Back to Journals » Clinical Ophthalmology » Volume 16
Effect of Light Conditions and Accommodation on Implantable Phakic Contact Lens Vault by Anterior Segment Optical Coherence Tomography
Authors Mahmoud MSE, AbdelHalim AS, Zein HA
Received 23 January 2022
Accepted for publication 11 April 2022
Published 5 May 2022 Volume 2022:16 Pages 1439—1447
DOI https://doi.org/10.2147/OPTH.S359296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohamed Salah El-Din Mahmoud, Ahmed Shawkat AbdelHalim, Hosny Ahmed Zein
Ophthalmology Department, Faculty of Medicine, Minia University, Minia, Egypt
Correspondence: Mohamed Salah El-Din Mahmoud, Ophthalmology Department, Faculty of Medicine, Minia University, Minia, Egypt, Tel +20 1003321802, Email [email protected]; [email protected]
Purpose: To investigate the dynamic pupil and vault changes in eyes with implantable phakic contact lens (IPCL) under photopic and scotopic settings, as well as during accommodation using the anterior segment optical coherence tomography (AS-OCT).
Methods: A prospective observational study included consecutive 36 eyes of myopic patients who underwent IPCL V2.0 implantation. Under photopic and scotopic light settings, as well as during accommodation, all patients were scanned using CASIA OCT (CASIA2; TOMEY, Nagoya, Japan). The pupil size, the vault (distance between the back surface of the IPCL and the anterior lens capsule), ACD-lens (distance between the posterior corneal surface and the anterior lens surface), IPCL-lens (distance between the posterior corneal surface and the anterior IPCL surface), and lens thickness (LT) were the study parameters.
Results: The vault was significantly lower under photopic conditions (p-value< 0.001). The pupil size was significantly smaller in photopic conditions (p-value< 0.001). LT (p-value=0.975) and ACD-lens (p-value=0.917) were not significantly different between scotopic and photopic conditions, while the ACD-IPCL was significantly larger during photopic conditions (p-value=0.013). There were significant changes in all parameters between accommodative and non-accommodative conditions.
Conclusion: The IPCL vault decreased significantly under photopic light conditions and accommodation.
Keywords: IPCL, photopic light, scotopic light, lens accommodation, vault, AS-OCT
Introduction
The implantable phakic contact lens (IPCL V2.0; Caregroup, Gujarat, India) is a new posterior chamber phakic intraocular lens (pIOL) that can be used to correct refractive problems.1 It was created as a cost-effective alternative to traditional refractive correction instead of an Implantable Collamer Lens (ICL). Furthermore, the maximal myopic correction attainable with ICL is restricted to −18.0 D, while the IPCL is freely available and can correct a wide range of ametropia up to −30.0 D.2
Recently, a new version of the IPCL (IPCL V2.0) with a 380 µm central artificial hole became commercially available. This would eliminate the necessity for a peripheral iridectomy (PI) and reduce the risk of cataracts and pupillary block glaucoma.3
The space between the back surface of the pIOL and the anterior surface of the crystalline lens is known as the central vault. A suitable vault has been recommended to be between 250 and 750 µm. The contact between the pIOL and the anterior lens capsule can cause an anterior subcapsular cataract if the vault is insufficient. Excessive vaulting can result in angle closure, pupillary obstruction, or pigmentary dispersion syndrome, all of which can raise intraocular pressure (IOP) and hence increase the risk of glaucoma. As a result, it’s critical to measure this distance in order to assure the technique’s safety.4,5
Using low-coherence interferometry, anterior segment optical coherence tomography (AS-OCT) obtains cross-sectional pictures of the anterior segment without making contact with the cornea.6 Although previous research has shown that pupil size can influence the vault measures, the dynamic vault alterations associated with dynamic pupil variations in eyes with IPCLs have not been investigated. The current study used AS-OCT to assess dynamic pupil size and vault changes in eyes with IPCL V2.0 in photopic and scotopic situations, as well as in the accommodative and nonaccommodative states.
Patients and Methods
This is a prospective observational study which included a consecutive 36 eyes of myopic patients who underwent IPCL V2.0 implantation in the Ophthalmology department of Minia University Hospital and International Eye Centre, Minia, Egypt, in the period from March 2021 to December 2021 after obtaining written informed consent from every included patient to participate in the study. The study was designed according to the Declaration of Helsinki and was approved by Minia University Ethical Committee.
The inclusion criteria were patients younger than 40 years of age with stable myopia higher than −8.0 D, myopic patients less than −8.0 D, but not candidates for corneal refractive surgery, an endothelial cell count (ECC) greater than 2,500 cells/mm2 (Topcon Corp, Tokyo, Japan), anterior chamber depth (ACD) greater than or equal to 3 mm, estimated from the endothelium to the anterior lenticular surface (Pentacam, HR; Oculus Optikgeräte GmbH, Wetzlar, Germany). IOP less than 21 mmHg by Goldmann applanation tonometer (AT 900; Haag-Streit, Zug, Switzerland) with normal fundus examination except myopic chorioretinal degenerations by Volk 90 D lens (Volk, Mentor, Ohio, USA). Patients younger than 18 years of age and older than 40 years, shallow ACD less than 3 mm and any ocular pathological problem such as glaucoma, chronic uveitis, diabetic retinopathy, or cataract were excluded from the study. Also, patients with chronic systemic diseases such as collagen vascular diseases or diabetes mellitus were excluded.
IPCL V2.0 Design, Power, and Size Calculation
The IPCL V2.0 is a hydrophilic acrylic copolymer single-piece PC pIOL. It can be injected through a 2.8 mm incision. It has a wide range of power from +15.0 to −30.0 D with astigmatic correction up to 10.0 D. It has six haptic, it has a central opening of about 380 μm designed to decrease light scattering and glare and to facilitate aqueous humor circulation to eliminate the need for PI. The data needed for power calculation were refraction, keratometric readings, pachymetry, and ACD which were measured by Pentacam. The size of the IPCL was selected according to the ACD and horizontal white to white (WTW) using IOL Master (Carl Zeiss Meditec, Jena, Germany).
AS-OCT Technique
All patients were examined 1 month or more after surgery (not before 1 month), to confirm stability of refraction and topical steroid withdrawal. All patients had no or postoperative complications.
After entering patient’s data and accurate patient poisoning on the AS-OCT instrument, one eye from each patient was examined with CASIA OCT (CASIA2; TOMEY, Nagoya, Japan) under different lighting conditions 1 month or more after the operation. Scans were obtained in the horizontal meridian and each scan was measured twice with the aid of the Light Intensity Meter (Pro’skit MT-4617, China) to measure the light intensity of the room. The measurements were taken after 5 minutes of the light on and off to give a chance for the adaptation to occur.
The Scotopic Measurement (0.5 LUX)
The lights of the patient room were turned off with light only coming from the OCT screen while the measurement was performed.
The Photopic Measurement (1,500 LUX)
After turning the lights of the patient room on, the light reflex (5 seconds from a distance of 15 cm) was induced by shining a penlight into the contralateral eye to induce miosis in the examined eye due to the consensual reflex.
The Accommodative Measurement
In dim illumination, the patients fixated on an accommodative target image in the OCT device internal target while looking through a 0.00-diopter (D) lens for the first 5 seconds and a −5.00 D lens (stimulate the physiologic accommodation) for the next 5 seconds. The patients were asked to specifically focus on the internal fixation target to achieve an accommodative state.
The study parameters were the pupil size, the vault (the distance between the back surface of the IPCL and the anterior lens capsule), anterior chamber depth (ACD)-lens (the distance between the posterior corneal surface and the anterior lens surface), IPCL-lens (the distance between the posterior corneal surface and the anterior IPCL surface), and the lens thickness (LT). All measurements were expressed in millimeters, except the vault, which was in micrometers.
Methods of Statistical Analysis
Data were collected, revised, verified, coded, then entered into a PC for statistical analysis done by using IBM SPSS (Chicago, IL) statistical package version 20. Mean and standard deviation (SD) were used for quantitative data. The Independent sample t-test was used for comparison of the quantitative data. For all tests, probability (p) was considered non-significant if ≥0.05 and significant if <0.05.
Results
Patient’s Data
Our study included 36 myopic eyes of 20 males and 16 females with a range of age from 19–37 years. Ten patients had bilateral surgery while 16 patients had unilateral IPCL implantation (nine right eye and seven left eye). The preoperative data, including the spherical error (SPH), cylindrical error (CYL), uncorrected distance visual acuity (UCDVA), and best corrected distance visual acuity (BCDVA) are expressed in Table 1.
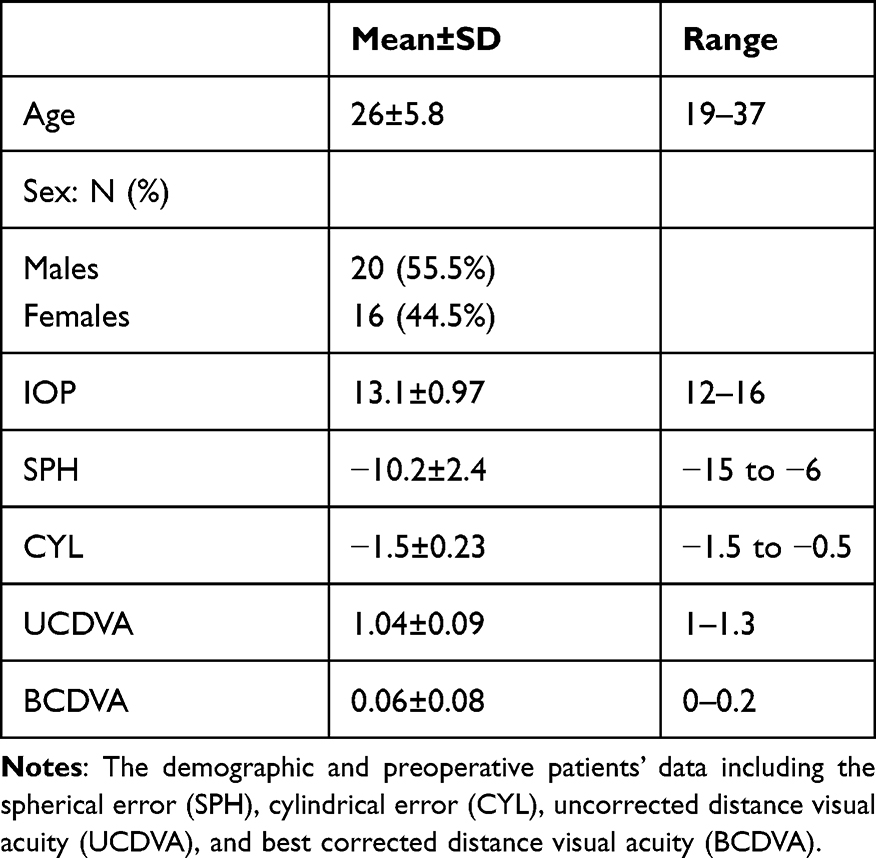 |
Table 1 The Demographic and Preoperative Data |
The Scotopic and Photopic Measurements
The vault was significantly lower under photopic conditions (p-value<0.001). The pupil size was significantly smaller in photopic conditions (p-value<0.001). LT (p-value=0.975) and ACD-lens (p-value=0.917) were not significantly different between scotopic and photopic conditions, while the ACD-I PCL was significantly larger during photopic conditions (p-value=0.013) (Table 2 and Figure 1).
 |
Table 2 The Scotopic and Photopic Measurements |
 |
Figure 1 The difference between the scotopic and photopic conditions in the ACD-lens, ACD-IPCL, LT, pupil size (A) and the vault (B). |
The Accommodative Condition
There were significant changes in all parameters between accommodative and non-accommodative conditions (Table 3 and Figure 2).
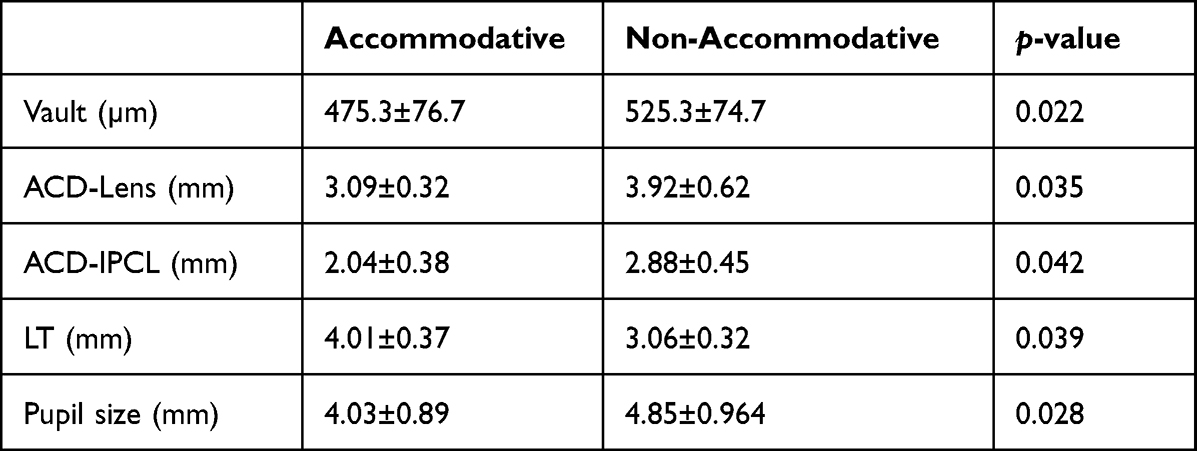 |
Table 3 The Accommodative and Non-Accommodative Conditions |
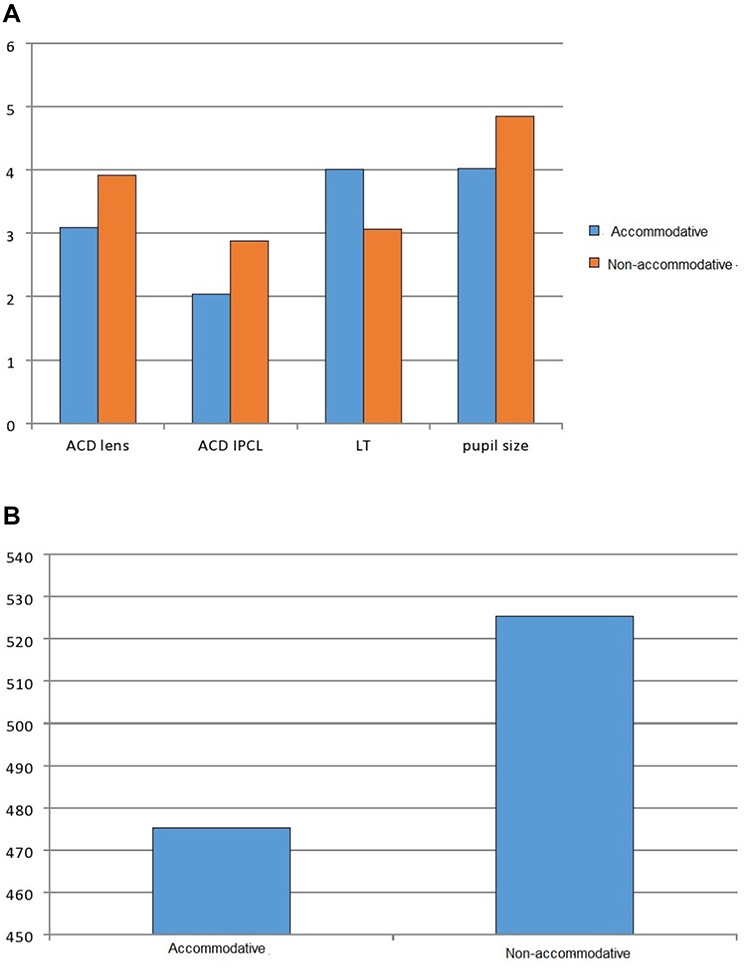 |
Figure 2 The differences between the accommodative and non-accommodative conditions in the ACD-lens, ACD-IPCL, LT, pupil size (A) and the vault (B). |
Discussion
The pIOL are a well-established alternative in myopic patients who are not fit for corneal refractive surgery. The most commonly used lenses are the ICL and IPCL. IPCL is a good alternative to ICL due to the economic burden of ICL (nearly twice IPCL). Cataract and glaucoma are the main postoperative complications, so the sizing of the lens was a very important issue that depends on WTW and ACD to avoid postoperative complications.7
The IPCL vault was defined as the distance between the back surface of the IPCL and the anterior lens capsule. The low vault had the risk of cataract formation, the high vault had the risk of glaucoma. So a suitable vault is necessary to avoid these complications and it is important to measure this distance to ensure the safety after IPCL implantation. The vault could be assessed by many instruments such as high-frequency ultrasound biomicroscopy, Scheimpflug imaging instrument, and AS-OCT. Also, it could be measured clinically by the slit-lamp at 0.5–1.5-times the corneal thickness (CT, 250–750 μm), but the vault is not static and affected by the pupillary size and lens condition.8,9
Accommodation has an effect on anterior segment parameters in normal subjects without IPCL implantation, according to a study by Mitsukawa et al,10 who used swept-source AS-OCT to analyze changes in the crystalline lens during accommodation and found that the ACD, anterior, and posterior curvature of the lens decreased, and LT increased significantly during 5.0 D accommodative stimulation.
Thirty-six myopic eyes were included in our study implanted with IPCL V2.0. We selected cases with no intraoperative or postoperative complications and AS-OCT was done 1 month or more after IPCL implantation to confirm stability of refraction and withdrawal of topical steroid. Our aim was to evaluate the dynamic vault changes with changes in the pupillary size under different light and lens conditions as the vault was not static to assess long-term safety of the IPCL, for example, driving a car at night (scotopic) and suddenly another car shining the light (photopic) and watching TV with light of the room off (scotopic) and suddenly the room light turned on (photopic). Also, the vault changes with accommodation as during reading. The scotopic and photopic light conditions were assessed with the aid of Light Intensity Meter for better estimation of the light intensity. Our results showed significant changes in the vault, pupillary size, and ACD-IPCL with no significant difference in the LT and ACD-lens, this indicated the safety of examination of patients with IPCL with OCT. Regarding the accommodation, there were significant changes in all study parameters with no complications.
While reviewing the literature, we found a study by Bianchi et al,11 which was a prospective case-series study performed on 44 eyes (22 patients) operated with IPCL V2.0 under three different lighting conditions (mesopic/scotopic/photopic). The central vault was measured with an OCT. The results obtained 1 and 2 years after surgery were compared, and the differences between the scotopic and the photopic conditions were evaluated and it was shown that the vault difference observed between the scotopic and the photopic conditions was 98.4±48.4 µm (p-value=0.001). Our results about the vault agreed with this study, but our study did not include the mesopic light condition and we included the accommodation.
The effect of varied light situations and accommodation was investigated with ICL and summarized in Table 4.
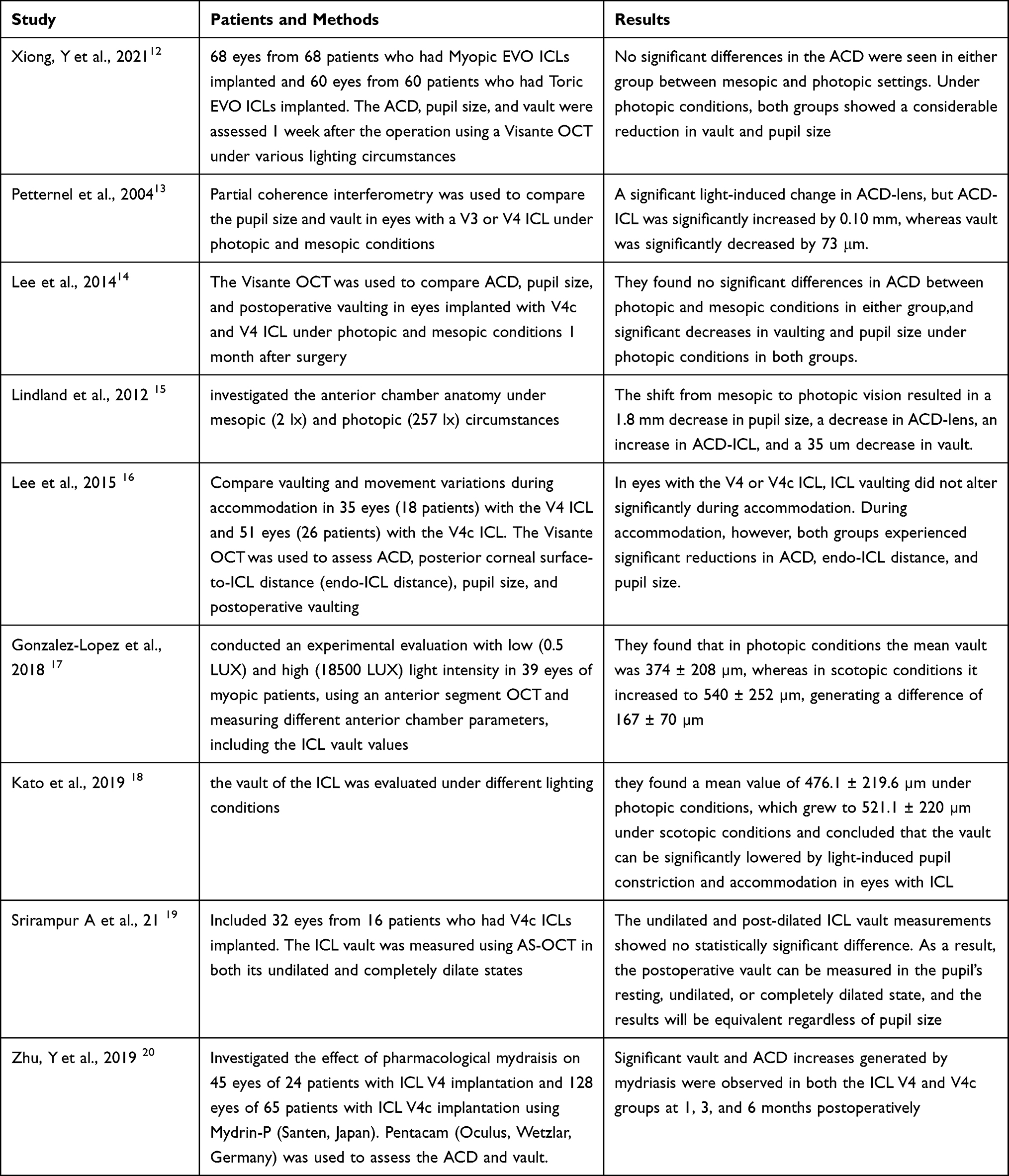 |
Table 4 Table Summarizing the Reported Literature on ICL |
Our study concluded that the AS-OCT was a valuable tool for evaluation of dynamic IPCL vault under photopic and scotopic light conditions and accommodation which showed that the vault had significant changes with frequent changes in the pupil size and accommodation as during daily activities such as the reading and watching TV in dim illumination. So it is better to examine the dynamic vault not the static one.
The limitations of our study were the small number of patients and we did not examine patients with variable postoperative periods. Also, not all light conditions and accommodations power were examined.
Human and Animal Rights
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
Data Sharing Statement
The raw data (Excel sheet) that support the findings of this study are available upon request from the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board and Research Ethics Committee of Minia University, Egypt under approval no. (134-2021). All patients signed their written informed consent to participate.
Acknowledgment
All authors contributed equally to this work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest for this work, financial or otherwise.
References
1. Elkareem AM, Nooreldin A. Visual and safety outcomes of a new implantable phakic contact lens in patients with a high degree of myopia. Delta J Ophthalmol. 2021;22:192–200. doi:10.4103/djo.djo_4_21
2. Sachdev G, Ramamurthy D. Long-term safety of posterior chamber implantable phakic contact lens for the correction of myopia. Clin Ophthalmol. 2019;13:137–142. doi:10.2147/OPTH.S185304
3. Bianchi GR. Initial results from a new model of posterior chamber implantable phakic contact lens: IPCL V2.0. Med Hypothesis Discov Innov Ophthalmol. 2019;8:57–63.
4. Nongpiur ME, He M, Amerasinghe N, et al. Lens vault, thickness, and position in Chinese subjects with angle closure. Ophthalmology. 2011;118(3):474–479. doi:10.1016/j.ophtha.2010.07.025
5. Almalki S, Abubaker A, Alsabaani NA, et al. Causes of elevated intraocular pressure following implantation of phakic intraocular lenses for myopia. Int Ophthalmol. 2016;36:259–265. doi:10.1007/s10792-015-0112-4
6. Wang Q, Ding X, Savini G, Wang Q, Ding X, Savini Get al. Anterior chamber depth measurements using Scheimpflug imaging and optical coherence tomography: repeatability, reproducibility, and agreement. J Cataract Refract Surg. 2015;41(1):178–185. doi:10.1016/j.jcrs.2014.04.038
7. Deshpande K, Shroff R, Biswas P, et al. Phakic intraocular lens: getting the right size. Indian J Ophthalmol. 2020;68(12):2880–2887. doi:10.4103/ijo.IJO_2326_20
8. Zhang X, Chen X, Wang X, et al. Analysis of intraocular positions of posterior implantable collamer lens by full-scale ultrasound biomicroscopy. BMC Ophthalmol. 2018;18:114. doi:10.1186/s12886-018-0783-5
9. Nakamura T, Isogai N, Kojima T, et al. Implantable collamer lens sizing method based on swept-source anterior segment optical coherence tomography. Am J Ophthalmol. 2018;187:99–107. doi:10.1016/j.ajo.2017.12.015
10. Mitsukawa T, Suzuki Y, Momota Y, et al. Anterior segment biometry during accommodation and effects of cycloplegics by swept-source optical coherence tomography. Clin Ophthalmol. 2020;14:1237–1243. doi:10.2147/OPTH.S252474
11. Bianchi GR, Campo DI, González AB. Preliminary results of a IPCL phakic lens vault pilot study under different lighting conditions. Oftalmol Clin Exp. 2021;14(1):e1–e13.
12. Xiong Y, Mao Y, Li J, et al. Vault changes and pupillary responses to light in myopic and toric implantable collamer lens. BMC Ophthalmol. 2021;21(1):366. doi:10.1186/s12886-021-02119-7
13. Petternel V, Köppl CM, Dejaco-Ruhswurm I, et al. Effect of accommodation and pupil size on the movement of a posterior chamber lens in the phakic eye. Ophthalmology. 2004;111(2):325–331. doi:10.1016/j.ophtha.2003.05.013
14. Lee H, Kang SY, Seo KY, et al. Dynamic vaulting changes in V4c versus V4 posterior chamber phakic lenses under differing lighting conditions. Am J Ophthalmol. 2014;158(6):1199–1204.e1. doi:10.1016/j.ajo.2014.08.020
15. Lindland A, Heger H, Kugelberg M, et al. Changes in vaulting of myopic and toric implantable collamer lenses in different lighting conditions. Acta Ophthalmol. 2012;90(8):788–791. doi:10.1111/j.1755-3768.2011.02224.x
16. Lee H, Kang DS, Ha BJ, et al. Effect of accommodation on vaulting and movement of posterior chamber phakic lenses in eyes with implantable collamer lenses. Am J Ophthalmol. 2015;160(4):710–6.e1. doi:10.1016/j.ajo.2015.07.014
17. Gonzalez-Lopez F, Mompean B, Bilbao-Calabuig R, et al. Dynamic assessment of light-induced vaulting changes of implantable collamer lens with central port by swept-source OCT: pilot study. Transl Vis Sci Technol. 2018;7(3):4. doi:10.1167/tvst.7.3.4
18. Kato S, Shimizu K, Igarashi A. Vault changes caused by light-induced pupil constriction and accommodation in eyes with an implantable collamer lens. Cornea. 2019;38:217–220. doi:10.1097/ICO.0000000000001785
19. Srirampur A, Pesala V, Mansoori T, et al. Effect of pupil size on posterior chamber phakic intraocular lens vault measurements. Indian J Ophthalmol. 2021;69(9):2289–2292. doi:10.4103/ijo.IJO_3429_20
20. Zhu Y, Zhang J, Zhu H, et al. The effect of mydriasis on moderate-to-high myopic eyes with implantable collamer lenses V4 and V4c. Eur J Ophthalmol. 2019;1120672119831218.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.