Back to Journals » Clinical Ophthalmology » Volume 16
Effectiveness of Current Treatments for Wet Age-Related Macular Degeneration in Japan: A Systematic Review and Pooled Data Analysis
Authors Takahashi K, Iida T, Ishida S, Crawford B, Sakai Y, Mochizuki A, Tsujiuchi R, Tanaka S, Imai K
Received 20 October 2021
Accepted for publication 4 February 2022
Published 25 February 2022 Volume 2022:16 Pages 531—540
DOI https://doi.org/10.2147/OPTH.S345403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kanji Takahashi,1 Tomohiro Iida,2 Susumu Ishida,3 Bruce Crawford,4 Yoko Sakai,4 Akikazu Mochizuki,5 Ryuta Tsujiuchi,5 Satoru Tanaka,5 Kota Imai5
1Department of Ophthalmology, Kansai Medical University, Hirakata, Osaka, Japan; 2Department of Ophthalmology, Tokyo Women’s Medical University, Shinjuku, Tokyo, Japan; 3Department of Ophthalmology, Graduate School of Medicine, Hokkaido University, Sapporo, Hokkaido, Japan; 4Syneos Health Clinical K.K., Chuo-ku, Tokyo, Japan; 5Novartis Pharma K.K., Minato-ku, Tokyo, Japan
Correspondence: Akikazu Mochizuki, Novartis Pharma K.K., 23-1, Toranomon 1-chome, Minato-ku, Tokyo, Japan, Tel +81 3 6899 8000, Fax +81 3 6257 3634, Email [email protected]
Purpose: We conducted a systematic review to investigate the effectiveness of clinical treatments for wet age-related macular degeneration (wAMD) in Japanese patients in the decade since anti-vascular endothelial growth factor (VEGF) therapies were introduced.
Methods: PubMed was searched for articles published in English between 1 January 2008 and 30 September 2018 using a multistring search strategy. Reviews were scanned for additional relevant studies and select gray literature was evaluated. Mean and/or median for the logarithm of the minimum angle of resolution (logMAR) visual acuity (VA), central retinal thickness (CRT), and the number of injections after 12 months of treatment were calculated using extracted data. Data were stratified by disease type and treatment modality.
Results: Of 335 studies identified, 94 were selected for data extraction (147 treatment arms; typical AMD, n = 25; polypoidal choroidal vasculopathy [PCV], n = 85). Mean (median) logMAR VA was 0.44 (0.32) for typical AMD and 0.34 (0.31) for PCV; the respective mean number of anti-VEGF injections was 5.6 and 4.6. The mean CRT was approximately 220 μm for both groups. For typical AMD, anti-VEGF monotherapy resulted in better VA outcomes than photodynamic therapy (PDT) alone. For PCV, anti-VEGF monotherapy or anti-VEGF plus PDT combination therapy resulted in better VA and CRT outcomes than PDT monotherapy. Combination therapy required fewer injections than anti-VEGF monotherapy (PCV, 3.2 versus 5.3).
Conclusion: wAMD treatment has advanced dramatically in the years since anti-VEGF drugs were introduced in Japan. Discrete patient populations may benefit from differing management regimens, including the fewer injections required with combination therapy.
Keywords: visual acuity, polypoidal choroidal vasculopathy, anti-vascular endothelial growth factor therapy, photodynamic therapy
Introduction
Globally, age-related macular degeneration (AMD) is the third leading cause of blindness following cataracts and glaucoma1 and is the primary cause of blindness in industrialized countries.2 AMD results from changes in the macular region of the retina in older people (aged >55 years), affecting photoreceptors and the retinal pigment epithelium, leading to a progressive loss of vision.3 The incidence of AMD is increasing as the global population ages,4,5 and management of age-related diseases over the coming decades is of particular concern in countries with a large proportion of elderly citizens, such as Japan. Population-based cohort studies in Japan have indicated that the overall prevalence of AMD ranges from 13.4%6 to 21.5%,7 with a notable increase between the ages of 50–59 years (16.4%) and 70–74 years (32.2%).8 Furthermore, the number of Japanese patients with AMD is expected to increase over the next 1–2 decades, potentially peaking in 2035.9
Wet AMD (wAMD), also known as exudative or neovascular AMD, develops in about 10% of all AMD cases10 and arises due to blood vessels from the choroid growing into the normally avascular retinal pigment epithelium and sub-retinal regions.11 wAMD is an infrequent complication of AMD, with an estimated global prevalence rate of 0.46%.4 However, wAMD accounts for 80–90% of the severe vision loss associated with AMD.12 Furthermore, one phenotype of wAMD called polypoidal choroidal vasculopathy (PCV) is known to occur at a higher prevalence in Japanese and Asian individuals than Caucasians.13–15 Patients with wAMD rapidly lose the central vision required for tasks such as reading, screen use, and driving,16 thus restricting both leisure activities and the ability to work, and severely reducing quality of life.16–18 The economic burden caused by visual impairment is substantial, in Japan; in 2007, it was estimated to be about 8785 billion yen, which equated to 1.7% of the gross domestic product in that year.19
The treatment algorithm for wAMD in Japan is driven by disease severity, and the recommended standard-of-care is anti-vascular endothelial growth factor (anti-VEGF) therapy.20 This class of drug binds to excess VEGF protein that would otherwise promote the erroneous growth of new blood vessels.21 As this protein is also essential for normal tissue healing and growth, VEGF must be only suppressed in the eye; therefore, these drugs are administered via intraocular injections on an intermittent or pro re nata (PRN) schedule.21 Anti-VEGF inhibitors first became available in Japan in 2008,22 and drugs in this class now approved in Japan include the monoclonal antibody ranibizumab and the synthetic protein aflibercept, both of which have proven clinical effectiveness in wAMD.23–27 To treat wAMD in Japan, anti-VEGF drugs are used either as monotherapy or in combination with photodynamic therapy (PDT).20
Drug development for wAMD is ongoing,28–30 and as new therapies become available, it is vital that Japanese patients and clinicians have the necessary information to assess management options critically. This, in turn, will allow them to make optimal treatment decisions. Thus, the primary objective of this study was to systematically review randomized controlled trials, observational studies, case studies, and treatment guidelines to investigate the effectiveness of clinical treatments for wAMD in Japanese patients in the decade following the 2008 introduction of anti-VEGF therapies.
Methods
Data Sources and Search Methodology
The methodology used for this systematic review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines31 (S1 Text) and documentation from the National Institute for Health and Clinical Excellence in the United Kingdom.32 The protocol was not registered. A comprehensive search was conducted in PubMed for articles published in English between 1 January 2008 and 30 September 2018. A multistring search strategy was implemented, and either title/abstract (TIAB) or medical subject heading (MeSH) entries were searched (S2 Text).
Study Selection Criteria
In the first round of screening, titles and abstracts of all records retrieved from the literature search were reviewed by YS and William YuanHao Kuan (Syneos Health, Tokyo, Japan). The relevance of each article was evaluated based on the inclusion and exclusion criteria (Table 1). A Population, Intervention, Comparison, and Outcome strategy was used to construct the specific research question. The AMD diagnostic criteria specified were those published by the Japanese Ministry of Health, Labour and Welfare.33 Studies of patients with retinal angiomatous proliferation were excluded, as this is a unique type of wAMD. Additional inclusion and exclusion criteria included the type of article, sample size, and geographic setting. Citations that did not match the eligibility criteria and duplicate citations were excluded. Unclear citations were included for more detailed evaluation. Any disparities were resolved by discussion between all authors. After reaching a consensus, the full text of studies identified as potentially relevant was reviewed in a second screening round and included in the analyses if the studies fulfilled the specified criteria.
 |
Table 1 Inclusion and Exclusion Criteria for the First Round of Literature Evaluation |
Data Extraction
The data presented in the selected studies were extracted by William YuanHao Kuan (Syneos Health), and the quality was checked by YS. The extracted information included type of study or article, number of sites, study duration, number of patients, baseline demographic and clinical characteristics, type of wAMD, risk factors, details of diagnosis and management, and clinical efficacy endpoints after 1 year of treatment (including visual acuity [VA], central retinal thickness [CRT], and number of injections [if applicable]). For dichotomous outcomes, the number of patients analyzed (N) and the number of patients with the outcome (n) were extracted. For continuous outcomes, N, mean, median, and interquartile range (IQR) were recorded.
Statistical Methods
Data from all relevant studies were pooled to report mean and/or median (IQR) for the logarithm of the minimum angle of resolution (logMAR) VA, CRT, and the number of injections. Data were stratified by type of wAMD and/or type of treatment. To explore the clinical efficacy endpoints stratified by these factors, Box and Whisker plots were created (indicating the median, 25th, and 75th percentile values). No adjustment was made for the data quantity (number of articles/treatment arms) or variations in baseline parameters. Data reported using the Early Treatment Diabetic Retinopathy Study scale was not converted into logMAR. As we did not adjust the data weighting of the papers included in the analysis, no tests for statistical difference were conducted. Microsoft Excel 2016 was used for all calculations.
Results
Article Selection
A PRISMA flowchart of the identification process is shown in Figure 1. The initial search identified 335 studies. After removing duplicates and those articles that did not meet the eligibility criteria, 280 articles remained for the detailed second-round assessment. An additional 17 gray literature articles were also subjected to detailed evaluation. Articles were excluded based on the patient population and study design, then by intervention, and finally by outcome. Following the full-text evaluation, 94 articles were selected for data extraction, resulting in a total of 147 individual treatment arms with available data. A full list of the 94 selected articles is provided as S1 Table.
 |
Figure 1 PRISMA flow diagram. aIncludes articles reporting epidemiology, treatment methodology, quality of life, and economic analyses. bNo data on VA or number of injections after 12 months of treatment. cTotal number of individual treatment arms for which data were reported. Abbreviations: PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; RAP, retinal angiomatous proliferation; VA, visual acuity. |
Stratification Factors
A breakdown of the disease types and treatment modalities in the 147 treatment groups is shown in Table 2. More treatment arms included patients with PCV (n = 85) than with typical AMD (n = 25). The two main types of treatments for wAMD were anti-VEGF injections (generally intravitreal aflibercept or intravitreal ranibizumab) and PDT, either as monotherapy or in combination. Interventions such as bevacizumab, pegaptanib, brolucizumab, and triamcinolone acetonide were rarely reported. A visualization of the treatment arms included in each outcome calculation is shown as S1 Figure. Outcomes for other types of wAMD were not calculated, as they were defined as neither typical AMD nor PCV. Additionally, outcomes were not calculated for other types of treatment because they included off-label steroid treatment and pegaptanib, which is rarely used in clinical practice.
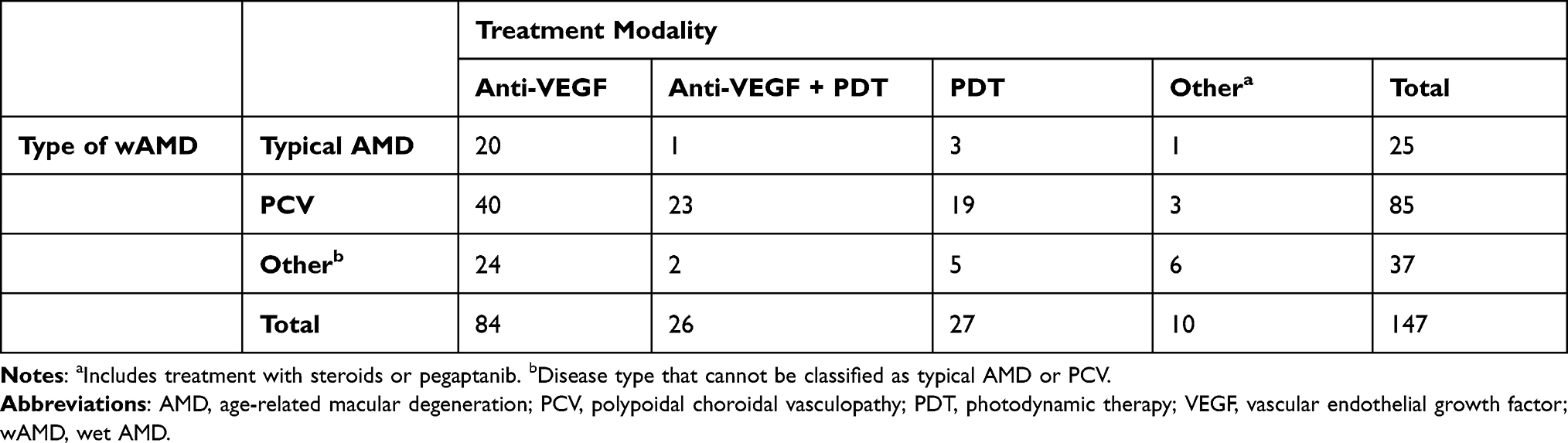 |
Table 2 Breakdown of Data Stratification Factors of the 147 Evaluable Treatment Groups |
Outcomes
Data for VA after 12 months of treatment, stratified by disease type, are shown in Figure 2A. The mean (median) logMAR VA after 12 months of treatment was 0.44 (0.32) for typical AMD and 0.34 (0.31) for PCV.
 |
Figure 2 Outcomes after 12 months of treatment: (A) VA stratified by disease type; (B) VA stratified by disease type (typical AMD) and treatment modality; (C) VA stratified by disease type (PCV) and treatment modality; (D) CRT stratified by disease type; (E) CRT stratified by disease type (PCV) and treatment modality; (F) Number of anti-VEGF injections stratified by disease type; and (G) Number of anti-VEGF injections stratified by disease type (PCV) and treatment modality; baseline values vary by treatment group. Abbreviations: AMD, age-related macular degeneration; CRT, central retinal thickness; logMAR, logarithm of the minimum angle of resolution; PCV, polypoidal choroidal vasculopathy; PDT, photodynamic therapy; VA, visual acuity; VEGF, vascular endothelial growth factor. |
Data for VA after 12 months of treatment, stratified by disease type and treatment modality, are shown in Figure 2B–C. For typical AMD, VA after 12 months of treatment tended to be better with anti-VEGF monotherapy than with PDT monotherapy. For PCV, post-treatment VA tended to be better with anti-VEGF monotherapy or with anti-VEGF plus PDT combination therapy than with PDT monotherapy.
Data for CRT after 12 months of treatment, stratified by disease type, are shown in Figure 2D. No notable difference between disease type was observed; in both groups, the mean CRT after 12 months was approximately 220 µm.
Data for CRT after 12 months of treatment, stratified by disease type and treatment modality, are shown in Figure 2E. Among the 13 typical AMD studies, anti-VEGF agents were the predominant treatment. Patients received either anti-VEGF monotherapy (12 studies) or anti-VEGF plus PDT (1 study); there were no studies in which patients were treated with PDT monotherapy. Therefore, we considered that stratification of the typical AMD group would not provide meaningful data; as a result, only data for the PCV group were stratified and evaluated. Anti-VEGF monotherapy and anti-VEGF plus PDT combination therapy resulted in lower mean CRT (ie, an improvement) after 12 months compared with PDT monotherapy.
Data for the number of anti-VEGF injections during the first 12 months of treatment, stratified by disease type, are shown in Figure 2F. The mean number of anti-VEGF injections during the first 12 months of treatment tended to be lower for patients with PCV (4.6) than those with typical AMD (5.6).
Corresponding data stratified by both disease type and treatment modality are shown in S2 Figure and Figure 2G. For patients with PCV, the mean number of anti-VEGF injections during the first 12 months of treatment was lower when receiving anti-VEGF plus PDT combination therapy (3.2) than anti-VEGF monotherapy (5.3).
When outcomes were calculated using only the treatment arms for which all outcome data were available (VA, CRT, and injection number), no differences were observed in the results (data not shown).
Discussion
In the decade since the introduction of anti-VEGF drugs for Japanese patients with wAMD, 94 studies including clinical effectiveness measures (VA, CRT, and injection number) have been published, totaling 147 individually evaluable treatment arms. Among Japanese patients with wAMD, more studies evaluated treatment for PCV than typical AMD. Previous studies have suggested that PCV occurs at a higher rate in Japanese/Asian individuals than Caucasians,13–15 and that PCV is a relevant problem in Japan;34 hence, there is likely to be clinical interest in evaluating treatments for AMD in Japanese populations. Overall, the most common treatments for AMD were anti-VEGF drugs and PDT, either as monotherapy or in combination, which is in line with current recommendations both in Japan and globally20,35–37 where anti-VEGF therapy is the current standard-of-care.
The production of high-quality systematic reviews can provide a strong evidence base to underpin clinical care.38 The use of this methodology to evaluate wAMD treatment in Japan allowed us to assess a large body of pooled evidence on clinical outcomes and observe whether effectiveness aligns with current practice recommendations. The pooled analysis of efficacy outcomes in patients with typical AMD indicated that anti-VEGF monotherapy yielded better results than PDT monotherapy in terms of VA after 12 months of treatment. However, baseline values varied between treatment groups because of the different studies that were included in our analyses. Both anti-VEGF monotherapy and anti-VEGF plus PDT combination therapy yielded better results in terms of VA and CRT for patients with PCV than PDT monotherapy after 12 months of treatment. Moreover, anti-VEGF plus PDT combination therapy required fewer injections than anti-VEGF monotherapy. The reduction in injection number is of particular interest to patients and clinicians. Intraocular injections require specialist expertise and can be labor-intensive and costly.39 Furthermore, many patients experience a psychosocial and practical burden from the treatment schedule.18,40,41 As a result, patients with wAMD in real-world practice are often undertreated, resulting in a lack of improvement (or even deterioration) in VA over time.42,43 Because of the highly invasive nature of treatment and the burdens associated with the treatment schedule, reduced dosing is desirable regardless of whether combination treatment or anti-VEGF monotherapy is used. As newer anti-VEGF agents are launched,44 it is hoped that treatments requiring fewer injections will become available.
It is clear from our study findings that progress has been made in the treatment of wAMD in the years since the introduction of anti-VEGF therapy in Japan. However, there remains a need for novel treatments and regimens that offer a better prognosis for VA while requiring fewer injections.39 Many recent studies have evaluated PRN, quarterly, and “treat and extend” dosing regimens instead of fixed dosing in an attempt to balance VA improvement and maintenance with fewer injections.45 The anti-VEGF antibody fragment brolucizumab, which is now approved in several countries including the United States and Japan,46 can be used with a 12-weekly maintenance schedule.47 In addition to the possibility of treatment with fewer doses, brolucizumab has excellent fluid control.48 There is also interest in sustained-release delivery devices for both novel and approved agents,49–52 in oral anti-VEGF formulations,53,54 and in gene therapy.55,56 The diversity of subject areas covered in wAMD research within an elderly Japanese population was narrow, with some search terms returning little evidence. Treatment comparisons may have suffered from heterogeneity in the study design and procedures, and no statistical comparisons were conducted.
Conclusions
The findings outlined in this study represent a large body of evidence relating to wAMD treatment and treatment outcomes in Japan. During the decade since the introduction of anti-VEGF drugs in Japan, wAMD treatment has advanced dramatically. The present results appear to confirm the treatment outcomes observed in clinical practice and suggest that discrete patient populations may gain optimal benefits from differing management regimens. Nevertheless, the development of new drugs and treatment regimens that offer an improved prognosis for VA and require fewer injections remains an important unmet clinical need.
Abbreviations
AMD, age-related macular degeneration; CRT, central retinal thickness; IQR, interquartile range; logMAR, logarithm of the minimum angle of resolution; MeSH, medical subject heading; PCV, polypoidal choroidal vasculopathy; PDT, photodynamic therapy; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PRN, pro re nata; TIAB, title/abstract; VA, visual acuity; VEGF, vascular endothelial growth factor; wAMD, wet AMD.
Data Sharing Statement
All data supporting the results are included in the manuscript.
Acknowledgments
The authors would like to thank William YuanHao Kuan, of Syneos Health, Tokyo, Japan, for assistance with the first round of screening and data extraction. We also thank Sally-Anne Mitchell, PhD, of Edanz, for providing medical writing assistance, which was funded by Novartis Pharma K.K. through EMC K.K. in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). Some data from this systematic literature review were previously presented at the 59th Annual Meeting of the Japanese Retina and Vitreous Society, Fukuoka, Japan, November 2020.
Funding
This study was funded by Novartis Pharma K.K., who were involved in the study design, data collection and analysis, decision to publish, and preparation of the manuscript.
Disclosure
KT reports receiving honoraria for advisory board participation from Novartis Pharma K.K. for the current work; and grants from Hoya Corporation, Otsuka Pharmaceutical Co., Ltd., and Santen Pharmaceutical Co., Ltd., consulting fees from Kyowa Kirin Co., Ltd. and Santen Pharmaceutical Co., Ltd., and honoraria for presentations from Bayer Yakuhin Ltd., Kyowa Kirin Co., Ltd., and Santen Pharmaceutical Co., Ltd., outside of the submitted work.
TI reports receiving honoraria for advisory board participation from Novartis Pharma K.K. for the current work; and grants from Alcon Japan Ltd., AMO Japan K.K., Bayer Yakuhin Ltd., Hoya Corporation, NIDEK Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Pfizer Japan Inc., Santen Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., and Topcon Corporation, consulting fees from Bayer Yakuhin Ltd., Chugai Pharmaceutical Co., Ltd., and Nippon Boehringer Ingelheim Co., Ltd., honoraria for presentations from Alcon Japan Ltd., Bayer Yakuhin Ltd., Canon Inc., Chugai Pharmaceutical Co., Ltd., JFC Sales Plan Co., Ltd., Novartis Pharma K.K., NIDEK Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Santen Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., and Topcon Corporation, payment for expert testimony from Nippon Boehringer Ingelheim Co., Ltd., and patent involvement with Topcon Corporation, outside of the submitted work.
SI reports receiving honoraria for advisory board participation from Novartis Pharma K.K. for the current work; and grants from AbbVie GK, Alcon Japan Ltd., Alpha Communication, AMO Japan K.K., Bayer Yakuhin Ltd., Bonac Corporation, Bloom Technology Corporation, NIDEK Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Santen Pharmaceutical Co., Ltd., SEED Co., Ltd., Senju Pharmaceutical Co., Ltd., Wakamoto Pharmaceutical Co., Ltd., and Whitemedical Co., Ltd., honoraria for presentations from Bayer Yakuhin Ltd., Chugai Pharmaceutical Co., Ltd., Hoya Corporation, Kowa Company, Ltd., NIDEK Co., Ltd., Nitto Medic Co., Ltd., Novartis Pharma K.K., Santen Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., and Wakamoto Pharmaceutical Co., Ltd., honoraria for manuscript writing from SENTAN IGAKU-SHA Ltd., payment for expert testimony from Bloom Technology Corporation, Chugai Pharmaceutical Co., Ltd., Kyowa Kirin Co., Ltd., Mylan EPD G.K., and SENTAN IGAKU-SHA Ltd., travel support from Alcon Pharma, Bayer Yakuhin Ltd., Chugai Pharmaceutical Co., Ltd., Hoya Corporation, Kowa Company, Ltd., NIDEK Co., Ltd., Nitto Medic Co., Ltd., Novartis Pharma K.K., Otsuka Pharmaceutical Co., Ltd., Santen Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., SENTAN IGAKU-SHA Ltd., and Wakamoto Pharmaceutical Co., Ltd., and patent involvement with Bonac Corporation, Chugai Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., SEED Co., Ltd., and NIDEK Co., Ltd., outside of the submitted work. SI also reports the following leadership roles: Director of the Japanese Ophthalmological Society; Executive Director of the Japanese Retina and Vitreous Society; Executive Director of the Japanese Society of Ophthalmic Diabetology; Director of the Japanese Society for Ocular Circulation; Councilor of the Japanese Ocular Inflammation Society; Councilor of the Japan Society of Diabetic Complications; Councilor of the Japanese Society of Anti-Aging Medicine; Councilor of the Japanese Society of Inflammation and Regeneration; Director of the Japanese Society for Ocular Pharmacology; Director of the Japanese Society for Microcirculation; International Commissioner of the Macula Society; and Vice Chairman of the Global Ocular Inflammation Workshops.
AM, RT, ST, and KI are employees of Novartis Pharma K.K. The authors report no other conflicts of interest in this work.
References
1. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–618. doi:10.1136/bjophthalmol-2011-300539
2. Taylor HR, Keeffe JE. World blindness: a 21st century perspective. Br J Ophthalmol. 2001;85(3):261–266. doi:10.1136/bjo.85.3.261
3. Ferris FL
4. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–116. doi:10.1016/S2214-109X(13)70145-1
5. Jonas JB, Cheung CMG, Panda-Jonas S. Updates on the epidemiology of age-related macular degeneration. Asia Pac J Ophthalmol. 2017;6(6):493–497. doi:10.22608/APO.2017251
6. Obata R, Yanagi Y, Inoue T, et al. Prevalence and factors associated with age-related macular degeneration in a southwestern island population of Japan: the Kumejima Study. Br J Ophthalmol. 2018;102(8):1047–1053. doi:10.1136/bjophthalmol-2016-309980
7. Nakata I, Yamashiro K, Nakanishi H, et al. Prevalence of AMD in the Japanese: the Nagahama study. Investig Ophthalmol Vis Sci. 2012;53:3807.
8. Nakata I, Yamashiro K, Nakanishi H, et al. Prevalence and characteristics of age-related macular degeneration in the Japanese population: the Nagahama study. Am J Ophthalmol. 2013;156(5):1002–1009. doi:10.1016/j.ajo.2013.06.007
9. Kume A, Ohshiro T, Sakurada Y, Kikushima W, Yoneyama S, Kashiwagi K. Treatment patterns and health care costs for age-related macular degeneration in Japan: an analysis of National Insurance claims data. Ophthalmology. 2016;123(6):1263–1268. doi:10.1016/j.ophtha.2016.01.042
10. Ferris FL
11. Lipecz A, Miller L, Kovacs I, et al. Microvascular contributions to age-related macular degeneration (AMD): from mechanisms of choriocapillaris aging to novel interventions. Geroscience. 2019;41(6):813–845. doi:10.1007/s11357-019-00138-3
12. Yasuda M, Kiyohara Y, Hata Y, et al. Nine-year incidence and risk factors for age-related macular degeneration in a defined Japanese population: the Hisayama study. Ophthalmology. 2009;116(11):2135–2140. doi:10.1016/j.ophtha.2009.04.017
13. Fujiwara K, Yasuda M, Hata J, et al. Prevalence and risk factors for polypoidal choroidal vasculopathy in a general Japanese population: the Hisayama study. Semin Ophthalmol. 2018;33(6):813–819. doi:10.1080/08820538.2018.1506483
14. Lorentzen T, Subhi Y, Sørensen TL. Prevalence of polypoidal choroidal vasculopathy in white patients with exudative age-related macular degeneration: systematic review and meta-analysis. Retina. 2018;38(12):2363–2371. doi:10.1097/IAE.0000000000001872
15. Yanagi Y, Foo VHX, Yoshida A. Asian age-related macular degeneration: from basic science research perspective. Eye. 2019;33(1):34–49. doi:10.1038/s41433-018-0225-x
16. Mitchell J, Bradley C. Quality of life in age-related macular degeneration: a review of the literature. Health Qual Life Outcomes. 2006;4(1):97. doi:10.1186/1477-7525-4-97
17. Yuzawa M, Fujita K, Tanaka E, Wang EC. Assessing quality of life in the treatment of patients with age-related macular degeneration: clinical research findings and recommendations for clinical practice. Clin Ophthalmol. 2013;7:1325–1332. doi:10.2147/OPTH.S45248
18. Honda S, Yanagi Y, Koizumi H, et al. Impact of neovascular age-related macular degeneration: burden of patients receiving therapies in Japan. Sci Rep. 2021;11(1):13152. doi:10.1038/s41598-021-92567-4
19. Roberts CB, Hiratsuka Y, Yamada M, et al. Economic cost of visual impairment in Japan. Arch Ophthalmol. 2010;128(6):766–771. doi:10.1001/archophthalmol.2010.86
20. Takahashi K, Ogura Y, Ishibashi T, Shiraga F, Yuzawa M. Treatment guidelines for age-related macular degeneration. J Jpn Ophthalmol Soc. 2012;116(12):1150–1155. [in Japanese]
21. Yorston D. Anti-VEGF drugs in the prevention of blindness. Community Eye Health. 2014;27(87):44–46.
22. Report on the deliberation results. Ministry of Health, Labour and Welfare. Available from: https://www.pmda.go.jp/files/000153104.pdf.
23. Bakri SJ, Thorne JE, Ho AC, et al. Safety and efficacy of anti-vascular endothelial growth factor therapies for neovascular age-related macular degeneration: a report by the American Academy of Ophthalmology. Ophthalmology. 2019;126(1):55–63. doi:10.1016/j.ophtha.2018.07.028
24. Solomon SD, Lindsley K, Vedula SS, Krzystolik MG, Hawkins BS. Anti-vascular endothelial growth factor for neovascular age-related macular degeneration. Cochrane Database Syst Rev. 2014;8(8):CD005139. doi:10.1002/14651858.CD005139.pub3
25. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
26. Schmidt-Erfurth U, Kaiser PK, Korobelnik JF, et al. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology. 2014;121(1):193–201. doi:10.1016/j.ophtha.2013.08.011
27. Ogura Y, Terasaki H, Gomi F, et al. Efficacy and safety of intravitreal aflibercept injection in wet age-related macular degeneration: outcomes in the Japanese subgroup of the VIEW 2 study. Br J Ophthalmol. 2015;99(1):92–97. doi:10.1136/bjophthalmol-2014-305076
28. Ishikawa M, Jin D, Sawada Y, Abe S, Yoshitomi T. Future therapies of wet age-related macular degeneration. J Ophthalmol. 2015;2015:138070. doi:10.1155/2015/138070
29. Papadopoulos Z. Recent developments in the treatment of wet age-related macular degeneration. Curr Med Sci. 2020;40(5):851–857. doi:10.1007/s11596-020-2253-6
30. Ammar MJ, Hsu J, Chiang A, Ho AC, Regillo CD. Age-related macular degeneration therapy: a review. Curr Opin Ophthalmol. 2020;31(3):215–221. doi:10.1097/ICU.0000000000000657
31. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269, W64. doi:10.7326/0003-4819-151-4-200908180-00135
32. Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document 1: Introduction to evidence synthesis for decision making. National Institute for Health and Clinical Excellence. Available from: https://www.ncbi.nlm.nih.gov/books/NBK395870/pdf/Bookshelf_NBK395870.pdf.
33. Takahashi K, Ishibashi T, Ogura Y, Yuzawa M. Working group for establishing diagnostic criteria for age-related macular degeneration. Classification and diagnostic criteria of age-related macular degeneration. J Jpn Ophthalmol Soc. 2008;112(12):1076–1084. [in Japanese]
34. Tsujikawa A, Akagi-Kurashige Y, Yuzawa M, et al. Baseline data from a multicenter, 5-year, prospective cohort study of Japanese age-related macular degeneration: an AMD2000 report. Jpn J Ophthalmol. 2018;62(2):127–136. doi:10.1007/s10384-017-0556-3
35. Flaxel CJ, Adelman RA, Vemulakonda A, et al. Age-related macular degeneration preferred practice pattern. Am Acad Ophthalmol. 2020;127(1):P1–65.
36. Age-related macular degeneration NICE guideline [NG82]. National Institute for Health and Care Excellence. Available from: https://www.nice.org.uk/guidance/ng82/chapter/recommendations.
37. 2019 Clinical Practice Guide for the diagnosis, treatment and management of age-related macular degeneration. Optometry Australia. Available from: https://www.optometry.org.au/wp-content/uploads/Professional_support/Practice_notes/AMD-Clinical-Practice-Guide-2019_final_designed_v5.pdf.
38. Lindsley K, Li T, Ssemanda E, Virgili G, Dickersin K. Interventions for age-related macular degeneration: are practice guidelines based on systematic reviews? Ophthalmology. 2016;123(4):884–897. doi:10.1016/j.ophtha.2015.12.004
39. Baumal CR. Wet age-related macular degeneration: treatment advances to reduce the injection burden. Am J Manag Care. 2020;26(5 Suppl):S103–S111.
40. Boyle J, Vukicevic M, Koklanis K, Itsiopoulos C, Rees G. Experiences of patients undergoing repeated intravitreal anti-vascular endothelial growth factor injections for neovascular age-related macular degeneration. Psychol Health Med. 2018;23(2):127–140. doi:10.1080/13548506.2016.1274040
41. Thier A, Holmberg C. The patients’ view: age-related macular degeneration and its effects – a meta-synthesis. Disabil Rehabil. 2020;1–11. doi:10.1080/09638288.2020.1775901
42. Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99(2):220–226. doi:10.1136/bjophthalmol-2014-305327
43. Ciulla TA, Hussain RM, Pollack JS, Williams DF. Visual acuity outcomes and anti-vascular endothelial growth factor therapy intensity in neovascular age-related macular degeneration patients: a real-world analysis of 49 485 eyes. Ophthalmol Retina. 2020;4(1):19–30. doi:10.1016/j.oret.2019.05.017
44. Pugazhendhi A, Hubbell M, Jairam P, Ambati B. Neovascular macular degeneration: a review of etiology, risk factors, and recent advances in research and therapy. Int J Mol Sci. 2021;22(3):1170. doi:10.3390/ijms22031170
45. Khanna S, Komati R, Eichenbaum DA, Hariprasad I, Ciulla TA, Hariprasad SM. Current and upcoming anti-VEGF therapies and dosing strategies for the treatment of neovascular AMD: a comparative review. BMJ Open Ophthalmol. 2019;4(1):e000398. doi:10.1136/bmjophth-2019-000398
46. Markham A. Brolucizumab: first approval. Drugs. 2019;79(18):1997–2000. doi:10.1007/s40265-019-01231-9
47. BEOVU (brolucizumab-dbll) injection, for intravitreal use [Prescribing Information]. East Hanover, NJ, USA: Novartis Pharmaceuticals Corp.; 2020. Available from: https://www.novartis.us/sites/www.novartis.us/files/beovu.pdf.
48. Nguyen QD, Das A, Do DV, et al. Brolucizumab: evolution through preclinical and clinical studies and the implications for the management of neovascular age-related macular degeneration. Ophthalmology. 2020;127(7):963–976. doi:10.1016/j.ophtha.2019.12.031
49. Chittasupho C, Kengtrong K, Chalermnithiwong S, Sarisuta N. Anti-angiogenesis by dual action of R5K peptide conjugated itraconazole nanoparticles. AAPS PharmSciTech. 2020;21(3):74. doi:10.1208/s12249-019-1568-8
50. Bhatt P, Narvekar P, Lalani R, Chougule MB, Pathak Y, Sutariya V. An in vitro assessment of thermo-reversible gel formulation containing sunitinib nanoparticles for neovascular age-related macular degeneration. AAPS PharmSciTech. 2019;20(7):281. doi:10.1208/s12249-019-1474-0
51. Liu W, Borrell MA, Venerus DC, Mieler WF, Kang-Mieler JJ. Characterization of biodegradable microsphere-hydrogel ocular drug delivery system for controlled and extended release of ranibizumab. Transl Vis Sci Technol. 2019;8(1):12. doi:10.1167/tvst.8.1.12
52. Lim JI, Niec M, Wong V. One year results of a Phase 1 study of the safety and tolerability of combination therapy using sustained release intravitreal triamcinolone acetonide and ranibizumab for subfoveal neovascular AMD. Br J Ophthalmol. 2015;99(5):618–623. doi:10.1136/bjophthalmol-2014-306002
53. Cohen MN, O’Shaughnessy D, Fisher K, et al. APEX: a Phase II randomised clinical trial evaluating the safety and preliminary efficacy of oral X-82 to treat exudative age-related macular degeneration. Br J Ophthalmol. 2021;105(5):716–722. doi:10.1136/bjophthalmol-2020-316511
54. Tarallo V, Iaccarino E, Cicatiello V, Sanna R, Ruvo M, De Falco S. Oral delivery of a tetrameric tripeptide inhibitor of VEGFR1 suppresses pathological choroid neovascularization. Int J Mol Sci. 2020;21(2):410. doi:10.3390/ijms21020410
55. Guimaraes TAC, Georgiou M, Bainbridge JWB, Michaelides M. Gene therapy for neovascular age-related macular degeneration: rationale, clinical trials and future directions. Br J Ophthalmol. 2021;105(2):151–157. doi:10.1136/bjophthalmol-2020-316195
56. Reid CA, Nettesheim ER, Connor TB, Lipinski DM. Development of an inducible anti-VEGF rAAV gene therapy strategy for the treatment of wet AMD. Sci Rep. 2018;8(1):11763. doi:10.1038/s41598-018-29726-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.