Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Effect of Progressive Resistance Strength Training on Body Mass Index, Quality of Life and Functional Capacity in Knee Osteoarthritis: A Randomized Controlled Trial
Authors Rafiq MT ![]() , A Hamid MS, Hafiz E
, A Hamid MS, Hafiz E
Received 27 May 2021
Accepted for publication 26 July 2021
Published 11 August 2021 Volume 2021:14 Pages 2161—2168
DOI https://doi.org/10.2147/JMDH.S317896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Muhammad Tariq Rafiq,1,2 Mohamad Shariff A Hamid,3 Eliza Hafiz2
1Rehmatul-Lil-Alameen Postgraduate Institute of Cardiology, Punjab Employees Social Security Institution, Lahore, Pakistan; 2Centre for Sport and Exercise Sciences, University of Malaya, Kuala Lumpur, 50603, Malaysia; 3Faculty of Medicine, Dean’s Office, University of Malaya, Kuala Lumpur, 50603, Malaysia
Correspondence: Muhammad Tariq Rafiq
Rehmatul-Lil-Alameen Postgraduate Institute of Cardiology, Punjab Employees Social Security Institution, Multan Chongi Multan Road, Lahore, Pakistan
Tel +92 42 99330102 Ext. 240
Fax +92 42 99330098
Email [email protected]
Purpose: This study aimed to investigate the effectiveness of progressive resistance strength training of the lower limb rehabilitation protocol (LLRP) on body mass index (BMI), quality of life, and functional capacity in patients with knee osteoarthritis (OA) who were overweight and obese.
Patients and Methods: Fifty-six patients were allocated into either the Rehabilitation Protocol Group (RPG) or the Control Group (CG) by a computer-generated random number. The patients in the RPG performed the strengthening exercises of the LLRP and followed the instruction of daily care (IDC). The patients in the CG only followed the IDC as a usual care. Gait Speed Test, quality of life, and BMI were taken at pre-test and post-test measurements. Paired samples t-test and two way mixed analysis of variance were used to analyze the change of BMI within and compare the difference of BMI between the groups, respectively. Wilcoxon signed ranked test and Mann–Whitney U-test were used to analyze the changes of quality of life and functional capacity within and compare the differences of quality of life and functional capacity between the groups, respectively.
Results: The patients in the RPG reported a significant reduction in BMI (p = 0.025), improvement in quality of life (p ≤ 0.001), and functional capacity (p ≤ 0.001) within group. The patients in the CG also reported a significant improvements in quality of life (p < 0.05). The improvement in quality of life score was greater in the patients with RPG than the CG (p = 0.053).
Conclusion: The progressive resistance strength training of LLRP is effective in terms of reducing BMI, improving quality of life and functional capacity.
Trial Registration: Name: Iranian Registry of Clinical Trials. Number: IRCT20191221045846N3. Enrollment of first participant: 27-07-2020.
Keywords: osteoarthritis, overweight, functional capacity, quality of life, body mass index
Introduction
Osteoarthritis (OA) is a major and most common health problem worldwide, causing illness and disability.1,2 Knee OA accounts for approximately 85% of the burden of OA worldwide.3 Prevalence of OA increases with age and the epidemic of obesity, it is set to rise.4 Knee OA causes loss of function and reduces quality of life.5 A study reported that the use of complementary and alternative medicine therapies was more common in obese knee OA patients with lower body mass index (BMI) than those with higher BMI levels. Use of conventional medications was more common in overweight and obese patients.6 A study suggested that the weakness of the quadriceps muscles preceded the onset of knee OA and therefore it could increase the risk of disease development, particularly in women.7 Ottawa Panel found evidence to support the use of therapeutic exercises, especially strengthening exercises and general physical activity, for the improvement of functional characteristics of the OA patients.8 Home-based exercise intervention may be effective for relieving Knee OA symptoms, increasing muscle strength of the lower limbs, physical functioning, and improving quality of life in community-dwelling Knee OA elderly patients.9 Clinical guidelines recommend exercise therapy as the primary non-pharmacologic treatment for Knee OA.10 A published article compared functional capacity and quality of life among obese and non-obese patients with knee OA. Results reported that patients with knee OA who were obese had the worst performance in the six-minute walk test, brisk walking speed, and timed up and go test. In addition, the obese group reported more difficulty in performing the tasks of standing, getting on/off the toilet, rising from a chair, and going downstairs. The quality of life scores in both groups was reduced.11 A recent study pointed out that an acceptable tool to estimate adiposity in OA patients was BMI.12 The study indicated that the significant improvement in Knee OA symptoms, quality of life, and muscle strength can be achieved by home-based exercise interventions. Currently, early-mid OA treatment options include visco-supplementation utilizing and reducing wear volume.13,14 In addition, a current study reported that OA is primarily the degradation of the articular cartilage tissue and can be treated with mechanotherapy.15 Currently, non-pharmacological knee OA treatment options include progressive resistance strength training of the lower limbs in nonweight bearing sitting or lying positions to reduce the mechanical load on the knee as well as to reduce wear volume of articular cartilage. The novelty of the current study could have been explained by the fact that the training sessions of progressive resistance strength training of the lower limb rehabilitation protocol (LLRP) were the strengthening exercises of the major muscle groups of the lower limbs in nonweight bearing sitting or lying positions to reduce the mechanical load on the knee in patients with knee OA who were overweight and obese. However, there is insufficient evidence on the effect of progressive resistance strength training of the LLRP in nonweight bearing sitting or lying positions on BMI, quality of life, and functional capacity in patients with knee OA. Hence, the current randomized controlled trial was conducted to investigate the effectiveness of progressive resistance strength training of the LLRP on BMI, functional capacity, and quality of life in patients with knee OA who were overweight and obese.
Materials and Methods
Participants
Participants were recruited from the urban area of Punjab, Lahore, Pakistan. Written informed consent was obtained prior to inclusion. The inclusion criteria were as follows: both males and females, overweight and obese knee OA patients having OA of one or both knees, age between 45 and 60 years, OA grading scale of 2-mild or 3-moderate according to Kellgren and Lawrence radiographic scale,16 symptoms of OA for more than three months and residing in the urban community of Lahore, Pakistan. Exclusion criteria were one or more of the following: flat feet, knee surgery, corticosteroid injection of the knee for the last 6-months, spinal deformities, cardiac problem, or hormonal problem.
Study Design
The study was a single blinded randomized controlled trial. The study was conducted at the urban area of Punjab, Lahore, Pakistan. The pre-test and post-test measurements were taken to carry out the records of demographics and clinical outcome measures of BMI, functional capacity, and quality of life.
In the initial interview, each treatment group was provided all details about their intervention protocol after screening by the predefined questionnaire of inclusion and exclusion criteria. Following an explanation of the purpose and constraints of the study, the participants were given written informed consent for their participation in the study. The current study was approved by the ethical committee of Rehmatul-Lil-Alameen Postgraduate Institute of Cardiology (RAIC), Punjab Employees Social Security Institution (PESSI), Lahore, Pakistan, with reference number RAIC PESSI/Estt/2020/2419 on date 30-03-2020 and the trial was registered in the Iranian Registry of Clinical Trials with registration number IRCT20191221045846N3 on date 20-07-2020. First participant was enrolled in the trial on date 27-07-2020.
Sample Size
To estimate the required sample size, the G* Power 3.1.3 software was used. By assuming the medium effect size f = 0.70, setting α = 0.05, power (1-B) = 0.80, number of groups = 2, number of measurements = 2, the total sample size was estimated to be 33 and as a result the study needed 33 participants. However, the researcher in the current study has taken the sample size of 56 for the two groups to cover the drop-out.
Participants’ Recruitment and Selection
The researcher recruited the participants by active recruitment strategies via word of mouth. A research article suggested that active recruitment strategies are 66.5 times more effective and personal compared to passive recruitment strategies.17 The researcher contacted the senior representatives of political and welfare organizations via word of mouth within the recruitment area and explained them the benefits of study participation. Two study coordinators prepared the list of potential participants of knee OA patients in the recruitment area. After obtaining the list of potential participants, they arranged a meeting with the knee OA patients by calling them on the phone. The meeting was held at the Teaching Bay of RAIC, PESSI, Lahore, Pakistan. Then the knee OA patients were screened for the study by a predefined questionnaire of inclusion and exclusion criteria. Those knee OA patients who did not fulfill the inclusion and exclusion criteria of the study were not invited to participate in the study. Overweight and obese knee OA patients fulfilling the inclusion and exclusion criteria were selected for the study.
Study Randomization
After completing the screening of Knee OA patients, the researcher allocated the 56 selected patients with knee OA who were overweight and obese into two groups, namely, Rehabilitation Protocol Group (RPG) and the Control Group (CG) using a computer-generated simple randomization technique. Each group was consisted of twenty-eight patients. Patients in the RPG performed the progressive resistance strength training of the LLRP in nonweight bearing sitting or lying positions as shown in Supplementary Table 1 and followed the instruction of daily care (IDC). Patients in the CG were not involved in the LLRP, but they only followed the IDC keeping in mind the ethical consideration of patients. The IDC is explained elsewhere.18 All patients were also given a diary and asked to record the attendance of completion their interventions based on leaflets.
Research Procedures
Rehabilitation Protocol Group (RPG)
Patients in the RPG performed the progressive resistance strength training of the LLRP in non-weight bearing sitting or lying positions three times a week and followed the IDC for a duration of 12-weeks at their homes. The progressive resistance strength training of LLRP were also translated into Urdu language by two language experts because the patients demanded the need of Urdu translation in a pilot study.18 This LLRP was consisted of a 45–60 minutes training session followed by 10 minutes’ warm-up at the start and 10 minutes cool down at the end of the training session. The frequency, intensity, and duration of training sessions of non-weight bearing progressive resistance strength training of the LLRP are explained in Supplementary Table 1. The whole body range of motion (ROM) exercises as part of warm-up or cool down are explained in Supplementary Table 2. A cool-down period is essential after a training session and should last approximately 5–10 minutes.19 When static stretching is used as part of a warm-up immediately prior to exercise, then it causes harm to muscle strength.20
Control Group (CG)
Patients in the CG followed the IDC only for a duration of 12-weeks. The IDC were also translated into Urdu language by two language experts as the patients’ preference of the Urdu translation for better understanding based on a recent pilot study.18
Clinical Outcome Measures
The measurements of demographics, BMI, quality of life, and functional capacity were taken at pre-test before the patients were randomized into two groups. The demographic questionnaire was consisted of age, gender, educational status, marital status, employment, and knee side involvement. The outcome measures were taken at pre-test and post-test measurements. Outcome measures were categorized into primary and secondary outcome measures.
Primary Outcome Measures
These were BMI and quality of life. For the assessment of BMI, the researcher measured the height (portable stadiometer, Perspective Enterprises, Portage, MI, USA) and weight (Seca 888 Scale, Seca, Hamburg, Germany). After the measurements of height and weight, BMI calculation was performed according to the formula (weight (kg)/height (m2) of the World Health Organization.21
The quality of life was measured by the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) summary score of pain, stiffness, and physical function. The WOMAC that is already adapted and validated was used. The WOMAC is a multidimensional questionnaire assessing pain, stiffness, and physical functional disability. Three dimensional (pain, stiffness, and physical function) quality of life questionnaire, WOMAC, is designed for the evaluation of hip and knee OA patients. The WOMAC score ranges from 0 to 4 on a Likert-type scale, the higher the score, the worse the pain, joint stiffness, and functionality.22,23
Secondary Outcome Measure
It was the functional capacity. Gait Speed Test was used for the assessment of functional capacity. Recording of the time was done when the patient completed a distance of 20 feet and then divided the distance with time for the calculation of gait speed. Gait speed measures obtained during a single test session are reliable. The coefficients (0.90) of comfortable gait speed were highly reliable.24 Gait speed test is used as an outcome measure in rehabilitation25 and in trials of interventions to delay the onset of disability or frailty.26
Statistical Analysis
Statistical Package for Social Sciences, version 23, Chicago, IL, was used to manage and analyze the data. For categorical demographic variables, chi-square test was used to assess the significance. Continuous variables were presented as mean (standard deviation (SD) for normal and median (interquartile range (IQR) for nonnormal variables. Categorical variables were presented as actual numbers (n) and percentages (%). Prior to data analysis, Shapiro–Wilk test was used to check the normality of all variables. The data of BMI were normally distributed, so the Paired Sample t-test was used to analyze the differences within groups from pre to post-test measurements. Two Way Mixed Analysis of Variance was used to compare the difference of BMI between the groups. The data of quality of life and functional capacity were not normally distributed; therefore, the nonparametric test (Wilcoxon Signed Ranked Test) was used to analyze the differences within groups from pre to post-test measurements. The Mann Whitney U-test was used to analyze the differences between groups for not normally distributed data. Value of P ≤ 0.05 was considered statistically significant.
Results
A total of 75 patients with knee OA were assessed for eligibility by a predefined questionnaire of inclusion and exclusion criteria. Of these, 19 patients were excluded for reasons as shown in Figure 1 and the remaining 56 patients were randomized and divided into the RPG and the CG. Five patients in the RPG were excluded because three were sick and the remaining two were outstations. Similarly, five in the CG were lost to follow-up because three got the urine problem and the remaining two were unwilling to continue due to domestic problems. A final total of 46 patients completed the study, and 23 of them completed the progressive resistance strength training of the LLRP in non-weight bearing sitting or lying positions (Figure 1).
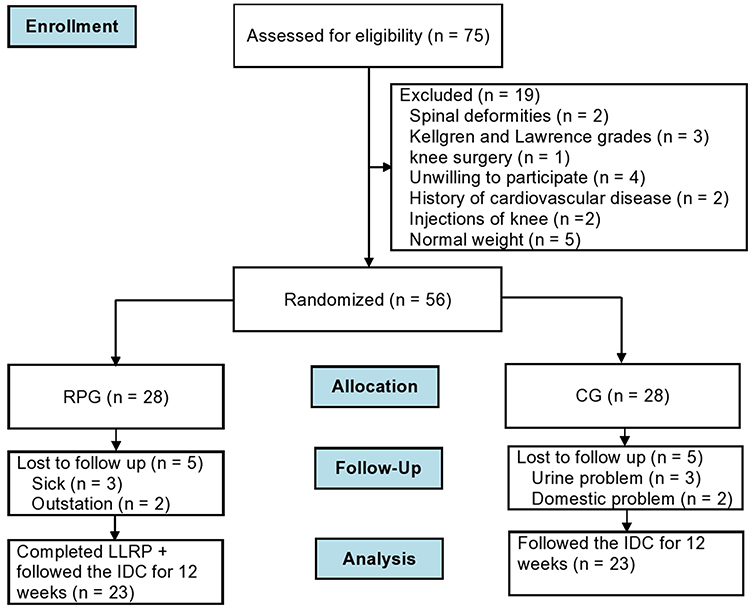 |
Figure 1 Flow diagram for study procedure. |
Both groups’ pre-test demographic characteristics and clinical outcome measures are shown in Table 1. No significant differences in pre-test demographic characteristics and clinical outcome measures were observed between the 2 groups.
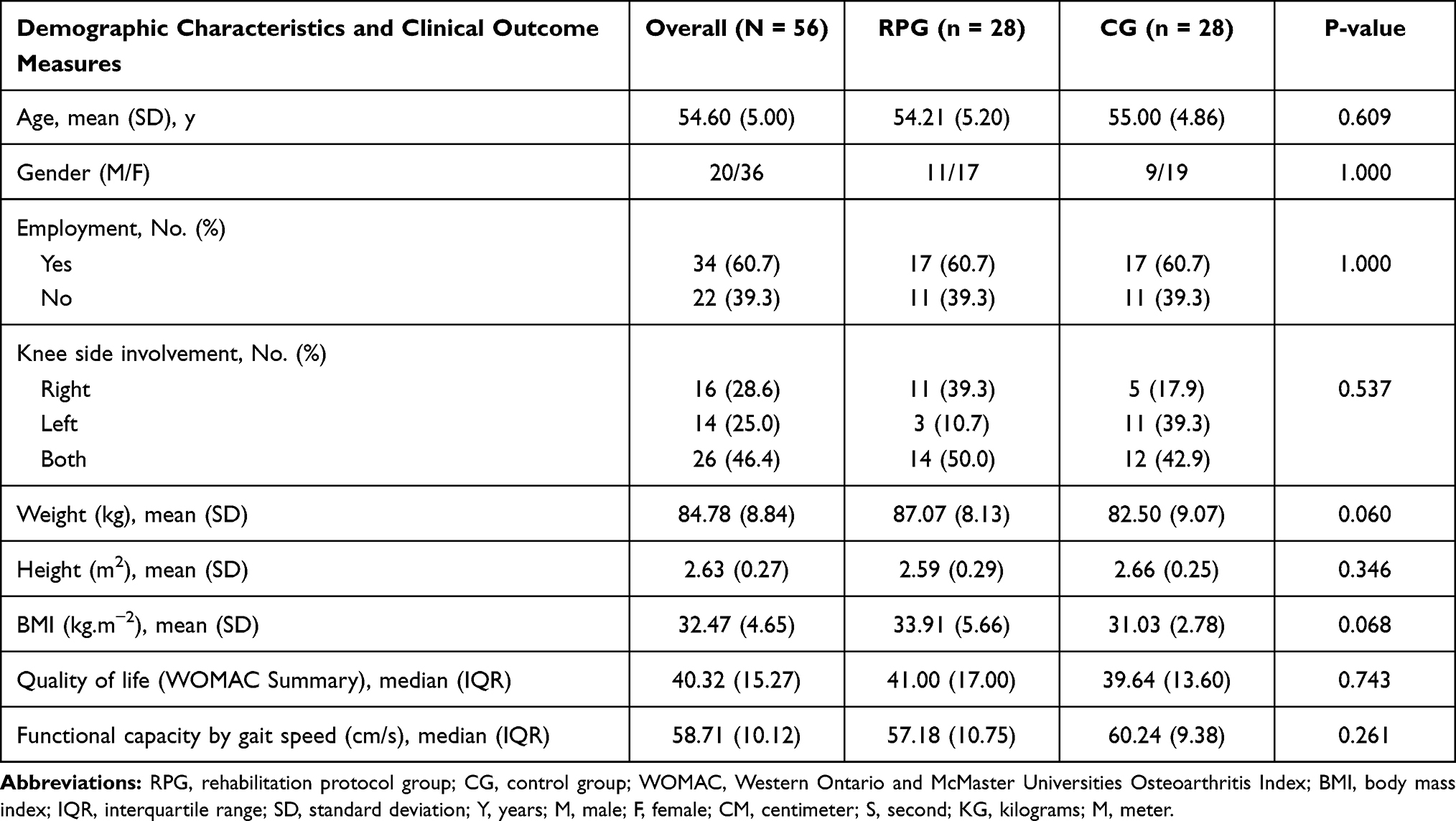 |
Table 1 Pre-Test Demographic Characteristics and Clinical Outcome Measures of Patients: Mean (SD), Median (IQR) or N (%) |
After 12 weeks of training sessions of progressive resistance strength training of the LLRP, patients in the RPG resulted a significant reduction in BMI (p = 0.025) measured by height and weight measurements, improvements in quality of life (p < 0.001) measured by the WOMAC summary and functional capacity (p < 0.001) measured by the Gait Speed Test scores (Supplementary Table 3). Similarly, a significant improvement was also reported in the scores of quality of life (p = 0.041) by the CG. By contrast, patients in the CG reported no significant reduction in BMI (p = 0.117) and improvement in the scores of functional capacity (p = 0.066) as shown in Supplementary Table 3.
When the effectiveness of clinical outcome measures was compared between the 2 groups, patients in the RPG showed more significant improvement in quality of life (p < 0.001) and functional capacity (p < 0.001) scores than the CG. However, patients in the RPG did not report significantly in BMI score than the CG (p = 0.806) (Table 2).
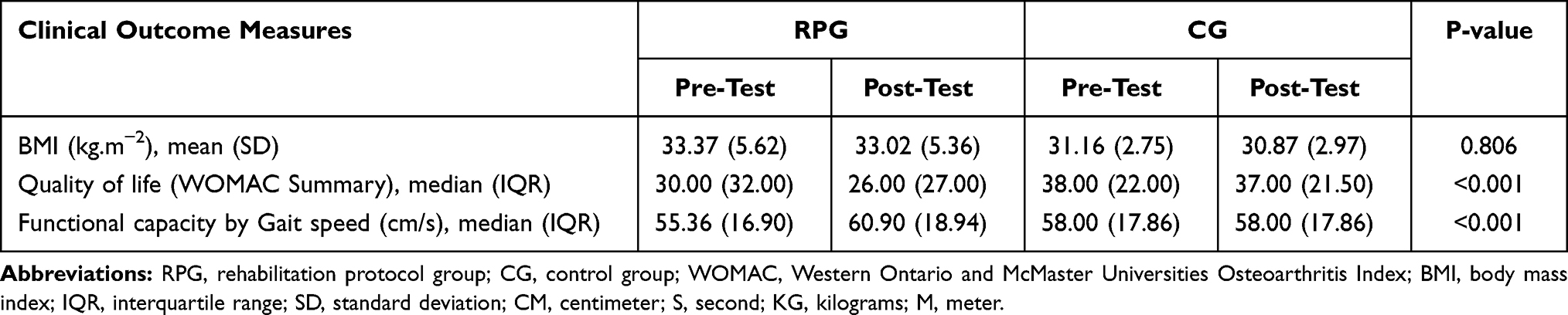 |
Table 2 Comparison of Clinical Outcome Measures Between the Groups (RPG and CG) |
There were no adverse as well as suspected unexpected serious adverse reactions reported in the current study.
Discussion
Exercise is often indicated as one of the main components in the rehabilitation process.27 Core recommended treatments for knee OA in OA clinical guidelines are lower limb muscle strengthening.28 Progressive resistance strength training of the LLRP in non-weight bearing sitting or lying positions may provide more objective data than the standard rehabilitation approaches we are using today to treat patients with knee OA. Therefore, the current study investigated the effectiveness of progressive resistance strength training of the LLRP on BMI, quality of life, and functional capacity in patients with knee OA who were overweight and obese. The results of the current study reported improvement in quality of life in patients of the RPG and CG, on the other hand, reduction in BMI and improvement in functional capacity could be seen only in patients of the RPG, but not in the CG. The results indicated that patients in the RPG, who performed the progressive resistance strength training of the LLRP in non-weight bearing sitting or lying positions to reduce the mechanical load on the knee, reported greater improvements in quality of life, and functional capacity than did the patients in the CG. However, patients in the RPG did not report significantly in BMI than patients in the CG. In the current study, knee OA was more common in females (64.28%) than males (35.71%). The mean age of the overall sample was 54.60 years (SD = 5.00 years). The majority of the study patients were employed (60.7%).
In a randomized clinical trial of 316 overweight or obese elderly men and women with knee OA, it was noted that the combination of diet and exercise was more successful in improving health-related quality of life, if compared with exercise or diet as single interventions.29 Because there is no cure for this disease, current medical practice focuses on such interventions that reduce the progression of the disease as well as the negative impact on health-related quality of life.30 In the current study, patients in the RPG resulted significant improvements in quality of life. Recently, a study demonstrated that a combination of dietary weight loss and exercise intervention was consistently better in improving a combination of performance and functional outcomes among participants with knee OA compared with exercise alone, diet alone, or a control group. A weight loss of 5% of body weight will improve function and increase mobility.31 The intervention group of the current study was also a combination of IDC and progressive resistance strength training of the LLRP that reported significant results in improving functional capacity. According to the Osteoarthritis Research Society International Committee for Clinical Trials Response Criteria Initiative and the Outcome Measures in Rheumatology Committee, response to treatment in clinical trials should be based on symptomatic response to therapy in the domain of function, and the patient’s global assessment.32 Obesity data highlights an opportunity to improve the quality of life scores in knee OA patients by following nutritional education and dietary guidelines.33 In the current study, the IDC also focused on caloric restriction diet. The feasibility and acceptability of the IDC in overweight and obese knee OA participants have been proved effective and the IDC is recommended as a usual care of treatment in a current randomized controlled trial.34 A pragmatic randomized controlled trial reported that telephone-based weight loss support did not affect weight and consequently no effect on BMI (mean score of 0.10).35 The results of the above pragmatic randomized controlled trial are inconsistent with the results of the current study, in which patients in the RPG reported a significant improvement in BMI (mean score of 0.34).
Study Limitations
The present study had some limitations. It was conducted in a single centre to recruit patients. No long-term follow-up records were taken. Thus, further blinded studies across multiple centres and long-term follow-up are required to confirm the results of the progressive resistance strength training of the LLRP in patients with knee OA.
Conclusion
The results of the current study showed effectiveness in reducing BMI as well as improving quality of life and functional capacity in patients with knee OA who were overweight and obese by the implementation of progressive resistance strength training of LLRP in non-weight bearing sitting or lying positions. The progressive resistance strength training of LLRP was more effective for improving quality of life and functional capacity than conventional treatment alone. In addition, the progressive resistance strength training of the LLRP is easy to use in the home care setting and can also be used for hemiplegia, paraplegia, or wheelchair patients with lower limb weakness.
Data Sharing Statement
The dataset of this manuscript is available on reasonable request through the corresponding author.
Ethics Approval and Consent to Participate
This study was performed in accordance with the ethical standards of the Declaration of Helsinki. This study was approved by the ethics committee of the Rehmatul-Lil-Alameen Postgraduate Institute of Cardiology, Punjab Employees Social Security Institution, Lahore, Pakistan (RAIC PESSI/Estt/2020/2419) and the trial was registered in the Iranian Registry of Clinical Trials (IRCT20191221045846N3). All participants gave their informed consent before participation.
Consent for Publication
All participants signed the consent for publication.
Acknowledgments
We would like express our deepest gratitude to University of Malaya, Centre for Sport and Exercise Sciences, 50603 Kuala Lumpur, Malaysia, for giving us the chance to do this paper.
Funding
This study did not receive financial resources.
Disclosure
The authors declare that they have no competing interests.
References
1. Nguyen US, Zhang Y, Zhu Y, et al. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: survey and cohort data. Ann Intern Med. 2011;155(11):725–732. doi:10.7326/0003-4819-155-11-201112060-00004
2. Johnson VL, Hunter DJ. The epidemiology of osteoarthritis. Best Pract Res Clin Rheumatol. 2014;28(1):5–15. doi:10.1016/j.berh.2014.01.004
3. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1545–1602. doi:10.1016/S0140-6736(16)31678-6
4. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet. 2011;377(9783):2115–2126. PMID: 21684382. doi:10.1016/S0140-6736(11)60243-2
5. McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr Cartil. 2014;22(3):363–388. doi:10.1016/j.joca.2014.01.003
6. Lapane KL, Yang S, Jawahar R, et al. CAM use among overweight and obese persons with radiographic knee osteoarthritis. BMC Complement Altern Med. 2013;13(1):241. doi:10.1186/1472-6882-13-241
7. Bennell KL, Hunt MA, Wrigley TV, et al. Muscle and exercise in the prevention and management of knee osteoarthritis: an internal medicine specialist’s guide. Med Clin North Am. 2009;93(1):161–177. doi:10.1016/j.mcna.2008.08.006
8. Brosseau L; Ottawa Panel Members, Ottawa Methods Group. Ottawa panel evidence-based clinical practice guidelines for therapeutic exercises and manual therapy in the management of osteoarthritis. Phys Ther. 2005;85(9):907–971. doi:10.1093/ptj/85.9.907
9. Chen H, Zheng X, Huang H, et al. The effects of a home-based exercise intervention on elderly patients with knee osteoarthritis: a quasi-experimental study. BMC Musculoskelet Disord. 2019;20(1):160. doi:10.1186/s12891-019-2521-4
10. Nelson AE, Allen KD, Golightly YM, et al. A systematic review of recommendations and guidelines for the management of osteoarthritis: the chronic osteoarthritis management initiative of the US bone and joint initiative. In: Seminars in Arthritis and Rheumatism. Vol. 43. WB Saunders;2014:701–712. doi:10.1016/j.semarthrit.2013.11.012
11. Gomes-Neto M, Araujo AD, Junqueira ID, et al. Comparative study of functional capacity and quality of life among obese and non-obese elderly people with knee osteoarthritis. Braz J Rheumatol. 2016;56(2):126–130. doi:10.1016/j.rbre.2015.08.014
12. Alfieri FM, Battistella LR, Battistella LR. Study of the relation between body weight and functional limitations and pain in patients with knee osteoarthritis. Einstein (São Paulo). 2017;15(3):307–312. doi:10.1590/s1679-45082017ao4082
13. Rebenda D, Vrbka M, Nečas D, et al. Rheological and frictional analysis of viscosupplements towards improved lubrication of human joints. Tribol Int. 2021;160:107030. ISSN0301-679X. doi:10.1016/j.triboint.2021.107030
14. Rebenda D, Vrbka M, Cípek P, et al. On the dependence of rheology of hyaluronic acid solutions and frictional behavior of articular cartilage. Materials. 2020;13(11):2659. doi:10.3390/ma13112659
15. Marian M, Shah R, Gashi B, et al. Exploring the lubrication mechanisms of synovial fluids for joint longevity–a perspective. Colloids Surf B Biointerfaces. 2021;16:111926. doi:10.1016/j.colsurfb.2021.111926
16. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494. doi:10.1136/ard.16.4.494
17. Mody L, Miller DK, McGloin JM, et al. Recruitment and retention of older adults in aging research: (see editorial comments by Dr. Stephanie Studenski, pp 2351–2352). J Am Geriatr Soc. 2008;56(12):2340–2348. doi:10.1111/j.1532-5415.2008.02015.x
18. Rafiq MT, A Hamid MS, Hafiz E, Amin S. Rehabilitation protocol with or without mobile health in overweight and obese knee osteoarthritis patients - a Pilot Study. Balneo Res J. 2019;10(4):580–584. doi:10.12680/balneo.2019.306
19. Powers SK, Howley ET. Exercise Physiology: Theory and Application to Fitness and Performance. New York, NY: McGraw-Hill; 2007.
20. McHugh MP, Nesse M. Effect of stretching on strength loss and pain after eccentric exercise. Med Sci Sports Exerc. 2008;40(3):566–573. doi:10.1249/MSS.0b013e31815d2f8c
21. Expert Consultation WHO. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
22. Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15(12):1833–1840.
23. Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes following total hip and knee arthroplasty in osteoarthritis. J Orthop Rheumatol. 1988;1:95–108.
24. Bohannon RW. Comfortable and maximum walking speed of adults aged 20–79 years: reference values and determinants. Age Ageing. 1997;26(1):15–19. doi:10.1093/ageing/26.1.15
25. Skinner A, Turner-Stokes L. The use of standardized outcome measures in rehabilitation centres in the UK. Clin Rehabil. 2006;20(7):609–615. doi:10.1191/0269215506cr981oa
26. Fairhall N, Aggar C, Kurrle SE, et al. Frailty intervention trial (FIT). BMC Geriatr. 2008;8(1):27. doi:10.1186/1471-2318-8-27
27. Bartholdy C, Juhl C, Christensen R, et al. The role of muscle strengthening in exercise therapy for knee osteoarthritis: a systematic review and meta-regression analysis of randomized trials. Semin Arthritis Rheum. 2017;47(1):9–21. doi:10.1016/j.semarthrit.2017.03.007
28. Heidari B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: part I. Casp J Intern Med. 2011;2(2):205–212.
29. Rejeski WJ, Focht BC, Messier SP, et al. Obese, older adults with knee osteoarthritis: weight loss, exercise, and quality of life. Health Psychol. 2002;21(5):419. doi:10.1037/0278-6133.21.5.419
30. Rejeski WJ, Brawley LR, Shumaker SA. Physical activity and health-related quality of life. Exerc Sport Sci Rev. 1996;24(1):71–108. doi:10.1249/00003677-199600240-00005
31. Messier SP, Loeser RF, Miller GD, et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the arthritis, diet, and activity promotion trial. Arthritis Rheum. 2004;50(5):1501–1510. doi:10.1002/art.20256
32. Pham T, van der Heijde DM, Altman RD, et al. Osteoarthritis research society international set of responder criteria for osteoarthritis clinical trials revisited. Osteoarthr Cartil. 2004;12(5):389–399. doi:10.1016/j.joca.2004.02.001
33. Gomes-Neto M, Araujo AD, Junqueira ID, et al. Comparative study of functional capacity and quality of life among obese and non-obese elderly people with knee osteoarthritis. Rev Bras Reumatol Engl Ed. 2016;56(2):126–130.
34. Rafiq MT, A Hamid MS, Hafiz E, et al. Feasibility and acceptability of instructions of daily care in overweight and obese knee osteoarthritis participants. Curr Rheumatol Rev. 2021Jul 26. doi:10.2174/1573397117666210727095552. Epub ahead of print. PMID: 34315379.
35. O’Brien KM, Wiggers J, Williams A, et al. Telephone-based weight loss support for patients with knee osteoarthritis: a pragmatic randomised controlled trial. Osteoarthritis Cartilage. 2018;26(4):485–494. doi:10.1016/j.joca.2018.01.003
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.