")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Effect of High-Intensity Macro-Focused Ultrasound on a Case of Morbihan Disease
Authors Li M, Tao M, Zhang Y, Pan R, Gu D , Xu Y
Received 14 April 2023
Accepted for publication 18 July 2023
Published 25 July 2023 Volume 2023:16 Pages 1949—1954
DOI https://doi.org/10.2147/CCID.S417070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Min Li, Meng Tao, Yue Zhang, Ruoxin Pan, Duoduo Gu, Yang Xu
Department of Dermatology, the First Affiliated Hospital of Nanjing Medical University (Jiangsu Province Hospital), Nanjing, 210029, People’s Republic of China
Correspondence: Yang Xu, Department of Dermatology, the First Affiliated Hospital of Nanjing Medical University (Jiangsu Province Hospital), 300 Guangzhou Road, Nanjing, 210029, People’s Republic of China, Tel/Fax +86-13851856794, Email [email protected]
Abstract: Morbihan disease is a rare entity involving the upper two-thirds of the face and characterized by chronic erythematous edema, which is recalcitrant to the traditional therapy of rosacea. We report a case of Morbihan disease effectively treated with macro-focused high-intensity focus ultrasound (MF-HIFU). After MF-HIFU treatment, an obvious reduction in swelling was observed with decreased erythema and hyperalgesia. In addition, in-vitro experiments were conducted to measure the actual temperature of the skin tissue under the epidermis. The results of the in-vitro experiments showed that the temperature plateau in the skin sample was reached at approximately 42°C after 5-min treatment or longer. MF-HIFU might be a promising energy-based therapy for Morbihan disease.
Keywords: erythema, edema, rosacea, energy-based treatment
Introduction
Morbihan disease, also referred to as rosacea lymphedema, is a rare entity involving the upper two-thirds of the face and characterized by chronic erythematous edema, which is recalcitrant to the traditional therapy of rosacea. Oral drugs (isotretinoin, thalidomide, clofazimine, ketotifen, etc.) and surgical intervention have been used alone or in combination with each other to treat Morbihan disease.1 Obstruction of lymphatic vessels is considered one of the potential mechanisms of Morbihan disease, so it seems that improvement of lymphatic drainage would be an effective adjunctive therapy which has been proved in patients with breast cancer-related lymphedema only showing increased lymphatic contraction frequency after hyperthermia therapy。2–4 We therefore hypothesized that proper heating of the subepidermal tissue to approximately 40°C might be a potential therapy for Morbihan disease.
Here, we present a case of Morbihan disease recalcitrant to traditional therapy that was effectively treated with macro-focused high-intensity focus ultrasound (MF-HIFU), considering that lymph obstruction might be improved by proper heating of the tissue under the epidermis. We also conducted an in vitro study to investigate the potential mechanism of the treatment and reviewed the current literature.
Materials and Methods
Case Report
A 56-year-old female patient presented to the Dermatology Department of our hospital with complaints of erythema and edema of the cheeks with discomfort, including swelling and hyperalgesia, for 10 years. She had been diagnosed with rosacea and treated intermittently with hydroxychloroquine and minocycline. Facial erythema improved, while the swelling of the cheeks and hyperalgesia did not. Oral antidepressants, such with a fixed-dose combination tablet of melitracen/flupentixol were also used for approximately 6 months, with no improvement. Exposure to hot and cold weather, sunlight, and cosmetics increased the discomfort.
Physical examination revealed firm swelling and erythema of the cheeks and forehead without any obvious scaling, papules, or pustules (Figure 1Aa–Ac). In the red area images taken by the VISIA® Complexion Analysis System (Canfield Scientific, NJ, USA), the erythema was more obvious (Figure 1Ad–Af). Sense of swelling and hyperalgesia were measured using a visual analog scale (VAS) and were 6.0 and 6.5 on a 10-point scale, respectively. The patient underwent routine blood examination, antinuclear antibodies, thyroid function test, full blood count, and CT scan of the lungs. The results were normal. Skin biopsy demonstrated a non-specific inflammatory reaction in the dermis, consistent with rosacea, and Morbihan disease was diagnosed. The patient refused further oral medications including isotretinoin, for possible side effects and personal reasons. Therefore, all systemic medications were discontinued, and a trial treatment using micro- and macro-focused high-intensity ultrasound (Peninsula Med, Shenzhen, China) therapy was initiated. An MF-HIFU tip was used (4 MHz, 3-mm focal depth, and intensity of 3.76 W) for 5 min on both cheeks. Hydrogel was applied evenly on both sides of the cheeks with a thickness of 2 mm, and the tip was in continuous smooth motion on the cheek without overheating one site. All areas, except the periorbital region, were treated. Maintenance treatment was administered for a further 2 months, every 4 weeks, and then discontinued due to improvement in clinical manifestations without relapse at 6 months follow-up (Figure 1Ba–Bc, Ca–Cc, and Da–Dc) and a reduction in erythema intensity (Figure 1Bd–Bf, Cd–Cf, and Dd–Df). At the 6-month follow-up, an obvious reduction in swelling was observed with decreased erythema and hyperalgesia (Figure 2).
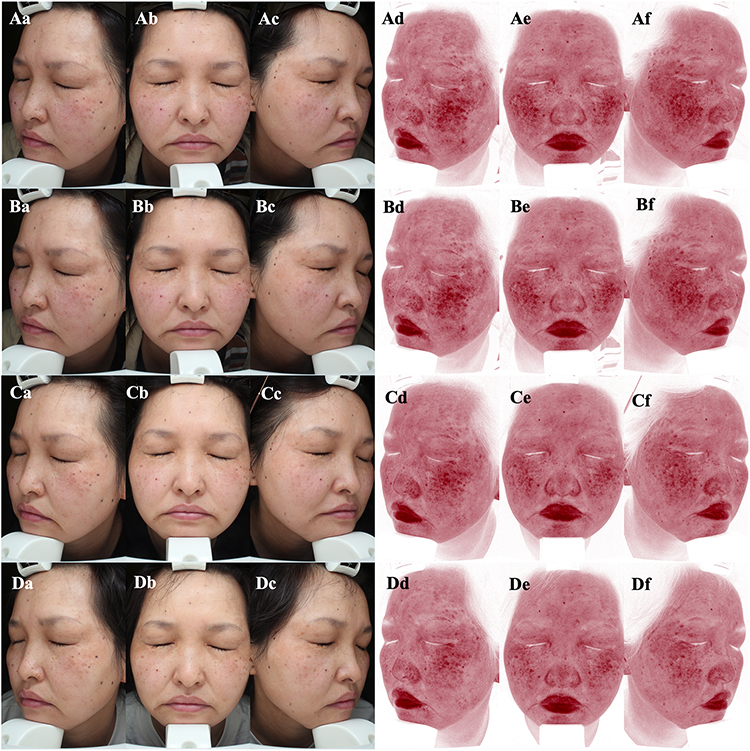 |
Figure 1 Clinical and erythema area images of the patient taken by the VISIA® Complexion Analysis System. (A) Before MF-HIFU treatment (Aa–Ac: Clinical manifestation images; Ad–Af: Red area images). (B) One month after the first treatment (Ba–Bc: Clinical manifestation images; Bd–Bf: Red area images). (C) One month after the second treatment (Ca–Cc: Clinical manifestation images; Cd–Cf: Red area images). (D) Six-month follow-up (Da–Dc: Clinical manifestation images; Dd–Df: Red area images). Abbreviation: MF-HIFU, macro-focused high-intensity focus ultrasound. |
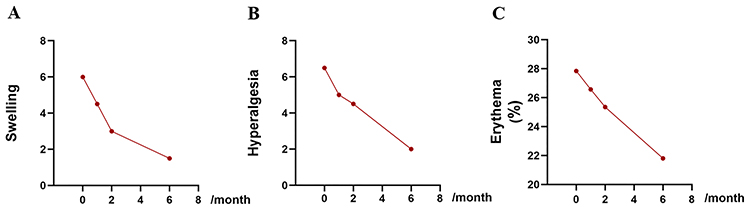 |
Figure 2 (A) VAS score for swelling at the 6-month follow-up. (B) VAS score for hyperalgesia at the 6-month follow-up. (C) Facial erythema extent at the 6-month follow-up. Abbreviation: VAS, visual analog scale. |
In-Vitro Experiments
Further in-vitro experiments were conducted to measure the actual temperature of the skin tissue under the epidermis. Surplus skin tissue from mastectomy were used with informed consent from the patients. The skin tissue was cut into blocks of approximately 3×2 × 1 cm and treated with MF-HIFU under the same conditions as those used for the Morbihan patients (4 MHz, 3-mm focal depth, 3.76 W intensity, Figure 3A). Temperature changes were recorded using an electric thermometer (Aikesi Electronic Technology, Changzhou, China), and the time-temperature curve was recorded (Figure 3B). After 5-min treatment, the temperature in the skin sample was 41.8°C; with more treatment time, a temperature plateau was reached at approximately 42°C.
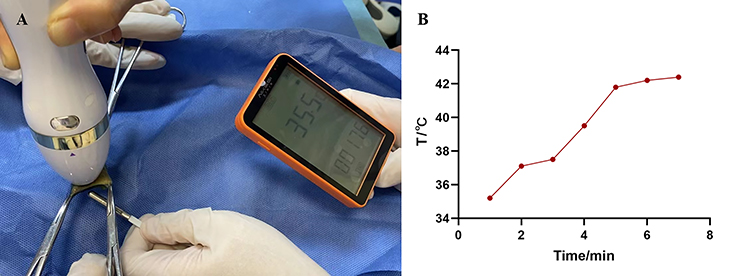 |
Figure 3 (A) Skin tissue treated with MF-HIFU and the temperature measuring device. (B) Temperature in the skin tissue beneath the epidermis. Abbreviation: MF-HIFU, macro-focused high-intensity focus ultrasound. |
Literature Review
Although the pathogenesis of Morbihan disease is not fully understood, it is characterized by erythema and solid edema of the upper two-thirds of the face, probably caused by bivascular dysregulation, fibrosis, and obstruction of lymphatic vessels.2 Differential diagnosis includes sarcoidosis, systemic lupus erythematosus, cutaneous leishmaniasis, foreign body granuloma, and Melkersson–Rosenthal syndrome.
A review of the literature was undertaken by searching PubMed using the keywords “Morbihan disease”, “high-intensity ultrasound”, “micro-focused ultrasound”, and “macro-focused ultrasound”, and revealed several Morbihan disease cases that were effectively treated with systemic therapy and surgical excision from 2004 to 2022 (Table 1), while no energy-based treatment has been reported to be effective.4–17
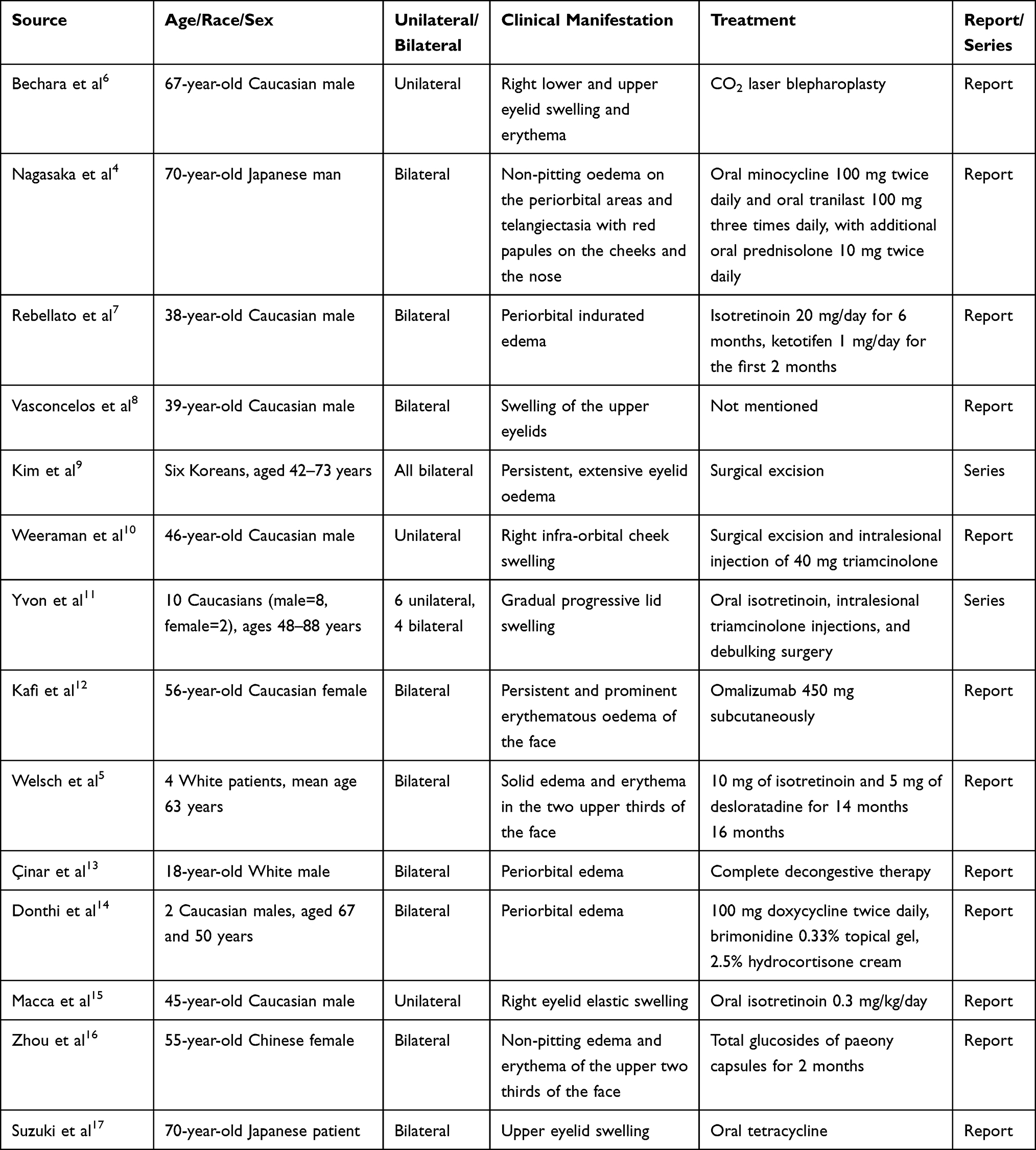 |
Table 1 Clinical Characteristics of Previously Reported Cases of Morbihan Disease |
Discussion
Ultrasound has mechanical, cavitation, and thermal effects. High-intensity micro-focused ultrasound was first used for noninvasive skin rejuvenation by White et al in 2007.18 It accurately focuses the heat in the dermal area and superficial musculoaponeurotic system, with minimal damage to surrounding structures. The wound-healing cascade activates fibroblast differentiation and collagen synthesis, together with skin tightening. HIFU has also been approved for dermatological and aesthetic usage in China, and has two handle pieces, micro- and macro-focused. The former is similar to the instrument approved by the FDA, while the latter has a more diffuse focus area, that is, a larger heated area which produces a smaller increase in temperature in the dermal and subcutaneous layers, with a maximum temperature of less than 42.4°C, in a time-dependent manner, as revealed by our in-vitro experiment.
The most common histological findings of Morbihan disease were dermal edema, sebaceous hyperplasia, perivascular lymphocytes and histiocytes, and granulomatous reaction.19 Previous research reported that complete decongestive therapy (CDT) can be considered as an effective therapeutic tool for the treatment of Morbihan disease, which consists of manual lymphatic drainage, compression therapy, skin care, exercise, and self-care.1 Apart from pressurization, it has been reported that heat can increase lymphatic drainage. Besides, it was demonstrated that compared to other temperatures, such as 24°C and 30°C, a temperature of 40°C significantly increased the transportation of lymph.20,21 Local hyperthermia can significantly increase lymphatic contraction frequency in those patients with breast cancer-related lymphedema patients while without lymphatic complications.6 Elevated skin temperature increases the dilatation of capillaries, thereby improving blood and lymph circulation and alleviating swelling. Another study found that assessment by electromagnetic diathermy heat could accelerate venous return, which might be the mechanism for treating lymph edema.22 The improvement in swelling and discomfort after MF-HIFU treatment confirmed our hypothesis that that the proper heating of the subepidermal tissue to approximately 40°C might be a potential therapy for Morbihan disease.
Conclusion
In conclusion, MF-HIFU might be a promising energy-based therapy for Morbihan disease. However, this study had some limitations. First, the generalizability of the effect of MF-HIFU on Morbihan disease is limited as this is the only case reported in the literature. Second, we failed to measure the dermis and epidermis temperatures both independently and simultaneously due to the constraints of the measuring conditions.
Ethics Approval and Informed Consent
The patient reported in this manuscript gave written informed consent to participate in this study, and for the details of her case and accompanying photographs to be published. Institutional approval is not required to publish the case details in accordance with local legislation and institutional requirements.
Acknowledgments
The authors wish to thank the patient, all participating investigators, and the study team involved in the conduct of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kutlay S, Ozdemir EC, Pala Z, et al. Complete decongestive therapy is an option for the treatment of rosacea lymphedema (Morbihan Disease): two cases. Phys Ther. 2019;99(4):406–410. doi:10.1093/ptj/pzy155
2. Mayur O, Martinez R, McNichol MC, et al. Clinical and histological features and treatment outcomes of patients with Morbihan disease: a systematic review. Arch Dermatol Res. 2023. doi:10.1007/s00403-023-02621-6
3. Johannessen AL, Alstrup M, Hjortdal VE, et al. Lymphatic function decreases over time in the arms of breast cancer patients following treatment. Plast Reconstr Surg Glob Open. 2022;10(9):e4507. doi:10.1097/GOX.0000000000004507
4. Nagasaka T, Koyama T, Matsumura K, et al. Persistent lymphoedema in Morbihan disease: formation of perilymphatic epithelioid cell granulomas as a possible pathogenesis. Clin Exp Dermatol. 2008;33(6):764–767. doi:10.1111/j.1365-2230.2008.02892.x
5. Welsch K, Schaller M. Combination of ultra-low-dose isotretinoin and antihistamines in treating Morbihan disease - A new long-term approach with excellent results and a minimum of side effects. J Dermatolog Treat. 2021;32(8):941–944. doi:10.1080/09546634.2020.1721417
6. Bechara FG, Jansen T, Losch R, et al. Morbihan’s disease: treatment with CO2 laser blepharoplasty. J Dermatol. 2004;31(2):113–115. doi:10.1111/j.1346-8138.2004.tb00518.x
7. Rebellato PR, Rezende CM, Battaglin ER, et al. Syndrome in question. An Bras Dermatol. 2015;90(6):909–911. doi:10.1590/abd1806-4841.20153818
8. Vasconcelos RC, Eid NT, Eid RT, et al. Morbihan syndrome: a case report and literature review. An Bras Dermatol. 2016;91(5 suppl 1):157–159. doi:10.1590/abd1806-4841.20164291
9. Kim JE, Sim CY, Park AY, et al. Case series of Morbihan disease (Extreme Eyelid Oedema Associated with Rosacea): diagnostic and therapeutic approaches. Ann Dermatol. 2019;31(2):196–200. doi:10.5021/ad.2019.31.2.196
10. Weeraman S, Birnie A. Rosacea causing unilateral Morbihan syndrome. BMJ Case Rep. 2019;12:e231074.
11. Yvon C, Mudhar HS, Fayers T, et al. Morbihan syndrome, a UK case series. Ophthalmic Plast Reconstr Surg. 2020;36(5):438–443. doi:10.1097/IOP.0000000000001589
12. Kafi P, Edén I, Swartling C. Morbihan syndrome successfully treated with omalizumab. Acta Derm Venereol. 2019;99(7):677–678. doi:10.2340/00015555-3168
13. Çinar GN, Özgül S, Nakip G, et al. Complex decongestive therapy in the physical therapist management of rosacea-related edema (Morbus Morbihan Syndrome): a case report with a new approach. Phys Ther. 2021;101:zab133. doi:10.1093/ptj/pzab133
14. Donthi D, Nenow J, Samia A, et al. Morbihan disease: a diagnostic dilemma: two cases with successful resolution. SAGE Open Med Case Rep. 2021;9:2050313x211023655. doi:10.1177/2050313X211023655
15. Macca L, Li Pomi F, Motolese A, et al. Unilateral Morbihan syndrome. Dermatol Rep. 2022;14(2):9270. doi:10.4081/dr.2021.9270
16. Zhou LF, Lu R. Successful treatment of Morbihan disease with total glucosides of paeony: a case report. World J Clin Cases. 2022;10(19):6688–6694. doi:10.12998/wjcc.v10.i19.6688
17. Suzuki M, Watari T. Morbihan syndrome. J Gen Intern Med. 2023;38(1):233. doi:10.1007/s11606-022-07858-x
18. Hu SW, Robinson M, Meehan SA, et al. Morbihan disease. Dermatol Online J. 2012;18(12):27. doi:10.5070/D37RC0M3KS
19. White WM, Makin IRS, Barthe PG, et al. Selective creation of thermal injury zones in the superficial musculoaponeurotic system using intense ultrasound therapy: a new target for noninvasive facial rejuvenation. Arch Facial Plast Surg. 2007;9(1):22–29. doi:10.1001/archfaci.9.1.22
20. Olszewski W, Engeset A, Jaeger PM, et al. Flow and composition of leg lymph in normal men during venous stasis, muscular activity and local hyperthermia. Acta Physiol Scand. 1977;99(2):149–155. doi:10.1111/j.1748-1716.1977.tb10365.x
21. Yasuda A, Ohshima N. In situ observations of spontaneous contractions of the peripheral lymphatic vessels in the rat mesentery: effects of temperature. Experientia. 1984;40(4):342–343. doi:10.1007/BF01952541
22. van der Veen P, Kempenaers F, Vermijlen S, et al. Electromagnetic diathermia: a lymphoscintigraphic and light reflection rheographic study of leg lymphatic and venous dynamics in healthy subjects. Lymphology. 2000;33(1):12–18.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.