Back to Journals » Risk Management and Healthcare Policy » Volume 16
Effect of Early versus Delayed Use of Norepinephrine on Short-Term Outcomes in Patients with Traumatic Hemorrhagic Shock: A Propensity Score Matching Analysis
Authors Zhang B, Dong X, Wang J, Li GK, Li Y, Wan XY
Received 8 February 2023
Accepted for publication 15 June 2023
Published 22 June 2023 Volume 2023:16 Pages 1145—1155
DOI https://doi.org/10.2147/RMHP.S407777
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Bing Zhang,1,* Xue Dong,2,* Jia Wang,2 Gong-Ke Li,1 Yong Li,3 Xian-Yao Wan2
1Department of Emergency Intensive Care Medicine, Affiliated Hospital of Yangzhou University, Yangzhou, 225000, People’s Republic of China; 2Department of Critical Care Medicine, The First Affiliated Hospital of Dalian Medical University, Dalian, 116000, People’s Republic of China; 3Department of Critical Care Medicine, Affiliated Hospital of Yangzhou University, Yangzhou, 225000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xian-Yao Wan, Department of Critical Care Medicine, The First Affiliated Hospital of Dalian Medical University, No. 193 Joint Road, Sha He Kou District, Dalian, 116000, People’s Republic of China, Tel +86 41183635963, Fax +86 41183635025, Email [email protected] Yong Li, Department of Critical Care Medicine, Affiliated Hospital of Yangzhou University, No. 368 Hanjiang Middle Road, Hanjiang District, Yangzhou, 225000, People’s Republic of China, Tel/Fax +86 51482981199, Email [email protected]
Background: Guidelines recommend norepinephrine (NE) for the treatment of fatal hypotension caused by trauma. However, the optimal timing of treatment remains unclear.
Objective: We aimed to investigate the effect of early versus delayed use of NE on survival in patients with traumatic haemorrhagic shock (HS).
Materials and Methods: From March 2017 to April 2021, 356 patients with HS in the Department of Emergency Intensive Care Medicine of the Affiliated Hospital of Yangzhou University were identified using the emergency information system and inpatient electronic medical records for inclusion in the study. Our study endpoint was 24 h mortality. We used a propensity score matching (PSM) analysis to reduce bias between groups. Survival models were used to evaluate the relationship between early NE and 24 h survival.
Results: After PSM, 308 patients were divided equally into an early NE (eNE) group and a delayed NE (dNE) group. Patients in the eNE group had lower 24 h mortality rates than those in the dNE group (29.9% versus 44.8%, respectively). A receiver operating characteristic analysis demonstrated that a cut-off point for NE use of 4.4 h yielded optimal predictive value for 24 h mortality, with a sensitivity of 95.52%, a specificity of 81.33% and an area under the curve value of 0.9272. Univariate and multivariate survival analyses showed that the survival rate of patients in the eNE group was higher (p < 0.01) than those in the dNE group.
Conclusion: The use of NE within the first 3 h was associated with a higher 24 h survival rate. The use of eNE appears to be a safe intervention that benefits patients with traumatic HS.
Keywords: norepinephrine, traumatic haemorrhagic shock, propensity score matching
Introduction
Severe trauma is a global public health problem, causing approximately 5.8 million deaths annually, with a mortality rate of more than 10%.1 Haemorrhagic shock (HS) is a severe complication of trauma and is the primary cause of early death in patients with trauma.2,3 Guidelines recommend restrictive fluid resuscitation4 and permissive hypotension strategies5–7 for HS until bleeding is controlled. The 2019 European guideline on the management of major bleeding and coagulopathy following trauma recommends the use of norepinephrine (NE) for maintaining target arterial blood pressure in patients with life-threatening hypotension.8 However, this guideline does not clearly state the optimal timing for the use of NE. Therefore, the timing of NE use remains unclear.
Rigorous data regarding the efficacy and safety of NE in patients with HS are currently lacking. One multicenter prospective cohort study showed that early use of vasopressors might be hemodynamically detrimental compared with using fluid resuscitation alone and should be used with caution.9 However, we found a significantly higher proportion of patients undergoing thoracotomy in the early cohort of this study, which may have influenced patient hemodynamic outcomes. In another prospective study of 518 patients with HS, after propensity score matching (PSM), the early use of NE (eNE) use had no adverse effect on 24 h mortality compared with no NE use.10 In a recent study of 4253 patients with septic shock, patients with HS in an eNE group had longer survival, shorter durations of NE use and possibly delayed or reversed organ failure.11 This suggests that eNE may benefit patients. However, whether eNE benefits patients with HS is unclear. Therefore, the optimal timing of NE use in patients with traumatic HS requires further investigation.
To date, uniform criteria for the timing of NE initiation in the management of HS have not been established. In this study, we extrapolated previous research results11–13 and defined eNE as an interval between NE treatment and HS of ≤3 h; delayed NE (dNE) was defined as an NE duration of >3 h. We aimed to investigate the impact of eNE versus dNE on the survival of patients with traumatic HS.
Materials and Methods
Study Population
This was an observational study in which we retrospectively analysed the medical history data of 518 patients with traumatic HS admitted to the emergency intensive care unit (ICU) of the Affiliated Hospital of Yangzhou University with a diagnosis of traumatic HS between March 2017 and April 2021. Traumatic HS was defined as a severely traumatised patient with mean arterial pressure (MAP) of <65 mmHg on admission, requiring surgical control of active bleeding, the transfusion of more than four units of red blood cells (RBCs) within 6 h of admission and the use of NE within 24 h of admission. The exclusion criteria included age <18 years or >65 years, cardiac arrest at admission, severe brain or spinal injury (because of different target blood pressures), death due to haemostatic failure within 6 h of admission and incomplete clinical data. This study was approved by the Medical Ethics Committee of the Affiliated Hospital of Yangzhou University, and informed consent was obtained from all participants (2021-YKL3-01-001).
The vasoactive drug NE was used for preliminary treatment, and the start time of traumatic HS was defined as the first recorded MAP of <65 mmHg. Based on the time of traumatic HS onset and the timing of NE treatment, patients were divided into two groups: an eNE group and a dNE group. Patients were allocated to the eNE group if the timespan was ≤3 h. Patients with an interval of >3 h between NE treatment and HS were allocated to the dNE group. The detailed flowchart of the enrolled patients is shown in Figure 1.
 |
Figure 1 Flowchart of study design and patient selection. |
Data Collection
The clinical data of all enrolled patients were extracted from the emergency information system and inpatient electronic medical records. Baseline characteristics were collected within 24 h after admission and included age, sex, Charlson Comorbidity Index (CCI), body mass index (BMI), complications (hypertension, myocardial infarction, congestive heart failure, chronic pulmonary disease, diabetes mellitus, kidney disease, cancer, leukaemia, lymphoma and metastatic cancer), mechanism of injury (blunt), cause of injury (motor vehicles, bikes, pedestrians, falls and other reasons), pre-hospital status (MAP, heart rate [HR], fluid amount, intubation and initial Glasgow Coma Scale [GCS] score), on-admission status (MAP, HR), intubation, initial GCS score, haemoglobin, blood glucose, blood lactate and serum creatinine), severity scores (sequential organ failure assessment [SOFA] score on the first day, injury severity score [ISS] score on the first day and acute physiology, age, chronic health evaluation [APACHE III] score on the first day), NE use (timing, maximum NE dose within 24 h, total dose within 24 h, and target MAP need time), fluid resuscitation within 24 h (RBCs, lyophilised plasma, fibrinogen, platelets, total of non-blood fluid infusion, total of all fluid infusion), damage control surgery, 24 h mortality, in-hospital mortality, acute kidney injury (AKI) within 24 h, continuous renal replacement therapy (CRRT)-free days, invasive mechanical ventilation (IMV)-free days, hospital length of stay (HLOS) and ICU length of stay (ICU LOS).
Study Endpoint
The primary endpoint was 24 h mortality, and the secondary endpoints were in-hospital mortality, incidence of AKI, duration of non-CRRT, duration of non-IMV therapy, HLOS and ICU LOS. The duration of non-IMV therapy and non-CRRT was expressed as 28 d after admission, ie the number of days the patient survived without IMV therapy or CRRT. If the patient died within 24 h, the time of death was used as the endpoint. According to the European guideline on the management of major bleeding and coagulopathy following trauma,8 the target MAP for fluid resuscitation was set at 50–60 mmHg. The diagnosis of AKI was based on the Improving the Global Prognosis Guidelines for kidney disease,14 and AKI was not assessed in patients with end-stage renal disease.
Statistical Methods
Stata 16.0 statistical software was used. The normality of the data was tested using the Shapiro–Wilk method. Normally distributed data were expressed as mean (±SD), and non-normally distributed data were expressed as M (Q1, Q3). Categorical variables were indicated as numbers and percentages. The results were depicted as boxplot diagrams. To reduce bias, PSM was used to obtain a control cohort of patients in the eNE group and the dNE group, with a matching ratio of 1:1 and a calliper value of 0.2, with age, male, CCI, BMI, complications, mechanism of injury, cause of injury, pre-hospital status, on-admission status, severity scores, NE use, fluid resuscitation within 24 h and damage control surgery as covariates without substitution. A Kaplan–Meier survival analysis and a Streg regression model were used to evaluate the relationship between eNE and the 24 h survival rate of patients. The area under the receiver operating characteristic (ROC) curve was calculated to determine the predictive abilities of the timing of NE use for 24 h mortality. A value of P < 0.05 was considered statistically significant.
Results
General Characteristics of the Patients
A total of 518 patients were diagnosed with traumatic HS. Of these, 162 were excluded, including 45 patients aged <18 years or >65 years, 18 patients with cardiac arrest on admission, 62 patients with a severe brain or spinal injury caused by different target blood pressures, 30 patients who died of haemostatic failure within 6 h of admission and 7 patients with incomplete clinical data. Finally, 356 patients met the inclusion criteria. The mean age of the patients was 49.8 ± 14.4 years, and 189 were male (53.1%). The most common injuries were bicycle injuries (143, 40.2%), followed by motor vehicle injuries (82, 23.0%), falls (74, 20.8%), pedestrian injuries (47, 13.2%) and other injuries (10, 2.8%). Ultimately, 176 patients (49.3%) were subordinated to the eNE group, and 180 patients (50.7%) were subordinated to the dNE group. After PSM, the eNE and dNE groups each had 154 patients. Therefore, 308 patients participated in the final analysis (Figure 1).
Before PSM, there were significant differences in age, complications (hypertension), mechanism of injury, pre-hospital status (MAP and initial GCS score), on-admission status (MAP and haemoglobin), first-day ISS score, first-day SOFA score, first-day APACHE III score, timing of NE use, target MAP need time, 24 h total of non-blood fluid infusion and 24 h total of all fluid infusion between the groups (P < 0.05). After PSM, there were significant differences in the timing of NE use, target MAP need time, total of non-blood fluid infusion and total of all fluid infusion between the eNE and dNE groups (P < 0.05) (Table 1, Figure 2).
 |
Table 1 Comparison of Baseline Data of Patients Between Early Norepinephrine and Delayed Norepinephrine Before and After Propensity Score Matching |
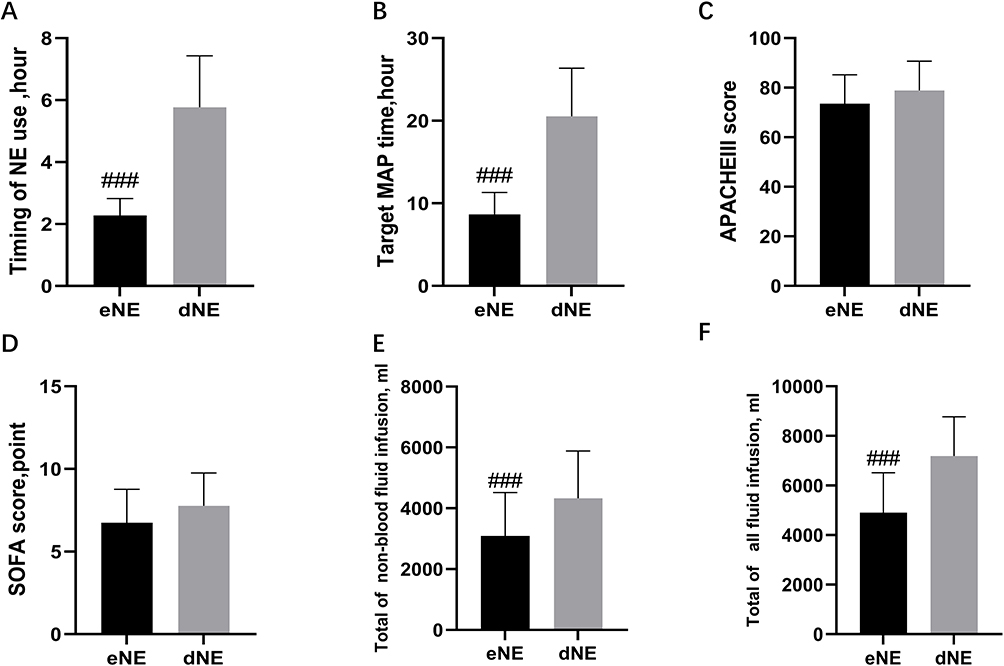 |
Figure 2 Comparison of the characteristics of patients in the early group and the delayed group. The timing of norepinephrine use (A); Target mean arterial pressure need time (B); APACHE III score 1st day (C); SOFA score 1st day (D); The total of non-blood fluid infusion (E); Total of all fluid infusion (F). ###Compared with dEN, P<0.001. Abbreviations: MAP, mean arterial pressure, APACHE, acute physiology, age, chronic health evaluation. SOFA, sequential organ failure assessment. eNE, early norepinephrine; dNE, delay norepinephrine. |
Primary Study Endpoint
Before PSM, the 24 h mortality rate in the eNE group was lower than that in the dNE group (54, 30.7% versus 45.0%; P < 0.001). After PSM, the 24 h mortality rate in the eNE group was still lower than that in the dNE group (46, 29.9% versus 69, 44.8%, P < 0.001) (Table 2). The ROC analysis demonstrated that a 4.4 h cut-off point for the timing of NE use gave the optimal predictive value for 24 h mortality, with a sensitivity of 95.52%, a specificity of 81.33% and an AUC of 0.9272; these were better than other potential risk factors, such as the ISS score (0.6859), APACHE III score (0.7232), SOFA score (0.7961), total of non-blood fluid infusion (0.8103) and total of all fluid infusion (0.8045) (Figure 3).
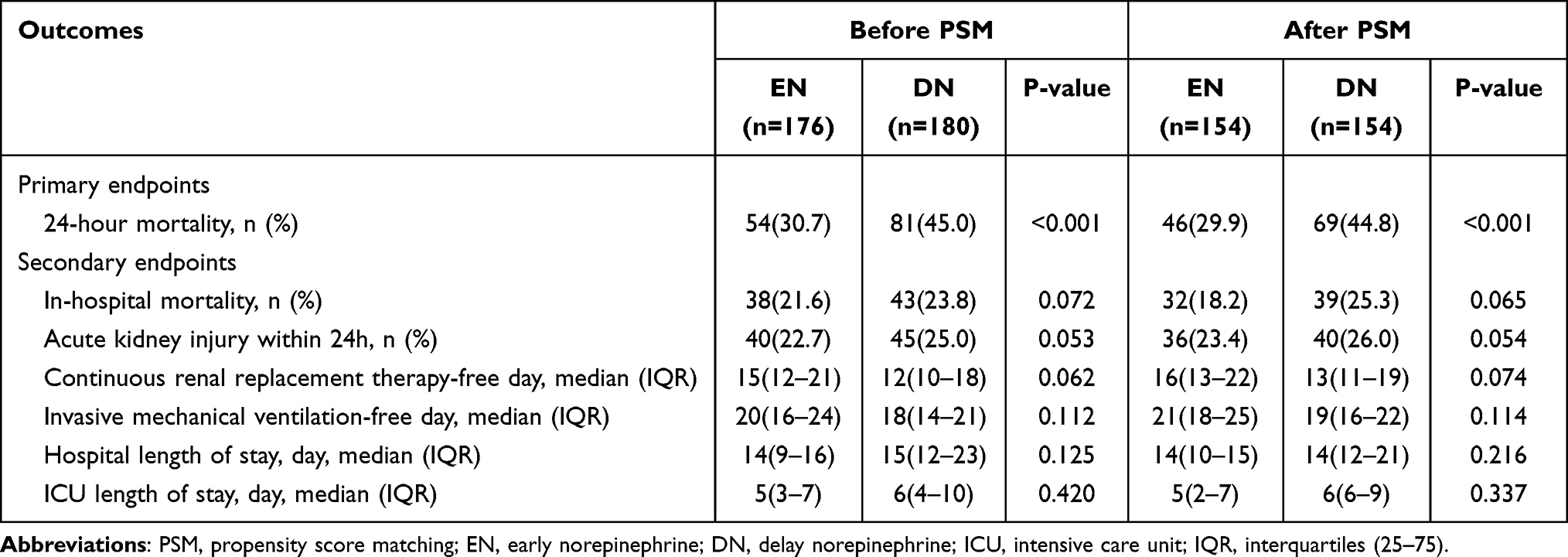 |
Table 2 Comparison of Clinical Outcomes of Patients Between Early Norepinephrine and Delayed Norepinephrine Before and After Propensity Score Matching |
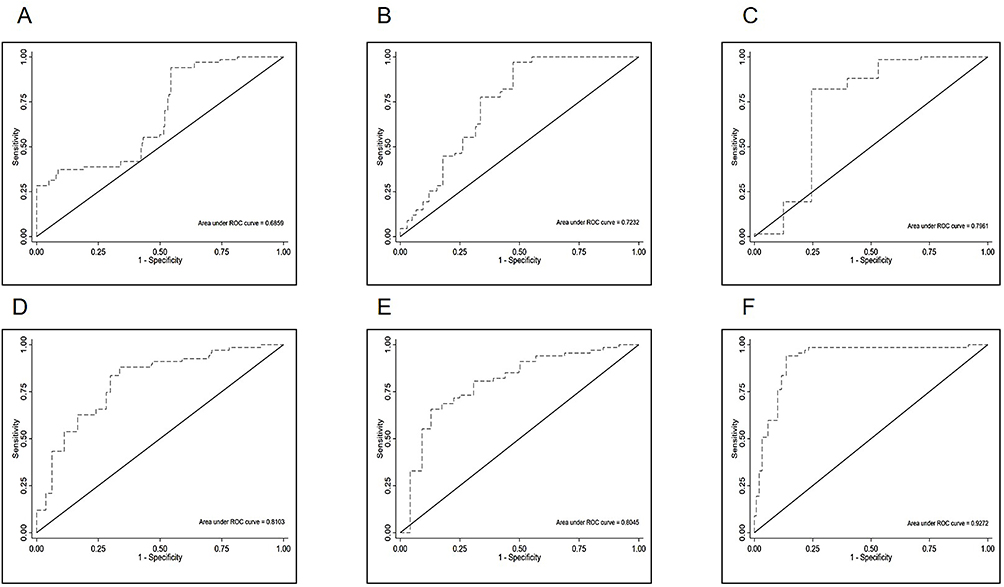 |
Figure 3 Receiver operating characteristic (ROC) curves of ISS score (A), APACHE III (B), SOFA score (C), Total of non-blood fluid infusion (D), Total of all fluid infusion (E), and Timing of NE use (F) for 24h mortality in patients with THS. Abbreviations: ISS, injury severity score; APACHE, acute physiology, age, chronic health evaluation; SOFA, sequential organ failure assessment; NE, norepinephrine. |
The Kaplan–Meier survival analysis of 24 h mortality showed that the survival rate of the eNE group was higher than that of the dNE group (P < 0.001) (Figure 4). The Streg regression model showed that the scores for ISS, APACHE III and SOFA; initial blood lactate, 24 h total of non-blood fluid infusion and dNE were significantly associated with 24 h survival (P < 0.05) (Table 3).
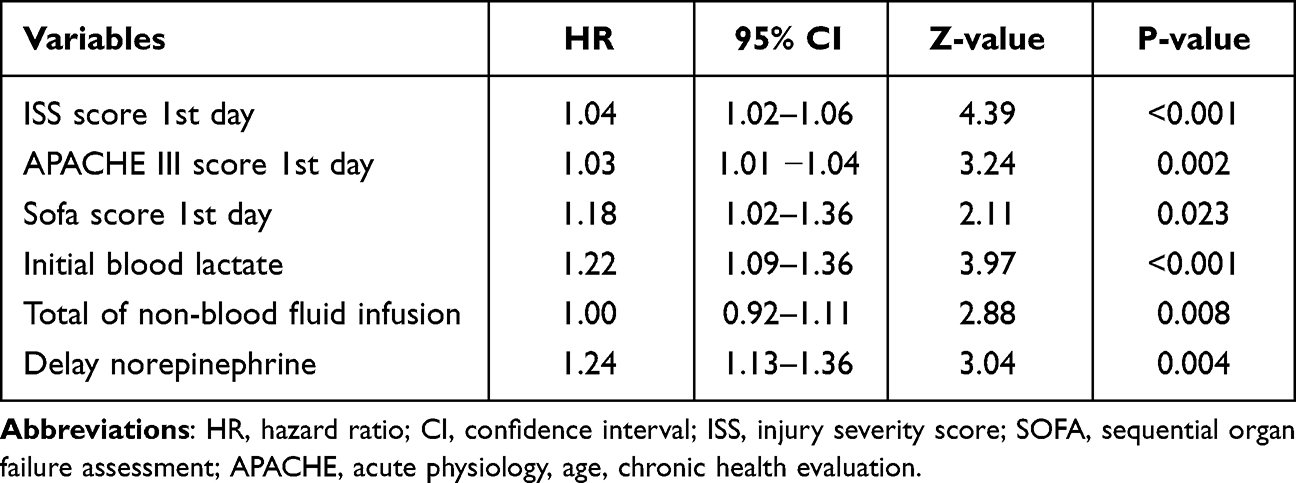 |
Table 3 The Streg Regression Model Analysis Based on Traumatic Hemorrhagic Shock Patients with 24 Hour-Mortality |
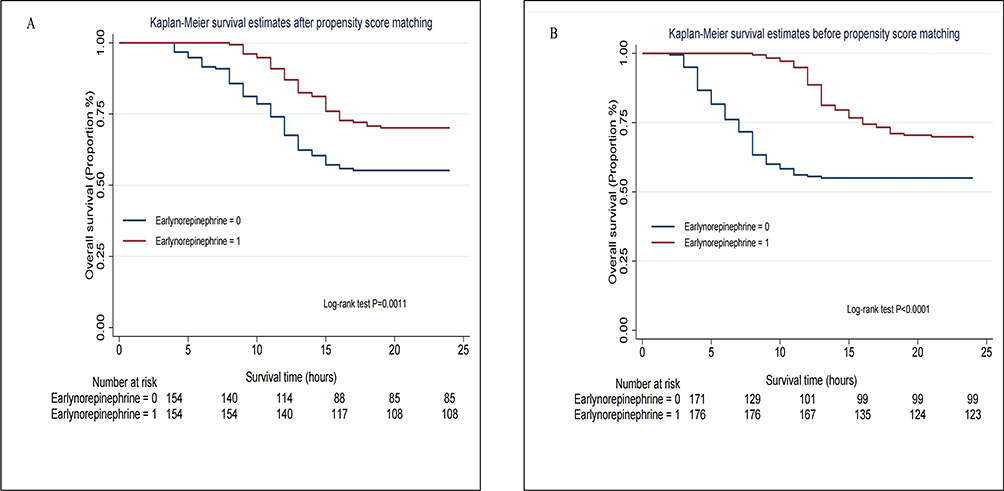 |
Figure 4 Kaplan-Meier survival estimates based on 24h mortality. After propensity score matching (A); Before propensity score matching (B). |
Secondary Study Endpoint
Regardless of PSM, compared with the dNE group, there was no significant difference in AKI incidence, HLOS, ICU LOS, duration of non-CRRT and non-IMV therapy and in-hospital mortality in the eNE group (P > 0.05) (Table 2).
Discussion
Early NE may be beneficial for the prognosis of patients with HS. However, the optimal timing of NE administration remains unclear. Our study showed that dNE was associated with a significant increase in 24 h mortality (OR = 1.30, P < 0.001). In addition, the Kaplan–Meier survival analysis of the pre-PSM and post-PSM cohorts showed that the patients in the eNE group had a higher survival rate after admission than those in the dNE group. The multivariate Streg regression analysis also showed that dNE was associated with a lower 24 h survival rate.
It has been found that trauma-induced haemorrhage and hypovolemia can trigger an intricate neurohormonal response.15 Thus, trauma-induced hypotension is associated not only with hypovolemia but also with sympathetic suppression-induced vasodilation.16 Vasopressor administration plays an important role in treating vascular paralysis and sustaining adequate perfusion pressure among patients with trauma and hypotension. Recent research has supported the biological plausibility of using NE for patients with trauma and HS.10 Haemorrhage is a time-dependent process, and its early recognition and management are critical. Our findings showed that eNE was associated with decreased mortality, which was consistent with previous studies. Poloujadoff et al17 found that NE infusion at a rate of 50 µg·100 g−1·h−1 within 75 minutes of traumatic HS significantly improved the survival rate of rats at 210 minutes. A recent study also showed that eNE was associated with increased short-term survival rates in patients with sepsis.18 Another retrospective study demonstrated that if the time from the onset of shock to the use of NE was more than 2 h, the 28 d mortality rate was significantly increased, and for each additional hour, mortality increased by 5.3%.19 Preliminary animal studies have shown that NE mainly acts as a vasoconstrictor, which can constrict arterial vessels and activate venous α-adrenergic receptors.20 This induces venous vasoconstriction, diverting splanchnic blood volume to the systemic circulation, while the activation of β2-adrenergic receptors reduces venous resistance and increases venous return.21 Recent data from an animal model showed improved survival after NE infusion, irrespective of a lower or higher blood pressure target.22
Therefore, we hypothesised that using eNE to improve hemodynamic status might have a positive effect on survival time. However, a few clinical trials have shown that eNE has no positive effect on the survival time of patients with traumatic HS10 or is even harmful.9 We believe that there might be selection bias, as the increased proportion of thoracotomies performed affects the hemodynamic status of patients and negatively impacts survival time. Additionally, other studies examined the combined exposure to any vasopressor, including phenylephrine, dopamine, vasopressin and NE. Furthermore, the grouping of the study population or the concentration of vasoactive drugs might have influenced the trial results. Singer et al23 found that higher maximum doses of NE were associated with increased mortality and that patients with trauma who commenced NE more than 24 h after injury may have a dire prognosis. Therefore, our study used a PSM analysis to reduce bias as much as possible and borrowed from the grouping method used by most studies.11–13
Our study found that eNE was not associated with a shorter ICU LOS, a shorter HLOS and a longer duration of non-IMV therapy. Animal studies have shown that the early administration of NE reduced blood loss and fluid requirements during MAP-directed fluid resuscitation in rats with HS.24 Other studies have also demonstrated eNE to be associated with less fluid infusion and improved outcomes.25,26 This is because, in critically ill patients, the higher the positive fluid balance, the worse the possible prognosis.17,27–30 Although there may be several reasons for the lower mortality in patients receiving eNE, the rapid restoration of blood flow in combination with lower fluid accumulation could restore tissue perfusion rapidly and avoid the harm caused by fluid overload.31 Our study found that eNE could reduce the time of target MAP need and reduce the 24 h total of all fluid infusion, especially that of 24 h total of non-blood fluid infusion. However, eNE was not beneficial in terms of lowering the risk of pulmonary oedema and congestive heart failure, improving respiratory function, shortening HLOS and reducing the duration of IMV therapy.
Our study also found that eNE did not reduce the incidence of AKI or shorten the duration of CRRT. Domizi et al32 found that high doses or a high frequency of NE could lead to serious complications, such as AKI or arrhythmia. A recent double-blind prospective study found that eNE neither caused AKI or serious cardiovascular events nor increased the duration of renal replacement therapy, although it might be beneficial for early fluid resuscitation in patients with shock.33 This interpretation was basically consistent with our findings. In addition, we also found that blood lactate levels were significantly reduced with eNE. Bai et al19 and Hernandez et al34 also found that after HS, blood lactate levels were significantly reduced at each time point of eNE.
Our results showed that higher SOFA and APACHE III scores, initial blood lactate levels, total non-blood fluid infusion and dNE were independent risk factors for 24 h mortality in patients with traumatic HS. This conclusion was basically consistent with those of recent studies.31,35,36
The highlights of our study are as follows: First, our research was the first to compare the effects of eNE versus dNE on the short-term outcomes of patients with traumatic HS. Second, we applied PSM to minimise selection bias and make the data from the early and delayed groups more comparable. Third, because the proportional hazards assumption of the Cox model did not hold, we used a Streg regression analysis to assess the association between eNE and 24 h survival.
Limitations
Our study has some limitations. First, the sample size of the study population was small, which might have led to selection bias. Second, although this study controlled for confounding factors by using PSM and a regression analysis, there might still be confounders. Finally, this was a retrospective study, although it was based on synthetic and abundant clinical data from high-level research university hospitals.
Conclusions
The use of NE within the first 3 h was associated with higher 24 h survival rates. The use of eNE appears to be a safe intervention that benefits patients with traumatic HS. Considering the conflicting evidence in the literature, there is a need for large-scale randomised controlled trials to investigate and clarify the potential clinical association of eNE use with survival among patients with traumatic HS.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Affiliated Hospital of Yangzhou University (2021-YKL3-01-001). Written informed consent was obtained from all participants.
Funding
Yong Li - Science and technology innovation cultivation fund of Yangzhou University (2019CXJ208). Jiangsu Province 333 High-level Talent. Training Project (BRA2020176). Funding agencies did not play a role in study design, data collection, analysis and interpretation, and manuscript writing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
2. Cothren CC, Moore EE, Hedegaard HB, Meng K. Epidemiology of urban trauma deaths: a comprehensive reassessment 10 years later. World J Surg. 2007;31(7):1507–1511. doi:10.1007/s00268-007-9087-2
3. Davenport RA, Guerreiro M, Frith D, et al. Activated protein C drives the hyperfibrinolysis of acute traumatic coagulopathy. Anesthesiology. 2017;126(1):115–127. doi:10.1097/ALN.0000000000001428
4. Maegele M, Lefering R, Yucel N, et al. Early coagulopathy in multiple injury: an analysis from the German trauma registry on 8724 patients. Injury. 2007;38(3):298–304. doi:10.1016/j.injury.2006.10.003
5. Hussmann B, Lefering R, Waydhas C, et al. Does increased prehospital replacement volume lead to a poor clinical course and an increased mortality? A matched-pair analysis of 1896 patients of the trauma registry of the German society for trauma surgery who were managed by an emergency doctor at the accident site. Injury. 2013;44(5):611–617. doi:10.1016/j.injury.2012.02.004
6. Harada MY, Ko A, Barmparas G, et al. 10-year trend in crystalloid resuscitation: reduced volume and lower mortality. Int J Surg. 2017;38:78–82. doi:10.1016/j.ijsu.2016.12.073
7. Joseph B, Azim A, Zangbar B, et al. Improving mortality in trauma laparotomy through the evolution of damage control resuscitation: analysis of 1030 consecutive trauma laparotomies. J Trauma Acute Care Surg. 2017;82(2):328–333. doi:10.1097/TA.0000000000001273
8. Spahn DR, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit Care. 2019;23(1):98. doi:10.1186/s13054-019-2347-3
9. Sperry JL, Minei JP, Frankel HL, et al. Early use of vasopressors after injury: caution before constriction. J Trauma. 2008;64(1):9–14. doi:10.1097/TA.0b013e31815dd029
10. Gauss T, Gayat E, Harrois A, et al. Effect of early use of noradrenaline on in-hospital mortality in haemorrhagic shock after major trauma: a propensity-score analysis. Br J Anaesth. 2018;120(6):1237–1244. doi:10.1016/j.bja.2018.02.032
11. Xu F, Zhong R, Shi S, Zeng Y, Tang Z. Early initiation of norepinephrine in patients with septic shock: a propensity score-based analysis. Am J Emerg Med. 2022;54:287–296. doi:10.1016/j.ajem.2022.01.063
12. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi:10.1007/s00134-017-4683-6
13. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
14. Mehta RL, Kellum JA, Shah SV, et al. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31. doi:10.1186/cc5713
15. Sims CA, Guan Y, Bergey M, et al. Arginine vasopressin, copeptin, and the development of relative AVP deficiency in hemorrhagic shock. Am J Surg. 2017;214(4):589–595. doi:10.1016/j.amjsurg.2017.06.015
16. Richards JE, Harris T, Dünser MW, Bouzat P, Gauss T. Vasopressors in trauma: a never event? Anesth Analg. 2021;133(1):68–79. doi:10.1213/ANE.0000000000005552
17. Poloujadoff MP, Borron SW, Amathieu R, et al. Improved survival after resuscitation with norepinephrine in a murine model of uncontrolled hemorrhagic shock. Anesthesiology. 2007;107(4):591–596. doi:10.1097/01.anes.0000281926.54940.6a
18. Li Y, Li H, Zhang D. Timing of norepinephrine initiation in patients with septic shock: a systematic review and meta-analysis. Crit Care. 2020;24(1):488. doi:10.1186/s13054-020-03204-x
19. Bai X, Yu W, Ji W, et al. Early versus delayed administration of norepinephrine in patients with septic shock. Crit Care. 2014;18(5):532. doi:10.1186/s13054-014-0532-y
20. Imai Y, Satoh K, Taira N. Role of the peripheral vasculature in changes in venous return caused by isoproterenol, norepinephrine, and methoxamine in anesthetized dogs. Circ Res. 1978;43(4):553–561. doi:10.1161/01.res.43.4.553
21. Gelman S, Mushlin PS, Weiskopf R. Catecholamine-induced changes in the splanchnic circulation affecting systemic hemodynamics. Anesthesiology. 2004;100(2):434–439. doi:10.1097/00000542-200402000-00036
22. Dunberry-Poissant S, Gilbert K, Bouchard C, et al. Fluid sparing and norepinephrine use in a rat model of resuscitated haemorrhagic shock: end-organ impact. Intensive Care Med Exp. 2018;6(1):47. doi:10.1186/s40635-018-0212-3
23. Singer KE, Kodali RA, Wallen TE, et al. The association of norepinephrine utilization with mortality risk in trauma patients. J Surg Res. 2022;280:234–240. doi:10.1016/j.jss.2022.06.042
24. Harrois A, Baudry N, Huet O, et al. Norepinephrine decreases fluid requirements and blood loss while preserving intestinal villi microcirculation during fluid resuscitation of uncontrolled hemorrhagic shock in mice. Anesthesiology. 2015;122(5):1093–1102. doi:10.1097/ALN.0000000000000639
25. Ranjit S, Natraj R, Kandath SK, Kissoon N, Ramakrishnan B, Marik PE. Early norepinephrine decreases fluid and ventilatory requirements in pediatric vasodilatory septic shock. Indian J Crit Care Med. 2016;20(10):561–569. doi:10.4103/0972-5229.192036
26. Byrne L, Obonyo NG, Diab SD, et al. Unintended consequences: fluid resuscitation worsens shock in an ovine model of endotoxemia. Am J Respir Crit Care Med. 2018;198(8):1043–1054. doi:10.1164/rccm.201801-0064OC
27. Vincent JL, Sakr Y, Sprung CL, et al. Sepsis occurrence in acutely ill patients investigators. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34(2):344–353. doi:10.1097/01.ccm.0000194725.48928.3a
28. Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med. 2011;39(2):259–265. doi:10.1097/CCM.0b013e3181feeb15
29. Sakr Y, Rubatto Birri PN, Kotfis K, et al. Intensive care over nations investigators. Higher fluid balance increases the risk of death from sepsis: results from a large international audit. Crit Care Med. 2017;45(3):386–394. doi:10.1097/CCM.0000000000002189
30. Marik PE, Linde-Zwirble WT, Bittner EA, Sahatjian J, Hansell D. Fluid administration in severe sepsis and septic shock, patterns and outcomes: an analysis of a large national database. Intensive Care Med. 2017;43(5):625–632. doi:10.1007/s00134-016-4675-y
31. Ospina-Tascón GA, Hernandez G, Alvarez I, et al. Effects of very early start of norepinephrine in patients with septic shock: a propensity score-based analysis. Crit Care. 2020;24(1):52. doi:10.1186/s13054-020-2756-3
32. Domizi R, Calcinaro S, Harris S, et al. Relationship between norepinephrine dose, tachycardia and outcome in septic shock: a multicentre evaluation. J Crit Care. 2020;57:185–190. doi:10.1016/j.jcrc.2020.02
33. Permpikul C, Tongyoo S, Viarasilpa T, Trainarongsakul T, Chakorn T, Udompanturak S. Early use of norepinephrine in septic shock resuscitation (CeNESER). A randomized trial. Am J Respir Crit Care Med. 2019;199(9):1097–1105. doi:10.1164/rccm.201806-1034OC
34. Hernandez G, Teboul JL. Is the macrocirculation really dissociated from the microcirculation in septic shock? Intensive Care Med. 2016;42(10):1621–1624. doi:10.1007/s00134-016-4416-2
35. Beck V, Chateau D, Bryson GL, et al; Cooperative Antimicrobial Therapy of Septic Shock (CATSS) Database Research Group. Timing of vasopressor initiation and mortality in septic shock: a cohort study. Crit Care. 2014;18(3):R97. doi:10.1186/cc13868
36. Sato R, Ariyoshi N, Hasegawa D, et al. Effects of inotropes on the mortality in patients with septic shock. J Intensive Care Med. 2021;36(2):211–219. doi:10.1177/0885066619892218
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.