")
Back to Journals » Journal of Blood Medicine » Volume 14
Effectiveness of COVID-19 Convalescent Plasma (CCP) During the Pandemic Era: A Literature Review
Authors Kandula UR , Tuji TS, Gudeta DB, Bulbula KL, Mohammad AA, Wari KD, Abbas A
Received 25 November 2022
Accepted for publication 8 February 2023
Published 22 February 2023 Volume 2023:14 Pages 159—187
DOI https://doi.org/10.2147/JBM.S397722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Usha Rani Kandula, Techane Sisay Tuji, Dinkinesh Begna Gudeta, Kassech Leta Bulbula, Anwar Abdulwahed Mohammad, Ketema Diriba Wari, Ahmad Abbas
Department of Nursing, College of Health Sciences, Arsi University, Asella, Ethiopia
Correspondence: Usha Rani Kandula, Department of Nursing, College of Health Sciences, Arsi University, Oromia Region, P.O. Box-396, Asella, Ethiopia, Tel +251-939052408, Email [email protected]
Abstract: Worldwide pandemic with coronavirus disease-2019 (COVID-19) was caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). As November 2, 2022, World Health Organization (WHO) received 628,035,553 reported incidents on COVID-19, with 6,572,800 mortalities and, with a total 12,850,970,971 vaccine doses have been delivered as of October 31, 2022. The infection can cause mild or self-limiting symptoms of pulmonary and severe infections or death may be caused by SARS-CoV-2 infection. Simultaneously, antivirals, corticosteroids, immunological treatments, antibiotics, and anticoagulants have been proposed as potential medicines to cure COVID-19 affected patients. Among these initial treatments, COVID-19 convalescent plasma (CCP), which was retrieved from COVID-19 recovered patients to be used as passive immune therapy, in which antibodies from cured patients were given to infected patients to prevent illness. Such treatment has yielded the best results in earlier with preventative or early stages of illness. Convalescent plasma (CP) is the first treatment available when infectious disease initially appears, although few randomized controlled trials (RCTs) were conducted to evaluate its effectiveness. The historical record suggests with potential benefit for other respiratory infections, as coronaviruses like Severe Acute Respiratory Syndrome-CoV-I (SARS-CoV-I) and Middle Eastern Respiratory Syndrome (MERS), though the analysis of such research is constrained by some non-randomized experiments (NREs). Rigorous studies on CP are made more demanding by the following with the immediacy of the epidemics, CP use may restrict the ability to utilize it for clinical testing, non-homogenous nature of product, highly decentralized manufacturing process; constraints with capacity to measure biologic function, ultimate availability of substitute therapies, as antivirals, purified immune globulins, or monoclonal antibodies. Though, it is still not clear how effectively CCP works among hospitalized COVID-19 patients. The current review tries to focus on its efficiency and usage in clinical scenarios and identifying existing benefits of implementation during pandemic or how it may assist with future pandemic preventions.
Keywords: convalescent plasma, COVID-19 convalescent plasma, effectiveness, CCP, COVID-19, coronavirus disease-2019, SARA-CoV-2, severe acute respiratory distress syndrome-coronavirus-2, pandemic era, literature review
Introduction
In recent years, coronavirus infections have been the source of epidemics, and the concern was raised about SARS (Severe Acute Respiratory Syndrome) and MERS in 2002 and 2012, respectively. The SARS-CoV-2, a current recruit among coronavirus family with the most recent outbreak and designated with COVID-19.1 The worldwide epidemic has been reported due to COVID-192 and, the WHO proclaimed worldwide pandemic immediately after its development and subsequent spread among human population during 2019. Around 4.4 million people have perished from virus affects, and infected with a minimum of 215 million.3 At that movement, WHO stated on March 11, 2020, the spread of COVID-19 may pose significant and ongoing problems to the entire globe.2
Patients with COVID-19 are usually undiagnosed or exhibit mild respiratory concerns,4 moreover, some patients appear with a variety of symptoms, ranging from mild or flu-symptomatology (81% of cases) to acute (14% of cases) and with severe (5%) clinical manifestations.5 In addition to affecting people’s daily lives, the SARS-CoV-2 infection also led to organ damage. An evidence reported that the SARS-CoV-2 either directly or indirectly promotes inflammasomes and, by inducing pyroptosis, an inflammatory form of cell demise, and aggravating tissue injury with endothelial malfunction, vasodilation and, the inflammatory cytokines may promote tissue damage and, the patient may exhibit with several clinical manifestations,2,6 and multiple-organ failure may occur as a severe side effect of this inflammatory reaction.2
The Acute respiratory distress syndrome (ARDS), abnormal coagulation, multiple organ failure syndrome, or septic shock are some examples of infection processes other than direct viral infection that can cause severe effects in SARS-CoV-2. In some circumstances, adapted immunity is suppressed, which forces the innate immune system to respond more vigorously, and produced more inflammatory compounds than it should, may delay the clearance of viruses, and increase the number of immune cells that are activated at inflammation sites.7 During pandemic demands, there is a need to move swiftly to offer therapeutic options in this circumstance. Considering advancements in vaccination and pharmaceutical research, notably medications using nanotechnology and naturally occurring bioactive constituents,8 and with particular coronavirus’s genetic diversity and rapid evolution, there is presently no special, effective treatment to prevent or treat the disease.9,10
People who are critically ill are more at risk of dying from an overactive immune system than from a viral infection alone. Significant increases in cytokines and other inflammatory biomarkers, such as interleukins, interferon, tumor necrosis factors, colony-stimulating factors, growth factors, ferritin, C-reactive proteins, and D-dimers, are present among majority of patients in the intensive care unit (ICU) with severe COVID-19.11,12 Infiltration of further immune cells, such as lymphocytes, macrophages, and dendritic cells, may ensue from this excessive and prolonged cytokine response, which may exponentially increase the inflammation.11,13 The patients with COVID-19 may experience illness exacerbation and mortality mostly because of this immune system imbalance, which causes a cytokine storm.14 To prevent the illness worsening and lower mortality among COVID-19 patients, treatment may include rapid control of the cytokine storm syndrome (CSS) in addition to supportive therapies.11,15
For the movement, the sole option for new coronavirus pneumonia is general supportive care only,4 with this reasons, from the hospital patients died at a rate ranging from 11% to 15%. Moreover, the amount of knowledge accessible in literary texts and official sources is steadily growing, despite the reality that COVID-19 is extremely contagious and has a high death rate.2 Since late 2019, COVID-19 has become a concern for public health all around the world, and there has been a significant amount of debate and research towards finding a solution. Although, few strategies have proven to be effective, while others have failed.16,17 In addition to that, almost two years into the COVID-19 epidemic, we still have a limited pharmacological arsenal to prevent or cure the disease’s devastating effects among affected population.18,19
In progress towards the introduction of novel variations emphasizes the need for surveillance systems with update vaccination programs and treatment methods.20 These variances are particularly worrisome because many regions of the world do not vaccinate their inhabitants due to a lack of infrastructure for mass manufacture and distribution, affordability and, with appropriate provisions.21 There are still many active infections with SARS-CoV-2 infectivity, transmission, and fatality are altering even though the percentage of people globally who are protected against COVID-19 is expanding as a consequence of the availability of various vaccinations.14 In this scenario, immunotherapies, cytokine inhibitors, monoclonal antibodies, and anti-inflammatory medications are instances of potentially effective therapy alternatives for COVID-19 prevention,22,23 and by removing inflammatory cytokines and infective markers, therapeutic plasma exchange may be a useful treatment for CSS.24,25
Convalescent Plasma Therapy (CPT)
CPT is a passive immunization technique that has been employed for more than a couple of centuries as a reliable and efficient therapy for a wide range of infectious diseases, including COVID-19,26 and it has been routinely employed in the treatment of hospitalized COVID-19 patients.27,28 CCP was a common form of passive immunization during the initial stages of pandemic, with the risk of antibody-dependent acceleration of viral illness even if the preventative vaccine and monoclonal antibody treatment had been quickly developed and used3 (Figure 1).
 |
Figure 1 COVID-19 Convalescent plasma (CCP) transfusion process. |
The United States Food and Drug Administration (FDA) currently suggests antivirals like remdesivir and anti-inflammatory medications like corticosteroids for hospitalized patients with who require supplementary oxygen (O2), as well as monoclonal antibodies targeted against SAS-CoV-2 spike protein for outpatients at high risk of disease development.29 As everyone is aware, passive immunization has played an essential role in the treatment of infectious illnesses.30 Soon as the commencement of COVID-19 epidemic, treatment options were predictably limited, forcing the reintroduction of a venerable method with passive immunization by transfusion of CP.31
Plasma transfusion from recuperating donors to acutely infected patients was one of the few treatment options available at the outset of the pandemic. In areas with limited resources, passive immunization employing CCP from formerly infected donors is still an effective therapeutic option. Despite a few positive results from CCP transfusion in patients with acute SARS-CoV-2 infection, the efficacy of this therapy still seems to be poorly or not thoroughly grasped.32 As before COVID-19 pandemic, clinical trials with CP were rare and produced contradictory results with range of research designs, patient demographics, infecting pathogens, timing of infusion delivery about the duration of the illness, dosage, and the controls used in previous research.33,34
Moreover, High-titer CCP early delivery was shown to be safe and effective, with a lower risk of hospitalization and mortality compared with control groups.35,36 These combined findings have influenced clinical guidelines that advocate for the early transfusion of CCP.37 The option of CCP is also available to hospitalized patients who are unable to take other available antiviral medicines due to safety concerns or contraindications, such as pregnant women, and patients with severe chronic kidney disease, or severe chronic cirrhosis of the liver.38
During the 1918 Spanish flu pandemic,39,40 and subsequent severe viral diseases, including SARS, H1N1 influenza, MERS, and the Ebola virus, we later adopted CP infusion method as passive immunization.41–43 The pre-clinical animal models suggested that passive immunization therapeutics would be useful during the COVID-19 pandemic,44–46 and non-human primate studies discovered that passive transfer of immunoglobulins could confer therapeutic efficacy after viral exposure and fight infection in a dose-dependent manner.47,48 Additionally, case studies conducted early during pandemic demonstrated on positive outcomes for patients receiving CP from donors recovered through CCP transfusions.49–51
As anti-SARS-CoV-2 neutralizing antibodies (NAbs) are present in CCP and may be utilized as COVID-19 passive immunization in patients with high risk of severe illness and, also the plasma from recuperating patients may have additional immune-modulatory abilities when administered to COVID-19 patients.52 Additionally, the use of CCP from previously infected individuals to passively transfer anti-SARS-CoV-2 antibodies and potentially treat or prevent COVID-19 is currently being investigated. Furthermore, CCP is acquired from individuals who have fully recovered from illness and preferably includes high titer of viral NAbs.53
Reduced Plasma Cryoprecipitate (Cryosupernatant)
As recent research findings suggest on using fresh frozen cryoprecipitate-depleted plasma or plasma with reduced cryoprecipitate instead of apheresis plasma from recovered COVID-19 patients as a source of anti-SARS-CoV-2 antibodies.54 Since Judith Pool’s original proposal in 1964,55 the vast majority of blood manufacturers have been able to produce cryoprecipitate supernatant from fast frozen plasma. The SARS-CoV-2 antibody-containing plasma is rapidly cooled to a temperature of −70 °C or lower.
Treatment with CCP Among Other Viral Diseases
According to research that has been published, the CCP can be used to treat a variety of viral diseases, including influenza, Ebola virus, Spanish influenza, SARS, and MERS. The majority of patients observed positive effects from CCP transfusion without any challenges.56,57
Ebola virus,56,57 the WHO has suggested the transfusion of CP or whole blood from patients who recovered from the Ebola virus as an empirical treatment for the Ebola outbreaks.58
The Spanish flu,57 as the studies that examined convalescent blood products to treat Spanish influenza-related pneumonia in hospitals as early as the 1918–1925 pandemic presented an assessment versus a control or comparison group. A meta-analysis performed in 2006, almost a century later, revealed a significant decrease in the total crude mortality rate, from 37% among controls to 16% among patients receiving CP.59
H1N1,57 a comparative study involving 99 patients, CP treatment was able to significantly lower respiratory tract viral load, serum cytokine response (interleukin-6, interleukin-19, and tumor necrosis factor-alpha), and mortality in context of pandemic influenza A (H1N1) 2009 virus infection. The probabilities of dying were reduced by 80%, making the decrease in mortality in that research study quite impressive.42
SARS,57 Following a comprehensive review and meta-analysis of 32 studies on severe influenza and the SARS coronavirus emphasized the consistent evidence for a decrease in mortality, particularly in cases of early administration of CP and hyperimmune immunoglobulin following symptom onset. The study results indicated a reduction in mortality odds of 75%,60 supporting the significant reduction in mortality odds as per the investigation findings.60
MERS,57 the management of MERS with CP therapy planned protocol for people with illness was established during 2015. In accordance with protocol, individuals who had an anti-MERS coronavirus indirect fluorescent antibody titer of 1:160 or higher would be evaluated to identify, if they were eligible to donate plasma in accordance with standard donation guidelines and, provided that they had no signs of active MERS infection in the form of clinical or laboratory findings.61
The CP had also been used to treat measles,62 poliomyelitis,63 and mumps,64 during the first half of 20th century (Figure 2).
 |
Figure 2 Possible convalescent plasma (CP) applications among viral agents. |
History of CP
Dr Emil von Behring introduced passive immunization as a revolutionary treatment modality at the turn of 20th century, and when he established that the plasma from horses afflicted with diphtheria or tetanus could be applied to heal humans also. He was awarded with Nobel Prize for Medicine or Physiology in the year of 1901. This discovery opened the door for the treatment of infectious diseases with plasma from recovering patients, and CP has been used throughout history to treat a variety of infections, including poliomyelitis, Spanish influenza, Korean hemorrhagic fever, and more notably, Ebola virus and influenza virus (H1NI).65
The Arbeitskreis Blut, a working party as blood of the “German federal ministry of health”, released a statement (S16) on the production and administration of CP in severe disease epidemics on October 20, 2015. During early 20th-century, occurrences of diphtheria as well as subsequent cases of SARS, H1N1, and Ebola were said to respond positively to this therapeutic intervention.66 As the first therapeutic efficacy using plasma with anti-SARS-CoV-2 antibodies from convalescent donors was reported by Chinese doctors at the same time.49,50,67 In addition to this, more than 15 years ago, the first CP infusions were undertaken to treat coronavirus infections. Further to this, the first published studies during the 2004 and 2005 Asian SARS outbreaks showed that patients who received plasma had shorter hospital stays and fewer deaths than those who received standard care.41,68
According to the study, the first collection of CPT cases in SARS-CoV-2 patients was revealed by researchers in Asia at the beginning of 2020. As per the, first such trial, clinical and biological markers in five critically ill patients were reported to be improved by plasma infusion. There was also report on rapid neutralization of viral load process.50 Further to this, the research paper below had 19 patients who had similar outcomes.69 However, the European Commission developed guidelines for acquiring, analyzing, processing, preserving, disseminating, and regulating the use of CP in light of these preliminary results and the dearth of a viable etiological therapy for COVID-19, and the early applications of CP arose as an alternate therapy with a favorable safety profile in the absence of competent treatment.70
CP Collection (CPC)
As per the following guidelines provided by the regulatory organizations of the nation in which it is delivered, CCP must be processed and utilized as an investigational patient’s blood. According to US, the FDA in charge of enforcing rule that only registered and authorized blood collection facilities may obtain blood products as strictly. The regulatory body is also in charge of establishing the criteria for donors to be eligible, which have been modified as per new information has emerged over the course of pandemic. As to direct newly recovered donors to blood facilities early in the epidemic, several strategies were employed, such as testing databases with automated referrals, conventional and social media, etc.71
Apheresis Technology (AT)
As per the requirement of higher output of plasma volumes per donation (approximately three to four units for a large donor) in comparison to whole blood collection, apheresis technology is broadly applied for collection, at least in high-income nations in order to treat complex diseases.72 A medical treatment known as apheresis involves the temporary removal of blood components using centrifugal force, structural and size variations between blood components, and surface forces in microchannels as the basis of separation.73
CP Donor Criteria
Plasma apheresis was performed on convalescent patients who were at least 14 days post-symptom resolution and eligible for plasma donation,74 as well as remaining protocols as per the regular blood donation and transfusion procedures.
CP Testing
Testing for blood-borne diseases, ABO type, and human leukocyte antigens (HLA) (in the context of parous women) is necessary in addition to anti-SARS-CoV-2 antibody testing. Throughout the pandemic, antibody levels for CCP qualification have been regularly revised. Additionally, inconvenient for high-throughput screening, formal neutralization assays are also challenging as for standardization. Instead, several tests have been proven to be effective, with a certain antibody level being shown to correspond to neutralization.72
CP Storage
Plasma treatment may be advantageous among patients with COVID-19 who have low humoral immunity or receiving B-cell depletion therapy for autoimmune diseases, multiple sclerosis, rheumatoid arthritis, or hematologic malignancies.75,76 Indeed, the beneficial effects of passive immunization on the clinical trajectory have been demonstrated, for instance, in a patient with a humoral immunodeficiency.77
Institutional blood banks frequently keep CCP inventories. Each ABO-compatible type should ideally have an adequate supply to meet clinical demands, because only 4% of the population donates blood, and as demand for several blood type demands, particularly Group AB (universal donor), have proven challenging to collect as required quantity. These donations are usually intended to support the urgent use of plasma for the control of bleeding disorders. As Group “A” plasma may be substituted during routine trauma resuscitation if approved by the institutional policy since Group “AB” plasma as in limited supply conditions.78
The CCP is still under investigation, which may restrict its use in comparison to plasma, which is frequently used to alleviate coagulopathy and hemorrhage conditions. As an organizational policy concerning non-group plasma should be formulated when transfusions are administered, and the patients should be informed on the benefits and dangers, and also the documentation for transfusion permission should include with any necessary disclosures as per the institutional policies.38
Accordingly, clinical demand of CCP was higher than supply at the start of the epidemic. Because of the collection’s rapid growth, most sizing-up blood facilities established a standing inventory, along with for responding to demand increases, having a CCP inventory on hand is crucial (eg, due to emerging variants). Later, as per the need decreased, and collecting came to an end as a result of vaccination process, and decrease in COVID-19 incidence, and evidence of the futility of treating advanced sickness. Due to this, earlier CCP inventories were inadequately suited to more recent variants like delta and omicron.78
This highlights the necessity of keeping a small supply of CCP on hand as well as the ability to find new donors, especially those who have recovered from an infection with a virus that is the same as the one that infected the intended recipient. It is logistically challenging, even though temporal and geographic matching are preferred. Despite poor matching, qualified CCPs (as described by the FDA) are still thought to be helpful.71
CP Transfusion Area
To protect patients, workers, and visitors in healthcare facilities from infection, providing clinical treatment to potentially infectious patients during a pandemic necessitates a special infrastructure. Numerous outpatient transfusion and infusion centers provide immunosuppressive or chemotherapeutic treatment to sensitive populations, and sharing space with individuals who are actively infected with SARS-CoV-2 poses a serious risk to these populations.38
It was a common infection control tactic to separate treatment facilities from ordinary care facilities. The logistical complexity of this system affects medical supplies and patients equally. Repurposing existing infrastructure for transfusion, such as negative pressure chambers used for the treatment of patients with airborne infections (such as TB), is one possibility for developing a new outpatient CCP transfusion center.38
CP Usage
Passive immunization with CP treatment became more common in patients with SARS-CoV-2 infection during COVID-19. To properly determine the use of this treatment in which patient groups at what dose and at what appropriate time interval, no controlled trial has been carried out. Studies have revealed that CP therapy is well tolerated, early treatment decisions can reduce mortality and ICU stay length, and it is not just a last-resort rescue strategy79 (Table 1).
 |
Table Evidences from Literature Report on the Efficacy of Convalescent Plasma Administration Among COVID-19 Patients |
Protective Mechanism of CP
Neutralizing Antibodies Had Antiviral Activity
Significantly, patients with severe disease who received COVID-19 had stronger neutralizing antibody responses against SARS-CoV-2,80,81 and SARS-CoV-2 is eliminated by CP, which acts as an antiviral agent.50
The Function of the ABO Blood Group
The observation that people with the blood type “O” are less likely to get a coronavirus infection than those with blood groups other than “O” was later noticed in SARS-CoV-2 infected subjects.82,83
Anti-Inflammatory and Immune-Modulating Qualities
Anti-spike IgG and IgG non-neutralizing antibodies present in CP may also contribute to improving recovery in COVID-19 patients through their neutralizing effects.53
Anti-Thrombotic Capability
CP, which is quickly frozen within six hours of collection and contains all pro- and anticoagulant elements in a physiologically balanced ratio84 (Figure 3).
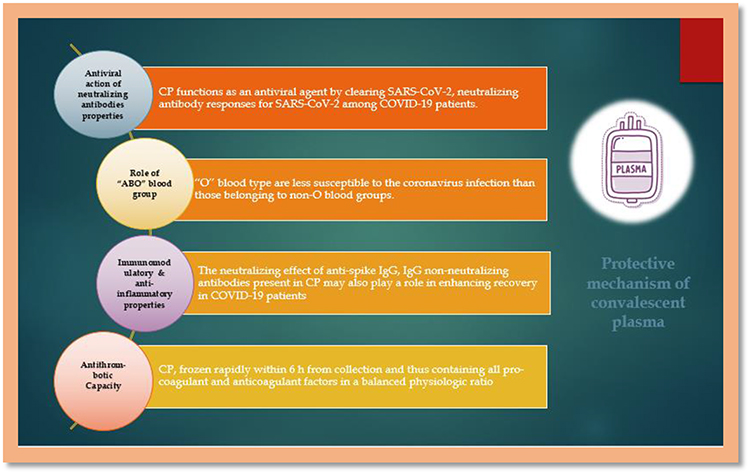 |
Figure 3 Protective mechanism of Convalescent plasma (CP). |
Discussion
The treatment to halt the course of early COVID-19 is still elusive, and CCP was first studied as a therapy among COVID-19 in patients.85 As CP treatment improved mortality in COVID-19 hospitalized patients,86 in contrast, the findings of another study on CP administered to hospitalized patients were ineffective, perhaps the antibodies needed to be administered earlier in the course of illness.87 These results differed from earlier research among hospitalized COVID-19 individuals with CP transfusions, and no randomized studies have shown a benefit for plasma in reducing mortality so far.88,89 Furthermore, the benefits were indicated by Libster et al on earlier plasma provision with high antibody titers. Hence, the investigators further examined the antibody titer of plasma provision, and the early infusion of high titer CP among COVID-19 infections can stop disease progression.87
At this point during pandemic, it looks like the compromised host with COVID-19 who is unable to mount their own antibody responses to the vaccine or past infection may benefit the most from passive antibody treatment. In that case, particularly in the absence of additional antiviral medications or progression despite normal therapy, high-titer CCP from a recently recovered donor is a viable option.90 The findings for monoclonal antibodies are highest when activity for the infective variation is maintained, and some but not all trials have indicated benefit for CCP. However, the precise niche for CCP and other antibody therapies remains unknown today, and in large part because of most available evidence was generated in the absence of current standard prevention and care strategies, such as vaccines and antiviral agents such as nirmatrelvir-ritonavir.91
The PLACID investigation (a multicenter clinical study) from India demonstrated that, while the CCP was effective in neutralizing the SARS-CoV-2 virus, it did not lower patient mortality.89 This conclusion might be explained by the fact that the most frequent cause of illness among COVID-19 individuals were SARS-CoV-2 virus-induced cytokine storm instead of the SARS-CoV-2 virus directly. The most likely cause of CCP therapy’s ineffectiveness on patient mortality is CCP infusion in people who have already developed significant COVID-19 symptoms. Moreover, non-neutralizing antibodies in CP can promote viral entry into macrophages. The virus multiplies rapidly in macrophages, creating a pro-inflammatory microenvironment that perpetuates the cytokine storm.92
Some RCT results have consistently demonstrated clear benefits only among outpatients managed within 5 days of the initial symptoms.87,93,94 Based on an optimistic case study, and an extensive case series,95,96 the FDA reauthorized CCP transfusion for immune-compromised patients on January 2022. A rising amount of data endorses the benefits of hybrid plasma, ie, CCP acquired from convalescent donors who have been vaccinated at least twice,97 as well as the significance of dose in CCP management.98 As per the findings demonstrated, among patients received 6 units of plasma from donors who were both sick and triple-vaccinated, and as a response, their anti-spike antibody values were exceedingly high.99
However, the initial data from the Mayo-sponsored extended access program revealed a positive safety profile among study samples; and adverse reaction rates were similar to those of non-immune plasma transfusions,36 and several observational studies, or NRSs, revealed beneficial results when compared to matched controls.100–103 As per the given limitations of available data as on August 2020 and the extent of outbreak and CCP usage under the expanded access protocol was escalated, and initial statistics on the potential efficacy of CCP were necessary to support the regulatory decision-making process.104
Recently, a mechanism on forecasting the potential benefit of CCP based on patient attributes was also revealed, and which may assist in identifying individuals who will benefit most from the CCP infusion,105 and as per the findings on 7 recently published RCTs, on treatment of CCP appears to be associated with improved outcomes, among 20 COVID-19 patients.106 As per the data on CP use for MERS,107,108 was limited, and studies in a small number of SARS patients suggested that CP may improve clinical outcomes when administered early in the illness or in those with severe disease.41,109,110 However, CCP treatment was initiated early in pandemic as a short-term strategy of providing immediate passive immunization to susceptible people and managing the disease until an effective and targeted drug could be discovered.111
Primarily, CCP was employed in a variety of nations since it was the only readily accessible therapy capable of avoiding SARS-CoV-2 cellular infection, inhibiting viral replication, and curing COVID-19.111,112 Fairly, CCP could be obtained swiftly as the number of patients recovering from the illness rose in high-income countries by exploiting established blood collection and transfusion infrastructures.111 Due to extended issues with donor recruitment, blood collection, inability to purchase CCP, and the characterization of CCP units, CCP was utilized less often in poor and middle-income countries during the early phases of the epidemic.113
The only difference between CCP and ordinary plasma infusions was that CCP contained anti-SARS-CoV-2 antibodies,37 and CCP was generally given to seriously or critically ill patients who were regularly in the ICU or under mechanical ventilation during the early phases of the epidemic.114–116 As few trials found that CCP may be beneficial when administered to patients at an earlier stage of illness,117,118 but these findings were not substantiated by more recent RCTs.119,120
The CCP NAbs may assist in restricting disease progression and activation of the inflammatory cascade leading to a cytokine storm in the early stages of the disease by blocking the viral entrance and intracellular replication.87,112 According to 2 controlled studies in this cohort,119,120 CCP treatment was shown to be related to considerably increased survival rates, while an uncontrolled case series revealed that CCP infusions resulted in clinical benefits.121,122 In Accordance with a preliminary study, immune-compromised patients with COVID-19 in an early stage of sickness and no detectable anti-SARS-CoV-2 antibodies are potential candidates for CCP treatment, and patients with a high post-transfusion antibody titer have the highest chance of success.123
Further to a recent evaluation, CCP with high titer NAbs is a safe and effective treatment for immune-compromised patients.95 The reported benefits of CCP in these patients may be explained by their lower risk of hyper-inflammation and cytokine storm as well as their higher risk of persistent SARS-CoV-2 infections, which may be treated with CCP infusions.96,123
Despite the low level of evidence for CP’s efficacy against other coronaviruses, the data indicated that CCP might be a potentially helpful treatment for COVID-19 patients,27 and CCP was associated with raised antibody levels but not with better outcomes in 59 patients compared to 15 controls.124 Another trial found that CCP infusions were well tolerated by the population. There were no reports related to transfusion reactions.27 A recently published RCT recommended that CCP with high titer NAbs levels in addition to high IgG levels be used if more studies evaluated its use in persons with low humoral immunity.125 So far, few data from adequately powered, randomized, controlled studies on CP therapy are available. In addition to that, several recent RCTs have revealed that CP treatment does not affect outcomes in patients with severe COVID-19.88,89
However, the current evidence, which is reinforced by the publication of Donated antibodies working against COVID-19 plasma and the clinical research of Sekine et al,126 does not warrant the use of CP in the standard COVID-19 treatment. More additional evidenced data is expected to emerge soon to help decide if CP transfusion, administered within 72 hours of the onset of symptoms, and may benefit some subgroups of individuals with very specific clinical and biological aspects. Mainly, these findings emphasize the need for restricting the compassionate use of treatment, conducting well-designed RCTs, and restricting treatments to those that are evidence-based.
As of July 8, 2022, the COVID-19 pandemic had caused 554 million illnesses and 6.35 million deaths worldwide. While the majority of immune-competent patients who have been triple vaccinated do not acquire severe illness following SARS-CoV-2 infection, immune compromised patients, particularly those with B-cell depletion, do not react to vaccinations and are thus at higher risk of sequelae.127
CP is a potentially useful therapy; nevertheless, the data on its effectiveness to date has not been well studied and consistent. There are currently no protocols in place for collecting and administering it during pandemics, and collecting enough CP with high titer NAb to treat a substantial number of patients and quickly and efficiently performing RCTs with low bias risks during a pandemic are major obstacles. Currently, researchers have a better grasp on how to prepare for next epidemic or pandemic, more than 1.5 years after the COVID-19 pandemic began. According to the findings, the CP is only beneficial if the antibody levels in the infused units are high and the etiology of the sickness is unknown enough to determine the optimal therapeutic strategies.27
Additionally, it is necessary to develop a reliable procedure for selecting potential donors who have been cured of the ailment. As a result, consistent viral nucleic acid diagnostics and antibody assays should be established as quickly as possible for screening necessities, and only men or nulliparous women with no history of transfusions should be regarded as donors in the absence of testing, as they should be anti-HLA negative.113
The establishment of a CP donor registry might be beneficial in identifying possible donors for future donations. A frozen and ready-to-use CP plasma bank might also be built by collecting plasma from all potential donors once or twice, especially in the early stages of a pandemic. It is critical to determine if the virus may be transmitted by transfusion, and pathogen inactivation techniques should be investigated until this is proven, particularly if prophylactic CP infusion after a potential exposure is contemplated. Furthermore, in epidemics or pandemics, finding CP patients with low antibody levels is crucial for implementing a successful CP strategy.27
Adoption and application of CP treatment in later stages of pandemics may vary by nation. Because of practical problems, the early stages of CP therapy may be more difficult and necessitate unique solutions in underdeveloped countries. Researchers believe that CP, in addition to standard therapy, might be utilized to treat severe cases of COVID-19 pneumonia or individuals with decreased antibodies response to SAR-CoV-2 in the first week of symptoms or during the viremia phase.113
At this point in the pandemic, it looks like the immune-compromised patients with COVID-19 hosts who are unable to mount their own antibody response to the vaccine or prior infection will gain the most from passive antibody treatment. In that scenario, particularly in the absence of additional antiviral therapies or progression despite normal therapy, high-titer CCP from a recently recovered donor is a feasible strategy. In that context, findings for monoclonal antibodies are highest when activity for the infecting variation is maintained, and some but not all trials have indicated benefit for CCP.
Given the limited therapy choices and historical precedence, the FDA approved CCP for use beginning in April 2020. Concurrently, several RCTs with diverse trial designs and research populations, such as preventive, early outpatient usage, and hospitalized patients with severe disease, were approved under investigational new drug applications. Simultaneously, many RCTs with varied trial designs and research groups, such as prophylaxis, early opioid usage, and hospitalized patients with severe illness, proceeded forward under investigational new drug applications. Several observational studies, or NRSs, revealed beneficial results when compared to matched controls.
The case findings are as follows: the strengths of the analysis on early administration of CCP with high titer antibody content by live viral neutralization assay are associated with modest clinical efficacy, providing greater precision concerning CCP biologic activity and the power to detect modest treatment effects in the overall heterogeneous hospitalized population, reflecting real-world use of CCP in the early pandemic.104
The findings of studies in the hospitalized population, where effects may be seen only in subgroups, must be interpreted in light of the timing of CCP transfusion relative to the onset of the illness, the host immunological condition, and the neutralizing activity of the CCP transfused. The inquiry into how to most effectively use CCP and which patients may benefit the most from it is ongoing; RCTs, as well as an analysis of subgroups within RCTs, will remain crucial in identifying the potential role of CCP in COVID-19 treatment. The CCP may have an influence on COVID-19 treatment in vulnerable patients in the future if variations arise that are not reduced by existing known treatments, despite having just a little clinical effect in the current trial.
A meta-analysis discovered that CCP treatment, like CP infusions, had a clinically acceptable safety profile in COVID-19 patients. While the bulk of the 7 newly published RCTs confirms CCP’s reassuring safety profile, the death rate was significantly lower or tended to be lower in all COVID-19 patients who took CCP compared to control patients. Individuals who got CCP had a longer hospital stay in several trials. Other studies found that CCP improved disease progression, hypoxic condition mitigation, WHO intensity score, respiratory specifications, rate and time to clinical benefit, need for mechanical ventilation, extubation rate, time for recovery from major illness, rate of mechanical ventilation and vasopressor assistance, rate of transition to mechanical ventilation, and clinical status in the overall study participants or specific subgroups of participants.
The most prevalent CCP transfusion-related issues in certain countries include allergic transfusion reactions, transfusion-related acute lung damage, and transfusion-associated circulatory overload, all of which are curable. Another potential risk of CCP infusions was antibody-dependent acceleration of infection, which is a process in which non-NAbs, commonly created after a previous infection with a different viral serotype, increase viral cellular entry, exacerbating symptoms.128,129 This possible danger has not been observed with CCP infusions. Even though CP transfusions may be a beneficial treatment option in critically ill patients with other ailments, no positive impact of CCP was discerned in patients with COVID-19 at a delayed disease stage who were at high risk of death due to hyper-inflammation or health complications rather than the SARS-CoV-2 infection itself.87,112
For any future use of CP in the context of an emerging infectious disease outbreak, well-defined patient scoring systems based on characteristics other than time from symptom start or hospital admission or ICU are essential. In addition to symptom persistence (though disease progression varies from patient to patient), standardized criteria should be based on viral pathophysiology, illness intensity (eg, even without mechanical ventilation), and number of days post-hospital admission (correlated to symptom severity).
Later in the disease course, antibody testing may be useful in identifying patients who have not yet generated sufficient antibody levels and may benefit from CP. Furthermore, in people with early infection, binding antibody signals may not accurately indicate N-Abs levels and should not be used as the sole justification for commencing CP infusions.125,130 Another option for characterizing sickness stages is to routinely use the WHO clinical progression scale.131
CCP may enhance clinical outcomes in some subpopulations of COVID-19 patients, but its use in the general population does not appear to be beneficial. Researchers recognized immune compromised patients (eg, organ transplant recipients or patients with primary or secondary immunodeficiencies, B-cell depletion, or malignancies) as a prospective target population that may benefit more from CCP treatment based on existing research, clinical experience, and the pathophysiology of COVID-19.96,123,132
Potentially CCP-related reactions included anemia, urticarial, nausea, shortness of breath, irregular heartbeats, and tachycardia, as well as local injection site reactions (pain, chills, rash, redness, and itchy skin), intravenous cannula obstruction, transfusion-related acute pulmonary injury, transfusion-associated cardiovascular burdening, respiratory, allergic, febrile non-hemolytic, and hypotensive reactions, etc.
The study demonstrated how a critical acute respiratory distress syndrome patient who was refractory to current standard medical treatment responded dramatically to ABO-incompatible CP transfusion without any transfusion reactions. They further argued that CP transfusion in severe COVID-19 pneumonia is clinically helpful, especially in the less compatible ABO-blood group. However, this is simply an anecdotal report; a larger evaluation of CP transfusion in critically ill COVID-19 pneumonia patients is necessary before this can be suggested as standard treatment.133
Studies believe that the clinical improvement in the patient’s condition was caused by other medications administered in conjunction with CP. In patients who do not have a conventional treatment and have a high death rate due to the underlying condition, CP can be used as an additional therapeutic agent. Finally, when administered to asymptomatic and immune-compromised patients with good infection control practices as soon as they are diagnosed, this therapy may be more beneficial.26
Complications and Limitations of CP Applications
Adverse Reactions
There have been reports of adverse reactions ranging from mild fever to allergic reactions to life-threatening bronchospasm, circulatory overload in patients with cardiorespiratory diseases, and renal impairment especially, among the elderly population.111,134
Immunological Reactions
The plasma administration may result in serious allergic responses. As allergic reaction to components of donor plasma or serum can cause serum sickness and anaphylaxis, and also bronchospasm may be linked to these reactions.135
Risk of Transfusion-Associated Infections
Administration of CP carries possibility of transferring possible pathogens, including SARS-CoV-2 itself as well as other pathogenic agents such as hepatitis B and C viruses, human immunodeficiency virus, and Treponema pallidum. This risk may present even though it is pretty uncommon, and thus necessary to screen for existence of these pathogens in order to reduce the risk of infections related to transfusions.135
Risk of Reinfection
Administration of CP, or passive antibodies, may decrease the formation of specific antibodies against SARS-CoV-2 by inhibiting or impairing the recipient’s humoral immune response (pathogen-specific antibodies). This could increase a person’s susceptibility to SARS-CoV-2 reinfection.135
Antibody-Dependent Enhancement
There is a remote possibility of antibody-dependent enhancement of the disease process. It is a process in which antibodies present in the donor’s plasma may exacerbate disease by enhancing the entry of viruses into host cells and the multiplication of viruses.135
Other Adverse Reactions
There is a tiny possibility that an antibody-dependent enhancement of illness process may occur. As by facilitating virus entry into host cells and virus replication, antibodies found in donor plasma may aggravate illness.135
One of the patients who underwent CP therapy reportedly developed an ephemeral facial red spot,49 and there have also been reports on phlebitis and widespread jaundice in certain patients.
Other limiting factors may be a lack of neutralizing antibodies in patient plasma, large infusion volumes, and the time of infusion administration, waning of plasma antibodies, bridging the gap between COVID-19 positive and recovered cases, basic administrative and logistical barriers, and also donor eligibility criteria.
Conclusion
The stability and high potential efficiency of CPT as a COVID-19 therapeutic approach CP treatment can reduce mortality in COVID-19 while enhancing respiration, inflammatory cytokines, interleukin-6, and ferritin with no rise in adverse effects. For immune compromised patients who do not react to vaccinations, the COVID-19 burden remains unchanged. Additionally, CCP therapy is being utilized as an experimental treatment as early as January 2020, and with the developing understanding of COVID-19, CCP treatment has emerged as an essential experimental therapeutic being employed in the management of the disease. Moreover, CP treatment is risk-free and may help COVID-19 patients.
Furthermore, the multiple trials have demonstrated that CCP infusions are ineffective in treating COVID-19 patients, the issue of whether plasma from vaccinated individuals could be useful remains unanswered. Along this, it was recently demonstrated that, while immunization reduced in vitro neutralization capacity against specific variations, vaccinated people preserved neutralization capability against the majority of developing variants. As a result, gathering CCP from people who have been vaccinated and recovered from the first illness is important.
The storage of plasma acquired after vaccination may have a role in the creation of a more aggressive variant or during the present vaccination gap in some countries, assisting in better preparedness for the next wave of diseases. However, CP infusions do not appear to be effective in critically ill patients for some viral infections when the life-threatening symptoms are not the direct result of viral cellular damage, such as COVID-19, but may enhance clinical outcomes in specific subpopulations.
In addition to this, the COVID-19 needs more investigation to determine whether CCP infusions may be beneficial in the early stages of immune-compromised disease. Focusing to, the CP treatment may stop infections in future pandemics or epidemics and should not be confined to seriously ill individuals but should be delivered at the early stages of the disease to all patients or certain subpopulations of vulnerable persons. Interestingly, in an ideal world, a standardized protocol for RCTs studying CP safety and efficacy would be devised, made available, and ready for use internationally.
Data Sharing Statement
The study used data available within the manuscript.
Acknowledgment
Arsi University, College of Health Sciences, Ethiopia
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; they took part in drafting, revising, or critically reviewing the article; they gave final approval of the version to be published; they agreed on the journal to which the article had been submitted; and they agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dhama K, Khan S, Tiwari R, et al. Coronavirus Disease 2019-COVID-19. Clin Microbiol Rev. 2020;33:e00028–20. doi:10.1128/CMR.00028-20
2. Dai R, Hu M, Tang H, Peng Z, Yan C, Emran TB. Efficacy and safety of convalescence plasma therapy in COVID-19 patients: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2022;2022:e7670817. doi:10.1155/2022/7670817
3. Clark NM, Janaka SK, Hartman W, et al. Anti-SARS-CoV-2 IgG and IgA antibodies in COVID-19 convalescent plasma do not enhance viral infection. PLoS One. 2022;17(3):e0257930. doi:10.1371/journal.pone.0257930
4. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of Coronavirus Disease 2019 (COVID-19): a Review. JAMA. 2020;324(8):782–793. doi:10.1001/jama.2020.12839
5. Wu Z, McGoogan JM. Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
6. Coomes EA, Haghbayan H. Interleukin-6 in Covid-19: a systematic review and meta-analysis. Rev Med Virol. 2020;30(6):1–9. doi:10.1002/rmv.2141
7. Chen R, Lan Z, Ye J, et al. Cytokine storm: the primary determinant for the pathophysiological evolution of COVID-19 deterioration. Front Immunol. 2021;12:589095.
8. Rahman M, Islam M, Shohag S, et al. Multifaceted role of natural sources for COVID-19 pandemic as marine drugs. Environ Sci Pollut Res. 2022;29:46527–46550. doi:10.1007/s11356-022-20328-5
9. Phan T. Genetic diversity and evolution of SARS-CoV-2. Infect Genet Evol. 2020;81:104260.
10. Islam F, Dhawan M, Nafady MH, et al. Understanding the omicron variant (B.1.1.529) of SARS-CoV-2: mutational impacts, concerns, and the possible solutions. Ann Med Surg. 2022;78:103737. doi:10.1016/j.amsu.2022.103737
11. Song P, Li W, Xie J, Hou Y, You C. Cytokine storm induced by SARS-CoV-2. Clin Chim Acta. 2020;509:280–287. doi:10.1016/j.cca.2020.06.017
12. Nagant C, Ponthieux F, Smet J, et al. A score combining early detection of cytokines accurately predicts COVID-19 severity and intensive care unit transfer. Int J Infect Dis. 2020;101:342–345. doi:10.1016/j.ijid.2020.10.003
13. Lippi G, Plebani M. Cytokine “storm”, cytokine “breeze”, or both in COVID-19? Clin Chem Lab Med. 2021;59(4):637–639. doi:10.1515/cclm-2020-1761
14. Boehm E, Kronig I, Neher RA, et al. Novel SARS-CoV-2 variants: the pandemics within the pandemic. Clin Microbiol Infect. 2021;27:1109–1117.
15. Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm’ in COVID-19. J Infect. 2020;80:607–613. doi:10.1016/j.jinf.2020.03.037
16. Cao B, Wang Y, Wen D, et al. A trial of lopinavir–ritonavir in adults hospitalized with severe Covid-19. N Engl J Med. 2020;382(19):1787–1799. doi:10.1056/NEJMoa2001282
17. Stone JH, Frigault MJ, Serling-Boyd NJ, et al. Efficacy of tocilizumab in patients hospitalized with Covid-19. N Engl J Med. 2020;383(24):2333–2344. doi:10.1056/NEJMoa2028836
18. Bakhiet M, Taurin S. SARS-CoV-2: targeted managements and vaccine development. Cytokine Growth Factor Rev. 2021;58:16–29. doi:10.1016/j.cytogfr.2020.11.001
19. Klassen SA, Senefeld JW, Senese KA, et al. Convalescent plasma therapy for COVID-19: a graphical mosaic of the worldwide evidence. Front Med. 2021;8. doi:10.3389/fmed.2021.684151
20. Harvey WT, Carabelli AM, Jackson B, et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat Rev Microbiol. 2021;19(7):409–424. doi:10.1038/s41579-021-00573-0
21. Wouters OJ, Shadlen KC, Salcher-Konrad M, et al. Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation, and deployment. Lancet Lond Engl. 2021;397(10278):1023–1034. doi:10.1016/S0140-6736(21)00306-8
22. Tharmarajah E, Buazon A, Patel V, et al. IL-6 inhibition in the treatment of COVID-19: a meta-analysis and meta-regression. J Infect. 2021;82(5):178–185. doi:10.1016/j.jinf.2021.03.008
23. Cron RQ. COVID-19 cytokine storm: targeting the appropriate cytokine. Lancet Rheumatol. 2021;3(4):e236–e237. doi:10.1016/S2665-9913(21)00011-4
24. Reeves HM, Winters JL. The mechanisms of action of plasma exchange. Br J Haematol. 2014;164(3):342–351. doi:10.1111/bjh.12629
25. Tabibi S, Tabibi T, Conic RRZ, Banisaeed N, Streiff MB. Therapeutic plasma exchange: a potential management strategy for critically ill COVID-19 patients. J Intensive Care Med. 2020;35(9):827–835. doi:10.1177/0885066620940259
26. Biçim S, Berber İ, Ali Erkurt M, et al. The prophylactic treatment of COVID-19 in a renal failure and Hodgkin lymphoma patient with convalescent plasma. IJR2H. 2022; 5 (2) : 1–5.
27. Beraud M, Goodhue Meyer E, Lozano M, Bah A, Vassallo R, Brown BL. Lessons learned from the use of convalescent plasma for the treatment of COVID-19 and specific considerations for immunocompromised patients. Transfus Apher Sci. 2022;61(3):103355. doi:10.1016/j.transci.2022.103355
28. Klassen SA, Senefeld JW, Johnson PW, et al. The effect of convalescent plasma therapy on mortality among patients with COVID-19: systematic review and meta-analysis. Mayo Clin Proc. 2021;96(5):1262–1275. doi:10.1016/j.mayocp.2021.02.008
29. Nabil A, Uto K, Elshemy MM, et al. Current coronavirus (SARS-CoV-2) epidemiological, diagnostic and therapeutic approaches: an updated review until June 2020. EXCLI J. 2020;19:992–1016. doi:10.17179/excli2020-2554
30. Keller MA, Stiehm ER. Passive immunity in prevention and treatment of infectious diseases. Clin Microbiol Rev. 2000;13(4):602–614. doi:10.1128/CMR.13.4.602
31. Casadevall A, Dadachova E, Pirofski L. Passive antibody therapy for infectious diseases. Nat Rev Microbiol. 2004;2(9):695–703. doi:10.1038/nrmicro974
32. Rejeki MS, Sarnadi N, Wihastuti R, et al. Convalescent plasma therapy in patients with moderate-to-severe COVID-19: a study from Indonesia for clinical research in low- and middle-income countries. eClinicalMedicine. 2021;36:100931. doi:10.1016/j.eclinm.2021.100931
33. Maiztegui JI, Fernandez NJ, de Damilano AJ. Efficacy of immune plasma in treatment of argentine haemorrhagic fever and association between treatment and a late neurological syndrome. Lancet Lond Engl. 1979;314(8154):1216–1217. doi:10.1016/S0140-6736(79)92335-3
34. Beigel JH, Tebas P, Elie-Turenne M-C, et al. Immune plasma for the treatment of severe influenza: an open-label, multicentre, Phase 2 randomised study. Lancet Respir Med. 2017;5(6):500–511. doi:10.1016/S2213-2600(17)30174-1
35. Arnold Egloff SA, Junglen A, Restivo JSA, et al. Convalescent plasma associates with reduced mortality and improved clinical trajectory in patients hospitalized with COVID-19. J Clin Invest. 2021;131(20):e151788. doi:10.1172/JCI151788
36. Joyner MJ, Bruno KA, Klassen SA, et al. Safety Update: COVID-19 convalescent plasma in 20,000 hospitalized patients. Mayo Clin Proc. 2020;95(9):1888–1897. doi:10.1016/j.mayocp.2020.06.028
37. Cohn CS, Estcourt L, Grossman BJ, et al. COVID −19 convalescent plasma: interim recommendations from the AABB. Transfusion. 2021;61(4):1313–1323. doi:10.1111/trf.16328
38. Bloch EM, Tobian AAR, Shoham S, et al. How do I implement an outpatient program for the administration of convalescent plasma for COVID −19? Transfusion. 2022;62(5):933–941. doi:10.1111/trf.16871
39. Marano G, Vaglio S, Pupella S, et al. Convalescent plasma: new evidence for an old therapeutic tool? Blood Transfus Trasfus Sangue. 2016;14:152–157.
40. McGuire LW, Redden WR. The use of convalescent human serum in influenza pneumonia—a preliminary report. Am J Public Health. 1918;8(10):741–744. doi:10.2105/AJPH.8.10.741
41. Cheng Y, Wong R, Soo YOY, et al. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur J Clin Microbiol Infect Dis. 2005;24(1):44–46. doi:10.1007/s10096-004-1271-9
42. Hung IF, To KK, Lee C-K, et al. Convalescent plasma treatment reduced mortality in patients with severe pandemic influenza A (H1N1) 2009 virus infection. Clin Infect Dis. 2011;52(4):447–456. doi:10.1093/cid/ciq106
43. van Griensven J, Edwards T, de Lamballerie X, et al. Evaluation of convalescent plasma for Ebola virus disease in Guinea. N Engl J Med. 2016;374(1):33–42. doi:10.1056/NEJMoa1511812
44. Imai M, Iwatsuki-Horimoto K, Hatta M, et al. Syrian hamsters as a small animal model for SARS-CoV-2 infection and countermeasure development. Proc Natl Acad Sci U S A. 2020;117(28):16587–16595. doi:10.1073/pnas.2009799117
45. Sun J, Zhuang Z, Zheng J, et al. Generation of a broadly useful model for COVID-19 pathogenesis, vaccination, and treatment. Cell. 2020;182(3):734–743.e5. doi:10.1016/j.cell.2020.06.010
46. Chan JF-W, Zhang AJ, Yuan S, et al. Simulation of the clinical and pathological manifestations of Coronavirus Disease 2019 (COVID-19) in a golden Syrian hamster model: implications for disease pathogenesis and transmissibility. Clin Infect Dis;2020. ciaa325. doi:10.1093/cid/ciaa325
47. McMahan K, Yu J, Mercado NB, et al. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature. 2021;590(7847):630–634. doi:10.1038/s41586-020-03041-6
48. Cross RW, Prasad AN, Borisevich V, et al. Use of convalescent serum reduces severity of COVID-19 in nonhuman primates. Cell Rep. 2021;34(10):108837. doi:10.1016/j.celrep.2021.108837
49. Duan K, Liu B, Li C, et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc Natl Acad Sci. 2020;117(17):9490–9496. doi:10.1073/pnas.2004168117
50. Shen C, Wang Z, Zhao F, et al. Treatment of 5 critically ill patients with COVID-19 with convalescent plasma. JAMA. 2020;323(16):1582–1589. doi:10.1001/jama.2020.4783
51. Zhang B, Liu S, Tan T, et al. Treatment with convalescent plasma for critically ill patients with severe acute respiratory syndrome coronavirus 2 infection. Chest. 2020;158(1):e9–e13. doi:10.1016/j.chest.2020.03.039
52. Cognasse F, Hamzeh-Cognasse H, Rosa M, et al. Inflammatory markers and auto-abs to type I IFNs in COVID-19 convalescent plasma; 2022;87:104414.
53. Casadevall A, Pirofski L-A. The convalescent sera option for containing COVID-19. J Clin Invest. 2020;130(4):1545–1548. doi:10.1172/JCI138003
54. Seghatchian J, Lanza F. Convalescent plasma, an apheresis research project targeting and motivating the fully recovered COVID 19 patients: a rousing message of clinical benefit to both donors and recipients alike. Transfus Apher Sci. 2020;59(3):102794. doi:10.1016/j.transci.2020.102794
55. Pool JG, Hershgold EJ, Pappenhagen AR. High-potency antihaemophilic factor concentrate prepared from cryoglobulin precipitate. Nature. 1964;203(4942):312. doi:10.1038/203312a0
56. Franchini M. Convalescent plasma therapy for managing infectious diseases: a narrative review. Ann Blood. 2021;6:17. doi:10.21037/aob-2020-cp-03
57. Psaltopoulou T, Sergentanis TN, Pappa V, et al. The emerging role of convalescent plasma in the treatment of COVID-19. HemaSphere. 2020;4(3):e409. doi:10.1097/HS9.0000000000000409
58. World Health Organization. Use of Convalescent Whole Blood or Plasma Collected from Patients Recovered from Ebola Virus Disease for Transfusion, as an Empirical Treatment During Outbreaks: Interim Guidance for National Health Authorities and Blood Transfusion Services. World Health Organization; 2014.
59. Luke TC, Kilbane EM, Jackson JL, Hoffman SL. Meta-analysis: convalescent blood products for Spanish influenza pneumonia: a future H5N1 treatment? Ann Intern Med. 2006;145(8):599–609. doi:10.7326/0003-4819-145-8-200610170-00139
60. Mair-Jenkins J, Saavedra-Campos M, Baillie JK, et al. The effectiveness of convalescent plasma and hyperimmune immunoglobulin for the treatment of severe acute respiratory infections of viral etiology: a systematic review and exploratory meta-analysis. J Infect Dis. 2015;211(1):80–90. doi:10.1093/infdis/jiu396
61. Arabi Y, Balkhy H, Hajeer AH, et al. Feasibility, safety, clinical, and laboratory effects of convalescent plasma therapy for patients with Middle East respiratory syndrome coronavirus infection: a study protocol. SpringerPlus. 2015;4(1):709. doi:10.1186/s40064-015-1490-9
62. Park WH, Freeman RG Jr. The prophylactic use of measles convalescent serum. J Am Med Assoc. 1926;87(8):556–558. doi:10.1001/jama.1926.02680080022009
63. Park WH. Therapeutic use of antipoliomyelitis serum in preparalytic cases of poliomyelitis. J Am Med Assoc. 1932;99(13):1050–1053. doi:10.1001/jama.1932.02740650008003
64. Rambar AC. Mumps; use of convalescent serum in the treatment and prophylaxis of orchitis. Am J Dis Child. 1946;71(1):1–13. doi:10.1001/archpedi.1946.02020240008001
65. Contreras-Barbeta E, Millan A, Rello J. Convalescent plasma for SARS-CoV-2 infection: win or learn. Eur Respir J. 2022;59(2):2102076. doi:10.1183/13993003.02076-2021
66. Brosig AM, Ossner T, Pamler I, et al. Multistep screening and selection of COVID-19 convalescent plasma donors at the early stage of the SARS-CoV-2 pandemic: a retrospective analysis. Health Sci Rep. 2022;5(5):e815. doi:10.1002/hsr2.815
67. Chen B, Xia R. Early experience with convalescent plasma as immunotherapy for COVID-19 in China: knowns and unknowns. Vox Sang. 2020;115(6):507–514. doi:10.1111/vox.12968
68. Soo YOY, Cheng Y, Wong R, et al. Retrospective comparison of convalescent plasma with continuing high-dose methylprednisolone treatment in SARS patients. Clin Microbiol Infect. 2004;10(7):676–678. doi:10.1111/j.1469-0691.2004.00956.x
69. Duan K, Liu B, Li C, et al. The feasibility of convalescent plasma therapy in severe COVID- 19 patients: a pilot study. MedRxiv. 2020;2020:2020. doi:10.1109/EMBC44109.2020.9175277
70. Cristelli MP, Langhi Junior DM, Viana LA, et al. Efficacy of convalescent plasma to treat mild to moderate COVID-19 in kidney transplant patients: a propensity score matching analysis. Transplantation. 2022;106:e92–e94. doi:10.1097/TP.0000000000003962
71. Budhai A, Wu AA, Hall L, et al. How did we rapidly implement a convalescent plasma program? Transfusion. 2020;60:1348–1355. doi:10.1111/trf.15910
72. FDA. Investigational COVID-19 convalescent plasma. U.S. Food and drug administration; 2022. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/investigational-covid-19-convalescent-plasma.
73. Bacal CJO, Maina JW, Nandurkar HH, et al. Blood apheresis technologies – a critical review on challenges towards efficient blood separation and treatment. Mater Adv. 2021;2:7210–7236. doi:10.1039/D1MA00859E
74. Tiberghien P, de Lamballerie X, Morel P, Gallian P, Lacombe K, Yazdanpanah Y. Collecting and evaluating convalescent plasma for COVID-19 treatment: why and how? Vox Sang. 2020;115:488–494. doi:10.1111/vox.12926
75. Jones JM, Faruqi AJ, Sullivan JK, Calabrese C, Calabrese LH. COVID-19 outcomes in patients undergoing b cell depletion therapy and those with humoral immunodeficiency states: a scoping review. Pathog Immun. 2021;6:76–103. doi:10.20411/pai.v6i1.435
76. Apostolidis SA, Kakara M, Painter MM, et al. Cellular and humoral immune responses following SARS-CoV-2 mRNA vaccination in patients with multiple sclerosis on anti-CD20 therapy. Nat Med. 2021;27(11):1990–2001. doi:10.1038/s41591-021-01507-2
77. Honjo K, Russell RM, Li R, et al. Convalescent plasma-mediated resolution of COVID-19 in a patient with humoral immunodeficiency. Cell Rep Med. 2021;2(1):100164. doi:10.1016/j.xcrm.2020.100164
78. Dunbar NM, Yazer MH. Biomedical Excellence for Safer Transfusion (BEST) collaborative and the STAT study investigators. Safety of the use of group A plasma in trauma: the STAT study. Transfusion. 2017;57(8):1879–1884. doi:10.1111/trf.14139
79. Bilir Y, Bilir A, Ciyiltepe F, Bombacı E, Saraçoglu A, Saraçoğlu KT. Comparison of the effectiveness of early and late convalescent plasma treatment given in patients diagnosed with coronavirus disease in intensive care unit. Kocaeli Med J. 2022;11(1):43–51. doi:10.5505/ktd.2022.39260
80. Wang P, Liu L, Nair MS, et al. SARS-CoV-2 neutralizing antibody responses are more robust in patients with severe disease. Emerg Microbes Infect. 2020;9:2091–2093. doi:10.1080/22221751.2020.1823890
81. Del Fante C, Franchini M, Baldanti F, et al. A retrospective study assessing the characteristics of COVID-19 convalescent plasma donors and donations. Transfusion. 2021;61:830–838.
82. Wu -B-B, Gu D-Z, Yu J-N, Yang J, Shen W-Q. Association between ABO blood groups and COVID-19 infection, severity and demise: a systematic review and meta-analysis. Infect Genet Evol. 2020;84:104485. doi:10.1016/j.meegid.2020.104485
83. Franchini M, Glingani C, Del Fante C, et al. The protective effect of O blood type against SARS-CoV-2 infection. Vox Sang. 2021;116:249–250.
84. Liumbruno GM, Marano G, Grazzini G, Capuzzo E, Franchini M. Solvent/detergent-treated plasma: a tale of 30 years of experience. Expert Rev Hematol. 2015;8(3):9490–9496. doi:10.1586/17474086.2015.1016906
85. Focosi D, Franchini M, Pirofski L, et al. COVID-19 convalescent plasma and clinical trials: understanding conflicting outcomes. Clin Microbiol Rev. 2022;35(3):e00200–e00221. doi:10.1128/cmr.00200-21
86. Cacilhas P, Caberlon E, Angoleri L, Fassina K, Ribeiro RN, Pinto LC. Convalescent plasma therapy in COVID-19 patients: a non-randomized case-control study with concurrent control. Braz J Med Biol Res. 2022;55:1.
87. Libster R, Pérez Marc G, Wappner D, et al. Early high-titer plasma therapy to prevent severe Covid-19 in older adults. N Engl J Med. 2021;384(7):610–618. doi:10.1056/NEJMoa2033700
88. Simonovich VA, Burgos Pratx LD, Scibona P, et al. A randomized trial of convalescent plasma in Covid-19 severe pneumonia. N Engl J Med. 2021;384(7):619–629. doi:10.1056/NEJMoa2031304
89. Agarwal A, Mukherjee A, Kumar G, Chatterjee P, Bhatnagar T, Malhotra P. Convalescent plasma in the management of moderate covid-19 in adults in India: open label Phase II multicentre randomised controlled trial (PLACID trial). BMJ. 2020;371:m3939. doi:10.1136/bmj.m3939
90. Baker JV, Lane HC. The fast and the furious: chasing a clinical niche for COVID-19 convalescent plasma. Ann Intern Med. 2022;175(9):1332–1334. doi:10.7326/M22-2329
91. Hammond J, Leister-Tebbe H, Gardner A, et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with Covid-19. N Engl J Med. 2022;386(15):115–408. doi:10.1056/NEJMoa2118542
92. Channappanavar R, Fehr AR, Vijay R, et al. Dysregulated type I interferon and inflammatory monocyte-macrophage responses cause lethal pneumonia in SARS-CoV-infected mice. Cell Host Microbe. 2016;19(2):695–703. doi:10.1016/j.chom.2016.01.007
93. Sullivan DJ, Gebo KA, Shoham S, et al. Early outpatient treatment for Covid-19 with convalescent plasma. N Engl J Med. 2022;386(18):44–46. doi:10.1056/NEJMoa2119657
94. Millat-Martinez P, Gharbharan A, Alemany A, et al. Prospective individual patient data meta-analysis of two randomized trials on convalescent plasma for COVID-19 outpatients. Nat Commun. 2022;13(1):2583. doi:10.1038/s41467-022-29911-3
95. Focosi D, Franchini M. Potential use of convalescent plasma for SARS-CoV-2 prophylaxis and treatment in immunocompromised and vulnerable populations. Expert Rev Vaccines. 2022;21(7):877–884. doi:10.1080/14760584.2021.1932475
96. Hueso T, Godron A-S, Lanoy E, et al. Convalescent plasma improves overall survival in patients with B-cell lymphoid malignancy and COVID-19: a longitudinal cohort and propensity score analysis. Leukemia. 2022;36(4):1025–1034. doi:10.1038/s41375-022-01511-6
97. Focosi D, Franchini M, Joyner MJ, Casadevall A, Sullivan DJ. Analysis of anti-omicron neutralizing antibody titers in different convalescent plasma sources. medRxiv. 2022;2021. doi:10.1101/2021.12.24.21268317
98. Rijnders BJA, Huygens S, Mitjà O. Evidence-based dosing of convalescent plasma for COVID-19 in future trials. Clin Microbiol Infect. 2022;28:667–671. doi:10.1016/j.cmi.2022.01.026
99. Belcari G, Conti A, Mazzoni A, Lanza M, Mazzetti P, Focosi D. Clinical and virological response to convalescent plasma in a chronic lymphocytic leukemia patient with COVID-19 Pneumonia. Life. 2022;12:1098. doi:10.3390/life12071098
100. Hegerova L, Gooley TA, Sweerus KA, et al. Use of convalescent plasma in hospitalized patients with COVID-19: case series. Blood. 2020;136:759–762. doi:10.1182/blood.2020006964
101. Liu STH, Lin H-M, Baine I, et al. Convalescent plasma treatment of severe COVID-19: a propensity score-matched control study. Nat Med. 2020;26:1708–1713. doi:10.1038/s41591-020-1088-9
102. Salazar E, Christensen PA, Graviss EA, et al. Treatment of coronavirus disease 2019 patients with convalescent plasma reveals a signal of significantly decreased mortality. Am J Pathol. 2020;190(11):2290–2303. doi:10.1016/j.ajpath.2020.08.001
103. Abolghasemi H, Eshghi P, Cheraghali AM, et al. Clinical efficacy of convalescent plasma for treatment of COVID-19 infections: results of a multicenter clinical study. Transfus Apher Sci. 2020;59(5):102875. doi:10.1016/j.transci.2020.102875
104. Belov A, Huang Y, Villa CH, et al. Early administration of COVID-19 convalescent plasma with high titer antibody content by live viral neutralization assay is associated with modest clinical efficacy. Am J Hematol. 2022;97:770–779. doi:10.1002/ajh.26531
105. Park H, Tarpey T, Liu M, et al. Development and validation of a treatment benefit index to identify hospitalized patients with COVID-19 who may benefit from convalescent plasma. JAMA Netw Open. 2022;5(1):e2147375. doi:10.1001/jamanetworkopen.2021.47375
106. Pardiwalla B, Yadav A, Bhatia A, et al. Convalescent plasma to limit coronavirus associated complications: a proof of concept phase-2 clinical study at a designated COVID-19 hospital in Mumbai city. J Curr Med Res Opin. 2021;4(05):940–949. doi:10.15520/jcmro.v4i05.419
107. Arabi YM, Hajeer AH, Luke T, et al. Feasibility of using convalescent plasma immunotherapy for MERS-CoV infection, Saudi Arabia. Emerg Infect Dis. 2016;22(9):1554–1561. doi:10.3201/eid2209.151164
108. Ko J-H, Seok H, Cho SY, et al. Challenges of convalescent plasma infusion therapy in Middle East respiratory coronavirus infection: a single centre experience. Antivir Ther. 2018;23(7):617–622. doi:10.3851/IMP3243
109. Zhang J-S, Chen J-T, Liu Y-X, et al. A serological survey on neutralizing antibody titer of SARS convalescent sera. J Med Virol. 2005;77(2):147–150. doi:10.1002/jmv.20431
110. Yeh K-M, Chiueh T-S, Siu LK, et al. Experience of using convalescent plasma for severe acute respiratory syndrome among healthcare workers in a Taiwan hospital. J Antimicrob Chemother. 2005;56(5):919–922. doi:10.1093/jac/dki346
111. Bloch EM, Shoham S, Casadevall A, et al. Deployment of convalescent plasma for the prevention and treatment of COVID-19. J Clin Invest. 2020;130(6):2757–2765. doi:10.1172/JCI138745
112. Franchini M, Liumbruno GM, Piacentini G, Glingani C, Zaffanello M. The three pillars of COVID-19 convalescent plasma therapy. Life. 2021;11(4):354. doi:10.3390/life11040354
113. Bloch EM, Goel R, Wendel S, et al. Guidance for the procurement of COVID-19 convalescent plasma: differences between high- and low-middle-income countries. Vox Sang. 2021;116(1):18–35. doi:10.1111/vox.12970
114. Pouladzadeh M, Safdarian M, Eshghi P, et al. A randomized clinical trial evaluating the immunomodulatory effect of convalescent plasma on COVID-19-related cytokine storm. Intern Emerg Med. 2021;16(8):2181–2191. doi:10.1007/s11739-021-02734-8
115. Rogers R, Shehadeh F, Mylona EK, et al. Convalescent plasma for patients with severe Coronavirus Disease 2019 (COVID-19): a matched cohort study. Clin Infect Dis. 2021;73(1):e208–e214. doi:10.1093/cid/ciaa1548
116. Shenoy AG, Hettinger AZ, Fernandez SJ, Blumenthal J, Baez V. Early mortality benefit with COVID-19 convalescent plasma: a matched control study. Br J Haematol. 2021;192(4):706–713. doi:10.1111/bjh.17272
117. Moniuszko-Malinowska A, Czupryna P, Zarębska-Michaluk D, et al. Convalescent plasma transfusion for the treatment of COVID-19—experience from Poland: a multicenter study. J Clin Med. 2020;10(1):E28. doi:10.3390/jcm10010028
118. Joyner MJ, Carter RE, Senefeld JW, et al. Convalescent plasma antibody levels and the risk of death from Covid-19. N Engl J Med. 2021;384:1015–1027. doi:10.1056/NEJMoa2031893
119. Korley FK, Durkalski-Mauldin V, Yeatts SD, et al. Early convalescent plasma for high-risk outpatients with Covid-19. N Engl J Med. 2021;385:1951–1960. doi:10.1056/NEJMoa2103784
120. Bégin P, Callum J, Jamula E, et al. Convalescent plasma for hospitalized patients with COVID-19: an open-label, randomized controlled trial. Nat Med. 2021;27:2012–2024. doi:10.1038/s41591-021-01488-2
121. Delgado-Fernández M, García-Gemar GM, Fuentes-López A, et al. Treatment of COVID-19 with convalescent plasma in patients with humoral immunodeficiency - three consecutive cases and review of the literature. Enferm Infecc Microbiol Clin. 2021;40:507–516.
122. Gupta A, Kute VB, Patel HV, et al. Feasibility of convalescent plasma therapy in kidney transplant recipients with severe COVID-19: a single-center prospective cohort study. Exp Clin Transplant. 2021;19:304–309.
123. Rodionov RN, Biener A, Spieth P, et al. Potential benefit of convalescent plasma transfusions in immunocompromised patients with COVID-19. Lancet Microbe. 2021;2(4):e138. doi:10.1016/S2666-5247(21)00030-6
124. Bennett-Guerrero E, Romeiser JL, Talbot LR, et al. Severe acute respiratory syndrome coronavirus 2 convalescent plasma versus standard plasma in coronavirus disease 2019 infected hospitalized patients in New York: a double-blind randomized trial. Crit Care Med. 2021;49(7):1015–1025. doi:10.1097/CCM.0000000000005066
125. Bainbridge ED, Hsue PY, Esensten JH, et al. Characteristics of high-titer convalescent plasma and antibody dynamics after administration in patients with severe coronavirus disease 2019. Open Forum Infect Dis. 2021;8(8):ofab385. doi:10.1093/ofid/ofab385
126. Sekine L, Arns B, Fabro BR, et al. Convalescent plasma for COVID-19 in hospitalised patients: an open-label, randomised clinical trial. Eur Respir J. 2022;59(2):2101471. doi:10.1183/13993003.01471-2021
127. Khoury E, Nevitt S, Madsen WR, Turtle L, Davies G, Palmieri C. Differences in outcomes and factors associated with mortality among patients with SARS-CoV-2 infection and cancer compared with those without cancer: a systematic review and meta-analysis. JAMA Netw Open. 2022;5(5):e2210880. doi:10.1001/jamanetworkopen.2022.10880
128. Ricke DO. Two Different Antibody-Dependent Enhancement (ADE) Risks for SARS-CoV-2 Antibodies. Front Immunol. 2021;12. doi:10.3389/fimmu.2021.640093
129. Wen J, Cheng Y, Ling R, et al. Antibody-dependent enhancement of coronavirus. Int J Infect Dis. 2020;100:483–489.
130. Körper S, Weiss M, Zickler D, et al. Results of the CAPSID randomized trial for high-dose convalescent plasma in patients with severe COVID-19. J Clin Invest. 2021;131(20):e152264. doi:10.1172/JCI152264
131. Marshall JC, Murthy S, Diaz J, et al. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect Dis. 2020;20(8):e192–e197. doi:10.1016/S1473-3099(20)30483-7
132. Fung M, Nambiar A, Pandey S, et al. Treatment of immunocompromised COVID-19 patients with convalescent plasma. Transpl Infect Dis. 2021;23:e13477.
133. Bhurayanontachai R, Siripaitoon P, Kositpantawong N, Chusri S. The success of non-ABO-identical convalescent plasma transfusion in coronavirus disease 2019 (COVID-19) related acute respiratory distress syndrome (CARDS): a case-report: convalescent plasma for COVID-19. Clin Crit Care. 2022;30:e0002–2022. doi:10.54205/ccc.v30.254752
134. Roback JD, Guarner J. Convalescent plasma to treat COVID-19: possibilities and challenges. JAMA. 2020;323(16):1561–1562. doi:10.1001/jama.2020.4940
135. Sullivan HC, Roback JD. Convalescent plasma: therapeutic hope or hopeless strategy in the SARS-CoV-2 pandemic. Transfus Med Rev. 2020;34(3):145–150. doi:10.1016/j.tmrv.2020.04.001
136. Amri N, Tessier N, Bégin R, et al. Blood endothelial-cell extracellular vesicles as potential biomarkers for the selection of plasma in COVID-19 convalescent plasma therapy. Cells. 2022;11(19):3122. doi:10.3390/cells11193122
137. Bajpai M, Maheshwari A, Kumar S, et al. Comparison of safety and efficacy of convalescent plasma with fresh frozen plasma in severe covid-19 patients. An Acad Bras Ciênc. 2022;94. doi:10.1590/0001-3765202220210202
138. Bansal N, Raturi M, Bansal Y, Singh P. A novel scoring system for selecting the target patients of COVID-19 convalescent plasma therapy: a hypothesis. Transfus Clin Biol. 2022;29:89–91. doi:10.1016/j.tracli.2021.06.004
139. Bruiners N, Guerrini V, Ukey R, et al. Biologic correlates of beneficial convalescent plasma therapy in a COVID-19 patient reveal disease resolution mechanisms. medRxiv. 2022;2022. doi:10.1101/2022.02.03.22269612
140. De Silvestro G, Marson P, La Raja M, et al. Outcome of SARS CoV-2 in patients treated with convalescent plasma: one-year of data from the Veneto region (Italy) Registry. Eur J Intern Med. 2022;97:42–49. doi:10.1016/j.ejim.2021.12.023
141. Gullo G, Cucinella G, Tumminello M, et al. Convalescent plasma use in pregnant patients with COVID19 related ARDS: a case report and literature review. Ital J Gynaecol Obstet. 2022;34:228. doi:10.36129/jog.2022.32
142. Duan L, Xie Y, Wang Q, et al. Research on antibody changes and nucleic acid clearance in COVID-19 patients treated with convalescent plasma. Am J Transl Res. 2022;14:2655–2667.
143. Emma Diletta S, Virginia P, Francesco P, et al. Convalescent plasma therapy in aHUS patient with SARS-CoV-2 infection. J Clin Nephrol. 2022;6:9. doi:10.29328/journal.jcn.1001088
144. Erol S, Tanaçan A, Apaydin H, et al. An evaluation of the results of convalescent plasma therapy applied to pregnant women diagnosed as COVID-19- positive in a pandemic center: a prospective cohort study. Turk J Med Sci. 2022;52:554–564. doi:10.55730/1300-0144.5346
145. Esteban I, Panighetti MT, Polack FP. Post-trial follow-up after a randomized clinical trial of COVID-19 convalescent plasma. Gates Open Res. 2022;6:110. doi:10.12688/gatesopenres.13725.1
146. Freise NF, Gliga S, Fischer J, et al. Convalescent plasma treatment for SARS-CoV-2 infected high-risk patients - a matched pair analysis to the LEOSS cohort. Sci Rep. 2022;12(1):19035. doi:10.1038/s41598-022-23200-1
147. Fazeli A, Sharifi S, Behdad F, et al. Early high-titer convalescent plasma therapy in patients with moderate and severe COVID-19. Transfus Apher Sci. 2022;61:103321. doi:10.1016/j.transci.2021.103321
148. Fernández-Lázaro D, Ortega CD, Sánchez-Serrano N, et al. Convalescent plasma therapy, therapeutic formulations of repurposed drugs in 20th century epidemics against COVID-19: a systematic review. Pharmaceutics. 2022;14:1020. doi:10.3390/pharmaceutics14051020
149. Fernández-Sánchez V, Ventura-Enríquez Y, Cabello-Gutiérrez C, et al. Convalescent plasma to treat Covid-19: a randomized double blind 2 centers trial. Review. 2022. doi:10.21203/rs.3.rs-1277990/v1
150. Fodor E, Müller V, Iványi Z, et al. Early transfusion of convalescent plasma improves the clinical outcome in severe SARS-CoV2 infection. Infect Dis Ther. 2022;11:293–304. doi:10.1007/s40121-021-00514-7
151. Franchini M, Glingani C, Donno GD, et al. Convalescent plasma for hospitalized COVID-19 patients: a single-center experience. Life. 2022;12:420. doi:10.3390/life12030420
152. Franchini M, Focosi D, Percivalle E, et al. Variant of concern-matched COVID-19 convalescent plasma usage in seronegative hospitalized patients. Viruses. 2022;14(7):1443. doi:10.3390/v14071443
153. Gharbharan A, GeurtsvanKessel CH, Jordans CCE, et al. Effects of treatment of Coronavirus Disease 2019 with convalescent plasma in 25 B-cell–depleted patients. Clin Infect Dis. 2022;74:1271–1274. doi:10.1093/cid/ciab647
154. Jain R, Mallya MV, Amoncar S, et al. Seroprevalence of SARS-CoV-2 among potential convalescent plasma donors and analysis of their deferral pattern: experience from tertiary care hospital in western India. Transfus Clin Biol. 2022;29:60–64. doi:10.1016/j.tracli.2021.07.004
155. Kutsuna S, Saito S, Takamatsu Y, et al. Safety of convalescent plasma therapy for COVID-19 patients and analysis of viral kinetics: a single-center, open-label, single-arm, interventional study in Japan. GHM Open. 2022;2(1):38–43.
156. Kurnianda J, Hardianti MS, Triyono T, et al. Efficacy and safety of convalescent plasma therapy in patients with moderate-to-severe COVID-19: a non-randomized comparative study with historical control in a referral hospital in Indonesia. J Infect Public Health. 2022;15:100–108. doi:10.1016/j.jiph.2021.10.028
157. Leon J, Merrill AE, Rogers K, et al. SARS-CoV-2 antibody changes in patients receiving COVID-19 convalescent plasma from normal and vaccinated donors. Transfus Apher Sci. 2022;61:103326. doi:10.1016/j.transci.2021.103326
158. Magyari F, Pinczés LI, Páyer E, et al. Early administration of remdesivir plus convalescent plasma therapy is effective to treat COVID-19 pneumonia in B-cell depleted patients with hematological malignancies. Ann Hematol. 2022;101(10):2337–2345. doi:10.1007/s00277-022-04924-6
159. Marconato M, Abela IA, Hauser A, et al. Antibodies from convalescent plasma promote SARS-CoV-2 clearance in individuals with and without endogenous antibody response. J Clin Invest. 2022;132(12). doi:10.1172/JCI158190
160. Mastroianni A, Greco S, Chidichimo L, et al. Challenges associated with convalescent plasma infusion therapy during pregnancy, a case report. Womens Health Bull. 2022;9:118–121.
161. Mesina F, Julian J, Relos J, et al. Use of convalescent plasma therapy with Best Available Treatment (BAT) among hospitalized COVID-19 patients: a multi-center study. medRxiv. 2022;2022:2022.
162. Nyström K, Hjorth M, Fust R, et al. Specific T-cell responses for guiding treatment with convalescent plasma in severe COVID-19 and humoral immunodeficiency: a case report. BMC Infect Dis. 2022;22(1):362. doi:10.1186/s12879-022-07323-4
163. Novacescu AN, Duma G, Buzzi B, et al. Therapeutic plasma exchange followed by convalescent plasma transfusion in severe and critically ill COVID‑19 patients: a single centre non‑randomized controlled trial. Exp Ther Med. 2022;23:1–8. doi:10.3892/etm.2021.10923
164. Novacescu AN, Duma G, Sandesc D, Sorescu T, Licker M. The successful recovery of a critically ill COVID-19 patient, following the combination of therapeutic plasma exchange and convalescent plasma transfusion: a case report. Medicina. 2022;58:1088. doi:10.3390/medicina58081088
165. Noor ES, Semedi BP, Kusuma E. The effect of convalescent plasma administration on increasing blood IGG and IGM levels as an effort to prevent death due to Covid-19 in ICU Panglima Sebaya hospital, Paser Regency, East Kalimantan. J Adv Health Med Sci. 2022;8. doi:10.20474/jahms-8.1
166. Ostrovskaya EA, Kostin AI, Bulanov A. Efficiency and safety of convalescent plasma therapy in patients with COVID-19: a systematic review. Ann Crit Care. 2022;2:108–120.
167. Ortigoza MB, Yoon H, Goldfeld KS, et al. Efficacy and safety of COVID-19 Convalescent plasma in hospitalized patients: a randomized clinical trial. JAMA Intern Med. 2022;182:115–126. doi:10.1001/jamainternmed.2021.6850
168. Pan C, Chen H, Xie J, et al. The efficiency of convalescent plasma therapy in the management of critically ill patients infected with COVID-19: a matched cohort study. Front Med. 2022;9:822821. doi:10.3389/fmed.2022.822821
169. Pratama A, Djaharuddin I. Effectiveness and efficacy of convalescent plasma therapy in Covid-19 patients. In: C62. Expanding Our Insight into Covid-19. American Thoracic Society; 2022:A4568–A4568.
170. Qin J, Wang G, Han D. Benefits of plasma exchange on mortality in patients with COVID-19: a systematic review and meta-analysis. Int J Infect Dis. 2022;122:332–336. doi:10.1016/j.ijid.2022.06.014
171. Soleimani Z, Soleimani A. ADRS due to COVID-19 in midterm pregnancy: successful management with plasma transfusion and corticosteroids. J Matern Fetal Neonatal Med. 2022;35:3040–3043. doi:10.1080/14767058.2020.1797669
172. Sanz C, Nomdedeu M, Pereira A, et al. Efficacy of early transfusion of convalescent plasma with high-titer SARS-CoV-2 neutralizing antibodies in hospitalized patients with COVID-19. Transfusion. 2022;62:974–981. doi:10.1111/trf.16863
173. Shibeeb S. Effectiveness of convalescent plasma therapy in COVID-19 patients with haematological malignancies (preprint); 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.