Back to Journals » Clinical Ophthalmology » Volume 20
Effectiveness and Safety of Combined Ab-Interno Canaloplasty and Microstent Implantation in Severe Glaucoma – A Retrospective Study
Authors Spaulding J
Received 14 November 2025
Accepted for publication 21 January 2026
Published 28 January 2026 Volume 2026:20 576540
DOI https://doi.org/10.2147/OPTH.S576540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Justin Spaulding
Cataract & Laser Institute of Southern Oregon, Medford, OR, USA
Correspondence: Justin Spaulding, Cataract & Laser Institute of Southern Oregon, 1408 E Barnett Road, Medford, OR, 97504, USA, Tel +1 541 779 2020, Email [email protected]
Purpose: To evaluate the efficacy and safety of ab-interno canaloplasty combined with microstent implantation in patients with severe glaucoma.
Patients and Methods: This retrospective study included patients with severe glaucoma (mean age 74.6± 8.7 years), predominantly primary open-angle (90%). All eyes underwent combined ab-interno canaloplasty using the iTrack (Nova Eye Medical) with concurrent Hydrus Microstent (Alcon) implantation during cataract surgery. The primary outcome measures were intraocular pressure (IOP), number of glaucoma medications, visual field mean deviation (VFMD), postoperative complications.
Results: Sixty-nine eyes of 56 patients were followed for mean 27.9± 13.8 months. Mean IOP decreased from 17.8± 6.3 at baseline to 15.5± 4.7 mmHg at last follow-up (p=0.012), and mean number of medications decreased by 47%, from 2.10± 1.1 to 1.12± 1.2 (p< 0.001). Medication-free eyes increased from 7% at baseline to 43% at last follow-up. Among eyes that were on 3 and 4 medications preoperatively (n=17; n=7), the number of medications significantly decreased by 53% (p< 0.001) and 57% (p=0.002) at last follow-up, while IOP remained stable. Eyes with baseline IOP > 18 mmHg (n=21) experienced a significant mean IOP reduction of 9.8 mmHg (from 24.8± 6.7 to 15.0± 4.6 mmHg; − 40%, p< 0.001). No intraoperative or postoperative complications were reported; 6 eyes (9%) required additional glaucoma procedures during follow-up.
Conclusion: Combining ab-interno canaloplasty with Hydrus Microstent implantation during cataract surgery resulted in modest but sustained reductions in intraocular pressure and glaucoma medication burden, with a favorable safety profile. However, postoperative IOP frequently remained above levels required for very low target pressures. These findings suggest that this mixed MIGS approach may be considered in carefully selected patients but should not be viewed as a substitute for traditional filtering surgery in advanced disease.
Keywords: primary open-angle glaucoma, minimally invasive glaucoma surgery, MIGS canaloplasty, Hydrus Microstent, combined MIGS, IOP reduction
Introduction
Glaucoma remains the leading cause of irreversible blindness worldwide, and elevated intraocular pressure (IOP) is the only proven modifiable risk factor.1,2 In patients with severe glaucoma, IOP control is particularly critical to prevent further visual field deterioration. Topical hypotensive agents often prove insufficient in advanced disease and is limited by ocular surface toxicity, adherence challenges, and diminishing long-term efficacy.3,4 At the other end of the treatment spectrum, filtering surgeries such as trabeculectomy and tube shunts offer significant IOP reduction but carry substantial risks, including hypotony, bleb-related infections, and long-term complications that impact quality of life.5–7 Non-perforating techniques such as deep sclerectomy offer a lower complication profile but may provide less consistent pressure reduction in eyes requiring very low target IOPs.8,9
Minimally invasive glaucoma surgery (MIGS) has emerged as a conjunctiva-sparing, ab-interno alternative with a favorable safety profile, though its IOP-lowering efficacy has traditionally limited its use to mild-to-moderate open-angle glaucoma (OAG).10,11 Increasing interest has therefore focused on combining MIGS procedures with complementary mechanisms to enhance pressure reduction and potentially extend their applicability to more advanced disease.12–15
Ab-interno canaloplasty and microstent implantation represent two MIGS approaches targeting different points along the conventional outflow pathway. Ab-interno canaloplasty achieves circumferential viscodilation of Schlemm’s canal and distal collector channels without leaving an implant, while microstents provide sustained trabecular bypass and segmental canal scaffolding.16–20
We hypothesize that combining these two procedures may address both proximal and distal outflow resistance: canaloplasty reactivates the conventional outflow pathway by mechanically dilating Schlemm’s canal and accessing distal collector channels—structures often collapsed in chronic glaucoma—while the microstent provides a sustained bypass across the trabecular meshwork and supports proximal flow for a prolonged period of time.
This study focuses on eyes with severe glaucoma, a cohort typically considered for traditional filtration procedures. We aim to evaluate the safety and effectiveness of mixed MIGS—specifically, the combination of iTrack ab-interno canaloplasty (Nova Eye Medical, Fremont, USA) and Hydrus Microstent implantation (Alcon, Geneva, Switzerland)—performed during cataract surgery in this high-risk population.
Patients and Methods
This was a retrospective, single-center study evaluating the outcomes of combined ab-interno canaloplasty using the iTrack microcatheter and Hydrus Microstent implantation performed in conjunction with phacoemulsification in patients with severe glaucoma. This retrospective study meets the criteria for exemption from IRB review under the US Code of Federal Regulations, (46.104;d4), as the research and the analysis of the data involved only secondary use of fully de-identified data collected during routine clinical care. The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Medical records were reviewed for all patients who underwent the combined procedure between 2018 and 2023 at the Cataract & Laser Institute of Southern Oregon, USA. Eligible patients were adults (≥18 years) diagnosed with severe open-angle glaucoma, classified based on visual field mean deviation (VFMD) and documented optic nerve damage on OCT, with gonioscopy records confirming an open anterior chamber angle. Eyes with a history of incisional glaucoma surgery within the previous six months, significant angle abnormalities, or uveitis were excluded.
Surgical Devices
The iTrack microcatheter is designed for 360° catheterization of Schlemm’s canal through a single intubation and dilation of the canal via pressurized delivery of OVD. It is equipped with an illuminated distal tip to aid visualization during surgery, ensuring accurate placement within the canal. The microcatheter allows for the pressurized delivery of over 100 µL of ophthalmic viscosurgical devices (OVD), a process known as pressurized viscodilation, enabling surgeons to titrate the volume as needed to achieve effective canal dilation. Building upon this platform, the second device generation, the iTrack Advance, received FDA clearance in 2023: the updated device incorporates a cannula and a handheld injector, eliminating the need for microforceps.
The Hydrus Microstent is a biocompatible, ab-interno microstent engineered to enhance conventional aqueous outflow by scaffolding Schlemm’s canal. Constructed from flexible nitinol, it features a curved, open-channel design with multiple side windows and anchoring spines, enabling secure placement and dilation of approximately 90 degrees of the canal. This structure facilitates sustained canal patency and improved access to distal collector channels.
Surgical Technique
All procedures were performed by a single experienced surgeon (JS) under standard operating room conditions. Following an uncomplicated clear corneal phacoemulsification and intraocular lens implantation, ab-interno canaloplasty was performed. After a small goniotomy was created at the nasal angle, the microcatheter was introduced into Schlemm’s canal and advanced 360 degrees. Viscodilation was performed by injecting high-molecular-weight ophthalmic viscosurgical devices (OVD) during catheter withdrawal; quantity was titrated at surgeon’s discretion. Subsequently, the Hydrus Microstent was implanted into Schlemm’s canal through the same goniotomy, spanning approximately 90 degrees of the canal.
Postoperatively, patients were prescribed topical antibiotics for the first week. Non-steroidal anti-inflammatory drugs (NSAIDs) and prednisolone acetate 1% were administered four times daily (QID) during the first week, followed by a tapering regimen: twice daily (BID) for two weeks, once daily (QD) for one week, and then discontinued.
All glaucoma medications were discontinued on the day of surgery, with no washout period prior to the procedure.
Data Collection
Preoperative data collected included patient demographics, number and type of preoperative glaucoma medications, distance-corrected visual acuity (CDVA), baseline IOP measured by Goldmann applanation tonometry, visual fields, preoperative surgeries, average retinal nerve fiber layer thickness (OCT RNFL) and VFMD. Glaucoma severity was classified as mild, moderate, or severe based on VFMD thresholds, according to the criteria by Hodapp et al endorsed by the European Glaucoma Society: mild (VFMD ≥ –6 dB), moderate (–6 dB to –12 dB), and severe (≤ –12 dB).21 OCT imaging was used as a supportive structural assessment but was not used to define disease severity.
Postoperative outcomes were assessed at multiple timepoints, specifically at 12, 24, 36 and 48 months following surgery. These included IOP, number of glaucoma medications, CDVA, VFMD and the occurrence of intraoperative or postoperative complications.
The primary efficacy endpoints included the mean change in IOP and glaucoma medications from baseline to postoperative follow-ups. Safety endpoints included the incidence of adverse events such as transient hyphema, corneal edema, device-related complications, or the need for additional glaucoma surgery.
Statistical Analysis
Descriptive statistics were used to summarize baseline characteristics. Changes in IOP, number of glaucoma medications, and VFMD at postoperative timepoints were analyzed using a mixed-effects model to account for inter-eye correlation.22 Subgroup comparisons such as those by glaucoma severity, prior glaucoma surgery, preoperative VFMD, OVD type, and OVD volume were assessed using the Mann–Whitney U-test when comparing two independent groups or Welch’s analysis of variance (ANOVA) when comparing more than two groups. Statistical significance was defined as a p-value <0.05 (no p values for groups of less than 5 eyes). Data were analyzed using SPSS version 28 (IBM, Armonk, NY, USA).
Results
A total of 69 eyes with severe glaucoma from 56 patients were included in this analysis. The mean patient age was 74.6±8.7 years, and 61% (n=34) were male. The majority of patients were Caucasian (89%, n=50), followed by Hispanic (7%, n=4), Asian (2%, n=1), and one patient (2%) who declined to specify. All eyes were phakic preoperatively and underwent combined surgery with phacoemulsification; no standalone MIGS procedures were performed. Primary open-angle glaucoma (POAG) was the most frequent diagnosis (90%, n=62), with pigmentary (3%, n=2), narrow-angle glaucoma (1%, n=1), and other types (6%, n=4) less common. The mean preoperative IOP was 17.8±6.3 mmHg on 2.10±1.1 medications. The average VFMD was −12.8±7.9 dB, and mean RNFL thickness was 58.6±8.9 µm. Mean follow-up duration was 27.9±13.8 months. Demographic data are summarized in Table 1.
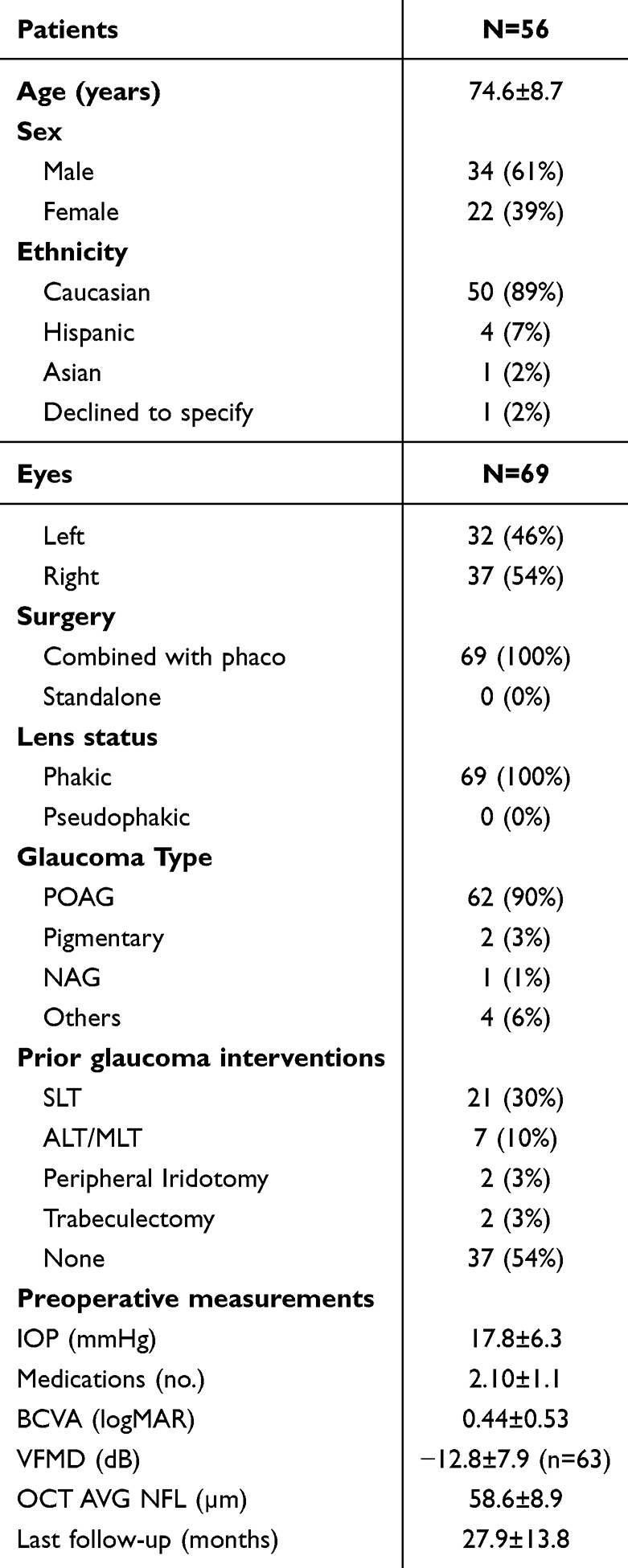 |
Table 1 Demographics and Preoperative Measurements |
At last follow-up, mean IOP significantly decreased by 13% from 17.8±6.3 mmHg to 15.5±4.7 mmHg (p=0.012), and mean medication burden reduced by 47% from 2.10±1.1 to 1.12±1.2 (p<0.001). These reductions were sustained across multiple timepoints up to 48 months (Figure 1, Table 2).
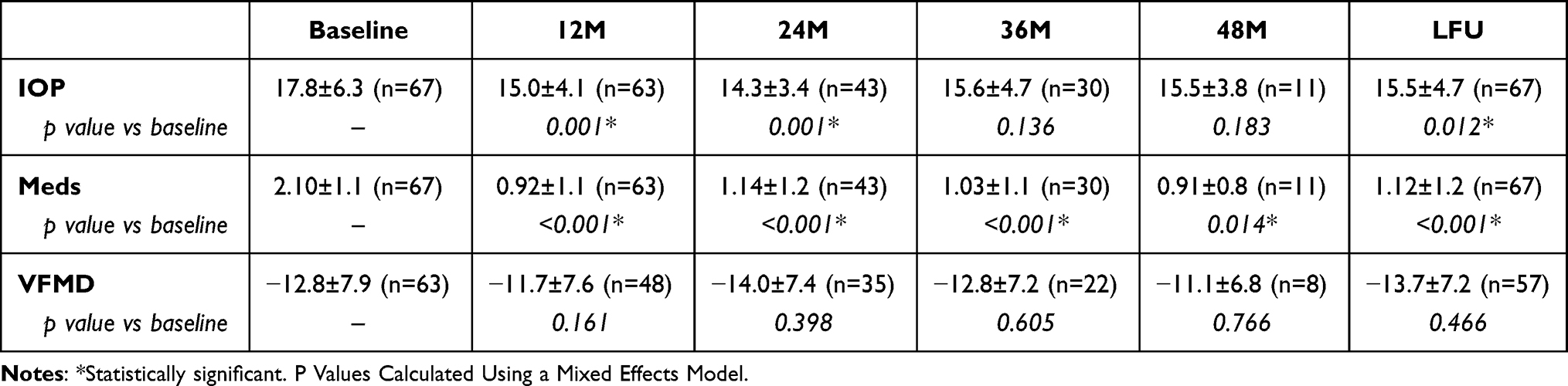 |
Table 2 Outcomes of IOP, Medications and VFMD at Baseline and Postop Timepoints |
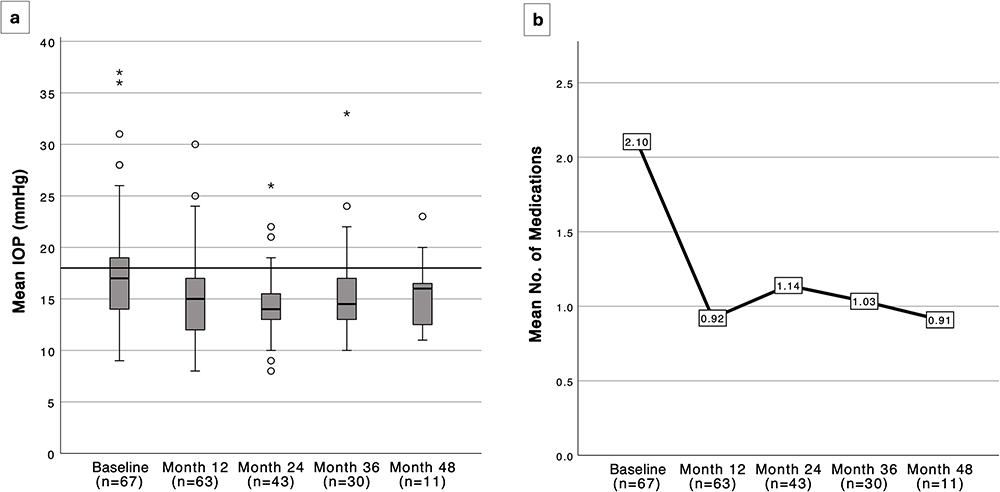 |
Figure 1 Outcomes at baseline and all postop timepoints: (a) box plot of IOP (mmHg); (b) line graph of number of medications. IOP=intraocular pressure. Circles (○) indicate outliers, defined as values between 1.5 and 3 times the interquartile range beyond the quartiles; asterisks (*) indicate extreme outliers. |
The proportion of eyes achieving medication-free status increased from 7% at baseline (5/69) to 43% (30/69) at last follow-up. Among eyes that were using 3 glaucoma medications preoperatively (n=17), the mean number of medications was reduced to 1.41±1.42 at last follow-up, representing a 53% reduction (p<0.001). Among eyes on 4 preoperative medications (n=7), the mean number of medications was reduced to 1.71±1.50, corresponding to a 57% reduction (p=0.002). In both groups, mean IOP remained stable (p>0.05) and below 18 mmHg (Table 3).
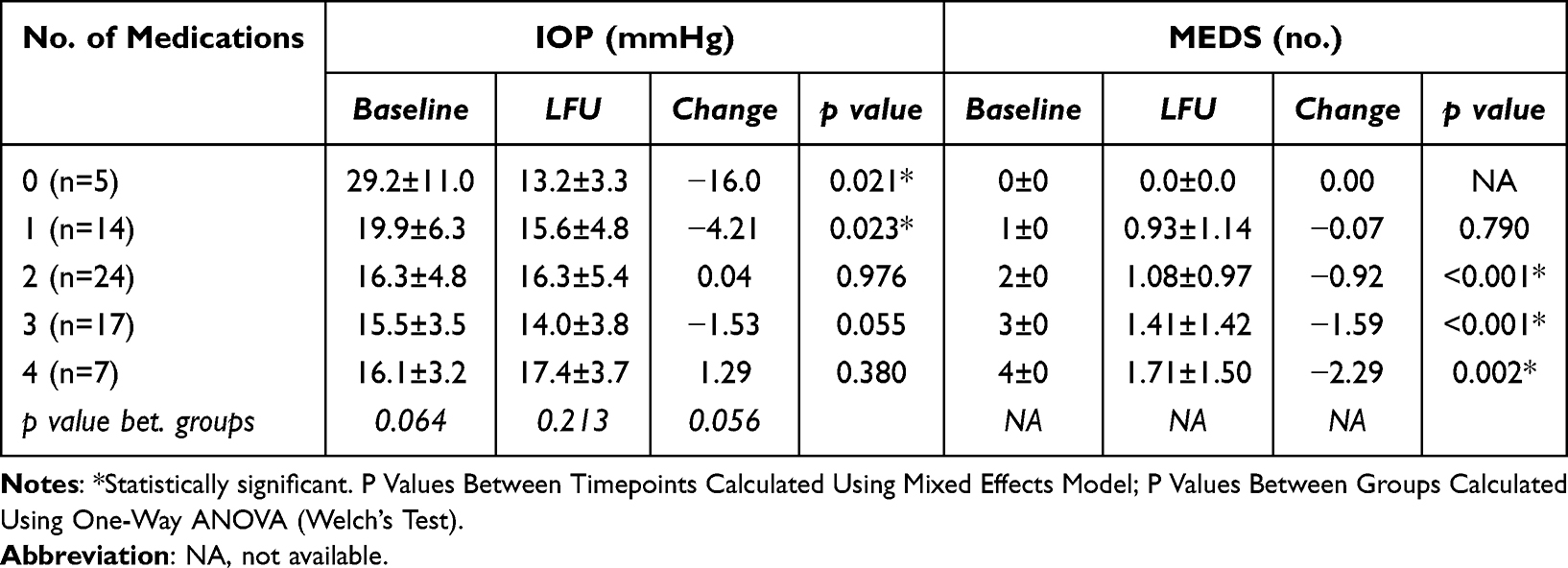 |
Table 3 Outcomes of IOP and Medications by Preop Number of Medications |
No significant change was observed in VFMD from baseline to last follow-up (−12.8±7.9 dB vs −13.7±7.2 dB; p=0.466).
Subgroup Analysis
Subgroup analyses confirmed consistent reductions in IOP and medications across different OVD volumes, baseline IOP and prior glaucoma interventions. Although prior glaucoma interventions in the cohort included laser procedures and trabeculectomy (Table 1), subgroup analyses were limited to eyes with prior laser treatment, as the number of eyes with prior trabeculectomy was insufficient for meaningful comparison. In eyes without prior laser glaucoma procedure (n=37), IOP was significantly reduced by 21% from 18.9±6.8 to 14.9±4.1 mmHg (p=0.003), while medication use declined from 1.84±1.2 to 0.97±1.2 (p<0.001). Among those with prior laser glaucoma procedure (n=28), IOP remained stable (16.4±5.6 to 16.0±5.4 mmHg; p=0.759), while medications decreased from 2.43±0.84 to 1.32±1.28 (p<0.001) (Table 4).
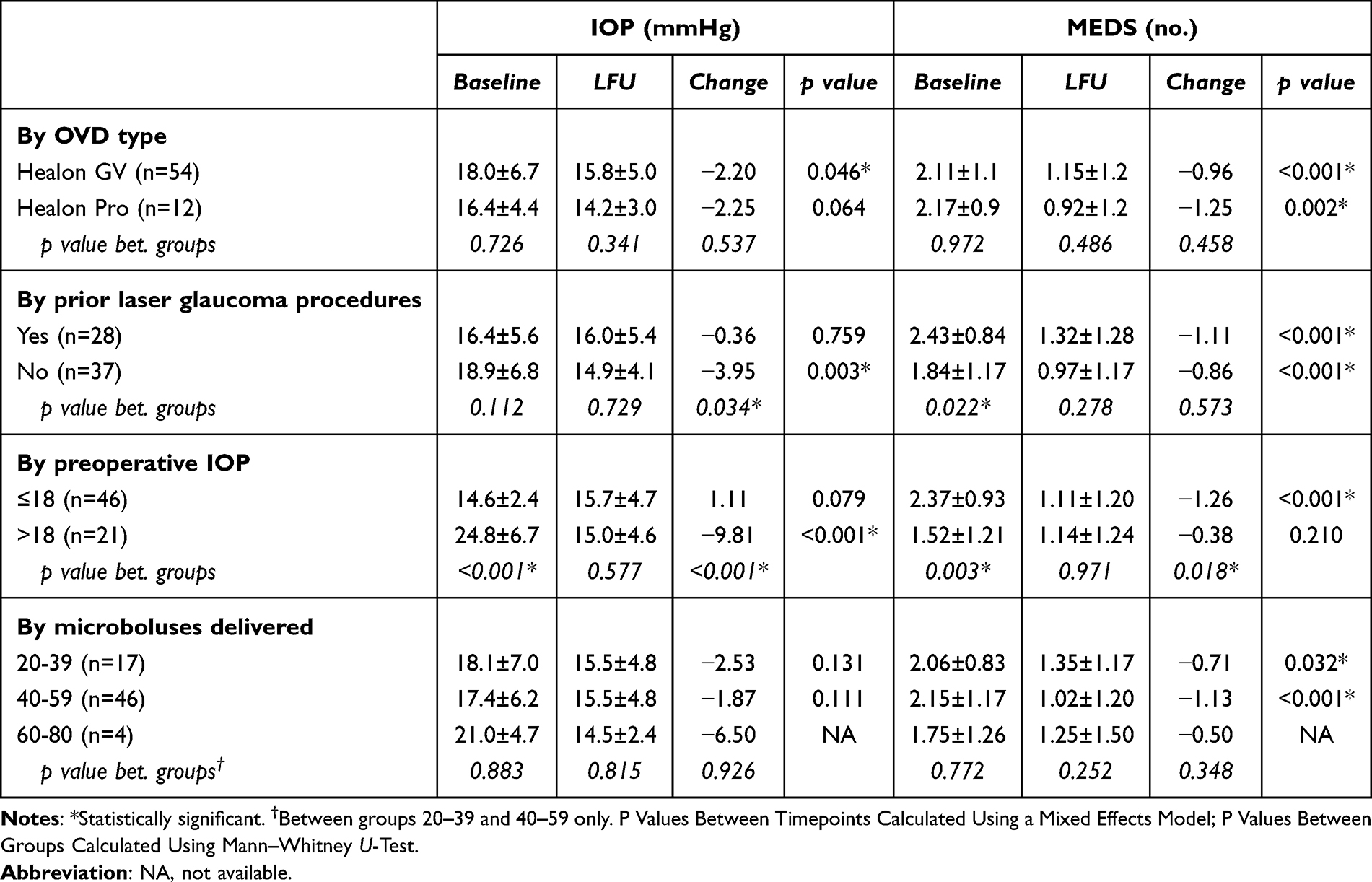 |
Table 4 Outcomes of IOP and Medications at Baseline and Last Follow-Up (LFU; Mean 27.9±13.8 Mos.) Split by Group |
When stratified by preoperative IOP, eyes with baseline IOP >18 mmHg (n=21) experienced a significant mean IOP reduction of 9.8 mmHg (from 24.8±6.7 to 15.0±4.6 mmHg; −40%, p<0.001). In contrast, in eyes with baseline IOP ≤18 mmHg (n=46), IOP remained stable while a significant 53% reduction in medication burden (from 2.37±0.93 to 1.11±1.20; p<0.001) was observed.
The mean OVD volume delivered was 45.0±9.5 microboluses, which equals to a mean volume of 112.5 μL. Full 360° catheterization of Schlemm’s canal was achieved in 84% of eyes (n=58), with partial canalization (181–270°) in 14% and 91–180° in 1% of cases. Outcomes were also analyzed based on the volume of ophthalmic viscosurgical devices (OVD) delivered, measured in microboluses (Table 4).
Safety Profile
The mixed MIGS procedure demonstrated a favorable safety profile. No intraoperative or immediate postoperative complications were reported. During the follow-up period, 6 of 69 eyes (9%) required further glaucoma procedures: 2 eyes (3%) underwent cyclophotocoagulation, 3 eyes (4%) underwent trabeculectomy, and 1 eye (1%) received a XEN gel stent. The remaining 63 eyes (91%) did not require any additional surgical intervention (Figure 2). Clinical data collected after any subsequent glaucoma surgery were excluded from the efficacy analysis.
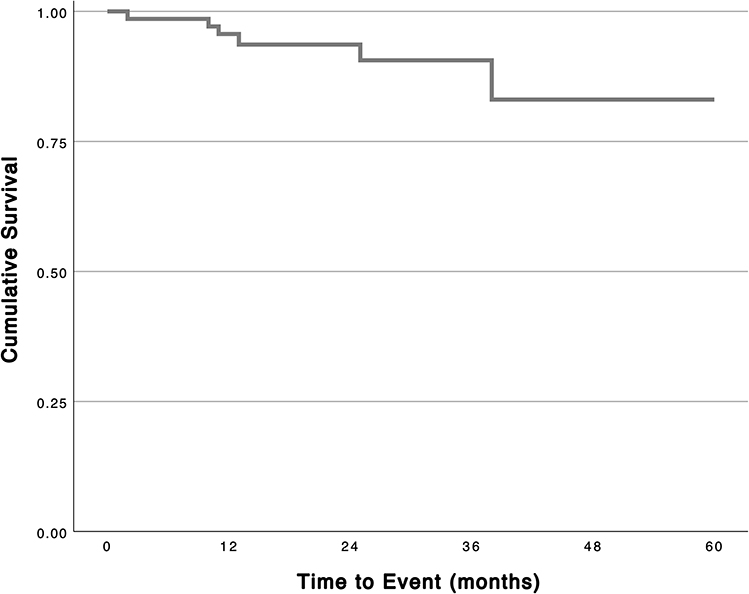 |
Figure 2 Kaplan-Meier survival analysis of all eyes (n=69); event defined as eye undergoing additional glaucoma surgery (n=6, 9%). |
Discussion
This retrospective study demonstrates that combining ab-interno canaloplasty using the iTrack microcatheter and Hydrus Microstent implantation at the time of cataract surgery can achieve sustained reductions in IOP and glaucoma medication use in eyes with severe glaucoma-a population traditionally considered for filtering surgery. By targeting multiple levels of aqueous outflow resistance, this mixed MIGS approach may offer a conjunctiva-sparing surgical option for selected patients. Accordingly, this strategy should not be viewed as a substitute for traditional filtering surgery in advanced disease, but rather as a potential alternative in carefully selected cases where conjunctiva preservation or reduced surgical risk is desirable.
In this cohort of eyes with severe glaucoma, medication burden decreased by 47%, from 2.10±1.1 to 1.12±1.2 (p<0.001), with nearly half of eyes (46%) on three or more medications preoperatively. These reductions were consistent across postoperative timepoints up to four years. Although no statistically significant change in VFMD was observed during follow-up, small changes in VFMD may still be clinically meaningful in advanced glaucoma, and VFMD alone has limited sensitivity for detecting progression in this disease stage. Accordingly, while no significant functional decline was detected, these results should be interpreted with caution and do not exclude the possibility of subtle visual field progression.
There is a growing body of evidence from various clinical studies that have demonstrated the safety and efficacy of iTrack canaloplasty in achieving sustained IOP reduction and decreased reliance on topical medications.23–29 Similarly, numerous studies have confirmed the safety and efficacy of the Hydrus Microstent in lowering IOP and reducing medication burden in patients with mild to moderate primary open-angle glaucoma.30–34
By combining ab-interno canaloplasty and Hydrus implantation, this mixed MIGS approach leverages distinct but complementary mechanisms targeting both proximal and distal components of the conventional outflow pathway. Ab-interno canaloplasty achieves 360-degree viscodilation of Schlemm’s canal, restoring outflow through the trabecular meshwork, canal wall, and distal collector channels via mechanical expansion. The Hydrus Microstent provides a permanent scaffold within Schlemm’s canal, bypassing the trabecular meshwork and maintaining patency over approximately 90 degrees. While ab-interno canaloplasty initiates immediate enhancement of outflow facility, the presence of a permanent stent may help sustain this benefit over time by preventing canal collapse or reclosure, thereby potentially prolonging the effect of canaloplasty. In severe glaucoma, where Schlemm’s canal may be narrowed, collapsed, or fibrotic due to chronic pressure elevation and structural remodeling, the addition of a permanent scaffold may be particularly advantageous.
Emerging evidence suggests that combining ab-interno canaloplasty with Hydrus Microstent implantation may offer enhanced IOP reduction and medication burden relief compared to either procedure alone.31,35–39 In a retrospective analysis, Porter et al reported favorable long-term outcomes with the same MIGS combination across a variety of glaucoma stages (iTrack canaloplasty and Hydrus), showing a sustained IOP reduction from 19.1±4.0 mmHg to 14.4±3.2 mmHg at 36 months (p<0.001), particularly in eyes with higher IOP (above 18 mmHg), where IOP declined from 21.9±3.1 mmHg to 14.6±4.2 mmHg (p=0.006). Although medication reduction at 36 months was not statistically significant, no eyes required additional glaucoma surgery, underscoring the durability and safety of the mixed MIGS procedure.39 Similarly, Dickinson et al, in a cohort of mild-to-moderate primary open-angle glaucoma patients, demonstrated enhanced outcomes at 6 months with OMNI canaloplasty plus Hydrus compared to Hydrus alone, with greater IOP reduction (13.6±3.1 mmHg −17% vs 14.1±3.5 mmHg - 13%) and a higher proportion of patients off medications (87.3% vs 64.3%).31
However, not all studies have demonstrated a significant advantage for the mixed MIGS approach. In an ARVO 2024 matched-cohort analysis of 164 eyes, the Hydrus/OMNI canaloplasty group achieved a smaller, non-significant IOP reduction to 14.9±4.1 (−3.8%) postoperatively compared to 14.6±3.4 mmHg (−7.5%) postoperatively in the Hydrus-alone group at one year, although the combined group showed greater medication reduction (63.0% vs 53.6%) and a higher proportion of medication-free eyes (69.0% vs 56.3%).35 Similarly, early data from a single-surgeon ARVO 2023 study found no significant IOP difference at one month between Hydrus alone and Hydrus with OMNI (15.4 vs 14.7 mmHg, p=0.512), despite greater reduction in medication burden in the mixed MIGS group.36 The OMNI system delivers a fixed volume of OVD (11 μL), whereas the iTrack system allows titration of the OVD volume based on intraoperative assessment, often exceeding 100 μL. This technique, known as pressurized viscodilation of Schlemm’s canal, may influence procedural efficacy and clinical outcomes. This mechanistic distinction could confer greater efficacy, particularly in eyes with more distal outflow resistance. However, these mixed findings underscore that the success of mixed MIGS approaches may depend on surgical technique, choice of devices, baseline disease severity, and follow-up duration. Further prospective trials are warranted to clarify the long-term benefits and optimal patient selection for dual MIGS strategies.
Subgroup analyses (Table 4) demonstrated that significant IOP and medication reductions were achieved regardless of OVD type or history of prior laser glaucoma procedures. Eyes with higher IOP seemed to receive more OVD and result in larger IOP reduction, but the cohort was not sufficiently powered to detect statistically significant differences. While the overall IOP reduction observed in the cohort was modest, this likely reflects the relatively low preoperative IOP (mean 17.8 mmHg). Notably, eyes with higher baseline IOP (>18 mmHg) exhibited a more substantial reduction, averaging nearly 10 mmHg (−40%, p<0.001), underscoring the potential effectiveness of the mixed MIGS approach in cases of uncontrolled IOP.
These findings suggest that, in selected cases, combining complementary MIGS procedures may extend the applicability of MIGS beyond mild-to-moderate glaucoma as a conjunctiva-sparing alternative to filtration surgery.
Importantly, the mixed MIGS procedure maintained a favorable safety profile: no intraoperative or early postoperative complications were observed, and the need for additional glaucoma surgeries was relatively low (9% overall).
This study provides mid-to long-term observational data on the safety and outcomes of combined ab-interno canaloplasty and Hydrus Microstent implantation. However, several limitations should be acknowledged. The retrospective, single-center design and absence of a control group limit direct comparison with other surgical approaches. Although mean follow-up exceeded two years, follow-up duration was variable, with relatively few eyes reaching longer-term time points, restricting conclusions regarding durability.
The magnitude of IOP reduction was modest, postoperative IOP frequently remained above 15 mmHg, and the hypotensive effect of concomitant cataract surgery may have influenced outcomes. These factors limit applicability in eyes requiring very low target IOPs.
The use of two MIGS devices raises cost considerations that were not assessed in this study, and alternative procedures such as deep sclerectomy may provide greater IOP reduction at lower cost in selected patients. Furthermore, the predominantly Caucasian study population may limit generalizability to more diverse populations, given known differences in angle anatomy and aqueous outflow characteristics. Future prospective, comparative studies with standardized follow-up and formal cost-effectiveness analyses are needed to better define the role of this combined approach.
Conclusion
The combination of ab-interno canaloplasty and Hydrus Microstent implantation during cataract surgery was associated with moderate and sustained reductions in intraocular pressure and medication burden over mid- to long-term follow-up. This mixed MIGS strategy may represent a conjunctiva-sparing option in carefully selected eyes, including some with more advanced disease, but should not be considered a substitute for traditional filtering or non-perforating surgery in cases requiring substantial IOP lowering. Larger prospective studies with comparator groups are needed to better define its relative efficacy, durability, and cost-effectiveness.
Abbreviations
ALT, Argon laser trabeculoplasty; BCVA, best-corrected visual acuity; IOP, intraocular pressure; LFU, last follow-up; MLT, Micropulse laser trabeculoplasty; OCT AVG NFL, optical coherence tomography average nerve fiber layer; OVD, ophthalmic viscosurgical devices; SLT, selective laser trabeculoplasty; VFMD, visual field mean deviation.
Acknowledgments
Writing and editorial support were provided by GP Communications, funded by Nova Eye Medical.
Disclosure
Dr Spaulding is a consultant to Nova Eye Medical, Iantrek, Alcon and BnL. All clinical decisions and outcome assessments were performed according to standard clinical practice and predefined criteria, independent of any commercial influence. The author reports no other conflicts of interest in this work.
References
1. Tham Y-C, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology. 2014;121:2081–10. doi:10.1016/j.ophtha.2014.05.013
2. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma. JAMA. 2014;311:1901. doi:10.1001/jama.2014.3192
3. Wang T, Cao L, Jiang Q, et al. Topical medication therapy for glaucoma and ocular hypertension. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.749858
4. Arbabi A, Bao X, Shalaby WS, et al. Systemic side effects of glaucoma medications. Clin Exp Optom. 2022;105:157–165. doi:10.1080/08164622.2021.1964331
5. Khaw PT, Chiang M, Henein C, et al. Glaucoma filtration surgery: indications, techniques, and complications. In: Albert and Jakobiec’s Principles and Practice of Ophthalmology. Cham: Springer International Publishing; 2020:1–38.
6. Gedde SJ, Schiffman JC, Feuer WJ, et al. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153:789–803.e2. doi:10.1016/j.ajo.2011.10.026
7. Stringa F, Kastner A, Heuer D, et al. Postoperative complications in glaucoma surgery: literature review-based recommendations to improve reporting consistency. Br J Ophthalmol. 2022;106:1696–1702. doi:10.1136/bjophthalmol-2021-318952
8. Abdelrahman AM. Nonpenetrating deep sclerectomy: challenges, innovations, and current evidence. Oman J Ophthalmol. 2025;18:267–274. doi:10.4103/ojo.ojo_389_24
9. Gabai A, Cimarosti R, Battistella C, et al. Efficacy and safety of trabeculectomy versus nonpenetrating surgeries in open-angle glaucoma: a meta-analysis. J Glaucoma. 2019;28:823–833. doi:10.1097/IJG.0000000000001323
10. Song Y, Zhang H, Zhang Y, et al. Minimally invasive glaucoma surgery in primary angle-closure glaucoma. Asia-Pac J Ophthalmol. 2022;11:460–469. doi:10.1097/APO.0000000000000561
11. Bicket AK, Le JT, Azuara-Blanco A, et al. Minimally invasive glaucoma surgical techniques for open-angle glaucoma. JAMA Ophthalmol. 2021;139:983. doi:10.1001/jamaophthalmol.2021.2351
12. Yang S-A, Mitchell W, Hall N, et al. Trends and usage patterns of minimally invasive glaucoma surgery in the United States. Ophthalmol Glaucoma. 2021;4:558–568. doi:10.1016/j.ogla.2021.03.012
13. Mai DD, Ingram Z, Oberfeld B, et al. Combined microinvasive glaucoma surgery – a review of the literature and future directions. Semin Ophthalmol. 2023;38:529–536. doi:10.1080/08820538.2023.2181665
14. Ferguson TJ, Swan R, Sudhagoni R, et al. Microbypass stent implantation with cataract extraction and endocyclophotocoagulation versus microbypass stent with cataract extraction for glaucoma. J Cataract Refract Surg. 2017;43:377–382. doi:10.1016/j.jcrs.2016.12.020
15. Myers JS, Masood I, Hornbeak DM, et al. Prospective evaluation of Two iStent® Trabecular Stents, One iStent Supra® Suprachoroidal Stent, and postoperative prostaglandin in refractory glaucoma: 4-year outcomes. Adv Ther. 2018;35:395–407. doi:10.1007/s12325-018-0666-4
16. Cagini C, Peruzzi C, Fiore T, et al. Canaloplasty: current value in the management of glaucoma. J Ophthalmol. 2016;2016:1–6. doi:10.1155/2016/7080475
17. Khaimi MA. Canaloplasty: a minimally invasive and maximally effective glaucoma treatment. J Ophthalmol. 2015;2015:1–5. doi:10.1155/2015/485065
18. Khaimi M. Ab Interno Canaloplasty. Glaucoma Today. 2015;13–15.
19. Ahmed IIK, Rhee DJ, Jones J, et al. Three-year findings of the HORIZON trial. Ophthalmology. 2021;128:857–865. doi:10.1016/j.ophtha.2020.11.004
20. Shareef S, Fea A, Ahmed IIK. The Hydrus Micro-stent. In: Surgical Innovations in Glaucoma. New York: Springer New York; 2014:171–174.
21. Hodapp E, Parrish RK, Anderson DDR. Clinical Decisions in Glaucoma. St Louis: The CV Mosby Co; 1993.
22. Ying G, Maguire MG, Glynn R, et al. Tutorial on biostatistics: statistical analysis for correlated binary eye data. Ophthalmic Epidemiol. 2018;25:1–12. doi:10.1080/09286586.2017.1320413
23. Khaimi M. Ab-Interno canaloplasty standalone versus combined with Cataract Surgery – 36-month outcomes in 1000+ eyes. In: American Society of Cataract and Refractive Surgery (ASCRS). Washington, D.C; 2022.
24. Khaimi MA. Long-term medication reduction in controlled glaucoma with iTrack ab-interno canaloplasty as a standalone procedure and combined with cataract surgery. Ther Adv Ophthalmol. 2021;13:251584142110457.
25. Koerber N, Ondrejka S. 6-year efficacy and safety of iTrack Ab-interno canaloplasty as a stand-alone procedure and combined with cataract surgery in primary open angle and pseudoexfoliative glaucoma. J Glaucoma. 2024;33:176–182. doi:10.1097/IJG.0000000000002311
26. Koerber NJ. 5-year efficacy and safety of iTrack Ab-interno canaloplasty as a standalone procedure and combined with cataract surgery in primary open-angle glaucoma. Eur Soc Cataract Refract Surgeons. 2021.
27. Koerber N, Ondrejka S. Four-year efficacy and safety of iTrack Ab-interno canaloplasty as a standalone procedure and combined with cataract surgery in open-angle glaucoma. Klin Monbl Augenheilkd. 2023;240:1394–1404. doi:10.1055/a-1737-4149
28. Gallardo MJ. 36-month effectiveness of Ab-interno canaloplasty standalone versus combined with cataract surgery for the treatment of open-angle glaucoma. Ophthalmol Glaucoma. 2022;5:476–482. doi:10.1016/j.ogla.2022.02.007
29. Patel S, Reiss G. Long‐term clinical and safety outcomes of canaloplasty performed across all grades of glaucoma severity. J Ophthalmol. 2023;2023:1–8.
30. Salimi A, Kassem R, Santhakumaran S, et al. Three-year outcomes of a Schlemm Canal Microstent (Hydrus Microstent) with concomitant phacoemulsification in open-angle glaucoma. Ophthalmol Glaucoma. 2023;6:137–146. doi:10.1016/j.ogla.2022.08.012
31. Dickinson A, Leidy L, Nusair O, et al. Short-term outcomes of Hydrus Microstent with and without additional canaloplasty during cataract surgery. J Glaucoma. 2023;32:769–776. doi:10.1097/IJG.0000000000002245
32. Laspas P, Garcia-Feijoo J, Martinez-de-la-Casa JM, et al. Three-year results of Hydrus Microstent with phacoemulsification. Ophthalmol Glaucoma. 2019;2:440–442. doi:10.1016/j.ogla.2019.08.006
33. Samet S, Ong JA, Ahmed IIK. Hydrus microstent implantation for surgical management of glaucoma: a review of design, efficacy and safety. Eye Vis. 2019;6:32. doi:10.1186/s40662-019-0157-y
34. Kiramira D, Voßmerbäumer U, Pfeiffer N, et al. Mid-term real world outcomes of the Hydrus® Microstent in open angle glaucoma. Eye. 2024;38(8):1454–1461. doi:10.1038/s41433-023-02920-2
35. Bhatnagar P, Dossantos J, Bonilla B, et al. One year outcomes of Hydrus Microstent with and without additional canaloplasty during cataract surgery. Invest Ophthalmol Vis Sci. 2024;65:3493.
36. Lewis K, Albo C, Wang A, et al. Comparison of Hydrus Microstent and Hydrus Microstent with OMNI canaloplasty for mild to moderate primary open angle glaucoma. Invest Ophthalmol Vis Sci. 2023;64:4272.
37. Rocks M, Dossantos J, Bonilla B, et al. Long-term efficacy of OMNI canaloplasty with and without Hydrus Microstent during cataract surgery. Invest Ophthalmol Vis Sci. 2024;65:3492.
38. Creagmile J, Kim WI, Scouarnec C. Hydrus Microstent implantation with OMNI surgical system Ab interno canaloplasty for the management of open-angle glaucoma in phakic patients refractory to medical therapy. Am J Ophthalmol Case Rep. 2023;29:101749. doi:10.1016/j.ajoc.2022.101749
39. Porter MS, Flowers A, Wood BP, et al. Efficacy and safety of cataract surgery combined with Ab interno canaloplasty and micro-trabecular bypass stent surgery in open-angle glaucoma. Clin Ophthalmol. 2025;19:469–481. doi:10.2147/OPTH.S504247
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Combined Phacoemulsification and Hydrus Microstent in Open-Angle Glaucoma Versus Combined-Mechanism/Primary Angle Closure Glaucoma
Nguyen K, Chansangpetch S, Vinh MK, Tran AQH, Radhakrishnan S, Nguyen N, Iwach AG, Lin S
Clinical Ophthalmology 2025, 19:3347-3356
Published Date: 11 September 2025