Back to Journals » Patient Preference and Adherence » Volume 19
Effect of Theme-Based Nursing Education on Disease Awareness, Serum Uric Acid Control, Quality of Life, and Acute Attacks in Patients with Gout: A Randomized Controlled Study at a Tertiary Hospital in Beijing
Received 14 January 2025
Accepted for publication 28 April 2025
Published 22 July 2025 Volume 2025:19 Pages 2119—2128
DOI https://doi.org/10.2147/PPA.S514475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Zhenlei Gao, Juan Meng
Department of Rheumatology and Immunology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China
Correspondence: Juan Meng, Department of Rheumatology and Immunology, Beijing Chao-yang Hospital, Capital Medical University, 8 Gong-Ti South Road, Beijing, 100020, People’s Republic of China, Tel +86-10-85231062, Email [email protected]
Objective: Patients with gout commonly face issues such as insufficient disease awareness and poor management outcomes. The innovative introduction of theme-based nursing education aims to enhance patients’ disease awareness, reduce acute attacks, and improve quality of life.
Methods: This study is a randomized controlled trial, A total of 72 patients with gout admitted to Beijing Chaoyang Hospital between 1 January 2023 and 31 November 2023 were randomly divided into the intervention group and the traditional nursing health education group. The traditional nursing health education group received traditional nursing health education, whereas the intervention group received theme-based nursing education. Both groups were continuously nursed for 12 weeks. Disease cognition, blood uric acid levels, QoL and frequency of acute attacks were assessed before and after the intervention. Statistical analysis was conducted using independent sample t-tests for between-group comparisons and paired t-tests for within-group comparisons.
Results: After the intervention, the gout knowledge score in the intervention group was significantly higher than that in the traditional nursing health education group. The blood uric acid level at 12 weeks in the intervention group was significantly lower than that in the traditional nursing health education group, and the blood uric acid compliance rate was significantly higher than that in the traditional nursing health education group. The intervention group scored higher in four dimensions of the SF-36 scale: physical function, bodily pain, general health and vitality. The frequency of acute attacks in the intervention group was significantly lower than that in the traditional nursing health education group.
Conclusion: Theme-based nursing education demonstrated superior outcomes in enhancing disease cognition, controlling blood uric acid, improving QoL and reducing acute attacks compared with traditional nursing health education.
Keywords: acute attacks, blood uric acid control, disease cognition, gout, quality of life, thematic nursing education
Introduction
Gout, a metabolic disease caused by abnormal purine metabolism, is characterized by hyperuricemia and recurrent acute arthritis attacks. The global prevalence is on the rise, with the prevalence in China ranging from 1% to 3%.1,2 Gout is a chronic condition that can be effectively managed through target-driven treatment, with the key being to maintain target serum uric acid levels to reduce attacks and prevent complications.3 However, patient compliance is poor, and there is a lack of adequate disease knowledge. Traditional health education methods have limitations and have not facilitated long-term self-management.
Research indicates that gout patients have low adherence to urate-lowering therapy (ULT),4 and their level of disease knowledge is insufficient.5 Traditional nursing health education is often passive, one-way, and lacks personalization, making it difficult to motivate patients for self-management or meet individual learning needs.6 This model neglects patients’ subjective initiative and individual differences, resulting in limited improvement in self-management and disease awareness capabilities, and insufficient sustainability of educational effects.7
Theme-based nursing education offers an alternative, patient-centred approach designed to overcome these limitations. This model emphasises interactive and practical learning, helping patients to systematically apply knowledge to their daily lives. Compared with the traditional model, theme-based nursing education offers the following advantages: 1) strong targeting, allowing for the development of educational content tailored to individual patient needs; 2) high engagement, enhancing patients’ interest in learning through interactive teaching methods; and 3) strong practicality, integrating theoretical knowledge with daily life practices.8 Previous studies have demonstrated that theme-based nursing education yields positive outcomes in chronic disease management, such as improving blood glucose control in patients with diabetes9 and enhancing treatment compliance in patients with hypertension.10 However, research on its application in managing patients with gout remains limited. The traditional health education model often focuses on one-way knowledge transfer, lacking personalization and interactivity, which results in low patient engagement and insufficient knowledge application. In contrast, theme-based nursing education, through customized content, interactive teaching, and practical integration, effectively enhances patient engagement and knowledge application skills. This study hypothesizes that theme-based nursing education will surpass traditional nursing health education, significantly improving gout patients’ disease knowledge, serum uric acid control levels, reducing the frequency of gout attacks, and enhancing quality of life, providing a more effective educational strategy for gout management.
This study aims to evaluate the impact of theme-based nursing education compared with traditional nursing health education on key outcomes in gout management, including disease knowledge, serum urate control, gout flare frequency and quality of life (QoL). By addressing the gaps in traditional approaches, this study seeks to provide evidence for integrating thematic nursing education into clinical practice to enhance patient outcomes.
Participants and Methods
Participants
China has a large number of gout patients with unique disease characteristics. The Department of Rheumatology and Immunology at Beijing Chaoyang Hospital is strong in professional expertise and representative, which facilitates in-depth research. Convenience sampling was used to select patients with primary gout who were hospitalized in the Department of Rheumatology and Immunology at Beijing Chaoyang Hospital between January 1, 2023, and November 30, 2023, as research subjects.
The inclusion criteria were as follows: all patients met the 2015 classification criteria for gout jointly developed by the American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR),11 and they were able to communicate normally. The exclusion criteria were as follows: 1) patients with severe cognitive or communication impairments that prevented them from providing informed consent or participating in educational interventions; 2) patients with rheumatoid arthritis or severe osteoarthritis meeting the 2019 EULAR criteria;12 3) patients with terminal illnesses or severe comorbidities; 4) patients with hematologic diseases or active gastrointestinal bleeding; 5) patients undergoing tumour radiotherapy or chemotherapy.
All patients voluntarily participated in this study, provided written informed consent and received integrated medical and nursing management via the hospital’s Whole-Course Chronic Rheumatic Disease Management Platform. The study was approved by Beijing Chaoyang Hospital’s medical ethics committee (approval No.: 2022-ke-439). This study complies with the ethical standards of the Declaration of Helsinki.
Research Methods
The patients were divided into a theme-based nursing health education group (intervention group, n = 36) and a traditional nursing health education group (traditional nursing health education group, n = 36) using a random number generator. Both groups received health education every 2 weeks during the 12-week follow-up period,13 delivered either in person or via remote telephone. The traditional nursing health education group received routine nursing health education alone with an average interaction time of 10–15 minutes per session, whereas the intervention group was additionally given theme-based nursing health education with an average interaction time of 20–30 minutes per session. The specific measures were as follows.
Theme Determination
The head nurse of our department, in collaboration with three specialist supervisor nurses, was responsible for designing and developing theme-based nursing health education prescriptions, which were reviewed by a chief physician. Based on issues identified in the management of patients with gout from the perspective of patient self-management behaviour, four prescription themes were ultimately determined: recognition of acute gouty arthritis attacks, diet, exercise and psychological support. These themes were established after fully considering patients’ understanding of disease control and health behaviours, as well as their knowledge and skill levels.
Theme-Based Nursing Health Education Prescription
The implementation process of thematic nursing health education prescription is shown in detail in Table 1.14
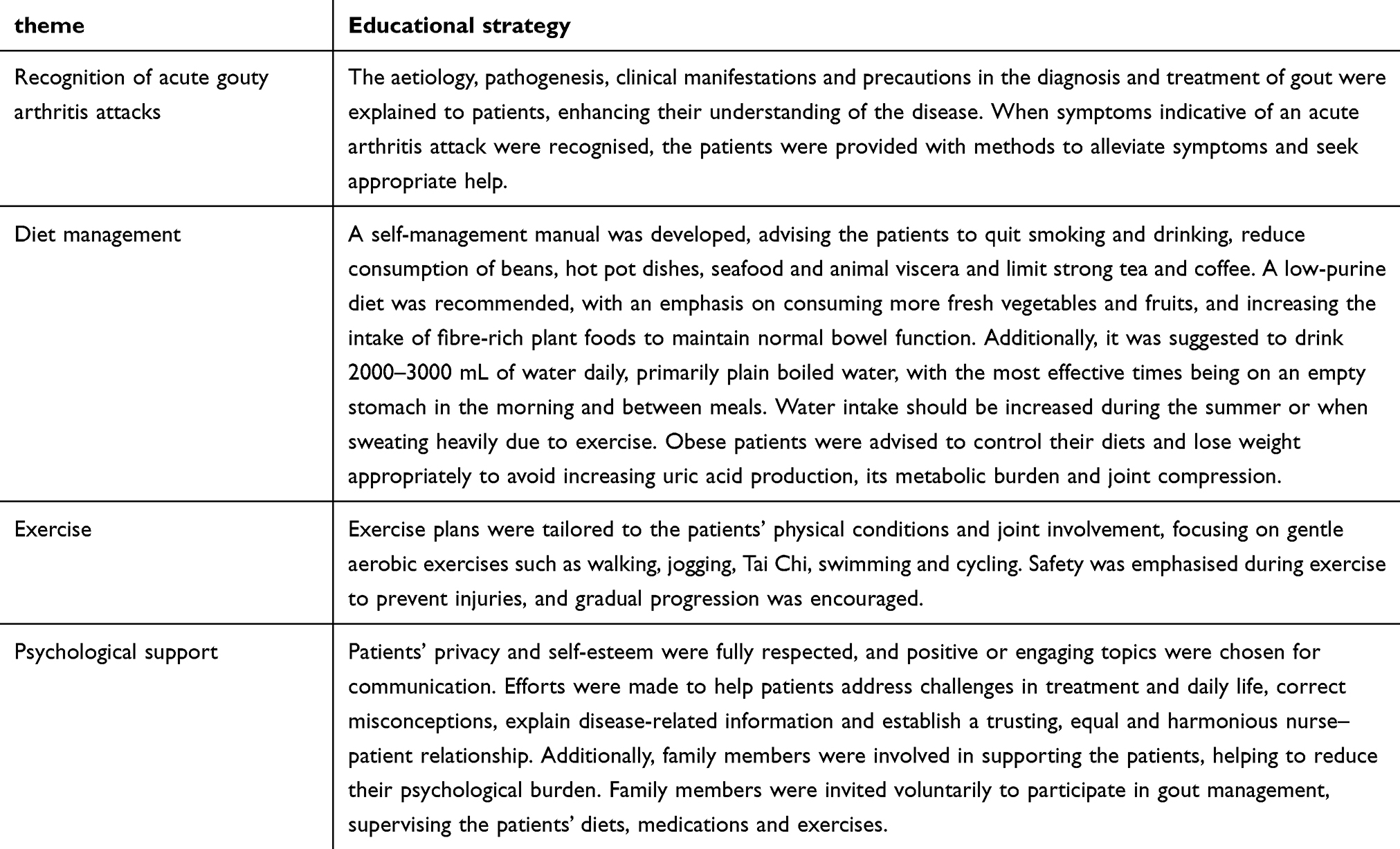 |
Table 1 Implementation Process of Theme-Based Nursing Health Education Prescription |
Application of the Theme-Based Nursing Health Education Prescription
An independent prescription was developed for each theme and printed. The responsible nurse informed the patients of its usage upon discharge, evaluated their application and sent the electronic content to the patients and/or their family members through the chronic disease management platform. Additionally, the responsible nurse communicated with and guided the patients and/or their family members every 2 weeks.
The Traditional Nursing Health Education
The traditional nursing health education group received general information on gout management, including the importance of ULT, dietary recommendations and the prevention of acute flares through one-on-one oral explanations and printed brochures during routine hospital visits. The patients were contacted biweekly via telephone to monitor adherence to their prescribed treatment plans and address basic queries regarding gout management. Each session lasted approximately 10–15 minutes.
Although this traditional model ensured that all patients received comprehensive medical and nursing care, it lacked the personalised and interactive components of the theme-based nursing education provided to the intervention group.
Observation Indicators
Demographic data collection
Demographic and baseline clinical characteristics were collected for all participants at enrolment, including age, gender, disease duration, number of involved joints, comorbidities and current use of ULT. These data were used to assess baseline comparability between the intervention and traditional nursing health education groups.
Disease Cognition
The gout knowledge questionnaire (GKQ),15 consisting of 10 questions developed by Zhang Liyun et al, was administered before and 3 months after the intervention, as shown in Supplementary Table 1. Each correct answer was worth 1 point, with a total score of 10 points. A score of ≥7 points was considered to indicate that the patient had a sufficient understanding of gout-related knowledge. Questionnaire surveys were conducted by nurses with standardised training through face-to-face interviews before the intervention and at 6 and 12 weeks after it.
Blood Uric Acid Levels and Standard-reaching Rate
Fasting venous blood samples were collected from the patients before the intervention and 6 and 12 weeks after it, and blood uric acid levels were measured using urate oxidase. Within 2 hours of collection, the blood samples were centrifuged and analysed using an automatic biochemical analyser (Beckman Coulter AU5800, USA). According to the 2020 ACR Guidelines for the Management of Gout,16 a blood uric acid level of <360 μmol/L was defined as the standard.
Quality of Life Assessment
Before and 12 weeks after the intervention, the QoL of the patients was assessed using the 36-item short-form health survey (SF-36),17 which included 8 dimensions: physical functioning, role-physical, bodily pain, general health perceptions, vitality, social functioning, role-emotional and mental health. A higher score indicated better QoL.
Frequency of Acute Gout Attacks
The frequency of acute gout attacks was recorded 3 months before and after the intervention.
Outcomes
The primary outcome of this study was the improvement in gout knowledge in the intervention group, as assessed by a validated GKQ at the 3-month follow-up. Secondary outcomes included significant differences between the intervention and traditional nursing health education groups in the number of gout episodes, QoL (measured by the SF-36 questionnaire) and serum uric acid levels (below the recommended target of 360 μmol/L), measured at baseline and 3 months post-intervention.
Statistical Processing
The sample size was calculated using PASS software (version 15.0). An effect size (d) of 0.7 was assumed for key outcome measures, with a significance level (α) of 0.05 (two-tailed) and a power (1−β) of 0.8. This calculation determined that a minimum of 34 participants per group was required. Accounting for a potential dropout rate of 10%, the final sample size was set at 36 participants per group, resulting in a total of 72 participants.
Statistical analysis was performed using SPSS (version 23.0) and R (version 4.3.1) with the lme4 package for advanced modeling. Measurement data were first tested for normality via the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation ( ). For between-group comparisons at individual time points (eg, baseline, 6 weeks, 12 weeks), independent sample t-tests with Bonferroni correction were applied. Within-group changes over time were analyzed using linear mixed-effects models (LMM) with restricted maximum likelihood (REML) estimation, incorporating time (baseline, 6 weeks, 12 weeks) and group (intervention vs control) as fixed effects, and participant ID as a random intercept to account for individual variability. The significance of the time × group interaction was tested to evaluate differential trends between groups. Effect sizes for between-group differences were reported as Cohen’s d (thresholds: d = 0.2 small, 0.5 medium, 0.8 large), and within-group variability was quantified using partial eta-squared (η²).
). For between-group comparisons at individual time points (eg, baseline, 6 weeks, 12 weeks), independent sample t-tests with Bonferroni correction were applied. Within-group changes over time were analyzed using linear mixed-effects models (LMM) with restricted maximum likelihood (REML) estimation, incorporating time (baseline, 6 weeks, 12 weeks) and group (intervention vs control) as fixed effects, and participant ID as a random intercept to account for individual variability. The significance of the time × group interaction was tested to evaluate differential trends between groups. Effect sizes for between-group differences were reported as Cohen’s d (thresholds: d = 0.2 small, 0.5 medium, 0.8 large), and within-group variability was quantified using partial eta-squared (η²).
For non-normally distributed data, values were presented as median (interquartile range) [M (Q1, Q3)], with between-group comparisons conducted via the Mann–Whitney U-test and within-group comparisons via the Friedman test. Categorical data were described as counts (percentages) [n (%)], and between-group differences were assessed using Pearson’s χ²-test or Fisher’s exact test (for expected cell counts <5). All hypothesis tests were two-tailed, and a P value of <0.05 was considered statistically significant.
Results
Comparison of General Data
A total of 72 patients were enrolled, all of whom were men. No statistically significant differences were found between the two groups in terms of age, disease duration, educational level, number of involved joints, complications and use of urate-lowering medications at baseline (P > 0.05), indicating comparability, as shown in Table 2.
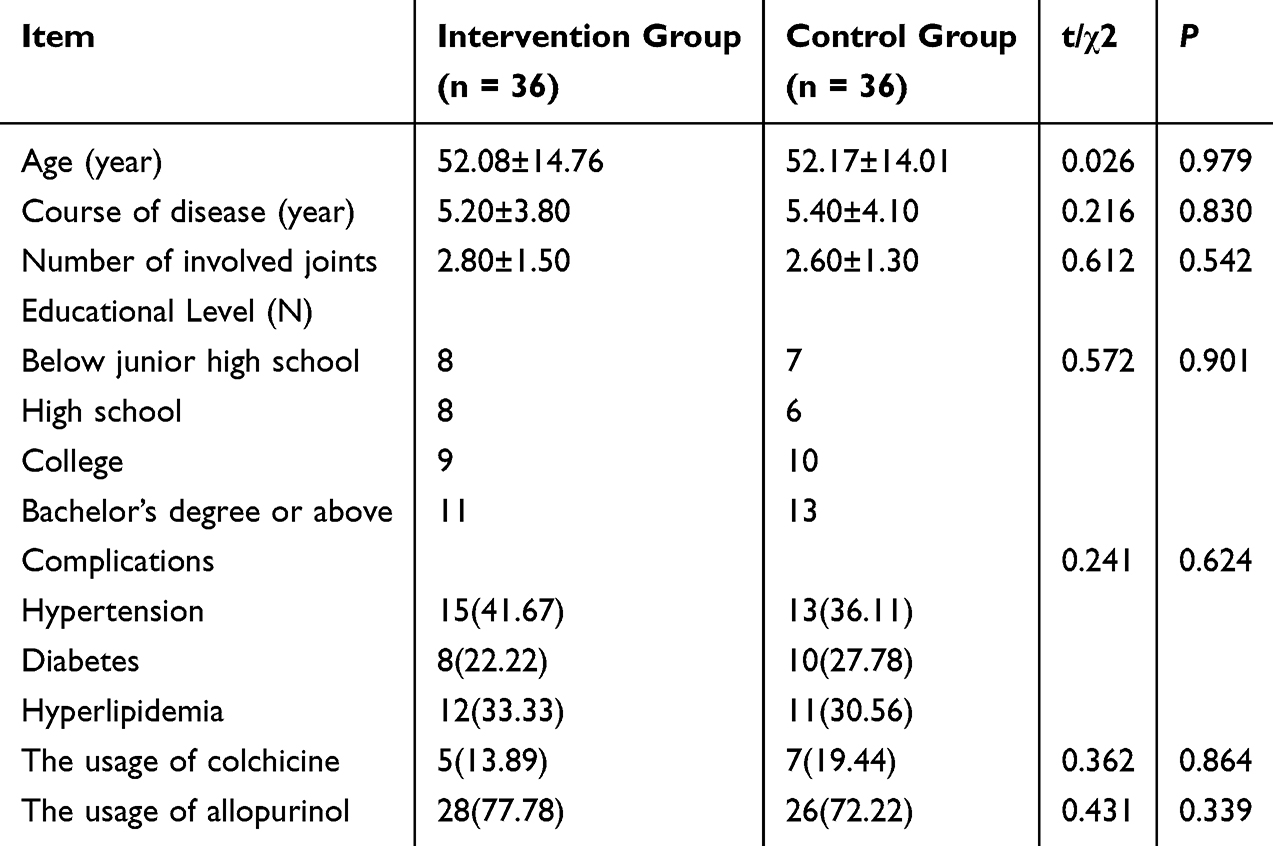 |
Table 2 Comparison of General Data Between Two Groups [n (%), |

Comparison of Disease Cognition between the Two Groups Before and After Intervention
Before the intervention, the gout cognition score showed no statistically significant difference between the two groups (P > 0.05). Six and 12 weeks after the intervention, the gout cognition score in the intervention group was higher than that in the traditional nursing health education group (P < 0.05). Both groups exhibited higher disease cognition scores after the intervention than those before the intervention (P < 0.05) (Table 3).
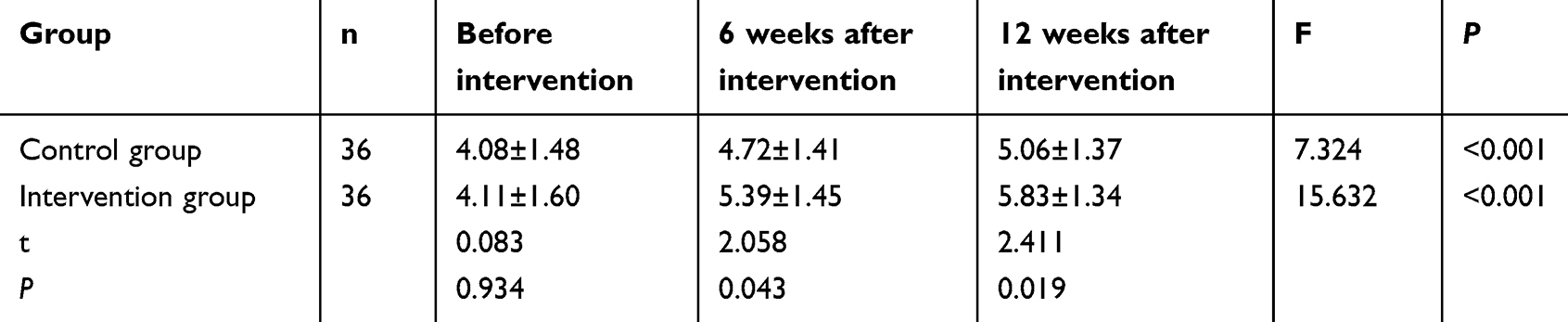 |
Table 3 Comparison of Disease Cognition Between Two Groups Before and After Intervention ( |

Comparison of Blood Uric Acid Levels and Standard-Reaching Rate between the Two Groups Before and After the Intervention
Before the intervention, blood uric acid levels showed no significant difference between the intervention group and the traditional nursing health education group (t = 0.750, P = 0.456). A linear mixed-effects model with repeated measures revealed a significant time × group interaction effect (F[2, 140] = 9.24, P < 0.001), indicating that the intervention group exhibited a steeper reduction in blood uric acid levels over time compared to the control group.
At 6 weeks post-intervention, the intervention group demonstrated significantly lower blood uric acid levels than the traditional nursing health education group (t = 3.12, P = 0.002, Cohen’s d = 0.72). This difference further increased at 12 weeks (t = 3.58, P < 0.001, Cohen’s d = 0.85), with the intervention group achieving a mean level of 343.89 ± 43.70 μmol/L compared to 382.36 ± 52.35 μmol/L in the control group. Both groups showed significant reductions in blood uric acid levels from baseline to 12 weeks (P < 0.001 for within-group comparisons), but the magnitude of reduction was greater in the intervention group (η² = 0.18 vs η² = 0.12 in the control group).
Three months after the intervention, the standard-reaching rate (blood uric acid <360 μmol/L) in the intervention group (63.89%) was significantly higher than that in the traditional nursing health education group (30.56%), with a chi-square test confirming statistical significance (χ² = 8.025, P = 0.005) (Table 4).
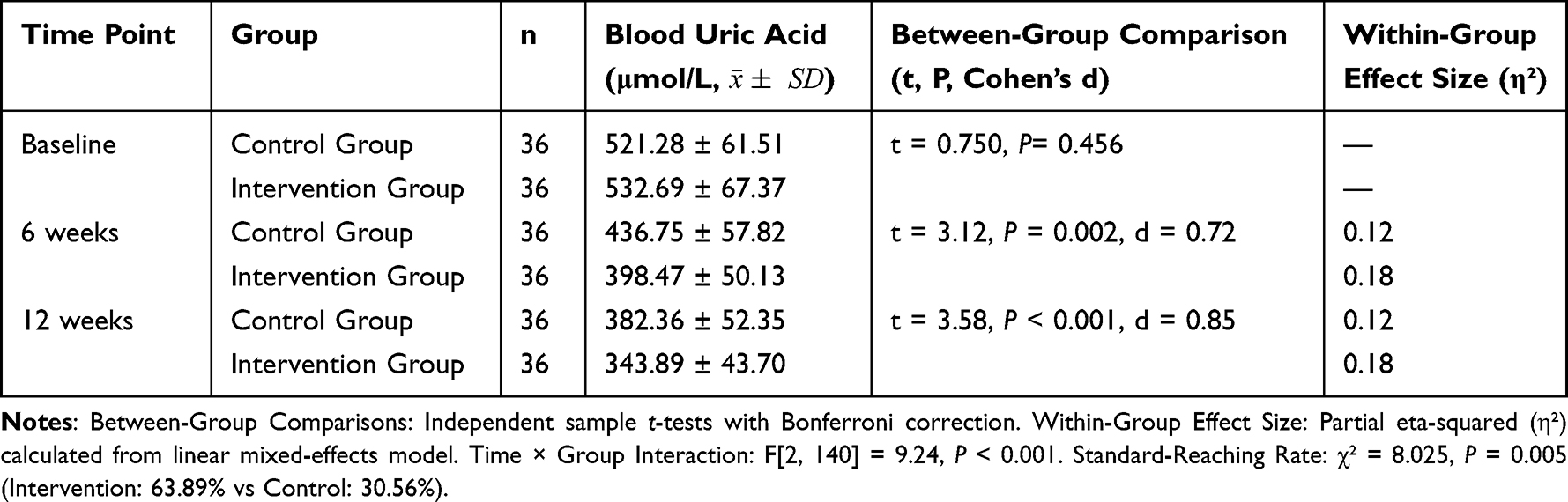 |
Table 4 Comparison of Blood Uric Acid Levels Between Two Groups Before and After Intervention |
Comparison of the Quality of Life between the Two Groups Before and After the Intervention
Before the intervention, no statistically significant differences were found in scores for each dimension on the SF-36 between the two groups (P > 0.05). Twelve weeks after the intervention, there were improvements in the scores of physical functioning, bodily pain, general health perceptions and vitality in the intervention group compared with the traditional nursing health education group (P < 0.05) (Table 5).
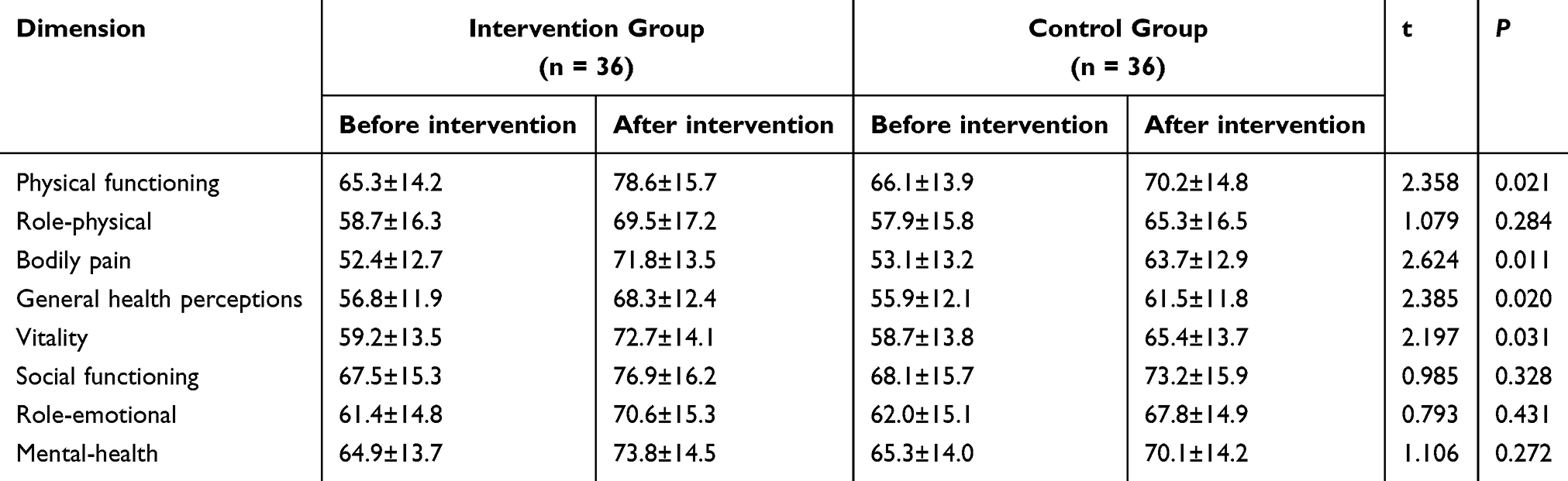 |
Table 5 Comparison of SF-36 Scores between Two Groups Before and After Intervention ( |

Comparison of the Frequency of Acute Gout Attacks between the Two Groups Before and After the Intervention
Three months before the intervention, the frequency of acute gout attacks was 2.6 ± 1.3 and 2.5 ± 1.2 in the intervention group and the traditional nursing health education group, respectively, without statistically significant differences (t = 0.343, P = 0.733). Three months after the intervention, the frequency of acute gout attacks was 0.9 ± 0.7 and 1.5 ± 0.9 in the Intervention group and the traditional nursing health education group, respectively. The frequency of acute gout attacks in the intervention group was significantly lower than that in the traditional nursing health education group (t = 3.217, P = 0.002).
Discussion
This study confirms that the theme-based nursing education model demonstrates significant advantages in the management of gout, with its core value lying in achieving a breakthrough from knowledge transfer to behavior change through a structured interaction model.18 Compared to the generalized approach of traditional education, theme-based nursing education focuses on three core modules: dietary management, exercise programs, and prevention of acute attacks, employing a three-stage pathway of “cognitive restructuring-skill training-continuous reinforcement” effectively addressing the key challenges in current gout management.19
At the level of disease awareness, the significant increase in the GKQ score of the intervention group after 12 weeks validates the targeted education theory proposed by Dalbeth et al.20 This cognitive leap originates from three innovations in the educational model: ① the adoption of a modular curriculum design, which transforms complex pathological knowledge into actionable daily practices; ② the introduction of scenario-based simulation training, which enhances the ability to respond to acute attacks through role-playing; ③ the establishment of a dynamic feedback mechanism, which adjusts educational priorities in real-time based on patients’ cognitive blind spots. This multi-dimensional educational system breaks through the limitations of traditional one-dimensional knowledge, enabling patients’ disease awareness to shift from passive reception to active construction.
Standardised treatment was first introduced in the field of gout by the EULAR in 2016.21 The 2020 ACR Guidelines for the Management of Gout set a goal of maintaining blood uric acid levels at 360 μmol/L.22 Multiple randomised controlled trials have demonstrated that targeted therapy can improve the outcomes of patients with gout, strongly recommending the control of serum uric acid levels below 6 mg/dl (360 μmol/L) and maintaining this standard.23 However, the current status of gout treatment is not optimistic, with a low standard-reaching rate of blood uric acid. According to research data from the Chinese Rheumatism Data Centre, the 6-month standard-reaching rate of blood uric acid is only 38.2% in patients with gout. Several factors contribute to this, such as insufficient understanding of the importance of long-term standardised uric acid-lowering treatment and poor medication adherence among patients.24 Disease-related knowledge plays a key role in the adherence of patients with gout to continuous ULT.25
Twelve weeks after the intervention, the blood uric acid level in the intervention group was significantly lower than that in the traditional nursing health education group, and the standard-reaching rate was also significantly higher, exceeding the results reported by Rees et al.26 This improvement in blood uric acid control highlights the potential of theme-based nursing education to influence patient behaviour and adherence to treatment. Achieving target serum urate levels is a key goal in gout management,27 and our study suggests that educational interventions can play a significant role in helping patients reach these targets.
Three months after the intervention, the frequency of acute gout attacks in the intervention group was significantly lower compared with the traditional nursing health education group, consistent with findings from the study by Wilson et al.28 Our study demonstrated that theme-based nursing health education effectively prevents acute gout attacks by improving patients’ disease cognition and self-management abilities. The reduction in the frequency of acute attacks in the intervention group is particularly noteworthy, as it directly impacts the QoL for patients with gout. This outcome aligns with the broader goal of enhancing patient self-management and underscores the value of holistic care that incorporates educational components.
Compared with the traditional model, this study deeply integrates theme-based nursing education, intelligent monitoring, and multidisciplinary collaboration, effectively breaking through the bottleneck in gout management and providing strong support and empirical evidence for the innovation of chronic disease management. This study offers three insights for clinical practice: Firstly, theme-based nursing education should be incorporated into the standardized treatment system for gout as a necessary complement to pharmacological therapy. Secondly, it is recommended to develop an intelligent education platform to dynamically monitor educational outcomes through digital means. Lastly, a multidisciplinary collaboration mechanism needs to be established to deeply integrate modules such as dietary management and exercise guidance with clinical treatment. These improvement measures will help break through the long-standing bottleneck of achieving target serum uric acid levels in gout management in our country, providing empirical evidence for the innovation of chronic disease management models.
Advantages
This study introduces an innovative approach to gout management by applying a theme-based nursing education model specifically designed to address the unique challenges of gout treatment, such as adherence to ULT and understanding self-management practices. While nurse-led education models have been explored in other chronic conditions – and a recent study published in The Lancet by Doherty et al demonstrated the efficacy of nurse-led treat-to-target strategies for gout29 – our study differs by implementing a structured thematic model focused on specific educational themes, including acute gout attack recognition, dietary guidance, exercise and psychological support. The theme-based nursing education model in this study surpasses conventional patient education by engaging patients through interactive, theme-based sessions tailored to their specific needs. This approach provides a more comprehensive understanding of gout-specific management compared with generalised nurse-led interventions.
By incorporating focused themes, this study presents a novel patient education strategy that is more personalised and adaptable to individual patient needs than standard care or broader nurse-led approaches. Future studies could expand on these findings by examining the long-term effects of thematic education in managing gout and other chronic diseases where patient self-management is crucial.
Limitations
This study has limitations such as a small sample size, single-center design, and short follow-up period, which may affect the generalizability of the results and the assessment of long-term effects. The single-center design restricts the external validity of the study, making it difficult to represent situations in different regions and medical environments. The short follow-up period prevents the observation of long-term effects and potential side effects. Future research should expand the sample size and include a more diverse group of participants to enhance the representativeness and generalizability of the results. Multicenter collaboration can improve the breadth and applicability of the study. Extending the follow-up period is necessary to comprehensively evaluate long-term effects and stability. Additionally, detailed records of medication adherence and adjustments should be maintained to ensure data integrity and analytical accuracy. Through these improvements, the effectiveness of theme-based nursing education can be more accurately validated.
Conclusion
This study confirms the significant advantages of theme-based nursing education in gout management, with its practical significance lying in providing patients with a more effective and personalized care plan. Through targeted education, patients can better control their condition, reduce the burden of acute attacks, and enhance their quality of life. This result highlights the core value of patient education in gout management and provides a new direction for clinical nursing practice. Meanwhile, the precision, participation, and practicality of this model give it immense potential for broader application. Its structured, patient-centered characteristics make it easy to promote among different medical institutions and patient groups. If implemented on a larger scale, it is expected to significantly improve the overall level of gout management and reduce the burden on social healthcare. Therefore, theme-based nursing education is not only worthy of clinical promotion but also represents an important development direction for future gout management.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu R, Han C, Wu D, et al. Prevalence of hyperuricemia and gout in mainland china from 2000 to 2014: a systematic review and meta-analysis. Biomed Res Int. 2015;2015:762820. doi:10.1155/2015/762820
2. Huang J, Ma ZF, Zhang Y, et al. Geographical distribution of hyperuricemia in mainland China: a comprehensive systematic review and meta-analysis. Glob Health Res Policy. 2020;5(1):52. doi:10.1186/s41256-020-00178-9
3. Robinson PC, Schumacher HR Jr. A qualitative and quantitative analysis of the characteristics of gout patient education resources. Clin Rheumatol. 2013;32(6):771–778. doi:10.1007/s10067-013-2168-8
4. Luo H, Fang WG, Zuo XX, et al. The clinical characteristics, diagnosis and treatment of patients with gout in China. Zhonghua Nei Ke Za Zhi. 2018;57(1):27–31. doi:10.3760/cma.j.issn.0578-1426.2018.01.005
5. Li QH, Dai L, Li ZX, et al. Questionnaire survey evaluating disease-related knowledge for 149 primary gout patients and 184 doctors in South China. Clin Rheumatol. 2013;32(11):1633–1640. doi:10.1007/s10067-013-2333-0
6. Rees F, Hui M, Doherty M. Optimizing current treatment of gout. Nat Rev Rheumatol. 2014;10(5):271–283. doi:10.1038/nrrheum.2014.32
7. Stamp LK, Merriman TR, Barclay ML, et al. Impaired response or insufficient dosage? Examining the potential causes of “inadequate response” to allopurinol in the treatment of gout. Semin Arthritis Rheumatism. 2014;44(2):170–174. doi:10.1016/j.semarthrit.2014.05.007
8. Kuo CF, Grainge MJ, Mallen C, et al. Rising burden of gout in the UK but continuing suboptimal management: a nationwide population study. Ann Rheumatic Dis. 2015;74(4):661–667. doi:10.1136/annrheumdis-2013-204463
9. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American diabetes association, the American association of diabetes educators, and the academy of nutrition and dietetics. Diabetes Care. 2015;38(7):1372–1382. doi:10.2337/dc15-0730
10. Mills KT, Obst KM, Shen W, et al. Comparative effectiveness of implementation strategies for blood pressure control in hypertensive patients: a systematic review and meta-analysis. Ann Internal Med. 2018;168(2):110–120. doi:10.7326/M17-1805
11. Neogi T, Jansen TL, Dalbeth N, et al. 2015 gout classification criteria: an American college of rheumatology / European league against rheumatism collaborative initiative. Ann Rheumatic Dis. 2015;74(10):1789–1798. doi:10.1002/art.39254
12. Smolen JS, Landewe RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi:10.1136/annrheumdis-2019-216655
13. Xue X, Yuan X, Han L, et al. Effect of clinical typing on serum urate targets of benzbromarone in Chinese gout patients: a prospective cohort study. Front Med Lausanne. 2022;8:806710. doi:10.3389/fmed.2021.806710
14. Latif ZP, Nakafero G, Jenkins W, Doherty M, Abhishek A. Implication of nurse intervention on engagement with urate-lowering drugs: a qualitative study of participants in a RCT of nurse led care. Joint Bone Spine. 2019;86(3):357–362. doi:10.1016/j.jbspin.2018.10.008
15. Zhang LY, Schumacher HR, Su HH, et al. Development and evaluation of a survey of gout patients concerning their knowledge about gout. J Clin Rheumatol. 2011;17(5):242–248. doi:10.1097/RHU.0b013e318228b4e2
16. Johnston ME, Treharne GJ, Chapman PT, et al. Patient information about gout: an international review of existing educational resources. J Rheumatol. 2015;42(6):975–978. doi:10.3899/jrheum.141442
17. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE Open Med. 2016;4:2050312116671725. doi:10.1177/2050312116671725
18. Lorenzo JPP, Sollano MHMZ, Salido EO, et al. 2021 Asia-Pacific league of associations for rheumatology clinical practice guideline for treatment of gout. Int J Rheum Dis. 2022;25(1):7–20. doi:10.1111/1756-185X.14266
19. Wang L, Mesa-Eguiagaray I, Campbell H, et al. A phenome-wide association and factorial Mendelian randomization study on the repurposing of uric acid-lowering drugs for cardiovascular outcomes. Eur J Epidemiol. 2024;39(8):869–880. doi:10.1007/s10654-024-01138-0
20. Dalbeth N, Petrie KJ, House M, et al. Illness perceptions in patients with gout and the relationship with progression of musculoskeletal disability. Arthritis Care Res. 2011;63(11):1605–1612. doi:10.1002/acr.20570
21. Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheumatic Dis. 2017;76(1):29–42. doi:10.1136/annrheumdis-2016-209707
22. Cohen RE, Pillinger MH, Toprover M. Something old, something new: the acr gout treatment guideline and its evolution from 2012 to 2020. Curr Rheumatol Rep. 2020;23(1):4. doi:10.1007/s11926-020-00967-8
23. Perez-Ruiz F, Moreno-Lledó A, Urionagüena I, et al. Treat to target in gout. Rheumatology. 2018;57(suppl_1):i20–i26. doi:10.1093/rheumatology/kex442
24. Xinping T, Xiaofeng Z. Strengthening long-term standardized gout management improves long-term prognosis of patients with gout. Zhejiang Med J. 2017;39(4):243–244.
25. Stamp LK, Dalbeth N. Critical appraisal of serum urate targets in the management of gout. Nat Rev Rheumatol. 2022;18(10):603–609. doi:10.1038/s41584-022-00816-1
26. Rees F, Jenkins W, Doherty M. Patients with gout adhere to curative treatment if informed appropriately: proof-of-concept observational study. Ann Rheumatic Dis. 2013;72(6):826–830. doi:10.1136/annrheumdis-2012-201676
27. Khanna PP, Perez-Ruiz F, Maranian P, et al. Long-term therapy for chronic gout results in clinically important improvements in the health-related quality of life: short form-36 is responsive to change in chronic gout. Rheumatology. 2011;50(4):740–745. doi:10.1093/rheumatology/keq346
28. Wilson L, Saseen JJ. Gouty arthritis: a review of acute management and prevention. Pharmacother J Human Pharmacol Drug Ther. 2016;36(8):906–922. doi:10.1002/phar.1788
29. Doherty M, Jenkins W, Richardson H, et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: a randomised controlled trial. Lancet. 2018;392(10156):1403–1412. doi:10.1016/S0140-6736(18)32158-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.