Back to Journals » OncoTargets and Therapy » Volume 13
Effective Treatment with Cabozantinib in an Advanced Non-Small-Cell Lung Cancer Patient Harboring a CD74-ROS1 Fusion: A Case Report
Authors Wang G, Gao J, Lv J, Chen X, Wu J, Wang R, Jiang J
Received 15 October 2019
Accepted for publication 17 December 2019
Published 11 February 2020 Volume 2020:13 Pages 1171—1177
DOI https://doi.org/10.2147/OTT.S234733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Gang Wang, 1, 2,* Jinqi Gao, 3,* Jinyan Lv, 1 Xi Chen, 1 Jinyu Wu, 1 Ruoyu Wang, 1, 2 Jianing Jiang 1, 2
1Department of Medical Oncology, The Affiliated Zhongshan Hospital of Dalian University, Dalian, Liaoning Province, People’s Republic of China; 2The Key Laboratory of Biomarker, High-Throughput Screening and Target Translation of Breast and Gastrointestinal Cancer, Dalian, Liaoning Province, People’s Republic of China; 3Department of Intervention, The Second Affiliated Hospital of Dalian Medical University, Dalian, Liaoning Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruoyu Wang; Jianing Jiang
Department of Medical Oncology, The Affiliated Zhongshan Hospital of Dalian University, Dalian, Liaoning Province 116001, People’s Republic of China
Tel/Fax +86-411-62897370
; +86-411-62897233
Email [email protected]; [email protected]
Abstract: Cabozantinib has been shown to have potent anti-ROS1 activity in many solid malignancies, particularly against those with solvent-front resistance mutations following crizotinib therapy. With regard to the most common CD74-ROS1 fusion, the efficacy of cabozantinib has only been demonstrated in vitro. Therefore, we evaluate the efficacy of cabozantinib in a patient with advanced non-small-cell lung cancer (NSCLC) harboring a CD74-ROS1 fusion in the present study. A 40-year-old female patient presented with 1-month history of cough, white sputum and chest pain. Chest CT scan revealed a consolidation in the middle lobe of the right lung together with multiple cavity lesions spreading in both lungs. Histopathological analysis of biopsy samples from the lesion in the middle lobe of the right lung suggested lung adenocarcinoma. After two lines of chemotherapy and EGFR-TKI therapy, a CD74-ROS1 rearrangement was detected and the patient was administered with cabozantinib for 1.5 years. Since cabozantinib resistance developed, crizotinib therapy was applied and demonstrated clinical effectiveness until now. Together, we report the first case of cabozantinib effectiveness in treating a CD74-ROS1-positive advanced NSCLC patient. Crizotinib remained as an effective therapeutic option following the acquisition of cabozantinib resistance.
Keywords: cabozantinib, CD74-ROS1 fusion, NSCLC, crizotinib
Introduction
Molecular-targeted therapy is an effective therapeutic strategy for lung cancer and yields markedly improved progression-free survival (PFS) and overall survival (OS) compared to conventional chemotherapy in patients carrying certain mutations. ROS1 arrangement is a well-known driver mutation present in 1–2% of non-small-cell lung cancer (NSCLC) patients, with CD74-ROS1 fusion being the most common one frequently occurring in light or non-smokers.1 Crizotinib has received full FDA approval for the treatment of advanced ROS1-rearranged lung cancer. Unfortunately, crizotinib resistance inevitably develops in ROS1-driven NSCLC and the vast majority of patients had disease progression on crizotinib therapy, dramatically impacting patient’s prognosis and quality of life.
Cabozantinib is a small-molecule tyrosine kinase inhibitor that selectively targets MET, VEGFR-2, RET, ROS1 and AXL and has displayed potent anti-ROS1 activity in many solid tumors, especially against those solvent-front ROS1 resistance mutations, such as G2032R, D2033N, L1519R and L2026M.2,3 A Phase II trial of cabozantinib is currently ongoing.4 To date, there is no clinical evidence regarding the potential efficacy of cabozantinib against CD74-ROS1-positive NSCLC. A previous preclinical study in NSCLC cell lines has shown that cabozantinib was capable to effectively target both wild-type and the resistant mutant CD74-ROS1.5 Here, we report for the first time the use of cabozantinib in treating an advanced NSCLC case carrying CD74-ROS1 fusion and crizotinib was an effective therapeutic strategy for overcoming cabozantinib resistance in this patient.
Case Report
A 40-year-old Chinese female with no smoking history visited our hospital with symptoms of cough, white frothy sputum, and right chest pain for more than a month. Chest CT scan revealed heterogeneous consolidation in the right upper lobe of the lungs (Figure 1A). Pathological examination of the percutaneous transthoracic needle aspiration biopsy samples from this lesion indicated lung adenocarcinoma (Figure 2A). Multiple cavity lesions were present in both lungs, while no other metastases were observed by imaging examinations. Since ARMS-PCR assay demonstrated an absence of EGFR mutation or ALK fusion in patient’s plasma circulating tumor DNA (ctDNA), we administered this patient with two lines of chemotherapy followed by gefitinib treatment according to the NCCN guidelines. Specifically, 6 curative cycles of gemcitabin plus cisplation were given as the first-line chemotherapy. The lesions remained unchanged within the first four cycles; however, they were enlarged in the 6th cycle. Thus, docetaxel was given as the second-line therapy, but the lesions continuously increased after 4 cycles of docetaxel therapy. Considering the false negative rate of the ARMS-PCR detection in plasm ctDNA due to intratumor heterogeneity, we changed the therapeutic strategy to gefitnib under the patient’s desire but the tumors still increased (Figure 1B). To identify further treatment options, targeted next-generation sequencing (NGS) using a cancer-relevant gene panel was performed on both biopsy sample of the right lung and plasma ctDNA. Interestingly, a CD74-ROS1 fusion (allele fraction (AF), 15.5%) and a L1433F missense mutation in MTOR (AF, 14.2%) were identified in the tissue specimen; no mutation was detected in the plasma ctDNA (Figure 3A1 and A2). Crizotinib was too expensive for the patient to afford, and cabozantinib was given orally daily. The lesions regressed within the initial 6 months (Figure 1C), and remained stable until progression 20 months later (Figure 1D).
To uncover potential resistance mechanisms, targeted NGS on a new percutaneous transthoracic needle aspiration biopsy in the right lung (Figure 2B) was performed and revealed the presence of a CD74-ROS1 fusion (AF, 13.5%) and a L1433F missense mutation in MTOR (AF, 26.5%), as well as a newly acquired G245S missense mutation in TP53 (AF, 19%) (Figure 3B1–B3). In addition, changes in the expression level of VEGFR-2, another target of cabozantinib, were considered to lead to drug resistance. To test this possibility, we performed immunohistochemical analyses of VEGFR-2 in tissue biopsy before (Figure 4A) and after the acquisition of resistance (Figure 4B) but there was no significant difference between the two groups (p>0.05). After that, crizotinib was orally given twice a day. A rapid reduction in the lesions of both lungs was observed (Figure 1E) and the patient experienced immediate relief of clinical symptoms. The lesions remained decreased for 6 months until now.
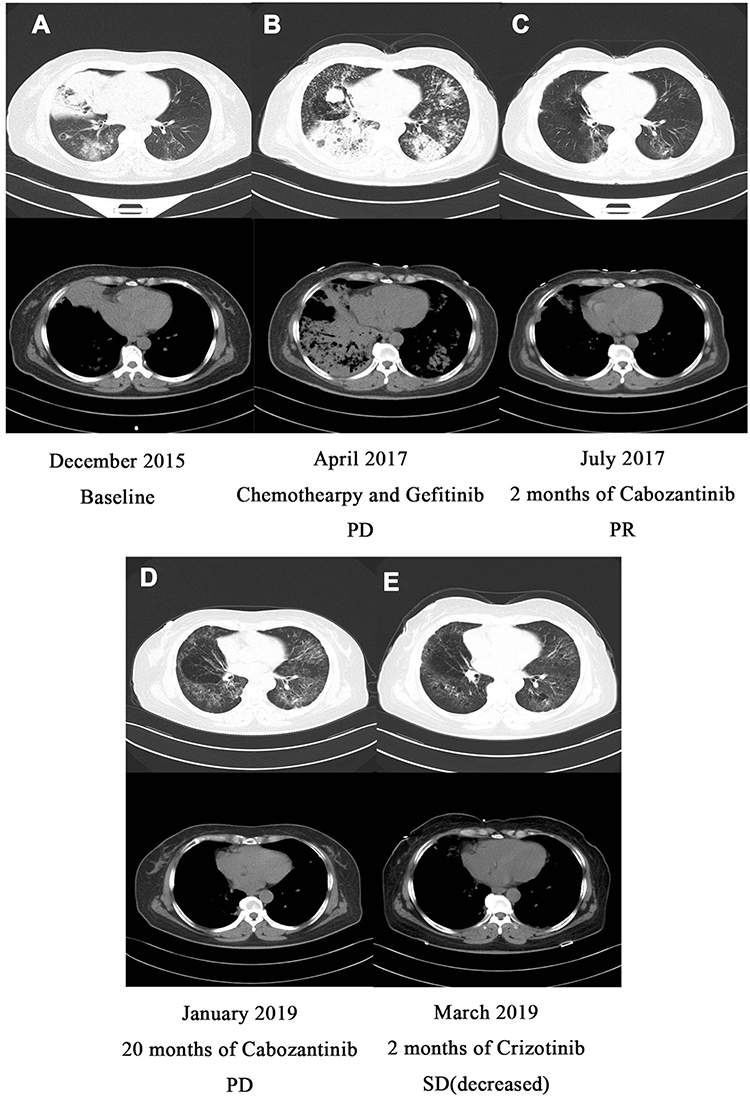 |
Figure 1 (A) The baseline CT scan of the patient’s chest in December 2015. (B) CT scan of the chest after gefitinib chemotherapy in April 2017. (C) CT scan of the chest after 2 months of cabozantinib treatment in June 2017. (D) CT scan of the chest after 20 months of cabozantinib treatment in January 2019. (E) CT scan of the chest after 2 months of crizotinib treatment in March 2019. |
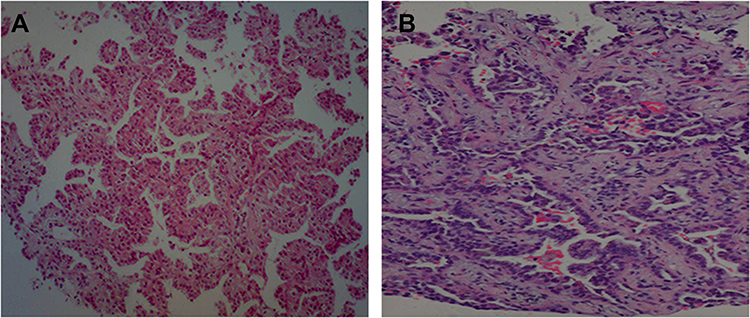 |
Figure 2 (A) Positive detection of adenocarcinoma cells in an aspiration biopsy sample of the lump in the right lung. (B) The second aspiration biopsy tissue sample in the right lung after 2 years when cabozantinib resistance occurred. |
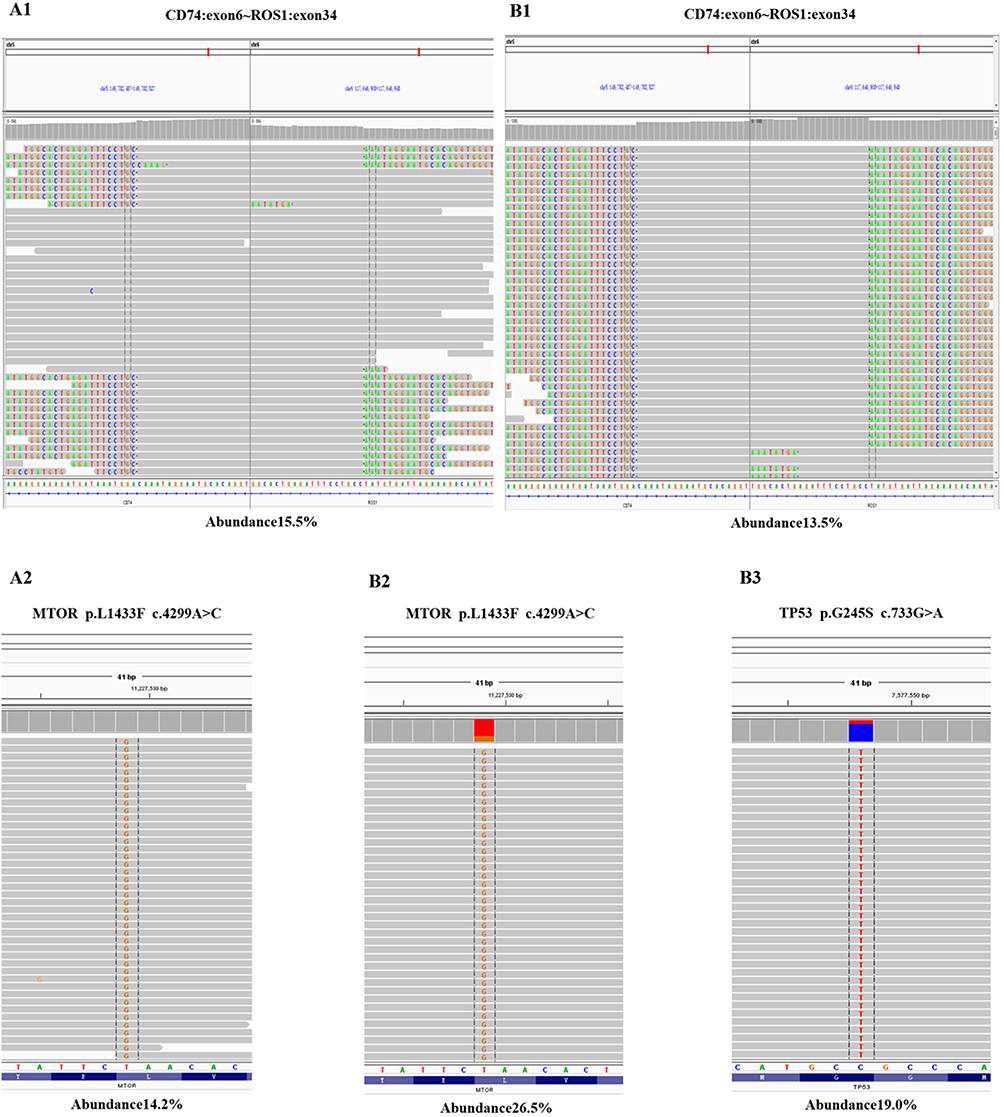 |
Figure 3 (A1 and A2) Next-generation sequencing (NGS) reads showing the CD74-ROS1 and MTOR regions from the first biopsy tissue were visualized using the integrated genomics viewer. (B1–B3) NGS reads showing the CD74-ROS1, MTOR and TP53 regions from the second biopsy tissue were visualized using the integrated genomics viewer. |
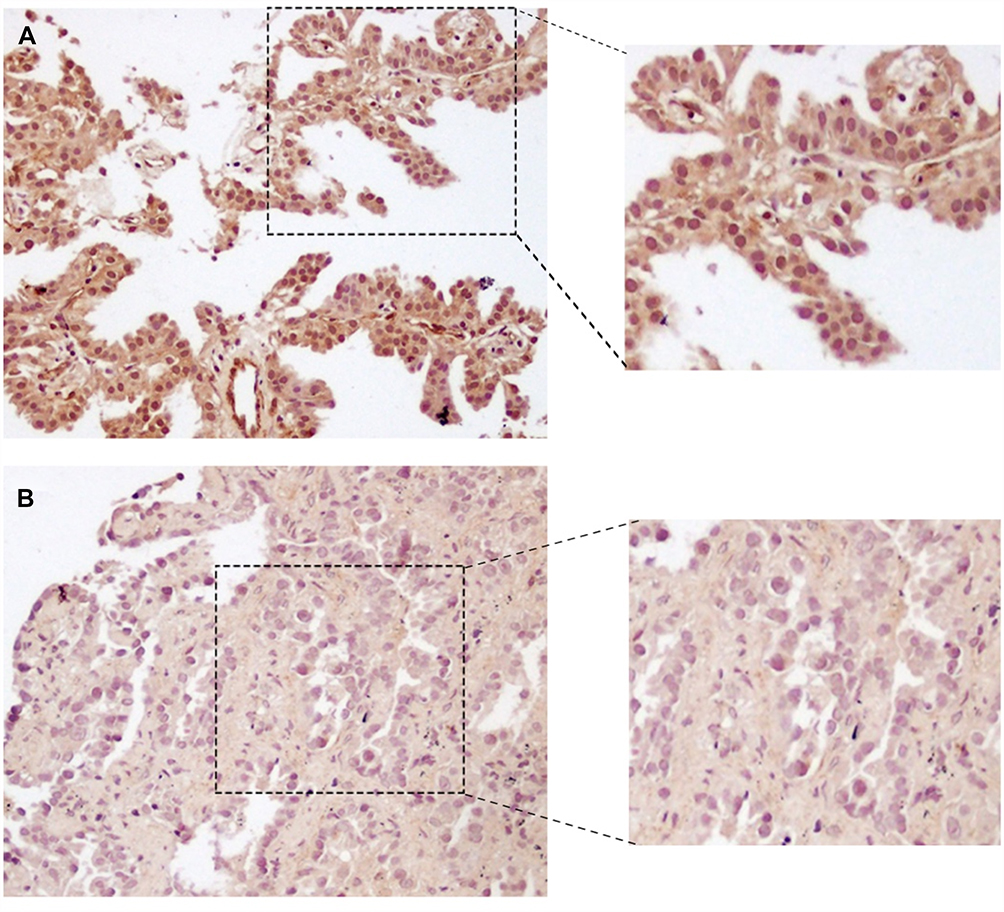 |
Figure 4 (A) Immunohistochemical staining of VEGFR2 in tissue biopsy before the occurrence of cabozantinib resistance. (B) Immunohistochemical staining of VEGFR2 in tissue biopsy after the acquisition of cabozantinib resistance. Magnification; ×200. |
Discussion
Molecular-targeted therapy play an important role in current lung cancer therapy. In addition to EGFR, ALK, KRAS, and AKT mutations, ROS1 arrangement is another major genetic alteration identified in 1–2% of NSCLC patients. Nine different ROS1 fusion partners have been identified so far, with CD74 being the most common. Crizotinib has received full approval from the US Food and Drug Administration (FDA) for treating advanced ROS1-rearranged lung cancer and remains the only approved drug for this molecularly defined subset. Cabozantinib, a small pan-target molecular tyrosine kinase inhibitor, has been approved by the FDA for the treatment of metastatic medullary thyroid cancer,6 and recently for advanced renal cell carcinoma after prior anti-angiogenic therapy.7 As to lung cancer, cabozantinib has been reported to have strong and selective anti-ROS1 activity, especially against solvent-front resistance mutations in ROS1, including G2032R, D2033N, L1519R and L2026M, and a phase II clinical trial is currently ongoing.4 However, there is no clinical evidence of cabozantinib efficacy against CD74-ROS1-positive NSCLC. Only one study using in vitro cell culture models has reported its effectiveness against both wild-type and the resistant mutant CD74-ROS1.5
In the present study, the patient initially disagreed to accept genome sequencing detection and received 6 cycles of first-line chemotherapy. Because of lesion enlargement, she underwent genome sequencing detection for EGFR and ALK but no mutation was identified in the plasma ctDNA. She next received gefitinib treatment, which unfortunately did not display efficacy. Thus, a NGS-based cancer gene panel test covering a total of 422 common mutation hotspots was performed in both cancer tissue and serum samples and revealed a CD74-ROS1 fusion in exon 34 (abundance, 15.5%). Cabozantinib treatment was then administered and yielded an incredible effect for 1.5 years. When cabozantinib resistance developed, another 422-gene cancer panel assay was performed, with a discovery of a CD74-ROS1 fusion mutation in exon 34 (abundance, 13.5%), a mTOR L1433F missense mutation in exon 29 (abundance, 26.5%) and a TP53 G245S missense mutation in exon 7 (abundance, 19%) in tumor tissue and none of these alterations in ctDNA (Figure 3B1–B3). To our knowledge, this is the first report case describing that cabozantinib may be a novel therapy for NSCLC patients with CD74-ROS1 fusion. In our case, cabozantinib treatment was associated with a remarkable PFS of 1.5 years. In addition, crizotinib remained effective after the patient gained cabozantinib resistance. Potential explanations for the resistance of cabozantinib in this case include: (1) Cabozantinib is a pan-target agent that may be ineffective in treating one certain point; (2) The increased abundance of mTOR and newly acquired TP53 mutations may be implicated in driving cabozantinib resistance. Earlier studies have indicated that concomitant mutation was more likely to occur in the CD74 group of ROS1 fusion mutation, with mTOR (23%) and TP53 (25%) mutations being the most frequent ones.8,9 Although cabozantinib resistance could not be conclusively related to mTOR and/or TP53 mutations, association of mTOR activation and genetic alterations of TP53 with treatment resistance in the clinic have been reported.10,11 Further studies are warranted to assess whether the increased abundance of mTOR mutation and newly acquired TP53 mutation contributes to the acquisition of resistance to cabozantinib.
In summary, we report the first clinical evidence that cabozantinib therapy significantly suppressed tumor growth and relieved respiration symptoms in an NSCLC patient harboring a CD74-ROS1 fusion. Crizotinib can also be administered after the acquisition of cabozantinib resistance. This therapeutic approach may serve as a potentially novel treatment option for such patients. Future clinical trials with a larger cohort are encouraged and will be beneficial to further study the efficacy of cabozantinib in treating NSCLC cases with CD74-ROS1 rearrangement. Moreover, our findings suggest that genome sequencing in tumor tissue biopsy may be more accurate than that in plasma ctDNA. If ctDNA detection yields negative results, tissue biopsy analysis may provide more information for monitoring disease progression and treatment response.
Abbreviations
ROS1, receptor tyrosine kinase1; NSCLC, Non-Small-Cell Lung Cancer; EGFR-TKI, epidermal growth factor receptor-tyrosine kinase inhibitor; MET(HGF), Hepatocyte Growth Factor; VEGFR-2, Vascular Endothelial Growth Factor Receptor-2; ALK, Anaplastic Lymphoma Kinase; ARMS-PCR, Amplification Refractory Mutation System-Polymerase Chain Reaction; NCCN, National Comprehensive Cancer Network; NGS, Next-Generation Sequencing; ctDNA, circulating tumor DNA; AF, allele fraction; mTOR, mechanistic Target of Rapamycin; TP53, Tumor Suppressor p53; FDA, the Food and Drug Administration; PFS, Progression-free survival; OS, overall survival.
Ethics Statements
The institution approves of publishing the case details.
Statistical Analysis
All statistical analyses were carried out using SPSS 13.0 statistical software package (Chicago, IL, USA). Data were expressed as mean±standard deviation (SD). Statistical significance of the differences between experimental groups was determined using Mann–Whitney test. P < 0.05 was considered statistically significant.
Acknowledgments
We thank the patient in this report and her family. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. This work was supported by grants from the National Natural Science Foundation of China (#81803109) and the Doctor Study-up Foundation of Liaoning Province (2019-BS-010).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Velcheti V, Bauer T, Subbiah V, et al. OA 12.07 - LOXO- 292, a potent, highly selective RET inhibitor, in MKI- resistant RET fusion-positive lung cancer patients with and without brain metastases. J Thorac Oncol. 2017;12:1778. doi:10.1016/j.jtho.2017.09.399
2. Drilon A, Somwar R, Wagner JP, et al. A novel crizotinib-resistant solvent-front mutation responsive to cabozantinib therapy in a patient with ROS1-rearranged lung cancer. Clin Cancer Res. 2016;22(10):2351–2358. doi:10.1158/1078-0432.CCR-15-2013
3. Lin JJ, Shaw AT. Recent advances in targeting ROS1 in lung cancer. J Thorac Oncol. 2017;12(11):1611–1625. doi:10.1016/j.jtho.2017.08.002
4. Chong CR, Bahcall M, Capelletti M, et al. Identification of existing drugs that effectively target NTRK1 and ROS1 rearrangements in lung cancer. Clin Cancer Res. 2017;23:204–213. doi:10.1158/1078-0432.CCR-15-1601
5. Katayama R, Kobayashi Y, Friboulet L, et al. Cabozantinib overcomes crizotinib resistance in ROS1 fusion positive cancer. Clin Cancer Res. 2015;21:166–174. doi:10.1158/1078-0432.CCR-14-1385
6. Viola D, Cappagli V, Elisei R. Cabozantinib (XL184) for the treatment of locally advanced or metastatic progressive med- ullary thyroid cancer. Future Oncol. 2013;9(8):1083–1092. doi:10.2217/fon.13.128
7. Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): final results from a randomised, open-label, Phase 3 trial. Lancet Oncol. 2016;17(7):917–927. doi:10.1016/S1470-2045(16)30107-3
8. Zeng L, Yizhi L, Xiao L, et al. Crizotinib presented with promising efficacy but for concomitant mutation in next-generation sequencing-identified ROS1-rearranged non- small-cell lung cancer. Onco Targets Ther. 2018;11:6937–6945. doi:10.2147/OTT.S176273
9. Jessica J, Lauren L, Siraj M, et al. ROS1 fusions rarely overlap with other oncogenic drivers in non-small cell lung cancer. J Thoracic Oncol. 2017;12(5):872–877. doi:10.1016/j.jtho.2017.01.004
10. Wendy A, David CL, Sandra A, John D. Molecular biology of lung cancer. J Thorac Dis. 2013;5(55):S479–S490. doi:10.3978/j.issn.2072-1439.2013.08.03
11. Jackie L, Pillai S, Srikumar P. Genetic and biochemical alterations in non-small cell lung cancer. Biochem Res Int. 2012;10:1155–1172.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.