Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Effectiveness of BHATIN (Behavior-Tailored Intervention) for Self-Care Management and Clinical Biomarkers Among Patients with Hypertension: A Quasi Experimental Study
Authors Usman AM ![]() , Kosasih CE
, Kosasih CE ![]() , Pramukti I
, Pramukti I ![]() , Sofiatin Y
, Sofiatin Y ![]() , Pamungkas RA
, Pamungkas RA ![]()
Received 22 January 2026
Accepted for publication 13 March 2026
Published 25 March 2026 Volume 2026:19 598078
DOI https://doi.org/10.2147/JMDH.S598078
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Andi Mayasari Usman,1,2 Cecep Eli Kosasih,3 Iqbal Pramukti,3 Yulia Sofiatin,4 Rian Adi Pamungkas5
1Department of Medicine, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Nursing, Faculty of Health Sciences, Universitas Nasional, Jakarta, South Jakarta, Indonesia; 3Department of Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 4Department of Epidemiology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 5Department of Nursing, Faculty of Health Sciences, Universitas Esa Unggul, Jakarta, West Jakarta, Indonesia
Correspondence: Cecep Eli Kosasih, Email [email protected]
Background: Sustained self-care is essential for effective hypertension management, particularly dietary salt reduction. In many community-based settings, including primary care areas in Indonesia, hypertension control remains suboptimal due to inadequate self-care practices and persistent high salt consumption, contributing to unfavorable biomarkers such as elevated blood pressure, BMI, and metabolic indicators.
Objective: This study aimed to evaluate the effectiveness of the Behavior-Tailored Intervention (BHATIN) model on knowledge, Theory of Planned Behavior (TPB) constructs, self-efficacy, hypertension self-care behaviors, salt preference, and clinical outcomes (blood pressure, BMI, and metabolic biomarkers) among adults with hypertension.
Methods: A quasi-experimental pretest–posttest design with a non-equivalent control group was conducted among 90 adults with hypertension (intervention = 45; control = 45). The intervention group received the BHATIN program integrating TPB-based behavioral strategies, mindfulness-informed coaching, skill-based training, and social support, while the control group received standard care. Data were collected using knowledge, TPB-based questionnaires and clinical measurements (salt preference, blood pressure, BMI, and metabolic biomarkers) and analyzed using paired and independent t-tests (p < 0.05).
Results: The intervention group showed significant improvements in attitude, subjective norm, perceived behavioral control, intention, self-efficacy, and self-care behaviors (all p < 0.001). Significant reductions were also observed in systolic and diastolic blood pressure, total cholesterol, random blood glucose, and salt preference (p < 0.05), where the control group showed minimal change.
Conclusion: The BHATIN model improves psychosocial determinants, self-care behaviors, salt preference, and selected clinical biomarkers among adults with hypertension, providing a feasible nurse-led strategy for community-based hypertension management.
Keywords: hypertension self-care, salt preference, behavior-tailored intervention, mindfulness-based health coaching, theory of planned behavior
A Letter to the Editor has been published for this article.
A Response to Letter by Dr B has been published for this article.
Introduction
Hypertension remains a major global public health challenge and a leading contributor to cardiovascular morbidity and premature mortality. Despite the availability of effective antihypertensive therapies, blood pressure control in real-world settings remains suboptimal, largely due to poor adherence and inadequate long-term self-management behaviors.1,2 Consequently, international guidelines emphasize comprehensive hypertension management that integrates pharmacological treatment with sustained lifestyle modification and ongoing support within primary care systems.3
Among lifestyle-related determinants, dietary sodium intake plays a critical role in blood pressure regulation. Robust evidence from randomized trials and meta-analyses demonstrates that sodium reduction leads to clinically meaningful decreases in systolic blood pressure, with greater benefits observed with sustained and substantial reduction.4 Large-scale pragmatic studies further highlight the clinical relevance of salt-related behavior change, showing that salt substitution strategies can reduce cardiovascular events in high-risk populations.5 However, translating this evidence into daily practice remains challenging, as salt consumption is strongly influenced by habitual taste preferences and culturally embedded dietary patterns.
A persistent challenge in hypertension management is the intention–behavior gap, whereby individuals express motivation to adopt healthier behaviors but struggle to maintain consistent implementation. The Theory of Planned Behavior (TPB) provides a well-established framework for understanding this gap, positing that attitudes, subjective norms, and perceived behavioral control (PBC) shape behavioral intention and subsequent action.6 Empirical studies in hypertension populations indicate that TPB constructs are associated particularly perceived behavioral control with adherence to dietary, physical activity, and treatment-related self-care behaviors.7,8 Nevertheless, TPB-based education alone may be insufficient to address practical barriers, emotional factors, and habitual behaviors that undermine sustained lifestyle change.
Beyond cognitive determinants, psychological stress and affective states can exacerbate unhealthy eating behaviors, including excessive salt intake. Mindfulness-based interventions have emerged as promising approaches to enhance self-regulation, reduce stress reactivity, and support behavioral control. Evidence suggests that mindfulness-based strategies can improve self-efficacy and contribute to blood pressure reduction through improved stress management and awareness of habitual behaviors.9 Integrating mindfulness with behavior change frameworks may therefore strengthen the translation of intention into sustained action.
Importantly, mindfulness-based self-regulation may complement TPB constructs by strengthening perceived behavioral control and enhancing the alignment between intention and action.10,11 By increasing awareness of habitual responses and improving emotional regulation, mindfulness practices may facilitate greater control over taste-driven behaviors, including salt consumption.12,13 Within this integrated framework, salt preference can be conceptualized as a modifiable behavioral mechanism through which cognitive intention and self-regulatory capacity influence measurable clinical outcomes such as blood pressure and metabolic biomarkers.4,14
Collectively, these findings underscore the need for theory-driven, behaviorally tailored interventions that go beyond education by explicitly targeting psychosocial mechanisms, self-regulation capacities, and taste-related behaviors. While multicomponent self-management interventions have shown promise in improving hypertension outcomes,15 limited evidence exists for integrated models that simultaneously operationalize TPB constructs, incorporate mindfulness-based coaching, and explicitly position salt preference as a behavioral mediator linking psychological intention to measurable clinical outcomes. Most prior studies have examined these components independently rather than within a unified theoretical pathway. Consequently, the pathway through which psychological intention and self-regulatory processes translate into sustained modification of salt preference and measurable clinical outcomes remains insufficiently understood.
The Behavior-Tailored Intervention (BHATIN) model was conceptually developed as an integrated, theory-driven framework designed to operationalize this behavioral pathway. The model combines TPB-based cognitive components targeting attitudes, subjective norms, and perceived behavioral control16,17 with mindfulness-guided self-regulation strategies aimed at enhancing emotional awareness and stress management.18 Within this integrated framework, salt preference modification is conceptualized as a central behavioral mechanism linking psychological intention and self-regulatory capacity to measurable clinical outcomes, including blood pressure and related metabolic biomarkers.14,19 To address this gap, the present study developed and evaluated the Behavior-Tailored Intervention (BHATIN) model, aiming to assess its effectiveness in improving TPB constructs, self-efficacy, self-care behaviors, knowledge, salt preference, blood pressure, BMI, and metabolic biomarkers.
Methods
Study Design
This study employed a quasi-experimental pretest–posttest design with a non-equivalent control group to evaluate the effectiveness of the Behavior-Tailored Intervention (BHATIN) on knowledge, Theory of Planned Behavior (TPB) constructs, self-care management, BMI, and clinical biomarkers among patients with hypertension. The study was conducted in a community-based primary healthcare setting in Jatinangor, West Java, Indonesia, from March to October 2025. Participants were allocated into two groups: an intervention group that received the BHATIN program in addition to usual hypertension care and a control group that received usual hypertension care only. This design was selected to allow evaluation of behavioral and clinical changes over time while considering practical and ethical constraints in real-world nursing practice. An overview of the BHATIN intervention structure, including session strategies, main activities, and multidisciplinary roles involved in each phase, is presented in Table 1.
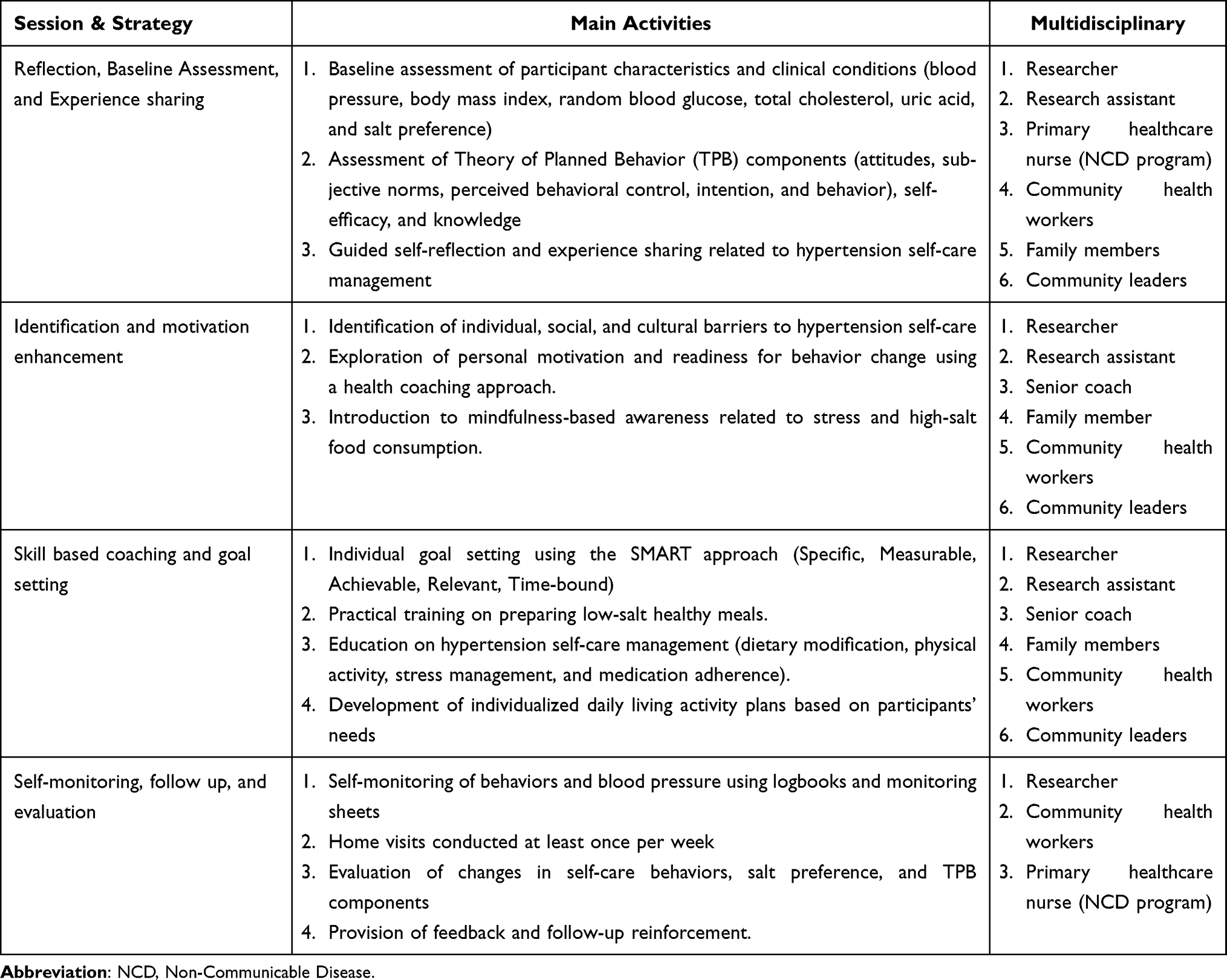 |
Table 1 Session, Main Activities, and Interdisciplinary Roles of the BHATIN Intervention |
Sample Size, Setting, and Intervention Procedure
The sample in this study consisted of patients with hypertension who met the eligibility criteria and agreed to participate. Sample size calculation was performed using G*Power software with a significance level (α) of 0.05 and a statistical power (1–β) of 0.95. The effect size was estimated based on mean and standard deviation values reported in a previous study,20 in which the mean ± SD was 2.42 ± 0.73 for the intervention group and 3.04 ± 0.92 for the control group, resulting in an effect size of 0.75. Based on this calculation, a minimum of 40 participants per group was required. To anticipate potential dropouts, an additional 10% was added, yielding 45 participants per group and a total sample size of 90 participants. In anticipation of potential attrition, the calculated sample size was increased by 10%. This adjustment was based on methodological recommendations for community-based behavioral interventions, where dropout rates typically range between 5–20%, depending on intervention duration and follow-up period.21,22 Given the 12-week intervention period and primary care setting, a conservative 10% attrition rate was considered appropriate to maintain adequate statistical power.
Participants were recruited from different villages within the same district to minimize potential contamination between intervention and control groups while maintaining comparable socio-demographic and healthcare contexts. One village was designated as the intervention site, while another served as the control site. Participants in the intervention area received the Behavior-Tailored Intervention (BHATIN) program, whereas participants in the control area received standard hypertension care routinely provided by primary healthcare services. Baseline demographic and clinical characteristics were assessed prior to intervention, and statistical comparisons indicated no significant differences between groups at baseline (Table 2).
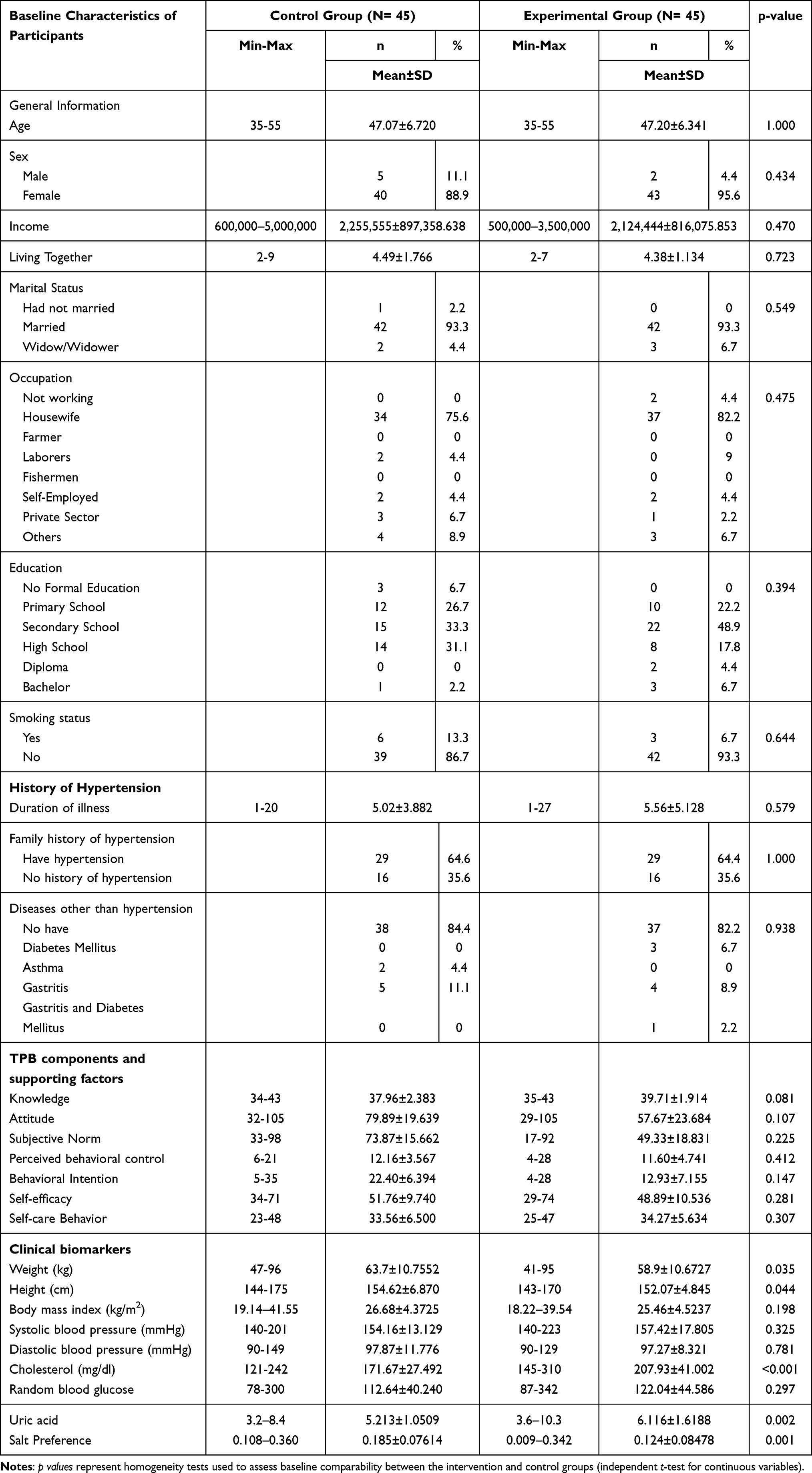 |
Table 2 Comparison of Baseline Demographic Data and Health Information Between the Experimental and the Control Group |
Both primary healthcare settings were located within the same district health authority and operated under comparable service structures. Routine hypertension care was delivered using the same standard management protocols, including regular blood pressure monitoring, antihypertensive medication management, and standard lifestyle counselling provided by primary healthcare staff. Therefore, the primary distinction between the two settings was the implementation of the BHATIN program in the intervention village, whereas the control village continued to receive standard hypertension care.
The inclusion criteria were: (1) adults aged 35–55 years; (2) diagnosed with hypertension and presenting uncontrolled blood pressure, defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg; (3) currently receiving routine antihypertensive treatment with stable medication for at least three months prior to enrolment; and (4) able to communicate effectively and provide informed consent. Exclusion criteria included: (1) documented cardiovascular complications such as coronary heart disease or stroke; (2) pregnancy; (3) diagnosed cognitive impairment or severe psychiatric disorders that could interfere with participation or adherence to the intervention; and (4) inability to complete all stages of the study. The BHATIN intervention implementation flow is presented in Figure 1.
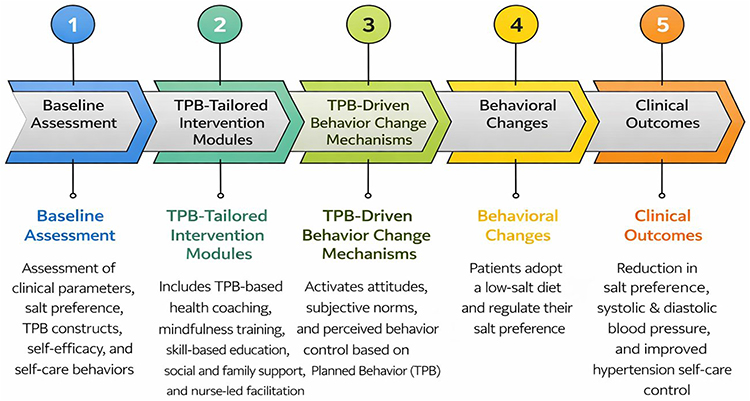 |
Figure 1 BHATIN Implementation flow. |
The intervention group received the Behavior-Tailored Intervention (BHATIN) program, a theory-driven and nurse-led intervention designed to improve hypertension self-care management by targeting behavioral determinants and salt preference. The program consisted of four structured sessions: reflection and baseline assessment, identification of barriers and motivation enhancement, skill-based coaching with goal setting, and self-monitoring with follow-up evaluation. The BHATIN intervention consisted of four structured sessions delivered over a 12-week period, following a 4-week preparatory phase. Each session was conducted in small group formats of 6–8 participants, delivered face-to-face by trained facilitators including researchers, senior health coaches, and community nurses experienced in hypertension management. Each session lasted approximately 60–90 minutes and followed a standardized session manual to ensure consistency of delivery. A standardized session manual and structured monitoring forms were used to ensure consistency in delivery across all phases.
The multidisciplinary team involved in the BHATIN program consisted of researchers, research assistants, primary healthcare nurses (NCD program), senior coaches, community health workers, family members, and community leaders. Researchers were responsible for overall coordination, baseline assessment procedures, and supervision of intervention implementation. Research assistants supported data collection, documentation, and monitoring activities. Primary healthcare nurses facilitated clinical assessments and reinforced standard hypertension management practices. Senior health coaches delivered behavioral coaching sessions, guided motivational discussions, and introduced mindfulness-based strategies. Community health workers assisted with follow-up activities and community-based reinforcement. Family members and community leaders contributed to strengthening social support, normative influence, and sustainability of behavior change. Implementation of each intervention phase involved these multidisciplinary team members according to their professional roles. Researchers and primary healthcare nurses conducted baseline clinical assessments, senior health coaches facilitated behavioral coaching sessions, while community health workers and family members supported follow-up monitoring and reinforcement of behavior change at the community level. Details of session was explained in detail as follows:
Phase 1: Reflection, Baseline Assessment, and Experience Sharing
At the beginning of the intervention, participants underwent a comprehensive baseline assessment conducted by trained nurses and researchers. This phase included assessment of sociodemographic characteristics, clinical parameters (blood pressure, body mass index, random blood glucose, total cholesterol, uric acid), salt preference, and self-care behaviors. In addition, TPB constructs: attitudes, subjective norms, perceived behavioral control, intention, as well as self-efficacy and knowledge were measured. Participants were then guided through reflective discussions to explore their daily experiences, challenges, and perceptions related to hypertension management, dietary habits, and salt consumption. This reflective process aimed to increase awareness of existing behaviors and establish rapport between participants and facilitators.
Phase 2: Identification of Barriers and Motivation Enhancement
In this phase, individualized behavioral, social, and cultural barriers to hypertension self-care were identified through guided interviews and group discussions. Using a health coaching approach, facilitators explored participants’ motivation, readiness to change, and perceived control over dietary and lifestyle behaviors. Mindfulness techniques were introduced to enhance self-awareness related to stress, emotional eating, and habitual salt consumption. This phase primarily targeted the strengthening of attitudes, subjective norm, and perceived behavioral control as core TPB determinants.
Phase 3: Skill-Based Coaching and Goal Setting
Participants then engaged in skill-based coaching sessions focused on translating intention into practical behavior. Individualized goals were established using the SMART (Specific, Measurable, Achievable, Relevant, and Time-bound) framework. Practical training included preparation of low-salt meals, portion control strategies, daily activity planning, stress management techniques, and adherence to antihypertensive medication. Family members and community health cadres were involved to reinforce social support and normative influences. This phase aimed to strengthen self-efficacy and facilitate sustained changes in salt preference and self-care practices.
Phase 4: Self-Monitoring, Follow-Up, and Evaluation
During the final phase, participants were encouraged to conduct self-monitoring of blood pressure and daily behaviors using logbooks and monitoring sheets. Regular follow-up was conducted through home visits and community-based meetings to provide feedback, address emerging barriers, and reinforce behavioral changes. At the end of the intervention period, participants underwent post-intervention assessment to evaluate changes in TPB constructs, self-care behaviors, salt preference, and clinical biomarkers.
Overall, the BHATIN intervention was designed to bridge the intention-behavior gap by positioning salt preference as a key behavioral mediator, supported by self-efficacy and mindfulness-based coaching. This structured, behavior-tailored approach reflects real-world nursing practice and emphasizes sustainable self-care management for patients with hypertension.
Instruments
The instruments used in this study consisted of structured questionnaires and clinical biomarker measurements, as described below.
Demographic and Health Information Questionnaire
A demographic and health information questionnaire was developed by the researchers to collect participants’ background and health-related data, including age, sex, occupation, educational level, marital status, clinical history, physiological data, and behavioral characteristics related to hypertension management. The content validity of this questionnaire was reviewed and approved by a panel of experts.
Hypertension Knowledge-Level Scale (HK-LS)
Hypertension-related knowledge was measured using the Hypertension Knowledge-Level Scale (HK-LS), adapted from the Hypertension Evaluation of Lifestyle and Management Knowledge Scale (HELM). The instrument consists of 10 items assessing general knowledge of hypertension, hypertension complications, and factors influencing hypertension management and control. Items are presented in true–false and multiple-choice formats. The questionnaire was translated into Indonesian and underwent validity and reliability testing. Construct validity was confirmed using Pearson correlation (r > 0.2632), and internal consistency reliability was high, with a Cronbach’s alpha of 0.890, indicating excellent reliability.23,24
Intention Behavior Questionnaire (IBQ)
The Intention Behavior Questionnaire (IBQ) was used to assess components of the Theory of Planned Behavior, including attitude, subjective norm, perceived behavioral control, intention, and supporting constructs such as behavioral beliefs, normative beliefs, control beliefs, outcome evaluation, and motivation to comply. The questionnaire consisted of favorable and unfavorable statements rated on a 7-point Likert scale, along with several multiple-choice and open-ended items. Lower scores indicate stronger confidence in performing the behavior, whereas higher scores reflect greater uncertainty. The IBQ has demonstrated acceptable validity and reliability, with a reported Cronbach’s alpha of 0.623.6,25,26
Self-Efficacy Questionnaire
Self-efficacy in hypertension management was measured using a questionnaire adapted from the self-efficacy instrument developed by Gheashlagh et al (2018) and modified to fit the Indonesian cultural context. The questionnaire consists of 16 items rated on a 5-point Likert scale, ranging from very confident to very unconfident. Higher scores indicate better self-efficacy in managing hypertension. Validity testing showed that all items met the criteria (r > 0.2632), and the instrument demonstrated good internal consistency, with a Cronbach’s alpha of 0.827.27
Hypertension Self-Care Profile (HBP-SCP)
Hypertension self-care management was assessed using the Hypertension Self-Care Profile (HBP-SCP), originally developed by Han et al28 to evaluate behavioral, motivational, and self-efficacy components of hypertension self-management. The instrument consists of 60 items divided into three domains: behavior (20 items), motivation (20 items), and self-efficacy (20 items). Each item is rated on a 4-point Likert scale, with higher scores indicating better hypertension self-care performance and stronger self-efficacy in blood pressure management.
The HBP-SCP has demonstrated strong psychometric properties in previous validation studies. In the present study, the instrument showed item validity coefficients ranging from 0.572 to 0.922, a Content Validity Index (CVI) of 0.964, and excellent internal consistency reliability (Cronbach’s α = 0.955), indicating high validity and reliability.29
BMI (Body Mass Index)
Body weight was measured using a calibrated digital scale with participants wearing light clothing and no shoes, and height was measured using a portable stadiometer. BMI values were classified according to the Asia-Pacific criteria as follows: <18.5 kg/m2 (underweight), 18.5–22.9 kg/m2 (normal weight), 23.0–24.9 kg/m2 (overweight), and ≥25.0 kg/m2 (obese). This classification is recommended for Asian populations due to evidence that cardiovascular and metabolic risk factors occur at lower BMI thresholds compared with global WHO cutoffs.30
Clinical Biomarker Measurements
Clinical biomarkers included blood pressure, salt preference, random blood glucose, total cholesterol, and uric acid levels. Blood pressure was measured using a digital sphygmomanometer following standard guidelines. All patents were seated comfortably for at least five minutes before measurement, with the arm supported at heart level. Two measurements were taken at one-minute intervals, and the average value was recorded. Salt preference was assessed using a handheld salinometer (temperature salt concentration tester hydrometer analyzer) through a graded salt solution test, in which salt solutions were prepared by mixing distilled water and 0.9% NaCl to produce a series of concentrations ranging from 0% to 100%. Participants’ preferred salt concentration was determined based on the selected concentration level and recorded as an indicator of salt preference. Random blood glucose levels were measured using a GlucoDr Super Sensor AGM 2200, provided by the primary healthcare center. Total cholesterol and uric acid levels were measured using the Autocheck GCU 3-in-1 device. Capillary blood samples were obtained using sterile procedures. All measurements were conducted at baseline and at the end of the intervention period using the same procedures to ensure consistency. BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2). Body weight was measured using a calibrated digital scale with participants wearing light clothing and no shoes. Height was measured using a portable stadiometer with participants standing upright in the Frankfort horizontal plane. BMI categories were classified according to the Asia-Pacific criteria, with values <18.5 kg/m2 classified as underweight, 18.5–22.9 kg/m2 as normal weight, 23.0–24.9 kg/m2 as overweight (at risk), 25.0–29.9 kg/m2 as obese class I, and ≥30 kg/m2 as obese class II.
Outcome Measures
All outcomes assessed in this study were predefined prior to data collection and included psychosocial, behavioral, and clinical parameters. Psychosocial outcomes comprised TPB constructs (attitude, subjective norm, perceived behavioral control, and intention), knowledge, and self-efficacy. Behavioral outcomes included hypertension self-care behaviors and salt preference. Clinical outcomes consisted of blood pressure, body mass index (BMI), random blood glucose, total cholesterol, and uric acid levels. All outcomes were measured at baseline and post-intervention.
Data Collection
Data collection was conducted in several stages following ethical approval and participant recruitment. Prior to data collection, all participants received an informed consents which is details of explanation on the study objectives, procedures, potential benefits, and risks of participation in this study. At baseline (pre-test), data were collected from both the intervention and control groups. Two trained research assistants were involved in this study. Their responsibilities included participant recruitment, scheduling assessments, assisting with informed consent procedures, conducting baseline and post-intervention data collection, recording anthropometric and clinical measurements, and performing data entry. However, for delivering the BHATIN intervention, they were not involved. Although full blinding was not feasible due to the quasi-experimental design and geographical allocation, research assistants responsible for outcome assessment were not involved in intervention facilitation and were instructed to adhere strictly to standardized measurement procedures.
Prior to data collection, research assistants underwent structured training conducted by the principal investigator. The training covered study protocols, ethical procedures, standardized administration of questionnaires, anthropometric measurement techniques, blood pressure assessment procedures, and documentation guidelines.
Following baseline assessment, participants in the intervention group received the BHATIN (Behavior-Tailored Intervention) program with the usual care, while participants in the control group received usual care provided by primary healthcare services. During the intervention period, data related to behavioral engagement and self-monitoring were documented using monitoring sheets and logbooks, particularly for blood pressure and daily self-care practices. At the end of the intervention period (post-test), the same set of measurements was repeated in both groups. Post-intervention data collection included reassessment of clinical biomarkers, salt preference, TPB components, self-efficacy, hypertension knowledge, and self-care behaviors. All data were collected by trained personnel who followed standardized data collection protocols to ensure consistency and reliability across measurements. The participant allocation process and overall program implementation are summarized in Figure 2.
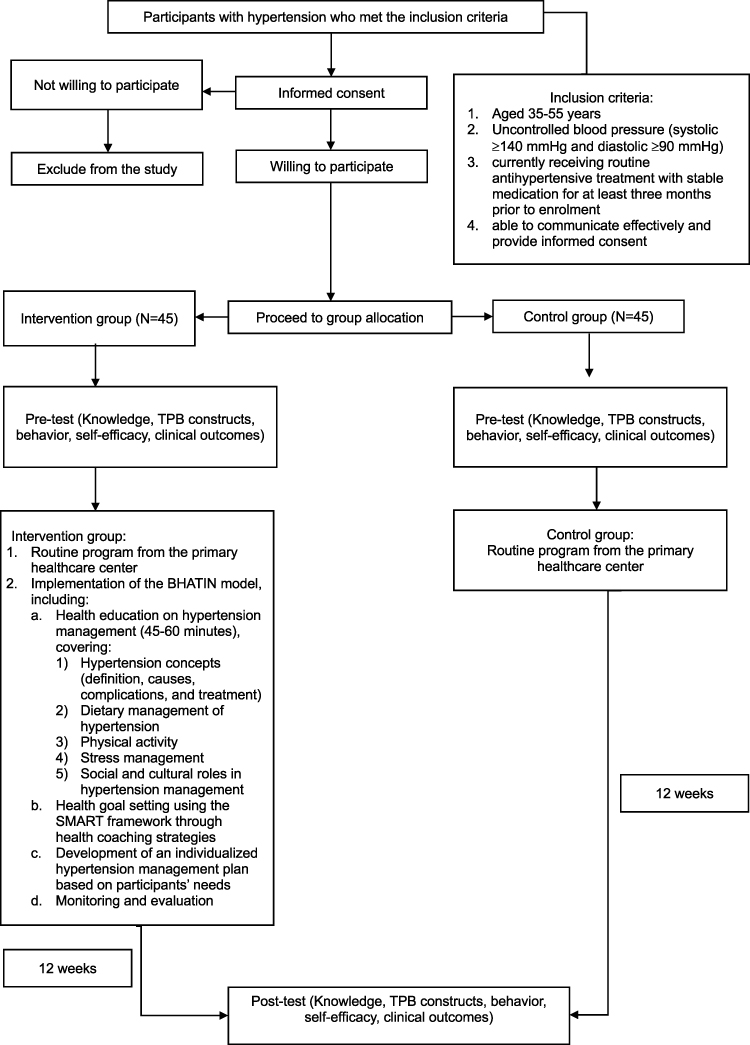 |
Figure 2 Samples allocation and program implementation. |
Data Analysis
The data were analysed using the descriptive analysis and inferential analysis. Demographic characteristics of the participants were analyzed using descriptive statistics and presented as frequencies, percentages, means, and standard deviations. Data normality was assessed using the Shapiro–Wilk test, which indicated that the study variables were normally distributed. To examine within-group differences before and after the implementation of the BHATIN model in both the intervention and control groups, a paired t-test was applied. To evaluate between-group differences between the intervention and control groups after the intervention, an independent t-test was used. All statistical analyses were performed using IBM SPSS Statistics software. The level of statistical significance was set at p < 0.05.
Ethical Considerations
This study was conducted in accordance with the principles of the declaration of Helsinki. Ethical approval for this study was obtained from the Ethics Committee of Universitas Padjadjaran (No. 54/UN6.KEP/EC/2025). The study was conducted in accordance with the ethical principles outlined by the Council for International Organizations of Medical Sciences (CIOMS) and the World Health Organization (WHO), including respect for persons, beneficence, and justice. Written informed consent was obtained from all participants prior to data collection.
Results
Comparison of Baseline Demographic Data and Health Information Between the Experimental and the Control Group
Most participants in both the experimental (95.6%) and control groups (88.9%) were female, with a comparable mean age of 47.20 ± 6.34 years in the experimental group and 47.07 ± 6.72 years in the control group. The majority of participants were married, lived with family members, and were housewives with secondary to high school educational backgrounds. Monthly income levels and smoking status were similar between groups. The mean duration of hypertension exceeded five years in both groups, and approximately two-thirds of participants reported a family history of hypertension. Baseline scores for knowledge, attitude, subjective norm, perceived behavioral control, intention, self-efficacy, and self-care behavior did not differ significantly between groups. Clinical biomarkers, including body mass index, systolic and diastolic blood pressure, and random blood glucose, were generally comparable at baseline, although differences were observed in cholesterol, uric acid levels, and salt preference. Overall, the experimental and control groups demonstrated comparable baseline characteristics prior to the implementation of the BHATIN intervention, as presented in Table 2.
Effect of BHATIN Model on Attitude, Subjective Norm, Perceived Behavioral Control and Intention Among Patients with Hypertension
Table 3 shows changes in attitude, subjective norm, perceived behavioral control, intention, self-efficacy, and self-care behavior before and after the BHATIN intervention. In the intervention group, all Theory of Planned Behavior components: attitude, subjective norm, perceived behavioral control, and intention along with self-efficacy and self-care behavior, improved significantly after the intervention (p < 0.001). The mean attitude score increased from 57.67 ± 23.68 to 90.91 ± 9.11, while subjective norm improved from 49.33 ± 18.83 to 91.18 ± 5.90. Similarly, perceived behavioral control increased from 11.60 ± 4.741 to 23.36 ± 4.024, and behavioral intention increased from 12.93 ± 7.155 to 32.07 ± 2.435. Improvements were also observed in self-efficacy (48.89 ± 10.53 to 62.67 ± 9.02) and self-care behavior (34.27 ± 5.634 to 54.73 ± 12.721). In contrast, the control group showed no significant changes in most variables; only attitude increased significantly (p = 0.003), while subjective norm, perceived behavioral control, intention, self-efficacy, and self-care behavior remained unchanged (p > 0.05).
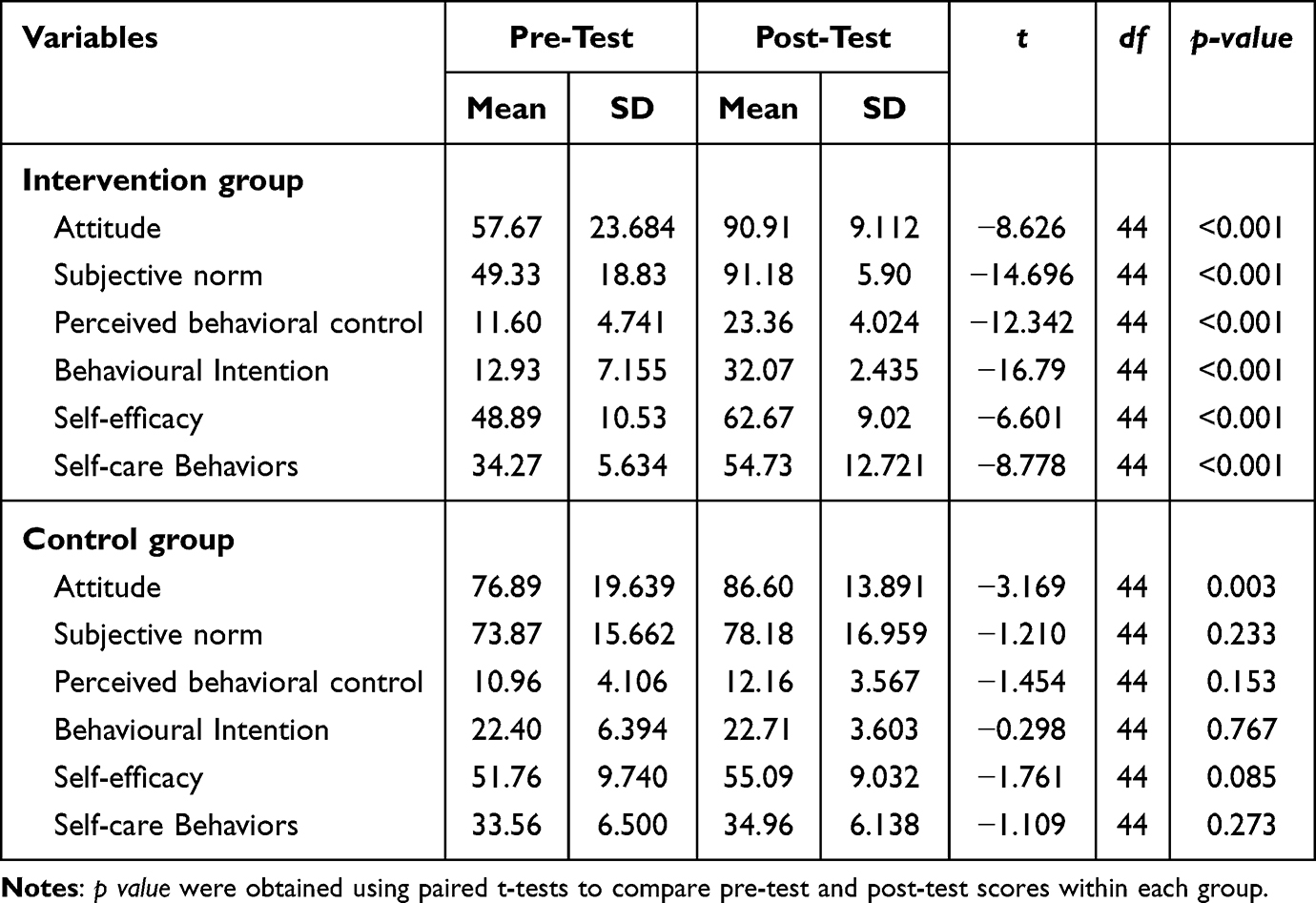 |
Table 3 Mean Difference of Attitude, Subjective Norm, Perceived Behavioral Control and Behavioral Intention Before and After Implementation of BHATIN Within Intervention and Control Group (N= 45) |
Effect of the BHATIN Model on Attitude, Subjective Norm, Perceived Behavioral Control and Intention Between the Intervention and Control Group
Table 4 presents the between-group comparison of Theory of Planned Behavior (TPB) components and self-care behavior after the intervention. Participants in the intervention group demonstrated substantially higher scores than those in the control group. Post-intervention attitude scores were slightly higher in the intervention group (90.91 ± 9.112) compared with the control group (86.60 ± 13.891). Subjective norm scores were 91.18 ± 5.902 in the intervention group compared with 78.18 ± 16.959 in the control group, while perceived behavioral control was 23.36 ± 4.042 versus 12.16 ± 3.567, respectively (p < 0.001). Similar differences were observed for behavioral intention, self-efficacy, and self-care behaviors (p < 0.001). No statistically significant difference was observed for attitude (p = 0.085).
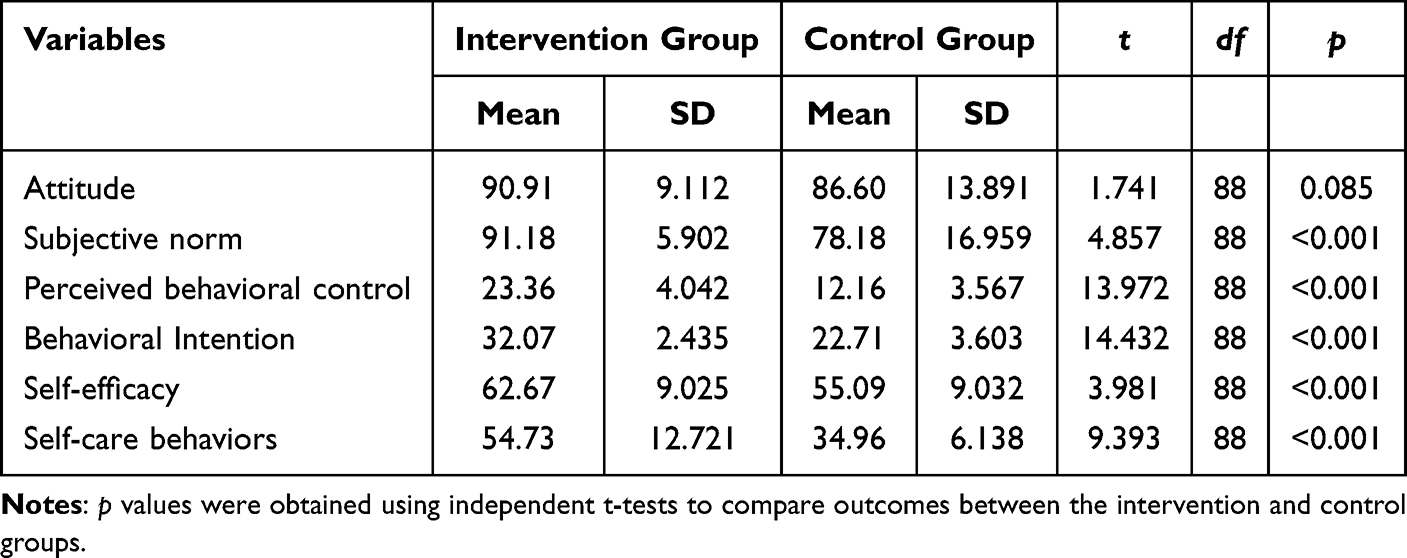 |
Table 4 Mean Difference of Attitude, Subjective Norm, Perceived Behavioral Control and Behavioral Intention After Implementation of BHATIN Between Intervention and Control Group (N= 45) |
Effect of BHATIN Model on Blood Pressure, Cholesterol Level, BMI, Random Blood Glucose, Salt Preference Before and After Intervention
Table 5 shows significant reductions in the intervention group for systolic blood decreased pressure from 157.42 ± 17.805 mmHg to 147.84 ± 10.805 mmHg (p = 0.008), diastolic blood pressure decreased from 97.27 ± 8.321 mmHg to 93.16 ± 6.502 mmHg (p = 0.010). Total cholesterol also declined from 207.93 ± 41.002 mg/dL to 188.33 ± 36.294 mg/dL (p = 0.040), while random blood glucose decreased from 122.04 ± 44.586 mg/dL to 100.87 ± 22.557 mg/dL (p = 0.010), and salt preference (p = 0.043) after receiving the BHATIN intervention, while body mass index and uric acid levels did not change significantly (p > 0.05). In the control group, no significant changes were observed in most clinical biomarkers and salt preference (p > 0.05), except for uric acid levels (p = 0.016).
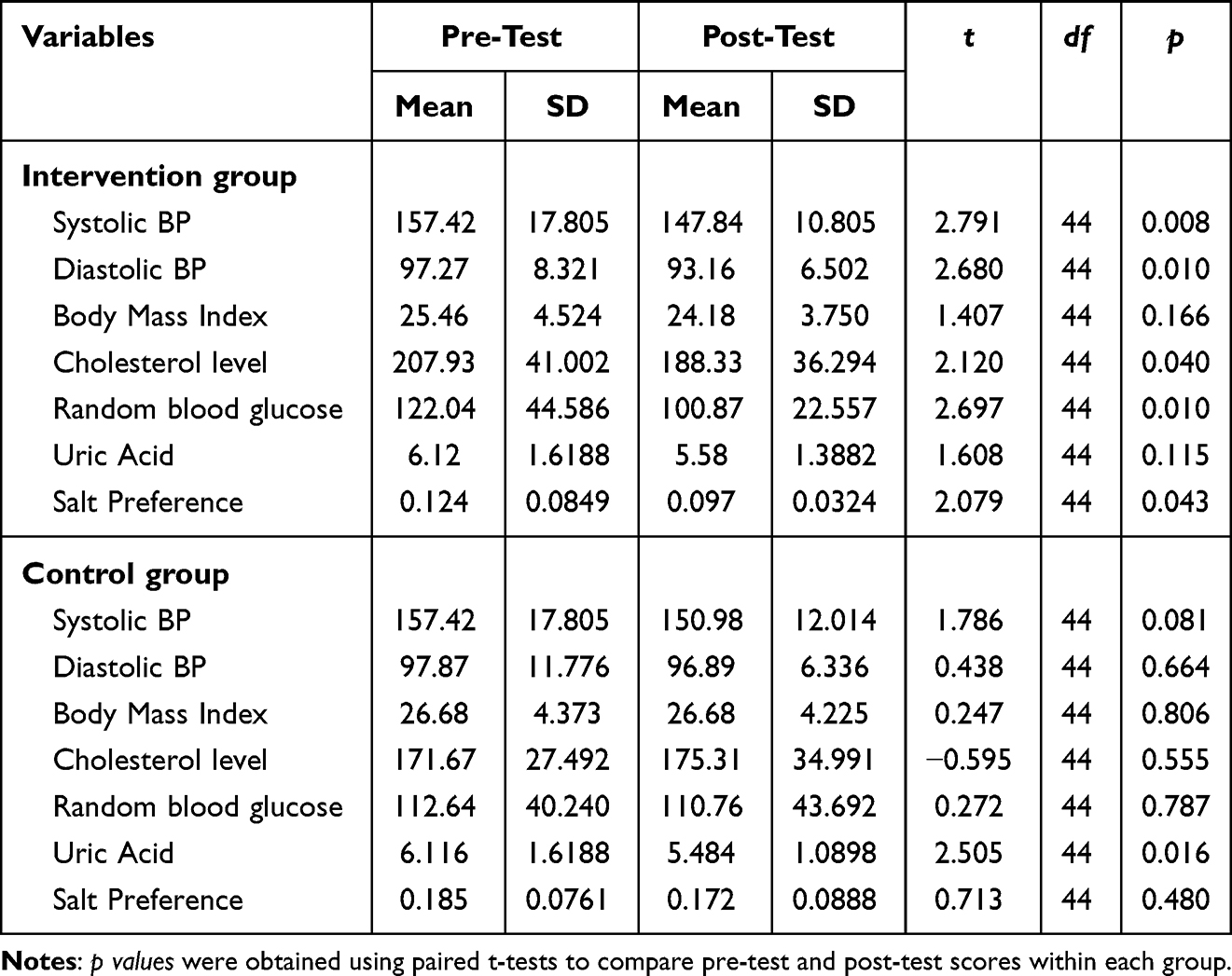 |
Table 5 Mean Difference of Blood Pressure, Cholesterol Level, BMI, Random Blood Glucose, Salt Preference Before and After Implementation of BHATIN Within Intervention and Control Group (N= 45) |
Effect of BHATIN Model on Blood Pressure, Cholesterol Level, BMI, Random Blood Glucose, Salt Preference Between the Intervention and Control Groups
Table 6 presents the between-group comparison of clinical biomarkers following the intervention. Significant differences were observed between the intervention and control groups in diastolic blood pressure in the intervention group 93.16 ± 6.502 mmHg compared with the control group 96.89 ± 6.336 mmHg (p = 0.007), body mass index (BMI) was also lower in the intervention group (24.178 ± 3.750) than in the control group (26.459 ± 4.225) (p = 0.008), and salt preference (p < 0.001). Participants in the intervention group demonstrated a greater reduction in BMI compared with those receiving usual care, indicating that the BHATIN model was associated not only with blood pressure improvement but also with modest anthropometric changes over the intervention period. No statistically significant between-group differences were identified for systolic blood pressure, total cholesterol, random blood glucose, or uric acid levels at post-intervention (p > 0.05).
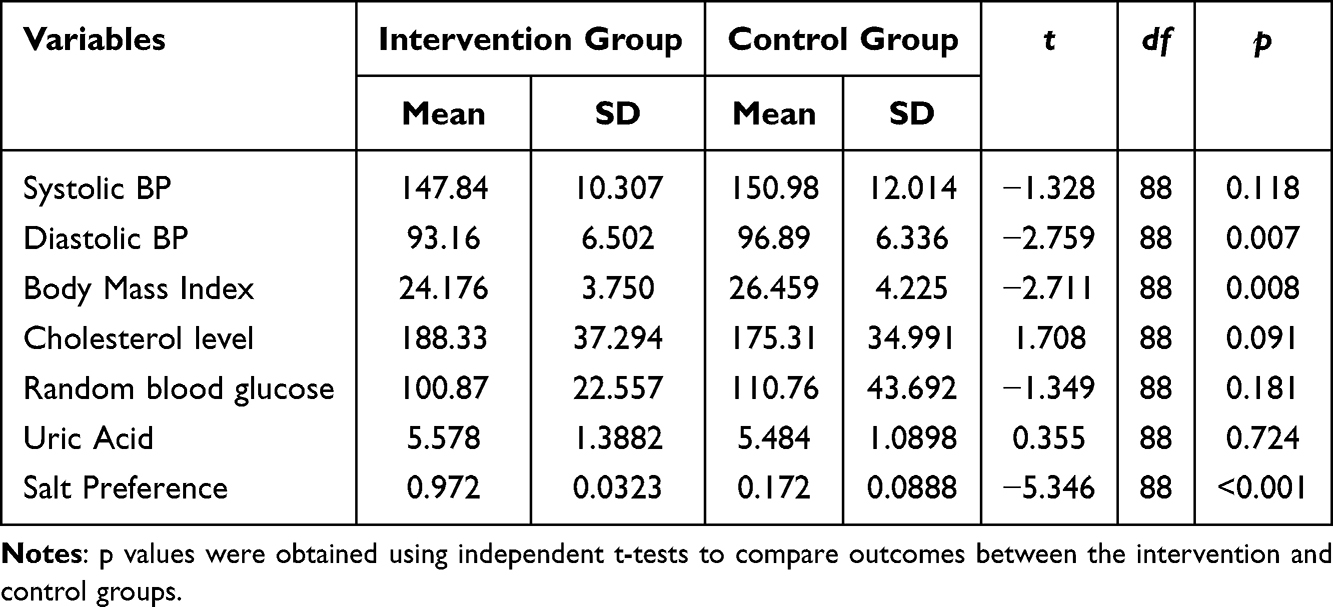 |
Table 6 Mean Difference of Blood Pressure, Cholesterol Level, BMI, Random Blood Glucose, Salt Preference After Implementation of BHATIN Between Intervention and Control Group (N= 45) |
Discussion
This study described the effect of the BHATIN model intervention the TPB components and clinical outcomes among hypertension patients. This study advances existing literature by illustrating how TPB constructs can be operationalized within a nurse-led, behaviorally tailored intervention that directly addresses self-regulation and dietary behavior in community settings.6,7
A key contribution of the BHATIN model lies in conceptualizing salt preference as a modifiable behavioral mediator, rather than a fixed dietary habit. While most TPB-based interventions have focused primarily on intention and adherence outcomes, the BHATIN model integrates mindfulness-based health coaching and skills-oriented strategies to address habitual taste preferences that often undermine dietary sodium reduction. The significant reduction in salt preference observed in this study supports evidence that taste-related behaviors are responsive to structured behavioral interventions, particularly when combined with reflective awareness and continuous reinforcement.31,32
Improvements in perceived behavioral control (PBC) and self-efficacy warrant particular attention, as these constructs functioned as proximal enablers of behavior change rather than distal cognitive outcomes. The inclusion of skills-based training, SMART goal setting, and self-monitoring enhanced participants’ capacity to manage real-world barriers, such as selecting low-sodium foods, managing stress, and maintaining physical activity. This finding aligns with previous studies showing that interventions targeting PBC and self-efficacy are more likely to bridge the intention–behavior gap in chronic disease self-management.33,34 The concurrent improvements in diastolic blood pressure and body mass index further suggest that strengthening behavioral control mechanisms can yield downstream cardiometabolic benefits, even in the absence of explicit weight-loss targets.
One important implication of these findings relates to the well-documented intention–behavior gap in hypertension self-management. Although individuals may report positive attitudes and intentions to reduce salt intake and improve lifestyle behaviors, sustaining these behaviors in daily practice is often hindered by contextual, emotional, and habitual influences. The BHATIN model appears to address this gap by integrating cognitive restructuring through the constructs of the Theory of Planned Behavior with self-regulatory strengthening via mindfulness-based training and structured skill development, consistent with contemporary behavior change frameworks that emphasize perceived behavioral control and self-regulation.10,12
Specifically, improvements in perceived behavioral control and self-efficacy likely strengthened participants’ capacity to manage dietary and emotional triggers in daily life,10 while mindfulness practices may have increased awareness of habitual responses related to salt consumption and emotional regulation.12,35 Within this integrated framework, salt preference functioned as a concrete behavioral mechanism through which psychological readiness was translated into measurable behavioral change. This sequential pathway illustrates how cognitive intention was progressively translated into sustained behavioral adjustment and subsequent physiological improvement. Thus, changes in psychosocial determinants did not remain at the cognitive level but were operationalized through strengthened self-regulation and modification of taste preference as a pathway toward physiological improvement. The subsequent reductions in blood pressure and cardiometabolic markers further suggest that behavioral modification extended beyond cognitive intention and resulted in clinically meaningful outcomes.
In contrast, the control group demonstrated significant improvement only in attitude, reinforcing evidence that education or routine care alone may influence cognitive evaluations but rarely produces sustained behavioral change. Previous research has consistently shown that attitude change without concurrent enhancement of behavioral control, self-regulation, and social support is insufficient to drive meaningful health behavior change.36,37 These findings highlight the limitations of education-only approaches in hypertension management.
Beyond psychosocial outcomes, the BHATIN model was also associated with significant reductions in clinical biomarkers, including blood pressure, total cholesterol, random blood glucose, and salt preference. These effects are consistent with evidence that structured behavioral and self-management interventions effectively improve blood pressure and cardiometabolic risk profiles among patients with hypertension.31,32 Importantly, the significant reduction in salt preference highlights the novelty of the BHATIN approach, as taste-related behaviors are often under-recognized in conventional interventions. Previous studies have shown that sustained salt reduction through education, behavioral reinforcement, and follow-up can stabilize blood pressure and improve long-term hypertension control.5,14,31
The clinical relevance of these findings warrants further consideration. Even modest reductions in blood pressure are associated with meaningful decreases in cardiovascular morbidity and mortality at the population level. Therefore, the observed improvements in blood pressure and cardiometabolic biomarkers in this study may have important implications for long-term cardiovascular risk management when maintained over time. The concurrent modification of salt preference suggests that behavioral adjustments extended beyond cognitive intention to tangible dietary practices directly linked to hypertension control. Importantly, these findings indicate that strengthening psychosocial determinants through structured behavioral support may translate into clinically meaningful improvements in cardiometabolic regulation, particularly in community-based populations where sustained lifestyle modification is often challenging.
From an implementation perspective, the BHATIN model was delivered within existing community-based primary healthcare structures and led by trained nurses, indicating feasibility without the need for highly specialized or resource-intensive infrastructure. The structured yet adaptable design comprising behavioral assessment, mindfulness-guided self-regulation, skills based coaching, and self-monitoring allows integration into routine hypertension follow-up visits without disrupting established service workflows. Furthermore, the involvement of family members and community health cadres strengthens continuity of behavioral support beyond clinical encounters, thereby enhancing sustainability at the community level. By reinforcing and systematizing roles that already exist within primary care and community health programs, the intervention enhances implementation capacity without creating parallel systems or excessive additional workload. This multidisciplinary and community-oriented framework increases the potential scalability and long-term integration of the intervention within routine primary healthcare practice.
Overall, these findings underscore the value of the BHATIN model as a comprehensive, nurse-led, behaviorally tailored intervention that integrates psychosocial mechanisms, practical skill development, and dietary behavior modification. By explicitly linking TPB constructs with mindfulness-based training and social support, the BHATIN model addresses the intention–behavior gap while remaining feasible within real world healthcare settings. As such, it offers a theoretically grounded and potentially sustainable framework for strengthening community-based hypertension self-care management.
Strength and Limitation
This study has several notable strengths. First, the BHATIN model was developed using a robust theoretical foundation, integrating the Theory of Planned Behavior with mindfulness-informed behavioral support and tailored strategies specifically targeting salt preference and self-regulation. This theory-driven design enhances conceptual coherence and intervention relevance. Second, the use of a quasi-experimental design with a comparison group enabled evaluation of both psychosocial determinants and objective clinical biomarkers within a real-world community setting. Third, the simultaneous assessment of behavioral constructs and cardiometabolic outcomes provides a multidimensional understanding of hypertension self-care management, strengthening the practical applicability of the findings. Nevertheless, several limitations warrant careful consideration. The allocation of participants based on geographical areas rather than individual randomization may introduce potential selection bias and limit internal validity. Although baseline characteristics were statistically comparable between groups, the possibility of unmeasured confounding factors cannot be fully excluded. Consequently, the observed between-group differences should be interpreted as associative rather than definitively causal. In addition, the follow-up duration of 12 weeks may not be sufficient to determine the long-term sustainability of behavioral modifications and clinical improvements. While short-term changes were observed, longer follow-up periods are required to assess durability of behavioral adherence and sustained cardiovascular risk reduction. Furthermore, although the intervention was conceptually grounded in the Theory of Planned Behavior, the proposed behavioral pathways linking psychosocial determinants, salt preference, and clinical biomarkers were not formally tested using mediation or causal modeling analyses. Therefore, the underlying mechanisms should be interpreted as theoretically informed rather than empirically confirmed. Future research employing randomized controlled designs, longer follow-up periods, and formal mediation analyses would provide stronger evidence regarding causal relationships and mechanism pathways.
Conclusion
The findings of this study demonstrate that the BHATIN (Behavior-Tailored Intervention) model effectively improves key psychosocial constructs, self-care behaviors, and selected clinical biomarkers among patients with hypertension. By addressing behavioral determinants, social support, self-efficacy, and salt preference, the BHATIN model offers a comprehensive and theory-driven approach to hypertension self-care management. This intervention has the potential to be integrated into community-based nursing practice to support sustainable lifestyle modification and blood pressure control.
Declaration of Use of AI in Scientific Writing
The authors declare that ChatGPT and paperpal was used solely to assist in improving the English language quality of this manuscript, including grammar, clarity, and sentence structure.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgment
The author thanked the participants in this study, community health workers, primary healthcare staff, and community leaders for their valuable participation and cooperation. Special appreciation is extended to Universitas Padjadjaran for ethical approval and academic support throughout the research process.
Author Biography
Andi Mayasari Usman is a doctoral student in the Medical Science Program at Universitas Padjadjaran, Indonesia, with research interests in medical surgical nursing for non-communicable diseases and mindfulness-based health coaching. Cecep Eli Kosasih is a nursing lecturer at Universitas Padjadjaran, Indonesia, whose research focuses on medical surgical nursing and emergency nursing. Iqbal Pramukti is a nursing lecturer with research interests in community nursing, HIV/AIDS, and health behavior interventions. Yulia Sofiatin is a public health lecturer specializing in hypertension prevention and community-based health interventions. Rian Adi Pamungkas is a nursing lecturer at Universitas Esa Unggul, Indonesia, with research interests in community nursing and diabetes mellitus management.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published, agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This publication charge is funded by Universitas Padjadjaran (UNPAD) through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhou B, Carrillo-Larco R, Danaei G, et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–18. doi:10.1016/S0140-6736(21)01330-1
2. Burnier M, Egan BM. Adherence in hypertension. Circ Res. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
3. W WHO. Global report on hypertension, the race against a silent killler. World Health Organization; 2023.
4. Huang L, Trieu K, Yoshimura S, et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials. BMJ. 2020. 368. m315. doi:10.1136/bmj.m315
5. Neal B, Wu Y, Feng X, et al. Effect of salt substitution on cardiovascular events and death. N Engl J Med. 2021;385(12):1067–1077. doi:10.1056/NEJMoa2105675
6. Ajzen I. Constructing A theory of planned behavior questionnaire. University of Massachusetts Amherst. 2016;1–7.
7. Pourmand G, Doshmangir L, Ahmadi A, et al. An application of the theory of planned behavior to self-care in patients with hypertension. BMC Public Health. 2020;20(1):1290. doi:10.1186/s12889-020-09385-y
8. Eslamimehr F, Hosseini Z, Aghamolaei T, Nikparvar M, Ghanbarnejad A. Predictors of self-care behaviors in patients with hypertension: the integrated model of theories of “planned behavior” and “protection motivation”. J Educ Health Promot. 2024;13:213. doi:10.4103/jehp.jehp_592_23
9. Zhang D, Lee EKP, Mak ECW, Ho CY, Wong SYS. Mindfulness-based interventions: an overall review. Br Med Bull. 2021;138(1):41–57. doi:10.1093/bmb/ldab005
10. Hagger MS, Hamilton K. Progress on theory of planned behavior research: advances in research synthesis and agenda for future research. J Behav Med. 2025;48(1):43–56. doi:10.1007/s10865-024-00545-8
11. Sniehotta FF, Presseau J, Araujo-Soares V. Time to retire the theory of planned behaviour. Health Psychol Rev. 2014;8(1):1–7. doi:10.1080/17437199.2013.869710
12. Tang YY, Tang R, Posner MI. Mindfulness meditation improves emotion regulation and reduces drug abuse. Drug Alcohol Depend. 2016. 163 1:S13–8. doi:10.1016/j.drugalcdep.2015.11.041
13. Goldberg SB, Tucker RP, Greene PA, et al. Mindfulness-based interventions for psychiatric disorders: a systematic review and meta-analysis. Clin Psychol Rev. 2018;59:52–60. doi:10.1016/j.cpr.2017.10.011
14. He Q, Du X, Wang L, Fang Y, Zhong J, Hu R. Taste preference for salt predicts salt intake in a chinese population. Nutrients. 2024;16(13). doi:10.3390/nu16132090
15. Weerahandi H, Paul S, Quintiliani LM, Chokshi S, Mann DM. A mobile health coaching intervention for controlling hypertension: single-arm pilot pre-post study. JMIR Form Res. 2020;4(5):e13989. doi:10.2196/13989
16. Ajzen I. The Theory of Planned Behavior. Organizat Behav Human Decis Proc. 1991;50:179–211. doi:10.1016/0749-5978(91)90020-T
17. Bosnjak M, Ajzen I, Schmidt P. The theory of planned behavior: selected recent advances and applications. Eur J Psychol. 2020;16(3):352–356. doi:10.5964/ejop.v16i3.3107
18. Rowland G, Hindman E, Hassmén P. Do group mindfulness-based interventions improve emotion regulation in children? A systematic review. J Child Family Stud. 2023;32(5):1294–1303. doi:10.1007/s10826-023-02544-w
19. Yang S, Zhou Z, Miao H, Zhang Y. Effect of weight loss on blood pressure changes in overweight patients: a systematic review and meta-analysis. J Clin Hypertens. 2023;25(5):404–415. doi:10.1111/jch.14661
20. Shamsi SA, Salehzadeh M, Ghavami H, Asl RG, Vatani KK. Impact of lifestyle interventions on reducing dietary sodium intake and blood pressure in patients with hypertension: a randomized controlled trial. Turk Kardiyol Dern Ars. 2021;49(2):143–150. doi:10.5543/tkda.2021.81669
21. Bell ML, Kenward MG, Fairclough DL, Horton NJ. Differential dropout and bias in randomised controlled trials: when it matters and when it may not. BMJ. 2013;346(jan21 1):e8668–e8668. doi:10.1136/bmj.e8668
22. Dettori J. Loss to follow-up. Evid Base Spine Care J. 2011;2(1):7–10. doi:10.1055/s-0030-1267080
23. Schapira MM, Fletcher KE, Hayes A, et al. The development and validation of the hypertension evaluation of lifestyle and management knowledge scale. J Clin Hypertens. 2012;14(7):461–466. doi:10.1111/j.1751-7176.2012.00619.x
24. Cabral AC, Moura-Ramos M, Castel-Branco M, Caramona M, Fernandez-Llimos F, Figueiredo IV. Cross-cultural adaptation of hypertension knowledge test into European Portuguese. Braz J Pharm Sci. 2018;53(4). doi:10.1590/s2175-97902017000400245
25. d M. Pengaruh Gaya Hidup Terhadap Penyakit Hipertensi Berdasarkan Teori TPB (Theory of Planned Behavior). J Pharmaceut Care Sci. 2022;2(2):30–38.
26. Traina SB, Mathias SD, Colwell HH, Crosby RD, Abraham C. The diabetes intention, attitude, and behavior questionnaire: evaluation of a brief questionnaire to measure physical activity, dietary control, maintenance of a healthy weight, and psychological antecedents. Patient Prefer Adherence. 2016;10:213–222. doi:10.2147/PPA.S94878
27. Gheshlagh RG, Parizad N, Ghalenoee M, et al. Psychometric features of the persian version of self-efficacy tool for patients with hypertension. Int Cardiovasc Res J. 2018;12(2):50–56.
28. Han HR, Lee H, Commodore-Mensah Y, Kim M. Development and validation of the hypertension self-care profile: a practical tool to measure hypertension self-care. J Cardiovasc Nurs. 2014;29(3):E11–20. doi:10.1097/JCN.0b013e3182a3fd46
29. Upoyo AS, Taufik A, Anam A, et al. Translation and validation of the indonesian version of the hypertension self-care profile. Open Access Maced J Med Sci. 2021;9(E):980–984. doi:10.3889/oamjms.2021.7119
30. Okawa Y, Mitsuhashi T, Tsuda T. The Asia-Pacific body mass index classification and new-onset chronic kidney disease in non-diabetic Japanese adults: a community-based longitudinal study from 1998 to 2023. Biomedicines. 2025;13(2). doi:10.3390/biomedicines13020373
31. Khalesi S, Williams E, Irwin C, et al. Reducing salt intake: a systematic review and meta-analysis of behavior change interventions in adults. Nutr Rev. 2022;80(4):723–740. doi:10.1093/nutrit/nuab110
32. Moghaddam FG, Hoseinzadeh-Chahkandak F, Salmani F, Norozi E. Effect of educational intervention based on the theory of planned behavior (TPB) on amount of salt intake in pregnant women with PreHypertension. BMC Womens Health. 2024;24(1):548. doi:10.1186/s12905-024-03385-5
33. Irwan AM, Potempa K, Abikusno N, Syahrul S. Health coaching intervention to improve self-care management of hypertension among older people in indonesia: a randomized controlled study protocol. J Multidiscip Healthc. 2024;17:2799–2808. doi:10.2147/JMDH.S461166
34. Bandura A. On the functional properties of perceived self-efficacy revisited. J Manage. 2012;38(1):9–44. doi:10.1177/0149206311410606
35. Kang AW, Pearlstein TB, Sharkey KM. Changes in quality of life and sleep across the perinatal period in women with mood disorders. Qual Life Res. 2020;29(7):1767–1774. doi:10.1007/s11136-020-02437-1
36. Kelly MP, Barker M. Why is changing health-related behaviour so difficult? Public Health. 2016;136:109–116. doi:10.1016/j.puhe.2016.03.030
37. Eslamimehr F, Hosseini Z, Aghamolaei T, Nikparvar M, Ghanbarnezhad A. Self-Care behaviors in patients with hypertension to prevent hypertensive emergencies: a qualitative study based on the theory of planned behavior. J Cardiovasc Emerg. 2022;8(4):75–85. doi:10.2478/jce-2022-0016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.