Back to Journals » Orthopedic Research and Reviews » Volume 17
Effectiveness of Microfracture Augmentation in the Intercondylar Notch on Meniscal Healing: A Retrospective Comparative Study of Patients with Bucket-Handle and Longitudinal Meniscal Tears
Authors Mohebi AS, Bek B ![]() , Wardak E, Naibkhil N, Obaide M
, Wardak E, Naibkhil N, Obaide M
Received 3 July 2025
Accepted for publication 24 November 2025
Published 4 December 2025 Volume 2025:17 Pages 563—572
DOI https://doi.org/10.2147/ORR.S551256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Ahmad Shakib Mohebi,1– 3 Basira Bek,4 Emal Wardak,2 Nommanudien Naibkhil,5,6 Meena Obaide1
1Department of Orthopedic Surgery and Traumatology, Ariana Medical Complex, Kabul, Afghanistan; 2Department of Orthopedic Surgery and Traumatology, Wazir Mohammad Akbar Khan Hospital, Kabul, Afghanistan; 3Department of Orthopedic Surgery and Traumatology, Kabul Atlas Hospital, Kabul, Afghanistan; 4Department of Medicine, Kateb University, Kabul, Afghanistan; 5Department of Biochemistry, Faculty of Pharmacy, Kabul University, Kabul, Afghanistan; 6Department of Research, Ariana Medical Complex, Kabul, Afghanistan
Correspondence: Ahmad Shakib Mohebi, Department of Orthopedic Surgery and Traumatology, Kabul Atlas Hospital, District 5, Karte Parwan, Kabul, 100202, Afghanistan, Tel +93749444913, Email [email protected]
Purpose: This study aimed to evaluate the effectiveness of microfracture augmentation in the intercondylar notch on healing outcomes after arthroscopic meniscal repair, with stratification by meniscal tear type (bucket-handle vs longitudinal).
Background: Meniscal tears are common knee injuries with variable healing potential. Microfracture augmentation, which involves small perforations in the intercondylar notch to release marrow elements, has been proposed as an adjunct to enhance meniscal repair. However, the impact of this technique across different tear types remains under investigation.
Patients and Methods: In this retrospective cohort study, 173 patients aged 18– 40 years with isolated bucket-handle or longitudinal meniscal tears undergoing arthroscopic repair were included. Patients were divided into two groups: microfracture-augmented repair (n = 87) and non-microfracture repair without augmentation (n = 86). All surgeries were performed by a single senior orthopedic surgeon, and postoperative rehabilitation protocols were standardized. Healing was assessed at 12 months using Barrett’s criteria, the Apley Grinding Test, and clinical evaluation. Statistical analyses included chi-square tests, odds ratios, risk ratios, ROC curve analysis, and binary logistic regression to evaluate associations between surgical technique, tear type, and postoperative outcomes.
Results: Microfracture augmentation was associated with significantly higher overall healing rates compared to non-microfracture repair (88.5% vs 64.0%, p < 0.001). Stratified by tear type, microfracture had the greatest benefit in bucket-handle tears (79.4% vs 37.8%, p < 0.001; OR = 6.353, 95% CI: 2.275– 17.737; RR = 3.022, 95% CI: 1.503– 6.076), while healing rates were similar for longitudinal tears between techniques (94.3% vs 92.7%, p = 0.745). Age, gender, and side of injury were not significant predictors of outcomes.
Conclusion: Microfracture augmentation enhances healing after arthroscopic meniscal repair, particularly in bucket-handle tears, while longitudinal tear outcomes are favorable regardless of augmentation. These findings emphasize the importance of tear type in guiding the choice of surgical technique.
Keywords: microfracture, meniscus tear, bucket-handle, longitudinal, arthroscopy, knee
Introduction
Meniscal injury is the most frequent orthopedic injury, with 66 tears per 100,000 persons per annum.1 The meniscus is a vital part of the knee joint with a minimal blood supply and vital functional, biomechanical, and anatomical consequences. 20 to 30% of the medial meniscus and 10 to 25% of the lateral meniscus in the peripheral parts have a blood supply, and the remaining 70 to 75% are fed by diffusion. Tears in well-blood-supplied regions have considerably better outcomes than avascular regions,2 due to the lack of endogenous healing capacity and the avascular nature of the tissue, which are a big challenge in repair and require augmentation methods.1 Surgery is the primary treatment for most meniscus tears.3 Since the meniscus is a crucial structure for weight-bearing and its absence can lead to osteoarthritis and knee instability, its repair and preservation following injuries have become important issues in both research and clinical practice. Therefore, all efforts are focused on preserving the meniscus.3 Despite the the growing prevalence of meniscus repair, about 95% of meniscal surgeries are still performed as partial meniscectomies. This trend may be attributed to factors such as the longer recovery period associated with repair compared to meniscectomy, limited surgical expertise and knowledge, higher failure rates of repair, and the elevated cost of the procedure-challenges that are particularly pronounced in low-income countries.4 Considering the importance of this topic, the phrase “save the meniscus” has been mentioned in various articles and conferences.1,4,5 The success rate of restoration is increasing with new techniques and tools.4 Studies have shown that meniscal repair, along with ACL (Anterior cruciate ligament) reconstruction, reduced the Reoperation rate and revealed ideal clinical outcomes.6 Hemarthrosis during ACL reconstruction leads to the accumulation of growth factors, clot formation, and repair cells at the site of the meniscal tear, which stimulates meniscal healing even in areas with poor vascularity. Therefore, meniscal repair with ACL reconstruction increased to a >90% successful healing rate.7 So, this principle paved the way for bone marrow stimulation.6 Microfracture augmentation is one of the new methods to increase the success of repair. This method is done by creating small holes in the subchondral bone, and through it, growth factors, mesenchymal stem cells, blood cells, and vascular precursors accumulate in the joint, stimulating the formation of fibrocartilage tissue, speeding up recovery, and reducing the rate of failure.8 Recent studies show that the microfracture augmentation enhances the healing rate. A study conducted by Howarth et al (2016) on goats (Capra hircus) demonstrated that 65% of tears treated with microfracture augmentation showed complete healing. Whereas, only 12% showed complete healing in non-microfracture augmentation group. This shows the significant effect of microfracture augmentation on meniscus healing. Broader research on humans and societies is needed to demonstrate the effectiveness.9 This procedure is promising for meniscus repair but needs more research.8 Another study conducted by Sakti et al (2024) showed that microfracture augmentation in the wall of the femoral condyle has a positive effect on meniscus repair and has better functional recovery with a significant healing rate of 35.7%.10
Despite these promising results, there is limited evidence on the effectiveness of this technique in low-resource settings like Afghanistan. Factors such as surgical techniques, rehabilitation protocols, and patient compliance may vary, potentially influencing the success of the procedure. This represents a critical population gap in the literature.
This retrospective cohort study aims to evaluate the success rate of meniscal healing in Afghan patients who underwent arthroscopic meniscal repair, comparing those treated with microfracture augmentation to those who received isolated meniscal repair. The findings will help determine whether this technique offers similar benefits in a low-resource clinical context.
Materials and Methods
Study Design and Setting
This retrospective cohort study was conducted at Ariana Medical Complex, a tertiary-level orthopedic center in Afghanistan. The medical records of patients who underwent arthroscopic meniscal repair for isolated meniscal tears between January 2021 and December 2023 were systematically reviewed.
Study Population and Eligibility Criteria
Patients were divided into two groups based on whether microfracture augmentation had been performed: those who received meniscal repair with microfracture augmentation and those who underwent isolated meniscal repair without microfracture augmentation. Initially, the non-microfracture augmentation repair technique was utilized; later, the protocol was shifted to include microfracture augmentation. This study retrospectively analyzed data from these two consecutive patient groups to compare the effectiveness of meniscal repair with and without microfracture augmentation. All procedures were performed by a single senior orthopedic surgeon following identical surgical steps and postoperative rehabilitation protocols to maintain consistency across both groups.
The study included patients aged 18–40 years with confirmed isolated bucket-handle and longitudinal meniscal tears treated through arthroscopic repair. Exclusion criteria comprised concomitant ligament injuries, previous open knee surgery, history of prior knee surgery, other types of tears, or age outside the specified range (Figure 1).
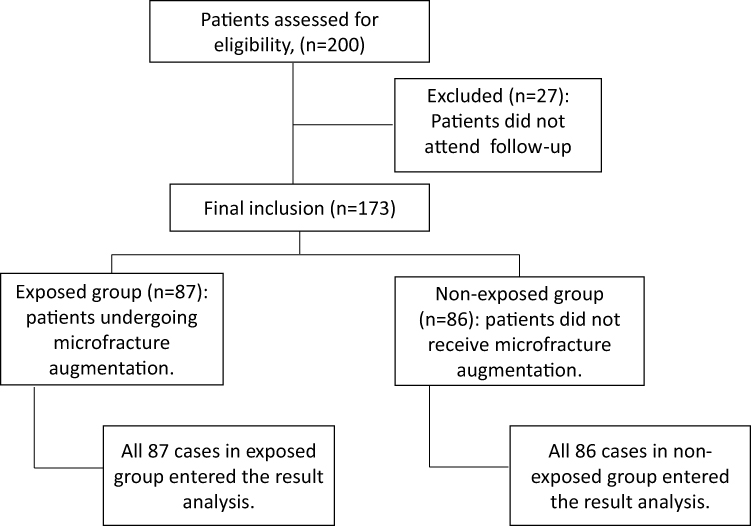 |
Figure 1 Flowchart of patient exclusion, inclusion and analysis. |
Surgical Technique and Postoperative Rehabilitation Protocol
All procedures were conducted under spinal anesthesia using the inside-out technique for meniscal repair. In this study, the microfracture augmentation refers to small perforations in the intercondylar notch to release marrow elements enhancing meniscal repair. In the microfracture augmentation group, microfracture augmentation was performed in some patients using a microfracture awl at 45° in the intercondylar notch adjacent to ACL (Anterior cruciate ligament) and PCL (Posterior cruciate ligament) origin. In each case, about 10 holes were made to a depth of 3–4 mm. In some patients, the same procedure was performed using a 1.2 mm Kirschner wire under low rotational speed and continuous saline irrigation to minimize thermal necrosis. Seven holes were made at the same angle but to a depth of 2-4 mm to prevent excessive thermal damage while maintaining marrow access. In both methods, the distance between the holes was approximately 2–3 mm, and penetration into the bone marrow was confirmed by observing the effusion fat droplets and marrow bleeding, according to the recommendations of the Steadman et al.11
Postoperative care followed a standardized rehabilitation protocol. During the first three weeks, the knee was immobilized in a full extension using a brace, and the patient was completely non-weight-bearing for the first two weeks. Partial weight-bearing was gradually initiated during weeks 3–4. Progressing to full weight-bearing by the end of the first month after surgery. Isometric quadriceps exercise and active straight-leg raising were recommended from the early postoperative period to prevent muscle atrophy. During the second postoperative month, patients were allowed to begin active and passive range-of-motion (ROM) exercises and achieve approximately 45° of knee flexion. After three months, patients were referred to physiotherapy for quadriceps and hamstring strengthening exercises and joint stability exercises. A concise summary of the postoperative rehabilitation protocol is provided in Table 1 for greater clarity.
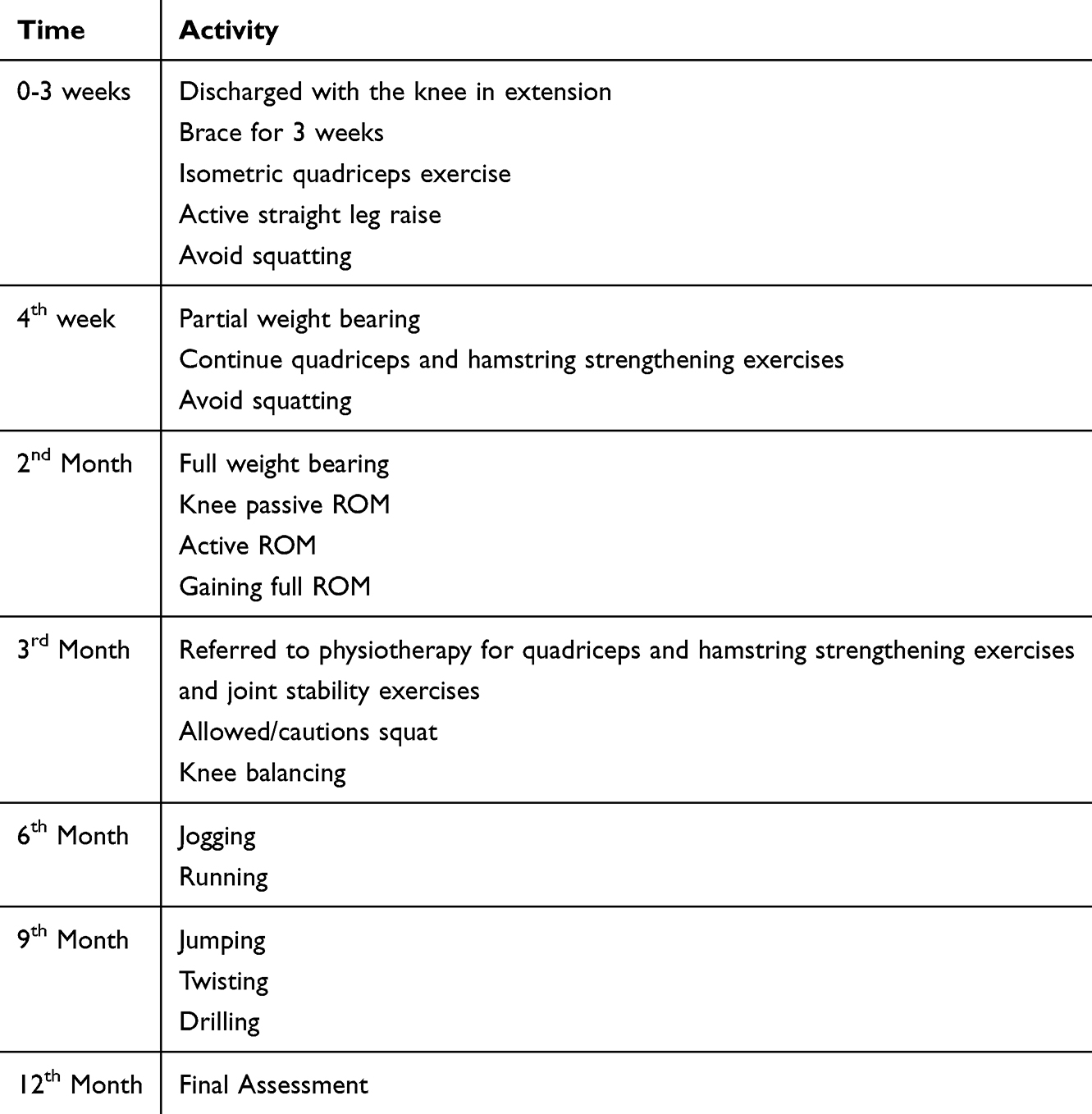 |
Table 1 Postoperative Rehabilitation Protocol |
All the patients underwent perioperative MRI (0.2–0.4 Tesla) to evaluate meniscus injury. However, MRI confirmed about 41.0% of the cases. For the patients with negative MRI the decision to proceed with surgery was based on physical examination and clinical evaluation. Outcome assessment occurred after 12-month follow-up period. Postoperative evaluation incorporated Barrett’s criteria and the Apley Grinding Test, with healing defined by the absence of joint line tenderness, effusion, mechanical locking, and a negative McMurray test. Cases exhibiting any of these clinical signs or requiring reoperation were classified as treatment failures.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics (version 26; IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means ± standard deviation (SD), and categorical variables as frequencies and percentages.
Associations between surgical technique, tear type, side of injury, gender, and postoperative outcomes (healing vs reoperation) were evaluated using the Pearson chi-square (χ2) test, with Phi and Cramer’s V values reported as measures of effect size. Crude odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to estimate the likelihood of reoperation between groups, and cohort-specific risk ratios (RRs) were computed to assess the relative probability of reoperation and healing for each technique.
A post-hoc power analysis was conducted to verify whether the achieved sample size provided ≥80% power to detect the observed effect sizes across tear types and surgical techniques. Receiver Operating Characteristic (ROC) curve analysis was performed to evaluate the predictive value of age for postoperative healing, with the area under the curve (AUC) and Youden’s index reported.
Binary logistic regression was used to examine the independent association between age and postoperative healing within surgical subgroups and tear types. Model fit was assessed using the chi-square goodness-of-fit test and Nagelkerke R2. A p-value < 0.05 was considered statistically significant.
Ethics Approval
The study was approved by the Institutional Review Board of Ariana Medical Complex with approval number (AF, AMC, IRB, REC 02, 25/12/2024). Informed consent was waived because of the retrospective nature of this study. Access to the data was restricted to the researchers. The confidentiality of all patients was protected, and no names or medical record numbers were used. Privacy and confidentiality were assured. The study was carried out following the Declaration of Helsinki.
Results
A total of 173 patients completed the 12-month follow-up period, achieving a follow-up rate of 86.5%. Of these, 15% were female and 85% male. The mean age was 25.47 ± 5.86 years (range: 18–40) in the non-microfracture group and 26.32 ± 6.06 years in the microfracture augmentation group. Patients in the non-microfracture group underwent meniscal repair without microfracture augmentation, whereas those in the microfracture augmentation group received meniscal repair combined with microfracture augmentation. Overall, 94 patients (54.3%) presented with longitudinal tears and 79 (45.6%) with bucket-handle tears (Table 2).
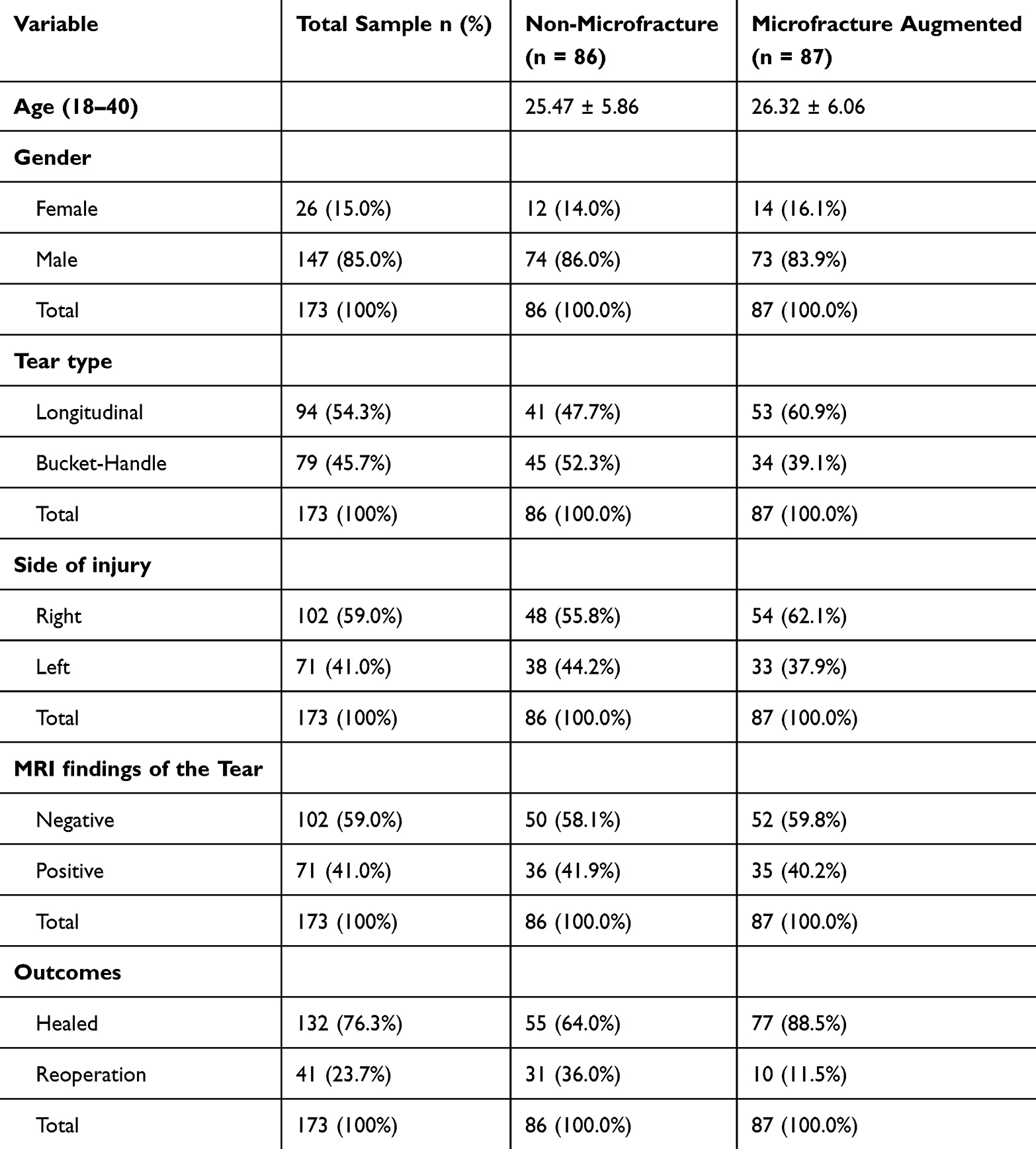 |
Table 2 Baseline Characteristics of Patients According to Microfracture Augmentation Status |
Of the 87 patients treated with microfracture augmentation, 77 (88.5%) achieved complete healing and returned to their pre-injury functional level, while 10 (11.5%) experienced failure requiring reoperation. In comparison, among the 86 patients treated without microfracture augmentation, 55 (64.0%) healed successfully and 31 (36.0%) underwent reoperation. This difference in healing outcomes between the two techniques was statistically significant (χ2 = 14.417, p < 0.001), demonstrating a clear advantage of the microfracture-augmented procedure.
A strong and significant association was also found between the type of tear and postoperative outcome (χ2 = 34.135, p = 0.003). Healing was achieved in 93.6% (88/94) of patients with longitudinal tears, whereas only 55.7% (44/79) of patients with bucket-handle tears healed successfully. Conversely, failure occurred in 44.3% (35/79) of bucket-handle tears, underscoring the greater complexity and poorer prognosis of this tear type compared with longitudinal tears.
Among patients with longitudinal tears (n = 94), 38 of 41 patients (92.7%) in the non-microfracture group achieved complete healing, while 3 (7.3%) required reoperation. In the microfracture-augmented group, 50 of 53 patients (94.3%) healed, and 3 (5.7%) required reoperation. The difference between the two techniques was not statistically significant (χ2(1) = 0.106, p = 0.745).
Post-hoc power analysis revealed a very small effect size (Cohen’s h = 0.094) and an observed power of only 15%, indicating that the two techniques produced nearly identical healing rates and that the sample size was insufficient to detect minor differences (Table 3).
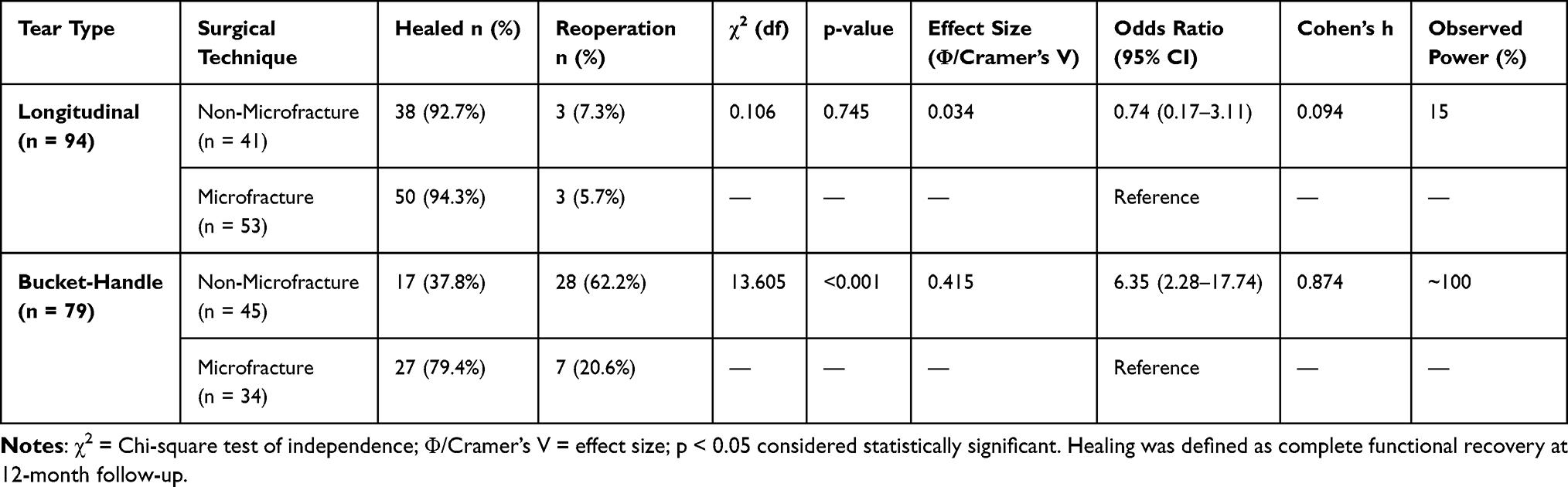 |
Table 3 Comparison of Healing Outcomes Between Microfracture-Augmented and Non-Microfracture Meniscal Repairs Stratified by Tear Type |
In patients with bucket-handle tears (n = 79), a striking difference was observed between the two surgical approaches. In the non-microfracture group, 17 of 45 patients (37.8%) healed, while 28 (62.2%) required reoperation. Conversely, in the microfracture-augmented group, 27 of 34 patients (79.4%) healed, and only 7 (20.6%) required reoperation. This difference was highly significant (χ2(1) = 13.605, p < 0.001), with a moderate-to-strong association between technique and outcome (Φ = 0.415, Cramer’s V = 0.415, p < 0.001).
The odds of reoperation were markedly higher in the non-microfracture group (OR = 6.353, 95% CI: 2.275–17.737). Cohort-specific estimates revealed that non-microfracture patients had a threefold greater risk of reoperation (RR = 3.022, 95% CI: 1.503–6.076) and a significantly reduced likelihood of healing (RR = 0.476, 95% CI: 0.315–0.718).
Post-hoc power analysis confirmed a large effect size (Cohen’s h = 0.874) and nearly 100% statistical power, reinforcing the robustness of the observed difference in outcomes between techniques for bucket-handle tears.
Receiver Operating Characteristic (ROC) curve analysis was used to evaluate the predictive value of age for postoperative healing. When analyzed across all patients, the area under the curve (AUC) was 0.309 for the non-microfracture group and 0.456 for the microfracture group, indicating that age was not a reliable predictor of surgical outcome.
Among patients with longitudinal tears, the AUC values were 0.654 (non-microfracture) and 0.623 (microfracture-augmented), suggesting poor-to-fair discrimination. ROC coordinate analysis indicated that younger patients (< 20 years) tended to exhibit slightly higher sensitivity for healing (62–78%), but specificity remained modest (33–67%). Based on Youden’s index, an approximate cutoff of 19–20 years offered the best balance between sensitivity and specificity for both microfracture augmentation and non-microfracture technique group. However, the low AUC values emphasize that age alone is a weak prognostic factor.
In bucket-handle tears, ROC curves yielded AUC values of 0.477 and 0.481 for non-microfracture and microfracture-augmented groups, respectively, demonstrating that age did not meaningfully influence healing in this tear type. No clear age threshold could effectively differentiate healed from reoperated patients with different repair techniques.
Binary logistic regression was performed further to assess the relationship between age and healing outcomes. In the non-microfracture group, the model was statistically significant (χ2(1) = 5.64, p = 0.018), explaining 6.3–8.7% of the variance in outcome. Increasing age was associated with a decreased likelihood of healing (B = −0.093, p = 0.022, OR = 0.911), indicating that each additional year of age reduced the odds of successful healing by approximately 8.9%. In the microfracture-augmented group, age was not a significant predictor (χ2(1) = 0.42, p = 0.515; OR = 0.965), and the model accounted for less than 1% of the variance.
When analyzed by tear type, age remained a nonsignificant predictor in both longitudinal and bucket-handle subgroups (all p > 0.30). The models had limited explanatory power (Nagelkerke R2 < 0.08) and poor classification accuracy, reinforcing that age alone does not independently predict postoperative healing (Table 4).
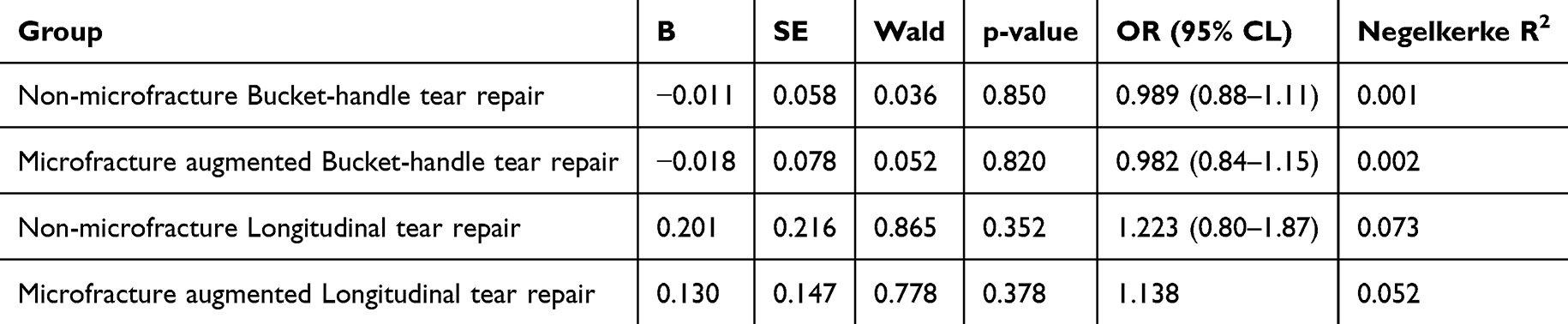 |
Table 4 Logistic Regression Analysis of Age as a Predictor of Healing Outcome |
Neither gender nor side of injury demonstrated any statistically significant association with healing outcomes in either group.
Discussion
This study uncovered substantial clinical outcomes, a significant difference in the healing rates of meniscus repair in the microfracture augmentation group compared to the non-microfracture group at a 12-month follow-up. In the microfracture augmentation group, the meniscus healing was higher, 88.5%, compared to the non-microfracture group, 64.0% without considering the tear types. The overall results in our study are similar to previous studies, which have shown improved healing from 35.7% to 100.0% in healing rate with microfracture augmentation.10,12,13 Howarth et al conducted a study on goats and examined both longitudinal and transverse tears with and without microfracture. After 6 months of follow-up, meniscal tears healed in 87% of menisci treated with bone marrow-stimulating microfracture, compared with only 29% of those without microfracture. Sakti et al, Sakti conducted a study on meniscal tears in the red-white zone reported better meniscal healing outcomes in the microfracture augmentation group (p = 0.001), 35.7% in comparison to 0% the group did not received microfracture augmentation.10 In addition, a randomized controlled trial by Kaminski et al reported a 100.0% healing rate with 6 to 7 microfracture augmentation holes in the intercondylar notch in 23 patients with better functional outcomes and pain levels.12
In the current study, we showed a failure rate of 11.5% in our microfracture augmentation group, which was comparable to the study of Dean et al applied intercondylar notch marrow venting augmentation with isolated meniscus repair and represented a 12.9% failure rate, which was a similar failure rate to meniscus repair with concomitant ACL repair.13 This result emphasizes the potential effect and importance of the microfracture augmentation technique in meniscal healing.
In our study, the clinical outcomes were significantly associated with the type of meniscal tear. The bucket-handle meniscal repair failure rate ranges from 0%,14–16 up to 75%.17 However, in our study, we found a 44.3% failure rate for bucket-handle meniscal tears. Our finding was comparable to Krych et al, who demonstrated a 38% isolated meniscal repair failure rate.18 A meta-analysis study represented a higher risk of failure for bucket-handle meniscal repair than longitudinal tears.19 On the other hand, our study showed microfracture augmentation has a potential role in the healing rate of complex tears as bucket-handle tears, which present challenges such as reduced vascularity and large displacement for healing. In contrast, among patients with longitudinal tears, healing rates were high in both groups with no statistically significant difference between techniques. These findings are supported by those of Screpis et al, who reported that longitudinal meniscal tears have excellent biological potential for healing, with a healing rate exceeding 90%.20 Moreover, globally, the longitudinal tear failure rate is lower (6–28%) with or without ACL reconstruction.21 In our study age showed a minor influence on healing outcomes, as evidenced by low AUC values in ROC analysis and nonsignificant results in regression analysis. We found a slightly higher sensitivity for healing among younger ages, but it was not an independent determinant of outcome. Our finding is close to that of Rothermel et al, who reported that age alone is not an independent predictor of meniscal repair failure, and no significant difference in failure rate was found between younger and older age groups.22
The microfracture augmentation technique was used based on the technique described by Steadman.11 It is one of the new methods to increase the success of repair by creating small holes in the subchondral bone, and through it, growth factors, mesenchymal stem cells, blood cells, and vascular precursors accumulate in the joint, stimulating the formation of fibrocartilage tissue, speeding up recovery, and reducing the rate of failure. We used the inside-out technique for all meniscal repairs. Although surgeons prefer the all-inside technique more due to the invention of advanced techniques, the inside-out is still the gold standard for meniscal repair, more economical, and advantageous.22,23
Meniscus repair with marrow venting augmentation is recommended as the best treatment option for young patients who have suffered an isolated meniscus tear because it is cost-effective and results in a higher number of quality-adjusted life years.24 Loss to follow-up is a significant challenge to the validity and reliability of study findings and can lead to bias. Epidemiologists suggested multiple acceptable follow-up rates, from 50% as sufficient to 70% as very good or 80% as optimal.25 Thus, our study’s 86.5% follow-up rate is ideal and ensures that the findings are less influenced by attrition bias. Our study has several notable strengths. First, it includes a relatively large number of cases, enhancing the reliability of the findings. Second, microfracture augmentation was performed using both an awl and a Kirschner wire, which are cost-effective, widely available, and do not require additional specialized skills or novel arthroscopic devices. Third, all procedures were conducted by a single senior orthopedic surgeon with extensive experience in arthroscopic techniques, ensuring consistency in both surgical execution and follow-up evaluation. Finally, the study specifically evaluates the effectiveness of microfracture augmentation across different tear types, allowing for a more nuanced understanding of its clinical benefits.
We recommend conducting further large-scale, randomized controlled trials with standardized microfracture augmentation protocols and long-term follow-up to validate our findings. As a cost-effective and low-risk adjunct, microfracture augmentation has the potential to improve patient outcomes and satisfaction. Orthopedic surgeons should consider incorporating microfracture augmentation into clinical practice and ensure that future surgeons are trained in evidence-based techniques. This study is intended to serve as a reference and foundation for future research, particularly on the role of microfracture augmentation in meniscal repair.
Limitations
Although these findings provide valuable insights, this study has several limitations. This study had a retrospective design, which has a lower degree of evidence than that of randomized clinical trials and prospective studies. In addition, the study had a short duration of follow-up which may have affected the result but it provides sufficient time to evaluate clinical outcomes after meniscal repair as reported in previous studies.10 Further research with longer follow-ups is needed to support the findings of this study. This study focused on only two types of tears longitudinal and bucket-handle, future research should investigate further tear types to provide more insights. Furthermore, we did not utilize knee-specific score or PROMIS and a second-look arthroscopy or repeat advanced imaging like MRI for healing assessment. Further studies are needed to fill this gap by utilizing knee-specific scoring system, MRI, and second look arthroscopy for the assessment of post-surgical outcomes.
However, we evaluated all the patients clinically and with physical examination. Failure was defined as reoperation with meniscectomy or revision meniscal repair. Barrett’s criteria and physical examination are more favored, non-invasive, and free of charge in postoperative recovery measurement and follow-up.26
Conclusion
The primary aim of this study was to evaluate the effect of microfracture augmentation on healing outcomes in patients undergoing repair of longitudinal and bucket-handle meniscal tears. Microfracture augmentation significantly improved healing and reduced reoperation rates in bucket-handle tears, whereas outcomes were comparable between techniques in longitudinal tears. These findings suggest that microfracture augmentation enhances meniscal repair by releasing bone marrow elements at the repair site, serving as an effective biological augmentation method to promote tissue healing.
Consent for Publication
All authors reviewed the manuscript and approved its submission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Bansal S, Floyd ER, Kowalski M, et al. Meniscal repair: the current state and recent advances in augmentation. J Orthopaedic Res. 2021;39(7):1368–1382. doi:10.1002/jor.25021
2. Bhan K. Meniscal tears: current understanding, diagnosis, and management. Cureus. 2020. doi:10.7759/cureus.8590
3. Luvsannyam E, Jain MS, Leitao AR, Maikawa N, Leitao AE. Meniscus tear: pathology, incidence, and management. Cureus. 2022. doi:10.7759/cureus.25121
4. Jha V. Editorial commentary: rate of meniscal repair versus meniscectomy has improved and should continue to improve. Arthroscopy. 2024;S0749806324007874. doi:10.1016/j.arthro.2024.10.006
5. Pujol N, Beaufils P. Save the meniscus again! Knee Surg Sports Traumatol Arthrosc. 2019;27(2):341–342. doi:10.1007/s00167-018-5325-4
6. Carlson Strother CR, Saris DBF, Verdonk P, Nakamura N, Krych AJ. Biological augmentation to promote meniscus repair: from basic science to clinic application—state of the art. J ISAKOS. 2020;5(3):150–157. doi:10.1136/jisakos-2019-000426
7. Toman CV, Dunn WR, Spindler KP, et al. Success of meniscal repair at anterior cruciate ligament reconstruction. Am J Sports Med. 2009;37(6):1111–1115. doi:10.1177/0363546509337010
8. Za P, Ambrosio L, Vasta S, et al. How to improve meniscal repair through biological augmentation: a narrative review. JCM. 2024;13(16):4688. doi:10.3390/jcm13164688
9. Howarth WR, Brochard K, Campbell SE, Grogan BF. Effect of microfracture on meniscal tear healing in a goat (Capra hircus) model. Orthopedics. 2016;39(2):105–110. doi:10.3928/01477447-20160119-04
10. Sakti M, Singjie LC, Horas N, Nelwan DA. The effectiveness of microfracture augmentation on the wall of femoral condyle in meniscal healing among patients with meniscus tears after sports injury. J Orthop Surg. 2024;32(3):10225536241306169. doi:10.1177/10225536241306169
11. Steadman JR, Rodkey WG, Rodrigo JJ. Microfracture: surgical technique and rehabilitation to treat chondral defects. Clin Orthop Relat Res. 2001;(391 Suppl):S362–369. doi:10.1097/00003086-200110001-00033
12. Kaminski R, Kulinski K, Kozar-Kaminska K, Wasko MK, Langner M, Pomianowski S. Repair augmentation of unstable, complete vertical meniscal tears with bone marrow venting procedure: a prospective, randomized, double-blind, parallel-group, placebo-controlled study. Arthroscopy. 2019;35(5):1500–1508.e1. doi:10.1016/j.arthro.2018.11.056
13. Dean CS, Chahla J, Matheny LM, Mitchell JJ, LaPrade RF. Outcomes after biologically augmented isolated meniscal repair with marrow venting are comparable with those after meniscal repair with concomitant anterior cruciate ligament reconstruction. Am J Sports Med. 2017;45(6):1341–1348. doi:10.1177/0363546516686968
14. Ahn JH, Kim K, Wang JH, Kyung BS, Seo MC, Lee SH. Arthroscopic repair of bucket‐handle tears of the lateral meniscus. Knee Surg Sports Traumatol Arthrosc. 2015;23(1):205–210. doi:10.1007/s00167-013-2764-9
15. Lucas G, Accadbled F, Violas P, Sales De Gauzy J, Knörr J. Isolated meniscal injuries in paediatric patients: outcomes after arthroscopic repair. Orthop Traumatol Surg Res. 2015;101(2):173–177. doi:10.1016/j.otsr.2014.12.006
16. Moatshe G, Cinque ME, Godin JA, Vap AR, Chahla J, LaPrade RF. Comparable outcomes after bucket-handle meniscal repair and vertical meniscal repair can be achieved at a minimum 2 years’ follow-up. Am J Sports Med. 2017;45(13):3104–3110. doi:10.1177/0363546517719244
17. Tucciarone A, Godente L, Fabbrini R, Garro L, Salate Santone F, Chillemi C. Meniscal tear repaired with Fast-Fix sutures: clinical results in stable versus ACL-deficient knees. Arch Orthop Trauma Surg. 2012;132(3):349–356. doi:10.1007/s00402-011-1391-5
18. Krych AJ, McIntosh AL, Voll AE, Stuart MJ, Dahm DL. Arthroscopic repair of isolated meniscal tears in patients 18 years and younger. Am J Sports Med. 2008;36(7):1283–1289. doi:10.1177/0363546508314411
19. Costa GG, Grassi A, Zocco G, et al. What is the failure rate after arthroscopic repair of bucket-handle meniscal tears? A systematic review and meta-analysis. Am J Sports Med. 2022;50(6):1742–1752. doi:10.1177/03635465211015425
20. Screpis D, Qordja F, De Berardinis L, et al. Saving the meniscus: a retrospective observational study of the incidence, treatment, and failure rate of the main meniscal tear types at 24-month follow-up. J Clin Med. 2025;14(10):3350. doi:10.3390/jcm14103350
21. Alhamdi H, Foissey C, Vieira TD, et al. High failure rate after medial meniscus bucket handle tears repair in the stable knee. Orthop Traumatol Surg Res. 2024;110(4):103737. doi:10.1016/j.otsr.2023.103737
22. Pace JL, Inclan PM, Matava MJ. Inside-out medial meniscal repair: improved surgical exposure with a sub-semimembranosus approach. Arthroscopy Techniq. 2021;10(2):e507–e517. doi:10.1016/j.eats.2020.10.032
23. Nelson CG, Bonner KF. Inside-out meniscus repair. Arthroscopy Techniq. 2013;2(4):e453–e460. doi:10.1016/j.eats.2013.07.006
24. Oeding JF, Berlinberg EJ, Lu Y, et al. Platelet-rich plasma and marrow venting may serve as cost-effective augmentation techniques for isolated meniscal repair: a decision-analytical markov model–based analysis. Arthroscopy. 2023;39(9):2058–2068. doi:10.1016/j.arthro.2023.02.018
25. Kristman V, Manno M, Côté P. Loss to follow-up in cohort studies: how much is too much? Eur J Epidemiol. 2004;19(8):751–760. doi:10.1023/b:ejep.0000036568.02655.f8
26. Karagöz B, Bombaci H. Evaluation of the relationship between clinical findings and magnetic resonance imaging findings of patients with arthroscopic meniscus repair. Middle Black Sea J Health Sci. 2021;7(3):429–435. doi:10.19127/mbsjohs.994952
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.