Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Effectiveness of Moringa oleifera Leaves on TNF-α Expression, Insulin Levels, Glucose Levels and Follicle Count in Rattus norvegicus PCOS Model
Authors Siahaan SCPT, Santoso B, Widjiati ![]()
Received 8 August 2022
Accepted for publication 16 October 2022
Published 26 October 2022 Volume 2022:15 Pages 3255—3270
DOI https://doi.org/10.2147/DMSO.S385492
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Antonio Brunetti
Salmon Charles PT Siahaan,1 Budi Santoso,2 Widjiati3
1Doctoral Program of Medical Science, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 2Department of Obstetrics and Gynecology, Faculty of Medicine, Dr. Soetomo Teaching Hospital, Universitas Airlangga, Surabaya, Indonesia; 3Department of Embryology, Faculty of Veterinary Medicine, Universitas Airlangga, Surabaya, Indonesia
Correspondence: Budi Santoso, Department of Obstetrics and Gynecology, Faculty of Medicine, Dr. Soetomo Teaching Hospital, Universitas Airlangga, Jl. Mayjen Prof. Dr. Moestopo No. 47, Surabaya, East Java, 60132, Indonesia, Tel +62 812-3581-706, Email [email protected]
Background: Polycystic ovary syndrome (PCOS) is a syndrome characterized by ovulation disorders accompanied by hyperandrogens. Women with PCOS are prone to develop insulin resistance which has metabolic characteristics similar to type 2 diabetes and leads to disturbance of follicular formation. PCOS is also known to increase the concentration of proinflammatory cytokines, namely TNF-α. Moringa oleifera leaves have been shown to have compounds that can reduce insulin levels and glucose levels in diabetes mellitus and should be able to reduce TNF-α and follicle count.
Purpose: This study aims to prove the effectiveness of Moringa oleifera leaf in reducing insulin, glucose levels, TNF-α and follicle count in PCOS.
Methods: The three-month-old white rats Wistar (Rattus norvegicus) 150– 170 grams were divided into four groups (n = 10), namely normal rats, PCOS model rats, PCOS model rats given metformin, and PCOS rats given 500mg of Moringa oleifera. The method of this study is taking PCOS model rats by injecting the 100mg/kg BW hormone testosterone propionate for 21 days. After 21 days of therapy, we analyzed insulin, glucose levels, TNF-α and follicle count.
Results: The PCOS control group showed an increase in insulin level, glucose levels, TNF-α expression, and a decrease in the follicle count compared to the normal control group. The insulin level, glucose level, TNF-α and follicle count in the Moringa oleifera 500 mg/kg BW treatment group were significantly lower than in the PCOS control group.
Conclusion: Moringa oleifera leaves have the potential in reducing insulin levels, blood glucose levels, TNF-α and follicle count in PCOS patients.
Keywords: follicle, glucose, insulin, Moringa oleifera, polycystic ovary syndrome, TNF-α
A Letter to the Editor has been published for this article.
Introduction
Polycystic ovary syndrome (PCOS) is a syndrome characterized by ovulation disorders accompanied by hyperandrogen conditions. Women with PCOS are prone to develop insulin resistance which has metabolic characteristics similar to type 2 diabetes and leads to disturbance of follicular formation.1,2
In women with PCOS with insulin resistance, a state of hyperinsulinemia is found which will result in a decreased effect of ovulation induction.3 This happens because, in women with insulin resistance, LH/FSH ratio are found to be fairly high and will affect oocyte quality.4 Ovulation induction agents cannot suppress insulin levels, high levels of luteinizing hormone (LH), and androgens in the blood. Therefore, the treatment of hyperinsulinemia in patients with PCOS will lead to an improvement in folliculogenesis, resulting in ovulation and high pregnancy rates.5
Insulin resistance plays an important role in the pathogenesis of PCOS.6 Endometrial cell differentiation depends on adequate glucose metabolism. Glucose transport (insulin-mediated) is carried out by Glucose Transporter 4 (GLUT4) as a carrier. With a decrease in GLUT4, insulin resistance occurs and leads to an increase in glucose and insulin levels which can cause damage to endometrial cell metabolism in patients with PCOS.7 This process may affect downstream insulin signal transduction and insulin receptors, and may therefore be associated with insulin resistance and PCOS.8
Insulin resistance causes the frequency of GnRH and secretion of LH pulses to increase, causing compensatory hyperinsulinemia and increased production of androgens in the ovaries.2 Ovarian theca androgen production increases and the production of SHGB by the liver will decrease due to hyperinsulinemia.9 Insulin resistance also causes oxidative stress due to hyperglycemia and increased levels of free fatty acids will produce reactive oxygen species (ROS). ROS will induce oxidative stress (OS). Oxidative stress is increased due to an imbalance between ROS and antioxidant defences.
Increased ROS will also increase NFkB which will then form TNF-α, AP-1 activation, HIF-1 as an inflammatory mediator. An increase in TNF-α, IL-6, IL-1β will then activate NF-κB. This increase will cause activation of the serine phosphorylation pathway in the IRS and will inhibit the formation of PI3K which will compensate for the occurrence of hyperandrogens.10
Several studies have reported that PCOS-IR mouse models can be made by subcutaneous injection of testosterone propionate in combination with a high-fat diet.11,12 These mice have features similar to the pathology of PCOS and endocrine disorders but externally added androgens can affect the endocrine level of PCOS.13 Metformin has been used as an insulin sensitizer for the treatment of polycystic ovary syndrome. Studies have shown that metformin can not only improve endocrine disorders in patients with PCOS but also regulate ovarian function and reduce body weight in overweight women with PCOS.14 Metformin acts by inhibiting hepatic glucose uptake, increasing peripheral glucose uptake, reducing peripheral insulin levels, and increasing GLUT-4. However, clinically, the results of long-term metformin treatment result in digestive disorders, such as diarrhea and other effects.15 The search for herbal plants that have the potential for prevention and treatment is certainly very much needed.
Research conducted by Arti Verma et al in 2009 aimed to determine the antioxidant effect of Moringa oleifera lies in its content which consists of various nutritional sources such as phytochemicals, viz, carotenoids, vitamins, minerals, amino acids, sterols, glycosides alkaloids, flavonoids, and phenolics.16 Moringa oleifera extract can work as an antioxidant that binds to ROS and inhibits the oxidative stress process that occurs in PCOS patients. The ethanol extract of Moringa oleifera will inhibit the formation of ROS so that the production of SOD will increase. And the anti-inflammatory effect of the ethanolic extract of Moringa oleifera will reduce inflammatory factors so that the activation of the JNK and NF-B pathways decreases.
Research by Lakshmipriya et al in 2016 found that extracts from this plant have potential as antioxidants, anti-diabetics, and antimicrobials.17 As an anti-diabetic, especially in diabetic cases with insulin resistance, research in mice found that Moringa oleifera can reduce fasting sugar levels. Moringa oleifera extract also plays a role in the treatment of insulin resistance, this is following the research of Chinedu et al, who showed that administration of the extract could increase insulin receptor sensitivity (p<0.0001).18
Based on the above background, we held a research to study the effect of Moringa oleifera on reducing insulin, glucose levels, TNF-α and follicle count in rats PCOS model through insulin resistance and inflammation mechanisms.
Materials and Methods
Materials
Moringa oleifera is a tree belonging to the Moringaceae family originating from South Asia. The leaves of this tree are rich in minerals, vitamins, and other important phytochemicals.19 Moringa oleifera extract process (Kelorina, Moringa Indonesia, Blora, Indonesia) was carried out using the ultrasonic method with 96% ethanol as solvent, the extraction results were then evaporated using a rotary evaporator and oven to form a dry extract. The extraction steps were: 1) Moringa oleifera simplicia was weighed as much as 50 grams, 2) The simplicia was put into a beaker glass (50 grams each) and 500 mL of 96% ethanol was added to the beaker, 3) The time for the extraction process is set using the UAE, which is 3×2 minutes while stirring at each time interval, 4) The extraction results are filtered, 5) The collected filtrate is put into a rotary evaporator flask, 6) The temperature of the tool is set at 40°C with a rotational speed of 70 rpm, 7) The extract from the rotary evaporator was re-evaporated (dried) in an oven at 40°C to obtain a solvent-free dry extract.
Rattus norvegicus female rats with Wistar strain were 3 months old and weighed 150–170 grams. Rattus norvegicus was chosen because they have stable genetics, shorter reproductive life, short estrogen cycle and easy to be handled. Previous research in 2020 also use Rattus norvegicus as a PCOS model with insulin resistance.20
Before the study began, an adaptation period was given for 1 week, with a health condition, normal behavior, and normal vaginal swab results. Exclusion criteria for rats are anatomic abnormalities (ie, ears are injured or not intact, tail is short or stump, one or all four legs are deformed, cannot stand, have sores on body parts, eyes are not clear) and pregnancy during the adaptation period. All of these procedures have been approved by the ethics committee of the Faculty of Veterinary Medicine, Airlangga University, Indonesia.
All experiments were performed following Airlangga University ethic principal (5F: Freedom from hunger and thirst; Freedom from discomfort; Freedom for pain, injury or disease; Freedom to express normal behaviour; freedom from fear and distress), Indonesian National Law: UU no.23 1992 article 69 par 1; UU no.36 2009 article 44 par 4; and UU no.18 2009 article 66 par 2 point C), and these following guidelines: Guide for Care and Use of Laboratory Animals, 8th edition; Report of the AVMA Panel on Euthanasia: 2013 edition (updated on 2020); ARRIVE 2010 (Animal Research: Reporting of In Vivo Experiments) point 8 (updated on 2020).
This research was conducted in a laboratory experimental type with a post-test-only control group design. The rat experiment was conducted with the PCOS model. Rats were divided into 4 major groups, namely the normal control group (K-), PCOS control rats’ model (K-), PCOS rats’ model given metformin (P1), and PCOS rats model given Moringa oleifera (P2). This research was conducted in the laboratory of the Faculty of Veterinary Medicine, Airlangga.
Therapeutic Protocols and Blood Collection Time Points
Forty Rattus norvegicus strain Wistar female rats were randomly divided into equal 4 large groups, consisting of a control group (K-) that was only given aquades for 42 days; a PCOS control group (K+) that was given the hormone testosterone propionate 100mg/kg body weight (BW) for 21 days and aquades for the next 21 days; the first treatment group (P1) that was given testosterone propionate for 21 days and Metformin 2mg/100gram BW for the next 21 days; and the second treatment group (P2) that was given testosterone propionate for 21 days and Moringa oleifera 500mg/kg BW for the next 21 days. Testosterone propionate injections were performed intraperitoneally at the proestrus stage on K+, P1 and P2 groups. On day 22, a vaginal swab was examined to determine the status of the rat’s lust cycle. PCOS rats will show the stage of diestrus on vaginal examination which shows ovulation disturbance. After administering testosterone propionate for 21 days, PCOS model rats will become IR (insulin resistance), characterized by an increase in HOMA IR (P<0.005).12 And in this study, it was seen from the increase in the ratio of glucose and insulin which increased in PCOS model rats compared to normal rats. Metformin was administered to the rats by sonde. Moringa oleifera leaf ethanol extract was administered to the rats by sonde. Testosterone propionate was used to simulate PCOS conditions in Rattus norvegicus because another research in 2009 has proved that prolonged exposure to androgens (testosterone propionate) affects insulin resistance index and free fatty acid levels in PCOS model rat serum.21 A significant increase in insulin resistance index in the group that got testosterone propionate for 14, 21, and 28 days was higher than the controls. Before and after treatment, a vaginal swab was performed to see changes in the cycle due to treatment. On the 43rd day, the rats were sacrificed by ester anesthesia and neck dislocation, then the ovaries and blood samples were taken.
Estimation of Serum Insulin, Glucose Parameters, Expression of TNF-α and Follicle Count
Before the experimental animals were sacrificed, they fasted for 12 hours for blood collection. Glucose levels were measured from the blood taken through rats’ blood vessels which are examined using glucometers. Blood glucose was collected at the end of the study. The units obtained are mg/dL. The data scale is a ratio.
Insulin levels in the serum of PCOS model rats were measured from the blood taken through rats’ blood vessels which were examined using Enzyme-linked immunosorbent assay (ELISA). ELISA is a labelled immunoassay that is considered the gold standard of immunoassays. This immunological test is very sensitive and is used to detect and quantify substances, including antibodies, antigens, proteins, glycoproteins, and hormones.22 Blood insulin was taken at the end of the study. The units obtained are mmol/L. The data scale is a ratio.
TNF- expression is a picture of an increased cell signaling protein (cytokine) and plays an important role in the inflammatory process.23 TNF-α count in the ovarium of PCOS model rats, taken directly from the ovarium organ. The units obtained are Metabolite Insulin Receptor Substrate −1 or IRS-1 which is the insulin signal at the receptor which is measured using a microscope (Cx41 microscope (Olympus, Japan)) with a magnification of 400 times in 10 fields of view measurements using immunohistochemical method, the measurement results are in IRS and is a ratio/interval scale.
Follicle count is the number of follicles in the ovarium tissue of PCOS model rats, taken directly from the ovarium organ which is examined microscopically (histopathology) to observe the follicular phase (primordial, primary, secondary, tertiary, DeGraff, and corpus luteum). Folliculogenesis is measuring the number of follicles that grow in the ovaries, through wedge cutting and microscopic observation. Anatomical pathology laboratory of the Faculty of Veterinary Medicine, Airlangga University conducts the examination. The result is an overview of folliculogenesis for each phase. In 5 visual fields with 400x magnification by counting the number of developments. The data scale was a ratio.
Statistical Analysis
This research data will be recorded in a data collection form that is specifically designed for this study, to observe insulin, glucose levels, TNF-α and follicle count in the PCOS rats’ model. First, the normality test (Shapiro-Wilk test) is carried out. When the distribution is normal, the ANOVA test or analysis of variance was used. However, if the distribution is not normal, the Kruskal Wallis non-parametric test or Mann–Whitney test will be carried out. Duncan’s test will be carried out when there was a significant difference in variable between groups. Statistical calculations will use SPSS version 22 software tools.
Results
Effect of Therapy on Parameters of TNF-α Expression
This histopathological examination aims to determine the expression of TNF-α in the ovaries. The data for each sample was assessed semi-quantitatively according to the modified Remmele method, where the Remmele scale index (Immuno Reactive Score/IRS) is the result of multiplying the percentage score of immunoreactive cells with the color intensity score on immunoreactive cells.24 The data for each sample is the average IRS value observed in ten different fields of view at 100x and 400x magnification.
The results of the examination carried out a normality test before data analysis was carried out. The results of the Shapiro–Wilk test showed that the TNF-α data in the K+ group was not normally distributed (p < 0.05), so it was analyzed using the Kruskal Wallis test. The results of the Kruskal Wallis test showed that there was a significant difference in TNF-α between groups (p < 0.05). The results of the Mann–Whitney test showed that the K- group was significantly different from K+ and P2 and the K+ group was significantly different from P1 and P2 (see the Supplemental File for raw data).
Effect of Therapy on Parameters of Serum Insulin
The results of the blood insulin examination were carried out for normality tests first. The results of the Shapiro–Wilk test showed that the insulin data of all groups were normally distributed (p > 0.05) so the differences in insulin between groups were analyzed using the analysis of variance test.
The results of the analysis of variance showed that there was a significant difference in insulin between groups (p < 0.05), so further tests were needed to determine which groups were different. Duncan’s test results showed that the insulin in the negative control group was significantly different from the positive control group and all treatment groups, the positive control group was significantly different from the negative control group and all treatment groups, but there was no significant difference between the treatment groups.
Effect of Therapy on Parameters of Serum Glucose
The results of the blood glucose examination were carried out for normality tests first. The results of the Shapiro–Wilk test showed that the glucose data of the P1 group was not normally distributed (p < 0.05) so the differences in glucose between groups were analyzed using the Kruskal Wallis test.
The results of the Kruskal Wallis test showed that there was a significant difference in glucose between groups (p < 0.05), so it was necessary to carry out further tests with the Mann–Whitney test to find out which groups were different. The results of the Mann–Whitney test showed that the negative control group was significantly different from the positive control group and all treatment groups, as well as the positive control group which was significantly different from the negative control group and all treatment groups. However, there was no difference between the treatment groups.
Effect of Therapy on Parameters of Follicle Counts
The number of follicles observed was primordial follicles, primary follicles, secondary follicles, tertiary follicles, and de Graff follicles and the corpus luteum. The results of the examination of the number of follicles and the corpus luteum were tested for normality first.
The results of the Shapiro–Wilk test showed that the data on the number of primordial follicles in all groups were normally distributed (p > 0.05) so the differences between groups were tested using analysis of variance.
The results of the Shapiro–Wilk test showed that data on the number of primary follicles in all groups were normally distributed (p > 0.05) so the differences between groups were tested using analysis of variance. The results of the analysis of variance with Brown-Forsythe showed that there was a significant difference between the primary follicles between groups (p < 0.05), so further tests were needed to determine which groups were different. The results of the further test using the Games Howell test showed that the K- group was significantly different from the K+ and P2 groups.
The results of the Shapiro–Wilk test showed that data on the number of secondary follicles were not normally distributed in all groups (p > 0.05), so the differences between groups were tested using the Kruskal Wallis test. The results of the Kruskal Wallis test showed that there were significant differences in secondary follicles between groups (p < 0.05). The results of the Mann–Whitney test showed that the K- group was significantly different from the other three groups. The K- group was significantly different from the K+ group and the treatment group, but the K+ group was not significantly different from all treatment groups.
The results of the Shapiro–Wilk test showed that the data on the number of tertiary follicles were not normally distributed in all groups (p > 0.05), so the differences between groups were tested using Kruskal Wallis analysis. The results of the Kruskal Wallis test showed that there was a significant difference in tertiary follicles between groups (p < 0.05). The results of the Mann–Whitney test showed that the K- group was significantly different from the K+ group and the P2 group, but not significantly different from the P1 group. The K+ group was significantly different from all groups, both the K- group and the treatment group. There were significant differences between treatment groups.
The results of the Shapiro–Wilk test showed that the data on the number of de Graff follicles were not normally distributed in all groups (p > 0.05), so the differences between groups were tested using Kruskal Wallis analysis. The results of the Kruskal Wallis test showed that there were significant differences in DeGraff follicles between groups (p < 0.05). The results of the Mann–Whitney test showed that the K- group was significantly different from all groups, both K+ and the treatment group. The K+ group was significantly different from the K- group, but not significantly different from all treatment groups. There were significant differences between the treatment groups.
The results of the Shapiro–Wilk test showed that the data on the number of corpus luteum in the K- and K+ groups were not normally distributed (p > 0.05), so the differences between groups were tested using Kruskal Wallis analysis. The results of the Kruskal Wallis test showed that there was a significant difference in the Corpus Luteum between groups (p < 0.05). The results of the Mann–Whitney test showed that the K- group was significantly different from K+ and P1.
The K- group was significantly different from all groups, both K+ and the treatment group. The K+ group was significantly different from the K- group, but not significantly different from all treatment groups. There were significant differences between the treatment groups.
Discussion
Comparison between the normal control group and the PCOS control group with insulin resistance showed significant differences, both in insulin levels (Table 1) and glucose levels (Table 2). The PCOS group with insulin resistance showed a corresponding increase in insulin levels as evidenced by a significant value of p < 0.05 in the PCOS control group with insulin resistance compared to the normal group.
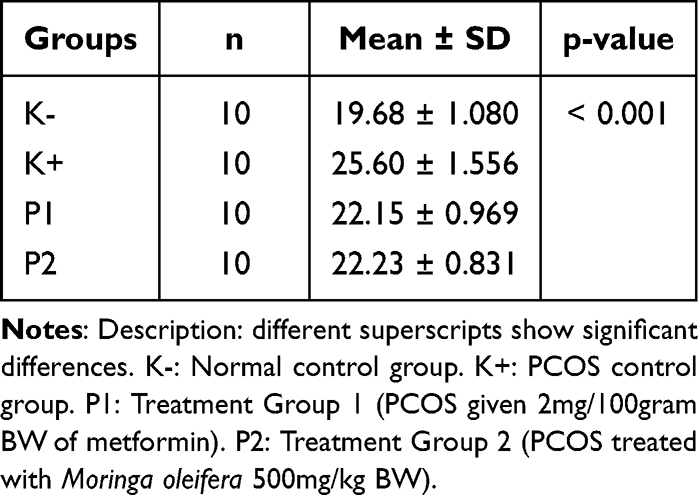 |
Table 1 Results of Differences in Insulin Levels Between Groups (p < 0.05) |
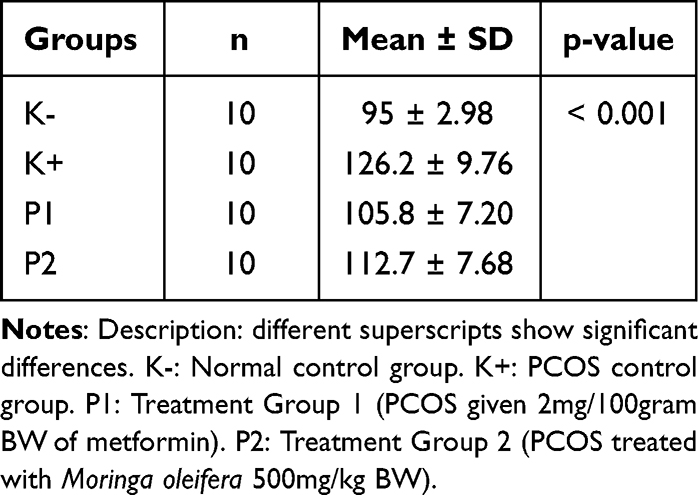 |
Table 2 Results of Differences in Blood Glucose Levels Between Groups (p < 0.05) |
The injected testosterone propionate hormone is an androgen that causes insulin resistance by decreasing the amount and effectiveness of glucose transport protein, especially GLUT-4 which plays a role in glucose transport in muscle and fat. Androgens directly inhibit insulin action in the periphery, and the liver, and indirectly affect insulin sensitivity by changing body composition through fat metabolism.25
Testosterone facilitates lipolysis and fat breakdown leading to an increase in free fatty acids. The increase in androgens and free fatty acids inhibits insulin excretion in the liver and glucose transport in muscle, which ultimately leads to hyperinsulinemia and insulin resistance.26
Glucose transporter type 4 (GLUT-4) is a transport protein for glucose that aims to carry glucose into cells. The process of translocation of GLUT-4 to the target cell surface begins with the binding of insulin and the insulin receptor subunit where this binding causes the subunit of the insulin receptor and other subunits of IRS-1 to be autophosphorylated. IRS-1 further activates PI3K which mediates the translocation of GLUT-4 to the target cell surface.27 The increase in GLUT-4 translocation causes an increase in glucose uptake from extra cells into cells. Increased glucose absorption increases the condition of insulin resistance.
We determined the condition of insulin resistance in a PCOS model. Then, the comparison of insulin resistance between normal and PCOS control groups showed a significant difference. PCOS model insulin resistance in female rats injected with testosterone propionate increased insulin and glucose levels as evidenced by a significant increase in insulin levels (Figure 1) and glucose levels (Figure 2) in the PCOS control group with insulin resistance compared to the normal group.
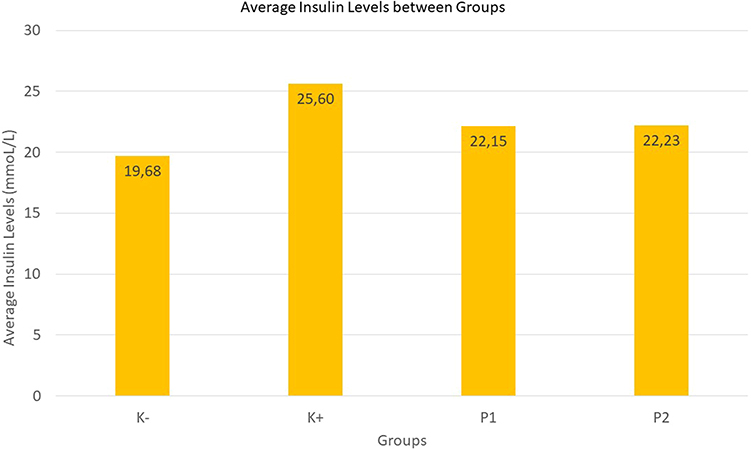 |
Figure 1 Graph of average insulin levels. |
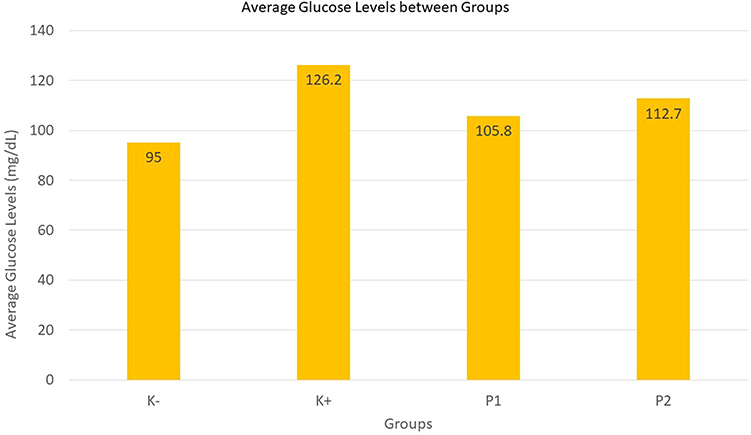 |
Figure 2 Graph of average glucose levels between groups. |
Metformin is the first therapy for PCOS by inhibiting hepatic glucose absorption, increasing peripheral glucose uptake, decreasing peripheral insulin levels, and increasing GLUT-4.15 Metformin also has a role in the endothelium and free adipose tissue in its role in insulin and glucose levels.28
Furthermore, Moringa leaf extract can reduce insulin and glucose levels in PCOS models with insulin resistance. Moringa leaf therapy treatment group and metformin treatment group for 21 days in female rats with PCOS insulin resistance model did not show significant differences. This shows that Moringa oleifera and metformin are equally good at lowering insulin levels and glucose levels. The Moringa leaf extract group and the metformin group showed significantly lower insulin (Figure 1) and glucose levels (Figure 2) than the insulin-resistant PCOS control group. This shows that the administration of Moringa leaf extract and metformin reduces insulin levels and glucose levels in female rats with PCOS insulin resistance.
Moringa leaves contain high concentrations of flavonol quercetin.17 Quercetin is a flavonoid that has strong bioactive elements with free radical, anti-inflammatory, anticancer, antihyperlipidemic, and antiplatelet effects.29
Decreased insulin levels in peripheral tissues will cause a decrease in androgens in the ovaries. Decreased insulin and IGF-1 levels can also indirectly reduce androgen levels by increasing the production of SHGB in the liver and increasing IGFBP-1 synthesis directly, quickly, and completely in both the liver and ovaries, resulting in decreased levels of IGF-I, IGF-I. II, and free testosterone.2
Moringa oleifera is a versatile plant that is consumed both as food and known in medicine. This plant is rich in nutrients with a high content of polyphenols in the form of phenolic acids, flavonoids, and glucosinolates. Moringa leaves have also been shown to have hypoglycemic activity, both aqueous extracts and organic solvents from leaves and seeds. This hypoglycemic effect is both acute and long-term administration, preventing other metabolic changes.
Moringa oleifera extract has strong antioxidant activity, so it can prevent and protect pancreatic cells from oxidative stress associated with hyperglycemic conditions.30 This plant also has isothiocyanate compounds that are important in glycemic control related to its ability to reduce resistance to insulin action and hepatic gluconeogenesis.31
Moringa oleifera leaves which have a hypoglycemic effect are attributed to their fiber content and the presence of flavonoids and phenolic acids. Several components of Moringa leaves such as kaempferol, quercetin, chlorogenic acid, gallic acid, and ellagic acid, among others, have been studied as protective agents against ROS and free radical oxidation of DNA, proteins, and lipids.32 This plant is referred to as an antidiabetic agent because it has been shown to induce strong changes in glycemic levels.33
A study in 2018 stated that Moringa oleifera leaf extract could decrease the expression of IGF-1 and expression of androgen receptors so that it could also decrease the thickness of endometrium in PCOS-Insulin Resistance model.34 Another study suggested Moringa oleifera could also be of benefit for the treatment of various metabolic and neurological conditions, including diabetes.35,36
TNF‑α is one of the aspirant molecules responsible for causing insulin resistance.37 TNF‑α expression is important in stimulating, proliferating, and steroidogenesis in ovarian follicular theca cells. In the PCOS model rat group, TNF‑α expression increased compared to the normal group. This proves that the administration of the hormone testosterone propionate for 21 days causes insulin resistance.
Metformin therapy and Moringa oleifera ethanol extract showed a decrease in TNF‑α expression (Figure 3), this proves that metformin therapy can effectively attenuate the production of pro-inflammatory cytokines, especially TNF‑α in macrophages.38 TNF‑α which is an important cytokine not only affects inflammation, but also metabolic diseases.39 Increased TNF‑α causes insulin resistance by inhibiting insulin signaling pathways, interfering with glucose transporter 4 expression and altering adipokine levels, downregulating adiponectin while increasing leptin.40 TNF‑α also interferes with lipid metabolism by increasing triglyceride and free fatty acid concentrations in the blood and altering the composition of lipoproteins such as LDL and VLDL.40
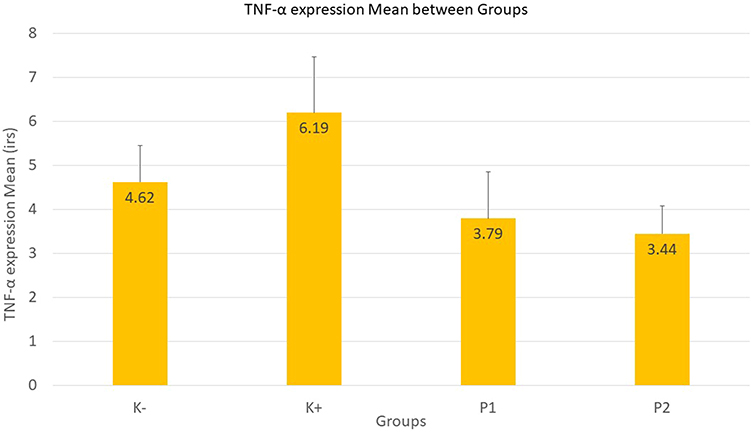 |
Figure 3 Graph of TNF-α expression mean between groups. |
Therapeutic administration of Moringa oleifera showed a significant reduction in pro-inflammatory mediators (TNF‑α) which is indicated by the presence of a chromogen brown color (Figure 4 and Table 3).41 This may play a role in increasing insulin sensitivity and reducing inflammation associated with metabolic syndrome.42 Moringa oleifera therapy could lower cholesterol, triglycerides, VLDL, LDL, and increase HDL in hypercholesterolemic rabbits, rats fed a high-fat diet and also STZ-induced diabetic rats.43
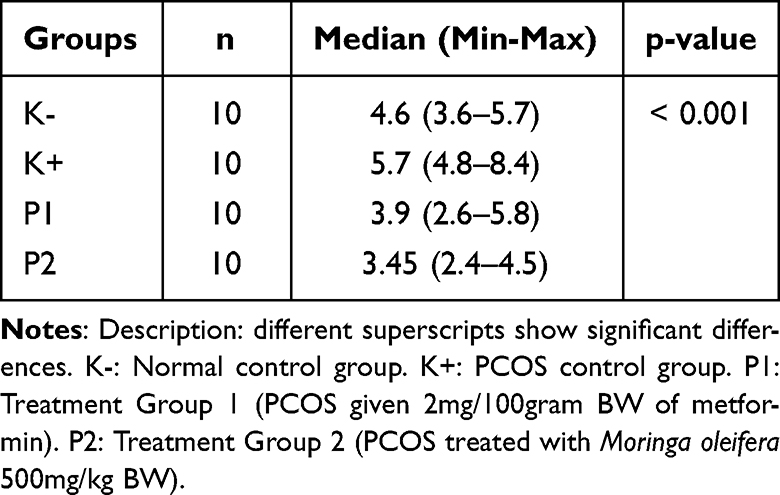 |
Table 3 Kruskal Wallis Test Results TNF-α Expression Between Groups (p < 0.05) |
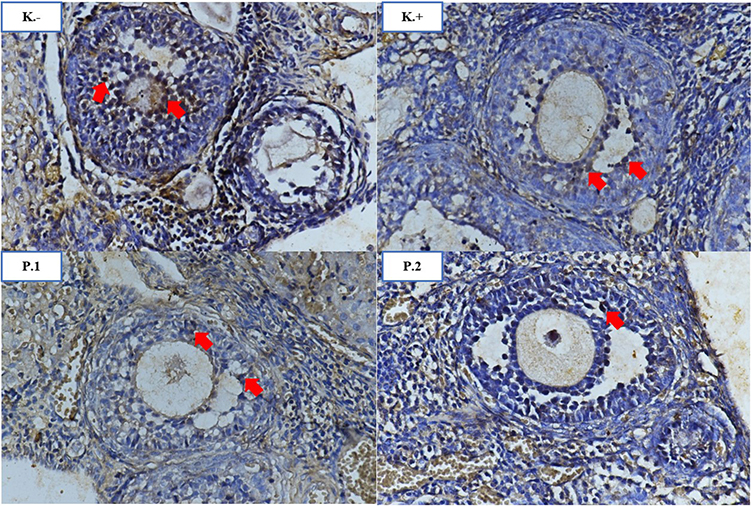 |
Figure 4 Comparison of TNF-α expression in the ovary groups (K-, K+, P1, P2). The red arrow indicates the expression of TNF-α in the granulosa cells of the follicle which is indicated by the presence of a chromogen brown color. IHC 400x. |
The growth and development of follicles are controlled by the complex system of the hypothalamic-pituitary axis of the ovary. Gonadotropin hormone plays an important role in controlling this system, the gonadotropin hormones involved in folliculogenesis are FSH and LH.44 The FSH hormone plays a role in initiating follicular growth, while LH functions in stimulating the growth and rupture of the follicle.
Primordial follicles are small follicles, and usually found close to the outer edge of the cortex, which surrounded by a single layer of flattened ovarian follicular epithelial cells. Primordial follicles are small, and usually found close to the outer edge of the cortex. When the primordial follicle is stimulated, it becomes a primary follicle. The oocyte enlarges, and the follicular cells divide. A follicle that has two layers of follicular cells is called a primary follicle. The primary follicle develops into a secondary follicle. The secondary follicles look very similar to primary follicles, except that they are larger, there are more follicular cells, and there are small accumulations of fluid in the intracellular spaces called follicular fluid. The secondary follicle develops into a de Graff follicle and starts its second meiotic division. After ovulation, the ruptured follicle collapses and fills with a blood clot (corpus haemorrhagicum) which then forms the corpus luteum.45
Based on the results of the number of primordial follicles (Figure 5), all groups did not show a significant difference (Table 4). However, there was a decrease in the number of primary (Figure 6) and secondary follicles (Figure 7) in the PCOS model rat group when compared to the normal group. While the treatment group, neither metformin therapy nor Moringa oleifera ethanol extract showed significant differences from the PCOS model rat group (Tables 5 and 6). The results of the number of tertiary follicles in the PCOS model rat group were higher than the normal group and the treatment group (Figure 8). The group given metformin showed no significant difference from the normal group but was significantly different from the group given Moringa oleifera ethanol extract therapy (Table 7.). This also happened to DeGraff follicles, the number of DeGraff follicles in the normal group was significantly different when compared to other groups, and the group treated with metformin was different from the group treated with Moringa oleifera ethanol extract (Table 8 and Figure 9). Metformin therapy and ethanol extract of Moringa oleifera did not show a significant increase in the number of follicles compared to the PCOS model rat group.
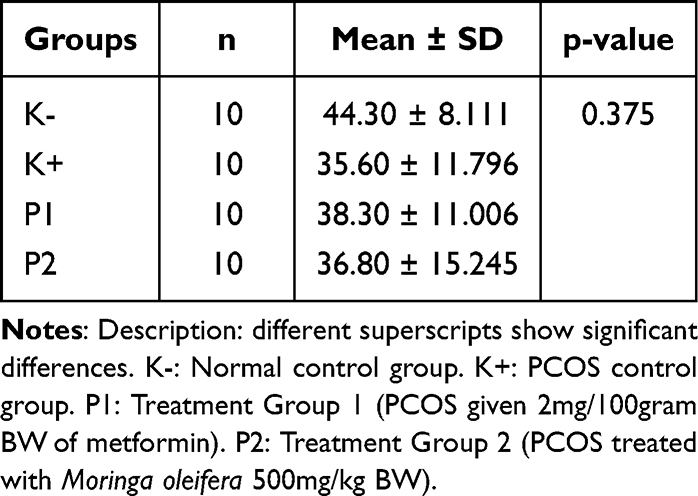 |
Table 4 The Results Showed That There Was No Significant Difference Between Primordial Follicles Between Groups (p > 0.05) |
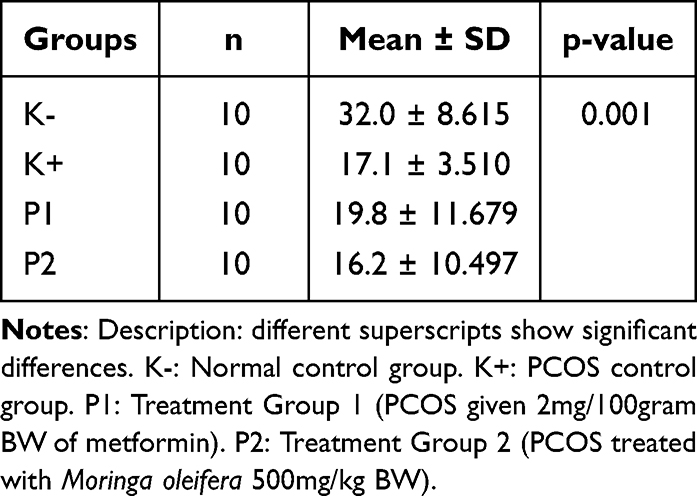 |
Table 5 Results of Primary Follicle Differences Between Groups (p < 0.05) |
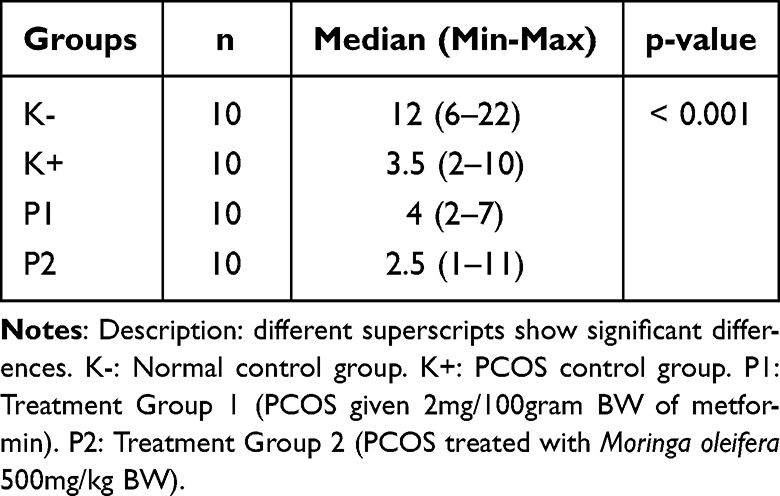 |
Table 6 Results of Secondary Follicle Differences Between Groups (p < 0.05) |
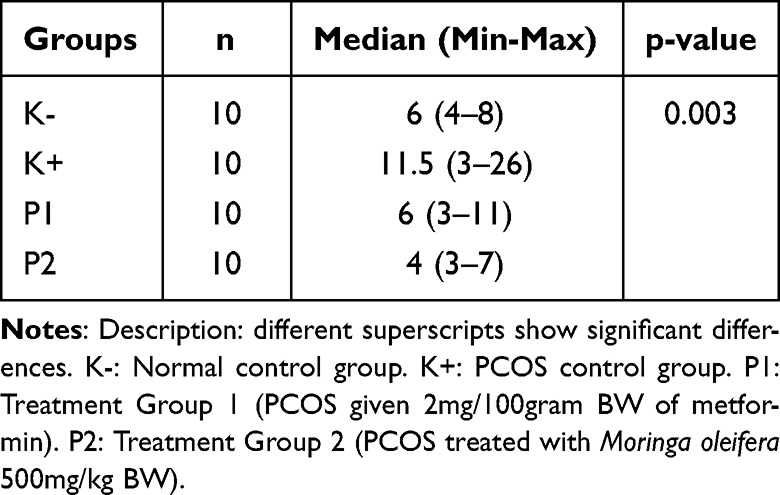 |
Table 7 Results of Tertiary Follicle Differences Between Groups (p < 0.05) |
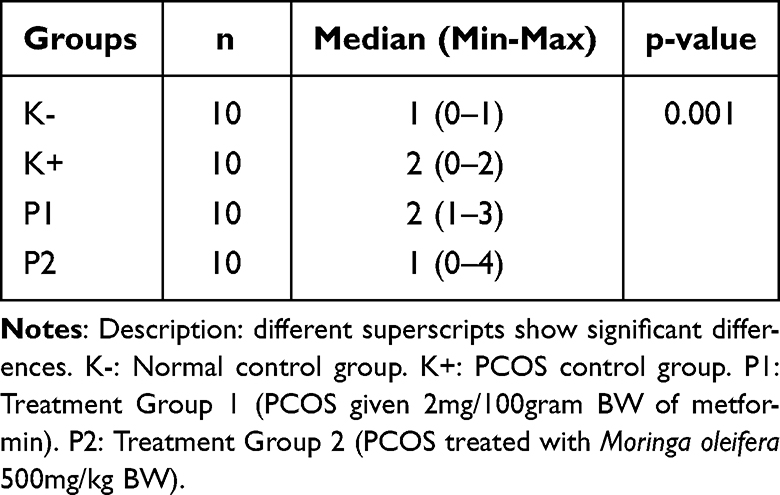 |
Table 8 Results of Follicle de Graff Differences Between Groups (p < 0.05) |
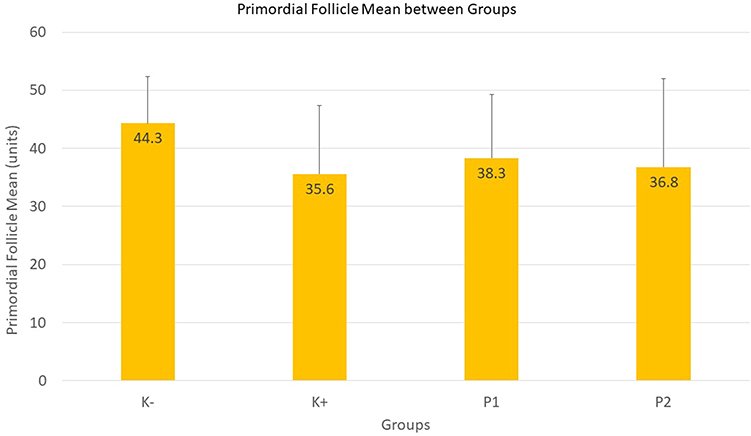 |
Figure 5 Graph of primordial follicle mean between groups. |
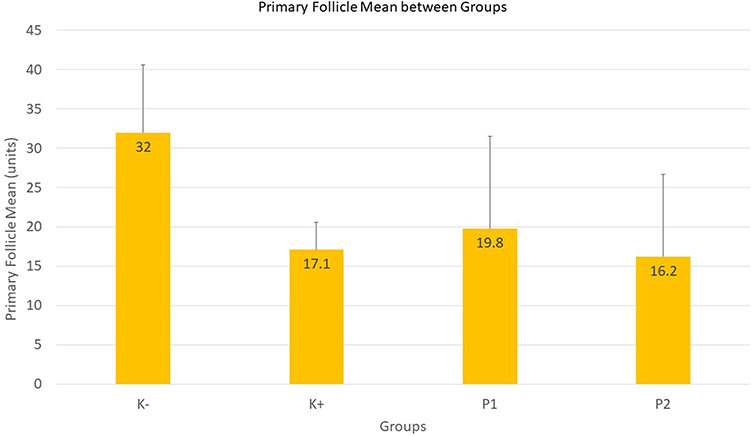 |
Figure 6 Graph of primary follicle mean between groups. |
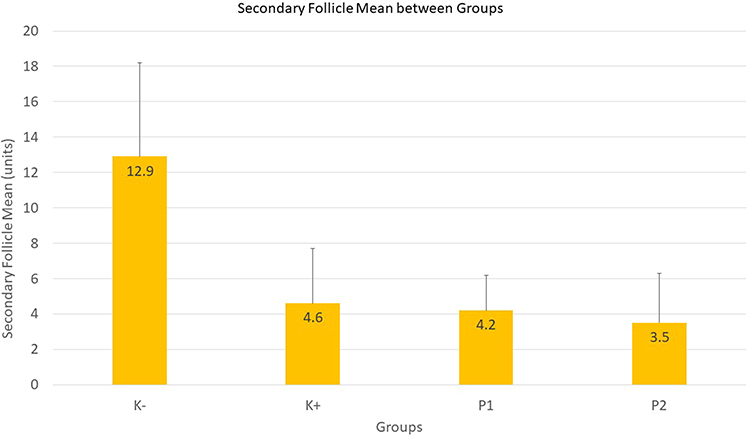 |
Figure 7 Graph of secondary follicle mean between groups. |
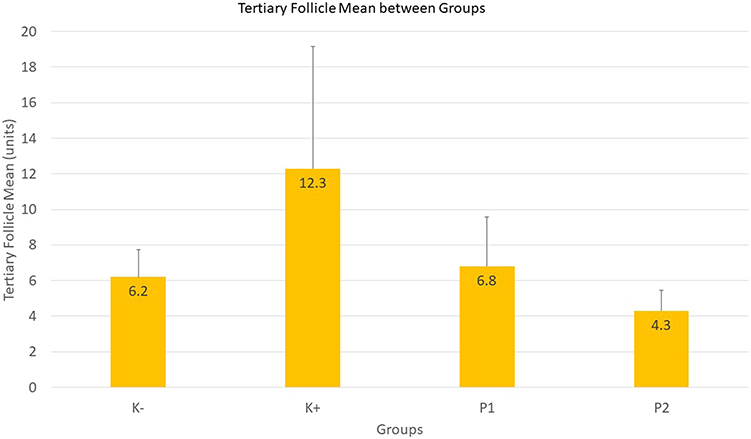 |
Figure 8 Graph of tertiary follicle mean between groups. |
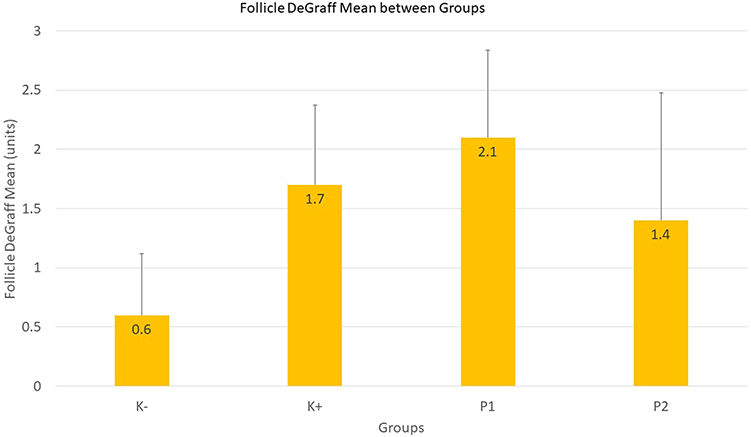 |
Figure 9 Graph of follicle DeGraff mean between groups. |
Corpus Luteum groups showed a significant difference between groups (Table 9). The normal control group was significantly different from PCOS model rat group and metformin treated group. The Normal control group was significantly different from all groups, both PCOS model rat group and the treatment group. The PCOS model rat group was significantly different from the K- group, but not significantly different from all treatment groups. There were differences between the treatment groups (Figure 10).
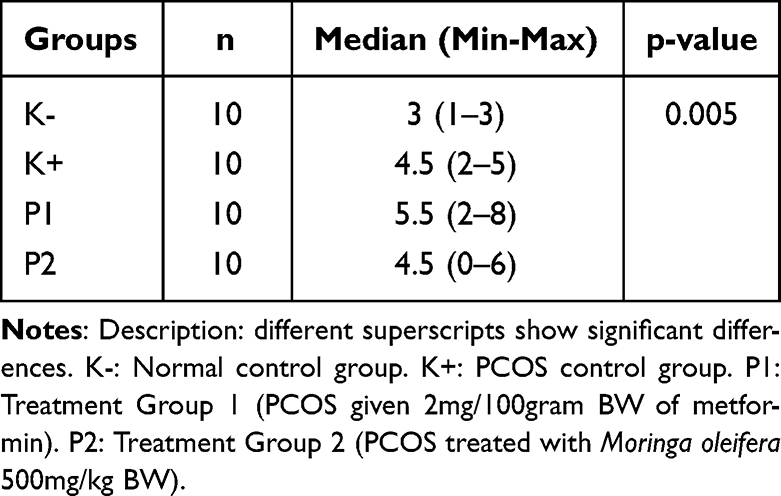 |
Table 9 Results of Differences in Corpus Luteum Between Groups (p < 0.05) |
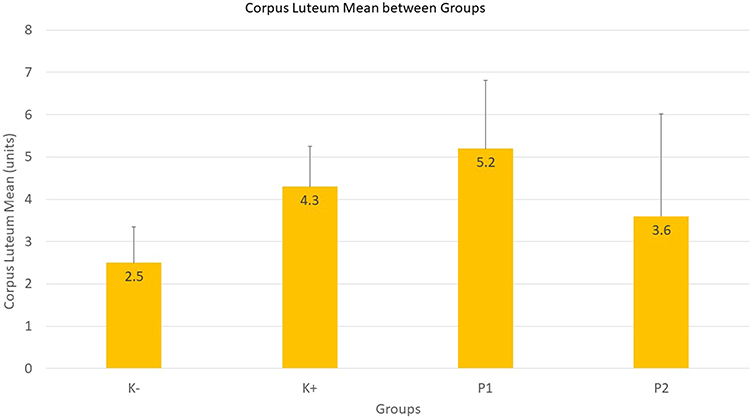 |
Figure 10 Graph of corpus luteum mean between groups. |
Ethanol extract of Moringa oleifera proved effective in reducing TNF- expression, glucose level, insulin level, and the number of follicles in PCOS model rats. Based on the results of the study, the researchers suggest further research to isolate the active compounds contained in the Moringa oleifera extract and its effectiveness against other benefits of this extract.
Ethics Approval
All of these procedures have been approved by the ethics committee of the Faculty of Veterinary Medicine, Airlangga University, Indonesia.
Acknowledgment
We wish to thank our staff in the Faculty of Veterinary Medicine and Dr. Soetomo General Hospital, the doctors, veterinarians, nurses, and the administrator for granting us the permission and necessary support to conduct our research.
Disclosure
This study was funded by the authors’ personal fund. The authors declare that there is no conflict of interest in this work.
References
1. Broskey NT, Tam CS, Sutton EF, et al. Metabolic inflexibility in women with PCOS is similar to women with type 2 diabetes. Nutr Metab. 2022;15(1):1–9
2. Rojas J, Chávez M, Olivar L, et al. Polycystic ovary syndrome, insulin resistance, and obesity: navigating the pathophysiologic labyrinth. Int J Reprod Med. 2014;2014:1–17.
3. Franks S, Berga SL. Does PCOS have developmental origins? Fertil Steril. 2012;97:2–6. doi:10.1016/j.fertnstert.2011.11.029
4. Hassani F, Oryan S, Eftekhari-Yazdi P, et al. Association between the number of retrieved mature oocytes and insulin resistance or sensitivity in infertile women polycystic ovary syndrome. Int J Fertil Steril. 2019;12(4):310. doi:10.22074/ijfs.2019.5422
5. Baptiste CG, Battista MC, Trottier A, Baillargeon JP. Insulin and hyperandrogenism in women with polycystic ovary syndrome. J Steroid Biochem Mol Biol. 2010;122(1–3):42–52. doi:10.1016/j.jsbmb.2009.12.010
6. Tang Y, Choi EJ, Han WC, et al. Moringa oleifera from Cambodia ameliorates oxidative stress, hyperglycemia, and kidney dysfunction in type 2 diabetic mice. J Med Food. 2022;20(5):502–510. doi:10.1089/jmf.2016.3792
7. Zhai HL, Wu H, Xu H, et al. Trace glucose and lipid metabolism in high androgen and high-fat diet induced polycystic ovary syndrome rats. Reprod Biol Endocrinol. 2022;10:5. doi:10.1186/1477-7827-10-5
8. Zuo T, Zhu M, Xu W. Roles of oxidative stress in polycystic ovary syndrome and cancers. Oxid Med Cell Longev. 2016;2016. doi:10.1155/2016/8589318
9. Azziz R, Carmina E, Dewailly D, et al. The androgen excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Fertil Steril. 2009;91(2): 456–488.
10. Velaga VSAR, Suryadevara N, Chee LL, Ismail NE. Phytochemical analysis and immuno-modulatory effect of moringa oleifera flowers. Int J Pharm Pharm Sci. 2017;9(6):24. doi:10.22159/ijpps.2017v9i6.16285
11. Lai H, Jia X, Yu Q, et al. High-fat diet induces significant metabolic disorders in a mouse model of polycystic ovary Syndrome. Biol Reprod. 2014; 915. doi:10.1095/biolreprod.114.120063
12. Wang MX, Yin Q, Xu X, Rat A. Model of polycystic ovary syndrome with insulin resistance induced by letrozole combined with high fat diet. Med Sci Monit. 2022;26:e922136–1.
13. Taylor H, Pal L, Sell E. Speroff’s Clinical Gynecologic Endocrinology and Infertility.
14. Guan Y, Wang D, Bu H, Zhao T, Wang H. The effect of metformin on polycystic ovary syndrome in overweight women: a systematic review and meta-analysis of randomized controlled trials. Int J Endocrinol. 2020;2020:12. doi:10.1155/2020/5150684
15. Huang Y, Sun J, Wang X, Tao X, Wang H, Tan W. Asymptomatic chronic gastritis decreases metformin tolerance in patients with type 2 diabetes. J Clin Pharm Ther. 2022;40(4):461–465.
16. Verma AR, Vijayakumar M, Mathela CS, Rao CV. In vitro and in vivo antioxidant properties of different fractions of Moringa oleifera leaves. Food Chem Toxicol. 2009;47(9):2196–2201. doi:10.1016/j.fct.2009.06.005
17. Gopalakrishnan L, Doriya K, Kumar DS. Moringa oleifera: a review on nutritive importance and its medicinal application. Food Sci Hum Wellness. 2016;5(2):49–56. doi:10.1016/j.fshw.2016.04.001
18. Sulaiman MR, Zakaria ZA, Bujarimin AS, Somchit MN, Israf DA, Moin S. Evaluation of moringa oleifera aqueous extract for antinociceptive and anti-inflammatory activities in animal models. Pharm Biol. 2008;46(12):838–845. doi:10.1080/13880200802366710
19. Patel P. Moringa oleifera-nature’s gold. Imp J Interdiscip Res. 2017;3:5.
20. Wang Y, Branicky R, Noë A, Hekimi S. Superoxide dismutases: dual roles in controlling ROS damage and regulating ROS signaling. J Cell Biol. 2018;217(6):1915. doi:10.1083/jcb.201708007
21. Muttaqin D, Santoso B. Pengaruh lama paparan androgen terhadap indeks resistensi insulin dan kadar asam lemak bebas pada serum tikus model sindroma ovarium polikistik (penelitian eksperimental dengan rattus novergicus sebagai hewan coba). Maj Obstet Ginekol. 2009;17(1):17–25.
22. Alhajj M, Farhana A. Enzyme Linked Immunosorbent Assay. StatPearls; 2022.
23. Wang X, Lin Y. Tumor necrosis factor and cancer, buddies or foes? Acta Pharmacol Sin. 2008;29(11):1275–1288. doi:10.1111/j.1745-7254.2008.00889.x
24. Nowak M, Madej J, Dziegiel P. Intensity of COX2 expression in cells of soft tissue fibrosacrcomas in dogs as related to grade of tumour malignancy. Bull Vet Inst Pulawy. 2007;51:275–279.
25. Amelia D, Santoso B, Purwanto B, Miftahussurur M, Joewono HT, Purwanto B. Effects of moringa oleifera on insulin levels and folliculogenesis in polycystic ovary syndrome model with insulin resistance. Immunol Endocr Metab Agents Med Chem. 2022;18(1):22. doi:10.2174/1871522218666180426100754
26. Wilcox G. Insulin and insulin resistance. Clin Biochem Rev. 2005;26(2):19.
27. Stöckli J, Fazakerley DJ, James DE. GLUT4 exocytosis. J Cell Sci. 2022;124(24):4147. doi:10.1242/jcs.097063
28. Diamanti-Kandarakis E, Christakou CD, Kandaraki E, Economou FN. Metformin: an old medication of new fashion: evolving new molecular mechanisms and clinical implications in polycystic ovary syndrome. Eur J Endocrinol. 2010;162(2):193–212.
29. Juźwiak S, Wójcicki J, Mokrzycki K, et al. Effect of quercetin on experimental hyperlipidemia and atherosclerosis in rabbits. Pharmacol Rep. 2005;57(5):604–609.
30. Coskun O, Kanter M, Korkmaz A, Oter S. Quercetin, a flavonoid antioxidant, prevents and protects streptozotocin-induced oxidative stress and beta-cell damage in rat pancreas. Pharmacol Res. 2005;51(2):117–123. doi:10.1016/j.phrs.2004.06.002
31. Rojas-Silva P, Tumer TB, Kuhn P, et al. Isothiocyanate-rich Moringa oleifera extract reduces weight gain, insulin resistance, and hepatic gluconeogenesis in mice. Mol Nutr Food Res. 2022;59(6): 1013–1024.
32. Sangkitikomol W, Rocejanasaroj A, Tencomnao T. Effect of Moringa oleifera on advanced glycation end-product formation and lipid metabolism gene expression in HepG2 cells. Genet Mol Res. 2022;13(1):723–735. doi:10.4238/2014.January.29.3
33. Vargas-Sánchez K, Garay-Jaramillo E, González-Reyes RE. Effects of moringa oleifera on glycaemia and insulin levels: a review of animal and human studies. Nutr. 2019;11(12):2907.
34. Setiawati I, Purwanto B, Miftahussurur M, Joewono H, Budiono B, Santoso B. Effects of moringa oleifera leaf extract to risk of endometrial hyperplasia in polycystic ovary syndrome model with insulin resistance. J Int Dent Med Res. 2018;11:1123–1129.
35. Vargas-Sánchez K, Garay-Jaramillo E, González-Reyes RE. Effects of moringa oleifera on glycaemia and insulin levels: a review of animal and human studies. Nutrients. 2022;11(12):2907.
36. Owens FS, Dada O, Cyrus JW, Adedoyin OO, Adunlin G. The effects of Moringa oleifera on blood glucose levels: a scoping review of the literature. Complement Ther Med. 2020;1(50):102362. doi:10.1016/j.ctim.2020.102362
37. Sudharshana Murthy KA, Bhandiwada A, Chandan SL, Gowda SL, Sindhusree G. Evaluation of oxidative stress and proinflammatory cytokines in gestational diabetes mellitus and their correlation with pregnancy outcome. Indian J Endocrinol Metab. 2022;22(1):79. doi:10.4103/ijem.IJEM_232_16
38. Hyun B, Shin S, Lee A, et al. Metformin Down-regulates TNF-α secretion via suppression of scavenger receptors in macrophages. Immune Netw. 2022;13(4):123. doi:10.4110/in.2013.13.4.123
39. Ziccardi P, Nappo F, Giugliano G, et al. Reduction of inflammatory cytokine concentrations and improvement of endothelial functions in obese women after weight loss over one year. Circulation. 2022;105(7): 804–809.
40. Popa C, Netea MG, Van Riel PL, Van Der Meer JWM, Stalenhoef AFH. The role of TNF-α in chronic inflammatory conditions, intermediary metabolism, and cardiovascular risk. J Lipid Res. 2007;48(4):751–762. doi:10.1194/jlr.R600021-JLR200
41. Rajanandh MG, Satishkumar MN, Elango K, Suresh B. Moringa oleifera Lam. A herbal medicine for hyperlipidemia: a pre–clinical report. Asian Pacific J Trop Dis. 2012;2(2):790–S795.
42. Jaiswal D, Kumar Rai P, Kumar A, Mehta S, Watal G. Effect of Moringa oleifera Lam. Leaves aqueous extract therapy on hyperglycemic rats. J Ethnopharmacol. 2009;123(3):392–396. doi:10.1016/j.jep.2009.03.036
43. Mbikay M. Therapeutic potential of moringa oleifera leaves in chronic hyperglycemia and dyslipidemia: a review. Front Pharmacol. 2012;3. doi:10.3389/fphar.2012.00024
44. Orisaka M, Miyazaki Y, Shirafuji A, et al. The role of pituitary gonadotropins and intraovarian regulators in follicle development: a mini‐review. Reprod Med Biol. 2022;20(2):169. doi:10.1002/rmb2.12371
45. Paxton S, Peckham M, Knibbs A, Paxton S, Knibbs A, Peckham M. The Leeds histology guide; 2003.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Level of Satisfaction Among Patients Using Insulin Administered by Pen vs Vial/Syringe. An Observational Prospective Study
Valladales-Restrepo LF, Delgado-Araujo AC, Oyuela-Gutiérrez MC, Ospina-Arzuaga HD, Machado-Alba JE
Patient Preference and Adherence 2025, 19:65-74
Published Date: 8 January 2025