Back to Journals » International Journal of Women's Health » Volume 14
Effect of Intimate Partner Violence on Birth Preparedness and Complication Readiness at Public Health Facilities, Southwest Ethiopia, 2021: Comparative Cross-Sectional Study
Authors Genetu Ejigu A ![]() , Girma Tilahun A, Tilahun Wassie S
, Girma Tilahun A, Tilahun Wassie S ![]() , Hailemariam Lambyo S
, Hailemariam Lambyo S
Received 15 February 2022
Accepted for publication 12 May 2022
Published 20 May 2022 Volume 2022:14 Pages 705—718
DOI https://doi.org/10.2147/IJWH.S361796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Amare Genetu Ejigu,1 Abel Girma Tilahun,2 Semahegn Tilahun Wassie,1 Shewangizaw Hailemariam Lambyo2
1Department of Midwifery, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia; 2Department of Reproductive Health and Nutrition, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia
Correspondence: Amare Genetu Ejigu; Semahegn Tilahun Wassie, Email [email protected]; [email protected]
Introduction: Birth preparedness and complication readiness (BPCR) strategy is a key to reducing delays of appropriate care for maternal and child health. Women’s autonomy in the decision of receiving care during pregnancy is essential for improvements in maternal health. However, there is a scarcity of information on the effect of intimate partner violence (IPV) on BPCR in Southwest Ethiopia.
Methods: A comparative cross-sectional study was conducted among 688 women (340: women who had experienced IPV and 348: women who had not experienced IPV). A multi-stage sampling technique was used to select study participants. Bivariate and multivariable logistic regression models were done. A P-value < 0.05 at a 95% confidence interval was used to declare a statistical significance.
Results: BPCR among IPV women was 30.59%, lower compared with 46.84% women who did not experience IPV. Higher education [AOR=4.00 (1.20, 13.28)], partner did not drink alcohol [AOR=2.53 (1.34, 4.78)], no childhood violence [AOR=2.70 (1.37, 5.32)], partner’s pregnancy desire [AOR=3.61 (1.41, 9.21)], and good knowledge of BPCR [AOR=8.59 (3.56, 20.70)] were more likely to practice BPCR among women who experienced IPV, whereas among women who did not experience IPV, no previous pregnancy complications [AOR=2.22 (1.08, 4.55)], good knowledge of BPCR [AOR=4.90 (2.59, 9.26)] and pregnancy danger signs [AOR=5.23 (1.47, 18.56)] were more likely practice BPCR.
Conclusion: BPCR among IPV women was lower compared with women who did not experience IPV. Likewise, women’s knowledge of BPCR, obstetric danger signs during pregnancy, labor, and postpartum were lower among women who faced IPV. Therefore, minimizing women’s IPV help to improve BPCR.
Keywords: birth preparedness, complication readiness, intimate partner violence, Ethiopia
Introduction
BPCR is recognized as a key component of safe motherhood programs that play a great role in reducing maternal mortality. BPCR is a comprehensive package to promote timely access to skilled maternal and neonatal health services. It also promotes active preparation and decision-making for birth among pregnant women and their families.1
Though skill-attendance is the most important intervention to prevent life-threatening complications, most sub-Saharan African women still give birth at home in the absence of skilled birth attendants.2 Studies were conducted in Ethiopia, nearly two-thirds of women received antenatal care (ANC) services, half of the pregnant women gave birth at a health institution, and one in every three women received postnatal care service, respectively.3–5
Poor access to and low utilization of key interventions due to different socio-cultural and economic factors are still major obstacles to optimum maternal health.3,6,7 Domestic violence against women, and men’s controlling behaviors in intimate relationships are factors that influence women’s ability to make decisions concerning their health, pregnancy, and health service care utilization.8
Intimate partner violence (IPV) of women is a violation of human rights and major public health concerns of women.9,10 Domestic violence against women has a complex structure in its occurrence, which can relate to different factors at individual, family, community and societal level.11 Globally, nearly one-third of all women have faced IPV or non-partner sexual violence.9 A meta-analysis study was conducted in Africa reveals the prevalence of IPV during pregnancy is 15.23%.12 In Ethiopia, the lifetime risk of IPV ranged from 20 to 78%.,13,14 and women who have experienced IPV during the pregnancy period are 40.8% and 41.1%, respectively.14,15 IPV should be given special concern during pregnancy when not one, but two lives are at risk.16 Studies indicate that IPV during pregnancy contributes to miscarriage, premature labour, low birth weight, postnatal depressive symptoms, and not breastfeeding at birth.10,16,17
In 2016, Sustainable Development Goals developed an agenda to eliminate all forms of violence against all women and girls in public and private spheres.18 Currently, WHO recommends screening IPV at ANC visits when assessing conditions that may be caused or complicated by IPV.19 Recognizing the opportunity that ANC provides for early identification and prevention of the recurrence of such violence.10 Although the Government of Ethiopia, incorporated and coordinated with other stakeholders, made concerted efforts to achieve millennium development goals still promote gender equality and empower women and improve maternal health were not successfully achieved.20
Therefore, this study aimed to assess the effect of IPV of women on BPCR by comparing women who had IPV and women who had not IPV during recent pregnancy of Benchi-Sheko zone, southwest Ethiopia.
Method
Study Setting
The study was conducted at public health facilities in a bench-sheko zone from Feb 1, to July 30, 2021. In this zone, there are 7 districts and 1 city administration as well as 26 health centers and 1 teaching Hospital. All public health facilities provide maternal and child care services. Based on the 2017 population forecasting, a total of 826,611 population, among them, 418,916 were females who lived in the Benchi-Sheko zone.21 An institutional-based comparative cross-sectional study was conducted among women who gave birth in the last 12 months and visited the public health facilities regardless of the birth outcome.
Sample Size Determination
The minimum sample size for each group was calculated using the formula of two-sample comparisons of proportion by using Epi-Info V.7 StatCalc, cohort or cross-sectional, based on the following assumptions: confidence level 95%, power 80, and the proportion of women prepared for BPCR and experienced IPV was assumed to be 50% due to the absence of a previous study based on which the proportion could be assumed. The proportion of prepared for BPCR in Farta district, in South Gondar Zone, Ethiopia: 34%22 (ie, a proportion difference of 16%; this was just an assumption as there was no previous study based on which this difference could be estimated). Adding of 10% non-response rate and a design effect of 2; the final minimum sample size calculated for both groups was 716.
Sampling Techniques
In our study, a multi-stage sampling technique was used to recruit 358 study participants from each group. Three districts and a city administration were selected randomly using lottery methods (considering at least 50% of districts in the zone). All public health facilities (13 health centers and 1 teaching Hospital) in selected districts were included in this study. First, a woman who gave birth within 12 months and visited health facilities was screened with a standard tool of IPV. Based on screening, two study populations (women who had an experience of IPV and women who had not experienced IPV) were created. The IPV screening was conducted in a private room, one-on-one, and in the absence of a third body. Then, women in both groups were assessed for the practice of BPCR. A systematic random sampling technique was used to select study participants in each health facility. The number of women who visited the health facilities was obtained by reviewing the post-partum register in each health facility before the actual data collection. A sampling (K) interval was calculated using the summation of 6 months of women who visited health facilities within 12 months of delivery, which were 2972. K=N/n, 2972/716=4.15≈4. Every 4th study participant was interviewed. The first interview started after 2 were selected from 1 to 4 by lottery method.
Operational Definition
IPV is physical violence, sexual violence, and psychological aggression by a current or former partner.23 If the respondent says “Yes” to any one of the ranges of sexually, psychologically, and physically or any combination of the three coercive acts used against adult and adolescent women, regardless of the legal status of the relationship with current/former intimate partner, it was considered as IPV.24
BPCR contains the following components; identifying a place of delivery, saving money, preparing essential items for childbirth, identifying a skilled provider, identifying a mode of transportation, arranging blood donors, arranging a way for communication, designating decision-maker on her behalf, identifying emergency funds, being aware of the obstetric danger signs and the need to act immediately.25
BPCR Practice: When a woman applied/implemented at least 6 items among 12 constituents of BPCR.
Knowledgeable for BPCR: When a woman mentioned a minimum of 6 items among 12 constituents of BPCR.
Knowledgeable for danger signs of pregnancy: When she mentioned a minimum of 3 among 6 components of key danger signs of pregnancy.
Knowledgeable for danger signs of labor and delivery: When she mentioned a minimum of 3 among 6 components of key danger signs of labor and delivery.
Knowledgeable for danger signs of postpartum: When she mentioned a minimum of 3 among 6 components of key danger signs of postpartum.
Data Collection Procedure and Quality Assurance
Validated tool, based on the standard of WHO (2005) Multicounty consider on women’s health and domestic violence against women were used to gather information related to IPV24 and the questionnaire for BPCR was taken from safe motherhood questionnaires developed by maternal and neonatal health programs of JHPIEGO.25 Data were collected by using a pre-tested and structured questionnaire (Supplementary Material). The interviewer administer a face-to-face interview was used to collect the data. To assure the quality of the data, technical training was given before data collection for data collectors, supervisors and also pre-testing was conducted on 10% (72) of a sample size to pilot test the survey tool on health facilities outside the actual data collection site that have similar characteristics to the study population. Data collection was done by 14 trained BSc. midwives and supervised by 5 MSc. Throughout the data collection period, the supervisor monitored the way of data collection and checked each filled questionnaire for its completeness. Finally, the data were cleaned after entry to ensure completeness.
Data Processing and Analysis
Data were checked, coded, and entered into Epi-data version 3.1 and exported to SPSS (Statistical Package for Social Science) version 22 for analysis. In descriptive statistics tables, graphs and chart was used to present the information. An independent variable that had a p-value <0.2 in the bivariate analysis was taken to multivariable logistic regression models for controlling confounding effects. An adjusted odds ratio (AOR) with a 95% confidence interval (CI) was used to identify factors associated with BPCR. A P-value less than 0.05 in multivariable logistic regression was set to consider a statistical significance.
Result
Socio-Demographic Characteristics of Respondents
In this study, 340 women with IPV experience and 348 women with no IPV experience were included in the analysis, and this made the response rate 95% and 97.2%, respectively. One hundred sixty-nine (49.7%) of women with IPV experience (50%) women with no IPV experience were in the age group of 25–34 with mean age 27.38±5.86 and 26.23±5.67, respectively. One hundred fifty-two (44.7%) IPV and two hundred thirty-eight (68.4%) women with no IPV experience lived in urban. Almost all (92.4%) IPV and (92%) women with no IPV experience married. Nearly one-fifth (20.3%) of IPV and one-third (35.6%) of women with no IPV experience were attended secondary and above levels of education. Approximately one-third (31.2%) of IPV and more than half (56%) women with no IPV experience were living within 30 minutes of walking from the nearest health facilities. Almost all (93.5%) IPV and (96.3%) women with no IPV experience were currently living with their partners (Table 1).
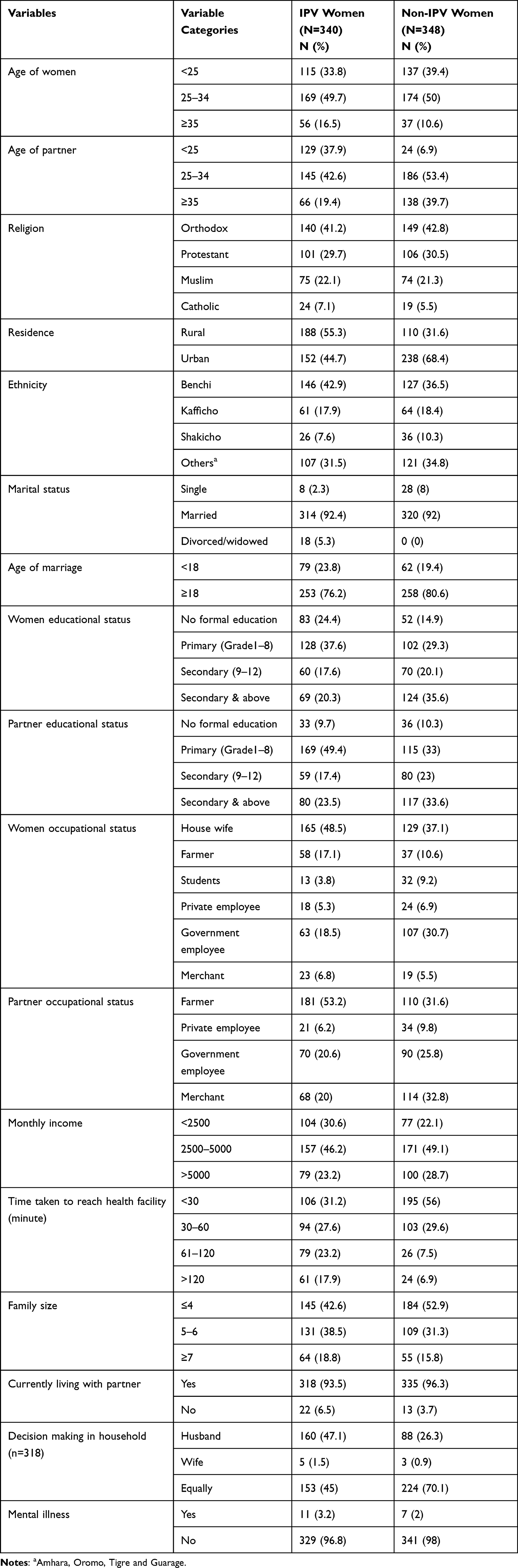 |
Table 1 Socio-Demographic Characteristics of Women Who Gave Birth in the Past One Year, in the Context of Exposure Status to IPV in Benchi-Sheko, Southwest Ethiopia, 2021 |
In this study, nearly half (47.9%) women with IPV experience and one every four (24.4%) women with no IPV experience partners drink alcohol. Seventy-seven (22.6%) women with IPV experience and 56 (16.1%) women with no IPV experience partners chew-chat. Forty (11.8%) women with IPV experience and 12 (3.4%) women with no IPV experience partners smoke a cigarette. Ninety-two (27.1%) women with IPV experience and 49 (14.1%) women with no IPV experience mothers hit by father during childhood. One hundred twenty-five (36.8%) of women with IPV experience and 59 (17%) of women with no IPV experience faced childhood violence (Table 2).
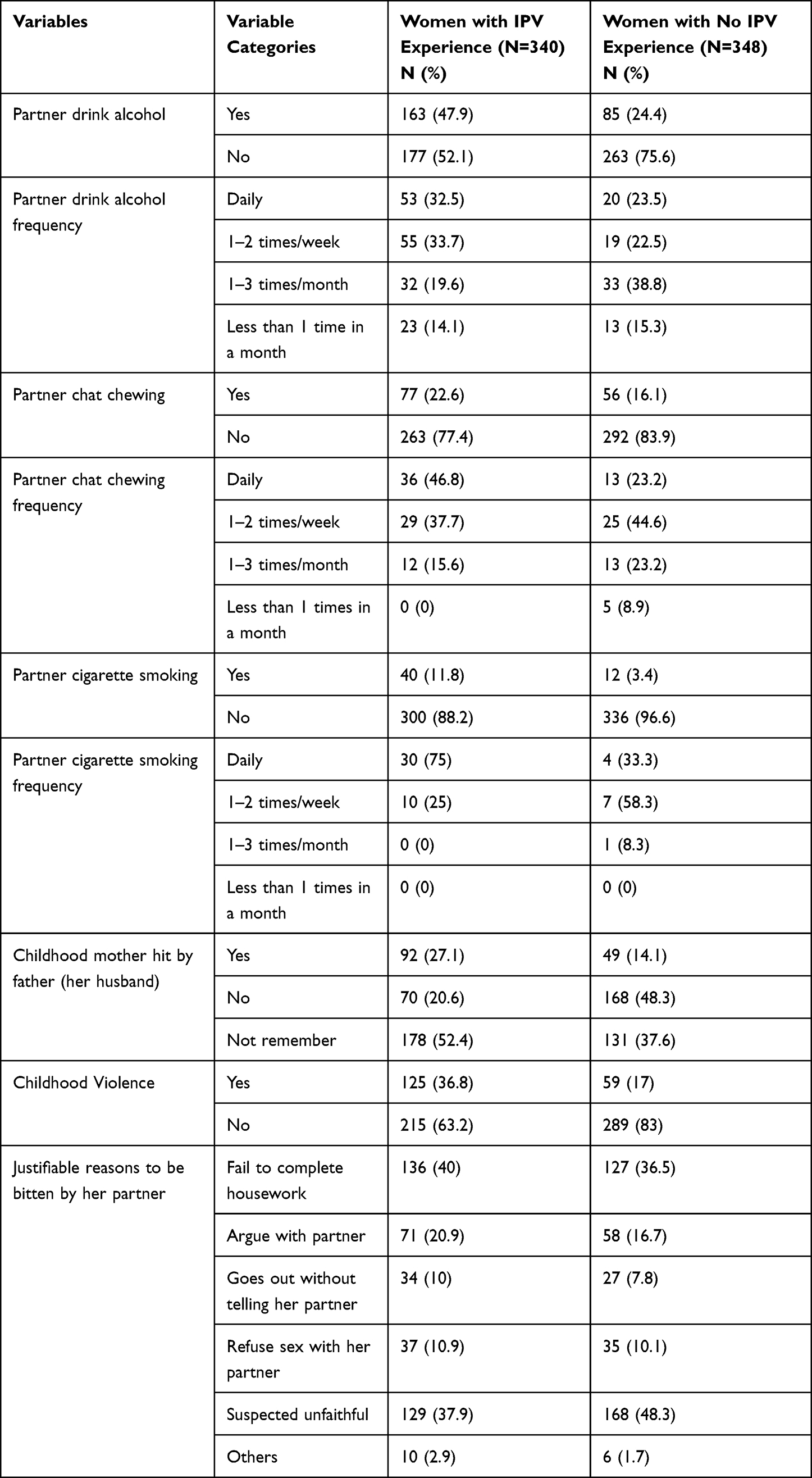 |
Table 2 Substance Experience of Partner and Childhood Violence, in the Context of IPV Exposure Status, in Benchi-Sheko, Southwest Ethiopia, 2021 |
Obstetric Characteristics
Two hundred eighty-nine (85%) women with IPV experience and 307 (88.2%) women with no IPV experience became pregnant for the first time at the age of ≥18 years old. One in every four (24.7%) women with IPV experience and one in every three (31.9%) women with no IPV experience gave birth to their first child. Concerning to desire for pregnancy, 278 (81.8%) women with IPV experience and 328 (94.3%) women with no IPV experience partners had the desire for the recent pregnancy. One hundred ninety-nine (59.2%) women with IPV experience and 257 (76.5%) women with no IPV experience had 4 and more ANC follow-up visits (Table 3).
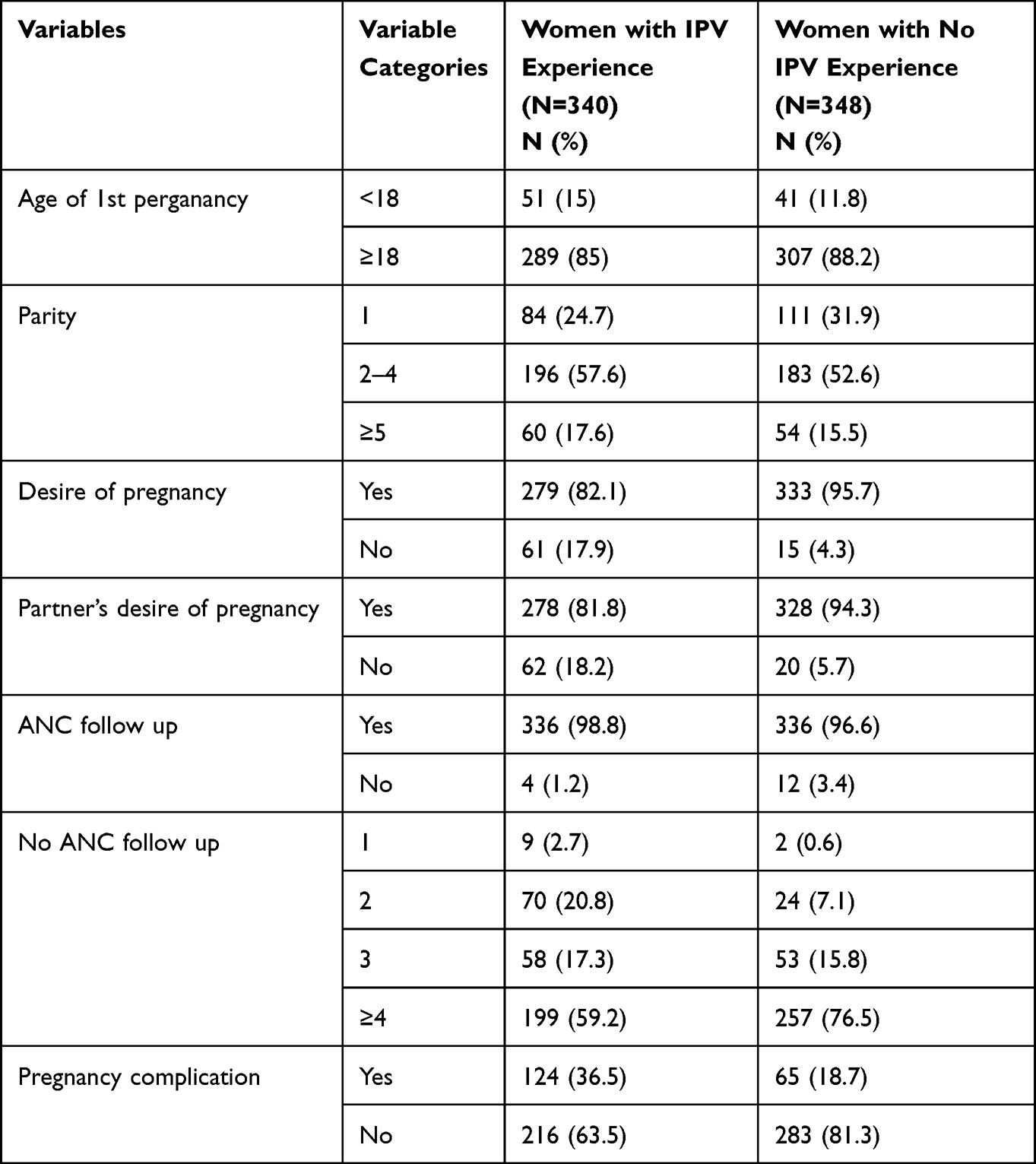 |
Table 3 Obstetric Characteristics of Women Who Gave Birth in the Past One Year; in the Context of Exposure Status to IPV, in Benchi-Sheko, Southwest Ethiopia, 2021 |
Knowledge of Respondents About BPCR and Key Obstetric Danger Signs
Nearly two-thirds (64.12%) of women with IPV experience and three-fourths (76.73%) of women with no IPV experience were knowledgeable for BPCR. The majority of (54.42%) women with IPV experience and nearly three-fourths (74.43%) women with no IPV experience were knowledgeable of danger signs that occurred during pregnancy. The majority of (58.2%) women with IPV experience and nearly three-fourths (76.44%) women with no IPV experience were knowledgeable of danger signs that occurred during labor and delivery. The majority of (55.89%) women with IPV experience and seven of 10 (70.12%) women with no IPV experience were knowledgeable for danger signs that occurred during the post-partum period (Figure 1).
 |
Figure 1 Distribution of knowledge on BPCR, danger sign of pregnancy, labor and delivery and postpartum in the context of IPV of women, Benchi-sheko, Southwest, Ethiopia, 2021. |
The Practice of BPCR
Nearly, three out ten (30.59%) women with IPV experience and nearly half (46.84%) of women with no IPV experience have practiced BPCR (Figure 2).
 |
Figure 2 Distribution of BPCR practice in the context of IPV of women in Benchi-Sheko, Southwest, Ethiopia, 2021. |
Factors Associated with BPCR
Bivariable and multivariable logistic regression analyses were done to assess the effect of IPV on BPCR. In bivariable analyses, age of women, residence, level of education, income, time taken to reach health facility, partner drinks alcohol, partner smoke cigarette, childhood violence, parity, previous pregnancy complication, pregnancy desire, partner’s desire of pregnancy, knowledge of BPCR, pregnancy, labor delivery and postpartum knowledge of danger sign were significantly associated with BPCR in both group.
Level of education, the partner who drinks alcohol, childhood violence, partner’s desire of pregnancy, and BPCR knowledge were significantly associated with BPCR among women who faced IPV. Whereas, among women who did not face IPV previous pregnancy complications, BPCR knowledge and pregnancy danger sign knowledge were significantly associated with BPCR. The odds of educated women whose level of education secondary (9–12) and secondary and above were 3.2 and 4 times more likely to implement BPCR compared to no formal education [AOR=3.28 (1.02, 10.45)] and [AOR=4.00 (1.20, 13.28)], respectively. Women whose partners did not drink alcohol were 2.5 times as likely to implement BPCR compared to women whose partners drink alcohol [AOR=2.53 (1.34, 4.78)]. The odds of women who did not face childhood violence were 2.7 times more likely to practiced BPCR compared to women who faced childhood violence [AOR=2.70 (1.37, 5.32)]. Women whose partners had a desire of pregnancy were 3.6 times as likely to implement BPCR compared to women whose partners did not have a desire of pregnancy [AOR=3.61 (1.41, 9.21)]. The odds of women who had good knowledge of BPCR were 8.5 more likely to implement BPCR compared to women who did not have good knowledge of BPCR [AOR=8.59 (3.56, 20.70)] (Table 4). Women who did not face previous pregnancy complications were 2.2 times as likely to implement BPCR as compared to women who faced previous pregnancy complication [AOR=2.22 (1.08, 4.55)]. The odds of women who had good knowledge of BPCR were 4.9 times more likely to implement BPCR as compared to women who had no good knowledge of BPCR [AOR=4.90 (2.59, 9.26)]. The odds of women who had good knowledge on pregnancy danger signs had 5.2 times more likely to practice BPCR as compared to women who did not have good knowledge on pregnancy danger signs. [AOR=5.23 (1.47, 18.56)] (Table 4).
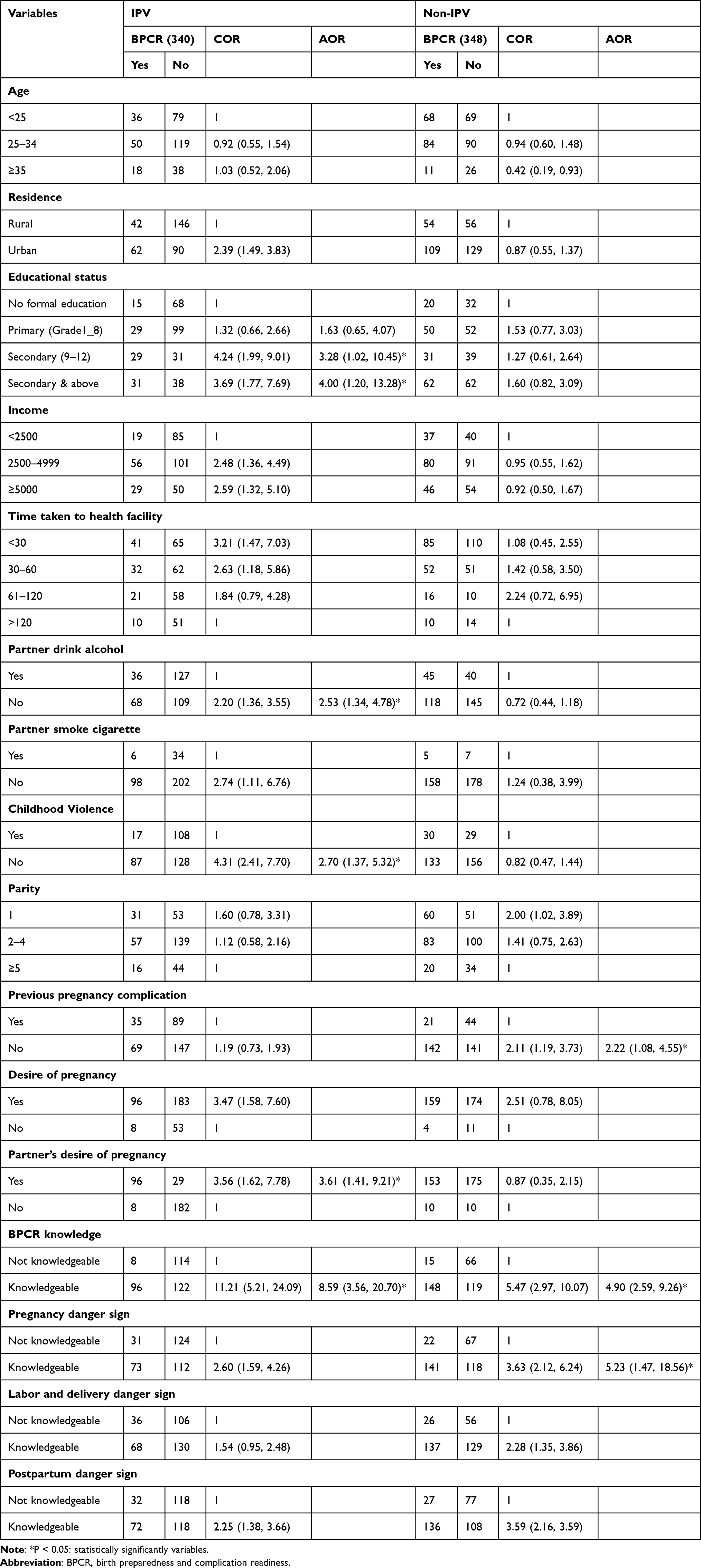 |
Table 4 Factors Affecting Birth Preparedness and Complication Readiness, in the Context of Exposure Status to IPV in Benchi-Sheko, Southwest Ethiopia, 2021 |
Discussion
Assessment of the effect of IPV on BPCR is essential to improve maternal and child health. Currently, the study showed that the involvement of men was a significant determinant of BPCR practice,26, and empowering the women improves maternal health service utilization.27
According to this study, the proportion of BPCR among women with IPV experience was 30.59% lower compared with 46.84% of women with no IPV experience. This finding is supported by a study done in Nepal, in which women who experienced domestic violence had a lower chance of preparing for birth (35.5% vs 54.2%).28 This might be due to; women who experienced IPV had a lower chance of receiving adequate ANC service, which leads to a lower chance to prepare for birth and its complication.29
The odds of BPCR implementation among women with IPV experience who had secondary and college/university levels of education were higher as compared to the primary level of education. This finding is in line with studies done in Ethiopia, Nepal, Tanzania, and Thailand in which a lower level of education was associated with poor BPCR.22,28,30,31 This might be due to women who had a higher level of education being more likely to prepare for birth and its complication readiness.22,32 This could also be due to, the level of maternal education having a positive association with maternal health care service utilization (ANC visit and skill birth attendant).33 Utilization of ANC is one of the determinants for maternal BPCR.22,34
Women with IPV experience whose partners did not drink alcohol were more likely to implement BPCR as compared to women whose partners drink alcohol. This might happen due to women whose partners drink alcohol more frequently being at risk of IPV.15,35 IPV results in a lower chance of receiving adequate ANC service,29,36 which leads to a lower chance of preparing for birth and its complication.22
The odds of BPCR were lower among women with IPV experience who faced childhood violence compared to women who did not face childhood violence. This might be due to the continuous nature of violence from childhood to adulthood.37,38 IPV affects pregnant women’s chance of receiving adequate ANC service,29,36 which leads to a lower chance of preparing for BPCR.22
Women with IPV experience whose partners had a desire for pregnancy were more likely to implement BPCR as compared to their counterparts. This could be due to wanted pregnancy being related to being more likely to receive ANC.39,40 This might also be due to male partner involvement in ANC had improved maternal health services utilization41 as well as women whose partners participated in counseling on BPCR during ANC improves women’s preparation for BPCR.42
In both groups, the odds of women who had good knowledge of BPCR were more likely to implement BPCR as compared to their counterparts. This is similar to the study done in Ethiopia, women’s knowledge of BPCR had a positive association with the practice of BPCR.22 The possible reason might be that women who know the importance of BPCR have more chances to implement BPCR.
Women who experienced previous pregnancy complications were less likely to implement BPCR as compared to women who did not experience previous pregnancy complications. This finding is not supported by a study done in Ethiopia, in which women who had a history of abortion were more likely to prepare for birth and its complication.22 A pregnant woman who faced disrespect while receiving care has less chance of coming to health facility for delivery.43
The odds of women with no IPV experience who had good knowledge of pregnancy danger signs had more likely to practice BPCR as compared to their counterparts. This is similar to a study done in Ethiopia where women who were knowledgeable of pregnancy danger signs were more likely to implement BPCR compared to non-knowledgeable women.22,44 This might happen; women who had a good knowledge of danger signs will also have a good knowledge of BPCR.45
Limitation of the Study
The limitation of this study that needs consideration while interpreting the result is that there might be an under-report of IPV due to the research title being sensitive to some women who may not be a volunteer to disclose their violence (social desirability bias). Some variables had wider confidence intervals; this might be due to the smaller sample size. There might be recall bias since the women did not remember all plans and activities related to BPCR that happened during pregnancy.
Conclusion
The practice of BPCR among women with IPV experience was lower compared with women with no IPV experience. Similarly, women’s knowledge of BPCR, obstetric danger signs during pregnancy, labor, and postpartum were lower among women with IPV experience. Higher educational level, partner not drinking alcohol, no childhood violence, partner’s desire for pregnancy, and good knowledge of BPCR increased the likelihood practice of BPCR among women who experienced IPV, whereas women who did not experience IPV, had no previous pregnancy complications, had good knowledge of BPCR, and pregnancy danger signs were more likely to practice BPCR. Therefore, minimizing women’s IPV help to improve preparation for birth and its complication through improving women’s knowledge on BPCR, empowering women through education, decreasing partner alcohol consumption, avoiding childhood violence, and male involvement in preconception care. It is better to use ANC for screening of IPV of women for early identification, prevention of recurrence violence as well as a way to improve BPCR.
Abbreviations
ANC, ante-natal care; BPCR, birth preparedness and complication readiness; IPV, intimate partner violence; WHO, World Health Organization.
Data Sharing Statement
After the ethical statement was gained from the health office, public health institution, and study participant, the agreement was done not to publish the retrieved raw data obtained from the women. However, the collected and analyzed datasets of this study are available from the corresponding author and can be obtained at a reasonable request.
Ethical Approval and Consent to Participate
Ethical clearance was gained from Mizan-Tepi University ethical review committee. The objective and purpose of the study were explained to the study participants. The study participants were involved in the study after they gave informed verbal and written consent to participate in the study. This study was conducted “following the Declaration of Helsinki.” Data were obtained from study participants. Therefore, the confidentiality of study participants’ data was kept and the data were not used for purposes other than the purpose of the current study. The minimum age of respondents who participated in this study was 18. Study respondents were informed about the right to refuse or withdraw from the study when they feel discomfort.
Acknowledgments
The authors would like to thank Mizan-Tepi University for technical support and ethical approval, respondents, and data collectors.
Funding
The work of this study was funded by Mizan-Tepi University for data collection. This institution did not participate in designing, analysis, and critical review of its intellectual content, manuscript preparation, and the budget funded by this institution did not include publication.
Disclosure
The authors report no conflicts of interest.
References
1. Maternal and Neonatal Health Program. Birth preparedness and complication readiness: a matrix of shared responsibilities. Baltimore, MD: Jhpiego; 2001.
2. Wang W, Alva S, Wang S, Fort A. Levels and trends in the use of maternal health services in developing countries. ICF Macro; 2011.
3. Weldemariam S, Kiros A, Welday M. Utilization of institutional delivery service and associated factors among mothers in North West Ethiopian. BMC Res Notes. 2018;11(1):194. doi:10.1186/s13104-018-3295-8
4. Tekelab T, Chojenta C, Smith R, Loxton D. Factors affecting utilization of antenatal care in Ethiopia: a systematic review and meta-analysis. PLoS One. 2019;14(4):e0214848. doi:10.1371/journal.pone.0214848
5. Akibu M, Tsegaye W, Megersa T, Nurgi S. Prevalence and determinants of complete postnatal care service utilization in northern Shoa, Ethiopia. J Pregnancy. 2018;2018:1–7. doi:10.1155/2018/8625437
6. Kassebaum NJ, Barber RM, Bhutta ZA, et al. Global, regional, and national levels of maternal mortality, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1775–1812. doi:10.1016/S0140-6736(16)31470-2
7. Hamdela B, Getnet Y, Abageda M. Predictors of health facility delivery service utilization in Lemo District, South Ethiopia: unmatched case control study. J Preg Child Health. 2015;2(2):
8. Pun KD, Infanti JJ, Koju R, Schei B, Darj E, Group AS. Community perceptions on domestic violence against pregnant women in Nepal: a qualitative study. Glob Health Action. 2016;9:31964. doi:10.3402/gha.v9.31964
9. World Health Organization. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. World Health Organization; 2013.
10. World Health Organization. Strengthening the role of the health system in addressing violence, in particular against women and girls, and against children. Geneva: Sixty-seventh World Health Assembly; 2014.
11. Mojahed A, Alaidarous N, Shabta H, Hegewald J, Garthus-Niegel S. Intimate partner violence against women in the Arab countries: a systematic review of risk factors. Trauma Violence Abuse. 2020;23(2):390–407. doi:10.1177/1524838020953099
12. Shamu S, Abrahams N, Temmerman M, Musekiwa A, Zarowsky C. A systematic review of African studies on intimate partner violence against pregnant women: prevalence and risk factors. PLoS One. 2011;6(3):e17591. doi:10.1371/journal.pone.0017591
13. Semahegn A, Mengistie B. Domestic violence against women and associated factors in Ethiopia; systematic review. Reprod Health. 2015;12(1):78. doi:10.1186/s12978-015-0072-1
14. Berhanie E, Gebregziabher D, Berihu H, Gerezgiher A, Kidane G. Intimate partner violence during pregnancy and adverse birth outcomes: a case-control study. Reprod Health. 2019;16(1):22. doi:10.1186/s12978-019-0670-4
15. Azene ZN, Yeshita HY, Mekonnen FA. Intimate partner violence and associated factors among pregnant women attending antenatal care service in Debre Markos town health facilities, Northwest Ethiopia. PLoS One. 2019;14(7):e0218722–e0218722. doi:10.1371/journal.pone.0218722
16. Donovan BM, Spracklen CN, Schweizer ML, Ryckman KK, Saftlas AF. Intimate partner violence during pregnancy and the risk for adverse infant outcomes: a systematic review and meta-analysis. BJOG. 2016;123(8):1289–1299. doi:10.1111/1471-0528.13928
17. Chaves K, Eastwood J, Ogbo FA, et al. Intimate partner violence identified through routine antenatal screening and maternal and perinatal health outcomes. BMC Pregnancy Childbirth. 2019;19(1):357. doi:10.1186/s12884-019-2527-9
18. Garcia-Moreno C, Amin A. The sustainable development goals, violence and women’s and children’s health. Bull World Health Organ. 2016;94(5):396. doi:10.2471/BLT.16.172205
19. World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. World Health Organization; 2016.
20. FDRE. The 2017 voluntary national reviews on SDGs of Ethiopia: government commitments, national ownership and performance trends. Addis Ababa: National Plan Commission; 2017.
21. Ababa A. Federal democratic republic of Ethiopia central statistical agency population projection of Ethiopia for all regions at wereda level from 2014–2017. Addis Ababa: Central Statistical Agency; 2014.
22. Limenih MA, Belay HG, Tassew HA. Birth preparedness, readiness planning and associated factors among mothers in Farta district, Ethiopia: a cross-sectional study. BMC Pregnancy Childbirth. 2019;19(1):171. doi:10.1186/s12884-019-2325-4
23. Ellsberg MC, Heise L. Researching violence against women: a practical guide for researchers and activists. World Health Organization; 2005.
24. World Health Organization. WHO multi-country study on women’s health and domestic violence against women: initial results on prevalence, health outcomes and women’s responses/authors: Claudia Garcia-Moreno … [et al.]. Geneva: World Health Organization; 2005.
25. Del Barco R. Monitoring Birth Preparedness and Complication Readiness. Tools and Indicators for Maternal and Newborn Health. Baltimore, MD: Jhpiego; 2004:330.
26. Sumankuuro J, Crockett J, Wang S. Factors influencing knowledge and practice of birth preparedness and complication readiness in sub-Saharan Africa: a narrative review of cross-sectional studies. Int J Community Med Public Health. 2016;3297–3307. doi:10.18203/2394-6040.ijcmph20164251
27. Kareem YO, Morhason-Bello IO, OlaOlorun FM, Yaya S. Temporal relationship between women’s empowerment and utilization of antenatal care services: lessons from four national surveys in sub-Saharan Africa. BMC Pregnancy Childbirth. 2021;21(1):198. doi:10.1186/s12884-021-03679-8
28. Pun KD, Rishal P, Infanti JJ, et al. Exposure to domestic violence influences pregnant women’s preparedness for childbirth in Nepal: a cross-sectional study. PLoS One. 2018;13(7):e0200234. doi:10.1371/journal.pone.0200234
29. Musa A, Chojenta C, Geleto A, Loxton D. The associations between intimate partner violence and maternal health care service utilization: a systematic review and meta-analysis. BMC Women's Health. 2019;19(1):36. doi:10.1186/s12905-019-0735-0
30. Bintabara D, Mohamed MA, Mghamba J, Wasswa P, Mpembeni RNM. Birth preparedness and complication readiness among recently delivered women in chamwino district, central Tanzania: a cross sectional study. Reprod Health. 2015;12(1):44. doi:10.1186/s12978-015-0041-8
31. Kiataphiwasu N, Kaewkiattikun K. Birth preparedness and complication readiness among pregnant women attending antenatal care at the Faculty of Medicine Vajira Hospital, Thailand. Int J Women's Health. 2018;10:797–804. doi:10.2147/IJWH.S185589
32. Ketema DB, Leshargie CT, Kibret GD, Assemie MA, Petrucka P, Alebel A. Effects of maternal education on birth preparedness and complication readiness among Ethiopian pregnant women: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020;20(1):149. doi:10.1186/s12884-020-2812-7
33. Mumtaz S, Bahk J, Khang Y-H. Current status and determinants of maternal healthcare utilization in Afghanistan: analysis from Afghanistan demographic and health survey 2015. PLoS One. 2019;14(6):e0217827. doi:10.1371/journal.pone.0217827
34. Ibadin SH, Adam VY, Adeleye O, Okojie OH. Birth preparedness and complication readiness among pregnant women in a rural community in southern Nigeria. S Afr J Obstet Gynaecol. 2016;22(2):47–51. doi:10.7196/SAJOG.2016.v22i2.1088
35. Ntaganira J, Muula AS, Siziya S, Stoskopf C, Rudatsikira E. Factors associated with intimate partner violence among pregnant rural women in Rwanda. Rural Remote Health. 2009;9(3):1153.
36. Singh JK, Evans-Lacko S, Acharya D, Kadel R, Gautam S. Intimate partner violence during pregnancy and use of antenatal care among rural women in southern Terai of Nepal. Women Birth. 2018;31(2):96–102. doi:10.1016/j.wombi.2017.07.009
37. Cui M, Ueno K, Gordon M, Fincham FD. The continuation of intimate partner violence from adolescence to young adulthood. J Marriage Fam. 2013;75(2):300–313. doi:10.1111/jomf.12016
38. Kivelä S, Leppäkoski T, Helminen M. Continuation of domestic violence and changes in the assessment of family functioning, Health, and Social Support in Finland. Health Care Women Int. 2019;40(11):1283–1297.
39. Ochako R, Gichuhi W. Pregnancy wantedness, frequency and timing of antenatal care visit among women of childbearing age in Kenya. Reprod Health. 2016;13(1):51. doi:10.1186/s12978-016-0168-2
40. Tessema ZT, Teshale AB, Tesema GA, Tamirat KS. Determinants of completing recommended antenatal care utilization in sub-Saharan from 2006 to 2018: evidence from 36 countries using demographic and health surveys. BMC Pregnancy Childbirth. 2021;21(1):192. doi:10.1186/s12884-021-03669-w
41. Suandi D, Williams P, Bhattacharya S. Does involving male partners in antenatal care improve healthcare utilisation? Systematic review and meta-analysis of the published literature from low- and middle-income countries. Int Health. 2020;12(5):484–498. doi:10.1093/inthealth/ihz073
42. Bitew Y, Awoke W, Chekol S. Birth preparedness and complication readiness practice and associated factors among pregnant women, Northwest Ethiopia. Int Sch Res Notices. 2016;2016:8. doi:10.1155/2016/8727365
43. Asefa A, Bekele D, Morgan A, Kermode M. Service providers’ experiences of disrespectful and abusive behavior towards women during facility based childbirth in Addis Ababa, Ethiopia. Reprod Health. 2018;15(1):4. doi:10.1186/s12978-017-0449-4
44. Markos D, Bogale D. Birth preparedness and complication readiness among women of child bearing age group in Goba woreda, Oromia region, Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):282. doi:10.1186/1471-2393-14-282
45. Mbalinda SN, Nakimuli A, Kakaire O, Osinde MO, Kakande N, Kaye DK. Does knowledge of danger signs of pregnancy predict birth preparedness? A critique of the evidence from women admitted with pregnancy complications. Health Res Policy Syst. 2014;12(1):60. doi:10.1186/1478-4505-12-60
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.