Back to Journals » Clinical Ophthalmology » Volume 13
Effect of Refresh Plus® preservative-free lubricant eyedrops on tear ferning patterns in dry eye and normal eye subjects
Authors Alanazi SA, Badawood YS, Aldawood MA, El-Hiti GA ![]() , Masmali AM
, Masmali AM ![]()
Received 24 April 2019
Accepted for publication 29 May 2019
Published 14 June 2019 Volume 2019:13 Pages 1011—1017
DOI https://doi.org/10.2147/OPTH.S213365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saud A Alanazi, Yousef S Badawood, Mohammed A Aldawood, Gamal A El-Hiti, Ali M Masmali
Cornea Research Chair, Department of Optometry, College of Applied Medical Sciences, King Saud University, Riyadh, 11433, Saudi Arabia
Purpose: To evaluate the tear ferning patterns in dry eye and normal eye subjects in the 3 hours following application of Refresh Plus® preservative-free lubricant eyedrops.
Methods: Thirty men with dry eye (mean age 22.14±2.34 years) and 30 age-matched men with normal eyes (mean age 23.91±3.24 years) were enrolled. Eyes were classified as normal or dry based on their Ocular Surface Disease Index score, tear meniscus height, and noninvasive tear breakup time. The tear ferning test was performed before and 30, 60, 120, and 180 minutes after application of a Refresh Plus eyedrop into the right eye in each subject.
Results: There was a significant change in tear ferning grade after application of Refresh Plus eyedrops (P=0.02, Wilcoxon test) in the group with dry eye, but not in the normal eye group (P=0.19, Wilcoxon test). The correlation of tear ferning grade was moderate (r=0.484, P=0.049) at 60 minutes after application of the eyedrops and strong at 120 minutes (r=0.560, P=0.019) and 180 minutes (r=0.726, P=0.001). There was also a strong correlation (r=0.865, P=0.001) between tear ferning grades obtained 120 and 180 minutes after application. In the normal eye group, there was a moderate (r=0.407, P=0.029) correlation between tear ferning grades obtained before and 60 minutes after application of the eyedrops. There was also a strong correlation (r=0.532, P=0.003) between tear ferning grades obtained 120 and 180 minutes after application.
Conclusion: Tear ferning patterns improved significantly after application of Refresh Plus preservative-free lubricant eyedrops in subjects with dry eye. Artificial tears containing sodium carboxymethylcellulose, such as Refresh Plus, can be used to improve tear ferning patterns in dry eye for at least 3 hours.
Keywords: dry eye, eyedrops, tear film, tear meniscus height
Plain language summary
This study was performed to determine the effect of Refresh Plus® preservative-free lubricant eyedrops on ocular tear film in patients with dry eye.
Tear ferning patterns obtained in subjects with dry eye improved significantly during 3 hours of observation after application of Refresh Plus preservative-free lubricant eyedrops. There was some improvement in the quality of tear ferning after application of artificial tears in normal eye subjects but the change was not statistically significant.
Artificial tears containing sodium carboxymethylcellulose, such as Refresh Plus, can improve ocular tear film in patients with dry eye for at least 3 hours after instillation.
Introduction
Tear film is a thin moist layer that covers and moisturizes the surface of the cornea.1 Upon blinking, the tear film spreads over the cornea to avoid drying of the ocular surface.2 Various factors affect the rate of spontaneous eye blinking, including stability of the tear film, thickness of the lipid layer, composition of meibum produced by the meibomian gland, and the eye-drying rate.3,4 Blink rate has been found to depend on age and high in infants and adults up to the age of 25 years.5,6 In adults, the meibum is less saturated, more oily, less ordered, and contains flexible chains of lipids, whereas in infants the meibum is highly saturated, stiff, and contains waxy lipids.7 Furthermore, there is more meibum in the lipid reservoir in adults than in infants.8 This explains why adults up to the age of 25 years have a higher rate of spontaneous eye blinking (15–30 blinks per minute) than infants (approximately four blinks per minute).9
Dry eye is a common ocular surface disorder that develops because of instability within the tear film, and causes uncomfortable symptoms in 5%–50% of the population worldwide.10 Dry eye can be caused by a high tear-evaporation rate, a deficiency in tear secretion, or both.10 Furthermore, a change in osmolarity of the ocular surface may occur, which can lead to apoptosis of cells on the epithelial surface and consequent loss of goblet cells that produce mucin.11,12 The symptoms of dry eye have a considerable impact on quality of life.13 Therefore, it is important to detect this condition as early as possible for optimal management.14 Given that eye dryness is complex and affected by a number of parameters, a combination of diagnostic tests, along with dry-eye questionnaires, such as the Ocular Surface Disease Index (OSDI), are needed for diagnosis. For example, tear-evaporation rate,15 Schirmer's test,16 phenol red thread,16 tear meniscus height (TMH),17 noninvasive tear breakup time (NITBUT),18 osmolarity,19 and the tear ferning (TF)20,21 test can be used to detect dry eye. Artificial tears can be used to lubricate the tear film and relieve some of the uncomfortable symptoms associated with moderate dry eye.22,23
Previous studies shown that the TF test can be used to assess the quality of tears in subjects with dry eye, including smokers,24 those with diabetes,25 subjects with normal eyes after consumption of a single dose of hot green tea26 or peppermint,27 and after oral vitamin A supplementation for 3 consecutive days.28 The aim of the present study was to compare TF patterns in the 3 hours following application of Refresh Plus® (Allergan, Marlow, UK) preservative-free lubricant eyedrops in dry- and normal eye subjects.
Methods
Subjects
Thirty men with dry eye (mean age 22.14±2.34 years) and 30 age-matched normal eye men (mean age 23.91±3.24 years) were enrolled. A slit lamp was used to examine abnormalities of the eyelids, eyelashes, conjunctiva, cornea, and iris. Subjects with no eyelid or lash abnormalities, those who had recently undergone ocular surgery or were receiving ophthalmic medication, contact-lens wearers, smokers, and patients with diabetes, anemia, or a thyroid disorder were excluded. OSDI and TMH scores and NITBUT test results were used to classify subjects as having or not having dry eye. The study was approved by the College of Applied Medical Sciences Ethics Committee, King Saud University and performed according to the tenets of the Declaration of Helsinki. Written informed consent was obtained from each study participant before commencement of the research. All tests were performed by the same examiner in an environment that was controlled for humidity (<40%) and temperature (23°C).25 After subjects had completed the OSDI questionnaire, the TMH, NITBUT, and TF tests were performed, with a 10-minute interval between each test.
Refresh Plus preservative-free lubricant eyedrops
Refresh Plus preservative-free lubricant eyedrops (30 single-use containers each containing 0.4 mL; Allergan, Marlow, UK) are aqueous-based artificial tears. The drops contain sodium carboxymethylcellulose (CMC) 0.5% as the active ingredient, as well as sodium lactate and various electrolytes, including sodium chloride, potassium chloride, magnesium chloride, and calcium chloride. They can be used to relieve symptoms of dry eye, ie, irritation, burning, and discomfort.22
Ocular Surface Disease Index
The OSDI was completed by each study participant first, and a score <13 was considered as normal eye.29
TMH and NITBUT tests
The TMH and NITBUT tests were performed in each subject’s right eye after completion of the OSDI, with a 5-minute interval between the two tests. Both tests were performed using a Keratograph 4 system (Oculus, Wetzlar, Germany). Fluorescein was added to the subject’s eye. For the NITBUT test, the subject was asked to refrain from blinking while the tear film was observed.30 A yellow barrier filter was used to enhance the visibility of tear-film breakup. TBUT was recorded as the number of seconds that elapsed between the last blink and the appearance of the first dry spot in the tear film. The inferior TMH images were captured and measured perpendicularly to the lid margin at the central point relative to the pupil center using an integrated ruler. Both tests were performed three times and average measurements recorded. The eye was defined as normal if the tear height in the lower lid was >0.2 mm for TMH and the TBUT was >10 seconds for NITBUT measurements.
Tear ferning test
A tear sample (1 μL) was collected from the lower meniscus of the right eye in each subject using a glass capillary tube (10 μL; Sigma-Aldrich; St Louis, MO, USA). The tear sample was dried at 23°C for 10 minutes at a humidity of <40%. A DP72 microscope (10× magnification; Olympus, Tokyo, Japan) was used to observe and capture the tear ferns. Each TF pattern was graded according to the 5-point TF-grading scale using increments of 0.1.21 The TF test was repeated for each subject at 30, 60, 120, and 180 minutes after application of the artificial eyedrops.
Statistical analysis
Data were tabulated using Excel (Office 2010; Microsoft, Redmond, WA, USA) and analyzed using SPSS version 22 (IBM, Armonk, NY, USA). The Spearman correlation coefficient was used to investigate relationships among the obtained data. Correlation coefficients was considered small (0.10‒0.29), moderate (0.30‒0.49), or large (0.50‒1).31
Results
Data collected from all tests were found not to be normally distributed (P˂0.05, Kolmogorov–Smirnov test); therefore, the median (IQR) was used to represent the average values. Median (IQR) scores for the OSDI and TMH, NITBUT, and TF tests in dry- and normaleye groups are shown in Table 1. There were significant differences (P<0.05, Wilcoxon test) in the OSDI scores and NITBUT measurements between dry- and normal eye subjects, but not significant between-group differences for TMH scores (P>0.05, Wilcoxon test). In the dry-eye group, there were significant differences (P˂0.05, Wilcoxon test) in TF grades obtained at the five different time points after administration of the eyedrops, but not in the normal eye group (P>0.05, Wilcoxon test).
 | Table 1 Median OSDI scores and TMH, NITBUT, and TF test results in dry eye and normal eye subjects |
Examples of the five TF images obtained from dry- and normal eye subjects before and 30–180 minutes after application of artificial tears are shown in Figure 1. Box plots for the TF scores on the tests are shown side by side for the dry- and normal eye groups in Figure 2.
 | Figure 1 Tear ferning (TF) images obtained before and after application of eyedrops in the right eye of (A) a dry-eye subject and (B) a normal eye subject. Notes: TF0-180, TF scores obtained 0-180 minutes after application of eyedrops. |
 | Figure 2 Box plots for tear ferning (TF) test scores in (A) dry-eye subjects and (B) normal eye subjects. Notes: TF0-180, TF scores obtained 0-180 minutes after application of eyedrops. |
Correlations between scores from the OSDI and TMH, NITBUT, and TF tests in dry- and normal eye groups are shown in Tables 2 and 3, respectively. In the group of subjects with dry eye, the correlation between the TF grades obtained before and after application of the eyedrops was moderate (r=0.484, P=0.049) at 60 minutes and strong at 120 minutes (r=0.560; P=0.019) and 180 minutes (r=0.726, P=0.001). There was a strong correlation (r=0.865, P=0.001) between TF grades obtained 120 and 180 minutes after application of the eyedrops. There was also a strong negative correlation (r=–0.542, P=0.025) between OSDI scores and TF grades obtained 60 minutes after application.
 | Table 2 Correlations between OSDI scores and TMH, NITBUT, and TF test results in subjects with dry eye — r (P-value) |
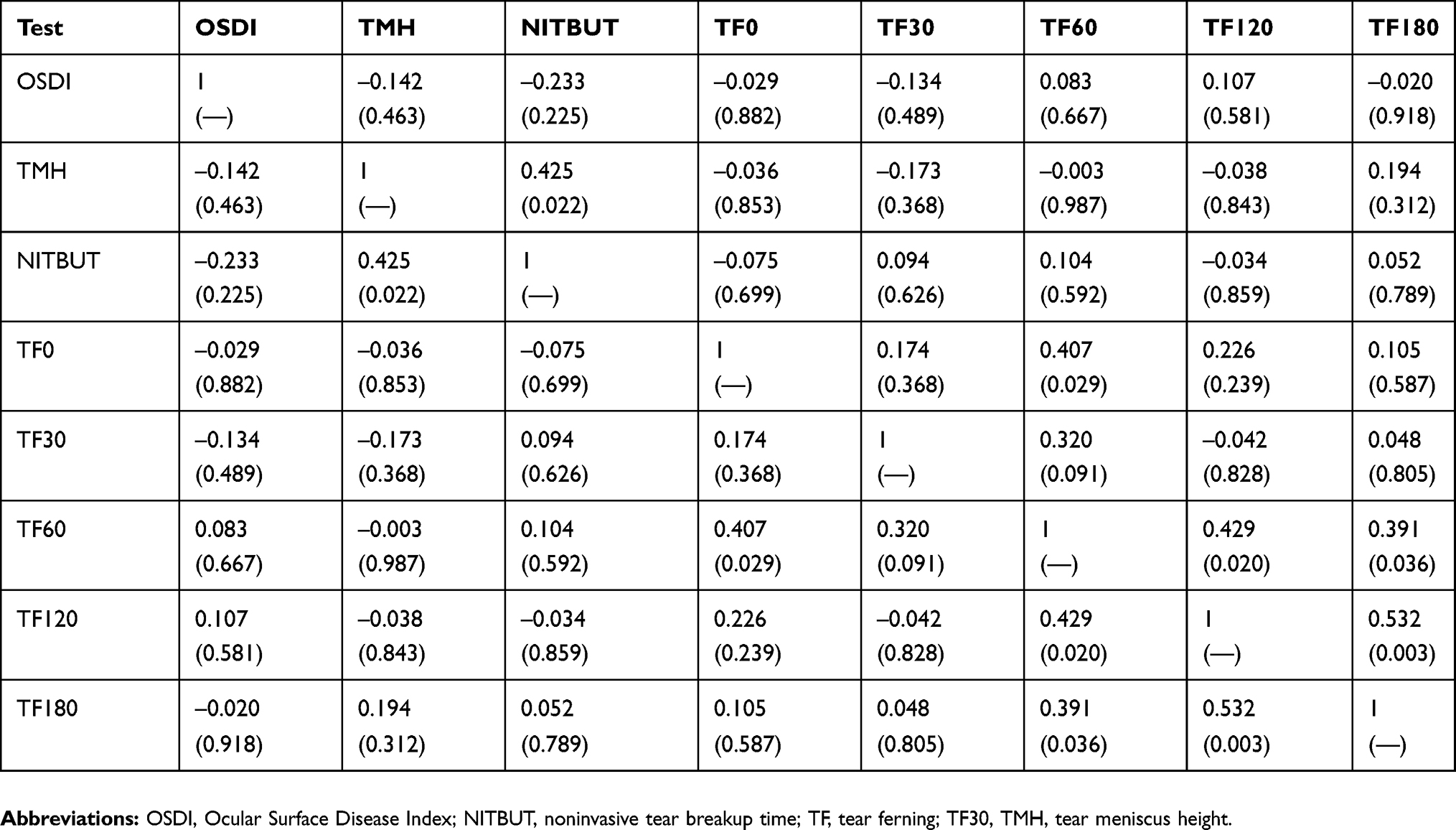 | Table 3 Correlations between OSDI scores and TMH, NITBUT, and TF test results in normal eye subjects — r (P-value) |
For normal eye subjects, there was a moderate correlation (r=0.407, P=0.029) between TF grades obtained before and 60 minutes after application of the eyedrops and a strong correlation (r=0.532, P=0.003) between those obtained 120 and 180 minutes after application. Furthermore, there was a moderate correlation (r=0.425, P=0.022) between TMH and NITBUT values.
Discussion
Dry eye is a common ocular problem that causes various uncomfortable symptoms. Artificial tears are the first choice for management of symptoms of dry eye. Indeed, most of the ocular discomfort, ie, inflammation, burning, itching, and dryness, can be relieved by the use of eye lubricants.32 Various types of eye lubricants with different pH, viscosity, physical, and chemical properties are available. Lubricants with a certain pH might be suitable for some but not all individuals with dry eye.33 Furthermore, artificial tears contain different active ingredients, preservatives, electrolytes, and polymers in varying concentrations.22 The different types of artificial tears also vary in their mode of action.32 For example, eyedrops containing hydrogel in borate solution tend to create a viscous matrix within the eye in which the comfort effect lasts longer when compared with other types of artificial tears.34 Another mechanism involves augmentation of some tear components and improvement in the thickness of the lipid layer.35
In the present study, Refresh Plus preservative-free lubricant eyedrops were used to improve the TF grade and decrease the symptoms of dry eye. These drops contain CMC 0.5% and have a pH of 6.5 and an osmolarity of 276 mmol/kg.32 There was a significant (P<0.05) improvement in TF grade obtained in subjects with dry eye after application of a single drop of these artificial tears that lasted for at least 3 hours. Lubricants containing CMC are known to improve the stability of tear film and increase the density of goblet cells.36,37 For example, Optive eyedrops, which contain sodium CMC 0.5% and glycerin 0.9%, can be used to relieve the symptoms of eye dryness.38,39 High-viscosity or gel-like artificial eyedrops are preferred by many patients with dry eye, because they have a longer ocular residence time.40 It has been reported that Refresh Plus eyedrops can significantly reduce the epithelial defects produced during laser in situ keratomileusis (P=0.020).41 Another study showed that use of Refresh Plus eyedrops led to significantly lower average ocular surface–staining scores following laser in situ keratomileusis in patients with myopia when compared with those obtained by Bion tears (P=0.015).42
Eyedrops containing sodium hyaluronate 0.1%–0.3% have been found to be more effective than saline for reducing the symptoms of dry eye and improving NITBUT scores in subjects with moderate eye dryness.43 Insertion of a cross-linked hyaluronic acid gel (0.2 mL) in the lower eyelid led to improvements in corneal fluorescein staining, increased TBUT scores, and improved Schirmer’s test results in subjects with dry eye.44 A combination of artificial tears containing a CMC salt and hyaluronic acid was found to be more effective in the management of symptoms of dry eye than eyedrops containing either ingredient alone.45–47 This combination lead to high shear viscosity and reduced stickiness and blur during blinking.
This study had some limitations, including a limited sample size and inclusion of only male subjects. Furthermore, the effect of artificial tears was observed for only 3 hours and only one type of artificial tears was used. Moreover, the possibility of a confounding effect of environmental factors, such as sunlight and extremes of humidity and temperature, immediately prior to taking part in the study cannot be excluded. Therefore, a further study is needed to test the longer-term effects of various type of artificial tears on tear film in a larger number of subjects with and without dry eye.
Conclusion
TF patterns obtained from subjects with dry eye improved significantly after application of Refresh Plus preservative-free lubricant eyedrops. There was some improvement in the quality of TF after application of artificial tears in normal eye subjects but the change was not statistically significant. Artificial tears containing sodium CMC, such as Refresh Plus, can be used to improve TF patterns in subjects with dry eye for at least 3 hours.
Abbreviations list
CMC, carboxymethylcellulose; NITBUT, noninvasive tear breakup time; OSDI, Ocular Surface Disease Index; TF, tear ferning; TMH, tear meniscus height.
Acknowledgment
This work was financially supported by the Deanship of Scientific Research, King Saud University, through the Vice Deanship of Scientific Research Chairs.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Georgiev GA, Eftimov P, Yokoi N. Structure-function relationship of tear film lipid layer: a contemporary perspective. Exp Eye Res. 2017;163:17–28. doi:10.1016/j.exer.2017.03.013
2. Belmonte C, Nichols JJ, Cox SM, et al. TFOS DEWS II pain and sensation report. Ocul Surf. 2017;15(3):404–437. doi:10.1016/j.jtos.2017.05.002
3. Bron AJ, Tiffany JM, Gouveia SM, Yokoi N, Voon LW. Functional aspects of the tear film lipid layer. Exp Eye Res. 2004;78(3):347–360. doi:10.1016/j.exer.2003.09.019
4. Borchman D, Foulks GN, Yappert MC, Milliner SE. Changes in human meibum lipid composition with age using nuclear magnetic resonance spectroscopy. Invest Ophthalmol Vis Sci. 2012;53(1):475–482. doi:10.1167/iovs.11-8341
5. Bacher LF. Factors regulating eye blink rate in young infants. Optom Vis Sci. 2010;87(5):337–343. doi:10.1097/OPX.0b013e3181d951b2
6. Sforza C, Rango M, Galante D, Bresolin N, Ferrario VF. Spontaneous blinking in healthy persons: an optoelectronic study of eyelid motion. Ophthalmic Physiol Opt. 2008;28(4):345–353. doi:10.1111/j.1475-1313.2008.00577.x
7. Borchman D, Yappert MC, Foulks GN. Changes in human meibum lipid with meibomian gland dysfunction using principal component analysis. Exp Eye Res. 2010;91(2):246–256. doi:10.1016/j.exer.2010.05.014
8. Chew CK, Hykin PG, Jansweijer C, Dikstein S, Tiffany JM, Bron AJ. The casual level of Meibomian lipids in humans. Curr Eye Res. 1993;12(3):255–259. doi:10.3109/02713689308999471
9. Doughty MJ, Naase T. Further analysis of the human spontaneous eye blink rate by a cluster analysis based approach to categorize individuals with ‘normal’ versus ‘frequent’ eye blink activity. Eye Contact Lens. 2006;32(6):294–299. doi:10.1097/01.icl.0000224359.32709.4d
10. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
11. Lemp MA, Bron AJ, Baudouin C, et al. Tear osmolarity in the diagnosis and management of dry eye disease. Am J Ophthalmol. 2011;151(5):792–798. doi:10.1016/j.ajo.2010.10.032
12. Kaercher T, Thelen U, Brief G, Morgan-Warren RJ, Leaback R. A prospective, multicenter, noninterventional study of Optive Plus® in the treatment of patients with dry eye: the Prolipid study. Clin Ophthalmol. 2014;8:1147–1155. doi:10.2147/OPTH
13. Miljanović B, Dana R, Sullivan DA, Schaumberg DA. Impact of dry eye syndrome on vision-related quality of life. Am J Ophthalmol. 2007;143(3):409–415. doi:10.1016/j.ajo.2006.11.060
14. Montani G, Murphy PJ, Patel S. Immediate effect of a tear enhancer and meibomian gland expression on the corneal surface and whole eye higher order aberrations. J Optom. 2018;11(4):223–231. doi:10.1016/j.optom.2018.01.004
15. Abusharaha A, Alturki AA, Alanazi SA, et al. An assessment of the tear evaporation rate in thyroid gland patients. Clin Ophthalmol. 2019;13:131–135. doi:10.2147/OPTH.S188614
16. Masmali A, Alqahtani TA, Alharbi A, El-Hiti GA. Comparative study of repeatability of phenol red thread test versus Schirmer’s test in normal adults in Saudi Arabia. Eye Contact Lens. 2014;40(3):127–131. doi:10.1097/ICL.0000000000000025
17. Ibrahim OM, Dogru M, Takano Y, et al. Application of Visante optical coherence tomography tear meniscus height measurement in the diagnosis of dry eye disease. Ophthalmology. 2010;117(10):1923–1929. doi:10.1016/j.ophtha.2010.01.057
18. Mzumara T, Afonne J. Assessing the relationship between non-invasive tear break-up time and maximum blink interval values among young adults at Mzuzu University. Clin Optom. 2018;10:87–91. doi:10.2147/OPTO.S164466
19. Masmali A, Alrabiah S, Alharbi A, El-Hiti GA, Almubrad T. Investigation of tear osmolarity using the TearLab™ osmolarity system in normal adults in Saudi Arabia. Eye Contact Lens. 2014;40(2):74–78. doi:10.1097/ICL.0000000000000002
20. Masmali AM, Al-Qhtani S, Al-Gasham TM, El-Hiti GA, Purslow C, Murphy PJ. Application of a new grading scale for tear ferning in non-dry eye and dry eye subjects. Cont Lens Anterior Eye. 2015;38(1):39–43. doi:10.1016/j.clae.2014.09.007
21. Masmali AM, Murphy PJ, Purslow C. Development of a new grading scale for tear ferning. Cont Lens Anterior Eye. 2014;37(3):178–184. doi:10.1016/j.clae.2013.09.011
22. Lievens C, Berdy G, Douglass D, et al. Evaluation of an enhanced viscosity artificial tear for moderate to severe dry eye disease: A multicenter, double-masked, randomized 30-day study. Cont Lens Anterior Eye. 2018. Epub ahead of print. doi:10.1016/j.clae.2018.12.003
23. Cuevas P, Outeiriño LA, Azanza C, Angulo J, Giménez-Gallego G. Improvement in the signs and symptoms of dry eye disease with dobesilate eye drops. Mil Med Res. 2015;2:35. doi:10.1186/s40779-015-0068-8
24. Masmali AM, Al-Shehri A, Alanazi SA, Abusharaha A, Fagehi R, El-Hiti GA. Assessment of tear film quality among smokers using tear ferning patterns. J Ophthalmol. 2016;2016:8154315. doi:10.1155/2016/8154315
25. Masmali AM, Maeni YA, El-Hiti GA, Murphy PJ, Almubrad T. Investigation of ocular tear ferning in controlled and uncontrolled diabetic subjects. Eye Contact Lens. 2018;44(Suppl 2):S70–S75. doi:10.1097/ICL.0000000000000419
26. Masmali AM, Alotaibi AG, Alanazi SA, Fagehi R, Abusharaha A, El-Hiti GA. The acute effect of a single dose of green tea on the quality and quantity of tears in normal eye subjects. Clin Ophthalmol. 2019;13:605–610. doi:10.2147/OPTH.S201127
27. Masmali AM, Alanazi SA, Almagren B, El-Hiti GA. Assessment of the tear film in normal eye subjects after consumption of a single dose of hot peppermint drink. Clin Optom. 2019;11:39–45. doi:10.2147/OPTO.S206904
28. Alanazi SA, El-Hiti GA, Al-Baloud AA, et al. Effects of short-term oral vitamin A supplementation on the ocular tear film in patients with dry eye. Clin Ophthalmol. 2019;13:599–604. doi:10.2147/OPTH.S198349
29. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
30. Lee R, Yeo S, Aung HT, Tong L. Agreement of noninvasive tear break-up time measurement between Tomey RT-7000 Auto Refractor-Keratometer and Oculus Keratograph 5M. Clin Ophthalmol. 2016;10:1785–1790. doi:10.2147/OPTH.S110180
31. Cohen JW. Statistical Power Analysis for the Behavioral Sciences. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988.
32. Tong L, Petznick A, Lee S, Tan J. Choice of artificial tear formulation for patients with dry eye: where do we start? Cornea. 2012;31(Suppl1):S32–S36. doi:10.1097/ICO.0b013e318269cb99
33. Norn MS. Tear fluid pH in normals, contact lens wearers, and pathological cases. Acta Ophthalmol (Copenh). 1988;66(5):485–489. doi:10.1111/j.1755-3768.1988.tb04368.x
34. Petricek I, Berta A, Higazy MT, Németh J, Prost ME. Hydroxypropyl-guar gellable lubricant eye drops for dry eye treatment. Expert Opin Pharmacother. 2008;9(8):1431–1436. doi:10.1517/14656566.9.8.1431
35. Maïssa C, Guillon M, Simmons P, Vehige J. Effect of castor oil emulsion eyedrops on tear film composition and stability. Cont Lens Anterior Eye. 2010;33(2):76–82. doi:10.1016/j.clae.2009.10.005
36. Gilbard JP, Rossi SR. An electrolyte-based solution that increases corneal glycogen and conjunctival goblet-cell density in a rabbit model for keratoconjunctivitis sicca. Ophthalmology. 1992;99(4):600–604. doi:10.1016/S0161-6420(92)31929-3
37. Grene RB, Lankston P, Mordaunt J, Harrold M, Gwon A, Jones R. Unpreserved carboxymethylcellulose artificial tears evaluated in patients with keratoconjunctivitis sicca. Cornea. 1992;11(4):294–301. doi:10.1097/00003226-199207000-00004
38. Wojtowicz JC, Arciniega JC, McCulley JP, Mootha VV. Effect of systane and optive on aqueous tear evaporation in patients with dry eye disease. Eye Contact Lens. 2010;36(6):358–360. doi:10.1097/ICL.0b013e3181f9b36e
39. Markoulli M, Sobbizadeh A, Tan J, Briggs N, Coroneo M. The effect of Optive and Optive Advanced artificial tears on the healthy tear film. Curr Eye Res. 2018;43(5):588–594. doi:10.1080/02713683.2018.1433860
40. Paugh JR, Nguyen AL, Ketelson HA, Christensen MT, Meadows DL. Precorneal residence time of artificial tears measured in dry eye subjects. Optom Vis Sci. 2008;85(8):725–731. doi:10.1097/OPX.0b013e3181824de3
41. Ahee JA, Kaufman SC, Samuel MA, Bogorad D, Wee C. Decreased incidence of epithelial defects during laser in situ keratomileusis using intraoperative nonpreserved carboxymethylcellulose sodium 0.5% solution. J Cataract Refract Surg. 2002;28(9):
42. Albietz JM, Lenton LM, McLennan SG, Earl ML. A comparison of the effect of refresh plus and bion tears on dry eye symptoms and ocular surface health in myopic LASIK patients. Clao J. 2002;28(2):
43. Johnson ME, Murphy PJ, Boulton M. Effectiveness of sodium hyaluronate eyedrops in the treatment of dry eye. Graefes Arch Clin Exp Ophthalmol. 2006;244(1):
44. Fezza JP. Cross-linked hyaluronic acid gel occlusive device for the treatment of dry eye syndrome. Clin Ophthalmol. 2018;12:2277–2283. doi:10.2147/OPTH.S187963
45. Simmons PA, Vehige JG. Investigating the potential benefits of a new artificial tear formulation combining two polymers. Clin Ophthalmol. 2017;11:1637–1642. doi:10.2147/OPTH.S135550
46. Simmons PA, Liu H, Carlisle-Wilcox C, Vehige JG. Efficacy and safety of two new formulations of artificial tears in subjects with dry eye disease: a 3-month, multicenter, active-controlled, randomized trial. Clin Ophthalmol. 2015;9:665–675. doi:10.2147/OPTH.S78184
47. Labetoulle M, Chiambaretta F, Shirlaw A, Leaback R, Baudouin C. Osmoprotectants, carboxymethylcellulose and hyaluronic acid multiingredient eye drop: a randomized controlled trial in moderate to severe dry eye. Eye (Lond). 2017;31(10):1409–1416. doi:10.1038/eye.2017.73
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.