Back to Journals » Cancer Management and Research » Volume 14
Effect of Propofol or Etomidate as General Anaesthesia Induction on Gastric Cancer: A Retrospective Cohort Study with 10 Years’ Follow-Up
Authors Lu X, Yu Y, Wang Y, Lyu Y
Received 4 March 2022
Accepted for publication 25 June 2022
Published 8 August 2022 Volume 2022:14 Pages 2399—2407
DOI https://doi.org/10.2147/CMAR.S361052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmet Emre Eşkazan
Xianfu Lu,1,2,* Yue Yu,2,* Yan Wang,1 Yi Lyu3
1Department of Anesthesiology High Tech Branch, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Department of Anesthesiology, Chaohu Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Department of Anesthesiology, Minhang Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xianfu Lu; Yi Lyu, Email [email protected]; [email protected]
Objective: The aim is to study the effect of intraoperative application of propofol and etomidate on the long-term prognosis of patients with gastric cancer at the same tumor stage.
Methods: A total of 1018 patients who underwent radical gastric cancer surgery at the First Affiliated Hospital of Anhui Medical University from January 2010 to December 2010 were selected and divided into the propofol and etomidate groups according to the different anesthetic induction drugs.
Results: Among 244 patients in TNM stage IIIA, survival times were 36.10 and 41.79 for etomidate and propofol, respectively, which were statistically different (p < 0.05). Among the 82 patients in TNM stage IIIC, survival times were 26.57 and 35.20 for etomidate and propofol, respectively, which were statistically different (p < 0.05).
Conclusion: In patients undergoing radical gastric cancer surgery, the application of propofol during induction of anaesthesia is more beneficial in improving the postoperative survival time compared to the application of etomidate at a specific TNM stage.
Keywords: propofol, etomidate, gastric cancer, prognosis
Globally, more than one million new cases of stomach cancer were diagnosed in 2018, making it the fifth most common cancer in the world. It is estimated that around 783,000 people died from stomach cancer worldwide in 2018, making it the third most deadly type of cancer.1 Most patients are already at an intermediate to advanced stage at the time of initial presentation, resulting in a low survival rate.2,3 With changing dietary factors, such as consumption of nitrites and salty foods, H. pylori infection is a major cause of gastric cancer.4 Identifying the factors affecting the long-term prognosis after radical gastric cancer surgery is crucial to improving patient prognosis and increasing their survival time. Therefore, how to reduce the probability of perioperative complications in patients with gastric cancer has been a major concern for clinicians.5 Currently, radical resection of gastric cancer is still the main clinical treatment, but many perioperative factors (including different anaesthetic methods and different anaesthetic drugs) may affect the prognosis of the tumor.6
TNM (tumor, lymph nodes and metastases) staging of gastric cancer is based on the depth of infiltration of the primary tumor (T), the number of metastatic lymph nodes (N) and distant metastases (M).7 The biological behavior of gastric cancer has important implications for the long-term prognosis of gastric cancer,8 but the prognosis of patients with gastric cancer who are induced with different anaesthetic drugs during surgery may also be very different. However, no studies have been reported on the prognosis of different intravenous anaesthetic drugs for gastric cancer with the same TNM stage. In this study, we retrospectively analyzed the case data of patients who underwent radical gastric cancer surgery in the Department of Gastroenterology, The First Affiliated Hospital of Anhui Medical University from 2010 to 2011 to investigate the effects of different anesthetic induction drugs on patients’ postoperative survival time under the same TNM stage, and to provide a reasonable and reliable clinical basis for the selection of appropriate anesthetic drugs for gastric cancer surgery.
Propofol is an intravenous anaesthetic drug that is commonly used for the induction and maintenance of general anaesthesia due to its short-acting and rapid awakening properties.9 Etomidate is a short-acting non-barbiturate hypnotic with cardiovascular stabilization and reduced respiratory depression advantages compared to other drugs.10,11 In this study, we followed up patients admitted to our hospital for radical gastric cancer surgery from January 2010 to December 2010 to understand and analyze the use of different anesthetic drugs that affect the long-term prognosis of patients undergoing radical gastric cancer surgery, in order to provide a basis for improving the prognosis and prolonging the survival time of patients.
Methods
Study Population
The study was performed according to the Helsinki declaration. Ethical approval was obtained from the Ethics Committee of the First Affiliated Hospital of Anhui Medical University. All data were anonymous, and no identifiable personal data of patients were available for analysis, so no additional informed consent was required. A total of 1018 patients who underwent radical surgery for gastric cancer at the First Affiliated Hospital of Anhui Medical University from January 2010 to December 2010 were enrolled in our retrospective cohort study.
Inclusion criteria were as follows: 1) age 18–84 years; 2) American Society of Anesthesiologists classification (ASA classification I–IV); 3) normal platelet and coagulation function; 4) patients undergoing elective radical gastric cancer surgery; 5) no residual tumor registered in the postoperative pathology report; 6) information on the type of anesthesia used was available; 7) Follow-up was not missed; and 8) all patients had no history of other tumors.
Exclusion criteria were as follows: 1) history of spinal surgery/surgery; 2) history of relevant drug allergies; 3) those with coagulation disorders; 4) patients with recurrent tumors who have undergone reoperation; 5) those found intraoperatively to be beyond radical tumor resection; and 6) lack of clinicopathological or follow-up data.
Anaesthetic methods
The patients were divided into propofol and etomidate groups according to the induction drug, all patients abstained from drinking for 8 h and fasting for 10 h. In the propofol group, patients were admitted to the operating room 30 minutes before surgery, intravenous access was routinely opened, cardiac monitoring was connected and propofol 1.5 mg/kg was given to induce tracheal intubation for general anesthesia. Subsequently, propofol was used to maintain the depth of anaesthesia. Etomidate group: Patients were admitted to the operating room 30 minutes before surgery, intravenous access was routinely opened, cardiac monitoring was connected and etomidate 0.5 mg/kg was given to induce tracheal intubation under general anaesthesia. Similarly, intraoperative propofol was pumped to maintain the depth of anaesthesia. There was no statistical difference (p > 0.05) in the dosage of other anaesthetic-inducing and maintenance drugs (analgesics, inotropes, anticholinergics and glucocorticoids) between the two groups. General anaesthesia by tracheal intubation in all cases.
The Mechanism of Follow-Up
We obtain follow-up content by contacting the patient or their family directly.
Primary Outcome
TNM stage and postoperative survival time of all patients who underwent radical gastric cancer surgery.
Statistical Analysis
SAS JMP 14.0 was used for statistical analysis of the data. Categorical information was expressed as examples (%) and the χ2 test was used for comparison between groups. Survival analysis was performed using GraphPad Prism 8.0 software to calculate survival rates and plot survival curves, and Log rank test for prognostic univariate analysis. Variables that were significant in the univariate analysis were included in the multifactor analysis, and a Cox proportional risk regression model was used for the prognostic multifactor analysis, which was statistically significant at P ˂ 0.05.
Results
We selected data relating to 1018 patients who underwent radical surgery for gastric cancer, and we excluded a total of 93 patients in whom anaesthesia was induced without propofol or etomidate and those in whom anaesthesia was induced with both propofol and etomidate. Finally, 925 eligible patients were identified for radical gastric cancer surgery, of which 455 patients were induced with propofol and 470 patients were induced with etomidate, as shown in Figure 1. These patients had no residual tumor registered in the post-operative pathology report and had information on the type of anaesthesia used and were not lost to follow-up. There were no significant differences in the general conditions such as age, gender, weight, cardiac function class, ASA class, surgical site, cancer site, tumor stage, pathological staging, tumor differentiation grade and TNM stage between each patient in the propofol and etomidate groups, as shown in Table 1. Among 26 patients in TNM stage 0, survival times were 44.64 and 38.67 for etomidate and propofol, respectively, which were not statistically different (p>0.05). Among the 102 patients in TNM stage IA, survival times were 57.73 and 64.54 for etomidate and propofol, respectively, which were not statistically different (p>0.05). Among 57 patients in TNM stage IB, survival times were 49.44 and 55.63 for etomidate and propofol, respectively, which were not statistically different (p>0.05). Among the 27 patients in TNM stage IIA, survival times were 52.6 and 58.35 for etomidate and propofol, respectively, which were not statistically different (p>0.05). Among 208 patients in TNM stage IIB, survival times were 45.82 and 48.29 for etomidate and propofol, respectively, which were not statistically different (p>0.05). Among 244 patients in TNM stage IIIA, survival times were 36.10 and 41.79 for etomidate and propofol, respectively, which were statistically different (p < 0.05). Among 161 patients in TNM stage IIIB, survival times were 35.25 and 30.18 for etomidate and propofol respectively, which were not statistically different (p>0.05). Among the 82 patients in TNM stage IIIC, survival times were 26.57 and 35.20 for etomidate and propofol, respectively, which were statistically different (p < 0.05). Among the 18 patients in TNM stage IV, survival times were 19.3 and 15 for etomidate and propofol, respectively, which were not statistically different (p>0.05) Table 2. The survival curves for each subgroup are shown in Figure 2. For stage I patients, the 5-year survival rate is shown in Figure 3. Table 3 lists all detailed TNM information of stage III patients. According to induction method with etomidate or propofol, we clearly stated 93 patients exclude from our main study analysis. The results of re-analysis of these patients are also listed in Table 4.
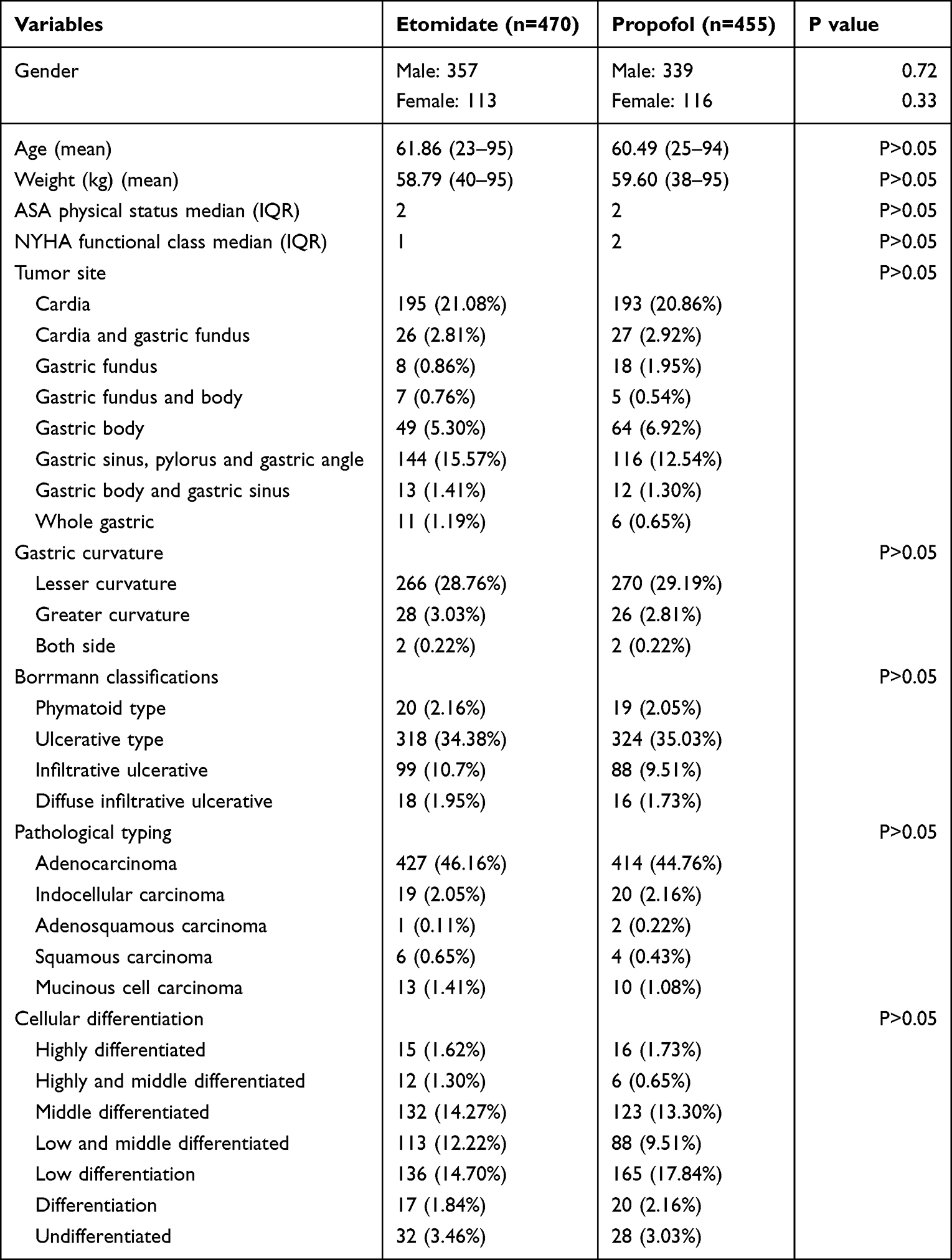 |
Table 1 Baseline and Perioperative Data of Two Groups |
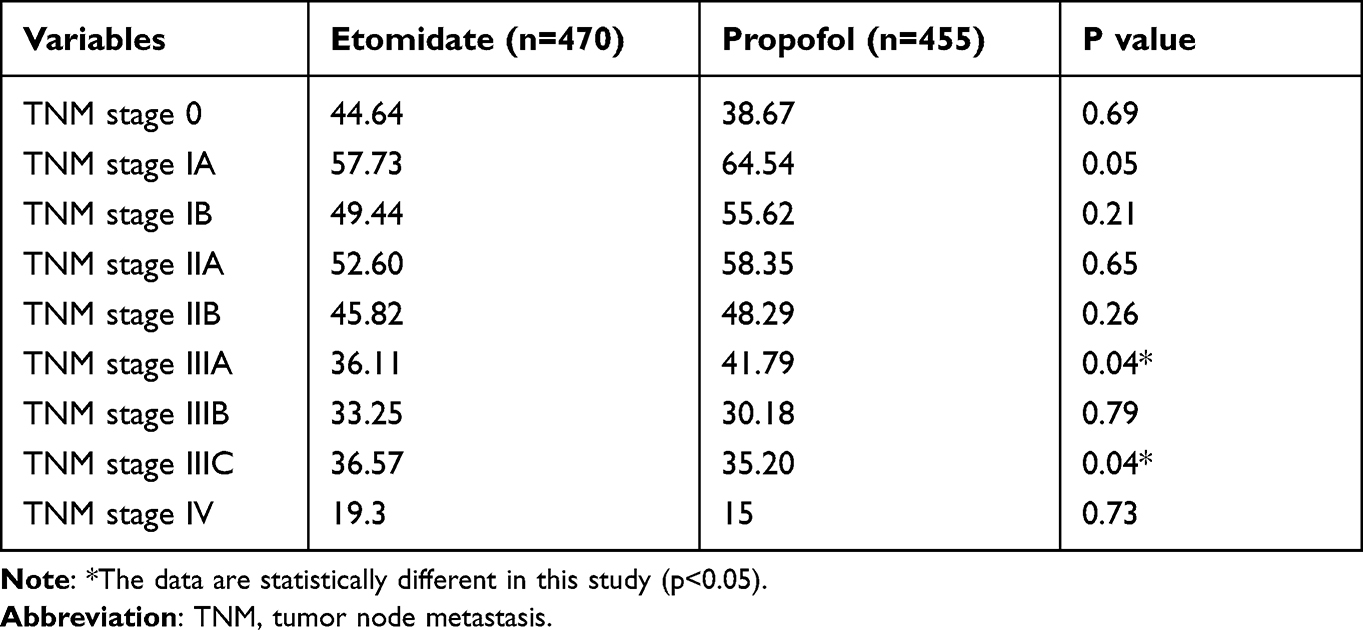 |
Table 2 Comparison of Mean Survival Time (Months) Between the Two Groups |
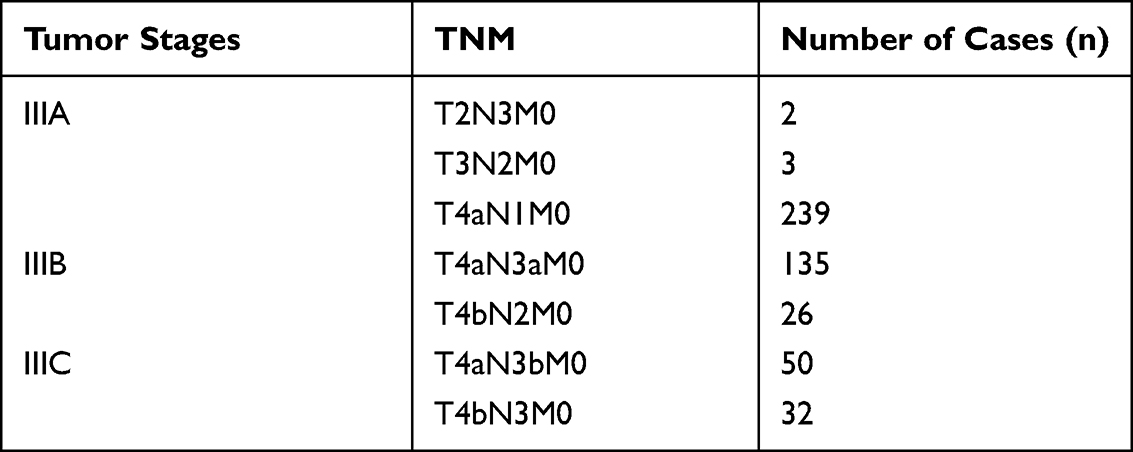 |
Table 3 Detailed TNM Information of Stage III Patients |
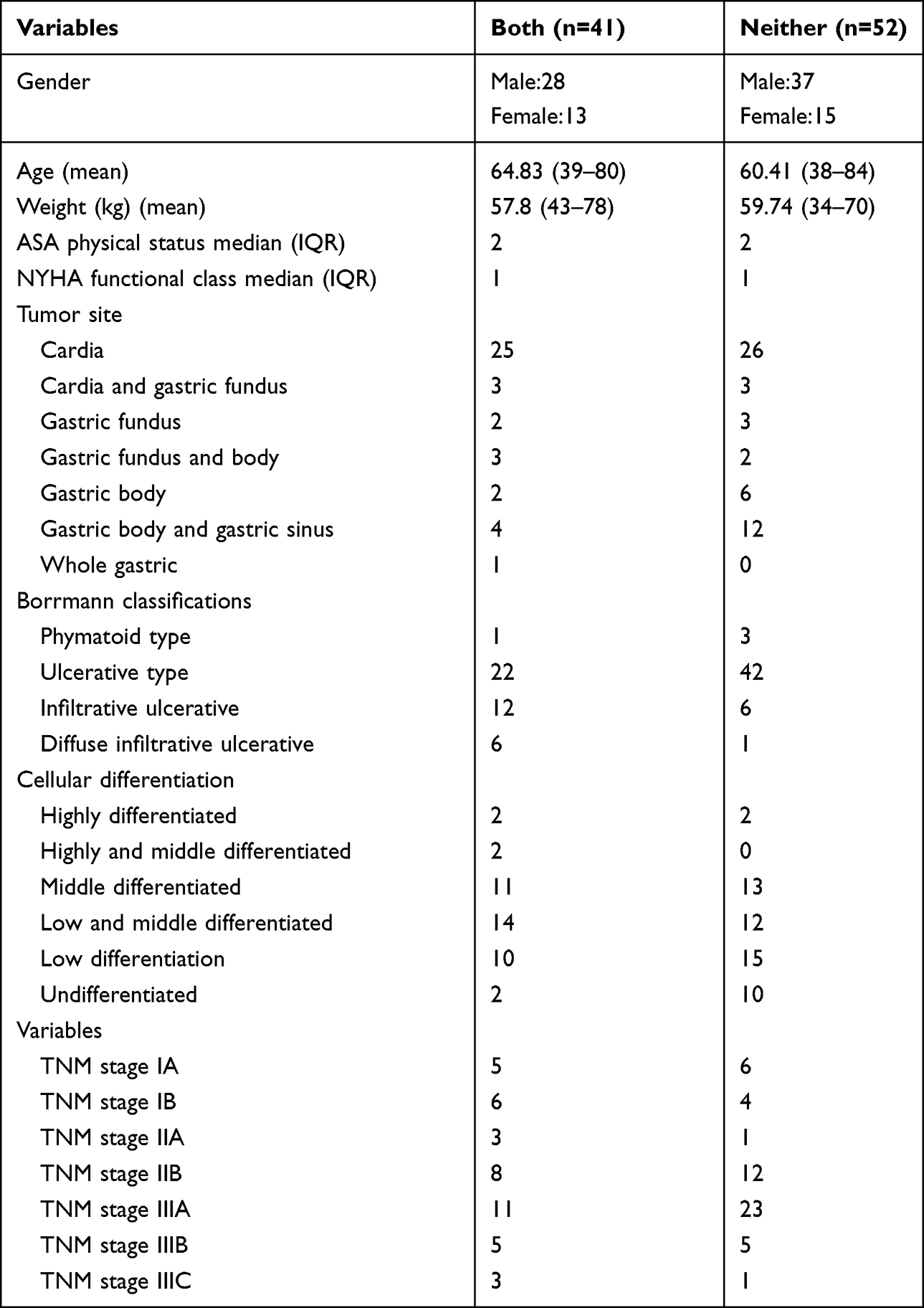 |
Table 4 Detailed Data of Both Induction with “Etomidate” and “Propofol” or Neither Patients |
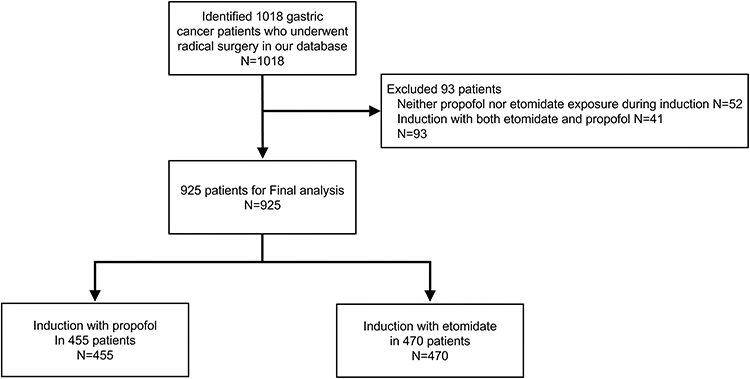 |
Figure 1 Case screening flowchart. |
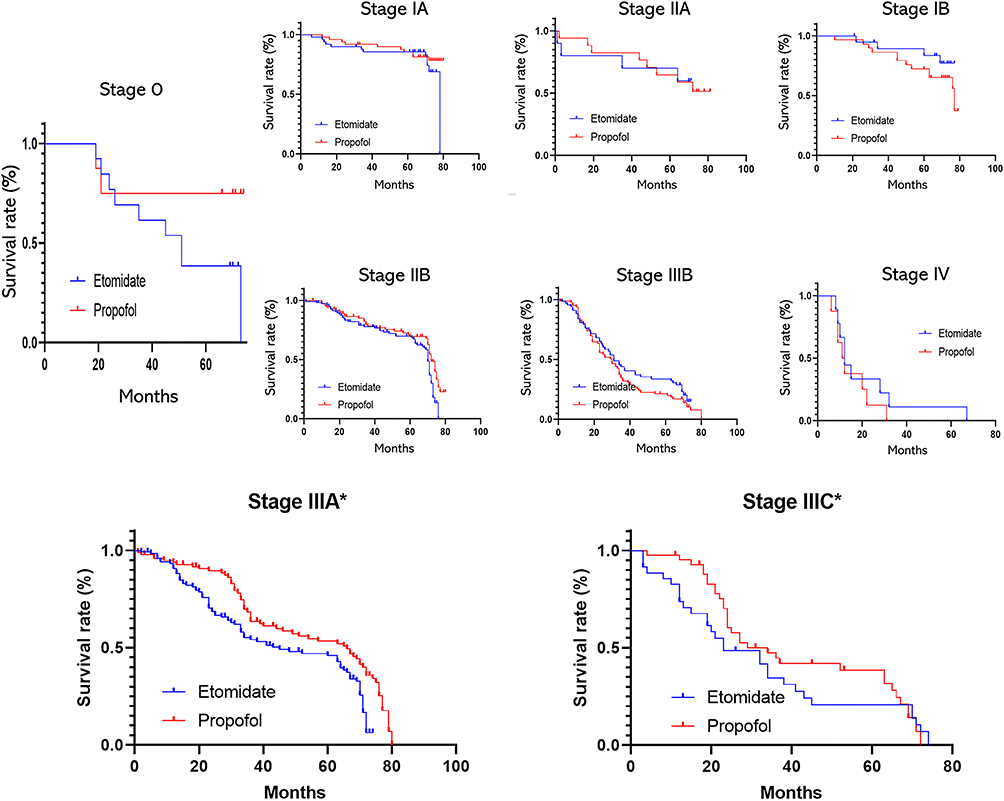 |
Figure 2 Demonstration of postoperative survival curves of gastric cancer patients with different tumor stages. The results of the seven groups (TNM stage 0, TNM stage IA, TNM stage IB, TNM stage IIA, TNM stage IIB, TNM stage IIIB, TNM stage IV) were not statistically different (P > 0.05). The results of the two groups (TNM stage IIIA, TNM stage IIIC) were statistically different (P < 0.05). The symbols with *Indicate statistical differences (P < 0.05). |
 |
Figure 3 Demonstration of postoperative survival curves of gastric cancer patients with TNM stage IA and IB. The horizontal coordinates represent the 5-year survival time (months) and the vertical coordinates represent the survival rate. |
Discussion
In 925 patients who underwent radical gastric cancer surgery, the effect of applying different anaesthetic induction drugs on survival time after surgery for radical gastric cancer patients was compared. We found a statistically significant difference in postoperative survival time between patients in TNM IIIA and TNM IIIC stages (p<0.05), ie, anesthesia induction with propofol may be more beneficial than etomidate in prolonging postoperative survival time and improving the quality of patients’ long-term prognostic survival, while other stages were not statistically different (p>0.05).
It is very interesting that stage III C survival rate is higher than stage III A and B survival rate in our study. This is probably because the number of cases in stage IIIC is significantly lower than in stage IIIA and IIIB, the patients we collected for follow-up tended to survive coincidentally. This may require further studies at a later date and follow-up of survival data in more stage IIIC patients.
Gastric cancer is a malignant tumour with a high incidence and mortality rate worldwide and has attracted widespread attention in recent years.12 With the accelerated pace of modern life and changes in people’s lifestyle and diet structure, the incidence of gastric cancer is on the rise year by year, and the incidence of the population is gradually becoming younger. Gastric cancer is a digestive system disease with a complex and diverse pathogenesis, mainly superficial gastritis and atrophic gastritis occurring in the stomach, with the lesions metastasising to the intestine, producing epithelial hyperplasia and eventually heterogeneous proliferation to induce cancer.13,14 Complete surgical resection is still the only way to cure gastric cancer, so it is vital to identify the factors that influence the long-term prognosis of patients with gastric cancer after radical surgery during anaesthesia in order to improve the prognosis.
Propofol, a widely used short-acting intravenous sedative drug, is gradually gaining attention due to its tumor-suppressive and non-anaesthetic effects,15 which can reduce the migration and invasion of gastric cancer MGC-803 cells by inhibiting HDAC1 expression and the downstream p38MAPK pathway,16 and also inhibit gastric cancer cell proliferation and migration by upregulating microRNA-29 cell proliferation and migration through upregulation of microRNA-29.17 Relevant clinical studies have shown that propofol can inhibit tumor growth and metastatic activity.18–20 It has also been shown in retrospective studies that propofol-based intravenous anaesthesia is associated with improved long-term survival after surgery in patients with solid cancer compared with volatile anaesthesia.21–26 Propofol improves survival in experimental animals after endotoxin injection by attenuating the inflammatory cytokine response,27,28 which may reduce postoperative organ dysfunction, vulnerability to postoperative complications, and mortality in humans.29–32 One study observed that high doses of propofol reduced the incidence of short-term cardiovascular, renal and inflammatory complications.33
This study has some limitations: 1) The study was conducted from data from a single Chinese institution, and the findings may vary between institutions. 2) The conclusions of this study are based on data collected between 2010 and 2011, and there is heterogeneity in diagnostic criteria, treatment techniques and postoperative treatment recommendations, especially for postoperative adjuvant treatment, as the data span a large period of time and the choice and protocols of postoperative adjuvant treatment vary from period to period, making it difficult to collect and data analysis, which may lead to bias in the study’s conclusions. Therefore, future prospective studies are needed to validate the findings of this retrospective analysis. (3) Surgery can cause an inflammatory response in the body; for example, colorectal surgery has been reported to often cause a systemic inflammatory response syndrome, which may increase postoperative morbidity and mortality.34 Studies have demonstrated that certain anaesthetic drugs are associated with an inflammatory response.35 However, no further observations were made in this study regarding the effects of inflammation and cognitive function in postoperative patients, and more in-depth studies in these areas should be conducted in the future.
In summary, TNM stage is currently the main basis for determining the prognosis of patients with gastric cancer, but the prognosis varies greatly with different interventions for the same tumor stage. Our analysis based on gastric cancer stage and postoperative survival status showed that propofol has a competitive preventive effect on mortality after radical gastric cancer surgery in patients with specific TNM stages. This provides new insights into the impact of anesthetic drugs on the long-term survival prognosis of patients with gastric cancer.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Department of Resources.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi:10.3322/caac.21492
2. Feng RM, Zong YN, Cao SM, et al. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics. Cancer Commun. 2019;39:22. doi:10.1186/s40880-019-0368-6
3. Sakamoto T, Fujiogi M, Matsui H, et al. Short-term outcomes of laparoscopic and open total gastrectomy for gastric cancer: a nationwide retrospective cohort analysis. Ann Surg Oncol. 2020;27:518–526. doi:10.1245/s10434-019-07688-y
4. Johnston FM, Beckman M. Updates on management of gastric cancer. Curr Oncol Rep. 2019;21:67. doi:10.1007/s11912-019-0820-4
5. Jeon BH, Choi M, Lee J, et al. Relationships between gastrointestinal symptoms, uncertainty, and perceived recovery in patients with gastric cancer after gastrectomy. Nurs Health Sci. 2016;18:23–29. doi:10.1111/nhs.12219
6. Longhini F, Bruni A, Garofalo E, et al. Anesthetic strategies in oncological surgery: not only a simple sleep, but also impact on immunosuppression and cancer recurrence. Cancer Manag Res. 2020;12:931–940. doi:10.2147/CMAR.S237224
7. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–99. doi:10.3322/caac.21388
8. Gong YB, Zhu Z, Wang X, et al. [Influence of different biological behaviors on prognosis of patients with advanced gastric cancer at the same TNM stage]. Zhong Hua Wei Chang Wai Ke Za Zhi. 2020;23:953–962. Chinese.
9. Sahinovic MM, Struys MM, Absalom AR. Clinical pharmacokinetics and pharmacodynamics of propofol. Clin Pharmacokinet. 2018;57:1539–1558. doi:10.1007/s40262-018-0672-3
10. Fengler BT. Should etomidate be used for rapid-sequence intubation induction in critically ill septic patients? Am J Emerg Med. 2008;26:229–232. doi:10.1016/j.ajem.2007.03.032
11. Song Z, Wu Y, Yang J, et al. Progress in the treatment of advanced gastric cancer. Tumor Biol. 2017;39:1010428317714626. doi:10.1177/1010428317714626
12. Forman SA, Warner DS. Clinical and molecular pharmacology of etomidate. Anesthesiology. 2011;114:695–707. doi:10.1097/ALN.0b013e3181ff72b5
13. Zhou M, Liu W, Peng J, et al. Impact of propofol epidural anesthesia on immune function and inflammatory factors in patients undergoing gastric cancer surgery. Am J Transl Res. 2021;13:3064–3073.
14. Miyauchi W, Shishido Y, Kono Y, et al. Less invasive surgery for remnant stomach cancer after esophago-proximal gastrectomy with ICG-guided blood flow evaluation: a case report. Yonago Acta Med. 2018;61:187–191. doi:10.33160/yam.2018.09.007
15. Cao Y, Fan L, Li L, et al. Propofol suppresses cell proliferation in gastric cancer cells through NRF2-mediated polyol pathway. Clin Exp Pharmacol Physiol. 2021. doi:10.1111/1440-1681.13595
16. Lin L, Jiang H, Huang M, et al. Depletion of histone deacetylase 1 inhibits metastatic abilities of gastric cancer cells by regulating the miR-34a/CD44 pathway. Oncol Rep. 2015;34:663–672. doi:10.3892/or.2015.4010
17. Yu X, Gao Y, Zhang F. Propofol inhibits pancreatic cancer proliferation and metastasis by up-regulating miR-328 and down-regulating ADAM8. Basic Clin Pharmacol Toxicol. 2019;125:271–278. doi:10.1111/bcpt.13224
18. Song J, Shen Y, Zhang J, et al. Mini profile of potential anticancer properties of propofol. PLoS One. 2014;9:e114440. doi:10.1371/journal.pone.0114440
19. Kushida A, Inada T, Shingu K. Enhancement of antitumor immunity after propofol treatment in mice. Immunopharmacol Immunotoxicol. 2007;29:477–486. doi:10.1080/08923970701675085
20. González-Correa JA, Cruz-Andreotti E, Arrebola MM, et al. Effects of propofol on the leukocyte nitric oxide pathway: in vitro and ex vivo studies in surgical patients. Naunyn Schmiedebergs Arch Pharmacol. 2008;376:331–339. doi:10.1007/s00210-007-0220-4
21. Lai HC, Lee MS, Lin C, et al. Propofol-based total intravenous anaesthesia is associated with better survival than desflurane anaesthesia in hepatectomy for hepatocellular carcinoma: a retrospective cohort study. Br J Anaesthesia. 2019;123:151–160. doi:10.1016/j.bja.2019.04.057
22. Wu ZF, Lee MS, Wong CS, et al. Propofol-based total intravenous anesthesia is associated with better survival than desflurane anesthesia in colon cancer surgery. Anesthesiology. 2018;129:932–941. doi:10.1097/ALN.0000000000002357
23. Wigmore TJ, Mohammed K, Jhanji S. Long-term survival for patients undergoing volatile versus IV anesthesia for cancer surgery: a retrospective analysis. Anesthesiology. 2016;124:69–79. doi:10.1097/ALN.0000000000000936
24. Jun IJ, Jo JY, Kim JI, et al. Impact of anesthetic agents on overall and recurrence-free survival in patients undergoing esophageal cancer surgery: a retrospective observational study. Sci Rep. 2017;7:14020. doi:10.1038/s41598-017-14147-9
25. Oh TK, Kim K, Jheon S, et al. Long-term oncologic outcomes for patients undergoing volatile versus intravenous anesthesia for non-small cell lung cancer surgery: a retrospective propensity matching analysis. Cancer Control. 2018;25:1073274818775360. doi:10.1177/1073274818775360
26. Enlund M, Berglund A, Andreasson K, et al. The choice of anaesthetic–sevoflurane or propofol–and outcome from cancer surgery: a retrospective analysis. Ups J Med Sci. 2014;119:251–261. doi:10.3109/03009734.2014.922649
27. Taniguchi T, Yamamoto K, Ohmoto N, et al. Effects of propofol on hemodynamic and inflammatory responses to endotoxemia in rats. Crit Care Med. 2000;28:1101–1106. doi:10.1097/00003246-200004000-00032
28. Taniguchi T, Kanakura H, Yamamoto K. Effects of posttreatment with propofol on mortality and cytokine responses to endotoxin-induced shock in rats. Crit Care Med. 2002;30:904–907. doi:10.1097/00003246-200204000-00032
29. Haga Y, Beppu T, Doi K, et al. Systemic inflammatory response syndrome and organ dysfunction following gastrointestinal surgery. Crit Care Med. 1997;25:1994–2000. doi:10.1097/00003246-199712000-00016
30. Becher RD, Hoth JJ, Miller PR, et al. Systemic inflammation worsens outcomes in emergency surgical patients. J Trauma Acute Care Surg. 2012;72:1140–1149. doi:10.1097/TA.0b013e3182516a97
31. Dieleman JM, Nierich AP, Rosseel PM, et al. Intraoperative high-dose dexamethasone for cardiac surgery: a randomized controlled trial. JAMA. 2012;308:1761–1767. doi:10.1001/jama.2012.14144
32. Laaninen M, Sand J, Nordback I, et al. Perioperative hydrocortisone reduces major complications after pancreaticoduodenectomy: a randomized controlled trial. Ann Surg. 2016;264:696–702. doi:10.1097/SLA.0000000000001883
33. Schaefer MS, Raub D, Xu X, et al. Association between propofol dose and 1-year mortality in patients with or without a diagnosis of solid cancer. Br J Anaesth. 2020;124:271–280. doi:10.1016/j.bja.2019.11.028
34. Wolfer AM, Scott AJ, Rueb C, et al. Longitudinal analysis of serum oxylipin profile as a novel descriptor of the inflammatory response to surgery. J Transl Med. 2017;15:83. doi:10.1186/s12967-017-1171-2
35. Jia J, Sun Y, Hu Z, et al. Propofol inhibits the release of interleukin-6, 8 and tumor necrosis factor-α correlating with high-mobility group box 1 expression in lipopolysaccharides-stimulated RAW 264.7 cells. BMC Anesthesiol. 2017;17:148. doi:10.1186/s12871-017-0441-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.