Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Effectiveness of Brodalumab in Patients with Moderate-to-Severe Plaque Psoriasis Located in Difficult-to-Treat Areas
Authors Cacciapuoti S, Potestio L ![]() , Guerrasio G, Fabbrocini G, Scalvenzi M, Ruggiero A
, Guerrasio G, Fabbrocini G, Scalvenzi M, Ruggiero A ![]() , Caiazzo G, Megna M
, Caiazzo G, Megna M ![]()
Received 20 June 2023
Accepted for publication 20 September 2023
Published 25 September 2023 Volume 2023:16 Pages 2637—2644
DOI https://doi.org/10.2147/CCID.S423234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sara Cacciapuoti,* Luca Potestio,* Gianluca Guerrasio, Gabriella Fabbrocini ,† Massimiliano Scalvenzi, Angelo Ruggiero,* Giuseppina Caiazzo,* Matteo Megna*
Section of Dermatology - Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy
*These authors contributed equally to this work
†Professor Gabriella Fabbrocini passed away on 3rd March 2023
Correspondence: Angelo Ruggiero, Section of Dermatology - Department of Clinical Medicine and Surgery, University of Naples Federico II, Via Pansini 5, Napoli, 80131, Italy, Tel +39 - 081 – 7462457, Fax +39 - 081 – 7462442, Email [email protected]
Background: Recent knowledge of psoriasis pathogenesis has led to the development of selective drugs. Among these, brodalumab is a monoclonal antibody targeting the interleukin (IL)-17A receptor approved for the treatment of moderate-to-severe plaque psoriasis. Biologics may be considered in patients with milder diseases in case of active psoriatic arthritis, severe impact on patient’s quality of life, and involvement of sensitive and difficult-to-treat areas. These skin locations commonly require systemic drugs. Recently, psoriasis severity monitoring has also changed. Indeed, the clinical evaluation by means of specific efficacy scores was combined with serological evaluation by means of the assay of specific inflammatory biomarkers.
Methods: An observational study enrolled patients affected by moderate-to-severe plaque psoriasis involving difficult-to-treat areas, undergoing treatment with brodalumab to evaluate the effectiveness and safety of brodalumab in patients with psoriasis affecting difficult-to-treat areas (scalp and palmoplantar regions). Secondary outcomes were the assessment of the development of serum markers of inflammation during the treatment period as well as the evaluation of the dermoscopic features of the affected sites to quantify disease activity and response to treatment.
Results: Twenty-five patients were included in the study. A statistically significant reduction from baseline in PASI, PSSI, ppPASI and DLQI values as early as week 24 was observed, with further improvement up to week 52. Plasma levels of MMP-3, VEGF-A, and hs-PCR decreased during treatment from week 0 to week 52.
Conclusion: Our real-life experience suggests brodalumab as a valuable option for the management of psoriasis located in difficult-to-treat areas. Moreover, our study highlights that the use of brodalumab reduces the plasmatic levels of inflammatory biomarkers (MMP-3, VEGF-A and hs-PCR), showing how the drug modulates the skin inflammatory response by reducing systemic inflammation.
Keywords: brodalumab, psoriasis, difficult-to-treat areas, biologic drugs, efficacy
Introduction
Psoriasis is a chronic inflammatory skin disease, affecting up to 2–3% of the worldwide population.1 Despite several clinical phenotypes may be distinguished, plaque psoriasis is the most common, accounting for 90% of cases and presenting as sharply demarcated erythematous plaques covered by silvery-white lamellar scales.2,3 Psoriasis management is challenging, particularly for moderate-to-severe forms of the disease.4 Moreover, several comorbidities (e.g psoriatic arthritis, inflammatory bowel disease, cardiovascular diseases, obesity, psychological and psychiatric disorders, uveitis, etc.) may be associated with psoriatic disease, necessitating early treatment to prevent systemic complications.5,6 Recently, the introduction of biologics revolutionized the treatment scenario.7,8 Indeed, recent knowledge on psoriasis pathogenesis has led to the development of selective biologic drugs, interfering with the action of cytokines such as Tumor Necrosis Factor (TNF) α, interleukin (IL)-23 and IL-17 by inhibiting the activation of the inflammatory cascade at various levels.9 In particular, IL-17 is a family of cytokines that consists of 6 homodimers from IL-17-A to IL-17-F and an IL-17-AF heterodimer.10,11 IL-17-A plays a crucial role in the pathogenesis of psoriasis and is the selective target of drugs such as ixekizumab and secukinumab.10,11 Moreover, IL-17-F has been shown to contribute to psoriatic inflammation by becoming the target of the joint blockade together with IL17A by bimekizumab.10–12 However, other isoforms such as IL-17-E and IL- 17-C also seem to play an important role in certain components of psoriatic symptoms such as itching.10,11 Of note, the A-type receptor for IL-17 acts as a common coreceptor for all IL-17 isoforms. Thus, the selective blockade of the receptor rather than the cytokine allows the advantages of simultaneous inhibition of all the IL-17 isoforms.10,11
In this scenario, brodalumab, a human monoclonal antibody targeting the IL-17A receptor, received both EMA and US FDA approval for the treatment of adult patients suffering from moderate-to-severe plaque psoriasis.13 The efficacy and safety profiles of brodalumab have been evaluated in three randomized, double-blind, Phase 3, placebo-controlled clinical trials (AMAGINE-1,-2, and −3), which showed its superiority to both placebo and ustekinumab.14–16 Moreover, these promising results have been confirmed by real-life studies.17–19
Current guidelines suggest the use of biologic drugs for moderate-to-severe psoriasis defined by Psoriasis Area and Severity Index (PASI) and/or body surface area (BSA) ≥10.20,21 However, biologics may be considered in patients with milder diseases in case of active psoriatic arthritis, severe impact on patient’s quality of life [Dermatology Life Quality Index (DLQI)>10], and involvement of sensitive and difficult-to-treat areas, such as face, scalp, palms, soles, nails, and genitalia.20,21 These skin locations commonly require systemic drugs as well as they are more resistant to conventional topical and systemic treatments, strongly affecting on patients’ quality of life.22 Thus, the treatment goal should be the use of the right drug for the right patient at the right moment.23
Moreover, psoriasis severity monitoring has also changed. Indeed, the clinical evaluation by means of specific efficacy scores was combined with serological evaluation by means of the assay of specific inflammatory biomarkers, ie metalloproteinase-3 (MMP3), vascular endothelial growth factor (VEGF), and high-sensitivity C-reactive protein (hs-CRP), the increase of which is an indirect sign of the active inflammatory state in psoriatic patients.24 Finally, the use of dermoscopy may help to quantify disease activity and response to treatment.25,26
The aim of our study was to evaluate the effectiveness and safety of brodalumab in patients with psoriasis affecting difficult-to-treat areas (scalp and palmoplantar regions). Secondary outcomes were the assessment of the development of serum markers of inflammation during the treatment period as well as the evaluation of the dermoscopic features of the affected sites to quantify disease activity and response to treatment.
Materials and Methods
A monocentric observational study was performed enrolling patients affected by moderate-to-severe plaque psoriasis, particularly in difficult-to-treat area (scalp and palmoplantar region), undergoing treatment with brodalumab and attending the Psoriasis Care Centre between 2020 and 2022. Inclusion criteria were i) diagnosis of moderate-to-severe plaque psoriasis assessed by a dermatologist for at least 6 months; ii) failure, contraindication or intolerance to 1 or more systemic therapies; iii) presence severe plaque psoriasis (PASI > 10 and/or BSA > 10) with localization on the scalp [Psoriasis Scalp Severity Index (PSSI)>8] or palmoplantar region [palmoplantar Psoriasis Activity Severity Index (ppPASI)>8]; iv) eligibility for treatment with brodalumab according to regional guidelines in the absence of contraindications to the administration of the drug. Exclusion criteria were i) Chron’s diseases; ii) clinically important active infections; iii) pregnancy; iv) breastfeeding or women of childbearing age who are unwilling to use appropriate contraceptive methods; iv) medical problems that in the investigator’s opinion would put the patient; v) history of allergy to any component of brodalumab.
Brodalumab was administered at labelled dosage [(210 mg administered by subcutaneous injection at weeks 0, 1 and 2, followed by 210 mg every 2 weeks (Q2W)]. The follow-up period of brodalumab treatment was 52 weeks. Patients already on biologic therapy underwent an adequate wash-out period on their current drug before starting brodalumab therapy.
Demographic (age, sex) and clinical features [psoriasis severity through PASI, BSA, PSSI and ppPASI, DLQI, comorbidities, previous and current psoriasis treatment] were collected for each patient at baseline.
Furthermore, psoriasis severity (PASI, BSA, PSSI, ppPASI and DLQI) was evaluated at each follow-up visit (week 2, week 4, week 12, week 24 and week 52) as well as adverse events (AEs) were monitored at the same timepoints.
Blood samples to assess circulating levels of MMP3, hsPCR and VEGF-A in order to evaluate these inflammatory biomarkers in psoriasis patients were collected at weeks 0, 12 and 52. In particular, blood samples (5 mL each) were collected from all patients using EDTA tubes (BD Vacutainer®) at week 0 and weeks 12 and 52. Plasma was separated from the samples by centrifugation at 3000 rpm for 10 minutes, aliquoted and immediately stored at −80°C before further analysis. Plasma levels of markers were detected by Ella Automated Immunoassay System using a cat#SPCKC-PS-000304 kit for VEGF-A and a cat#SPCKC-PS-000200 kit for hsPCR.
At the same timepoints (week 0.12 and 52), dermoscopic images at scalp and palmoplantar level were acquired with the DermLite Foto II Pro-Canon 11 digital camera to assess clinical improvement. The dermoscopic criteria considered including erythema and desquamation. The present study was conducted respecting the Declaration of Helsinki and all patients signed an informed consent before starting the study.
Statistical Analysis
Clinical and demographic data were evaluated through descriptive statistics. Continuous variables were presented as mean ± standard deviation, while number and proportion of patients were used for categorical ones. Statistical analysis using GraphPad Prism 5.0 (GraphPad Software Inc., La Jolla, CA, USA) was performed to assess the statistically significance of clinical response. Two-Way ANOVA test and the paired t-Test were used to evaluate the statistical significance of the differences in values obtained at the different time points of therapy for psoriasis severity scores and the inflammatory biomarkers, respectively. P values <0.05 were considered to be statistically significant.
Results
Twenty-five patients treated with brodalumab (15 males, 60.0%; mean age 46.6 ± 12.5 years) respected the inclusion criteria and completed the follow-up period. As regards previous treatments, 12 (48.0%) patients received only topical corticosteroid and vitamin D therapies and had contraindications to the use of conventional systemic drugs, 9 (36.0%) subjects previously received topical and systemic therapies (methotrexate and cyclosporine) and 4 (16.0%) were previously treated with biological drugs, such as adalimumab (1, 4.0%), ixekizumab (1, 4.0%) and ustekinumab (2, 8.0%), with poor symptom control. Baseline clinical evaluation showed a mean PASI of 20.86 ± 6.9, mean PSSI of 24.15 ± 16, mean ppPASI of 20.33 ± 2.12 and a mean DLQI of 19.71 ± 6.85.
A statistically significant reduction from baseline in PASI, PSSI, ppPASI and DLQI values as early as week 24 was observed, with further improvement up to week 52 (Figure 1).
 |
Figure 1 Scalp psoriasis in patient 3 at baseline (a–c) and after 12 weeks of treatment (d–f). |
At week 24 and week 52 the mean PASI values were 3.92 ± 4.09 and 2.08 ± 3.41, respectively, compared to a baseline value of 20.8 ± 6.9. Similarly, the mean PSSI values were 23.6 ± 15.56 (at week 2), 15.70 ± 14.47 (at week 4) 4.29 ± 7.64 (at week 24) and 2.46 ± 4.89 (at week 52) as well as at week 24 and week 52 the mean ppPASI values were 1.42 ± 2.94 and 1.25 ± 2.80, respectively, compared to a baseline value of 20.33 ± 2.12. Figure 2 shows how the DLQI decreased over time compared with PASI (Figure 2a), PSSI (Figure 2b) and ppPASI (Figure 2c).
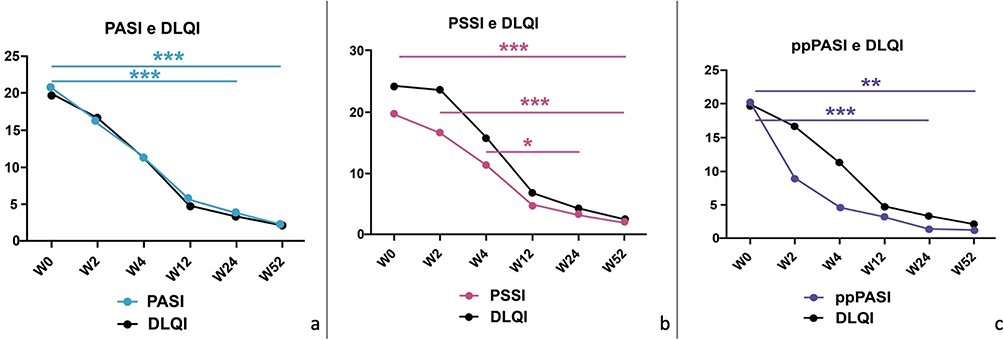 |
Figure 2 PASI (a), PSSI (b) and ppPASI (c) values and relative DLQI trends in patients at baseline (W0) and after 2, 4, 12, 24 and 52 (W2, W4, W12, w24 and w52) weeks of brodalumab treatment. Statistical significance was assessed with the two-way ANOVA test. ***p < 0.001; **p < 0.05; *p < 0.1. |
As regards the safety, 5 (20.0%) patients reported at least one AE (pharyngitis: 2, 40.0%; flu-like illness, 2, 40.0%; headache: 1, 20.0%). Of note, all the AEs were mild, not requiring treatment discontinuation.
The study of plasma levels of MMP-3, VEGF-A and hs-PCR was used to assess the inflammatory status of patients during treatment (Figure 3). In line with the literature data, the biological markers decreased during the course of therapy from week 0 to week 52. The results show a downward trend in protein levels already evident after 12 weeks of treatment, with a further reduction at week 52. In particular, MMP3 and VEGF are significantly (**p < 0.01) reduced after 52 weeks of treatment while in the case of hs-PCR, a reduction trend already evident after 12 weeks is further confirmed at measurements at week 52, although not in a statistically significant manner.
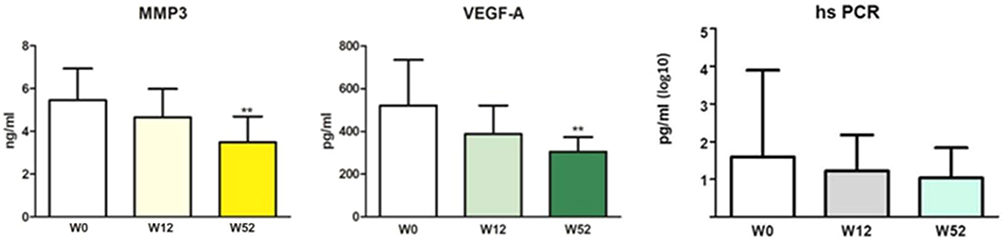 |
Figure 3 Plasma levels of MMP-3, VEGF-A and hs-PCR at baseline (W0), after 12 (W12) and after 52 (W52) weeks of brodalumab treatment. The results show a downward trend in protein levels already evident after 12 weeks of treatment, with a further reduction at week 52. Statistical significance was assessed with the paired t-Test. **p < 0.01. |
Finally, before the start of brodalumab therapy, all patients underwent dermoscopic investigation: in 11 patients (44%) this investigation was performed at the scalp, in 7 at the palmoplantar surface (28%) and in 7 at both sites (28%). Dermoscopic evaluation revealed a punctuated vascular pattern over the entire area examined in most lesions and the presence of superficial scales in all lesions. After 52 weeks of treatment, dermoscopic analysis showed regression of the vascular component and disappearance of desquamation.
Discussion
Psoriasis management is challenging,27 particularly for difficult-to-treat areas. Indeed, the involvement of these regions (nails, palmoplantar, scalp and genitalia) is often associated with a significant negative impact on patients’ quality of life, and a consensus on the best treatment options is still limited, leading to unmet needs for safe and efficacious therapies.28,29 Moreover, poor accessibility to lesions, therapy resistance, sensitivity to strong topicals, and reduced treatment-adherence further complicate the therapeutic landscape.30,31 The introduction of biologic drugs revolutionized treatment scenario, showing promising data in terms of efficacy and safety.32–36 Among these, brodalumab, a human IL-17 receptor A antagonist, seems to be a valuable option.37 Our 52-week prospective study enrolling 25 patients affected by psoriasis located in difficult-to-treat areas (palmoplantar and scalp) treated with brodalumab showed a statistically significant reduction from baseline in PASI, PSSI, ppPASI and DLQI values as early as week 24, with further improvement up to week 52. Clinical results have been confirmed by laboratory parameters and dermoscopic assessment. Even if limited, our study seems to confirm data from current literature.
As regards scalp psoriasis, in a post hoc analysis of the phase 3 AMAGINE- 1 study, 177 patients with scalp psoriasis (PSSI ≥ 15) were randomized to receive brodalumab 210mg Q2W (n = 82) or placebo (n = 95). At week 12, PSSI75 and PSSI100 were reached by 89.0% and 63.4% of patients in brodalumab cohort and 9.5% and 3.2% of subjects receiving placebo, respectively.38 In a sub-analysis of a Phase 2 Japanese trial, the effectiveness of brodalumab in moderate-to-severe scalp psoriasis management has been evaluated in 75 receiving brodalumab 210mg Q2W (n = 37, mean PSSI at baseline: 24.3 ± 15.7) or placebo (n = 38, mean PSSI at baseline 26.2 ± 15.5).39 After 12 weeks of treatment, a statistically significant reduction of PSSI was reported in patients received brodalumab (94.5% ± 14.8%) compared with placebo (12.6% ± 63.0%), respectively (p < 0.001).39
As regards palmoplantar psoriasis, Politou et al reported the results of a case series on 4 patients receiving brodalumab after failing treatment with secukinumab, showing that all patients (4/4) with palmoplantar pustulosis achieved PASI100 at week 16.38
The unique mechanism of action of brodalumab, the faster onset of response compared with other biologics, its effectiveness and safety make this drug a valuable option in psoriasis management, also in patients with inadequate response to other biologics and with the involvement of difficult-to-treat area.39 To the best of our knowledge, our study is the first investigating the efficacy of brodalumab in palmoplantar and scalp psoriasis in a real-world setting.
Moreover, our study is the first evaluating the clinical response of brodalumab using dermoscopic examination as well as the clinical correlation between clinical improvement and reduction in inflammatory biomarkers. Indeed, recent knowledge in psoriasis pathogenesis, showing the presence of protein in the pathological cellular environment of both skin lesions and serum of affected patients, opened a new era in psoriasis management.40 Several serum biomarkers are currently under investigation for their potential role in the anticipation of psoriasis diagnosis and treatment.40 In our study, we investigated three biomarkers: VEGF, MMP3 and hs-CRP, usually increased in psoriasis patients. In particular, hs-CRP is an acute-phase protein, recognized as one of the most sensitive markers of inflammation as well as an independent risk factor for cardiovascular disease. Recent studies showed that hs-CRP can work interchangeably with PASI as a measure of disease severity in the case of untreated patients with moderate-to-severe forms of the disease.41 Similarly, VEGF is a key angiogenic factor in psoriasis pathogenesis, increased both in the skin and in the plasma of affected patients and these levels correlate with disease activity and treatment response.42 All these biomarkers decreased during brodalumab treatment. This reduction became evident at week 12, with a statistically significance for MMP3 and VEGF (**p < 0.01) after 52 weeks of treatment.
As regards dermoscopy, it is a noninvasive tool which allows to increase the accuracy of the diagnosis of psoriasis.43 Generally, dermoscopic examination of plaque psoriasis shows a distinctive pattern characterized by diffuse white scales and regularly and symmetrically distributed dotted vessels on a light or dull red background.44,45 In our study, we reported that dermoscopic examination may be used not only during the diagnosis but also for assessing the severity of the disease. Indeed, a significant reduction of the vascular pattern as well as the disappearance of desquamation during treatment with brodalumab was shown.
To sum up, the management of psoriasis located at difficult-to-treat areas is challenging. Our study investigated the use of brodalumab in the management of palmoplantar or scalp psoriasis, with the secondary aim of assessing the level of serum markers of inflammation during the treatment period as well as the utility of dermoscopic examination to quantify disease activity and response to treatment. Despite limited, our results suggest that brodalumab may be an effective option for palmoplantar or scalp psoriasis, even in patients showing inadequate response to other biologic drugs. Our data showed dermoscopy as a useful tool in the assessment of psoriasis severity and response to treatment. Finally, data derived from the evaluation of inflammatory biomarkers during treatment suggested that brodalumab acts not only on psoriatic disease but it seems to reduce the patient’s overall inflammatory state. Certainly, further studies are needed to confirm our results.
Strengths and Limitations
The prospective design and the statistical significance of our results are the main strengths of our study. The size of our cohort as well as the lack of a comparison with other anti-IL17 are the main limitations, reducing the generalizability of our results.
Conclusions
Our real-life experience suggests brodalumab as a valuable option for the management of psoriasis located in difficult-to-treat areas. Clinical results were confirmed by a dermoscopic examination which showed to be a useful tool in assisting the evaluation of treatment response, allowing skin inflammation to be assessed at a higher magnification than is possible with the naked eye. Moreover, our study highlights that the use of brodalumab reduces the plasmatic levels of inflammatory biomarkers (MMP-3, VEGF-A and hs-PCR), showing how the drug modulates the skin inflammatory response by reducing systemic inflammation. Further studies with a larger sample size are required to confirm our data, as well as to improve the decision-making process in choosing the best treatment option for each patient.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Ethical Approval
Local Ethic Committee University of Naples Federico II, 408/19.
Patient Consent
Informed consent was obtained from all subjects involved in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Langley RGB, Krueger GG, Griffiths CEM. Psoriasis: epidemiology, clinical features, and quality of life. Ann Rheum Dis. 2005;64(Suppl 2):ii18–23. doi:10.1136/ard.2004.033217
2. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960. doi:10.1001/jama.2020.4006
3. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–271. doi:10.1016/S0140-6736(07)61128-3
4. Korman NJ. Management of psoriasis as a systemic disease: what is the evidence? Br J Dermatol. 2020;182(4):840–848. doi:10.1111/bjd.18245
5. Oliveira MD, Rocha BD, Duarte GV. Psoriasis: classical and emerging comorbidities. An Bras Dermatol. 2015;90(1):9–20. doi:10.1590/abd1806-4841.20153038
6. Megna M, Ocampo-Garza SS, Potestio L, et al. New-onset psoriatic arthritis under biologics in psoriasis patients: an increasing challenge? Biomedicines. 2021;9(10):1482. doi:10.3390/biomedicines9101482
7. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part II: focus on elderly patients. Expert Opin Drug Saf. 2023:1–16. doi:10.1080/14740338.2023.2173171
8. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: focus on pediatric patients. Expert Opin Drug Saf. 2023:1–17. doi:10.1080/14740338.2023.2173170
9. Tokuyama M, Mabuchi T. New treatment addressing the pathogenesis of psoriasis. Int J Mol Sci. 2020;21(20):7488. doi:10.3390/ijms21207488
10. Blauvelt A, Chiricozzi A. The immunologic role of IL-17 in psoriasis and psoriatic arthritis pathogenesis. Clin Rev Allergy Immunol. 2018;55(3):379–390. doi:10.1007/s12016-018-8702-3
11. Furue K, Ito T, Tsuji G, Kadono T, Furue M. Psoriasis and the TNF/IL23/IL17 axis. G Ital Dermatol Venereol Organo Uff Soc Ital di dermatologia e Sifilogr. 2019;154(4):418–424. doi:10.23736/S0392-0488.18.06202-8
12. Ruggiero A, Potestio L, Martora F, Villani A, Comune R, Megna M. Bimekizumab treatment in patients with moderate to severe plaque psoriasis: a drug safety evaluation. Expert Opin Drug Saf. 2023;22:355–362. doi:10.1080/14740338.2023.2218086
13. Iznardo H, Puig L. The safety of brodalumab for the treatment of psoriasis. Expert Opin Drug Saf. 2020;19(4):365–372. doi:10.1080/14740338.2020.1730326
14. Reich K, Iversen L, Puig L, et al. Long-term efficacy and safety of brodalumab in moderate-to-severe plaque psoriasis: a post hoc pooled analysis of AMAGINE-2 and −3. J Eur Acad Dermatol Venereol. 2022;36(8):1275–1283. doi:10.1111/jdv.18068
15. Farahnik B, Beroukhim K, Abrouk M, et al. Brodalumab for the treatment of psoriasis: a review of phase III trials. Dermatol Ther. 2016;6(2):111–124. doi:10.1007/s13555-016-0121-x
16. Lebwohl M, Strober B, Menter A, et al. Phase 3 studies comparing brodalumab with ustekinumab in psoriasis. N Engl J Med. 2015;373(14):1318–1328. doi:10.1056/NEJMoa1503824
17. Mastorino L, Cariti C, Susca S, et al. Brodalumab efficacy in bio-naïve psoriasis patients: real-life experience of 202 subjects up to 48 weeks. J Dermatolog Treat. 2022;33(8):3211–3213. doi:10.1080/09546634.2022.2125265
18. Galluzzo M, Caldarola G, De Simone C, et al. Use of brodalumab for the treatment of chronic plaque psoriasis: a one-year real-life study in the Lazio region, Italy. Expert Opin Biol Ther. 2021;21(9):1299–1310. doi:10.1080/14712598.2021.1941862
19. Megna M, Potestio L, Camela E, Fabbrocini G, Ruggiero A. Ixekizumab and brodalumab indirect comparison in the treatment of moderate to severe psoriasis: results from an Italian single-center retrospective study in a real-life setting. Dermatol Ther. 2022;35:e15667. doi:10.1111/dth.15667
20. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–2498. doi:10.1111/jdv.16915
21. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol. 2021;35(2):281–317. doi:10.1111/jdv.16926
22. Nicolescu AC, Ionescu MA, Constantin MM, et al. Psoriasis management challenges regarding difficult-to-treat areas: therapeutic decision and effectiveness. Life. 2022;12(12):2050. doi:10.3390/life12122050
23. Camela E, Potestio L, Fabbrocini G, Ruggiero A, Megna M. New frontiers in personalized medicine in psoriasis. Expert Opin Biol Ther. 2022;1–3. doi:10.1080/14712598.2022.2113872
24. Pourani MR, Abdollahimajd F, Zargari O, Shahidi Dadras M. Soluble biomarkers for diagnosis, monitoring, and therapeutic response assessment in psoriasis. J Dermatolog Treat. 2022;33(4):1967–1974. doi:10.1080/09546634.2021.1966357
25. Cacciapuoti S, Ruggiero A, Gallo L, Fabbrocini G. Proactive vs. reactive psoriasis therapy: a long-term evaluation with dermoscopic and confocal microscopy assessment. Eur Rev Med Pharmacol Sci. 2022;26(6):2018–2024. doi:10.26355/eurrev_202203_28350
26. Golińska J, Sar-Pomian M, Rudnicka L. Dermoscopy of plaque psoriasis differs with plaque location, its duration, and patient’s sex. Ski Res Technol off J Int Soc Bioeng Ski. 2021;27(2):217–226. doi:10.1111/srt.12933
27. Megna M, Potestio L, Fabbrocini G, Camela E. Treating psoriasis in the elderly: biologics and small molecules. Expert Opin Biol Ther. 2022;1–18. doi:10.1080/14712598.2022.2089020
28. Kivelevitch D, Frieder J, Watson I, Paek SY, Menter MA. Pharmacotherapeutic approaches for treating psoriasis in difficult-to-treat areas. Expert Opin Pharmacother. 2018;19(6):561–575. doi:10.1080/14656566.2018.1448788
29. Callis Duffin K, Mason MA, Gordon K, et al. Characterization of patients with psoriasis in challenging-to-treat body areas in the corrona psoriasis registry. Dermatology. 2021;237(1):46–55. doi:10.1159/000504841
30. Merola JF, Qureshi A, Husni ME. Underdiagnosed and undertreated psoriasis: nuances of treating psoriasis affecting the scalp, face, intertriginous areas, genitals, hands, feet, and nails. Dermatol Ther. 2018;31(3):e12589. doi:10.1111/dth.12589
31. Hjuler KF, Iversen L, Rasmussen MK, Kofoed K, Skov L, Zachariae C. Localization of treatment-resistant areas in patients with psoriasis on biologics. Br J Dermatol. 2019;181(2):332–337. doi:10.1111/bjd.17689
32. Kamata M, Tada Y. Efficacy and safety of biologics for psoriasis and psoriatic arthritis and their impact on comorbidities: a literature review. Int J Mol Sci. 2020;21(5):1–12. doi:10.3390/ijms21051690
33. Ruggiero A, Potestio L, Cacciapuoti S, et al. Tildrakizumab for the treatment of moderate to severe psoriasis: results from a single center preliminary real-life study. Dermatol Ther. 2022;35(12):e15941. doi:10.1111/dth.15941
34. Megna M, Ruggiero A, Battista T, Marano L, Cacciapuoti S, Potestio L. Long-term efficacy and safety of risankizumab for moderate to severe psoriasis: a 2-year real-life retrospective study. J Clin Med. 2023;12(9):3233. doi:10.3390/jcm12093233
35. Ruggiero A, Camela E, Potestio L, Fabbrocini G, Megna M. Drug safety evaluation of tildrakizumab for psoriasis: a review of the current knowledge. Expert Opin Drug Saf. 2022;21(12):1445–1451. doi:10.1080/14740338.2022.2160447
36. Megna M, Potestio L, Fabbrocini G, Cinelli E. Tildrakizumab: a new therapeutic option for erythrodermic psoriasis? Dermatol Ther. 2021;34:e15030. doi:10.1111/dth.15030
37. Menter A, Bhutani T, Ehst B, Elewski B, Jacobson A. Narrative review of the emerging therapeutic role of brodalumab in difficult-to-treat psoriasis. Dermatol Ther. 2022;12(6):1289–1302. doi:10.1007/s13555-022-00746-6
38. Elewski B, Rich P, Lain E, Soung J, Lewitt GM, Jacobson A. Efficacy of brodalumab in the treatment of scalp and nail psoriasis: results from three phase 3 trials. J Dermatolog Treat. 2022;33(1):261–265. doi:10.1080/09546634.2020.1749546
39. Nakagawa H, Niiro H, Ootaki K. Brodalumab, a human anti-interleukin-17-receptor antibody in the treatment of Japanese patients with moderate-to-severe plaque psoriasis: efficacy and safety results from a Phase II randomized controlled study. J Dermatol Sci. 2016;81(1):44–52. doi:10.1016/j.jdermsci.2015.10.009
40. Yadav K, Singh D, Singh MR. Protein biomarker for psoriasis: a systematic review on their role in the pathomechanism, diagnosis, potential targets and treatment of psoriasis. Int J Biol Macromol. 2018;118(Pt B):1796–1810. doi:10.1016/j.ijbiomac.2018.07.021
41. Beygi S, Lajevardi V, Abedini R. C-reactive protein in psoriasis: a review of the literature. J Eur Acad Dermatol Venereol. 2014;28(6):700–711. doi:10.1111/jdv.12257
42. Malecic N, Young HS. Novel investigational vascular endothelial growth factor (VEGF) receptor antagonists for psoriasis. Expert Opin Investig Drugs. 2016;25(4):455–462. doi:10.1517/13543784.2016.1153064
43. Wang ZY, Fei WM, Li CX, Cui Y. Comparison of dermoscopy and reflectance confocal microscopy accuracy for the diagnosis of psoriasis and lichen planus. Ski Res Technol off J Int Soc Bioeng Ski. 2022;28(3):480–486. doi:10.1111/srt.13158
44. Errichetti E, Stinco G. Dermoscopy in general dermatology: a practical overview. Dermatol Ther. 2016;6(4):471–507. doi:10.1007/s13555-016-0141-6
45. Lallas A, Kyrgidis A, Tzellos TG, et al. Accuracy of dermoscopic criteria for the diagnosis of psoriasis, dermatitis, lichen planus and pityriasis rosea. Br J Dermatol. 2012;166(6):1198–1205. doi:10.1111/j.1365-2133.2012.10868.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.