Back to Journals » Nature and Science of Sleep » Volume 17

Effect of Propofol on Postoperative Sleep Quality in Patients Undergoing Elective Cesarean Section with Spinal Anesthesia:A Retrospective Cohort Study Using Propensity Score Matching at a Single Center
Authors Zhou J ![]() , Hu B
, Hu B ![]() , Zhang Y, Wang Q, Wu Y, Wang H
, Zhang Y, Wang Q, Wu Y, Wang H
Received 13 August 2025
Accepted for publication 24 October 2025
Published 3 November 2025 Volume 2025:17 Pages 2853—2862
DOI https://doi.org/10.2147/NSS.S559802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Jie Zhou, Bingwei Hu, Yu Zhang, Qing Wang, Yong Wu, Hongwei Wang
Department of Anesthesiology, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Hongwei Wang, Department of Anesthesiology, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: To assess the impact of propofol on postoperative sleep quality in patients undergoing spinal anesthesia for cesarean section.
Patients and Methods: This study included a total of 245 patients, aged over 18 yr, who underwent elective cesarean section under spinal anesthesia from 1 January 2024 to 31 December 2024. Outcomes were compared between the propofol group, which received propofol after infant delivery, and the control group, which received no intravenous anesthetics. Primary and secondary outcomes were postoperative sleep quality and depressive symptoms, evaluated using the Pittsburgh Sleep Quality Index (PSQI) and Edinburgh Postnatal Depression Scale (EPDS) at 30 days post-surgery. Propensity-score matching ensured balanced baseline characteristics.
Results: Following propensity score matching, 29 patients per group were included in this study. After matching, the propofol group showed significantly lower PSQI scores (8.3 ± 3.4 vs 10.9 ± 3.1; mean difference − 2.6, 95% CI: − 3.1 to − 2.1; P< 0.001) and lower EPDS scores (7.9 ± 3.0 vs 10.2 ± 3.1; mean difference − 2.3, 95% CI: − 3.0 to − 1.7; P< 0.001) compared to the control group on the 30th day after surgery.
Conclusion: : Using propofol following extraction of the infant was associated with lower incidence of postoperative sleep disorders in patients undergoing spinal anesthesia for cesarean section.
Clinical Trial Registration Number: ChiCTR2500097811.
Registration Date: 02/26/2025.
Keywords: postpartum sleep disorder, cesarean section, pittsburgh sleep quality index, propofol
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Gou has been published for this article.
Introduction
Women undergoing cesarean section (CS) exhibit a significantly higher incidence of postpartum sleep disturbances disruption compared with vaginal delivery.1,2 Postpartum sleep disturbances are characterized by reduced sleep efficiency and increased wakefulness.3 Sleep quality after CS is associated with various factors, including pregnancy-associated comorbidities, antenatal sleep quality, anesthesia or surgical duration, postpartum pain, post-cesarean recovery, neonatal care demands, lactation and feeding patterns, environmental stressors, and other maternal discomfort-inducing factors.4–7 A prospective study tracking postoperative sleep trajectories demonstrated persistent sleep disturbances in most CS patients through 6 months postpartum.8 Within the 6 months postpartum, the prevalence of insomnia was 20.4%, and the prevalence of poor sleep quality was 67.8%, it can longitudinally predict more severe postpartum anxiety symptoms and depression.9 Importantly, the frequent co-occurrence of depressive symptoms, fatigue, and compromised sleep quality in postpartum women appears to collectively impair infant developmental outcomes.10 Moreover, sleep disturbances may serve as clinical indicators of postpartum psychosis risk.11 However, the physiological complexity of the maternal-neonatal dyad and pharmacological restrictions during lactation have resulted in a paucity of effective interventions, particularly with pharmacologic interventions.
During our investigation into maternal sleep quality, we identified that a subset of women undergoing CS received intraoperative propofol administration by attending physicians based on real-time clinical assessment. The causes encompass multiple dimensions, including maternal voluntary requests, severe anxiety states, and profound fatigue. Propofol has been found to significantly alter sleep architecture.12 In recent years, propofol has been established to improve postoperative sleep quality in non-obstetric surgical populations. For instance, studies have demonstrated that, compared to sevoflurane, propofol-based anesthesia reduces postoperative sleep disturbances and improves sleep efficiency in laparoscopic surgery patients,13 and has been shown to prolong total sleep time on the first postoperative night in elderly patients undergoing major abdominal surgery.14 Furthermore, propofol was associated with a greater improvement in sleep quality on the first post-procedure day compared to remimazolam for patients undergoing ambulatory painless gastroscopy.15
Therefore, we hypothesize that intraoperative administration of propofol following extraction of the infant during CS may confer favorable effects on maternal postpartum outcomes. Even so, conducting a randomized controlled study on the use of propofol during CS for pregnant women poses a challenge to medical ethics. This means that some pregnant women were randomly assigned to receive propofol, rather than based on medical necessity. Accordingly, conducting a preliminary analysis of the hypothesis utilizing real-world clinical data represents a judicious strategic approach.
This study aimed to evaluate whether pharmacological intervention of propofol following extraction of the infant influences sleep quality on postpartum day 30 among CS patients undergoing spinal anesthesia, with the goal of informing future study. The data were retrieved from the electronic medical record database of a tertiary Level III Grade A teaching hospital in China.
Materials and Methods
Ethics and Study Design
This study was approved by the Medical Ethics Committee of Tongde Hospital of Zhejiang Province (No: ZTD-2025S-068). As a retrospective study, the institutional ethics committee granted a waiver of written informed consent in accordance with institutional ethical policies. With approval from the ethics committee, verbal consent was obtained via standardized telephone interviews prior to administering follow-up scale assessments. The entire consent process, including the verbal explanation of the study and the participant’s agreement, was audio-recorded. These recordings are stored securely with the research data under a unique participant ID and are available for audit by the ethics committee upon request. Patients who declined participation were excluded from the study. The trial was registered prior to patient enrollment at the Chinese Clinical Trial Registry (https://www.chictr.org.cn/showproj.html?proj=262780, Registration number: ChiCTR2500097811, Registration date: 02/26/2025). The study adhered to the Declaration of Helsinki.
Inclusion and Exclusion Criteria
The inclusion criteria were patients aged over 18 yr with American Society of Anesthesiologists (ASA) physical status II–III undergoing elective CS with spinal anesthesia.
The exclusion criteria were patients who received other intravenous anesthetics except propofol following extraction of the infant, failure of spinal anesthesia, chronic life-threatening comorbidities (eg, chronic obstructive pulmonary disease, pulmonary hypertension, or a history of congestive heart failure), severe mental disorder, long-term use of hypnotics and sedatives, inability to communication. Patients who refused to participate were excluded.
This retrospective cohort study included the patients who underwent elective CS under spinal anesthesia in 2024. In clinical practice, a subset of patients undergoing cesarean section under spinal anesthesia may receive propofol after extraction of the infant due to specific indications including maternal request, acute anxiety, or preoperative sleep deprivation. The decision to administer propofol was made by attending anesthesiologists based on their clinical assessment. Based on actual anesthesia records, we divided the patients who were received propofol following extraction of the infant into the propofol group, and those who were not received intravenous anesthetics following extraction of the infant into the control group.
Data were retrospectively collected by research assistants using a standardized data collection form from two sources: electronic medical records system and telephone follow-ups of patients discharged after CS. The collected variables included age, BMI, gestational age, ASA classification, parity, smoking status, diabetes, hypertension, hypothyroxinemia during pregnancy, education level, employment status, prenatal exercise, infant sex, duration of anesthesia, postoperative complications, duration of hospital stays. The 30-day postoperative assessment was conducted via a home telephone interview to evaluate sleep quality and depressive symptoms using PSQI and the EPDS. We tried to be as objective as possible in the assessment, without insinuating the patient, but rather a review of the entire postoperative recovery. The primary outcome was postoperative sleep quality, and the secondary outcomes were depressive symptoms.
Measures
Quality of Postoperative Sleep
The postoperative sleep quality was assessed using Pittsburgh Sleep Quality Index (PSQI), which was initially described by Buysse in 1989.16 The PSQI has seven components including sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction. Score in each group ranged from 0 to 3 and total score ranging from 0 to 21 was obtained by summing the seven component scores. PSQI total score of more than 5 was generally considered to poor sleep quality, higher PSQI score indicated lower sleep quality. PSQI has good construct validity and reliability (Cronbach’s alpha 0.73) and has been used to assess sleep quality among childbearing women.17
Edinburgh Postnatal Depression Scale
The postoperative depressive symptoms were assessed using Edinburgh Postnatal Depression Scale (EPDS).18 Its 10 items were scored ranged from 0 to 3 with total scores ranging from 0 to 30. The higher the score indicated the more severe the symptoms. EPDS has good construct validity and reliability (Cronbach’s alpha 0.86) among childbearing women.18
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for mac (version 27). Continuous data were tested for normality using the Shapiro–Wilk test. Normally distributed data are presented as the means and standard deviations (mean ±SD), while skewed data are reported as the medians (M) and interquartile ranges (IQR). Count data are presented as numbers and percentages (%).
Given the differences in the baseline characteristics between eligible participants in the two groups (Table 1), propensity-score matching was performed using the PSMATCH procedure in SPSS Statistics. The propensity score was estimated using a logistic regression model incorporating the following baseline covariates: age, BMI, gestational age, ASA classification, parity, smoking status, diabetes, hypertension, hypothyroxinemia during pregnancy, education level, employment status, prenatal exercise, infant sex, duration of anesthesia, postoperative complications, duration of hospital stays, global PSQI score before surgery and EPDS score before surgery. Participants in the intervention group were matched 1:1 to those in the control group using the nearest neighbor method within a specified caliper width. The caliper was set to 0.02 on the propensity score scale. The matching order was unspecified (as per the software default). Standardized mean differences (SMD) were estimated for all the baseline covariates before and after matching to assess pre-match imbalance and post-match balance. SMD of less than 10.0% for a given covariate indicate a relatively small imbalance. For non-essential matching variables, an SMD of less than 20.0% was considered acceptable. The magnitude of SMD was measured using Hedges’g as the effect size.
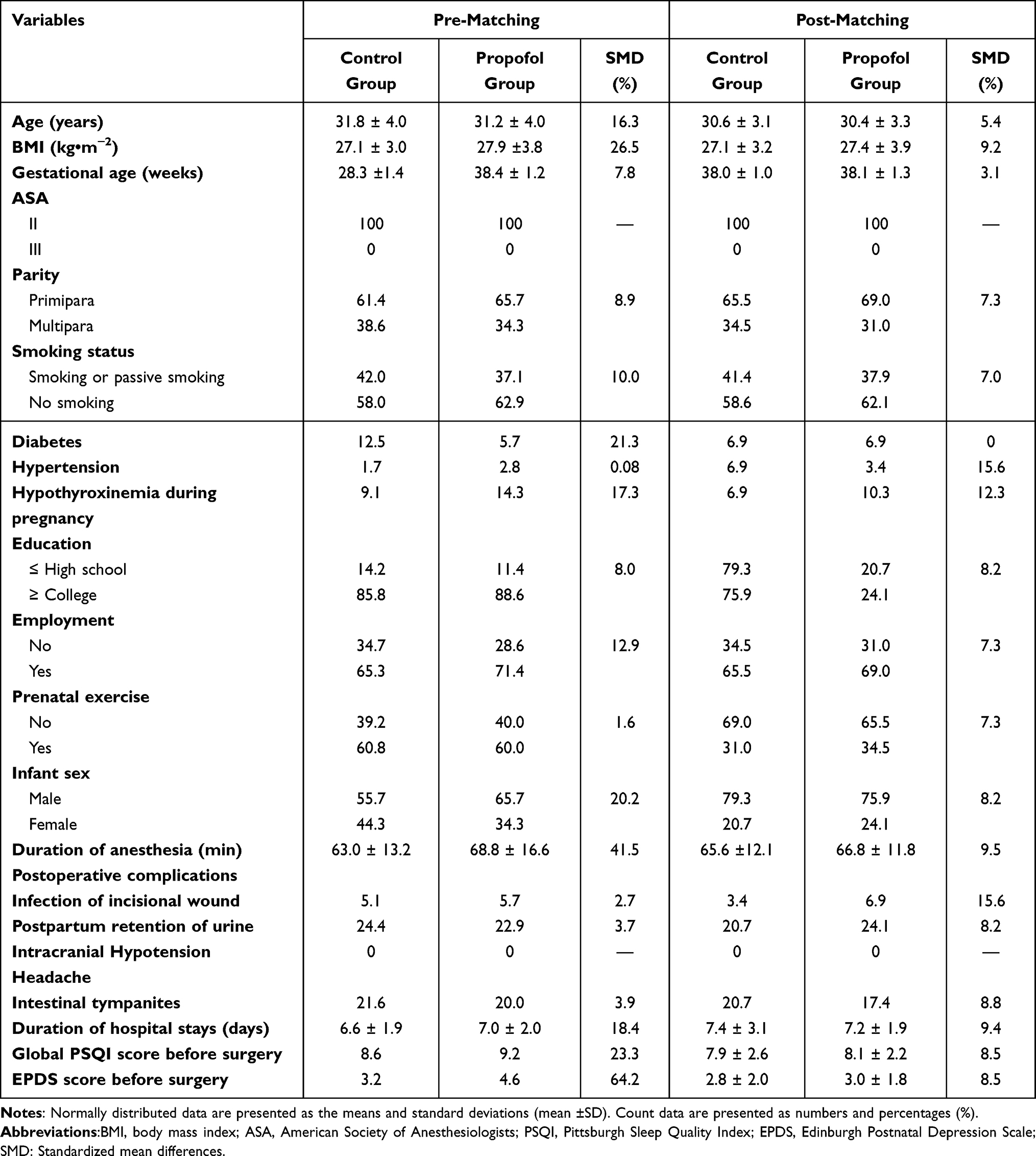 |
Table 1 Demographic Data |
In the original cohort, independent Student’s t-tests and Mann–Whitney U-tests were employed to compare between-group differences for normally distributed continuous variables and non-normally distributed continuous variables. In the matched cohort, paired Student’s t test and Wilcoxon signed-rank test were employed to compare between-group differences for normally distributed continuous variables and non-normally distributed continuous variables, respectively.
Results
Participant Characteristics
Through the electronic medical record system (Docare Clinical Anesthesia Information System V5.0, Madison Medical Technology), a total of 245 patients meeting the inclusion criteria were retrieved from 1 January 2024 to 31 December 2024. Six patients in the propofol group and 22 patients in the control group were excluded. Two patients in the propofol group and four patients in the control group were lost to follow-up (Figure 1).
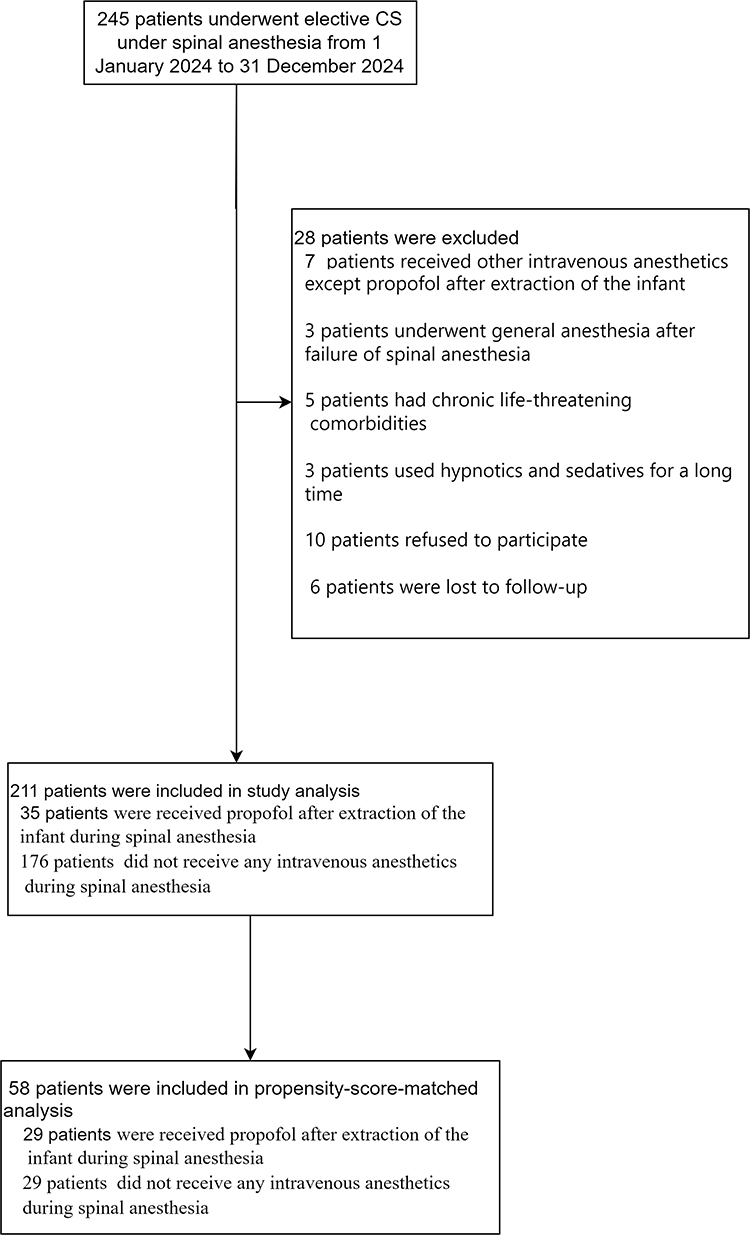 |
Figure 1 Flowchart of patient selection, inclusion, and matching for the study cohort. Abbreviation:CS, cesarean section. |
Before propensity-score matching, there were differences between the two groups in several of the baseline variables (Table 1). With the use of propensity-score matching, 29 patients who underwent pharmacological intervention of propofol following extraction of the infant were matched with 29 patients in the control group. After matching, the standardized differences for the key variables were less than 10.0%, indicating the differences between the two groups were very small (Table 1). The matching rate was 82.9% in the propofol group. After propensity score matching, the distributions of propensity scores showed similarity and overlap between the two groups (Figure 2).
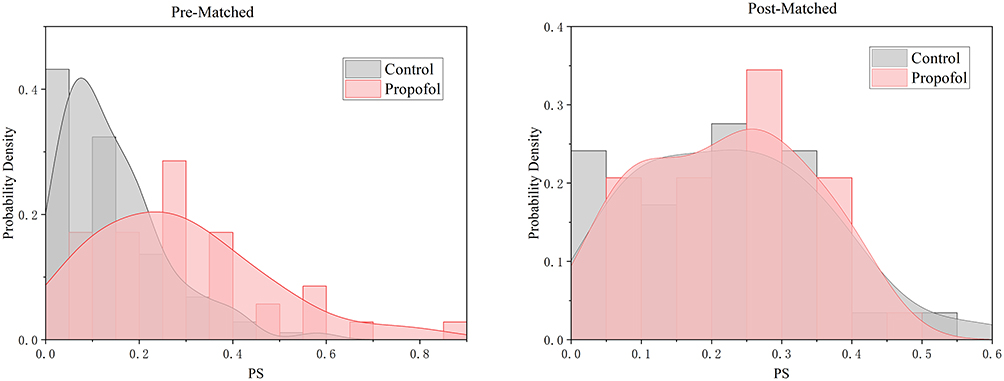 |
Figure 2 Propensity score distributions in the control and propofol groups, before and after matching. Abbreviation:PS, propensity score. |
Primary Outcome
The results of between-groups comparisons remained consistent before and after propensity score matching (Table 1). After matching, the PSQI scores on the 30th day after surgery were 8.3 ± 3.4 in the propofol group versus 10.9 ± 3.1 in the control group, with a difference of −2.6 (95% CI: −3.1 to −2.1), and the difference was statistically significant (t = −11.154, P < 0.001) (Table 2). The estimated Hedges’ g effect size was −2.043 (95% CI: −2.679 to −1.395). The Pearson correlation was observed between groups (r = 0.926, P < 0.001) (Figure 3A). Among the seven components of the PSQI scale, significant intergroup differences were observed in sleep quality, sleep latency, sleep duration and sleep disturbances (P < 0.05), while no significant differences were found in the remaining components (Table 2 and Figure 4).
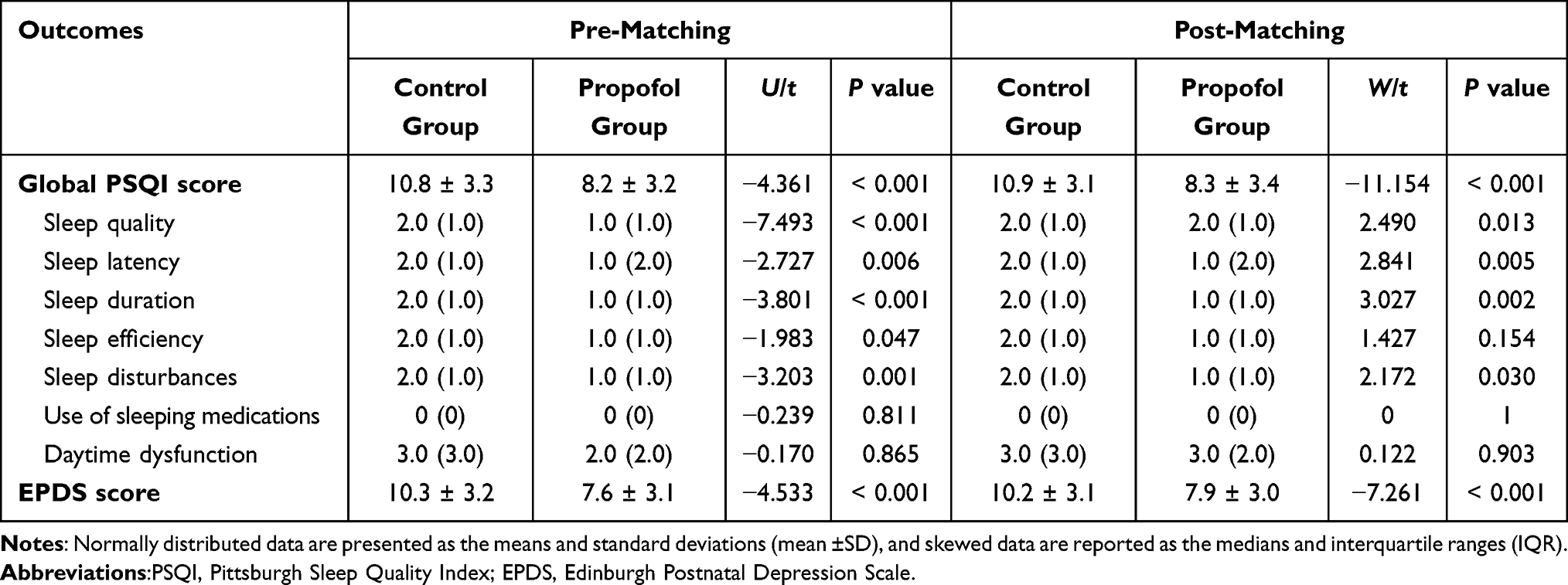 |
Table 2 Comparison of PSQI and EPDS Score After Surgery Between Two Groups |
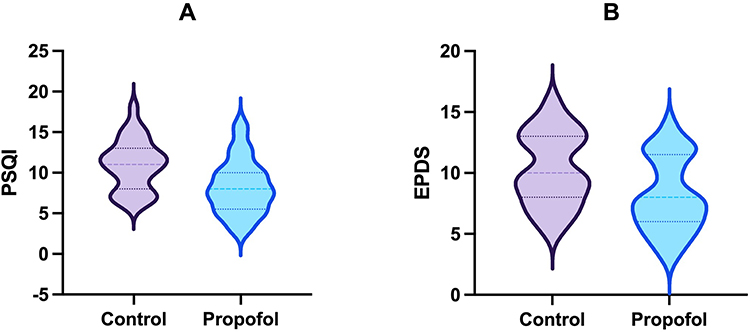 |
Figure 3 Comparison of postoperative PSQI and EPDS between the two groups. (A) Global PSQI scores. (B) EPDS scores. Abbreviation: PSQI, Pittsburgh Sleep Quality Index; EPDS, Edinburgh Postnatal Depression Scale. |
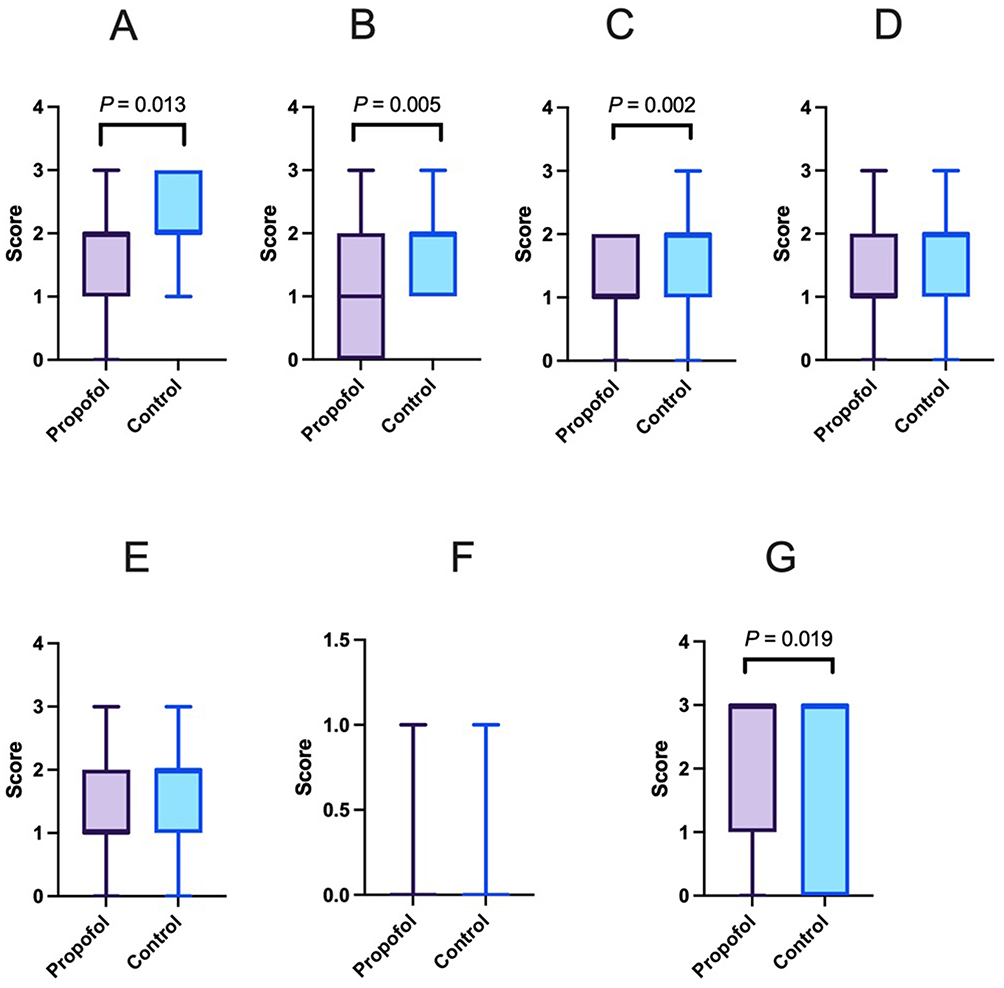 |
Figure 4 Comparison of Pittsburgh Sleep Quality Index (PSQI) component scores between the propofol and control groups after matching. The seven components are: (A) Sleep quality, (B) Sleep latency, (C) Sleep duration, (D) Sleep efficiency, (E) Sleep disturbances, (F) Use of sleeping medication, and (G) Daytime dysfunction. P-values were derived from the Wilcoxon signed-rank test, indicating statistical significance for most components between the two groups. |
Secondary Outcome
After matching, the postoperative EPDS scores on the 30th day after surgery were 7.9 ± 3.0 in the propofol group compared with 10.2 ± 3.1 in the control group, with a difference of −2.3 (95% CI:-3.0 – −1.7), and the difference was statistically significant (t = −7.261, P < 0.001) (Table 2). The estimated Hedges’g effect size was −1.330 (95% CI: −1.823 to −0.825). The Pearson correlation was observed between groups (r = 0.842, P < 0.001) (Figure 3B).
Discussion
Our trial assessed the efficacy of propofol as a pharmacological intervention on sleep quality in patients undergoing elective CS with spinal anesthesia. Our study found that intravenous propofol administration following extraction of the infant significantly reduced occurrence of postpartum sleep disorders.
Due to the influence of physiological, psychological and social factors, postpartum sleep disturbances are common. The changes of neuroendocrine during postpartum period affect sleep regulation.19 The interaction between progesterone and GABAA receptor are highly selective. The decline in progesterone levels within postpartum alter GABAA receptor structure and function, significantly impairing sleep maintenance.20 Moreover, a deficiency in GABAA receptor regulation during postpartum may make individuals prone to postpartum-related mood disorders.21 Propofol’s GABAA receptor-mediated modulation has been empirically demonstrated to enhance sleep.22 Current evidence demonstrates that propofol administration significantly improves postoperative sleep quality in non-obstetric surgical patients.13,14 Based on the above research, we reasonably suppose that intravenous administered propofol following extraction of the infant might have improved postpartum sleep quality by GABA receptor-mediated modulation.
Our study was the first to investigate the impact of intravenous drug intervention on sleep quality after elective CS, utilizing subjective PSQI. Our results showed that intravenous propofol administration following extraction of the infant lowered the PSQI score on postoperative days 30. As for each component of PSQI scores, the postoperative PSQI components of sleep quality, sleep latency, sleep duration and sleep disturbances scored significantly lower in the propofol group.
Postpartum depression (PPD), akin to postpartum sleep disturbance, exhibits high prevalence rates and exerts profound adverse effects on both maternal psychological well-being and physiological recovery. A multicenter cross-sectional study of 1065 postpartum mothers in Northeast China revealed a 23.57% prevalence of depressive symptoms at 6 weeks postpartum.23 Our results showed that intravenous propofol administration following extraction of the infant lowered the EPDS score on postoperative days 30. This phenomenon may involve dual mechanistic pathways: (1) propofol exerts direct anxiolytic and antidepressant effects24 and (2) propofol indirectly alleviates PPD by improving the postpartum sleep quality. Sleep disturbances constitute a significant modifiable risk factor for PPD, improving sleep quality can help alleviate PPD.25–28
Although studies in non-obstetric surgeries have demonstrated that intraoperative propofol administration improves postoperative sleep quality and reduces depression, its use during CS remains restricted due to safety concerns. Pregnant women frequently present with full stomach and difficult airways, increasing risks of regurgitation/aspiration and airway obstruction with propofol use. Additionally, propofol crosses the placental barrier, raising concerns about fetal drug exposure. Importantly, administering propofol after extraction of the infant eliminates fetal drug exposure. In clinical practice, anesthesiologists report that propofol use is primarily driven by maternal request, acute anxiety, or preoperative sleep deprivation. This explains why the propofol group in our original cohort predominantly comprised mothers with more severe baseline sleep disturbances and mood disorders. Propofol rapidly ameliorates acute emotional distress and preoperative sleep deprivation.
While maternal sleep disturbances have been extensively studied, with numerous interventions targeting pregnancy and postpartum periods, the compounded effects of surgical stress and anesthesia emerged during CS. This critical perioperative window—where sleep and mood disturbances peak—has paradoxically received minimal therapeutic attention. Our study bridges this gap by demonstrating that intraoperative propofol administration reduces both postoperative sleep disorders and PPD, thereby enabling continuum-of-care from pregnancy through postpartum.
This study is a retrospective cohort analysis with certain limitations. One of the limitations of our study is that despite rigorous propensity-score matching, residual confounding remains possible due to unmeasured variables such as detailed socioeconomic status, specific psychosocial stressors and specific breastfeeding practices. Second, the relatively small proportion of propofol use in our cohort resulted in a limited sample size after matching. This not only increases the risk of a type II error but also limits the generalizability of our findings. We were unable to maintain standardized mean differences (SMDs) below 10% for all covariates, achieving this balance only for key variables, which may somewhat compromise the overall comparability between groups. Third, the assessment of the primary outcome via telephone interview at 30 days postoperatively is susceptible to recall bias. Recalling sleep quality and emotional states over such an extended period is challenging and can be influenced by a patient’s most recent experiences or their current mood state. Subjective recall has the potential to underestimate or overestimate the true postoperative situation, impacting the accuracy of our effect estimates. Finally, patients assigned to the propofol regimen, characterized by greater severity of sleep disorders and depression, demonstrated a propensity for meticulous retrospection and focused attention on risk factors. Nevertheless, our findings suggest a potential protective effect of propofol use during CS on postpartum sleep quality and depression, warranting further validation through randomized controlled trials to establish its true effect.
Conclusions
In summary, our study suggested that use of propofol significantly improved postoperative sleep quality and reduced the postpartum depression in in patients undergoing elective CS with spinal anesthesia. Future prospective studies are needed to confirm the causal efficacy of propofol in improving postoperative sleep quality after cesarean section and to elucidate its underlying mechanisms.
Data Sharing Statement
The data are available from the corresponding author upon reasonable request.
Author Contributions
Jie Zhou: Conceptualization, Data curation, Methodology, Investigation, Writing – original draft. Bingwei Hu: Methodology, Formal analysis, Writing – review and editing. Yu Zhang: Writing – original draft, Investigation. Qing Wang: Writing – review and editing, Investigation, Validation.
Yong Wu: Formal analysis, Investigation, Writing – review and editing. Hongwei Wang: Writing – review and editing, Methodology, Formal analysis, Project administration, Supervision.
All authors have given final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
All the authors declare that they have no conflicts of interest.
References
1. Hunter LP, Rychnovsky JD, Yount SM. A selective review of maternal sleep characteristics in the postpartum period. J Obstet Gynecol Neonatal Nurs. 2009;38(1):60–68. doi:10.1111/j.1552-6909.2008.00309.x
2. Lee SY, Lee KA. Early postpartum sleep and fatigue for mothers after cesarean delivery compared with vaginal delivery: an exploratory study. J Perinat Neonatal Nurs. 2007;21(2):109–113. doi:10.1097/01.JPN.0000270627.73993.b0
3. Mindell JA, Cook RA, Nikolovski J. Sleep patterns and sleep disturbances across pregnancy. Sleep Med. 2015;16(4):483–488. doi:10.1016/j.sleep.2014.12.006
4. Witkowska-Zimny M, Zhyvotovska A, Isakov R, Boiko DI, Nieradko-Iwanicka B. Maternal sleeping problems before and after childbirth - a systematic review. Int J Women’s Health. 2024;16. doi:10.2147/IJWH.S446490
5. Motta AJ, Lucchese R, Leão GC, Rosa D, Junior VD, Mendonça RS. Factors associated with poor sleep quality in postpartum women: a crossectional study. Sleep Sci. 2024;17(3). doi:10.1055/s-0044-1782174
6. Carr C, Borges D, Lewis K, et al. Sleep and postpartum psychosis: a narrative review of the existing literature. J Clin Med. 2023;12(24):7550. doi:10.3390/jcm12247550
7. Su X, Wang DX. Improve postoperative sleep: what can we do? Curr Opin Anaesthesiol. 2018;31(1):83–88. doi:10.1097/ACO.0000000000000538
8. Tzeng YL, Chen SL, Chen CF, Wang FC, Kuo SY. Sleep trajectories of women undergoing elective cesarean section: effects on body weight and psychological well-being. PLoS One. 2015;10(6):e0129094. doi:10.1371/journal.pone.0129094
9. Ml O, L A. Postpartum insomnia and poor sleep quality are longitudinally predictive of postpartum mood symptoms. Psychosomatic Med. 2023;85(8). doi:10.1097/PSY.0000000000001234
10. Wang M, Bai T, Zhang J, Liu H, Wu L, Zhang F. Relationship between maternal postpartum depression, fatigue, sleep quality and infant growth: a cross-sectional study. Japan J Nurs Sci. 2024;21(4). doi:10.1111/jjns.12614
11. Petrosellini C, Eriksson SH, Meyer N, et al. Sleep disturbance as a marker of postpartum psychosis risk: a prospective actigraphy study. BMC Psychiatry. 2025;25(1). doi:10.1186/s12888-025-07017-6
12. Liu H, Yang C, Wang X, et al. Propofol improves sleep deprivation-induced sleep structural and cognitive deficits via upregulating the BMAL1 expression and suppressing microglial M1 polarization. CNS Neurosci Ther. 2024;30(7):e14798. doi:10.1111/cns.14798
13. Li S, Song B, Li Y, Zhu J. Effects of intravenous anesthetics vs inhaled anesthetics on early postoperative sleep quality and complications of patients after laparoscopic surgery under general anesthesia. Nat Sci Sleep. 2021;13:375–382. doi:10.2147/NSS.S300803
14. Chen NP, Sun P, Li CJ, et al. Propofol versus sevoflurane anesthesia on postoperative sleep quality in older patients after major abdominal surgery: a randomized clinical trial. J Clin Anesthesia. 2025;105:111875. doi:10.1016/j.jclinane.2025.111875
15. Zhou R, Fu L, Liu S, et al. Influences of propofol, ciprofol and remimazolam on dreaming during anesthesia for gastrointestinal endoscopy: a randomized double-blind parallel-design trial. Drug Des Devel Ther. 2024;18:1907–1915. doi:10.2147/DDDT.S455915
16. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
17. Ko SH, Chang SC, Chen CH. A comparative study of sleep quality between pregnant and nonpregnant taiwanese women. J Nurs Scholarsh. 2010;42(1):23–30. doi:10.1111/j.1547-5069.2009.01326.x
18. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item edinburgh postnatal depression scale. Br J Psychiatry. 1987;150:782–786. doi:10.1192/bjp.150.6.782
19. Blyton DM, Sullivan CE, Edwards N. Lactation is associated with an increase in slow-wave sleep in women. J Sleep Res. 2002;11(4):297–303. doi:10.1046/j.1365-2869.2002.00315.x
20. Belelli D, Lambert JJ. Neurosteroids: endogenous regulators of the GABAA receptor. Nat Rev Neurosci. 2005;6(7):565–575. doi:10.1038/nrn1703
21. Maguire J, Mody I. Steroid hormone fluctuations and GABAAR plasticity. Psychoneuroendocrinology. 2009;34(Suppl 1):S84. doi:10.1016/j.psyneuen.2009.06.019
22. Rudolph U, Knoflach F. Beyond classical benzodiazepines: novel therapeutic potential of GABAA receptor subtypes. Nat Rev Drug Discov. 2011;10(9):685–697. doi:10.1038/nrd3502
23. Huang X, Zhang L, Zhang C, Li J, Li C. Postpartum depression in Northeastern China: a cross-sectional study 6 weeks after giving birth. Front Public Health. 2025;13. doi:10.3389/fpubh.2025.1570654
24. Breault MS, Orguc S, Kwon O, et al. Anesthetics as treatments for depression: clinical insights and underlying mechanisms. Annu Rev Neurosci. 2025;48(1):103–124. doi:10.1146/annurev-neuro-112723-062031
25. Chen X, Zhao S, Chen D, Zhang D. The impact of sleep disorders on brain network connectivity in postpartum women: a functional near-infrared spectroscopy-based study. Front Neurol. 2024;15. doi:10.3389/fneur.2024.1487985
26. Wang Y, Lu H, Zhang F, Gu J. Path analysis of the factors associated with postpartum depression symptoms in postpartum women. J Psychiatric Res. 2025;182. doi:10.1016/j.jpsychires.2025.01.018
27. Khan-Afridi Z, Ruchat SM, Jones PA, et al. Impact of sleep on postpartum health outcomes: a systematic review and meta-analysis. British J Sports Med. 2025;59(8). doi:10.1136/bjsports-2024-109604
28. Fu T, Wang C, Yan J, Zeng Q, Ma C. Relationship between antenatal sleep quality and depression in perinatal women: a comprehensive meta-analysis of observational studies. J Affect Disord. 2023;327:38–45. doi:10.1016/j.jad.2023.01.125
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.