Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Oliceridine on Sufentanil-Induced Cough During General Anesthesia: A Prospective Randomized Controlled Clinical Study
Authors Gong WY, Li CG, Ge CL, Zhao CX, Yuan W, Yue XF, Fan K ![]()
Received 19 May 2025
Accepted for publication 21 November 2025
Published 17 December 2025 Volume 2025:19 Pages 11317—11324
DOI https://doi.org/10.2147/DDDT.S541146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Wen-Yi Gong,1,* Chen-Guang Li,2,* Chun-Lin Ge,1,* Chun-Xia Zhao,3 Wei Yuan,1 Xiao-Fang Yue,4 Kun Fan5
1Department of Anesthesiology, Shanghai Xuhui Central Hospital, Shanghai, People’s Republic of China; 2Department of Anesthesiology, The First People’s Hospital of Tianshui, Gansu, People’s Republic of China; 3Department of Medical Education and Research, The First People’s Hospital of Tianshui, Gansu, People’s Republic of China; 4Department of Neurology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China; 5Department of Anesthesiology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kun Fan, Department of Anesthesiology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiaotong University School of Medicine, No. 600, Yishan Road, Shanghai, 200233, People’s Republic of China, Tel +8618964917372, Fax +8602164701361, Email [email protected] Xiao-Fang Yue, Department of Neurology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiaotong University, No. 600, Yishan Road, Shanghai, 200233, People’s Republic of China, Tel +8615821237895, Fax +8602164701361, Email [email protected]
Background: Sufentanil-induced cough (SIC) frequently occurs during the induction of general anesthesia and may result in serious clinical complications, occasionally posing life-threatening risks. In clinical practice, we observed that oliceridine—a G protein-biased μ-opioid receptor agonist—demonstrates a potent suppressive effect on SIC. This study aimed to evaluate the efficacy of oliceridine in preventing SIC and to assess any associated adverse events.
Methods: In this prospective, randomized, double-blind, placebo-controlled trial, 286 adult patients undergoing elective surgery under general anesthesia were enrolled and randomly assigned to receive either 2 mg oliceridine (OS group) or an equal volume of normal saline (SS group) before intravenous administration of sufentanil. The primary outcome was the incidence of SIC. Secondary outcomes included the severity of cough, vital sign changes, and adverse events.
Results: The incidence of SIC was 42.66% in the SS group and 0% in the OS group (95% upper confidence bound ≈ 2.6%; P < 0.001). Among the SS group, mild, moderate, and severe cough occurred in 12.59%, 26.57%, and 3.50% of patients, respectively. No significant differences were observed in systolic or diastolic blood pressure, heart rate, or SpO2 between the two groups at baseline or 2 minutes post-sufentanil administration. The incidence of adverse events was low and comparable between groups, with no reported cases of apnea, nausea, or vomiting.
Conclusion: Pretreatment with 2 mg oliceridine demonstrated favorable effevtiveness in suppressing SIC without significant adverse effects. Oliceridine appears to be a safe and effective prophylactic strategy for preventing SIC and may have valuable clinical utility in anesthesia practice.
Keywords: oliceridine, sufentanil, opioid-induced cough, general anesthesia, μ-opioid receptor
Introduction
Sufentanil, a potent synthetic opioid analgesic, is widely used in clinical anesthesia for its rapid onset and strong analgesic properties. However, intravenous administration during anesthetic induction may provoke a reflex cough, with a reported incidence of up to approximately 35%.1 Clinically, sufentanil-induced cough (SIC) has been associated with abrupt increases in blood pressure, as well as elevated intraocular, intracranial, intrapulmonary, and intra-abdominal pressures, and may even result in upper airway obstruction. In certain cases, the cough reflex can be spasmodic and explosive, and may occasionally become life-threatening.2,3 These adverse events pose significant risks to patient safety and perioperative outcomes.
Various pharmacological interventions, including lidocaine, atropine, magnesium sulfate, dexamethasone, propofol, midazolam, muscle relaxants (rocuronium, vecuronium), ketamine, pentazocine, tramadol, α2-agonists (clonidine, dexmedetomidine), β2-agonists (terbutaline, ephedrine), sodium cromoglycate, beclomethasone, salbutamol, and dextromethorphan, as well as non-pharmacological methods such as opioid pretreatment, dilution, and slow injection, have been employed to manage opioid-induced coughing (OIC).4 Unfortunately, the efficacy and safety of these antitussive interventions remain controversial.4
Oliceridine is a biased μ-opioid receptor agonist approved by the US Food and Drug Administration (FDA) in 2020, primarily as an alternative therapy for acute pain in adults inadequately managed with traditional opioids.5 Clinically, we observed that oliceridine significantly suppresses SIC during induction, yet this has been rarely reported previously. To address this clinical issue, we designed a prospective, randomized, double-blind, placebo-controlled study to clarify the effects of oliceridine on SIC during anesthesia induction.
Materials and Methods
Study Design and Ethics
This study was a prospective, single-center, randomized, double-blind, placebo-controlled, clinical trial. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of the First People’s Hospital of Tianshui (Approval No.: 2025–06; Date of approval: April 2, 2025). The trial was registered in the Chinese Clinical Trial Registry (Registration No.: ChiCTR2500100414). This report adheres to the Consolidated Standards of Reporting Trials (CONSORT) guidelines. Written informed consent was obtained from all participants and their legal guardians prior to study enrollment.
Enrollment
Patients were initially recruited through informational brochures distributed in the surgical wards of the First People’s Hospital of Tianshui. Inclusion criteria were as follows: age between 18 and 70 years, American Society of Anesthesiologists (ASA) physical status I–III, and scheduled to undergo elective surgery under general anesthesia. Patients were excluded based on the following criteria: history of drug allergy; sinus bradycardia; severe neurological, respiratory, or cardiovascular disorders; anesthetic drug dependence or recent opioid use; smoking history; hepatic or renal dysfunction; pregnancy, lactation, or delivery-related surgeries; and upper respiratory tract infection within two weeks prior to surgery, which could predispose patients to spontaneous coughing.
Randomization and Blinding
Patients were randomly assigned to either the Oliceridine group (OS) or Saline group (SS) in a 1:1 ratio using simple randomization via random sequence generator (http://www.random.org). The allocation results were concealed in sealed opaque sequentially numbered envelopes that were provided to the research coordinator. On the day of surgery, the research coordinator delivered the envelope to an unblinded drug preparer, who was not involved in subsequent study procedures. According to the assigned protocol indicated within the envelope, the drug preparer prepared the study medications. In the OS group, oliceridine (2 mg) was diluted with normal saline to a final volume of 5 mL; in the SS group, 5 mL normal saline alone was used. The two study drugs were placed into identical syringes, which were subsequently labeled as “Syringe 1” and “Syringe 2”. After preparation, the drug preparer delivered the syringes containing the study drugs to the investigator responsible for drug administration. They resealed the envelopes and then returned them to the research coordinator. The study medications were maintained at room temperature (20°C–22°C) and administered within 10 minutes of preparation. Patients, the research coordinator, the investigator responsible for drug administration, and the statistician were all blinded to the group allocation and drug identity throughout the study.
Anesthesia and Procedure
An intravenous (IV) cannula (22G) was inserted into the dorsum of the right forearm for each patient, followed by continuous infusion of balanced crystalloid solution. Standard monitoring, including heart rate, noninvasive blood pressure, and peripheral oxygen saturation, was initiated upon arrival in the operating room and maintained until the completion of surgery.
Sufentanil was diluted with normal saline to achieve a final concentration of 5 µg/mL, and the syringe was clearly labeled with the drug name and concentration. All patients received an intravenous injection of either 2 mg oliceridine (OS group) or an equal volume of 0.9% normal saline (SS group), administered over 3–5 seconds prior to anesthetic induction. The selected 2 mg intravenous dose was determined with reference to the dosing standards approved by the US Food and Drug Administration for oliceridine in the management of acute pain, and considering an appropriate balance between efficacy and safety. This was immediately followed by an intravenous bolus of prepared sufentanil 0.5 µg/kg, administered over 2 seconds. The occurrence and severity of reflex cough were assessed in real time by a blinded observer positioned at the patient’s bedside within 2 minutes following sufentanil administration. The present study determined the observation period for SIC to be within 2 minutes, in accordance with methodological designs reported in previous studies6–8 on OIC and supported by clinical practice experience. No other medications were given to the patients prior to the administration of the study drugs.
Upon completion of the observation period or in the event that oxygen saturation dropped below 90%, anesthesia induction was initiated with propofol (1–1.5 mg/kg) and rocuronium (0.9 mg/kg), followed by positive pressure ventilation.
Outcome Measurement
All outcomes were assessed and documented by the research coordinator. The primary outcome of this study was the incidence of cough following intravenous administration of sufentanil. Secondary outcomes included: (1) The number of patients experiencing varying degrees of cough severity (mild [1–2 coughs], moderate [3–5 coughs], and severe [>5 coughs]);9 (2) Systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and peripheral oxygen saturation (SpO2), recorded at baseline immediately prior to administration of oliceridine or normal saline (T0), and at 2 minutes after sufentanil injection (T1); (3) Other adverse events related to oliceridine and sufentanil, such as truncal rigidity, oxygen desaturation (defined as SpO2 <90%), apnea, nausea and vomiting.
Sample Size Calculation
The sample size calculation was performed using PASS 15 software (NCSS, LLC, Kaysville, UT, USA) based on the primary outcome, which was the incidence of cough following intravenous administration of sufentanil. Referring to previous reports, the incidence of SIC during anesthetic induction was approximately 35%.1 We hypothesized that pretreatment with oliceridine would reduce this incidence by 50%, to an expected incidence of 17.5%. The sample size was estimated using a two-sided Z-test for two independent proportions (unpooled variance). Therefore, at least 128 patients per group were required to achieve 90% statistical power at a two-tailed significance level (α) of 0.05. Considering a potential dropout rate of approximately 10%, a total of 143 patients per group were enrolled in this study.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics software (Version 22.0; IBM Corp., Armonk, NY, USA) in the intention-to-treat (ITT) population, which included all randomized patients. A two-tailed P-value < 0.05 was considered statistically significant. Secondary outcomes were designated as exploratory, without adjustment for multiplicity.
Categorical variables were expressed as numbers (percentages) and compared using Fisher’s exact test owing to zero-cell issues. Effect sizes were reported as absolute risk reduction (ARR) and number needed to treat (NNT), with corresponding 95% confidence interval (CI). Relative risks (RR) were additionally calculated using the Haldane–Anscombe correction for zero-cell counts. Between-arm comparisons of ordinal categorical variables were not estimable due to zero-cell counts in the treatment group; therefore, only descriptive distributions were presented for the control group.
Continuous variables were presented as means ± standard deviation (mean ± SD). Given the large sample size, t-tests were considered acceptable, with distributional assumptions assessed using Q–Q plots and residual diagnostics. Repeated-measures mixed-effects models with fixed effects for group, time, and their interaction (group×time), and random intercepts for subjects, were used to analyze continuous outcomes. Results were presented as a single group×time P value with β estimates and 95% CI.
Outcomes
A total of 318 patients were initially screened for eligibility. Among them, 286 met all inclusion and exclusion criteria and were randomly assigned in a 1:1 ratio to the OS group or the SS group. Thirty-two patients were excluded due to not meeting eligibility criteria, declining participation, or changes in the planned anesthesia protocol. All randomized patients completed the study and were included in the final analysis, with no dropouts observed (Figure 1). Because of the randomization procedure, baseline demographic characteristics and sufentanil administered during induction were well balanced between the two groups (Table 1).
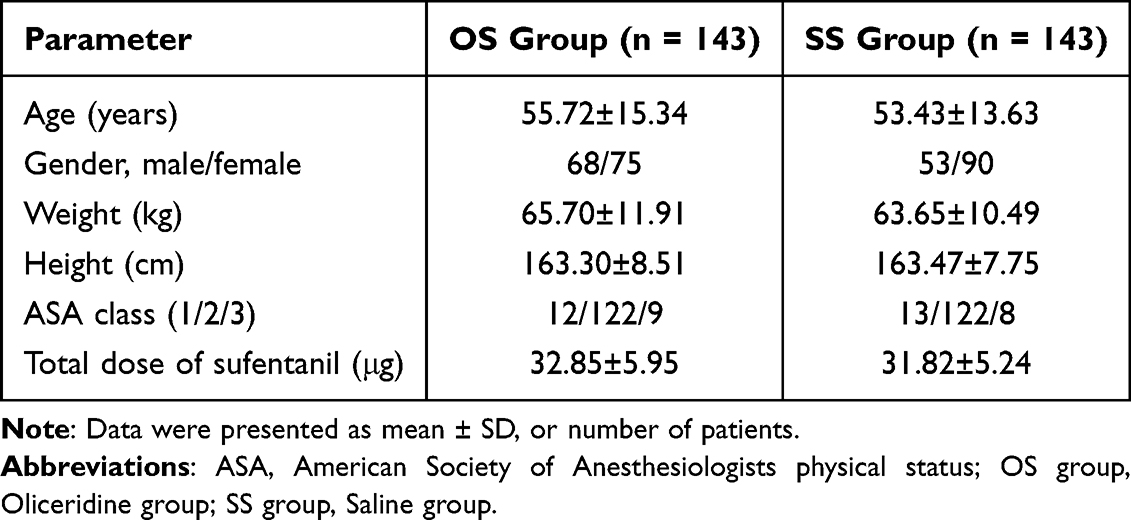 |
Table 1 Demographic Characteristics and Total Dose of Sufentanil |
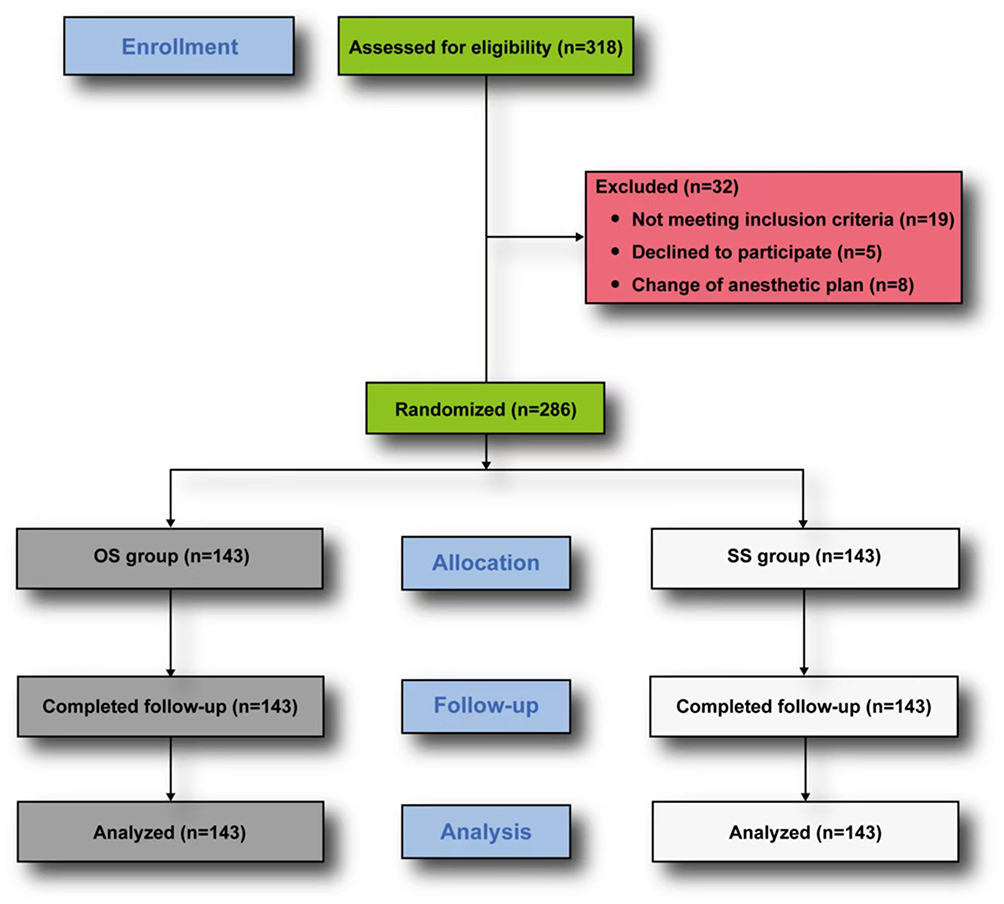 |
Figure 1 Consolidated standards of reporting trials flow diagram. Abbreviations: OS group, Oliceridine group; SS group, Saline group. |
No patients in the OS group experienced SIC during anesthetic induction (95% upper confidence bound ≈ 2.6%), whereas the incidence in the SS group was 42.66%, with rates of mild, moderate, and severe coughing at 12.59%, 26.57%, and 3.50%, respectively. The difference in the incidence of SIC between the two groups was statistically significant (P < 0.0001; 42.66% vs 0%; Table 2). The difference in the incidence of severity of SIC between the two groups could not be compared because no coughing events occurred in the OS group.
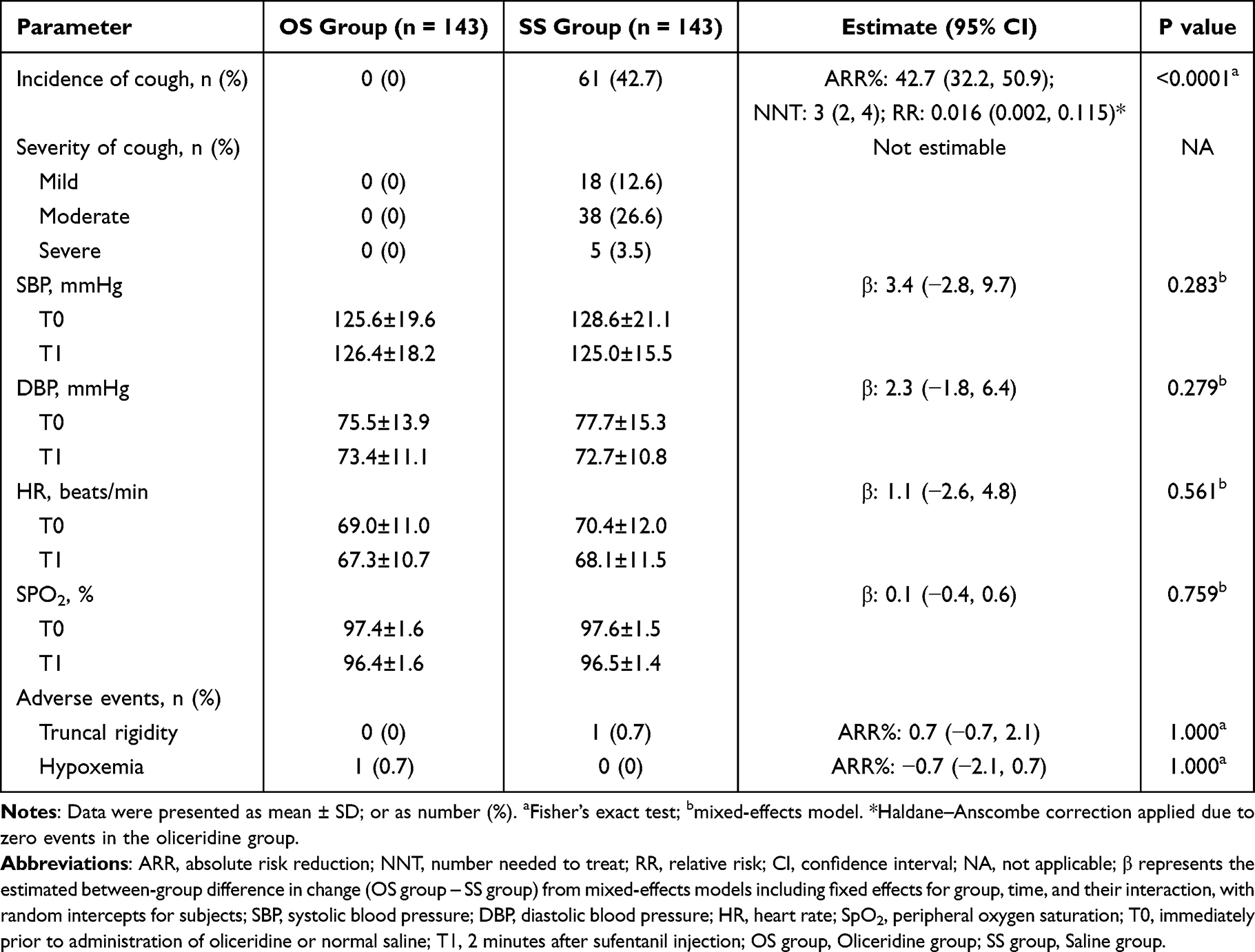 |
Table 2 Incidence and Severity of Sufentanil-Induced Cough, Vital Sign Changes, and Adverse Events After Treatment in Both Groups |
Repeated-measures mixed-effects models showed no significant group×time interactions for SBP, DBP, HR, or SpO2, indicating comparable peri-induction trajectories between the two groups. (Table 2). In the SS group, one patient developed transient limb rigidity without accompanying oxygen desaturation, and no intervention was required. In the OS group, one patient experienced a transient drop in oxygen saturation to 87%, which resolved promptly after jaw lift, with SpO2 returning above 90% (Table 2). However, the between-group differences in the incidence of muscle rigidity and oxygen desaturation were not statistically significant. No patients in either group experienced apnea or nausea and vomiting as adverse events.
Discussion
The results of this study demonstrated that the incidence of SIC reached as high as 42.7%, consistent with previously reported findings. Pretreatment with oliceridine was associated with no observed cases of SIC in this study (95% upper confidence bound ≈ 2.6%), while maintaining stable vital signs and without significant adverse effects. To our knowledge, this finding has not been previously reported.
Reflex coughing frequently occurs after opioid administration during anesthetic induction. The reported incidence of OIC varies widely across studies.10–13 Numerous factors may influence the occurrence of OIC, including opioid dose and concentration, order of administration, speed and site of intravenous injection, individual physiological characteristics, age, sex, body weight, medical history, smoking status, and genetic predisposition.14 However, the underlying mechanisms of opioid-induced cough remain poorly understood. One hypothesis suggests that opioids significantly suppress central sympathetic nervous system activity following injection, leading to a relative increase in vagal tone that may trigger coughing.15 Another proposed mechanism involves the activation of pulmonary chemoreflex pathways mediated by vagal C-fiber receptors located near pulmonary vessels, resulting in bronchoconstriction and cough.16 Reduced chest wall compliance following opioid administration may also lead to sudden vocal cord adduction or supraglottic obstruction, provoking a cough reflex.17
Furthermore, the release of substances like histamine and neuropeptides acting on presynaptic μ-opioid receptors has been implicated in cough induction.3 In addition, a previous study suggested that opioid receptor dualism may also play a role in mediating cough. Opioids primarily produce antitussive effects through their actions on central opioid receptors, whereas preferential activation of peripheral receptors has been associated with cough induction.9
A randomized controlled trial conducted by Zhang J demonstrated that pretreatment with remifentanil significantly reduced the incidence of SIC. The authors attributed this effect to the preferential occupancy of μ-opioid receptors by remifentanil, thereby preventing sufentanil from eliciting its tussive effect through the same receptor pathway.1 As a G protein-biased μ-opioid receptor agonist,18 oliceridine may exert a similar receptor-occupying effect when used as a pretreatment, which could represent a primary mechanism by which it suppresses SIC. Additionally, a randomized controlled study by Chengyong Gu reported that low-dose fentanyl pretreatment attenuated cough responses induced by subsequent high-dose fentanyl administration. This effect was hypothesized to result from the depletion of neurotransmitters in peripheral nerve fibers, particularly in pulmonary vagal C-fiber terminals.12 Accordingly, it is plausible that oliceridine pretreatment similarly depletes neurotransmitters from rapidly adapting receptors, constituting another potential mechanism for the suppression of SIC. Moreover, the concurrent use of two opioids may enhance central inhibitory effects, leading to simultaneous suppression of both sympathetic and vagal tones and thereby preventing autonomic imbalance. Central muscle relaxation induced by opioid co-administration may also help prevent vocal cord closure and preserve respiratory muscle tone, further contributing to the attenuation or elimination of SIC.
Currently, several agents have been identified as effective in reducing opioid-induced cough, including butorphanol, lidocaine, ketamine, dexmedetomidine, fentanyl, propofol, dezocine, dexamethasone, and magnesium sulfate.19–21 However, most of these agents do not completely eliminate OIC and are associated with a variety of adverse events. High-dose lidocaine, when used during induction of general anesthesia, may cause arrhythmias and cardiovascular depression.22 Ketamine has been reported to induce hallucinations and elevate blood pressure, intraocular pressure, and intracranial pressure.20 Dexmedetomidine may result in hypotension and bradycardia,23 while dexamethasone is associated with hyperglycemia and increased risk of infection. Magnesium sulfate has been linked to nausea, vomiting, and dyspnea.24 Although dezocine and butorphanol have shown near-complete suppression of OIC, they are also associated with adverse events such as respiratory depression and postoperative nausea and vomiting.8,14,19,25 Additionally, both propofol and fentanyl carry the risk of significant respiratory and cardiovascular depression.20 In contrast, the results of the present study demonstrated that pretreatment with oliceridine effectively suppressed SIC without inducing any clinically significant adverse events. Compared to the aforementioned agents, oliceridine may offer superior clinical utility due to its favorable efficacy and safety profile.
This study has several limitations. First, it did not evaluate the efficacy of oliceridine pretreatment in suppressing cough induced by other opioid agents. Second, the optimal dose of oliceridine for the prevention of SIC was not explored. Additionally, potential long-term adverse effects associated with the combined use of these two opioids were not assessed. In future studies, we aim to further investigate the efficacy and safety profile of oliceridine in preventing OIC.
Conclusion
In conclusion, pretreatment with 2 mg of oliceridine demonstrated favorable effectiveness in reducing both the incidence and severity of SIC without producing any significant adverse effects. These findings suggest that oliceridine may be a promising adjunct for use during the induction of general anesthesia. As a preventive strategy against SIC, oliceridine demonstrates clinical potential and merits further investigation and broader application.
Data Sharing Statement
The data are available from the corresponding author ([email protected]) on reasonable request.
Ethical Statement
This study strictly abided by the CONSORT reporting criteria for RCT. The study was ethically endorsed by the First People’s Hospital of Tianshui (Approval No.: 2025-06; Date of approval: April 2, 2025) and registered at the Chinese Clinical Trial Registry (Registration No.: ChiCTR2500100414).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang J, Zhang D, Liu Y, et al. Effects of remifentanil pretreatment on sufentanil-induced cough suppression during the induction of general anesthesia. J Perianesth Nurs. 2025;40(1):90–94. doi:10.1016/j.jopan.2024.03.015
2. Tweed WA, Dakin D. Explosive coughing after bolus fentanyl injection. Anesth Analg. 2001;92(6):1442–1443. doi:10.1097/00000539-200106000-00018
3. Ambesh SP, Singh N, Gupta D, Singh PK, Singh U. A huffing manoeuvre, immediately before induction of anaesthesia, prevents fentanyl-induced coughing: a prospective, randomized, and controlled study. Br J Anaesth. 2010;104(1):40–43. doi:10.1093/bja/aep333
4. He LX, Yao YT, Shao K, Zhao YY, Ma J. Efficacy of dezocine on preventing opioid-induced cough during general anaesthesia induction: a PRISMA-compliant systematic review and meta-analysis. BMJ Open. 2022;12(4):e052142. doi:10.1136/bmjopen-2021-052142
5. Oliceridine. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2012.
6. Xiong Z, Yi P, Song J, Tan M. Dezocine prevents sufentanil-induced cough during general anesthesia induction: a meta-analysis of randomised controlled trials. BMC Anesthesiol. 2020;20(1):154. doi:10.1186/s12871-020-01076-w
7. Tan W, Li S, Liu X, et al. Prophylactic intravenous lidocaine at different doses for Fentanyl-Induced Cough (FIC): a meta-analysis. Sci Rep. 2018;8(1):9946. doi:10.1038/s41598-018-27457-3
8. Yin F, Zhang T. A small dose of butorphanol prevents sufentanil-induced cough during general anesthesia induction. J Craniofac Surg. 2019;30(8):2499–2501. doi:10.1097/SCS.0000000000005967
9. Phua WT, Teh BT, Jong W, Lee TL, Tweed WA. Tussive effect of a fentanyl bolus. Can J Anaesth. 1991;38(3):330–334. doi:10.1007/BF03007623
10. Bohrer H, Fleischer F, Werning P. Tussive effect of a fentanyl bolus administered through a central venous catheter. Anaesthesia. 1990;45(1):18–21. doi:10.1111/j.1365-2044.1990.tb14496.x
11. Lin CS, Sun WZ, Chan WH, Lin CJ, Yeh HM, Mok MS. Intravenous lidocaine and ephedrine, but not propofol, suppress fentanyl-induced cough. Can J Anaesth. 2004;51(7):654–659. doi:10.1007/BF03018421
12. Gu C, Zhou M, Wu H, Li F, Tang Q. Effects of different priming doses of fentanyl on fentanyl-induced cough: a double-blind, randomized, controlled study. Pharmacol Rep. 2012;64(2):321–325. doi:10.1016/s1734-1140(12)70771-5
13. Sun S, Huang SQ. Effects of pretreatment with a small dose of dexmedetomidine on sufentanil-induced cough during anesthetic induction. J Anesth. 2013;27(1):25–28. doi:10.1007/s00540-012-1470-y
14. Sun ZT, Yang CY, Cui Z, Zhang J, Han XP. Effect of intravenous dezocine on fentanyl-induced cough during general anesthesia induction: a double-blinded, prospective, randomized, controlled trial. J Anesth. 2011;25(6):860–863. doi:10.1007/s00540-011-1237-x
15. Agarwal A, Azim A, Ambesh S, et al. Salbutamol, beclomethasone or sodium chromoglycate suppress coughing induced by iv fentanyl. Can J Anaesth. 2003;50(3):297–300. doi:10.1007/BF03017801
16. Kim JE, Min SK, Chae YJ, Lee YJ, Moon BK, Kim JY. Pharmacological and nonpharmacological prevention of fentanyl-induced cough: a meta-analysis. J Anesth. 2014;28(2):257–266. doi:10.1007/s00540-013-1695-4
17. Wang J, Duan J, Wang Q, Lu Y. Pretreatment with nalbuphine prevents sufentanil-induced cough during the anesthesia induction: a randomized controlled trial. Ther Clin Risk Manag. 2020;16:281–286. doi:10.2147/TCRM.S247437
18. Song C, Huang X, Chen N, Song Q, Qiu Y. A bibliometric and visual analysis of oliceridine research (2013–2024). Drug Des Devel Ther. 2025;19:1305–1321. doi:10.2147/DDDT.S497186
19. Zhang J, Miao S, Tu Q, et al. Effect of butorphanol on opioid-induced cough: a meta-analysis of randomized controlled trials. Drug Des Devel Ther. 2018;12:3263–3268. doi:10.2147/DDDT.S180533
20. Shuying L, Ping L, Juan N, Dong L. Different interventions in preventing opioid-induced cough: a meta-analysis. J Clin Anesth. 2016;34:440–447. doi:10.1016/j.jclinane.2016.05.034
21. Dong Y, Chang X. Comparison of five prophylactically intravenous drugs in preventing opioid-induced cough: a bayesian network meta-analysis of randomized controlled trials. Front Pharmacol. 2021;12:684276. doi:10.3389/fphar.2021.684276
22. Schlimp CJ, Wiedermann FJ. Does fentanyl-induced cough justify pre-treatment with iv lidocaine 2 mg.kg-1. Can J Anaesth. 2005;52(2):207. doi:10.1007/BF03027731
23. Ebert TJ, Hall JE, Barney JA, Uhrich TD, Colinco MD. The effects of increasing plasma concentrations of dexmedetomidine in humans. Anesthesiology. 2000;93(2):382–394. doi:10.1097/00000542-200008000-00016
24. de Souza ATB, de Lima Machado ML, Sarmento ACA, et al. Magnesium sulfate versus nifedipine for tocolysis: meta-analysis of randomized controlled trials. Women Health. 2025;65(1):29–49. doi:10.1080/03630242.2024.2436414
25. Liu XS, Xu GH, Shen QY, et al. Dezocine prevents sufentanil-induced cough during general anesthesia induction: a randomized controlled trial. Pharmacol Rep. 2015;67(1):52–55. doi:10.1016/j.pharep.2014.08.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Comparative Evaluation of the Safety and Efficacy of Oliceridine and Sufentanil in Gastrointestinal Endoscopy: A Single-Center, Randomized Controlled Trial
Ma B, Li Y, Leng C, Ji A, Zhang N, Tao X, Cao Q, Wang S
Drug Design, Development and Therapy 2025, 19:5111-5121
Published Date: 17 June 2025
Effect of Oliceridine Combined with Sufentanil on Patient-Controlled Intravenous Analgesia in Elderly Patients After Laparoscopic Radical Resection of Rectal Cancer: A Prospective Randomized Controlled Study
Tian Y, Hu J, Pan H, Bai G, Zhang Z, Zhang P
Drug Design, Development and Therapy 2025, 19:10033-10043
Published Date: 8 November 2025
Comparison of Postoperative Analgesic Efficacy of Oliceridine and Sufentanil in Total Laparoscopy Hysterectomy, a Clinical Double-Blind Controlled Trial
Duan J, Liu N, Lu Q, Gao W, Hou C, Liu H, Lu Y, Xu S
Drug Design, Development and Therapy 2026, 20:582143
Published Date: 27 February 2026
The Satisfactory Analgesia and Minimal Emesis of Elderly Patients After Thoracoscopic Lung Surgery: Oliceridine versus Sufentanil in a Randomized Controlled Trial
Cai Y, Jiang Y, Zhang Q, Yang J, Wang Z, Sun H
Drug Design, Development and Therapy 2026, 20:593306
Published Date: 7 May 2026
Efficacy and Safety of Oliceridine for Patient-Controlled Intravenous Analgesia in Elderly Patients Undergoing Laparoscopic Radical Resection Surgery for Gastrointestinal Malignant Tumors: A Prospective Randomized Controlled Non-Inferiority Clinical Trial
Wang J, Shang Y, Wang C, Zhang D, Li H, Yu Q, Tao L, Sun L, Gao C
Drug Design, Development and Therapy 2026, 20:593111
Published Date: 8 May 2026