Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Ephedrine versus Phenylephrine on Postoperative Delirium in Elderly Patients Undergoing Total Hip or Knee Arthroplasty: A Randomized Controlled Trial
Authors Song JL ![]() , Zhang JT, Wang XJ, Yu X, Li Q, Lu B, Chen GY
, Zhang JT, Wang XJ, Yu X, Li Q, Lu B, Chen GY ![]()
Received 14 July 2025
Accepted for publication 27 November 2025
Published 12 December 2025 Volume 2025:19 Pages 10991—11005
DOI https://doi.org/10.2147/DDDT.S553478
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Jian-Li Song,* Jun-Tao Zhang,* Xu-Jiao Wang, Xuan Yu, Qiang Li, Bin Lu, Guan-Yu Chen
Department of Anesthesiology, Zigong Fourth People’s Hospital, Zigong City, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Lu; Guan-Yu Chen, Zigong Fourth People’s Hospital, No. 19, Tanmulin Street, Ziliujing District, Zigong City, Sichuan, People’s Republic of China, Email [email protected]; [email protected]
Background: Postoperative delirium (POD) is a common complication in elderly patients. Since ephedrine and phenylephrine have different effects on cerebral perfusion and oxygenation, this randomized controlled trial aimed to compare the impact of these two drugs on the incidence of POD in elderly patients undergoing total hip or knee arthroplasty under general anesthesia.
Patients and Methods: A total of 142 elderly patients, aged 65 to 80 years, who underwent elective surgery for total hip or knee arthroplasty were randomly assigned to either the ephedrine group (Group E) or the phenylephrine group (Group P). POD was evaluated using the 3-minute Diagnostic Confusion Assessment Method (3D-CAM). The primary outcome was the incidence of POD within three days after surgery, while secondary outcomes included the subtypes of delirium, intraoperative hemodynamic changes, intraoperative analgesic consumption, and the occurrence of intraoperative and postoperative adverse events.
Results: Delirium occurred in 5 out of 65 cases (7.7%) in Group E and in 15 out of 67 cases (22.4%) in Group P (relative risk [RR], 0.344; 95% confidence interval [CI], 0.132 to 0.891; p = 0.019). Compared to Group P, Group E exhibited a significantly lower incidence of intraoperative bradycardia (RR, 0.241; 95% CI, 0.114 to 0.508; p < 0.001). However, Group E also demonstrated a significantly higher consumption of intraoperative opioids (median difference [MD], 23.0; 95% CI, 2.0 to 25.0 mg; p = 0.020). Notably, despite the higher intraoperative opioid consumption in Group E, there was no statistically significant difference in postoperative pain scores between the two groups (p > 0.05). Additionally, there were no statistically significant differences between the two groups in other indicators, including intraoperative hemodynamic changes and the incidence of postoperative nausea and vomiting (p > 0.05).
Conclusion: In conclusion, among elderly patients undergoing hip or knee arthroplasty, the use of ephedrine to correct intraoperative hypotension was associated with a reduced incidence of POD within three days compared to phenylephrine. However, the absence of cerebral oxygen saturation monitoring and the limited follow-up period of only three days for POD assessment represent significant limitations. These factors should be carefully considered when interpreting our results.
Keywords: ephedrine, phenylephrine, delirium, elderly patients, orthopedic surgery
Introduction
Postoperative delirium (POD) is a common complication among elderly surgical patients, with incidence rates ranging from 29% to 64%, reaching up to 50% in those undergoing total hip or knee arthroplasty.1–3 POD has been associated with prolonged hospital stay, increased mortality, and elevated medical costs.4–6 Additionally, it is correlated with long-term outcomes such as cognitive decline and an increased risk of dementia.7,8 The etiology of delirium is diverse and complex, with numerous risk factors.9,10 Among these factors, intraoperative hypotension has attracted widespread attention as a critical and modifiable factor contributing to POD, with evidence from multiple study types—including multicenter cohort studies and meta-analyses—consistently identifying it as an independent and intervenable risk factor.10–13
Intraoperative sustained or severe hypotension elevates the risk of POD, primarily by inducing cerebral ischemia and hypoxia due to insufficient cerebral perfusion.14,15 This ischemic-hypoxic state can cause neuronal damage through the release of pro-inflammatory cytokines and disrupt the blood-brain barrier via the TLR4/NF-κB pathway, coupled with inhibited ATP production. These processes ultimately contribute to POD, especially in elderly patients with compromised cerebral autoregulation.16,17 Furthermore, with an aging population, 36% of inpatient surgical patients are aged 65 years and older—an age group that may face a relatively higher risk of intraoperative hypotension.18,19 Notably, elderly patients undergoing total hip or knee arthroplasty are at an even higher risk of intraoperative hypotension due to perioperative fluid shifts and anesthesia-related vasodilation.20 Therefore, effectively preventing intraoperative hypotension in these patients, minimizing its duration when it occurs, and reducing its incidence are critically important for decreasing the occurrence of POD.
Ephedrine and phenylephrine, two commonly used perioperative vasoactive drugs, differ significantly in their effects on cardiac output (CO) and cerebral tissue oxygen saturation (SctO2).21–23 Ephedrine, a mixed α/β-agonist, increases CO by enhancing myocardial contractility and heart rate, whereas phenylephrine, a selective α-agonist, raises blood pressure through peripheral vasoconstriction but may reduce CO and cause cerebral vasoconstriction, potentially impairing SctO2.22,23 Recent studies have demonstrated that ephedrine is superior to phenylephrine in improving both cerebral macro- and microhemodynamics, as well as oxygenation, in patients with brain tumors.24 This suggests that the differential effects of ephedrine and phenylephrine on cerebral perfusion may translate to differences in POD incidence. Previous research has indicated that imbalances in cerebral perfusion and oxygenation are among the most significant causes of POD in surgical patients.25,26 A retrospective study further indicated that ephedrine might reduce the incidence of POD when used to correct intraoperative hypotension; however, this finding requires validation in prospective trials.27
This study compares ephedrine and phenylephrine in elderly patients undergoing hip or knee arthroplasty, hypothesizing that ephedrine’s beneficial effects on cerebral perfusion and oxygenation will lead to a lower incidence of POD compared to phenylephrine.
Methods
Study Design and Participants
This was a prospective, single-blind, single-center, randomized clinical trial (RCT). The study received approval from the Medical Ethics Committee of Zigong Fourth People’s Hospital (Ethical approval number: EC-2024-084) and was conducted in accordance with the Helsinki Declaration. Additionally, the trial was registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn/) with the registration identifier ChiCTR2400088799 on August 27, 2024. The research was carried out at Zigong Fourth People’s Hospital, and written informed consent was obtained from all participants or their legal representatives prior to enrollment in the trial.
All patients who participated in the trial received comprehensive information about the study protocol prior to enrollment. The inclusion criteria were as follows: (1) patients aged 65 to 80 years with a body mass index (BMI) ranging from 18 to 30 kg/m2; (2) American Society of Anesthesiologists (ASA) physical status II to III; (3) an expected postoperative hospital stay of ≥ three days or more. The exclusion criteria included: (1) patients with a history of alcohol, sedative-analgesic, psychotropic, or substance abuse and addiction; (2) patients with speech or hearing impairments, as well as severe neuropsychiatric disorders that prevent effective communication; (3) patients with combined vital organ insufficiency, such as cardiac failure or severe hepatic or renal failure (Child-Pugh classification C or an estimated glomerular filtration rate of less than 60 mL min−1 per 1.73 m2); (4) patients with allergies to or contraindications for ephedrine or phenylephrine; and (5) patients who refuse to sign the informed consent. The criteria for withdrawal were as follows: more than 1000 mL of blood loss during surgery or failure to use vasoactive drugs according to the anesthetic protocol of this trial.
Randomization and Masking
Enrolled patients were randomly allocated to receive either ephedrine or phenylephrine following an episode of transient hypotension, in a 1:1 ratio. This allocation was determined using a computer-generated random sequence—specifically, the sequence was generated via SPSS Statistics 26.0 software using its built-in “Random Number Generator” function. Sealed, opaque envelopes were utilized to conceal group assignments, and an assistant who was not involved in the anesthesia prepared the drugs for administration. To ensure safe intraoperative medication management, the anesthesiologists were informed of the group assignments but were not involved in the follow-up evaluations. Patients, surgeons, data collectors, and the attending anesthesiologist in charge of the post-anesthesia care unit (PACU) were blinded to the group assignments. The group allocation was disclosed only after the completion of data collection and analysis.
Anesthesia Method
All patients were required to fast for eight hours prior to the procedure. No preoperative medication was administered to either group. Upon arrival in the operating room, preoxygenation was provided using a mask with an oxygen flow rate of 6 L/min, and standard monitoring was implemented, which included pulse oximetry (SpO2), electrocardiography (ECG), heart rate (HR), non-invasive blood pressure measurement, and bispectral index (BIS) monitoring. Before the induction of anesthesia, invasive arterial blood pressure (IBP) was monitored in all patients through radial artery cannulation under local anesthesia.
General anesthesia was induced using sufentanil at a dosage of 0.3 to 0.5 μg/kg, etomidate at 0.1 mg/kg, rocuronium at 1 mg/kg, and propofol at 1 to 1.5 mg/kg. Tracheal intubation was performed under laryngoscopic guidance once sufentanil and muscarinic agents had taken full effect, followed by the initiation of mechanical ventilation. Intraoperative respiratory parameters were set as follows: a tidal volume of 6 to 8 mL/kg, a respiratory rate of 12 breaths per minute, an inspired oxygen concentration of 60%, and an inspiratory-expiratory ratio of 1:1.5. These parameters were adjusted as necessary to maintain the end-tidal carbon dioxide partial pressure (PetCO2) within the range of 35 to 45 mmHg. Anesthesia maintenance was achieved through a combination of intravenous and inhalational agents. Remifentanil was administered intravenously at a rate of 0.1 to 0.4 μg/kg/min, while sevoflurane was inhaled to maintain a BIS value of 40 to 60. Both sevoflurane and remifentanil were discontinued 5 minutes before the end of surgery. Intraoperative fluid balance was maintained using Ringer’s lactate, with the infusion rate controlled at 5 to 7 mL/kg per hour. Rehydration was provided with succinyl gelatin in cases of significant intraoperative bleeding. In this study, hypotension was corrected with either ephedrine or phenylephrine when the intraoperative mean arterial pressure (MAP) fell below 65 mmHg, based on the results of random group assignment.
After surgery, all patients were transferred to the PACU for resuscitation. Patients with a Steward score of 6 or higher were subsequently returned to the ward. Each patient was provided with a patient-controlled analgesia (PCA) device, which was connected at the end of the surgical procedure. The PCA solution contained 1 μg/mL of sufentanil, 2 mg of hydromorphone, and 9 mg of granisetron, totaling a volume of 150 mL. The PCA device was programmed to deliver a continuous background dose of 0.4 mL/kg, along with a bolus dose of 2 mL, and featured a lockout interval of 15 minutes.
Perioperative Hemodynamic Management
The baseline MAP of the patients was determined by averaging three consecutive non-invasive blood pressure measurements, each with an error margin of less than 10%, taken every three minutes following their admission to the operating room. Intraoperative hypotension is defined as a MAP below 65 mmHg, which is the most commonly used threshold for identifying systemic hypotension, particularly intraoperative hypotension.28 Furthermore, evidence suggests that this threshold is more strongly associated with POD and other postoperative adverse outcomes.29,30 When the MAP remains persistently below 65 mmHg, confirmed by continuous monitoring for at least 30 seconds, 1 mL of ephedrine (6 mg/mL) or phenylephrine (75 μg/mL) is administered intravenously, based on the equivalent doses of these agents.31 If the MAP does not return to 65 mmHg or above within 2 minutes after the first dose, the same drug and dosage may be administered again. The maximum number of consecutive doses should not exceed three. If the MAP still fails to reach the target after three doses, the anesthesiologist may switch to alternative blood pressure management strategies based on clinical judgment and must document the adjustment process in detail in the case report form. Intraoperative hypertension was defined as a MAP exceeding 160 mmHg or an increase of more than 20% from the baseline value. If the patient developed hypertension, the rate of remifentanil infusion or the concentration of sevoflurane was increased to deepen the anesthesia. In the event of intraoperative bradycardia (defined as a heart rate of less than 50 beats per minute), 0.5 mg of atropine was administered. In the cases of tachycardia (defined as a heart rate greater than 120 beats per minute), 20 mg of esmolol was administered.
Outcome Measures
Primary Outcome
The primary outcome was the incidence of delirium during the first three postoperative days. Delirium assessments were conducted using the 3-minute Diagnostic Confusion Assessment Method (3D-CAM) twice daily, between 8:00–10:00 and 16:00–20:00, by the same research team member who had received training prior to the study and was blinded to group allocation. Patients with POD were further classified into three subtypes based on their levels of consciousness, as evaluated by the Richmond Agitation Sedation Scale (RASS) immediately prior to the delirium assessment. Hyperactive delirium was defined as a consistently positive RASS score (+1 to +4), hypoactive delirium was defined as a consistently neutral or negative RASS score (–3 to 0), and mixed delirium was characterized by the presence of both hypoactive and hyperactive delirium episodes during the observation period.
Secondary Outcomes
The secondary outcomes included MAP, HR, SpO2, BIS and PetCO2 at the following time points: at the baseline (T0), 5 minutes after intubation (T1), at the beginning of surgery (T2), 30 minutes after the start of surgery (T3), 60 minutes after the start of surgery (T4), and at the end of surgery (T5). Additionally, the secondary outcomes encompassed the incidence of delirium subtypes, the number of days with delirium, total intraoperative opioid consumption, total vasoactive drug consumption, length of stay in the PACU, postoperative pain scores, and length of hospital stay. The following adverse events were recorded: intraoperative hypotension, intraoperative hypertension, tachycardia, bradycardia, incidence of low BIS, incidence of hypothermia, incidence of postoperative nausea and vomiting (PONV) within three days postoperatively, unplanned transfer to the intensive care unit (ICU), intraoperative awareness, and postoperative hypoxemia. The total intraoperative consumption of opioids will be converted to intravenous morphine milligram equivalents (IMME) using the following conversion standards: 1 microgram of sufentanil is equivalent to 1 milligram of morphine, and 1 milligram of morphine is equivalent to 10 micrograms of remifentanil.32 Postoperative hypoxemia was defined as SpO2 levels below 90% in the PACU and on the ward during postoperative follow-up. Postoperative pain scores were evaluated using the Numerical Rating Scale (NRS, 0–10 points) by trained clinical staff. Assessments were conducted during two fixed time windows (8:00–10:00 a.m. and 4:00–8:00 p.m.) on the first, second, and third postoperative days, corresponding to the time points for POD assessment. At each time point, two scores were recorded separately: one at rest and the other during activity (such as deep breathing or coughing). All assessors completed a standardized 2-hour NRS training session and passed a pre-study competency test to ensure consistency in assessments. Intraoperative low BIS is defined as a BIS value below 40 sustained for 5 minutes or longer. Intraoperative hypothermia is defined as a nasopharyngeal temperature below 36.0°C.
Sample Size Calculation
The sample size was determined a priori using PASS 15.0. Based on previously published studies on POD, the incidence of POD in orthopedic surgery patients ranges from 12% to 51%.2 Therefore, we estimated that the incidence of POD after lower limb arthroplasty in elderly patients in Group P is approximately 30%. To achieve 80% power in detecting a true difference with a two-tailed significance level (α) of 0.05, and assuming a POD incidence of 10% in Group E, a total of 118 patients would need to be included across both groups. Considering a 20% dropout rate, a total of 142 patients should be recruited, with 71 patients in each group.
Statistical Analysis
Statistical analyses were conducted using SPSS version 26.0 (IBM Corp, Armonk, NY, USA). Continuous variables were initially assessed for normality using the Shapiro–Wilk test. Variables with a normal distribution were reported as mean ± standard deviation (SD), and between-group comparisons were performed using the unpaired two-tailed t-test. Variables with a non-normal distribution were presented as median (interquartile range, IQR), with between-group comparisons conducted using the Mann–Whitney U-test. Categorical variables were expressed as counts (percentages), and comparisons were made using either the chi-square test or Fisher’s exact test, as appropriate. For comparisons of the primary outcome measure (POD) between the two groups, effect sizes were expressed as relative risk (RR) with 95% confidence intervals (CIs). Additionally, survival analysis was employed for further comparisons, with results presented as hazard ratios (HRs) and 95% CIs. Given that this two-treatment study involves repeated measurements, we will utilize either repeated-measures analysis of variance (RM-ANOVA) or generalized estimating equations (GEE) to compare various indices between the two groups at multiple time points. These indices include MAP, HR, SpO2, BIS, and PetCO2, depending on whether the study data conform to a normal distribution. Univariate and multivariate logistic regression models were utilized to evaluate potential risk factors associated with POD. Subgroup analyses comprised two components: first, a prespecified analysis based on surgical type (hip surgery versus knee surgery); second, subgroup tests that included some variables with a p-value of less than 0.1 from univariate logistic regression analyses. For the subgroup analyses, odds ratios (ORs) and 95% CIs for each subgroup were calculated, and heterogeneity between subgroups was evaluated using interaction tests. All statistical tests were two-sided, and a p-value of less than 0.05 was considered statistically significant.
Results
From September 2024 to May 2025, a total of 162 patients who met the inclusion criteria were assessed. Among these, 20 patients were excluded for various reasons, including refusal to participate, inability to communicate effectively, and significant organ dysfunction. Ultimately, 142 patients were randomized into Group E (n=71) and Group P (n=71). Of these 142 patients, 10 were withdrawn from the analysis: 7 patients did not experience intraoperative hypotension, and 3 patients switched to alternative vasoactive agents. Consequently, 132 patients were randomly assigned to either Group E (n=65) or Group P (n=67). A flowchart illustrating patient enrollment is provided in Figure 1.
 |
Figure 1 Consolidated Standards of Reporting Trials flow study diagram describing patient progress through the study. |
Baseline Demographics and Clinical Characteristics
The baseline demographic characteristics were evenly randomized between the two groups (Table 1). Furthermore, most intraoperative characteristics were similar between the two groups, with the exception of intraoperative total opioid consumption (IMME median difference [MD], 23.0; 95% confidence interval [CI], 2.0 to 25.0 mg; P = 0.020) and the incidence of bradycardia during surgery (RR, 0.241; 95% CI, 0.114 to 0.508; P < 0.001) (Table 2). The median total intraoperative doses administered were 0.2 mg [IQR: 0.05 to 0.35 mg] for phenylephrine and 12.0 mg [IQR: 7.5 to 16.5 mg] for ephedrine. However, we found that neither ephedrine nor phenylephrine demonstrated a dose-effect relationship with the incidence of POD (RR, 0.053, 95% CI, −0.753 to 0.795; P = 0.958 and RR, 0.406, 95% CI, −0.230 to 0.350; P = 0.685, respectively). In terms of postoperative adverse events, only one patient in Group E developed hypoxia, while the incidence of all other adverse events was zero.
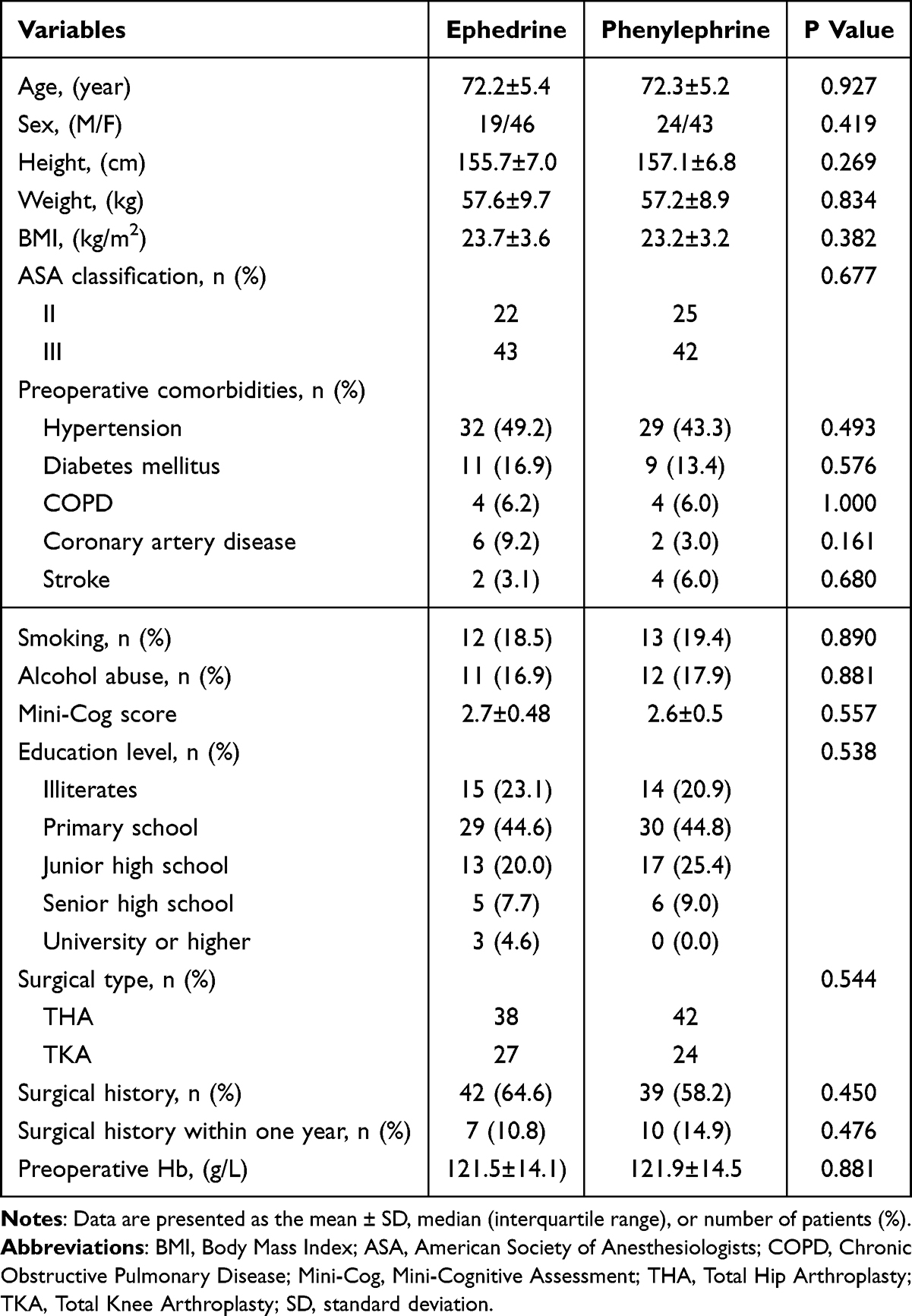 |
Table 1 Baseline Demographic Characteristics of the Study Patients |
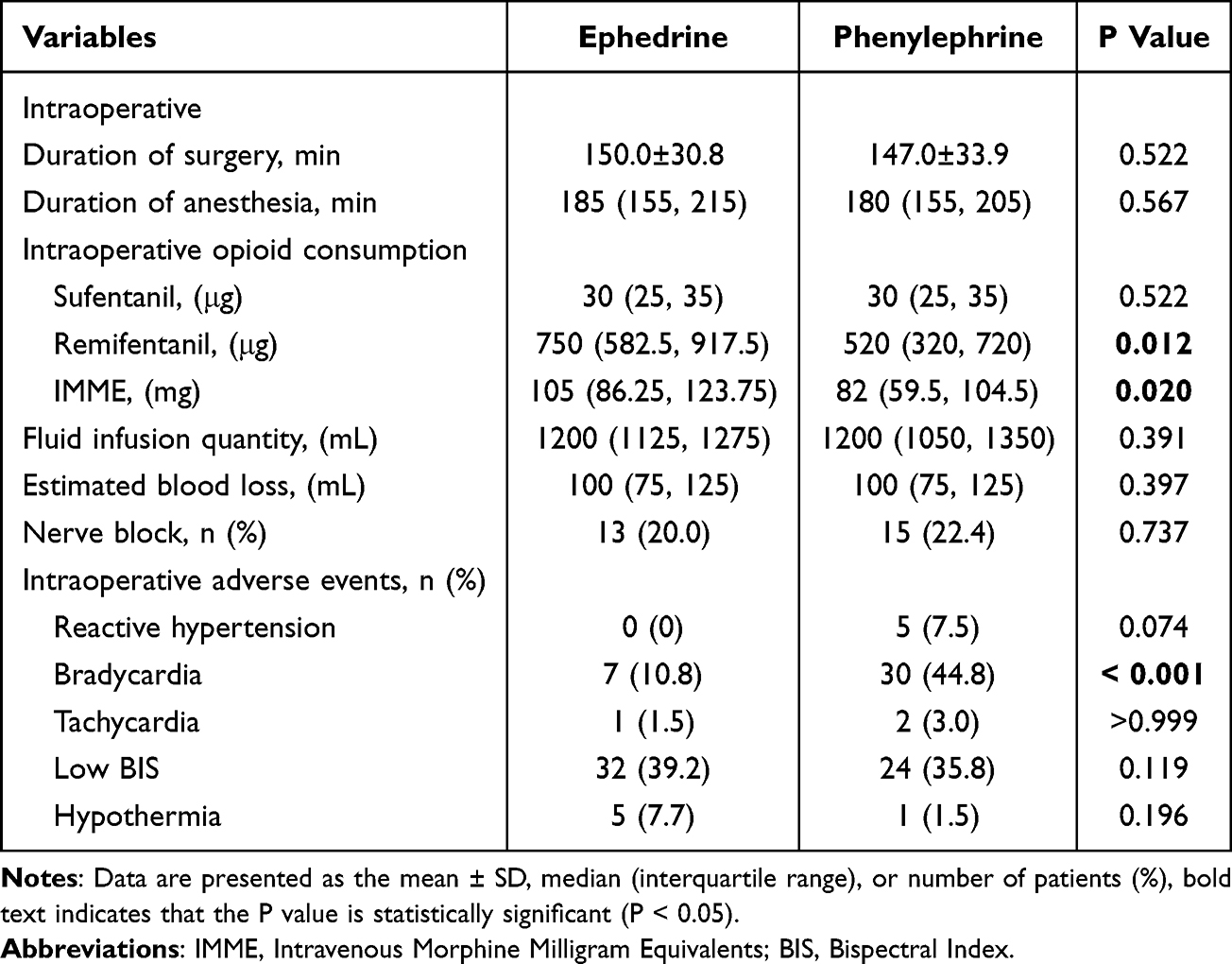 |
Table 2 Intraoperative Data of the Study Patients |
Primary Outcome
The overall incidence of POD was observed in 20 out of 132 patients (15.2%), with 5 out of 65 patients (7.7%) in Group E and 15 out of 67 patients (22.4%) in Group P (RR, 0.344; 95% CI, 0.132 to 0.891; P = 0.019) (Table 3). Survival curve analysis of the incidence of POD within three days postoperatively, using the Log rank test, further demonstrated a statistically significant difference between the two groups (HR, 0.358; P = 0.033; Figure 2). Additionally, the incidence of POD on the third postoperative day was significantly lower in Group E compared to Group P [0 vs 6 (67), P = 0.040]. However, there were no significant differences in the incidence of POD between the two groups on the first postoperative day (RR, 0.644; 95% CI, 0.222 to 1.867; P = 0.413) or the second postoperative day (RR, 0.206; 95% CI, 0.025 to 1.717; P = 0.224) (Table 3).
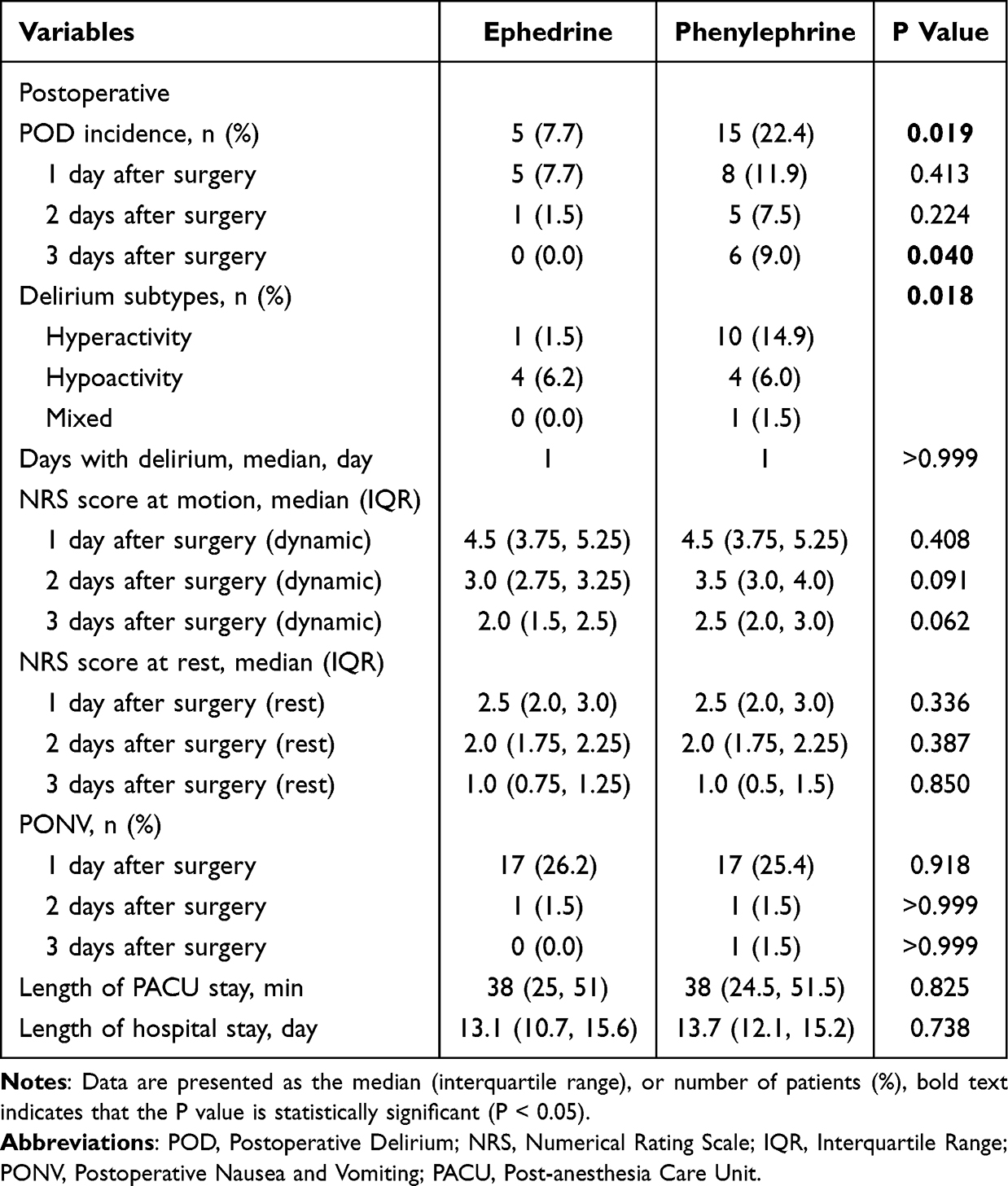 |
Table 3 Postoperative Data of the Study Patients |
 |
Figure 2 Kaplan-Meier curve showing the cumulative incidence of postoperative delirium during postoperative days 1 to 3 in Group E and Group P. Red dashed shaded area, confidence interval for Group E; Blue dashed shaded area, confidence interval for Group P. Abbreviations: Group E, the ephedrine group; Group P, the phenylephrine group; HR, hazard ratio. |
Secondary Outcome
There were significant differences in delirium subtypes between the two groups (P = 0.018). The majority of individuals in group E exhibited hypoactive delirium, while most individuals in group P displayed hyperactive delirium. However, there was no significant difference in the duration of delirium between the two groups (MD, 0; 95% CI, 0 to 0 days; P > 0.999).
In terms of patients’ intraoperative vital signs, GEE indicated no significant time-group interaction (P > 0.05). Furthermore, there were no significant intergroup differences in the temporal changes of MAP, HR, SpO2, BIS, and PetCO2 between the two groups (P > 0.05). Regarding MAP, there were no statistically significant differences in MAP at any time point between Group E and Group P (all P > 0.05). However, MAP in Group P consistently remained higher than in Group E. Specifically, at T0, MAP was 98.0 ± 8.9 mmHg in Group E and 99.8 ± 9.3 mmHg in Group P; at T1, MAP was 80.6 ± 11.2 mmHg in Group E and 83.0 ± 13.5 mmHg in Group P; at T2, MAP was 77.4 ± 10.4 mmHg in Group E and 80.3 ± 11.6 mmHg in Group P; at T3, MAP was 78.7 ± 9.7 mmHg in Group E and 79.7 ± 10.9 mmHg in Group P; at T4, MAP was 75.2 ± 9.5 mmHg in Group E and 75.7 ± 10.0 mmHg in Group P; and at T5, MAP was 80.9 ± 9.9 mmHg in Group E and 84.0 ± 12.9 mmHg in Group P. The changes in various vital signs of patients during surgery are illustrated in Figure 3.
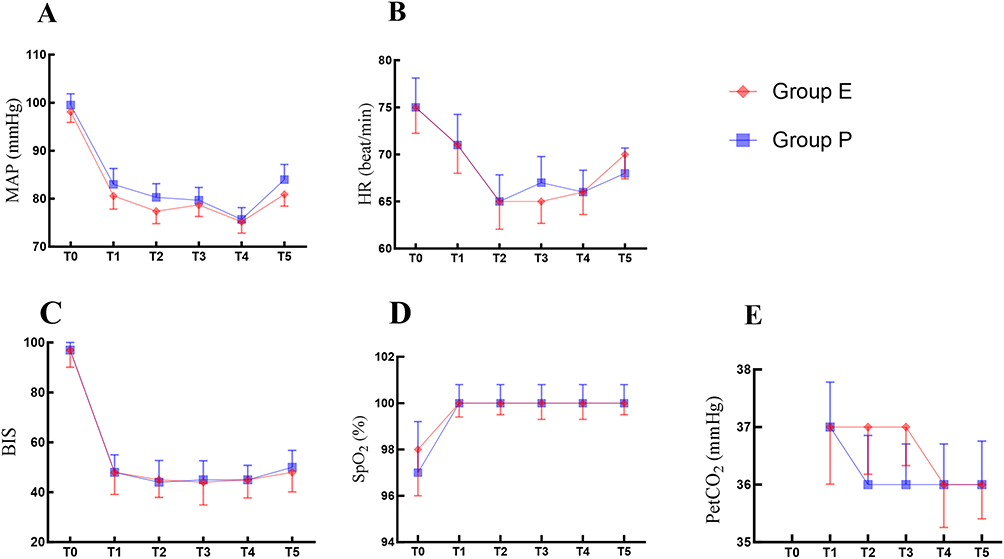 |
Figure 3 Intraoperative vital signs include (A) MAP, (B) HR, (C) BIS, (D) SpO2, (E) PetCO2. Values are expressed as means. Abbreviations: T0, at the baseline; T1, 5 minutes after intubation; T2, at the beginning of surgery; T3, 30 minutes after the start of surgery; T4, 60 minutes after the start of surgery; T5, at the end of surgery; MAP, mean arterial pressure; HR, heart rate; BIS, bispectral index; SpO2, pulse oxygen saturation; PetCO2, end-tidal CO2 pressure. |
In terms of postoperative pain, adverse events, and other relevant postoperative indicators, our findings demonstrated that there were no statistically significant differences in pain scores between the two patient groups, both at rest and during movement, within three days after surgery (P > 0.05, Table 3). Similarly, no statistically significant differences were observed in the incidence of PONV within three days postoperatively, nor in other adverse events between the two groups (P > 0.05, Table 3). Furthermore, there were no statistically significant differences in the length of stay in the PACU (MD, 0; 95% CI, −6.0 to 5.0 minutes; P = 0.825) or in the overall length of hospital stay (MD, 0.5; 95% CI, −18.1 to 7.5 hours; P = 0.825) between the two groups (Table 3).
Logistic Regression Analysis of POD-Associated Risk Factors
The results of the logistic regression analysis revealed several factors associated with the risk of POD. Ephedrine rather than phenylephrine was used to correct intraoperative hypotension during surgery (OR, 0.289; 95% CI, 0.098 to 0.849; P = 0.024). Additionally, age (OR, 1.122; 95% CI, 1.027 to 1.225; P = 0.011), the ASA classification (OR, 0.273; 95% CI, 0.075 to 0.985; P = 0.047), and the length of stay in the PACU (OR, 1.047; 95% CI, 1.024 to 1.070; P < 0.001) were identified as risk factors related to POD. The single-factor logistic regression analysis indicated that the P values for vasoactive drugs, age, sex, ASA classification, type of surgery, Mini-Cog score, nerve block, and length of stay in the PACU were all less than 0.1 (Table 4). When these factors were incorporated into the multivariate logistic regression analysis, we found that vasoactive drugs (OR, 0.173; 95% CI, 0.042 to 0.708; P = 0.015) and the length of stay in the PACU (OR, 1.050; 95% CI, 1.021 to 1.080; P = 0.001) showed significant statistical differences (Table 4).
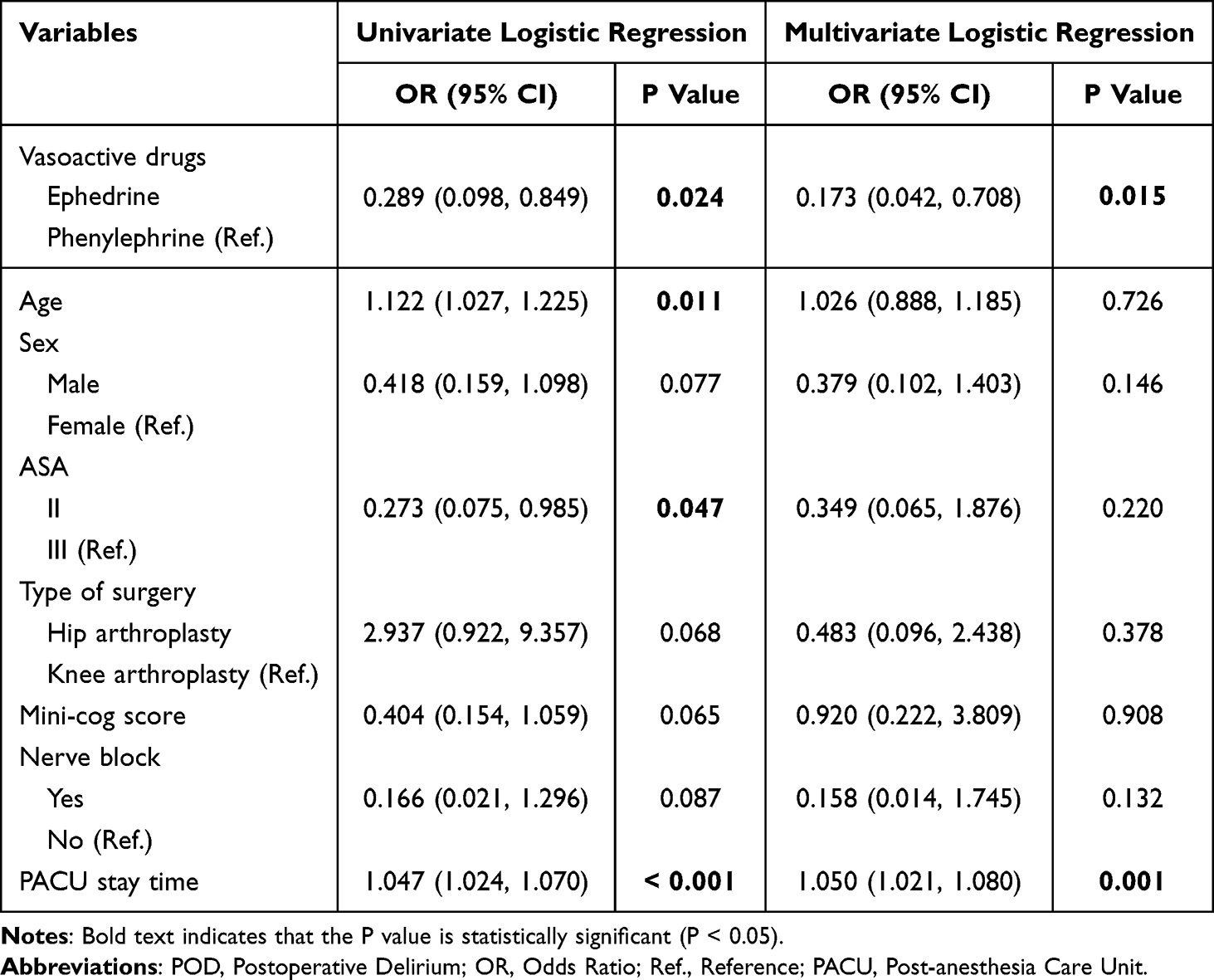 |
Table 4 Logistic Regression Analysis of Risk Factors for POD |
Subgroup Analysis
The results of the subgroup analysis indicated that in the subgroups of patients undergoing hip surgery, patients with a Mini-Cog score of 2, and patients with a PACU stay time ≥ 60 minutes or longer experienced a significantly reduced incidence of POD in Group E compared to Group P (p < 0.05). In the other subgroups, no statistically significant differences were observed in the effects on POD between the ephedrine and phenylephrine groups. However, there was no interaction among the subgroups, suggesting that the effect of ephedrine on POD was consistent across all subgroups (Figure 4).
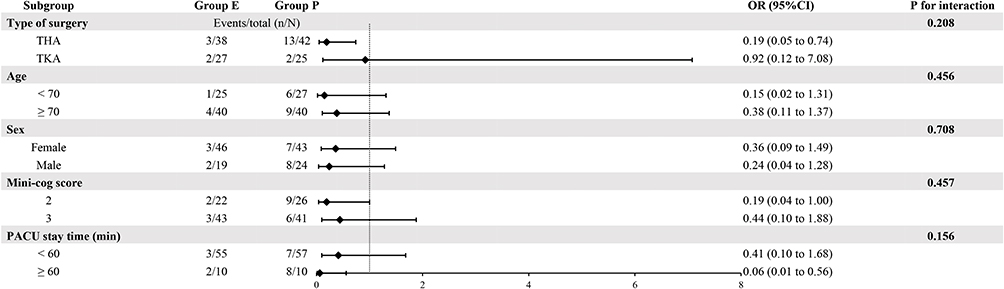 |
Figure 4 Forest plot of the subgroup analysis for the primary outcome. The interaction term is a test of whether the effect of the experimental intervention is statistically different in significance between subgroups. Abbreviations: OR, Odds Ratio; CI, Confidence Interval; THA, Total Hip Arthroplasty; TKA, total knee arthroplasty; Mini-cog, Mini-Cognitive Assessment; PACU, Post-Anesthesia Care Unit. |
Discussion
The findings of this prospective randomized controlled trial indicate that, in elderly patients undergoing hip or knee arthroplasty, the intraoperative administration of ephedrine for the management of hypotension is associated with a significantly lower incidence of POD compared to phenylephrine. Furthermore, the intraoperative use of ephedrine significantly reduces the incidence of intraoperative bradycardia when compared to phenylephrine. Additionally, results from the multivariate logistic regression analysis showed that, compared with phenylephrine, ephedrine was a protective factor against POD, whereas a prolonged length of stay in the PACU was a risk factor for POD; both factors were clearly associated with the incidence of POD. There were no statistically significant differences between the two vasoactive drugs regarding intraoperative vital signs, postoperative indicators, or the incidence of adverse events.
Notably, the lower incidence of POD in the ephedrine group supports the core hypothesis that ephedrine reduces POD risk by enhancing cerebral circulation and oxygenation. However, in our study, although Group P exhibited a slightly higher intraoperative MAP, this systemic blood pressure advantage did not reduce POD risk; in fact, Group P experienced a significantly higher incidence of POD. This paradox—higher MAP accompanied by increased POD risk—is corroborated by recent hemodynamic studies identifying 65 mmHg as the critical MAP threshold for preventing intraoperative organ injury.33 Prolonged exposure below this threshold doubles the risk of complications, while higher pressures confer no additional benefit. Collectively, these findings demonstrate that a higher MAP does not necessarily equate to optimal cerebral circulation and oxygenation, particularly in elderly orthopedic patients who may have impaired cerebral autoregulation due to age-related vascular changes or comorbidities. This evidence reinforces the proposed mechanism that ephedrine’s POD-lowering effect may not depend solely on elevating systemic blood pressure but rather on optimizing cerebral perfusion through mechanisms independent of global hemodynamic elevation.
A retrospective multicenter study first confirmed associations between the choice of intraoperative vasoactive drugs and POD, as well as a dose-dependent relationship between phenylephrine and POD risk.27 Consistent with Ma’s research, our study found that phenylephrine was associated with a higher risk of delirium despite marginally higher MAP compared to ephedrine; however, we observed no dose-response relationship, potentially due to the administration of lower doses. Ma’s study reported an increased risk of delirium associated with phenylephrine doses exceeding their median of 12.4 μg/kg (OR = 1.21) in a cohort with a median BMI of 28—corresponding to an absolute dose range of 838–1,064 μg for adults of typical height (155–175 cm). In contrast, our median intraoperative dose was only 200 μg, which is well below this range. This discrepancy likely explains the absence of a dose-effect relationship in our study: our 200 μg dose may not have reached the threshold necessary to detect an association with POD.
Previous studies have demonstrated that ephedrine and phenylephrine exert differential effects on POD, which may be attributed to their varying impacts on cerebral circulation and oxygenation.34,35 Phenylephrine, a selective α-adrenergic receptor agonist, effectively increases MAP. However, it may also reduce CO due to reflex bradycardia and decrease cerebral blood flow by constricting cerebral blood vessels through sympathetic nerve activity in the carotid ganglia.36,37 These two factors collectively contribute to a reduction in SctO2, thereby increasing the risk of ischemic brain injury and increases the incidence of delirium.38,39 Nevertheless, this mechanism remains a subject of debate.40–42 For instance, a study by Li’s study demonstrated that both ephedrine and phenylephrine can effectively increase MAP and middle cerebral artery flow velocity; furthermore, mixed linear model analysis indicated no statistically significant difference between the two drugs regarding SctO2 and the cerebral oxygen index. Other studies have suggested that the relationship between SctO2 and POD is also contentious.43,44 Unfortunately, due to limitations in monitoring equipment, this study was unable to assess indicators such as cerebral perfusion and SctO2. Nonetheless, our research findings further support the view that ephedrine offers more advantages than phenylephrine in correcting intraoperative hypotension in elderly patients, as it reduces the risk of POD.
In addition to its role in improving cerebral perfusion and oxygenation, the neuroprotective properties of ephedrine may also significantly contribute to its effectiveness in reducing POD. In a rat study, ephedrine was identified as a potential anti-inflammatory agent that can significantly diminish brain inflammatory responses through the NF-κB signaling pathway and effectively mitigate cerebral ischemia-reperfusion injury.45 Furthermore, an analysis employing a comprehensive bioinformatics approach based on multi-omics networks suggests that the anti-inflammatory, central nervous system-stimulating, and neuroprotective properties of ephedrine may play a crucial role in the treatment of delirium.46 These studies indicate that the mechanism by which ephedrine reduces POD extends beyond merely improving cerebral perfusion and oxygenation; its inherent neuroprotective properties also contribute significantly. However, the specific mechanisms involved require further validation through relevant pharmacological studies.
Secondary endpoints with significant differences also provide valuable insights for selecting clinical vasoactive drugs. First, the incidence of intraoperative bradycardia was significantly lower in the ephedrine group compared to the phenylephrine group, consistent with findings from previous studies.47,48 This suggests that ephedrine may be a more appropriate vasoactive agent for elderly patients with preoperative bradycardia or impaired heart rate regulation. Second, although the ephedrine group received a significantly higher dose of IMME, this did not increase the incidence of POD; in fact, Group E exhibited a lower risk of POD. No significant differences were observed between groups in postoperative pain scores, duration of PACU stay, or incidence of PONV. Previous research has confirmed that increased opioid use is associated with a heightened risk of POD.4,49 However, other studies have shown no significant association between opioid use and POD when doses are adjusted to achieve effective pain control.10,50 In our study, the similar postoperative pain control and recovery observed between groups confirm the clinical appropriateness of opioid use in Group E. Moreover, the lower incidence of POD in this group further supports the hypothesis that ephedrine’s neuroprotective effects may counteract the potential POD-inducing effects of opioids. These findings suggest that the relationship between opioids and POD is not absolute and may be modulated by perioperative interventions, such as ephedrine, which target pathways involved in POD development. Future studies should further elucidate the synergistic mechanisms between ephedrine and opioids to provide a theoretical basis for optimizing perioperative analgesic strategies.
Our subgroup analysis revealed that hip surgery patients with a Mini-Cog score of 2 and a PACU stay of 60 minutes or longer had a significantly lower risk of POD in Group E compared to Group P (p < 0.05). The clinical implications of this finding warrant further discussion. This subgroup is inherently at high risk for POD: hip surgery—often performed in elderly patients, as indicated by our baseline data—involves perioperative factors such as bone cement use and hemodynamic fluctuations that can impair cognition through inflammation or altered cerebral perfusion.51,52 A Mini-Cog score of 2 indicates mild cognitive impairment prior to surgery, which increases the likelihood of patients developing POD.53 Additionally, prolonged PACU stay may indicate complications such as delayed emergence or hemodynamic instability, which can exacerbate neuroinflammation and increase POD risk. Clinically, these findings are consistent with the pharmacological profile of ephedrine: its α- and β-adrenergic agonist effects stabilize intraoperative blood pressure and reduce cerebral perfusion fluctuations, potentially providing enhanced neuroprotection for this subgroup.22,27 This suggests that ephedrine could serve as a targeted strategy to reduce POD risk in these patients. However, as these are exploratory subgroup results, they should be interpreted with caution.
Although this study demonstrates the advantages of ephedrine in reducing POD among elderly patients undergoing lower extremity joint replacement, it has several limitations. Firstly, critical intraoperative indicators such as SctO2 and CO were not monitored. These parameters are closely linked to cerebral perfusion and oxygenation, which are central to the hypothesis of this study. The absence of such data prevents verification of whether the benefits of ephedrine are achieved by maintaining cerebral oxygen balance, thereby weakening the robustness of mechanistic validation. Future studies should incorporate real-time monitoring of SctO2 and CO to elucidate the relevant pathways of action. Secondly, the postoperative follow-up period was limited to just three days, in contrast to some studies that employed a one-week follow-up. This shorter duration may have resulted in missed cases of delirium occurring later. Although delirium primarily manifests on postoperative days 1 to 3, the potential bias introduced by this relatively brief follow-up period cannot be excluded.54 Thirdly, this study employed a hypotension event-triggered dosing approach, which differs from methodologies used in previous research, such as continuous intravenous infusion protocols. This discrepancy may reduce the comparability of results and obscure the potential dose-effect relationship of phenylephrine. Standardizing dosing protocols in future studies will help improve the reliability of the findings. Finally, the single-blind design of this study presents a notable limitation. Because anesthesiologists were directly responsible for administering trial-related drugs and managing patients during surgery, their awareness of group allocation could introduce bias in drug dosage adjustments and intraoperative intervention decisions. This potential bias may compromise the objectivity of evaluating key outcomes such as drug efficacy and intraoperative safety. Therefore, readers should consider the possible influence of these intraoperative variables when interpreting our findings. These limitations may induce some bias in the results of this study.
Conclusions
In conclusion, compared to phenylephrine, ephedrine used to correct intraoperative hypotension significantly reduces the incidence of POD within three days in elderly patients undergoing total hip or knee arthroplasty (overall incidence: 15.2%; ephedrine group: 7.7% vs phenylephrine group: 22.4%; RR, 0.344, 95% CI, 0.132–0.891, P = 0.019). Subgroup analysis indicates that ephedrine’s protective effect is more pronounced in patients undergoing hip surgery, those with a Mini-Cog score of 2, and patients with a PACU stay of 60 minutes or longer. Clinically, ephedrine may be preferred for managing intraoperative hypotension in these elderly arthroplasty patients—particularly in the high-benefit subgroups—to reduce the risk of early POD. However, the mechanism by which ephedrine alleviates POD remains unclear and warrants further pharmacological investigation. Additionally, its long-term efficacy and generalizability require validation through multicenter studies.
Data Sharing Statement
The original data analyzed in this study are included in the article; data supporting the findings of this study are available from corresponding author (Guan-Yu Chen) upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Medical Ethics Committee of the Zigong Fourth People’s Hospital (Ethical approval number: EC-2024-084) and conducted following the Helsinki Declaration. The trial was also registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn/) with the registration identifier ChiCTR2400088799 on August 27, 2022. This study was conducted at the Zigong Fourth People’s Hospital and written informed consent was obtained from all participants or their legal representatives before enrolment in this trial. The study protocol followed the CONSORT guidelines.
Acknowledgments
We sincerely thank our colleagues from the Department of Anesthesiology at Zigong Fourth People’s Hospital for their assistance in collecting clinical trial data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Key Science and Technology Plan of Zigong City (Collaborative Innovation Category of Zigong Integrated Traditional Chinese and Western Medicine Research Institute) (2023ZXYXT07), Zigong Key Science and Technology Program - Zigong Academy for Medical Big Data and Artificial Intelligence Joint Project(2022ZCYGY10).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Zhao J, Liang G, Hong K. et al. Risk factors for postoperative delirium following total Hip or knee arthroplasty: a meta-analysis. Front Psychol. 2022;13:993136. doi:10.3389/fpsyg.2022.993136
2. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. doi:10.1016/s0140-6736(13)60688-1
3. Mattison MLP. Delirium. Ann Internal Med. 2020;173(7):Itc49–itc64. doi:10.7326/aitc202010060
4. Jin Z, Hu J, Ma D. Postoperative delirium: perioperative assessment, risk reduction, and management. Br J Anaesth. 2020;125(4):492–504. doi:10.1016/j.bja.2020.06.063
5. Leslie DL, Marcantonio ER, Zhang Y, Leo-Summers L, Inouye SK. One-year health care costs associated with delirium in the elderly population. Archives of Internal Medicine. 2008;168(1):27–32. doi:10.1001/archinternmed.2007.4
6. Hshieh TT, Inouye SK, Oh ES. Delirium in the Elderly. Psychiatric Clinics of North America. 2018;41(1):1–17. doi:10.1016/j.psc.2017.10.001
7. Saczynski JS, Marcantonio ER, Quach L, et al. Cognitive trajectories after postoperative delirium. New Engl J Med. 2012;367(1):30–39. doi:10.1056/NEJMoa1112923
8. Sprung J, Roberts RO, Weingarten TN, et al. Postoperative delirium in elderly patients is associated with subsequent cognitive impairment. Br J Anaesth. 2017;119(2):316–323. doi:10.1093/bja/aex130
9. Iglseder B, Frühwald T, Jagsch C. Delirium in geriatric patients. Wiener medizinische Wochenschrift. 2022;172(5–6):114–121. doi:10.1007/s10354-021-00904-z
10. Swarbrick CJ, Partridge JSL. Evidence-based strategies to reduce the incidence of postoperative delirium: a narrative review. Anaesthesia. 2022;77(S1):92–101. doi:10.1111/anae.15607
11. Duan W, Zhou C-M, Yang -J-J, et al. A long duration of intraoperative hypotension is associated with postoperative delirium occurrence following thoracic and orthopedic surgery in elderly. J Anesthesia. 2023;88:111125. doi:10.1016/j.jclinane.2023.111125
12. Wachtendorf LJ, Azimaraghi O, Santer P, et al. Association Between Intraoperative Arterial Hypotension and Postoperative Delirium After Noncardiac Surgery: a Retrospective Multicenter Cohort Study. Anesthesia Analg. 2022;134(4):822–833. doi:10.1213/ane.0000000000005739
13. Scholz AF, Oldroyd C, McCarthy K, Quinn TJ, Hewitt J. Systematic review and meta-analysis of risk factors for postoperative delirium among older patients undergoing gastrointestinal surgery. Journal of British Surgery. 2016;103(2):e21–8. doi:10.1002/bjs.10062
14. Maheshwari K, Ahuja S, Khanna AK, et al. Association Between Perioperative Hypotension and Delirium in Postoperative Critically Ill Patients: a Retrospective Cohort Analysis. Anesthesia Analg. 2020;130(3):636–643. doi:10.1213/ane.0000000000004517
15. Wang X, Feng K, Liu H, et al. Regional cerebral oxygen saturation and postoperative delirium in endovascular surgery: a prospective cohort study. Trials. 2019;20(1):504. doi:10.1186/s13063-019-3586-y
16. Czok M, Pluta MP, Putowski Z, Ł J K. Postoperative Neurocognitive Disorders in Cardiac Surgery: investigating the Role of Intraoperative Hypotension. A Systematic Review. Int J Environ Res Public Health. 2021;18(2):786. doi:10.3390/ijerph18020786
17. Li W, Shi Q, Bai R, et al. Advances in research on the pathogenesis and signaling pathways associated with postoperative delirium (Review). Molecular Medicine Reports. 2025;32(2):13585. doi:10.3892/mmr.2025.13585
18. Hall MJ, DeFrances CJ, Williams SN, Golosinskiy A, Schwartzman A. National Hospital Discharge Survey: 2007 summary. National Health Statistics Reports. 2010;2010(29):1–20.
19. Südfeld S, Brechnitz S, Wagner JY, et al. Post-induction hypotension and early intraoperative hypotension associated with general anaesthesia. Br J Anaesth. 2017;119(1):57–64. doi:10.1093/bja/aex127
20. Liu Y, Zhang Y, Wang A, et al. Efficacy of the inferior vena cava collapsibility index in predicting anaesthesia-induced hypotension in elderly patients undergoing Hip arthroplasty. Sci Rep. 2024;14(1):27156. doi:10.1038/s41598-024-78718-3
21. Nissen P, Brassard P, Jørgensen TB, Secher NH. Phenylephrine but not ephedrine reduces frontal lobe oxygenation following anesthesia-induced hypotension. Neurocritical Care. 2010;12(1):17–23. doi:10.1007/s12028-009-9313-x
22. Aliane J, Dualé C, Guesmi N, et al. Compared effects on cerebral oxygenation of ephedrine vs phenylephrine to treat hypotension during carotid endarterectomy. Clin Exp Pharmacol Physiol. 2017;44(7):739–748. doi:10.1111/1440-1681.12759
23. Larson S, Anderson L, Thomson S. Effect of phenylephrine on cerebral oxygen saturation and cardiac output in adults when used to treat intraoperative hypotension: a systematic review. JBI Evidence Synth. 2021;19(1):34–58. doi:10.11124/jbisrir-d-19-00352
24. Koch KU, Mikkelsen IK, Espelund US, et al. Cerebral Macro- and Microcirculation during Ephedrine versus Phenylephrine Treatment in Anesthetized Brain Tumor Patients: a Randomized Clinical Trial Using Magnetic Resonance Imaging. Anesthesiology. 2021;135(5):788–803. doi:10.1097/aln.0000000000003877
25. Lu Y, Di M, Li C, Chen M, Yuan K, Shangguan W. Comparing the response of pulse oximetry and regional cerebral oxygen saturation to hypoxia in preschool children. Exp Ther Med. 2020;19(1):353–358. doi:10.3892/etm.2019.8199
26. Ahrens E, Tartler TM, Suleiman A, et al. Dose-dependent relationship between intra-procedural hypoxaemia or hypocapnia and postoperative delirium in older patients. Br J Anaesth. 2023;130(2):e298–e306. doi:10.1016/j.bja.2022.08.032
27. Ma H, Ahrens E, Wachtendorf LJ, et al. Intraoperative Use of Phenylephrine versus Ephedrine and Postoperative Delirium: a Multicenter Retrospective Cohort Study. Anesthesiology. 2024;140(4):657–667. doi:10.1097/aln.0000000000004774
28. Weinberg L, Li SY, Louis M, et al. Reported definitions of intraoperative hypotension in adults undergoing non-cardiac surgery under general anaesthesia: a review. BMC Anesthesiol. 2022;22(1):69. doi:10.1186/s12871-022-01605-9
29. Wesselink EM, Kappen TH, van Klei WA, Dieleman JM, van Dijk D, Slooter AJ. Intraoperative hypotension and delirium after on-pump cardiac surgery. Br J Anaesth. 2015;115(3):427–433. doi:10.1093/bja/aev256
30. Langer T, Santini A, Zadek F, et al. Intraoperative hypotension is not associated with postoperative cognitive dysfunction in elderly patients undergoing general anesthesia for surgery: results of a randomized controlled pilot trial. J Anesthesia. 2019;52:111–118. doi:10.1016/j.jclinane.2018.09.021
31. Saravanan S, Kocarev M, Wilson RC, Watkins E, Columb MO, Lyons G. Equivalent dose of ephedrine and phenylephrine in the prevention of post-spinal hypotension in Caesarean section. Br J Anaesth. 2006;96(1):95–99. doi:10.1093/bja/aei265
32. Nielsen S, Degenhardt L, Hoban B, Gisev N. A synthesis of oral morphine equivalents (OME) for opioid utilisation studies. Pharmacoepidemiol Drug Saf. 2016;25(6):733–737. doi:10.1002/pds.3945
33. Zhao B, Zhang J, Xie Y, et al. Intensive vs Conventional Intraoperative Blood Pressure Management on Cardiovascular Events After Major Abdominal Surgery: the BP-CARES Randomized Trial. J Am College Cardiol. 2025;86(12):892–906. doi:10.1016/j.jacc.2025.07.027
34. Meng L, Cannesson M, Alexander BS, et al. Effect of phenylephrine and ephedrine bolus treatment on cerebral oxygenation in anaesthetized patients. Br J Anaesth. 2011;107(2):209–217. doi:10.1093/bja/aer150
35. Zheng C, Wang B, Fu J, Peng H, Chen Y, Hu X. Effect of phenylephrine versus ephedrine on the incidence of postoperative delirium in olderly adults undergoing knee arthroplasty under general anesthesia: a single-center trial. Sci Rep. 2024;14(1):17333. doi:10.1038/s41598-024-68273-2
36. Cassaglia PA, Griffiths RI, Walker AM. Sympathetic nerve activity in the superior cervical ganglia increases in response to imposed increases in arterial pressure. Am J Physiol Regulatory Integr Comp Physiol. 2008;294(4):R1255–61. doi:10.1152/ajpregu.00332.2007
37. Orbach-Zinger S, Bizman I, Firman S, et al. Perioperative noninvasive cardiac output monitoring in parturients undergoing cesarean delivery with spinal anesthesia and prophylactic phenylephrine drip: a prospective observational cohort study. J Matern Fetal Neonatal Med. 2019;32(19):3153–3159. doi:10.1080/14767058.2018.1458835
38. Slater JP, Guarino T, Stack J, et al. Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg. 2009;87(1):36–44. doi:10.1016/j.athoracsur.2008.08.070
39. Kim J, Shim JK, Song JW, Kim EK, Kwak YL. Postoperative Cognitive Dysfunction and the Change of Regional Cerebral Oxygen Saturation in Elderly Patients Undergoing Spinal Surgery. Anesthesia Analg. 2016;123(2):436–444. doi:10.1213/ane.0000000000001352
40. Li X, Zheng Y, Zhang J. Cerebral oxygenation and hemodynamic changes during ephedrine and phenylephrine administration for transient intraoperative hypotension in patients undergoing major abdominal surgery: a randomized controlled trial. BMC Anesthesiol. 2025;25(1):87. doi:10.1186/s12871-025-02944-z
41. Pedersen SS, Meyhoff CS, Olsen MH, et al. Impact of hyperoxia and phenylephrine on cerebral oxygenation: an experimental clinical study. Acta anaesthesiologica Scandinavica. 2023;67(1):57–65. doi:10.1111/aas.14149
42. Rasmussen M, Koch KU, Espelund US, et al. Blood-brain Barrier Permeability May Influence Vasopressor Effects in Anesthetized Patients With Brain Tumor: an Analysis of Magnetic Resonance Imaging Data. J Nurosurg Anesthesiol. 2024;36(4):357–362. doi:10.1097/ana.0000000000000948
43. Kahn RA, Egorova N, Ouyang Y, et al. Perioperative Near Infrared Spectroscopy Measurements of Cerebral Regional Oxygen Desaturations Are Not Associated With Delirium After Cardiac Surgery. J Cardiothoracic Vascular Anesthesia. 2025;39(5):1153–1161. doi:10.1053/j.jvca.2025.01.034
44. Qiu L, Ma Y, Ge L, Zhou H, Jia W. Efficacy of Cerebral Oxygen Saturation Monitoring for Perioperative Neurocognitive Disorder in Adult Noncardiac Surgical Patients: a Systematic Review and Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 2025;194:123570. doi:10.1016/j.wneu.2024.123570
45. Shi C, Li J, Li J. Ephedrine attenuates cerebral ischemia/reperfusion injury in rats through NF-κB signaling pathway. Hum Exp Toxicol. 2021;40(6):994–1002. doi:10.1177/0960327120975456
46. Mosharaf MP, Alam K, Gow J, Mahumud RA. Exploration of key drug target proteins highlighting their related regulatory molecules, functional pathways and drug candidates associated with delirium: evidence from meta-data analyses. BMC Geriatr. 2023;23(1):767. doi:10.1186/s12877-023-04457-1
47. Ibrahim SS, Patil B. A Comparative Study of Infusion of Ephedrine and Phenylephrine on Hemodynamic Stability After Spinal Anesthesia in Elderly Patients Undergoing Lower Limb Orthopedic Surgeries. Cureus. 2024;16(9):e69977. doi:10.7759/cureus.69977
48. Zhang Y, Jin L, Liu H, Meng X, Ji F. Ephedrine vs. phenylephrine effect on sublingual microcirculation in elderly patients undergoing laparoscopic rectal cancer surgery. Front Med. 2022;9:969654. doi:10.3389/fmed.2022.969654
49. Laferrière-Langlois P, Morisson L, Jeffries S, Duclos C, Espitalier F, Richebé P. Depth of Anesthesia and Nociception Monitoring: current State and Vision For 2050. Anesthesia Analg. 2024;138(2):295–307. doi:10.1213/ane.0000000000006860
50. Leong AY, Edginton S, Lee LA, et al. The association between pain, analgesia, and delirium among critically ill adults: a systematic review and meta-analysis. Intensive Care Med. 2025;51(2):342–352. doi:10.1007/s00134-025-07784-6
51. Zhou Q, Zhou X, Zhang Y, et al. Predictors of postoperative delirium in elderly patients following total Hip and knee arthroplasty: a systematic review and meta-analysis. BMC Musculoskeletal Disorders. 2021;22(1):945. doi:10.1186/s12891-021-04825-1
52. Zhang G, Wang Z, Wang D, Jia Q, Zeng Y. A systematic review and meta-analysis of the correlation between operation time and postoperative delirium in total Hip arthroplasty. Ann Palliative Medi. 2021;10(10):10459–10466. doi:10.21037/apm-21-2190
53. Varpaei HA, Robbins LB, Farhadi K, Bender CM. Preoperative cognitive function as a risk factor of postoperative delirium in cancer surgeries: a systematic review and meta-analysis. J Surg Oncol. 2024;130(2):222–240. doi:10.1002/jso.27730
54. Scott JE, Mathias JL, Kneebone AC. Incidence of delirium following total joint replacement in older adults: a meta-analysis. General Hospital Psychiatry. 2015;37(3):223–229. doi:10.1016/j.genhosppsych.2015.02.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Intraoperative Sleep Spindle Activity and Postoperative Sleep Disturbance in Elderly Patients Undergoing Orthopedic Surgery: A Prospective Cohort Study
Dai Y, Shi K, Liu Q, Shen C, Lu X, Qiu X, Sun J
Nature and Science of Sleep 2024, 16:2083-2097
Published Date: 17 December 2024