Back to Journals » Journal of Pain Research » Volume 18
Effect of Succinylcholine on Postoperative Sore Throat in Hysteroscopic Surgery with Laryngeal Mask Airway (LMA): A Randomized Trial
Authors Deng X, Hao X, Bi Y, Li H ![]() , Lin X
, Lin X ![]()
Received 23 September 2024
Accepted for publication 25 November 2025
Published 8 December 2025 Volume 2025:18 Pages 6607—6616
DOI https://doi.org/10.2147/JPR.S497466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Xiao Deng,1,2 Xin Hao,1,2 Yanmei Bi,1,2 Hao Li,1,2 Xuemei Lin1,2
1Department of Anesthesiology, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Ministry of Education, Chengdu, Sichuan, People’s Republic of China
Correspondence: Xuemei Lin, Department of Anesthesiology, West China Second University Hospital, Sichuan University, 20, Section 3, Renmin South Road, Wuhou District, Chengdu, People’s Republic of China, Tel +86 15982261680, Email [email protected] Hao Li, Department of Anesthesiology, West China Second University Hospital, Sichuan University, 20, Section 3, Renmin South Road, Wuhou District, Chengdu, People’s Republic of China, Tel +86 18190963549, Email [email protected]
Objective: This study aimed to evaluate the impact of succinylcholine on the incidence of postoperative sore throat (POST) in patients undergoing hysteroscopy under laryngeal mask airway (LMA)-assisted general anesthesia.
Design: A prospective, randomized, double-blind clinical study.
Setting: A tertiary-level hospital.
Patients: Out of 154 screened patients, 144 completed the study. Participants were those undergoing daytime hysteroscopic surgery under LMA-assisted general anesthesia.
Interventions: Patients were randomly assigned to receive either succinylcholine group (Group S) or 0.9% saline (Group N) during anesthesia induction. Groups S received succinylcholine at 1 mg/kg, while Group N received an equal volume of 0.9% saline.
Primary and Secondary Outcomes: The primary outcome was the incidence of POST 24 hours postoperatively. Secondary outcomes included the incidence of POST in the post-anesthesia care unit (PACU) and at 6 hours postoperatively.
Results: Of the 144 participants, 76 were in Groups S and 68 in Group N. The incidence of POST at 24 hours was significantly higher in Group S compared to Group N (57.90% vs 29.40%, P = 0.001). Additionally, the LMA insertion time was shorter in Group S [34.00 (28.50– 40.00) vs 36.00 (30.00– 50.00), P = 0.048], and LMA insertion conditions were improved in Group S (Group S vs N: 76/0/0 vs 48/18/2, P < 0.001). Binary logistics regression analysis, adjusted for age, revealed that the risk of POST was approximately 2.62 times higher in Group S compared to Group N (OR:2.62, 95% CI: 1.27– 5.40, P = 0.009).
Conclusion: The administration of succinylcholine (1 mg/kg) during LMA-assisted general anesthesia was associated with an increased risk of POST 24 hours postoperatively. Further longitudinal research with extended follow-up is warranted to explore the relationship between succinylcholine-induced myalgia and POST development.
Trial Registration Number: ChiCTR2200056918.
Keywords: laryngeal mask airway, postoperative sore throat, sore throat, succinylcholine
Introduction
Hysteroscopy has been widely used for the treatment of various intrauterine diseases, including adenomyosis, endometrial polyps, endometrial tumors, uterine septum surgery, intrauterine adhesions, and fallopian tube obstructions.1–4 Advances in surgical technology and innovative equipment have reduced trauma and accelerated recovery for patients undergoing hysteroscopic procedures. However, young female patients, such as those undergoing hysteroscopy, are associated with a higher incidence of POST. Follow-up data from our hospital indicated that the primary anesthesia-related complication for patients undergoing hysteroscopic surgeries was POST, with an incidence rate as high as 45% (internal audit).
POST is a common complication following general anesthesia, often presenting as a sore throat, that can impact patients’ ability to chew or speak in severe cases. The incidence of POST in tracheal intubation and LMA patients was 14.4%-50%5–7 and 5.8%-30%,8,9 respectively. POST is generally self-limiting and associated with few serious adverse effects, it has historically been overlooked as a minor postoperative complication. However, with the advent of enhanced recovery after surgery (ERAS) protocols and a heightened focus on patient comfort, POST has recently garnered enormous attention.10–12
The occurrence of POST is commonly related to the compression and mechanical injury to the laryngeal mucosa.5 Hysteroscopy, a brief procedure with minimal surgical stimulation and trauma, is typically performed under LMA anesthesia with short-acting anesthetic agents in our hospital. Despite being a short procedure, we often use succinylcholine in hysteroscopic procedures to ensure optimal conditions, which includes preventing any coughing or patient movement, but its benefits come with potential side effects. Succinylcholine-induced muscle fasciculations and myalgias represent a plausible mechanism for postoperative sore throat, even in the absence of direct airway trauma. Previous studies in patients undergoing endotracheal intubation have reported that succinylcholine, the only depolarizing muscle relaxant in clinical use, is associated with a higher incidence of POST compared with non-depolarizing neuromuscular blocking agents or no relaxant.7,13–15 This association, initially highlighted in early investigations such as the classic study by Capan et al7 lends plausibility to the hypothesis that succinylcholine may similarly contribute to POST following LMA placement—a connection that has not been previously examined. However, the impact of succinylcholine on POST in patients with LMA has not been explored to date. Thus, the association of succinylcholine usage with a higher POST incidence remains unknown. Therefore, our study aimed to investigate whether succinylcholine increases the incidence of POST in patients undergoing LMA anesthesia.
Methods
This double-blind, randomized controlled trial was registered with the Chinese Registry of Clinical Trials (registration number: ChiCTR2200056918). The study was also approved by the Medical Ethics Committee of West China Second University Hospital, Sichuan University (Chairperson Prof. Yiling Xing) on 5 September 2022 (Ethical number: 2022 No. (178)). Written informed consent was obtained from all participants. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and followed the Consolidated Standard of Reporting Trails (CONSORT) guidelines.
Participants
Participants were selected from various daytime hysteroscopic surgeries, including endometrial polypectomy, uterine adhesion treatment, abnormal uterine bleeding management, and submucosal hysteroscopic myomectomy, performed from August to December 2022 at West China Second University Hospital, Sichuan University. Following approval from the ethics committee, written informed consent was obtained from all participants before their inclusion.
The inclusion criteria specified patients aged from 18 to 55 years with a body mass index (BMI) between 16 and 28 kg·m–2, classified as American Society of Anesthesiologists (ASA) physical status I or II, and those who fully understood the study’s content. The exclusion criteria included patients with an interincisal distance less than 3 cm, those at high risk of reflux aspiration (eg, satiety, gastroesophageal reflux disease, or hiatal hernia), patients with laryngeal lesions (hematoma, edema, inflammation), individuals contraindicated for succinylcholine usage (eg, cerebral hemorrhage, glaucoma, hyperkalemia, and personal or family history of malignant high fever), patients with pulmonary diseases [eg, chronic obstructive pulmonary disease (COPD), asthma], and those who had undergone invasive ventilation within the past 30 days.
Randomization and Blinding
Patients were randomly assigned into two groups via electronic randomization: the succinylcholine group (Group S) and the normal saline group (Group N). The group assignment details were concealed in sequentially numbered opaque envelopes. After receiving the sealed envelopes, the anesthesia nurses were asked to prepare the experimental drugs according to the group allocations. Both the patients and anesthesiologists were blinded to the group assignments. While one anesthesiologist performed anesthesia induction and LMA insertion, another collected data and interviewed the patients about POST or hoarseness.
Anesthesia Protocol
A total of 148 subjects were randomly assigned to receive either succinylcholine (1 mg/kg) or 0.9% saline (control) via computer-generated randomization blocks. All subjects received intravenous metoclopramide (10 mg) as premedication and underwent standard clinical monitoring. Following 5–6 min of preoxygenation with a face mask (oxygen flow: 6L/min), anesthesia was induced with fentanyl (2 µg/kg) and propofol (2.5 mg/kg) in both groups. Group S received succinylcholine while Group N received 0.9% saline equivalent in volume. Anesthesia maintenance was achieved with continuous propofol infusion initiated at 10mg/kg/h with real-time titration by the attending anesthesiologist based on hemodynamic responses (eg, blood pressure, heart rate) and clinical signs of anesthetic depth. To ensure blinding, anesthesiologists temporarily exited the operating room during drug administration and returned only for LMA insertion. LMA placement criteria required: 1. Loss of consciousness (no response to verbal commands); 2. Apnea (absence of spontaneous respirations); 3. Jaw relaxation (assessed via mandibular mobility test). Patients meeting these criteria were positioned supine, and a fully lubricated paraffin LMA (size 3.0#, double chamber) was inserted by the same anesthesiologist. LMA insertion conditions were evaluated according to modified Scheme of Lund and Stovener:16 “Excellent”—No gagging or coughing, no patient movement, and no laryngospasm; “Good”—Mild-to-moderate gagging or coughing, mild-to-moderate patient movement, and no laryngospasm; “Poor”—Moderate-to-severe gagging or coughing, moderate-to-severe patient movement, no laryngospasm; “Unacceptable”—Severe gagging or coughing, severe patient movement, laryngospasm. If intubating conditions were “unacceptable”, or if clinical signs suggested inadequate anesthesia (eg, limb movement, cough, tachycardia, or a systolic blood pressure increase exceeding 20% of the preinduction value), supplemental intravenous propofol (0.5mg/kg) was administered. No supplemental intraoperative or postoperative opioids or non-opioid analgesics were administered until after the 24-hour POST assessment was complete.
After the operation, the follow-up blinded investigator asked the patients if they had sore throat. If the patient answered “Yes”, it was considered that the patient had POST, and the pain degree was scored using the visual analogue scale (VAS). Follow-up assessments at 6 and 24 hours were performed by the blinded investigator via telephone interviews. Patients were considered lost to follow-up and excluded from analysis if they were unreachable by telephone on all three pre-specified follow-up attempts. In PACU, if necessary, patients with POST and VAS≥4 points were given intravenously 8mg of lornoxicam or 1mg/kg tramadol after excluding related contraindications. If the patients have been discharged from the hospital, POST was managed conservatively with warm saline gargles and, if needed, oral nonsteroidal anti-inflammatory drugs (NSAIDs). Both the patients and anesthesiologists remained blinded to the group assignments.
Data Collection
Age, body mass index (BMI), Mallampati score, interincisal distance, fentanyl dosage, and duration of LMA in situ were recorded as demographic and perioperative variables. The incidence of POST at 24 h postoperatively was designed as the primary outcome. The incidence of POST in the PACU (within approximately 2 h postoperatively) and at 6 hours postoperatively were considered secondary outcomes. Additional outcomes included LMA insertion time, LMA insertion condition, first-attempt success, presence of bloodstain on the LMA, and recovery duration.
Sample Size
Due to the lack of relative studies between succinylcholine and POST in LMA anesthesia patients, we firstly conducted a pilot study including 40 subjects for evaluating sample size. The incidence of POST was 73.1% and 45.8% in Groups S and N respectively in the pilot study. With a significance level (α) of 0.05 (two-sided), and a test power (1-β) of 80%, the required sample size was determined to be 130, accounting for a 5% loss of follow-up. The calculation was performed using PASS 15.0 software.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 software (IBM, Armonk, NY, USA). The Shapiro–Wilk and Kolmogorov–Smirnov tests assessed the normality of the data distribution. Continuous data with normal distribution (eg, age and BMI) were reported as mean±standard deviation (SD) and compared using a two-sided independent t-test for equal variances. Non-normally distributed interval and ordinal data were reported as median (interquartile range [IQR]) and were analyzed with the Mann–Whitney U-test. Categorical data were assessed using the either χ2 or the Fisher’s exact test, depending on the expected frequencies.
Results
A total of 154 patients were assessed for eligibility, with six patients were excluded for not meeting the inclusion criteria. The remaining 148 participants were randomized into either Group S (n = 76) or Group N (n = 72). Four participants in Group N were lost to follow-up resulting in 144 participants being included in the final analysis. The participants selection process is illustrated in Figure 1.
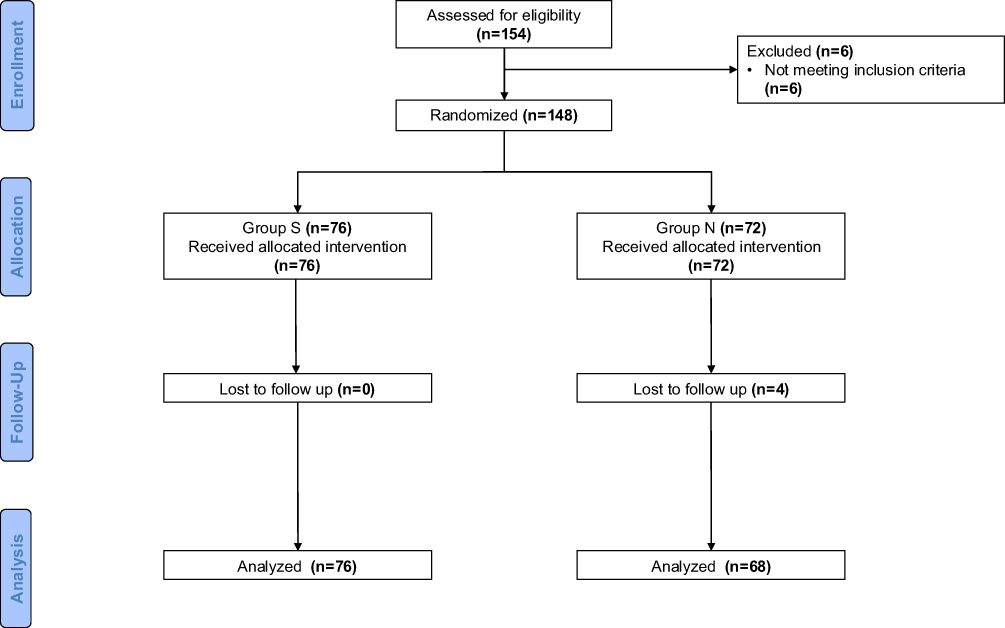 |
Figure 1 CONSORT flow diagram. Abbreviations: Group S, succinylcholine group; Group N, normal saline group; CONSORT, Consolidated Standard of Reporting Trails. |
Demographic and Perioperative Characteristics
Table 1 presents the demographic and perioperative characteristics of the study participants. There were no significant differences between Group S and Group N in terms of BMI, Mallampati score, interincisal distance, fentanyl dosage, or the duration of LMA duration in situ was observed. However, a significant difference in age between the two groups [Group S vs Group N: 33 (30–36) vs 37 (32–42), P <0.001].
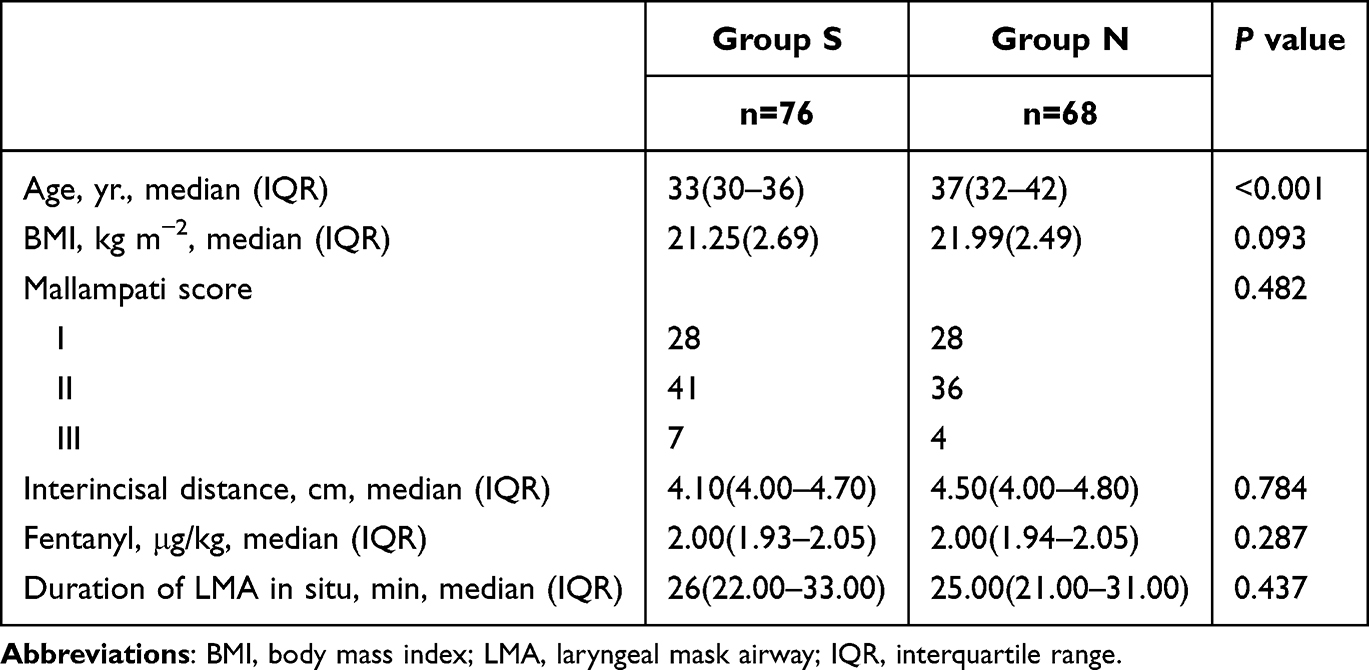 |
Table 1 Demographic and Perioperative Characteristics |
Primary and Secondary Outcomes
Group S exhibited a higher incidence of POST at 24 h postoperatively compared to Group N (Group S vs Group N: 57.9% vs 29.4%, P = 0.001). However, no significant difference in POST incidence was observed at the PACU or 6 h postoperatively (Table 2). The trend of POST incidence over different follow-up times is shown in Figure 2. As visualized in Figure 2, the incidence of POST was comparable between the Group S and Group N immediately upon arrival in the PACU. However, the trajectories diverged over time, with Group S demonstrating a clear increase in POST incidence, culminating in a significantly higher rate at the 24-hour postoperative assessment. The incidence of hoarseness, which was found to be low and not significantly different between groups. No clinically significant adverse events were observed in either group during the study period.
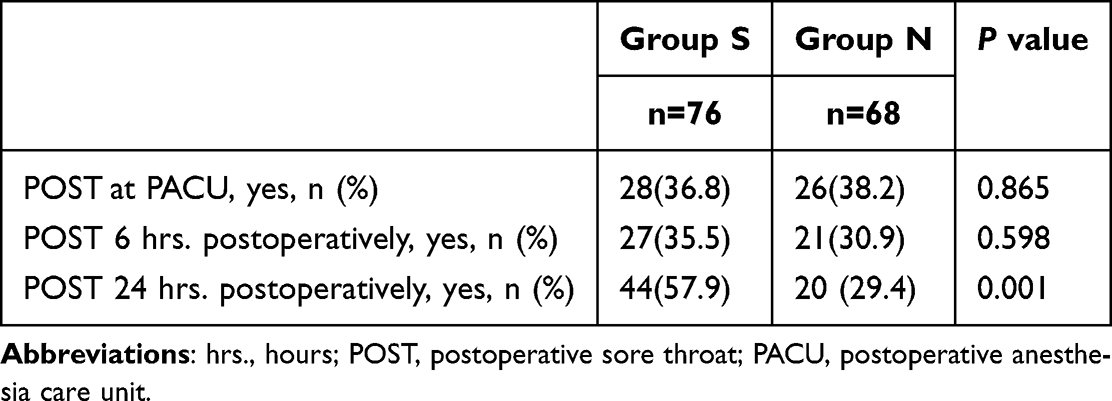 |
Table 2 Primary and Secondary Outcomes of the Study |
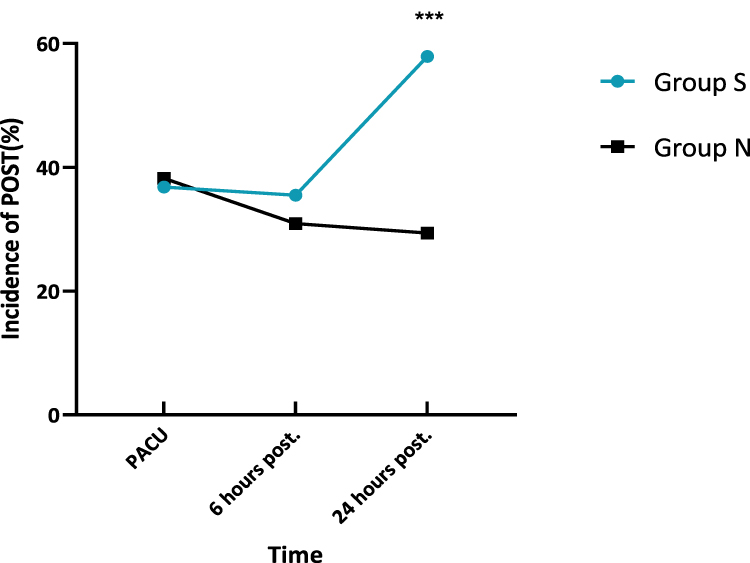 |
Figure 2 The trends of the incidence of POST. *** P=0.001. Abbreviations: POST, postoperative sore throat; PACU, postoperative anesthesia care unit; post., postoperatively. |
Additional Outcomes
Succinylcholine significantly reduced the LMA insertion time [Group S vs Group N: 34.00 (28.50–40.00) vs 36.00 (30.00–50.00), P = 0.048] and improve the LMA insertion conditions (Group S vs Group N: 76/0/0/0 vs 48/18/2/0, P < 0.001). However, no significant difference was observed in the first-attempt success rate [Group S vs Group N: 72 (93.4) vs 59 (86.8), P = 0.260], nor was there a reduction in bloodstains on the LMA [Group S vs Group N: 32 (42.1) vs 33 (48.5), P = 0.504, Table 3].
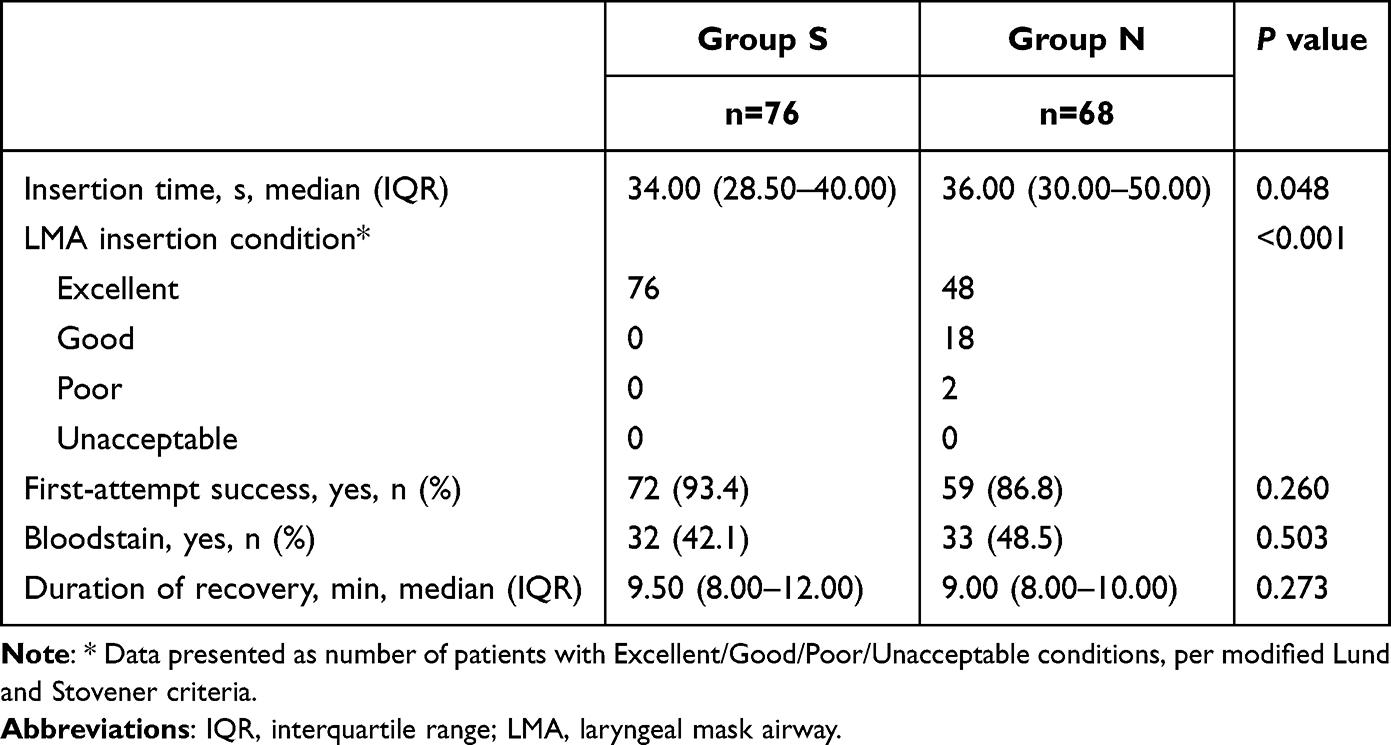 |
Table 3 Additional Outcomes of the Study |
Binary Logistic Regression
Given that the patient’s age in both groups showed a significant difference, and age was inversely proportional to the incidence of POST,14,17–19 the binary logistic regression analysis after age adjustments revealed that the administration of succinylcholine significantly increased the risk of POST [OR (95% CI): 2.62 (1.27–5.40), P = 0.009, Table 4].
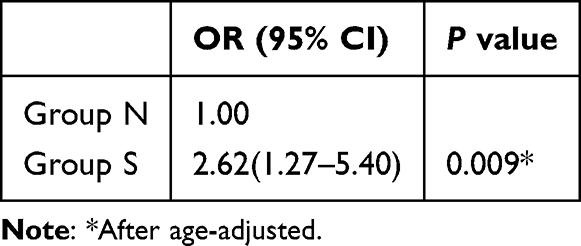 |
Table 4 Binary Logistic Regression (Age-Adjusted) |
Discussion
Our study indicated that, compared with Group N, succinylcholine (1mg/kg) significantly improved LMA insertion conditions and reduced the LMA insertion time during hysteroscopy. The clinical relevance of this 2-second difference in a controlled, elective setting is likely marginal, but the superior insertion condition in Group S, characterized by a complete absence of coughing and resistance, appears to be the primary clinical advantages that may enhance the safety and quality of the induction sequence, particularly in patients who need to avoid sudden changes in hemodynamics is critical.
Our findings reveal a fascinating temporal pattern in POST incidence (Figure 2). The comparable POST rates between two groups upon PACU arrival suggest that initial, direct trauma from LMA insertion was equivalent. The significant divergence that emerged by 24 hours in the succinylcholine group, however, points to a distinct, delayed mechanism. This time course aligns with the known pathophysiology of succinylcholine-induced myalgia, which involves microscopic muscle damage and a subsequent inflammatory response that peaks hours after administration.20 It is therefore plausible that the delayed POST observed in our study represents a localized manifestation of this same process, specifically affecting the pharyngeal and laryngeal musculature.
Postoperative myalgia (POM), a main side effect of succinylcholine resulting from muscle damage,21–24 can persist for several days and be a troublesome symptom for patients.20,25 Succinylcholine administration can induce tonic muscle contractions,26 which may result in muscle fibrillation. The uncoordinated muscle contractions generate shear stresses between muscle fibers, resulting in muscle fiber damage and fractures.27,28 It also can cause lactic acid accumulation, contributing to postoperative muscle soreness. This phenomenon may explain why POM is often described as myalgia following “unaccustomed exercise”.20,29
Furthermore, increased serum potassium levels might also contribute to POM. The damaged muscle fiber following muscle fibrillation can lead to hyperkalemia, which, in turn, can exacerbate POM.30,31 Additionally, Figure 2 indicates that the incidence of POST in Group S significantly increased from 6h to 24h postoperatively rather than earlier postoperatively, thus we supposed that POST in Group S was not associated with mechanical injury but with the changes of serum biochemical substances. However, no correlation has been found between the severity of muscle fasciculations, serum potassium changes, and the incidence of POM.20
Generally, muscle relaxants paralyze the vocal cords, minimize post-intubation coughing and bucking, improve intubation conditions, and reduce the incidence of POST.32 It is plausible that by suppressing cough and patient movement, muscle relaxation reduces immediate mechanical trauma to the pharyngeal mucosa, thereby exerting a protective effect on early POST. However, the association we observed between succinylcholine and POST at 24 hours suggests a different, time-dependent mechanism. We propose that the unique side effect of succinylcholine-induced myalgia manifests as a later-onset, referred pain in the throat region, which becomes the predominant contributor to POST after the resolution of early mechanical irritation. This distinction in the timing of assessment and the underlying pathophysiology likely accounts for the differing results across studies.
This is the first study to investigate the relationship between succinylcholine and POST in patients undergoing LMA-assisted general anesthesia. In contrast, previous studies have primarily focused on POST in patients with tracheal intubation. The incidence of POST is lower in patients using LMA than those with tracheal intubation.5–9 Additionally, POST following tracheal intubation differs from LMA-induced POST in terms of pain location, mechanism of injury, and relative risk factors. POST following LMA placement is associated with the type of LMA, insertion techniques, and the use of local anesthetic in lubricants applied to the LMA.33 In our study, all patients were inserted with the same type of deflated LMA, lubricated with aqueous gel, to prevent pharyngeal mucosa injuries caused by the folds formed after LMA inflation,9,34,35 and to enhance the LMA insertion success rates.36–39 As a result, this study minimized the influence of these confounding factors. It is important to note that our findings are specific to the standard intubating dose of succinylcholine (1 mg/kg) used in this study. Future investigations are warranted to explore a potential dose-response relationship between succinylcholine and POST. Specifically, comparing the efficacy and side effect profile of standard-dose versus lower (eg, 0.3–0.5 mg/kg) would be highly valuable. Such research could determine if a lower dose provides a superior therapeutic ratio, achieving satisfactory intubating conditions while minimizing the dose-dependent side effect of myalgia and its contribution to delayed POST.
Initially, we proposed that succinylcholine-induced LMA in patients undergoing general anesthesia poses a higher risk of POST, thereby providing clinical guidelines for its usage. Furthermore, it is important to note that our study cohort consisted exclusively of young female patients undergoing short-duration anesthesia for elective gynecological surgery. Therefore, the generalizability of our findings may be limited to this specific demographic and surgical context. The incidence and mechanisms of POST might differ in procedures of longer duration, in surgeries that inherently cause significant throat irritation, or in other patient populations. Our conclusions are thus most directly applicable to short, ambulatory cases managed with an LMA. Given its adverse effects, such as bradycardia, increased secretions, hyperkalemia, and POM,20,40,41 succinylcholine should be avoided in surgery when sufficient analgesia and sedation are available. If succinylcholine is necessary to improve intubation conditions during short operations, we recommend pre-treatment strategies, including non-depolarizing muscle relaxants, lidocaine, parecoxib, or magnesium, to mitigate the incidence and severity of succinylcholine-induced POM.25,42
This study has several limitations. First, all enrolled subjects were young and females, demographically belonging to the high-risk POST populations. Thus, future research involving other surgical interventions and patient groups should be conducted to verify our study results. Second, we did not record the specific regions and degrees of myalgia, which could have provided a clearer understanding of the relationship between POM and POST. Last, further studies are required to explore the incidence of sore throats beyond the 24-hour postoperative period.
Strengths and Limitations of This Study
- This is the first study to explore the relationship between succinylcholine and POST in patients under LMA-assisted general anesthesia.
- This study showed that the administration of succinylcholine would significantly increase the risk of POST in patients under LMA-assisted general anesthesia.
- The study provided a clinical guideline for succinylcholine usage in short day and ambulatory surgeries.
- All enrolled subjects were young and females who were high-risk POST populations. Thus, future research involving other surgical interventions and patient groups should be conducted to verify our study results.
- Our study did not record the regions and degree of myalgia, which could have strongly reflected the relationship between postoperative myalgia and POST and further studies are required to explore the incidence of sore throat beyond postoperative 24 hours.
Conclusion
In young female patients undergoing short gynecological procedures with an LMA, succinylcholine significantly improved insertion conditions but was associated with an increased incidence of POST at 24 hours. These findings suggest that, although succinylcholine may facilitate airway management, its routine use should be carefully weighed against the risk of POST-related morbidity. Future studies should explore strategies to mitigate this side effect and investigate alternative approaches for LMA insertion, including the role of extended follow-up in understanding the relationship between postoperative myalgia and POST.
Abbreviations
POST, Postoperative sore throat; LMA, Laryngeal mask airway; PACU, post-anesthesia care unit; ERAS, Enhanced recovery after surgery; CONSORT, Consolidated Standard of Reporting Trails; VAS, Visual analogue scale; NSAIDs, Nonsteroidal anti-inflammatory drugs; BMI, Body mass index; ASA, American Society of Anesthesiologists; COPD, Chronic obstruction pulmonary disease; SD, Standard deviation; IQR, Interquartile range; POM, Postoperative myalgia.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Loffer FD. The time has come to quit relying on a blind endometrial biopsy or dilation and curettage to rule out malignant endometrial changes. J Minim Invasive Gynecol. 2019;26(7):1207–1208. doi:10.1016/j.jmig.2019.04.011
2. Mollo A, De Franciscis P, Colacurci N, et al. Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: a prospective controlled trial. Fertil Steril. 2009;91(6):2628–2631. doi:10.1016/j.fertnstert.2008.04.011
3. Dakhly DMR, Abdel Moety GAF, Saber W, et al. Accuracy of hysteroscopic endomyometrial biopsy in diagnosis of adenomyosis. J Minimally Invasive Gynecol. 2016;23(3):364–371. doi:10.1016/j.jmig.2015.11.004
4. Török P, Major T. Accuracy of assessment of tubal patency with selective pertubation at office hysteroscopy compared with laparoscopy in infertile women. J Minimally Invasive Gynecol. 2012;19(5):627–630. doi:10.1016/j.jmig.2012.03.016
5. Mchardy FE, Chung F. Postoperative sore throat: cause, prevention and treatment. Anaesthesia. 1999;54(5):444–453. doi:10.1046/j.1365-2044.1999.00780.x
6. Joshi GP, Inagaki Y, White PF, et al. Use of the laryngeal mask airway as an alternative to the tracheal tube during ambulatory anesthesia. Anesth Analg. 1997;85(3):573–577. doi:10.1213/00000539-199709000-00016
7. Capan LM, Bruce DL, Patel KP, Turndorf H. Succinylcholine-induced postoperative sore throat. Anesthesiology. 1983;59(3):202–206.
8. Dingley J, Whitehead MJ, Wareham K. A comparative study of the incidence of sore throat with the laryngeal mask airway. Anaesthesia. 1994;49(3):251–254. doi:10.1111/j.1365-2044.1994.tb03434.x
9. Wakeling HG, Butler PJ, Baxter PJ. The laryngeal mask airway: a comparison between two insertion techniques. Anesth Analg. 1997;85(3):687–690. doi:10.1213/00000539-199709000-00037
10. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–298. doi:10.1001/jamasurg.2016.4952
11. Tong D, Chung F, Wong D. Predictive factors in global and anesthesia satisfaction in ambulatory surgical patients. Anesthesiology. 1997;87(4):856–864. doi:10.1097/00000542-199710000-00020
12. Flexman AM, Duggan LV. Postoperative sore throat: inevitable side effect or preventable nuisance? Can J Anaesth. 2019;66(9):1009–1013. doi:10.1007/s12630-019-01397-6
13. Alcock R, Peachey T, Lynch M, Mcewan T. Comparison of alfentanil with suxamethonium in facilitating nasotracheal intubation in day-case anaesthesia. Br J Anaesth. 1993;70(1):34–37. doi:10.1093/bja/70.1.34
14. Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J Anaesth. 2002;88(4):582–584. doi:10.1093/bja/88.4.582
15. Deacock SJ. Sore throat after suxamethonium. Br J Anaesth. 1993;71(1):164. doi:10.1093/bja/71.1.164-b
16. Lund I, Stovner J. Dose-Response curves for tubocurarine, alcuronium and pancuronium. Acta Anaesthesiol Scand Suppl. 1969;37:238–242. doi:10.1111/j.1399-6576.1970.tb00916.x
17. Jaensson M, Olowsson LL, Nilsson U. Endotracheal tube size and sore throat following surgery: a randomized-controlled study. Acta Anaesthesiologica Scandinavica. 2010;54(2):147–153. doi:10.1111/j.1399-6576.2009.02166.x
18. Biro P, Seifert B, Pasch T. Complaints of sore throat after tracheal intubation: a prospective evaluation. European J Anaesthesiol. 2005;22(4):307–311. doi:10.1017/S0265021505000529
19. Lundstrøm LH, Duez CH, Nørskov AK, et al. Avoidance versus use of neuromuscular blocking agents for improving conditions during tracheal intubation or direct laryngoscopy in adults and adolescents. Cochrane Database Syst Rev. 2017;5(5):CD009237. doi:10.1002/14651858.CD009237.pub2
20. Wong SF, Chung F. Succinylcholine-associated postoperative myalgia. Anaesthesia. 2000;55(2):144–152. doi:10.1046/j.1365-2044.2000.055002144.x
21. Bourne JG, Collier HOJ, Somers GF. Succinylcholine (Succinoylcholine) muscle-relaxant of short action. Lancet. 1952;259(6721):1225–1229. doi:10.1016/S0140-6736(52)92058-8
22. Paton WDM. The effects of muscle relaxants other than muscular relaxation. Anesthesiology. 1959;20(4):453–463. doi:10.1097/00000542-195907000-00006
23. Wig J, Bali IM. Relation of precurarization to suxamethonium to provide ease of intubation and to prevent post-suxamethonium muscle pains. Canadian Anaesthetists’ Soc J. 1979;26(2):94–98. doi:10.1007/BF03013776
24. Tsui BCH, Reid S, Gupta S, et al. A rapid precurarization technique using rocuronium. Can J Anaesthesia. 1998;45(5):397–401. doi:10.1007/BF03012573
25. Schreiber JU, Lysakowski C, Fuchs-Buder T, Tramèr MR. Prevention of succinylcholine-induced fasciculation and myalgia: a meta-analysis of randomized trials. Anesthesiology. 2005;103(4):877–884. doi:10.1097/00000542-200510000-00027
26. Booij LHDJ. Part 1: neuromuscular transmission and general aspects of its blockade. Pharm World Sci. 1997;19(1):1–12. doi:10.1023/A:1008694726564
27. Spence D, Domen-Herbert R, Boulette E, et al. A comparison of rocuronium and lidocaine for the prevention of postoperative myalgia after succinylcholine administration. Aana j. 2002;70(5):367–372.
28. Waters DJ, Mapleson WW. Suxamethonium pains: hypothesis and observation. Anaesthesia. 1971;26(2):127–141. doi:10.1111/j.1365-2044.1971.tb04753.x
29. Von Konig W. Complications after the use of succinylcholine] [J. Anaesthesist. 1956;5(2):50–53.
30. Moore WE, Watson RL, Summary JJ. Massive myoglobinuria precipitated by halothane and succinylcholine in a member of a family with elevation of serum creatine phosphokinase. Anesth Analg. 1976;55(5):680–682. doi:10.1213/00000539-197609000-00014
31. Collier CB. Suxamethonium pains and early electrolyte changes. Anaesthesia. 1978;33(5):454–461. doi:10.1111/j.1365-2044.1978.tb12464.x
32. Clergue F, Auroy Y, Péquignot F, et al. French survey of anesthesia in 1996. Anesthesiology. 1999;91(5):1509–1520. doi:10.1097/00000542-199911000-00045
33. L’Hermite J, Dubout E, Bouvet S, et al. Sore throat following three adult supraglottic airway devices: a randomised controlled trial. Eur J Anaesthesiol. 2017;34(7):417–424. doi:10.1097/EJA.0000000000000539
34. Brimacombe J, Berry A. Insertion of the laryngeal mask airway--a prospective study of four techniques. Anaesth Intensive Care. 1993;21(1):89–92. doi:10.1177/0310057X9302100121
35. Matta BF, Marsh DS, Nevin M. Laryngeal mask airway: a more successful method of insertion. J Clin Anesth. 1995;7(2):132–135. doi:10.1016/0952-8180(94)00027-2
36. Jeon YT, Na HS, Park SH, et al. Insertion of the ProSeal laryngeal mask airway is more successful with the 90 degrees rotation technique. Can J Anaesth. 2010;57(3):211–215. doi:10.1007/s12630-009-9241-4
37. Ghai B, Makkar JK, Bhardwaj N, Wig J. Laryngeal mask airway insertion in children: comparison between rotational, lateral and standard technique. Paediatr Anaesth. 2008;18(4):308–312. doi:10.1111/j.1460-9592.2008.02434.x
38. Hwang JW, Park HP, Lim YJ, et al. Comparison of two insertion techniques of ProSeal laryngeal mask airway: standard versus 90-degree rotation. Anesthesiology. 2009;110(4):905–907. doi:10.1097/ALN.0b013e31819b5d40
39. Dingley J, Asai T. Insertion methods of the laryngeal mask airway. A survey of current practice in Wales. Anaesthesia. 1996;51(6):596–599. doi:10.1111/j.1365-2044.1996.tb12575.x
40. AL-Takrouri H, Martin TW, Mayhew JF. Hyperkalemic cardiac arrest following succinylcholine administration: the use of extracorporeal membrane oxygenation in an emergency situation. J Clin Anesth. 2004;16(6):449–451. doi:10.1016/j.jclinane.2003.09.020
41. Baraka A. Severe bradycardia following propofol-suxamethonium sequence. Br J Anaesth. 1988;61(4):482–483. doi:10.1093/bja/61.4.482
42. Schreiber JU, Mencke T, Pradarutti S, et al. Does preoperatively administered parecoxib prevent succinylcholine-associated myalgia? A randomized, placebo-controlled trial. Eur J Anaesthesiol. 2006;23(4):332–337. doi:10.1017/S026502150600007X
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.