Back to Journals » International Journal of General Medicine » Volume 17
Effect of Electronic Moxibustion in Patients with IDH: A Randomized Crossover Pilot Study
Authors Liu TJ, Pan HC, Lee CC, Chen CY, Wu IW, Sun CY, Chen KS, Hsu HJ ![]() , Chen YT, Hsu CK, Yeh YC
, Chen YT, Hsu CK, Yeh YC ![]()
Received 12 August 2024
Accepted for publication 19 November 2024
Published 4 December 2024 Volume 2024:17 Pages 5793—5805
DOI https://doi.org/10.2147/IJGM.S481418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Franco Musio
Tai-Jan Liu,1,2 Heng-Chih Pan,3– 6 Chin-Chan Lee,3,4,6 Chun-Yu Chen,3,4,6 I-Wen Wu,3,7,8 Chiao-Yin Sun,3,4 Kuo-Su Chen,3,4 Heng-Jung Hsu,3,4,6 Yih-Ting Chen,3,4 Cheng-Kai Hsu,3,4 Yuan-Chieh Yeh1,9
1Department of Traditional Chinese Medicine, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan; 2Department of Traditional Chinese Medicine, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan; 3Division of Nephrology, Department of Internal Medicine, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan; 4Chang Gung University College of Medicine, Taoyuan, Taiwan; 5Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan; 6Community Medicine Research Center, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan; 7Division of Nephrology, Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 8Division of Nephrology, Department of Internal Medicine, Taipei Medical University Hospital, Taipei, Taiwan; 9Program in Molecular Medicine, College of Life Sciences, National Yang Ming Chiao Tung University, Taipei, Taiwan
Correspondence: Yuan-Chieh Yeh, Department of Traditional Chinese Medicine, Keelung Chang Gung Memorial Hospital, No. 222, Maijin Road, Anle Dist, Keelung, Taipei, Taiwan, Tel +886975362713, Fax +886224313161, Email [email protected]
Objective: Intradialytic hypotension (IDH), a common complication of hemodialysis (HD), is associated with increased cardiovascular risk, morbidity, and mortality. Fatigue is one of the most frequent symptoms of IDH, and deteriorates the quality of life of patients. This study aimed to evaluate the efficacy and safety of electronic moxibustion for improving IDH and its associated symptoms.
Methods: We prospectively recruited 32 end-stage renal disease patients with IDH who underwent regular HD at our hospital’s dialysis center between April 2019 and April 2020. A randomized, controlled, two-arm crossover trial was performed to evaluate the efficacy of adding one-hour electronic moxibustion during HD. The outcome measurements included patients’ subjective assessment of the degree of fatigue, recovery time of fatigue from HD, cold intolerance before and after each intervention, frequency of IDH episodes and nursing interventions needed during HD, and blood pressure changes during HD.
Results: Thirty (94%) patients completed the study. Intervention with electronic moxibustion improved the degree of fatigue (95% CI, − 2.95 to − 0.18, p = 0.027), specifically in patients prescribed with midodrine (95% CI, − 4.20 to − 0.53, p = 0.013). The short-term use of electronic moxibustion during HD did not significantly alter the frequency of IDH or reduce the degree of decrease in blood pressure. Serious adverse effects were not observed. One patient complained of heat, whereas two patients had local transient erythema and pruritus.
Conclusion: Electronic moxibustion appears to be safe and efficacious for improving IDH-related fatigue, thus acting as an adjuvant therapy in HD units to enhance patient comfort and treatment adherence. Further studies with larger sample sizes are required to confirm the benefits of this novel technique.
Plain Language Summary: Intradialytic hypotension (IDH) during hemodialysis is linked to increased mortality, often results in fatigue, and reduces the patients’ quality of life. This study assessed the effectiveness of electronic moxibustion, an infrared device that mimics traditional moxibustion, in alleviating fatigue in IDH patients. In a 4-week randomized controlled crossover trial, patients underwent 12 sessions of electronic moxibustion at acupoint CV4 during hemodialysis. While the treatment notably improved fatigue, especially in patients on regular midodrine, it did not significantly affect IDH frequency or blood pressure drop. No major adverse events were reported. This pioneering study evaluated this device for IDH-related fatigue and offered insights for future research on its potential to stabilize blood pressure.
Keywords: cross-over studies, moxibustion, fatigue, renal dialysis
Graphical Abstract:

Introduction
Intradialytic hypotension (IDH) occurs in approximately 10–12% of patients receiving hemodialysis (HD).1 The features of IDH include a considerable symptom burden, end-organ ischemia, underdialysis, vascular access thrombosis, and mortality.2–5 The pathogenesis of IDH is multifactorial and is associated with intravascular hypovolemia, impaired vascular resistance, and reduced cardiovascular reserve.1,6 The risk factors include older age, female sex, longer dialysis vintage, and several medical diseases.7,8 Moreover, it can lead to dialysis inadequacy, as patients often shorten treatments owing to associated symptoms such as muscle cramps, pruritus, nausea, and fatigue, which can be debilitating.7,9,10 The prevalence of intradialytic fatigue ranges from 60% to 97%,11–14 and in HD patients, it has been associated with lower quality of life15–17 and survival rates.18 A self-reported questionnaire interviewing weekly HD patients revealed that the most common symptoms were fatigue (62%) and low blood pressure (BP) (42%).10
Frequent assessment of dry weight, modification of dialysate composition and temperature, and increased dialysis time and frequency can reduce the incidence of IDH. Antihypertensive medications may be discontinued before dialysis. Moreover, the administration of a predialysis dose of the alpha agonist midodrine 30 minutes prior to dialysis initiation can be used off-label for the prevention of IDH.19 However, complete prevention of IDH is unlikely, given the intermittent nature of dialysis therapy. In addition, current interventions are reactive, relying on rapid nursing assessment and management, thus posing a burden to nursing care. Immediate management of IDH includes repositioning patients to optimize hemoperfusion of vital organs (supine or Trendelenburg position), cessation of ultrafiltration, fluid resuscitation, albumin supplementation, and cessation of dialysis.7,20–22 Although these interventions are necessary and beneficial, they may not prevent the adverse consequences of IDH events. Therefore, it remains necessary to seek novel, effective, and safe interventions.
According to the theory of traditional Chinese medicine (TCM), moxibustion, an external treatment, can dredge meridians and regulate qi-blood. Traditional moxibustion involves burning herbal preparations containing Artemisia argyi (mugwort) on or above the skin at the acupuncture points. The leaves of mugwort, in Chinese called ai ye, are the main material used for moxibustion. Mugwort is considered to be warm, acidic and bitter. It has the ability to warm the body’s meridians, thereby promoting better circulation. TCM considers chronic fatigue to be the result of an unbalanced state among internal organs, or a deficient vital energy (called Qi) condition with characteristic blood symptoms. Previous research on moxibustion and acupressure has found beneficial results in chronic fatigue syndrome, cancer-related fatigue, and fatigue in patients with end-stage renal disease patients.23–28 Another study suggested that moxibustion might modulate the autonomic nervous system, thus improving fatigue.24 Indirect moxibustion on CV4 and CV8 has been shown to improve chronic fatigue and its effect may be due to the antioxidant properties of moxibustion.23 CV4 belongs to the Conception Vessel and has connections with three Yin meridians as well as internal organs. A previous study utilizing herbal acupoint, a type of modified moxibustion therapy, had beneficial effects on improving the frequency of IDH and fatigue recovery.29
However, traditional moxibustion is not entirely risk-free, with potential adverse events such as allergies, burns and infection.30 Moxibustion with moxa burner seems safe with less adverse effects but may be more skill-dependent.31 Some studies have found that the smoke of moxa contains a variety of complex components, and previous research reported some anti-inflammatory effects through nitric oxide production,32 but smoke may also be harmful to the human body, such as causing allergic reactions.33 Research has been carried out to evaluate the efficacy of conventional moxibustion and smokeless moxibustion.34 To date, no study has evaluated the effectiveness of traditional moxibustion therapy during HD. Herbal acupoint therapy may be effective in improving the frequency of IDH and fatigue recovery; however, it may also cause local erythema and pruritus.29 Moreover, the thermal and radiation effects of traditional moxibustion are difficult to quantify. A modern, precise, microchip-controlled device can help solve this issue. The objective of this study was to determine whether infrared (IR) electronic moxibustion with a controlled temperature of 56 ± 8 °C, mimicking traditional moxibustion, offers any benefits for the prevention of IDH-related symptoms or complications. A randomized controlled trial was designed for this study.
Material and Methods
This two-period, randomized, controlled, two-arm crossover pilot study was conducted at the dialysis center of Keelung Chang Gung Memorial Hospital, Taiwan, from April 2019 to April 2020. The crossover design is used to reduce the influence of confounding covariates, since patients on ESRD often have multiple comorbidities and parallel controls may be hard to balance in randomized trials. The study protocol was approved by the Institutional Review Board of Chang Gung Memorial Hospital (IRB no. 201801853A3), registered at ClinicalTrials.gov (NCT03856151) and conducted following the Declaration of Helsinki. All patients provided written informed consent before participation.
Study Participants
Patients were recruited from outpatient HD units and their IDH diagnoses were confirmed by certified nephrologists. IDH was defined as (1) KDOQI criteria: a decrease in systolic blood pressure (SBP) ≥ 20 mmHg or a decrease in mean arterial pressure (MAP) ≥ 10 mmHg with accompanying symptoms (dizziness, cramps, or fatigue), according to the Kidney Disease Outcomes Quality Initiative (KDOQI) of the National Kidney Foundation for IDH; (2) NADIR criteria: intradialytic nadir SBP less than 90 mmHg; or (3) regular prescription of midodrine.7,21
Participants who were (1) aged 20–80 years, (2) on thrice-weekly HD with a dialysis time of at least 180 minutes, and (3) had IDH in at least 15% of their dialysis sessions during the past 8 weeks or regular administration of midodrine were included. Participants were excluded if they had (1) severe comorbidities, including cirrhosis, heart failure, and autoimmune diseases; (2) active malignancy; (3) insensitivity to heat or inability to effectively express themselves in heated situations; (4) pregnancy or lactation; (5) undergoing other types of alternative treatments, including Chinese medicine and regional remedies; or (6) were unable to fill out questionnaires.
Sample Size Calculation
This study used a preliminary, open-label design. Because this trial was a pilot study, statistical power and sample size were not calculated.
Randomization and Allocation Concealment
Patients were randomly and equally assigned to Group 1 or Group 2 using permuted block randomization at http://www.jerrydallal.com/random/randomize.htm. Masking the treatment allocation for doctors, nurses, and patients was not feasible.
Study Design
The study design is illustrated in Figure 1. Treatment 1 was regular HD according to the nephrologists’ suggestions for 4 weeks for a total of 12 sessions. Questionnaire assessments were conducted at the beginning and end of the study period. Treatment 2 was regular HD with an electronic IR heating device (HEALTHYBOX® Powered heating pad) with wavelength ranging from 5–14 µm and fixed temperatures at 56 ± 8°C on acupoint CV4 (Figure 2) during the second hour of HD. The intervention also lasted for 4 weeks, with a total of 12 sessions. To prevent heat injury, a piece of cork wood pad provided by the manufacturer was placed between the skin and the heating device (Figure 3). Moreover, for patients’ safety, the whole process was monitored by certified nurses to prevent burn injury caused by the device. Similarly, questionnaire assessments were made at the beginning and end of this study period.
 |
Figure 1 Study design. |
 |
Figure 2 Location of CV4. |
 |
Figure 3 Electronic moxibustion device with its insulating material. |
Study Outcomes
Subjective Questionnaire Assessment: Degree of Fatigue, Recovery Time of Fatigue from HD and Degree of Cold Intolerance
Questionnaires assessed the patients’ subjective assessment of the degree of fatigue after dialysis using a visual analog scale (VAS) (scale from 0 to 10; 0, not at all, 10, extremely. Specific questions like if the patient is bothered by fatigue, gets tired quickly, do not do much in the day, feeling exhausted or energetic is asked)., the recovery time of fatigue from HD using a scale modified from Gil et al and rated as within minutes (0), when arriving home (0), at bedtime (2), the next morning (5), and by the next HD (10),30 and the degree of cold intolerance using a VAS (scale from 0 to 100, 25 per range; 0 not at all, 100, extremely. Specific questions like shivering, extremities numbness, still feeling cold after adding clothes, the feeling of coldness bothers me is asked).
Frequency of IDH Episodes and Number of Nursing Interventions During HD
The number of HD sessions affected by IDH episodes and nursing interventions (Trendelenburg position, reduction in ultrafiltration rate, infusion of isotonic saline or hypertonic fluid, and lowering of dialysate temperature) was counted. Data was collected by reviewing the patient’s nursing records which included the above interventions.
BP Change During HD
BP was measured using an electronic digital sphygmomanometer before dialysis, every 60 min during HD, and after dialysis in each HD session. In the event of IDH, BP was measured every 10 minutes. Pre-, nadir-, and post-dialysis SBP, diastolic blood pressure (DBP) and MAP values were recorded during each HD session. Differences in SBP, DBP, and MAP between pre-and nadir HD and between pre- and post-HD were calculated. In addition, data on dialysis adequacy, hemoglobin levels, and blood chemistry results were collected.
Statistical Analyses
Statistical analyses were performed using the per-protocol population, defined as participants who followed the study protocol and completed therapy.
Differences in IDH frequency and nursing interventions were analyzed using Poisson regression. Differences in BP, degree of fatigue after dialysis, recovery time of fatigue from HD, and cold intolerance between Treatments 1 and 2 were analyzed using a generalized linear mixed model. Data comparing dialysis adequacy and laboratory parameters were analyzed using a generalized linear mixed model. The generalized linear mixed model is chosen as it can incorporate both random and fixed effects of the study. Poisson regression is a type of generalized linear model used for counts of events, in this case, IDH frequency and nursing interventions occurring during HD. Differences were considered statistically significant when the P-value < 0 0.05. Data were collected and analyzed using IBM SPSS version 22.0, and Microsoft Excel 2016.
Results
This study was conducted between April 2019 and April 2020. A total of 52 patients undergoing chronic HD in our hospital were eligible for this study. Twenty patients declined to participate, and the remaining 32 patients were enrolled (Figure 4). Two patients were excluded because they received alternative treatments during enrollment. Thirty participants were randomly divided into groups 1 and 2, and both groups received IR electronic moxibustion.
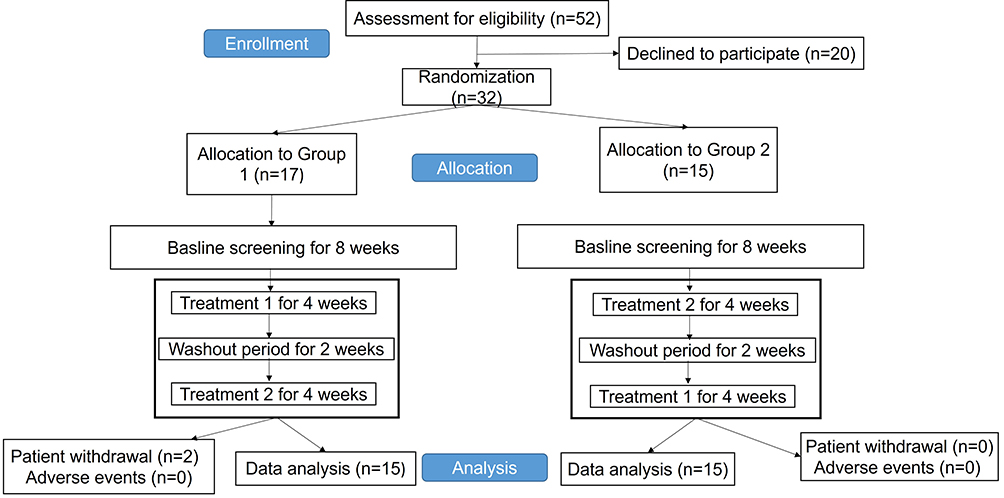 |
Figure 4 Flow chart of patient recruitment. |
Table 1 shows the baseline characteristics of the 30 Taiwanese participants. For the IDH criteria, a total of 19 patients had regular midodrine prescriptions, with 9 in Group 1 and 10 in Group 2; 20 patients met the KDOQI criteria, 9 in Group 1 and 10 in Group 2; and 23 patients met the NADIR criteria, 14 in Group 1 and 9 in Group 2 (Table 1).
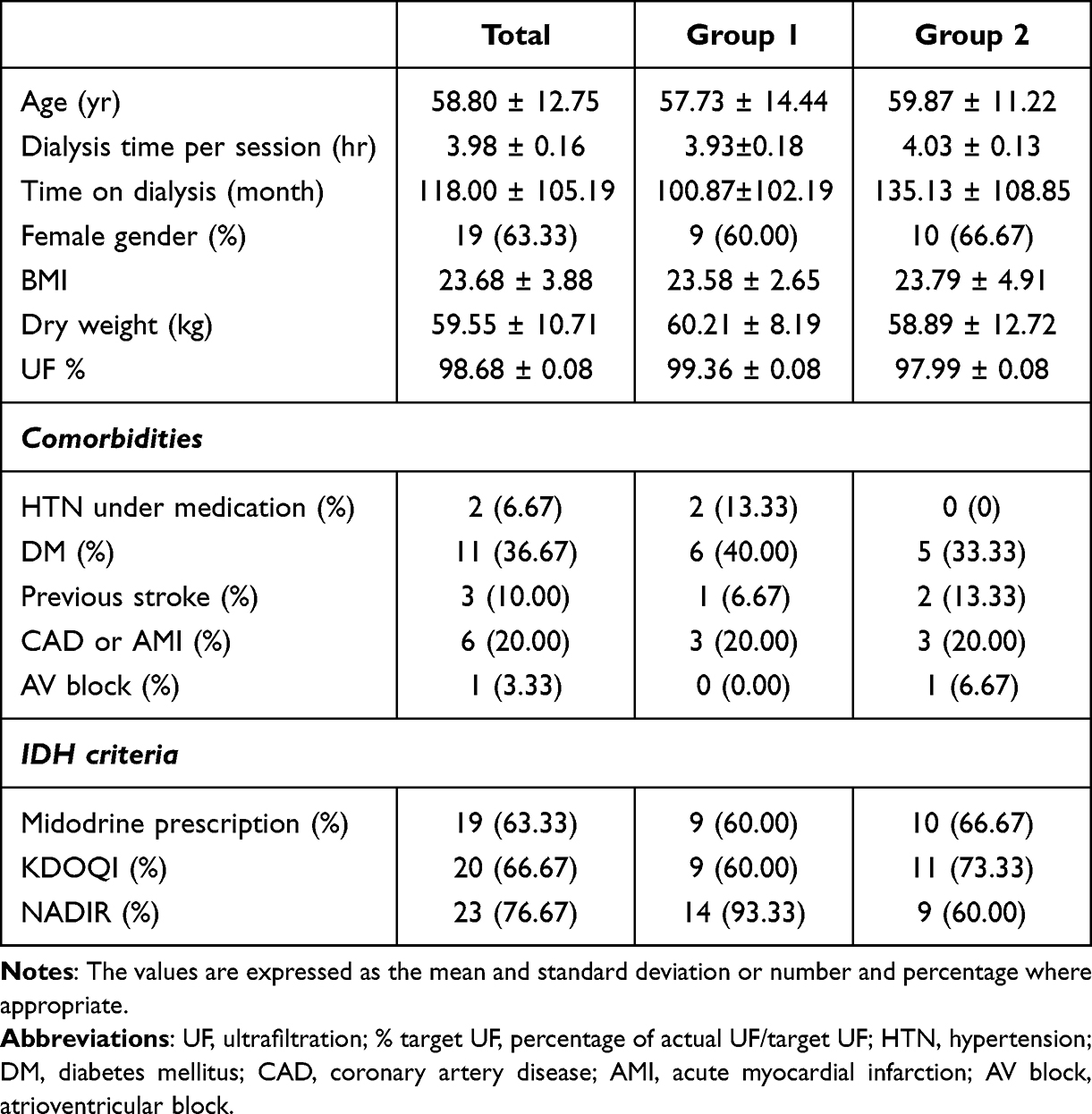 |
Table 1 Baseline Characteristics of Study Population |
Efficacy Assessment
Tables 2–5 show the results of this study.
 |
Table 2 Patients’ Subjective Questionnaire Assessments |
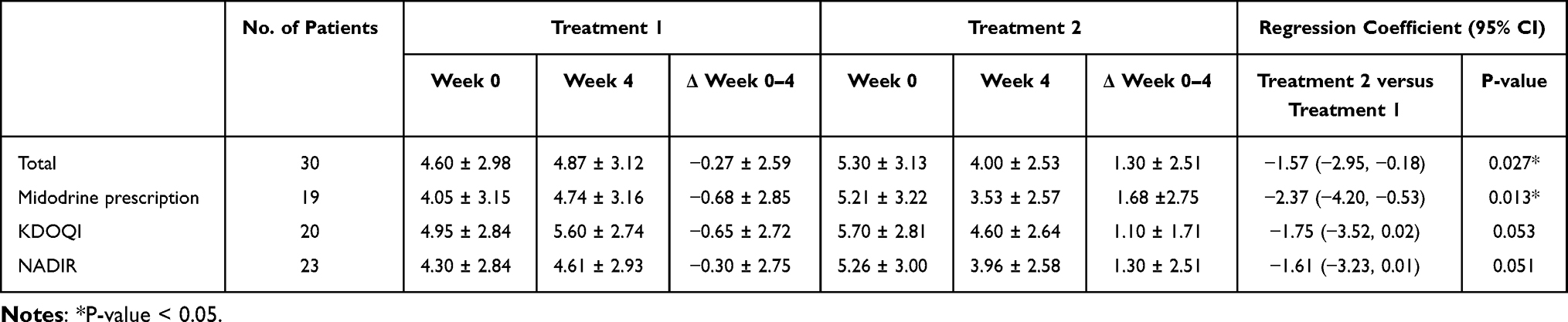 |
Table 3 Subgroup Analysis of Degree of Fatigue According to Different IDH Criteria |
 |
Table 4 Comparison of Number of IDH Frequency, Nursing Intervention Needed and BP Changes During HD in 2 Months Before Study, After Treatment 1 and Treatment 2 |
 |
Table 5 Comparison of Laboratory Parameters and Dialysis Adequacy in 2 Months Before Study, After Treatment 1 and Treatment 2 |
Effect of Electronic Moxibustion on Severity of Fatigue and Cold Intolerance
The subjective assessments of the degree of fatigue, recovery time of fatigue from HD, and cold intolerance in both groups are shown in Table 2. Figure 5 presents the degree of fatigue after dialysis in week 0 and 4 during Treatment 1 and 2 for all IDH criteria. The overall baseline VAS score for the degree of fatigue was 4.60 ± 2.95. In Treatment 1, the VAS scores for the degree of fatigue were 4.60 at week 0 and 4.87 at week 4; in Treatment 2, the VAS scores for the degree of fatigue were 5.30 at week 0 and 4.00 at week 4 (Figure 5a) indicated a notable improvement (p = 0.027) in the degree of fatigue between the two treatments (Δ Fatigue Week 0–4). In contrast, there was no significant reduction in the recovery time of fatigue from HD (Δ Recovery Week 0–4), and cold intolerance (Δ Cold intolerance Week 0–4) between Treatments 1 and 2. Upon further assessment of the degree of fatigue, a notable improvement was found in the subgroup prescribed with midodrine (p = 0.013). In the KDOQI and NADIR subgroups, there was also an improvement in the degree of fatigue; however, this difference was not statistically significant (p = 0.053 and 0.051, respectively) (Table 3 and Figure 6).
 |
Figure 5 Degree of fatigue after dialysis in weeks 0 and 4 during Treatment 1 and Treatment 2. VAS score of degree of fatigue in (a) all IDH patients, (b) patients with midodrine prescription, (c) patients meeting KDOQI criteria, and (d) patients meeting NADIR criteria. A decreasing trend of degree of fatigue was found in all groups during Treatment 2. |
 |
Figure 6 Comparison of the degree of fatigue in Treatment 1 and Treatment 2. Change in VAS score (ΔWeeks 0–4) between Treatment 2 vs Treatment 1 (a) −1.30 vs 0.27, P = 0.027 in all IDH patients, (b) −1.68 vs 0.68, P = 0.013 in patients with midodrine prescription, (c) −1.10 vs 0.65, P = 0.053 in KDOQI criteria, and (d) −1.30 vs 0.30, P = 0.051 in NADIR criteria. Notes: *P-value < 0.05. |
Effect of Electronic Moxibustion on IDH Frequency and Nursing Intervention
Among the three study periods, there was no significant reduction in the number of IDH frequencies according to the KDOQI and NADIR criteria or the number of sessions that required nursing intervention. (Table 4).
Effect of Electronic Moxibustion on BP
Among the three study periods, there was no significant difference in BP changes due to IR electronic moxibustion (Table 4).
Effect on HD Parameters
Among the three study periods, there were no significant differences in the mean pre- and post-dialysis body weight, dry weight, target ultrafiltration, amount of actual ultrafiltration, dialysis adequacy measured by % target ultrafiltration achieved, and hematologic or biochemical parameters. (Table 5)
Assessment of Adverse Events
Serious adverse events were not observed. One of the patients complained of heat tolerance. Two other 2 patients had local transient erythema and pruritus that subsided within a few hours after moxibustion treatment. None of the patients experienced skin burns during the moxibustion course.
Discussion
This randomized, two-arm crossover trial included 30 patients with IDH. While moxibustion improved the degree of fatigue, it did not affect IDH frequency, BP changes, fatigue recovery time and cold intolerance. The overall baseline VAS score for the degree of fatigue was 4.60 ± 2.95. The average VAS score of the degree of fatigue before Treatment 1 and Treatment 2 was 4.60 and 5.30, respectively. A slight increase in the degree of fatigue was noted after four weeks of Treatment 1. In contrast, a decreasing trend was noted in Treatment 2 during the 4 weeks. This study found that one-hour electronic moxibustion treatment during HD for 4 weeks improved the degree of fatigue in IDH patients (Δ Fatigue Week 0–4 in Treatment 2 = 1.30 ± 2.51 vs Treatment 1 = −0.27±2.59, p = 0.027), especially in the subgroup with midodrine prescription (Δ Fatigue Week 0–4 in Treatment 2 = 1.68 ± 2.75 vs Treatment 1 = −0.68 ± 2.85, p = 0.013).
Midodrine is the prodrug of the specific alpha 1 adrenergic receptor agonist, desglymidodrine. This metabolite induces constriction of both arterial and venous capacitance vessels, and prevents venous pooling of the blood whilst increasing BP.35,36 It is now often prescribed to patients and administered before dialysis to lessen the chance of an adverse hypotension event during HD.37–39 Patients who meet the IDH criteria of the KDOQI and NADIR have a BP drop or nadir BP within a certain range; however, their IDH-associated symptoms may still be tolerable. Clinically, midodrine is often prescribed as the last option for attempting additional volume removal during HD37 in patients with severe associated symptoms interfering with ultrafiltration. Our study observed that patients on midodrine experienced greater fatigue improvement with moxibustion compared to those not on midodrine. While the improvement in fatigue was statistically significant, there was no corresponding significant change in IDH frequency or BP. The potential reasons for this interaction may be due to sympathetic nervous system modulation, difference in fatigue mechanisms and increased resilience. Midodrine works by increasing peripheral vascular resistance to counteract the drop in BP during dialysis, which is closely tied to autonomic nervous system regulation.35,40–42 Moxibustion, particularly via its thermal effects33,43 and potential modulation of the autonomic nervous system,24 may complement midodrine by reducing the physical and psychological strain associated with dialysis. This synergistic effect might help explain the improved fatigue outcomes in patients on midodrine. While midodrine focuses on BP regulation, it may not directly address the broader range of symptoms contributing to fatigue, such as inflammation, sleep disturbances, or discomfort during dialysis. Moxibustion, known for its potential to promote relaxation and improve energy flow (Qi) according to Traditional Chinese Medicine (TCM), could be addressing these broader fatigue-related mechanisms,23,26,44 particularly in patients on midodrine, whose overall treatment regimen is more complex. The combination of midodrine and moxibustion may increase patients’ resilience to the physical stresses of dialysis. Midodrine helps prevent severe BP drops, while moxibustion might mitigate the subjective feelings of fatigue, leading to an overall sense of well-being, despite the lack of significant changes in BP or IDH frequency. Clinically, this suggests that while moxibustion alone may not have a strong impact on BP or IDH frequency, its use as an adjunct therapy, particularly in patients on midodrine, could enhance fatigue recovery and improve patient outcomes during dialysis.
While trends in BP changes were observed, they did not reach statistical significance and were consistent with baseline data upon review, suggesting that moxibustion did not impact BP directly in our study. This observation aligns with previous studies29 on intradialytic hypotension (IDH) adjunct therapies, which also reported limited effects on BP parameters despite improvements in subjective symptoms like fatigue.
In addition, we recognize that our study adds a new perspective on combining moxibustion with midodrine. While prior research, such as Tsai et al29 demonstrated that herbal acupoint therapy reduced IDH frequency and improved fatigue, it did not specifically address midodrine interactions and utilized narrower IDH criteria (limited to KDOQI). While herbal acupoint therapy may show more effectiveness in reducing IDH frequency, potential drug interactions are a clinical concern, especially considering the common use of multiple medications among HD patients. Our findings suggest that moxibustion, when combined with midodrine, may primarily benefit patients by alleviating fatigue rather than altering BP or IDH frequency.
Shengmai Injection45 or oral intake of Ginseng46 may help BP in HD but increases the medication burden and therefore may not be widely accepted by patients and physicians.
A case report by Jung et al45 found that intradialytic acupuncture decreased IDH frequency in one patient and another study done by Kim et al47 found acupuncture may be beneficial in HD patients in terms of symptom management. These studies, like moxibustion, may not independently affect BP or IDH frequency but can contribute to patient well-being when used alongside other treatments.
The patients’ subjective assessment results showed a significant improvement in the degree of fatigue, but not in the recovery time of fatigue from HD and cold intolerance. TCM categorizes patients with the same disease into different patterns or constitutions, and the major constitution of chronic HD patients is Yang deficiency (up to 43.7%).48 Nevertheless, the feeling of weakness and chronic fatigue is also highly associated with Qi-deficiency, while preference for warm things is associated with Yang-deficiency.49 Another study has suggested that Yin-deficiency may also play a role in chronic fatigue.50 Given the heterogeneity of different TCM constitutions in patients with IDH, the improvement in cold intolerance was not significant in these patients, and further investigations should be conducted.
This study applied electronic moxibustion in the second hour of HD; however, a previous study that explored the behavior of SBP during HD noted a relatively steeper decline in the first quarter of HD, followed by a gentler decrease.51 This phenomenon seems less likely to be explained by the excessive volume removal during the early period.21 Therefore, we speculated that electronic moxibustion could be applied before HD to stabilize BP in patients with IDH. To further optimize electronic moxibustion, a decrease in BP during different quarters of HD should be observed to better understand its effect on BP.
To our knowledge, this is the first crossover study to apply electronic moxibustion to patients with IDH. The results showed that electronic moxibustion can improve the severity of IDH-related fatigue, thus contributing to better quality of life and HD treatment adherence. Moreover, electronic moxibustion is generally safe and causes no skin burn injuries, allergic reactions, or hazardous smoke exposure. Compared to frequent nursing interventions which puts a burden on healthcare or additional TCM consultation fee and charges (about 360–400 USD per month treatment), the price is about 45–75 USD per device and easy to instruct patients to use by themself. The feeling of heat intolerance can be alleviated by slightly moving the device up and down the Conception Vessel, although most patient feel comfortable using this warm device.
However, our study had some limitations. First, only 30 patients were recruited for this preliminary study, which may affect the study’s power and further large-scale clinical trials are warranted. Second, due to the crossover design, patient blinding was not feasible and may have potential bias when assessing questionnaires. Third, the inclusion criteria for IDH were broad, and this heterogeneity made it more difficult for trials to achieve significant stabilization of BP and decrease in IDH frequency during HD. Fourth, most patients with IDH have multiple comorbidities, and our study patients were no exception. Three patients were hospitalized during the trial due to gastrointestinal bleeding, bacteremia suspected of arteriovenous graft infection, and ventricular tachycardia. The other two patients had emergency visits due to vascular access malfunction. All of these factors reflect the clinical instability and heterogeneity of patients with IDH.
Conclusions
We conclude that our thermostatic electronic moxibustion is safe and beneficial in improving fatigue in patients with IDH. Electronic moxibustion is more effective than harmful; hence, this cost effective and easy-to-use device is worth promoting in HD units. Our results may also provide novel concepts for designing further studies that aim to optimize the intervention timing and narrow specific IDH patient groups such as those with midodrine prescription to evaluate the efficacy of electronic moxibustion in stabilizing BP.
Abbreviations
IDH, intradialytic hypotension; HD, hemodialysis; BP, blood pressure; TCM, traditional Chinese medicine; IR, infrared; SBP, systolic blood pressure; MAP, mean arterial pressure; KDOQI, Kidney Disease Outcomes Quality Initiative; VAS, Visual Analogue Scale; DBP, diastolic blood pressure.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted according to the principles of Declaration of Helsinki and good clinical practice guidelines. Prior to the commencement of the study, ethical approval was obtained from the Institutional Review Board of the Chang Gung Medical Foundation (IRB no. 201801853A3). All methods were performed in accordance with the relevant guidelines and regulations. All the participants provided written informed consent.
Acknowledgments
The authors would like to thank the dialysis staff at the hemodialysis center in Keelung Chang Gung Memorial Hospital for their excellent technical assistance and all participants who completed the study protocol.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Sars B, van der Sande FM, Kooman JP. Intradialytic Hypotension: mechanisms and Outcome. Blood Purif. 2020;49(1–2):158–167. doi:10.1159/000503776
2. Flythe JE, Xue H, Lynch KE, Curhan GC, Brunelli SM. Association of mortality risk with various definitions of intradialytic hypotension. J Am Soc Nephrol. 2015;26(3):724–734. doi:10.1681/asn.2014020222
3. Kuipers J, Verboom LM, Ipema KJR, et al. The Prevalence of Intradialytic Hypotension in Patients on Conventional Hemodialysis: a Systematic Review with Meta-Analysis. Am J Nephrol. 2019;49(6):497–506. doi:10.1159/000500877
4. Assimon MM, Flythe JE. Definitions of intradialytic hypotension. Semin Dial. 2017;30(6):464–472. doi:10.1111/sdi.12626
5. Saran R, Bragg-Gresham JL, Rayner HC, et al. Nonadherence in hemodialysis: associations with mortality, hospitalization, and practice patterns in the DOPPS. Kidney Int. 2003;64(1):254–262. doi:10.1046/j.1523-1755.2003.00064.x
6. Davenport A. Why is Intradialytic Hypotension the Commonest Complication of Outpatient Dialysis Treatments? Kidney Int Rep. 2023;8(3):405–418. doi:10.1016/j.ekir.2022.10.031
7. Gul A, Miskulin D, Harford A, Zager P. Intradialytic hypotension. Curr Opin Nephrol Hypertens. 2016;25(6):545–550. doi:10.1097/MNH.0000000000000271
8. Chou JA, Kalantar-Zadeh K, Mathew AT. A brief review of intradialytic hypotension with a focus on survival. Semin Dial. 2017;30(6):473–480. doi:10.1111/sdi.12627
9. Obialo CI, Hunt WC, Bashir K, Zager PG. Relationship of missed and shortened hemodialysis treatments to hospitalization and mortality: observations from a US dialysis network. Clin Kidney J. 2012;5(4):315–319. doi:10.1093/ckj/sfs071
10. Alvarez L, Brown D, Hu D, Chertow GM, Vassalotti JA, Prichard S. Intradialytic Symptoms and Recovery Time in Patients on Thrice-Weekly In-Center Hemodialysis: a Cross-sectional Online Survey. Kidney Med. 2020;2(2):125–130. doi:10.1016/j.xkme.2019.10.010
11. Bossola M, Tazza L. Postdialysis Fatigue: a Frequent and Debilitating Symptom. Semin Dial. 2016;29(3):222–227. doi:10.1111/sdi.12468
12. Weisbord SD, Carmody SS, Bruns FJ, et al. Symptom burden, quality of life, advance care planning and the potential value of palliative care in severely ill haemodialysis patients. Nephrol Dial Transplant. 2003;18(7):1345–1352. doi:10.1093/ndt/gfg105
13. Horigan AE. Fatigue in hemodialysis patients: a review of current knowledge. J Pain Symptom Manage. 2012;44(5):715–724. doi:10.1016/j.jpainsymman.2011.10.015
14. Horigan AE, Schneider SM, Docherty S, Barroso J. The experience and self-management of fatigue in patients on hemodialysis. Nephrol Nurs J. 2013;40(2):113–22;quiz123.
15. Yong DS, Kwok AO, Wong DM, Suen MH, Chen WT, Tse DM. Symptom burden and quality of life in end-stage renal disease: a study of 179 patients on dialysis and palliative care. Palliat Med. 2009;23(2):111–119. doi:10.1177/0269216308101099
16. Jhamb M, Weisbord SD, Steel JL, Unruh M. Fatigue in patients receiving maintenance dialysis: a review of definitions, measures, and contributing factors. Am J Kidney Dis. 2008;52(2):353–365. doi:10.1053/j.ajkd.2008.05.005
17. Weisbord SD, Fried LF, Arnold RM, et al. Prevalence, severity, and importance of physical and emotional symptoms in chronic hemodialysis patients. J Am Soc Nephrol. 2005;16(8):2487–2494. doi:10.1681/asn.2005020157
18. Jhamb M, Argyropoulos C, Steel JL, et al. Correlates and outcomes of fatigue among incident dialysis patients. Clin J Am Soc Nephrol. 2009;4(11):1779–1786. doi:10.2215/cjn.00190109
19. Van Buren PN, Inrig JK. Special situations: intradialytic hypertension/chronic hypertension and intradialytic hypotension. Semin Dial. 2017;30(6):545–552. doi:10.1111/sdi.12631
20. Chou JA, Streja E, Nguyen DV, et al. Intradialytic hypotension, blood pressure changes and mortality risk in incident hemodialysis patients. Nephrol Dial Transplant. 2018;33(1):149–159. doi:10.1093/ndt/gfx037
21. Reeves PB, Mc Causland FR. Mechanisms, Clinical Implications, and Treatment of Intradialytic Hypotension. Clin J Am Soc Nephrol. 2018;13(8):1297–1303. doi:10.2215/CJN.12141017
22. Hamrahian SM, Vilayet S, Herberth J, Fulop T. Prevention of Intradialytic Hypotension in Hemodialysis Patients: current Challenges and Future Prospects. Int J Nephrol Renovasc Dis. 2023;16:173–181. doi:10.2147/IJNRD.S245621
23. Kim HG, Yoo SR, Park HJ, Son CG. Indirect moxibustion (CV4 and CV8) ameliorates chronic fatigue: a randomized, double-blind, controlled study. J Altern Complement Med. 2013;19(2):134–140. doi:10.1089/acm.2011.0503
24. Shu Q, Wang H, Litscher D, et al. Acupuncture and Moxibustion have Different Effects on Fatigue by Regulating the Autonomic Nervous System: a Pilot Controlled Clinical Trial. Sci Rep. 2016;6(1):37846. doi:10.1038/srep37846
25. Tsay SL. Acupressure and fatigue in patients with end-stage renal disease-a randomized controlled trial. Int J Nurs Stud. 2004;41(1):99–106. doi:10.1016/s0020-7489(03)00079-8
26. Han K, Kim M, Kim EJ, et al. Moxibustion for treating cancer-related fatigue: a multicenter, assessor-blinded, randomized controlled clinical trial. Cancer Med. 2021;10(14):4721–4733. doi:10.1002/cam4.4020
27. Lee S, Jerng UM, Liu Y, Kang JW, Nam D, Lee JD. The effectiveness and safety of moxibustion for treating cancer-related fatigue: a systematic review and meta-analyses. Support Care Cancer. 2014;22(5):1429–1440. doi:10.1007/s00520-014-2161-z
28. Mao H, Jin M, Xie L, et al. Infrared laser moxibustion for cancer-related fatigue in breast cancer survivors: a randomized controlled trial. Breast Cancer Res. 2024;26(1):80. doi:10.1186/s13058-024-01838-1
29. Tsai MY, Wu CH, Huang YC, et al. Treatment of intradialytic hypotension with an herbal acupoint therapy in hemodialysis patients: a randomized pilot study. Complement Ther Med. 2018;38:67–73. doi:10.1016/j.ctim.2018.04.007
30. Park JE, Lee SS, Lee MS, Choi SM, Ernst E. Adverse events of moxibustion: a systematic review. Complement Ther Med. 2010;18(5):215–223. doi:10.1016/j.ctim.2010.07.001
31. Yeh YC, Chen CC, Cheng CY, Chang HN, Huang TH. The Beneficial Effects of Moxibustion on Overweight Adolescent Girls. Evid Based Complement Alternat Med. 2021;2021:1943181. doi:10.1155/2021/1943181
32. Chiu JH. How does moxibustion possibly work? Evid Based Complement Alternat Med. 2013;2013:198584. doi:10.1155/2013/198584
33. Deng H, Shen X. The mechanism of moxibustion: ancient theory and modern research. Evid Based Complement Alternat Med. 2013;2013:379291. doi:10.1155/2013/379291
34. Zhu LL, Zhou JY, Luo L, et al. Comparison of the efficacy between conventional moxibustion and smoke-free moxibustion on knee osteoarthritis: study protocol of a randomized controlled trial. Trials. 2017;18(1):188. doi:10.1186/s13063-017-1846-2
35. Park J-W, Okamoto LE, Shibao CA, Biaggioni I. Pharmacologic treatment of orthostatic hypotension. Autonomic Neuroscience. 2020;229:102721. doi:10.1016/j.autneu.2020.102721
36. Kanbay M, Ertuglu LA, Afsar B, et al. An update review of intradialytic hypotension: concept, risk factors, clinical implications and management. Clin Kidney J. 2020;13(6):981–993. doi:10.1093/ckj/sfaa078
37. Hammes M, Bakris GL. Intradialytic Hypotension: is Midodrine the Answer? Am J Nephrol. 2018;48(5):378–380. doi:10.1159/000494805
38. Saja ALH, Maryam ALD, Mohammed ALE, Maha ALA, Yousef ALR, Rami B. Midodrine for Prevention of Intradialytic Hypotension in High Risk Patients at a Tertiary Referral Hospital: a Retrospective Study. Journal of Hypertension and Management. 2021;7(1). doi:10.23937/2474-3690/1510060
39. Srinivasa V. A Review of Midodrine for the Treatment of Intradialytic Hypotension. International Journal of Nephrology and Kidney Failure. 2019;5:1. doi:10.16966/2380-5498.169
40. Park S, Kim WJ, Cho NJ, et al. Predicting intradialytic hypotension using heart rate variability. Sci Rep. 2019;9(1):2574. doi:10.1038/s41598-019-39295-y
41. Pelosi G, Emdin M, Carpeggiani C, et al. Impaired sympathetic response before intradialytic hypotension: a study based on spectral analysis of heart rate and pressure variability. Clin Sci (Lond). 1999;96(1):23–31. doi:10.1042/cs0960023
42. Koda Y, Aoike I. Prevention of Intradialytic Hypotension with Intermittent Back-Filtrate Infusion Haemodiafiltration: insights into the Underlying Mechanism. Blood Purif. 2019;48(1):1–6. doi:10.1159/000503878
43. Shen X, Ding G, Wei J, et al. An infrared radiation study of the biophysical characteristics of traditional moxibustion. Complement Ther Med. 2006;14(3):213–219. doi:10.1016/j.ctim.2005.09.003
44. Yi T, Qi L, Li J, et al. Moxibustion upregulates hippocampal progranulin expression. Neural Regen Res. 2016;11(4):610–616. doi:10.4103/1673-5374.180746
45. Chen C-Y, Lu L-Y, Chen P, et al. Shengmai injection, a traditional Chinese patent medicine, for intradialytic hypotension: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:703815. doi:10.1155/2013/703815
46. Chen IJ, Chang MY, Chiao SL, et al. Korean red ginseng improves blood pressure stability in patients with intradialytic hypotension. Evid Based Complement Alternat Med. 2012;2012:595271. doi:10.1155/2012/595271
47. Kim KH, Kim TH, Kang JW, et al. Acupuncture for symptom management in hemodialysis patients: a prospective, observational pilot study. J Altern Complement Med. 2011;17(8):741–748. doi:10.1089/acm.2010.0206
48. Liao YC, Chou CY, Chang CT, et al. Qi deficiency is associated with depression in chronic hemodialysis patients. Complement Ther Med. 2017;30:102–106. doi:10.1016/j.ctim.2016.12.008
49. Kim J, Ku B, Kim KH. Validation of the qi blood yin yang deficiency questionnaire on chronic fatigue. Chin Med. 2016;11(1):24. doi:10.1186/s13020-016-0092-y
50. Leong PK, Wong HS, Chen J, Ko KM. Yang/Qi invigoration: an herbal therapy for chronic fatigue syndrome with yang deficiency? Evid Based Complement Alternat Med. 2015;2015:945901. doi:10.1155/2015/945901
51. Dinesh K, Kunaparaju S, Cape K, Flythe JE, Feldman HI, Brunelli SM. A model of systolic blood pressure during the course of dialysis and clinical factors associated with various blood pressure behaviors. Am J Kidney Dis. 2011;58(5):794–803. doi:10.1053/j.ajkd.2011.05.028
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.