyaguchi,3 Masao Kobayashi1,4
1Department of Pediatrics, Hiroshima University Graduate School of Biomedical Sciences, Hiroshima, Japan; 2Department of Pediatrics, Chiba University Hospital, Chiba, Japan; 3Japan Medical Office, Takeda Pharmaceutical Company Limited, Tokyo, Japan; 4Japanese Red Cross, Chugoku-Shikoku Block Blood Center, Hiroshima, Japan
Correspondence: Yasuo Miyaguchi, Japan Medical Office, Takeda Pharmaceutical Company Limited, 2 Chome-1-1 Nihonbashihoncho, Chuo-ku, Tokyo, 103-0023, Japan, Tel +81 70-4921-7966, Email [email protected]
Purpose: Prophylaxis with recombinant factor VIII (rFVIII) products is the gold-standard treatment for hemophilia A. However, interindividual differences affect the half-life and clearance of rFVIII products. The myPKFiT is a web-based medical-device software program for population pharmacokinetic (PK) simulation of FVIII products to guide accurate FVIII doses and dosing intervals. In this Japanese multicenter observational study, the efficacy of regimen adjustment using myPKFiT was examined.
Patients and Methods: Male patients with hemophilia A undergoing personalized treatment with myPKFiT using either octocog alfa or rurioctocog alfa pegol were included. Patients were aged < 18 years. Primary endpoint was annualized bleeding rate (ABR). Secondary endpoints were ABR by type of bleeding, rFVIII product consumption, physical activity level, quality of life, and frequency of rFVIII administrations. Results are presented descriptively; however, for exploratory analysis, data before and after regimen adjustment were compared using the Wilcoxon signed-rank test.
Results: Seven patients aged 3– 17 years (median age 13 years) participated in the study. Mean ABR for all bleeds decreased by 0.86 after PK-guided regimen adjustment. Four patients showed zero ABR before and after regimen adjustment using myPKFiT. No significant differences were noted in the consumption of rFVIII products. However, mean rFVIII consumption decreased in two patients after PK-guided regimen adjustment. Three patients increased physical activity and, according to the treatment based on the PK-guided regimen adjustment, this resulted in no increased bleeding.
Conclusion: The results from this study in a small number of patients suggest that PK-guided regimen adjustment with myPKFiT may support optimization of the individual prophylactic administration of the FVIII products octocog alfa and rurioctocog alfa pegol.
Study Registration: UMIN000044800.
Keywords: annual bleeding rate, myPKFiT, prophylaxis, pharmacokinetic adjustment
Introduction
Hemophilia A is a congenital bleeding disorder characterized by either decreased production or dysfunction of blood coagulation factor VIII (FVIII).1 Hemophilia A is caused by a genetic abnormality that shows an X-linked pattern of inheritance.2 Most patients are male, with an estimated global prevalence for all severities of 17.1 per 100,000 males.3 Patients with hemophilia A are deficient in FVIII activity and are less able to form blood clots and achieve hemostasis once they bleed.1 Patients with severe hemophilia may experience spontaneous and more frequent bleeding with joint arthropathy and may suffer from life-threatening hemorrhagic episodes.
In the past, standard-of-care treatment for hemophilia was on-demand coagulation factor replacement therapy, in which bleeding was treated.4 In the 1990s, with the development of recombinant FVIII (rFVIII) concentrates, prophylaxis became widespread, with increasing numbers of patients using prophylaxis over time.4 The reduction in the frequency of bleeding in patients with hemophilia A with prophylaxis has led to the prevention of arthropathy and has contributed to improvements in quality of life (QOL).5 However, the half-life and clearance of FVIII products used in prophylaxis vary depending on factors such as the severity of hemophilia, patient’s age, body weight, and blood type, resulting in large interindividual differences and the need for individualized treatment.6
Although FVIII concentrates are dosed according to a patient’s body weight, there is still variability in the pharmacokinetic (PK) profile of the concentrates.7–9 Treatment guidelines prepared by the World Federation of Haemophilia state that for patients with a severe phenotype (which includes patients with moderate hemophilia with a severe phenotype), prophylaxis should be individualized for patients by taking individual PK into consideration.8 This is further supported by guidelines prepared by the Japanese Society on Thrombosis and Hemostasis,10 which state that “individual differences in PK are large and the half-life can range from 8 to 23 hours”. Thus, information on the PK of individual patients has become a very useful guide to help optimize administration of FVIII in patients with hemophilia A.8 However, an accurate PK analysis for optimization of regular replacement therapy usually requires full PK blood sampling (10 times or more) per patient,11,12 which is not feasible in clinical practice due to issues such as patient burden, time constraints, and costs.13
MyPKFiT is a web-based medical-device program that allows the profiling of individual patient PK for octocog alfa (INN, rurioctocog alfa; JAN) or rurioctocog alfa pegol (INN) to simulate dose and dosing intervals with sparse sampling14,15 (at least two blood specimens16). However, reports of the usefulness of a PK-guided adjusted replacement therapy regimen using myPKFiT are limited, and there have been no reports in Japan. The present study was designed to evaluate the usefulness of personalized treatment using myPKFiT in male patients with hemophilia A treated with rFVIII in Japan.
Materials and Methods
Study Design
This was a multicenter observational study in male patients with hemophilia A undergoing personalized treatment with myPKFiT using either octocog alfa or rurioctocog alfa pegol. The study period was August 13, 2021, to July 19, 2022. Data were collected in the 6 months before the treatment regimen was adjusted (baseline period) and in the 6 months after the treatment regimen was adjusted via myPKFiT (observation period) (Supplementary Figure 1). For patients who provided informed consent after the 6-month observation period, data were collected retrospectively at baseline and for the whole of the 6-month observation period. For patients who provided informed consent during the 6-month observation period, data were collected retrospectively at baseline and up until informed consent was obtained. Thereafter, data were collected prospectively until the end of the observation period. The evaluation period for target patients was a maximum of 18 months from the start of baseline to the end of the observation period.
Visit 1 was the time during which written informed consent was obtained from patients, or if applicable their legally acceptable representative, prior to the initiation of data collection. The study investigator prepared electronic case report forms for all patients or representatives who gave written informed consent. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and all applicable local regulations. The study protocol was approved by the central ethics review board (MINS Institutional Review Board) and local institutional review boards (Hiroshima University Hospital and Chiba University Hospital). This study was registered with UMIN Clinical Trial Registry (Identifier: UMIN000044800).
Study Population
Patients were eligible for inclusion if they were male and had been previously diagnosed with congenital severe hemophilia A (coagulation factor VIII:C [FVIII:C] levels <1% at baseline) or moderate hemophilia A (FVIII:C levels ≥1% to <5% at baseline and receiving prophylaxis). Further inclusion criteria comprised patients with either current or previous treatment with octocog alfa or rurioctocog alfa pegol, and patients currently undergoing PK-guided personalized therapy (rFVIII replacement therapy) with myPKFiT. Patients must have been aged ≥12 years at the time of initiation of myPKFiT if on rurioctocog alfa pegol treatment. Patients were excluded if they had been treated with rFVIII products that had been modified using a PK-guided tool that is not approved in Japan or if they were taking FVIII inhibitors.
Treatment Protocol
Patients were treated at the investigator’s discretion in accordance with the package insert of each drug: octocog alfa (rFVIII: ADVATE® [Baxalta Incorporated, a Takeda company, Bannockburn, IL, USA]) or rurioctocog alfa pegol (pegylated rFVIII: Adynovate® [Baxalta Incorporated, a Takeda company, Bannockburn, IL, USA]). Rurioctocog alfa pegol has an extended half-life compared with octocog alfa;9 the half-life is extended by the binding of polyethylene glycol moieties to the octocog alfa backbone. Please note the official Japanese adopted name for ADVATE is rurioctocog alfa. Analysis of data from patients who switched rFVIII products (octocog alfa to rurioctocog alfa pegol only) as PK-guided treatment was allowed in the study plan.
Endpoints
The primary endpoint was annualized bleeding rate (ABR). Secondary endpoints were:
ABR by bleed type (traumatic bleeding, spontaneous bleeding, joint bleeding, and non-joint bleeding); consumption of rFVIII products; amount of physical activity; and QOL. Number of rFVIII product administrations per week was an exploratory endpoint.
Outcome Measures
Demographic data collected included date of birth and body weight at Visit 1. To reduce the risk of re-identification, age was categorized via the school structure in Japan, <6, ≥6 to <12 (elementary school), ≥12 to <15 (junior high school), and ≥15 to <18 years (high school). Baseline data collected at Visit 1 included hemophilic disease history, concomitant medications and procedures, and previous complications including clinically relevant symptoms. The number of patient-reported bleeding episodes and details of the bleeding (spontaneous, traumatic, joint, or non-joint) was recorded, as well as the dosage and dosing frequency of rFVIII product. Physical activity and QOL were recorded using an electronic tablet. Patients recalled and reported their physical activity level using the Japanese version of the International Physical Activity Questionnaire (IPAQ) short version,17 for patients aged ≥15 years at Visit 1, or the Japanese version of the IPAQ for Japanese Early Adolescents (IPAQ-JEA),18 for patients aged ≥12 years and <15 years at Visit 1. As reference data, the physical activity level of patients aged <12 years was collected using IPAQ-JEA. Patients aged ≥16 years recalled and reported their QOL using the 36-Item Short Form Survey (SF-36).19 Patients aged ≥8 years and <16 years at Visit 1 recalled and reported their QOL using KIDSCREEN-27.20 As reference data, QOL of patients aged <8 years were collected by asking their guardians to complete the SF-36.
For patients who provided informed consent after the 6-month observation period, number of bleeding episodes, the amount of rFVIII products consumed, physical activity, and QOL during the 6-month observation period were collected at Visit 1 (ie, at the same time that data were collected for the 6-month baseline period). For patients who provided informed consent during the 6-month observation period, number of bleeding episodes, the amount of rFVIII products consumed, physical activity, and QOL during the 6-month observation period were collected after the 6-month observation period was completed (Visit 2).
Statistical Analysis
The planned sample size of ≥30 patients was based on a previous Spanish study of 36 patients with severe hemophilia A who were treated with octocog alfa, which showed a significant effect on ABR and annualized joint bleeding frequency after PK-guided regimen adjustment via myPKFiT.21 The planned sample number for this current study was not based on statistical rationale. The analysis set consisted of all patients who provided written informed consent, satisfied the inclusion/exclusion criteria, and received study treatment. For categorical values, frequencies in each category and the proportion in the category with the total frequency in each category as the denominator were calculated. Wilcoxon signed-rank test was performed to compare data before and after regimen adjustment for continuous variables, taking distribution into account. Statistical hypothesis testing was two-sided with a significance level of 0.05. Confidence intervals were set at the 95% confidence level.
Bleeding and rFVIII consumption were recorded as a 6-month observation; therefore, mean ABR was calculated by multiplying the observed values by 2. rFVIII consumption grouped by specific replacement therapy was calculated in the following manner: Prophylaxis and extra dosing (eg, dosing for preventing bleeding before activities with bleed risk such as sports): when the administration interval was reported on a weekly basis: (Weeks actually taken) × (Dose [international units (IU)]) × (Number of doses per week); when the administration interval was reported on a daily basis: (Weeks actually taken) × (Dose [IU]) × 7 / N (N = number of administrations per day); on-demand dosing for bleeding: (Dose unit [IU]) × (number of administrations); total consumption: sum of prophylaxis plus extra dosing plus on-demand dosing for bleeding. Patients’ individual physical activities were grouped by intensity (vigorous, moderate, low [walking]). No imputation was performed for missing data and multiplicity adjustment was not performed. Statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic and Baseline Clinical Characteristics
Overall, seven patients were enrolled in the study and all seven patients were included in the analysis (Table 1). Two patients were treated with octocog alfa and five patients were treated with rurioctocog alfa pegol. The median (Quartile 1−Quartile 3 [Q1−Q3]) age at initiation of regimen adjustment was 13 (8.50−15.50) years (range: 3−17 years). The median (Q1−Q3) body weight at initiation of regimen adjustment was 44.70 (30.80−54.55) kg (range: 16.40−62.00 kg). No concomitant medication use considered to influence bleeding outcomes was reported for any of the seven patients.
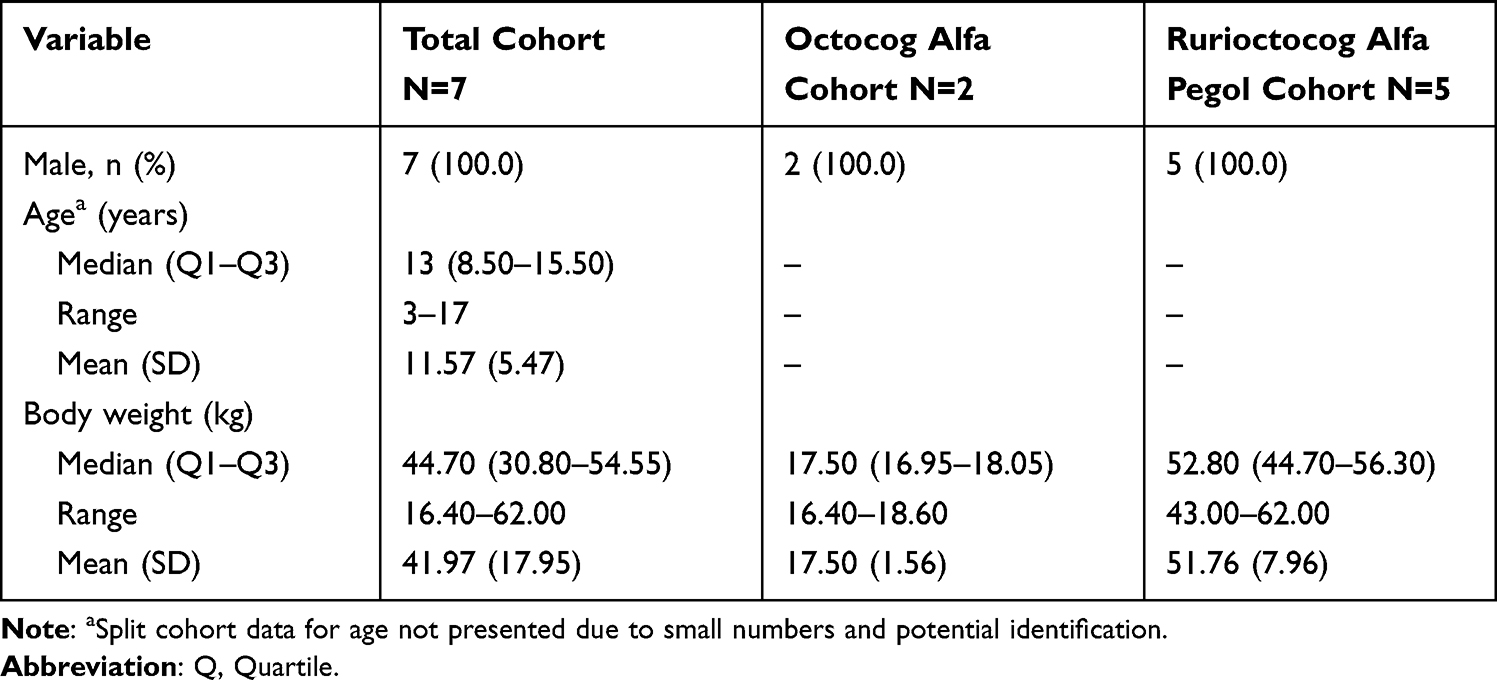 |
Table 1 Patient Demographics and Baseline Characteristics |
Of the five patients treated with rurioctocog alfa pegol, one patient was switched from octocog alfa to rurioctocog alfa pegol at the time of regimen adjustment. All patient regimens were adjusted with respect to PK profiling using the myPKFiT application, and all patients completed the 6-month observation period after PK-guided regimen adjustment. Observational data after regimen adjustment were collected retrospectively for four patients and prospectively for three patients (Table 2).
 |
Table 2 Individual Patient Data and ABR Before and After PK-Guided Regimen Adjustment (Analysis Set, N=7) |
Primary Outcome Measure: ABR Before and After rFVIII Regimen Adjustment
The median ABR for all bleeding types was zero before and after PK-guided regimen adjustment, and thus no overall change in ABR was observed (Table 3). However, changes in ABR after PK-guided regimen adjustment were observed for individual patients (Table 2). A clinically relevant reduction in ABR (12 bleeds to two bleeds) was observed in a patient aged ≥15 to <18 years (Patient D). This patient had a reduction in ABR for traumatic bleeding and joint bleeding. ABR increased slightly in two patients aged <6 years (Patients A and B). For the remaining four patients, ABR was zero both before and after PK-guided regimen adjustment. No statistically significant changes in ABR from before or after regimen adjustment were observed.
 |
Table 3 Observed ABR Before and After PK-Guided Regimen Adjustment |
Annual Consumption of rFVIII Products
Median rFVIII consumption (IU) numerically increased for total treatment and remained unchanged for prophylaxis after PK-guided regimen adjustment (Table 4). Median rFVIII consumption for extra and on-demand dosing was zero both before and after regimen adjustment. When rFVIII consumption was analyzed for individual patients (Figure 1), consumption for prophylaxis treatment numerically increased in five patients and numerically decreased in two patients after PK-guided regimen adjustment. rFVIII consumption for extra-dosing treatment numerically increased in three cases; for the remaining patients, rFVIII consumption for extra-dosing treatment was not required. rFVIII consumption for on-demand treatment numerically increased in one patient and numerically decreased in another patient; for the remaining patients, rFVIII consumption for on-demand treatment was not required. No significant differences were observed in the consumption of rFVIII products.
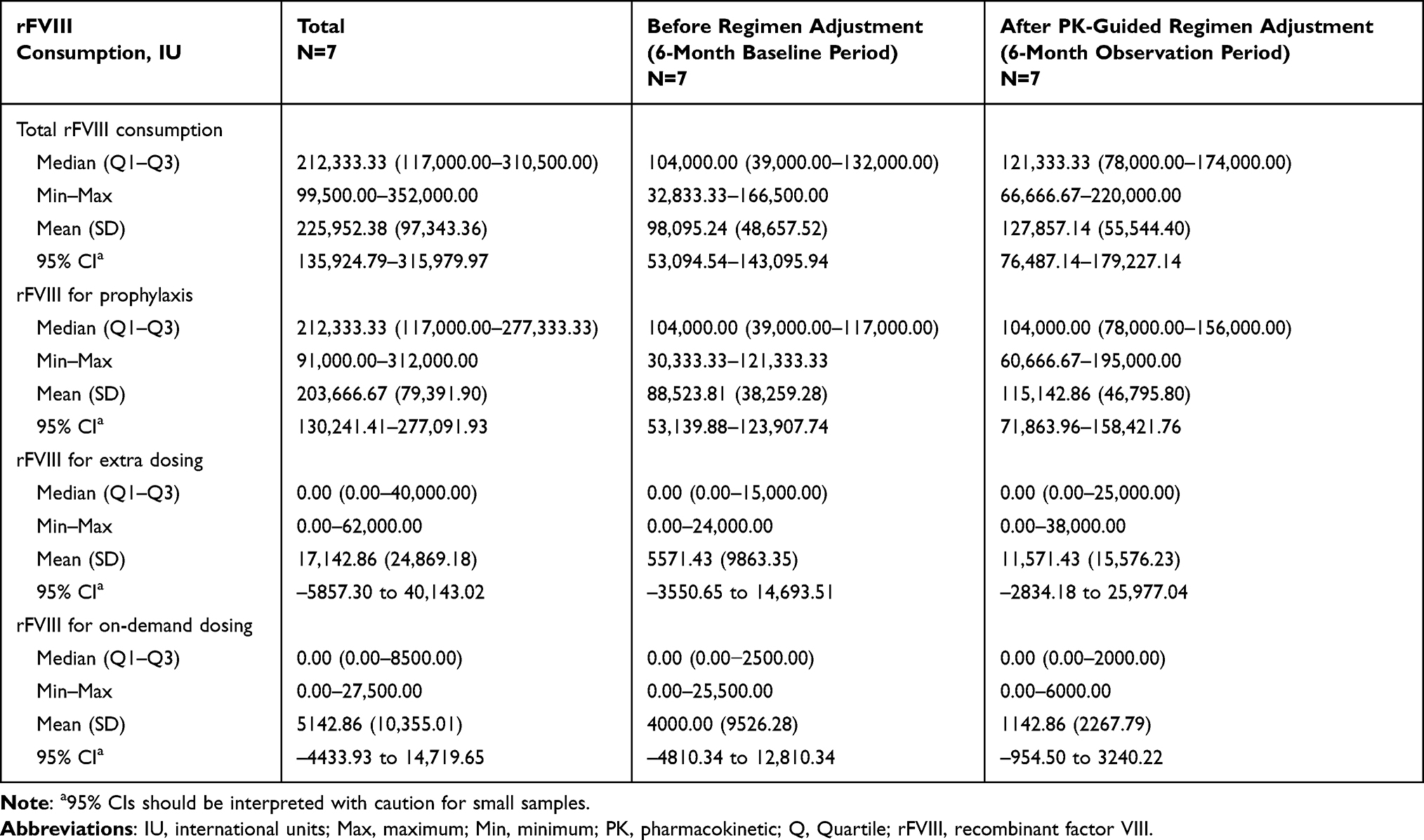 |
Table 4 Annual Consumption of rFVIII Products Before and After PK-Guided Regimen Adjustment |
 |
Figure 1 Annual consumption of rFVIII products before and after PK-guided regimen adjustment by therapy type. (A) Total consumption. (B) Prophylaxis treatment. (C) Extra-dosing treatment. (D) On-demand treatment. Abbreviations: FVIII, factor VIII; IU, international units; PK, pharmacokinetic; rFVIII, recombinant factor VIII. |
Frequency of rFVIII Product Administrations per Week
The median frequency of rFVIII administrations per week did not change for total replacement and prophylaxis treatment. The median (Q1–Q3) number of rFVIII doses per week, before and after regimen adjustment, was 2.53 (2.33–3.19) versus 2.56 (2.28–2.88) for total replacement (median change 0.00 [–0.18 to 0.00]) and 2.33 (2.33–3.00) versus 2.33 (2.00–2.66) for prophylaxis (median change 0.00 [–0.29 to 0.00]). The median frequency of rFVIII administrations per week of on-demand dosing and extra dosing was zero both before and after regimen adjustment. No significant differences were observed in the frequency of rFVIII administrations per week after PK-guided regimen adjustment.
Physical Activity
Three patients reported physical activity with the IPAQ short form, and three patients reported physical activity with the JEA form; answers were not collected for one patient. Overall, total activity increased in three patients (Patient E: 4400 vs 5592, Patient F: 3372 vs 10290, Patient B: 3324 vs 3444) and remained unchanged in three patients after PK-guided regimen adjustment (Figure 2). Vigorous activity increased in one patient and was unchanged in the remaining five patients. These five patients reported vigorous activity >3 times a week during the baseline period. Moderate activity increased in three patients and was unchanged in the remaining three patients. Low activity (walking) increased in two patients and was unchanged in the remaining four patients.
 |
Figure 2 Amount of physical activity per individual patient assessed by either the IPAQ form (A–D) or the JEA form (E–H). Abbreviations: IPAQ, International Physical Activity Questionnaire; JEA, Japanese Early Adolescents. |
Qol
QOL was reported using the SF-36 questionnaire for four patients, and the KIDSCREEN-27 questionnaire for three patients (Supplementary Figure 2). No significant differences were reported after PK-guided regimen adjustment for any category in either questionnaire.
Discussion
This observational study in patients with hemophilia A shows clinical outcomes for individual patients who underwent PK-guided adjustment of their rFVIII regimen with myPKFiT and is the first study to focus on comparing rFVIII regimen adjustment in children and adolescents with hemophilia in a real-world setting in Japan. Although no substantial differences were shown, the overall trend and individual patient outcomes indicated that myPKFiT may be effective for the reduction in ABR. Further, some children who were adjusted by prophylactic administration of FVIII by myPKFiT have increased their levels of physical activity without leading to any bleeding episodes. These data suggest that myPKFiT may potentially contribute to the optimization of treatment for patients with hemophilia A during school life as well as daily life. However, it is difficult to draw any firm conclusions because of the small sample size.
In this study, it was difficult to show a statistically significant effect on ABR because four of seven patients were well controlled by the prophylactic administration of FVIII, showing no ABR before adjustment by myPKFiT. In a Spanish study of 36 patients (aged 7–53 years), myPKFiT use resulted in a significant decrease in ABR. Similar to this study, a decrease (non-significant) in ABR in a subgroup analysis of 13 patients aged ≤15 years21 following PK-guided adjustment with myPKFiT (0.7 ± 0.7 vs 0.6 ± 0.8) was found. In the current study, the number of bleeding episodes was profoundly reduced in Patient D after PK-guided regimen adjustment. Part of Patient D’s regimen adjustment was a switch from the standard half-life octocog alfa to the extended half-life rurioctocog alfa pegol; a similar switch to an extended half-life FVIII product after PK assessment was described for five patients in an earlier study.22 Following regimen adjustment, Patient D’s joint bleeding ABR decreased from 10.00 to zero, despite the patient continuing to play basketball and maintaining high physical activity levels post PK-guided adjustment. Therefore, the use of myPKFiT was partly effective for preventing bleeding episodes through the PK-guided regimen adjustment of prophylactic administration.
Two patients showed a decrease in rFVIII consumption without affecting the frequency of ABR. Based on the PK-guided adjustment, octocog alfa was switched to rurioctocog alfa pegol in one patient, and the prophylactic administration was reduced from two times per week to every 4 days in the other patient. The sufficient trough level as prophylaxis in an individual patient may be estimated by myPKFiT, resulting in the decrease in medical costs as well as in the patient’s effort for prophylaxis. For the remaining five patients, their rFVIII dose increased by PK-guided adjustment, but frequency of dosing did not increase. Consequently, the increased dose of rFVIII in these patients may have resulted in increased medical costs.
Traumatic subcutaneous ABR increased for Patients A and B irrespective of the PK-guided adjustment. This may be due to unstable physical activity patterns in daily life due to the patients’ ages (<6 years old). Therefore, it may be difficult to prevent bleeding by sudden trauma in early childhood. In contrast, the risk of bleeding by regular exercise may be preventable by PK-guided prophylaxis, particularly in elementary school-aged children and adolescents, who tend to participate in exercise on fixed schedules. Thus, myPKFiT has the potential to be especially effective in elementary school-aged children or adolescent patients. It is noteworthy that no patients had increased joint bleeding and all patients were able to maintain joint bleeding to zero after myPKFiT simulation. Similar results were published in another Japanese cohort study, where joint bleeding decreased, but not to a statistically significant level, post PK-guided regimen adjustment.22 Therefore, the use of myPKFiT was partly effective for preventing bleeding episodes through the PK-guided dose adjustment of prophylactic administration.
Equivalent or higher levels of physical activity were observed in older children (>6 years old) enrolled during this study compared with younger children. The increase in physical activity during the regimen-adjusted observation period in Patients E and F resulted in zero episodes of bleeding. Patient D had high levels of physical activity with large total ABR (12.00) before the regimen adjustment; however, regimen adjustment and switching from octocog alfa to rurioctocog alfa pegol resulted in the decreases in total ABR and rFVIII consumption during higher levels of physical activity. Patients D and E regularly played physical contact sports associated with increased bleeding risks (eg, basketball and football). These results suggest the efficacy of personalized prophylactic administration of rFVIII by PK visualization with myPKFiT.
Regarding QOL, patient results were variable, with improvement reported by some and worsening by others. One patient (Patient G) reported a dramatic decrease in QOL, but there is a possibility that QOL was affected by other factors because all reported bleeding rates for this patient were zero before and after PK-guided adjustment of their rFVIII regimen. This is supported by a previous systematic review and meta-analysis showing that health-related QOL assessment in young people with hemophilia A is heterogeneous and context specific.23 Overall, because of the limited sample size and the variability of the questionnaires implemented due to the varying ages of the patients, it was difficult to show an overall trend for QOL in this study. Evaluating the QOL of patients with hemophilia A undergoing PK-guided treatment is important for improving their QOL to a level similar to that of people without hemophilia A, which is a goal of the International Society on Thrombosis and Haemostasis hemophilia treatment guidelines.24
The serial examination of major joints is important to evaluate joint health. Previous reports have shown that some patients with hemophilia A, and without symptomatic bleedings, could have joint damage.25 Of particular concern are a synovitis or hemosiderin deposition, which might be caused by asymptomatic bleeding.25,26 As symptomatic bleeding is a subjective parameter reported by patients, treatment based on objective parameters may contribute toward the continuation of patients’ joint health.27 Reports have indicated that joint outcomes were better for patients receiving care in hemophilia treatment centers than in non-hemophilia treatment centers.28 To evaluate joints of patients with hemophilic arthropathy, the Haemophilia Early Arthropathy Detection with Ultrasound scoring and ultrasound scanning procedure was developed,29 and the joint health of six of seven patients enrolled in this study was annually evaluated by joint examination using this method. All patients examined showed no deterioration of joint findings after regimen adjustment based on myPKFiT simulation data (data not shown). This suggests that specialized care, including PK-guided therapy with continuously precise examination of joints, may contribute to better joint health.28
This multicenter observational study was designed to incorporate patient-centered outcome measures in the real-world setting. This study included children and adolescents, but the small study population size was a major limitation to providing conclusive data on the efficacy of rFVIII regimen adjustment via the myPKFit. However, hemophilia is a very rare disease, and therefore even observational data from a small study population can contribute to our understanding of real-world treatment. Because of the small sample size, the results of the Wilcoxon signed-rank test need to be interpreted with caution and are provided for exploratory purposes only. In Japan, current utilization of regimen adjustment tools in clinical practice may be restricted, thus limiting the number of patients eligible for inclusion in this study. Furthermore, because data for most patients were collected retrospectively, interpretation of patient-reported outcomes may be limited by recall bias. For physical activity and QOL, different types of questionnaires were used for different age groups because a single validated QOL questionnaire for all age groups is not available. The questionnaires have all been validated appropriately for the different age groups, but the use of multiple questionnaires further reduced the number of patients in each assessment. Moreover, all enrolled patients were children and adolescents, and changes in the living environment during the growth period may have affected the results. Lastly, the COVID-19 pandemic occurred during the study period and may have affected the results, especially QOL data.30
Conclusion
The overall trends and results from individual patients suggest that PK-guided regimen adjustment with myPKFiT may contribute to the optimization of treatment. However, no statistical differences in each observation item before and after rFVIII regimen adjustment were noted due to the small number of patients enrolled.
Abbreviations
ABR, annualized bleeding rate; FVIII, factor VIII; FVIII:C, coagulation factor VIII:C; IPAQ, International Physical Activity Questionnaire; IPAQ-JEA, International Physical Activity Questionnaire for Japanese Early Adolescents; IU, international units; PK, pharmacokinetic; Q, Quartile; QOL, quality of life; rFVIII, recombinant factor VIII; SF-36, 36-Item Short Form Survey.
Data Sharing Statement
The data generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and all applicable local regulations. The study protocol was approved by the central ethics review board (MINS Institutional Review Board) and local institutional review boards (Hiroshima University Hospital and Chiba University Hospital). This study was registered with UMIN Clinical Trial Registry (Identifier: UMIN000044800). Written informed consent was obtained from patients, or if applicable their legally acceptable representative, prior to the initiation of data collection.
Acknowledgments
The authors would like to thank all study participants and study team members. Linical Company Limited, Osaka, Japan, contributed to support of study execution as contract research organization. Medical writing assistance was provided by Jessica Reid, PhD, and Prudence Stanford, PhD, CMPP, of ProScribe – Envision Pharma Group, and was funded by Takeda Pharmaceutical Company Limited. ProScribe’s services complied with international guidelines for Good Publication Practice.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Takeda Pharmaceutical Company Limited, manufacturer of rurioctocog alfa or rurioctocog alfa pegol. Takeda Pharmaceutical Company Limited was involved in the study design, data collection, data analysis, and preparation of the manuscript.
Disclosure
YMiz reports receiving honoraria payments for lectures from Takeda Pharmaceutical Company Limited. MH reports receiving consulting fees for advisory boards, honoraria for lectures, and support for attending meetings and/or travel from Takeda Pharmaceutical Company Limited. HU and YMiy are employees of Takeda Pharmaceutical Company Limited. HU has received shares from Takeda Pharmaceutical Company Limited. MK reports no conflict of interest.
References
1. Peyvandi F, Garagiola I, Young G. The past and future of haemophilia: diagnosis, treatments, and its complications. Lancet. 2016;388(10040):187–197. doi:10.1016/s0140-6736(15)01123-x
2. Castaman G, Matino D. Hemophilia A and B: molecular and clinical similarities and differences. Haematologica. 2019;104(9):1702–1709. doi:10.3324/haematol.2019.221093
3. Iorio A, Stonebraker JS, Chambost H, et al. Establishing the prevalence and prevalence at birth of hemophilia in males: a meta-analytic approach using national registries. Ann Intern Med. 2019;171(8):540–546. doi:10.7326/m19-1208
4. Trinchero A, Sholzberg M, Matino D. The evolution of hemophilia care: clinical and laboratory advances, opportunities, and challenges. Hamostaseologie. 2020;40(3):311–321. doi:10.1055/a-1175-6530
5. Knobe K, Berntorp E. Haemophilia and joint disease: pathophysiology, evaluation, and management. J Comorb. 2011;1:51–59. doi:10.15256/joc.2011.1.2
6. Turecek PL, Johnsen JM, Pipe SW, O’Donnell JS, the iPATH study group. Biological mechanisms underlying inter-individual variation in factor VIII clearance in haemophilia. Haemophilia. 2020;26(4):575–583. doi:10.1111/hae.14078
7. Björkman S, Oh M, Spotts G, et al. Population pharmacokinetics of recombinant factor VIII: the relationships of pharmacokinetics to age and body weight. Blood. 2012;119(2):612–618. doi:10.1182/blood-2011-07-360594
8. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26 Suppl 6:1–158. doi:10.1111/hae.14046
9. Ay C, Napolitano M, Hassoun A, et al. Classification of recombinant factor VIII products and implications for clinical practice: a systematic literature review. Haemophilia. 2024;30(3):577–588. doi:10.1111/hae.15001
10. Fujii T, Amano K, Atsumi T et al. 2013 revised edition: hemostatic treatment guidelines for hemophilia patients without inhibitors [Japanese]. Japanese J Thromb and Hemost. 2013;24(6):619–639. doi:10.2491/jjsth.24.619
11. Morfini M, Lee M, Messori A. The design and analysis of half-life and recovery studies for factor VIII and factor IX. Factor VIII/Factor IX Scientific and Standardization Committee of the International Society for Thrombosis and Haemostasis. Thromb Haemost. 1991;66(3):384–386. doi:10.1055/s-0038-1646423
12. Lee M, Morfini M, Schulmann S, Ingerslev J The Factor VIII/Factor IX Scientific and Standardization Committee of the International Society for Thrombosis and Haemostasis: the design and analysis of pharmacokinetic studies of coagulation factors 2001. Available from: https://cdn.ymaws.com/www.isth.org/resource/group/d4a6f49a-f4ec-450f-9e0f-7be9f0c2ab2e/official_communications/fviiipharmaco.pdf.
13. Collins PW, Fischer K, Morfini M, Blanchette VS, Björkman S. Implications of coagulation factor VIII and IX pharmacokinetics in the prophylactic treatment of haemophilia. Haemophilia. 2011;17(1):2–10. doi:10.1111/j.1365-2516.2010.02370.x
14. BK170028: myPKFiT for Advate. Available from: https://www.fda.gov/vaccines-blood-biologics/substantially-equivalent-510k-device-information/bk170028-mypkfit-advate.
15. MyPKFiT(®) [Package Insert]. Takeda Pharmaceuticals U.S.A. Inc.; 2023.
16. Björkman S. Limited blood sampling for pharmacokinetic dose tailoring of FVIII in the prophylactic treatment of haemophilia A. Haemophilia. 2010;16(4):597–605. doi:10.1111/j.1365-2516.2009.02191.x
17. Lee PH, Macfarlane DJ, Lam TH, Stewart SM. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act. 2011;8(1):115. doi:10.1186/1479-5868-8-115
18. Oshima Y, Hikihara Y, Kasanami R, Murase N, Ishii K. Validity of moderate to vigorous physical activity according to the modified version of the International Physical Activity Questionnaire for Japanese Early Adolescents. Japanese J Physical Fitness Sports Med. 2017;66:427–436.
19. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
20. Ravens-Sieberer U, Auquier P, Erhart M, et al. The KIDSCREEN-27 quality of life measure for children and adolescents: psychometric results from a cross-cultural survey in 13 European countries. Qual Life Res. 2007;16(8):1347–1356. doi:10.1007/s11136-007-9240-2
21. Mingot-Castellano ME, Parra R, Núñez R, Martorell M. Improvement in clinical outcomes and replacement factor VIII use in patients with haemophilia A after factor VIII pharmacokinetic-guided prophylaxis based on Bayesian models with myPKFiT(®). Haemophilia. 2018;24(5):e338–343. doi:10.1111/hae.13540
22. Nagao A, Yeung CHT, Germini F, Suzuki T. Clinical outcomes in hemophilia A patients undergoing tailoring of prophylaxis based on population-based pharmacokinetic dosing. Thromb Res. 2019;173:79–84. doi:10.1016/j.thromres.2018.11.017
23. Azeredo-da-Silva AF, Zanotto BS, Kuwabara YS, Mata VE. Quality of life in children and adolescents with hemophilia A: a systematic review and meta-analysis. Res Pract Thromb Haemost. 2023;7(1):100008. doi:10.1016/j.rpth.2022.100008
24. Rezende SM, Neumann I, Angchaisuksiri P, et al. International Society on Thrombosis and Haemostasis clinical practice guideline for treatment of congenital hemophilia A and B based on the Grading of Recommendations Assessment, Development, and Evaluation methodology. J Thromb Haemost. 2024;22(9):2629–2652. doi:10.1016/j.jtha.2024.05.026
25. Olivieri M, Kurnik K, Pfluger T, Bidlingmaier C. Identification and long‐term observation of early joint damage by magnetic resonance imaging in clinically asymptomatic joints in patients with haemophilia A or B despite prophylaxis. Haemophilia. 2012;18(3):369–374. doi:10.1111/j.1365-2516.2011.02682.x
26. Di Minno M, Iervolino S, Soscia E, et al. Magnetic resonance imaging and ultrasound evaluation of “healthy” joints in young subjects with severe haemophilia A. Haemophilia. 2013;19(3):e167–e173. doi:10.1111/hae.12107
27. Rodriguez-Merchan EC, Jimenez-Yuste V, Aznar JA, et al. Joint protection in haemophilia. Haemophilia. 2011;17(s2):1–23. doi:10.1111/j.1365-2516.2011.02615.x
28. Mizoguchi Y, Tani C, Aizawa M, et al. Age-specific incidence of joint disease in paediatric patients with haemophilia: a single-centre real-world outcome based on consecutive US examination. Haemophilia. 2023;29(5):1359–1365. doi:10.1111/hae.14848
29. Martinoli C, Alberighi ODC, Di Minno G, et al. Development and definition of a simplified scanning procedure and scoring method for Haemophilia Early Arthropathy Detection with Ultrasound (HEAD-US). Thromb Haemost. 2013;109(06):1170–1179. doi:10.1160/TH12-11-0874
30. Hangai M, Piedvache A, Sawada N, et al. Children’s daily lives and well-being: findings from the Corona-CODOMO survey 1st wave. Pediatr Int. 2022;64(1):e14981. doi:10.1111/ped.14981
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.