Back to Journals » Open Access Emergency Medicine » Volume 15
Effect of Contact-Restricted Basic Life Support Training During the Nation’s Contact Restriction Policy on Learning Outcomes
Received 4 March 2023
Accepted for publication 29 April 2023
Published 9 May 2023 Volume 2023:15 Pages 157—164
DOI https://doi.org/10.2147/OAEM.S411096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Suhattaya Boonmak, Polpun Boonmak
Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, 40002, Thailand
Correspondence: Polpun Boonmak, Email [email protected]
Objective: Basic life support (BLS) training aimed at building knowledge and skills in cardiopulmonary resuscitation. During training, there is the possibility of airborne COVID-19 transmission. The aim was to evaluate students’ knowledge, skills, and course satisfaction following contact-restricted BLS training under the contact restriction policy.
Methods: From July 2020 to January 2021, a prospective, descriptive study was conducted among fifth-year dental students. Contact-restricted BLS training consisted of online learning, online pre-testing, non-contact training with automated real-time feedback manikins, and remote monitoring. The participants’ skills, knowledge through online testing, and course satisfaction were all evaluated after training. At three months and six months after training, their knowledge was re-evaluated through online testing.
Results: Fifty-five participants were included in this study. Their mean (SD) knowledge scores after training, at three and six months, were 81.5 (10.8)%, 71.1 (16.4)%, and 65.8 (14.5)%, respectively. The percentage of participants, who passed the skills test on their first, second, and third attempts had been 83.6%, 94.5%, and 100%, respectively. The mean (SD) satisfaction score with the course was 4.87 (0.34) on a five-point Likert score. After training, no participants had COVID-19 infection.
Conclusion: Training in contact-restricted BLS had produced acceptable knowledge, skills, and satisfaction results. Knowledge tests, competence tests, and course satisfaction were comparable to conventional pre-pandemic trainings with similar participants. Due to the significant dangers of aerosol disease transmission, it became a viable training alternative.
Trial Registration: TCTR20210503001 (Thai Clinical Trials Registry).
Keywords: basic life support training, contact restrictions, COVID-19 pandemic, evaluation, online learning
Plain Language Summary
We already know that basic life support (BLS) training aims to build knowledge and skills in cardiopulmonary resuscitation. Because of the possibility of airborne or contact transmission of COVID-19 during training, it is recommended that contact be restricted and that no equipment be shared. Such restrictions may limit the instructor’s ability to train students effectively. This study provides the data that contact-restricted BLS training consisting of online learning, non-contact training with an automated real-time feedback manikin, and remote monitoring during the COVID-19 pandemic resulted in satisfactory knowledge, skill, and course satisfaction outcomes. No participants had COVID-19 infection. It is comparable knowledge (immediate and long term), skill, and satisfaction with the previous study in similar participants and outcome measurement. This technique may be a viable option for BLS for health care provider courses in situations in which there is a high risk of aerosol transmission of disease.
Introduction
During cardiac arrests, cardiopulmonary resuscitation (CPR) assists patients until adequate medical treatment can be delivered.1 Training in Basic life support for healthcare providers (BLS) aims at building CPR knowledge, as well as developing skills in evaluation, chest compression, ventilation, and automated external defibrillator (AED) usage. In order to improve cardiac arrest survival outcomes, effective BLS education is critical.2 BLS training requires approximately 3–4 hours of combined knowledge and skills practice, including lessons in knowledge, video demonstrations, and instructor-led skills training.3,4 All participants receive training in simulated clinical settings. At the end of the course, the trainees take a skills performance test and a written examination. The expected outcomes are improved BLS skills, BLS knowledge, and affective (willingness to perform CPR), including high course satisfaction. Previous studies reported that after formal training, the scores of the students’ immediate knowledge had been between 73.3–83.4%, while knowledge retention appeared to have been reduced by between 9.6–15.4% at the three-month and six-month post-training periods, while the skill scores remained high.5–7 In a previous study, it was found that after training, the course satisfaction had been between 4.53–4.59 on a five-point Likert scale.5
During the Coronavirus disease 2019 (COVID-19) pandemic, the possibility of airborne transmission of COVID-19 existed during the training through contact transmission between students, instructors, and training materials. The pandemic recommendations were the restriction of contact and no sharing of equipment.8,9 However, the instructor was required to demonstrate, facilitate, observe, and provide feedback to the students during the skills training so that contact restrictions could be demolished. Online learning is a method of learning that integrates technology so that students can be given more flexibility to achieve their learning goals. It has offered opportunities for roles to be shifted during the pandemic, thus allowing self-directed learning and self-evaluation to be used as an alternative. Online learning showed comparable knowledge, skills, and course satisfaction with didactic lectures in traditional BLS training during the non-pandemic period.5 Instructor-led skills training can be replaced with automated real-time feedback CPR manikins, and the remote monitoring of the skills, which is an alternative that reduces contact.10
However, online learning requires access to hardware, a reliable internet connection, and computer literacy. In many Asian countries, education consists of teacher-centered didactic lectures that are aimed at passive learning.11 Little is known about the effects of conducting non-contact CPR trainings by using automated real-time feedback manikins and remote monitoring in combination with online learning, while following the contact restriction policy. The objective was to study the effects of contact-restricted BLS training on the knowledge, skills, and course satisfaction of learners, including knowledge retention, while following Thailand’s contact restriction policy. That makes it a feasible training option when there is the elevated risk of aerosol disease transmission. However, we did not evaluate their willingness to perform CPR because the severity of the COVID-19 pandemic may attenuate the result.
Materials and Methods
Study Design
This prospective descriptive study obtained Institute Review Board approval before the study commenced. The investigation was launched under Thailand’s COVID-19 policy of contact restriction. Its aim was to compare the outcomes with previous pre-pandemic formal BLS trainings. Therefore, fifth-year dental students were the participants, and the outcome measurements were compared to a previous study.5 The data was reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The study period was from July 2020 to January 2021 and was conducted at the Department of Anesthesiology at the Faculty of Medicine of Khon Kaen University under Thailand’s COVID-19 contact restriction policy.
Participants
We included 55 fifth-year Thai dental students (totally in their class) from the Khon Kaen University, Faculty of Dentistry, who attended a BLS for healthcare providers course at the Khon Kaen University, Faculty of Medicine’s Anesthesiology Department. The following individuals were excluded from the study: 1) those, who had taken a BLS course in the preceding six months; 2) those, who had physical limitations that precluded BLS training; and 3) those individuals, who had exhibited a history of COVID-19 risk. All subjects gave their written informed consent prior to their participation (Figure 1).
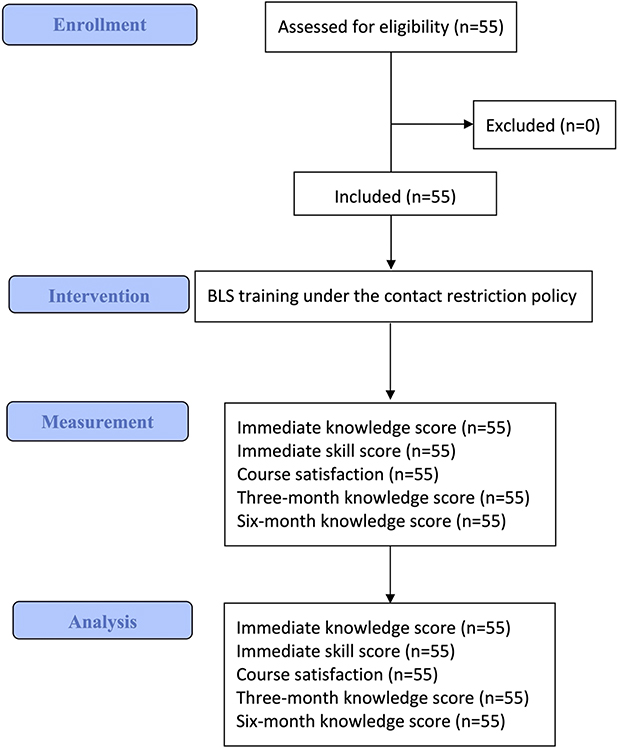 |
Figure 1 Study flow diagram. |
 |
Figure 2 Intervention diagram. |
Interventions
Contact-restricted BLS learning is composed of online learning and skills set training. Online learning was conducted by using the Google Classroom software (Google, USA), which required an Internet connection and was about 90 minutes in length. The content consisted of lessons focusing on BLS knowledge and video demonstrations of the skills. Topics included high-quality resuscitation, the chain of survival, evaluation for cardiac arrest, ventilation, compression, and AED usage based on 2020 American Heart Association Guidelines for CPR and ECC (see Appendix 1).1,3,4 Two weeks before the skills training, participants received a QR code, which could be used to attend the asynchronous online learning session. Also, to encourage participation, there was a pre-course assessment with 20 randomized true/false questions, which were resampled with every new attempt with unlimited attempts, and which was based on the learning objectives. A score of over 80% was required to complete the session. Moreover, the instructor would respond to any questions via chat room.
With the aim of upholding the contact restrictions, six participants were assigned to train simultaneously in each period on the skill training day. The participant’s body temperatures, COVID-19 symptoms, and COVID-19 risk history were screened. During the training, all contact restriction policies, including wearing facemasks, were deployed. All students installed the QCPR training application (Laerdal, Norway) on their smartphones and were trained on how to use the application so that their skills could be monitored during the training. The training session began with a 10-minute knowledge and skills summary briefing and a BLS skill demonstration video. This was followed by a question-and-answer period with an instructor in a 56 square meter conference training room. Then, six participants received a 40-minute skills training in an 80 square meter training room. The participants wore gloves during the training, and before the training, they cleaned their training equipment with 70% isopropyl alcohol. Each participant was assigned to his/her own station that was provided with a set of BLS manikins (Little Anne QCPR, Laerdal Medical, Norway), an AED trainer (Easyport trainer, Schiller, Switzerland), and a bag-mask unit (AMBU, Laerdal Medical, Norway) for the participants to use. The BLS manikins have automated real-time feedback on the learner’s ventilation (volume and rate) and chest compression (depth, position, and rate), including the steps of CPR, suggestions, and instructions on the participants’ smartphones. The training covered one rescuer resuscitation, bag-mask ventilation, chest compression, and AED usage (Appendix 1).3 During the exercise, one instructor remotely monitored learner performance via the QCPR® classroom application (Laerdal Medical, Norway). In addition, a large screen monitor could be seen by the instructor and the learners. On the screen, the information was shown from the instructor’s smartphone on which the QCPR® classroom application had been installed. At the same time, the participants received feedback on their performance on CPR steps, ventilation, chest compression, and AED usage from the QCPR training application. After the training, each participant once again disinfected the training equipment. Using the same protocol, ten groups with six participants each were consecutively trained (Figure 2).
Outcomes and Measurement
The knowledge and the skills of all the participants were evaluated after the training. Instructors (who did not participate in the training session) directly observed the participants’ management of a simulated unresponsive adult patient and evaluated the skills of the participants using a standard checklist for BLS skills evaluation (Appendix 1).3 They were assessed on managing patient consciousness, breathing and circulation, and AED usage. Those participants, who were able to perform all the procedures correctly, passed. Any participants, who initially failed, were given the opportunity to repeat the test until they passed. The participants’ knowledge was assessed using a 25-question multiple-choice test (100 points) based on specific BLS guidelines following the learning objectives of the previous study (Appendix 1)5 on their smartphones with Google Forms (Google, USA). Immediately after the testing, the overall course satisfaction, online learning satisfaction, and skill training satisfaction were evaluated by using a five-point Likert-type scale (1 = Very dissatisfied, 2 = Dissatisfied, 3 = Neither satisfied nor dissatisfied, 4 = Satisfied, and 5 = Very satisfied). The participants’ genders and ages were also recorded. At three months after training and six months after training, the participants were given another multiple-choice test consisting of 25 questions. Both the three-month and six-month post-test covered the same content as the first test and had a total score of 100 points. Incidences of COVID-19 infection among the participants were also recorded at two weeks.
Statistical Methods
Data analysis was performed using STATA/SE 10.0 for Macintosh (Stata Corporation, TX, USA). Descriptive statistics were used to describe the participant characteristics. The categorical data was summarized as percentages and frequencies, and the continuous data as means and standard deviations. Proportions were calculated based on the number of participants with non-missing data. Knowledge scores and satisfaction scores were reported as means (SD). A one-sample t-test was utilized to compare the retention of knowledge scores. The required sample sizes were calculated based on an immediate post-training knowledge score of 74.8 with an SD of 7.8, which was also examined with similar participants during the pre-pandemic period.5 To detect a 5% difference in knowledge score (Type I error of 0.05) with a power of 90%, it was determined that a sample size of 50 participants would be required.
Results
Participant Characteristics
Fifty-five fifth-year dental students were included in the study (the total number in their class). Their mean (SD) age was 22.5 (0.6), while 74.6% were female. Before the training, no participants were found to have a COVID-19 infection. In this study, there was no missing data. Knowledge, skills, and course satisfaction after BLS training were shown in Table 1. Two weeks after the training, none of the participants or instructors had COVID-19 infections.
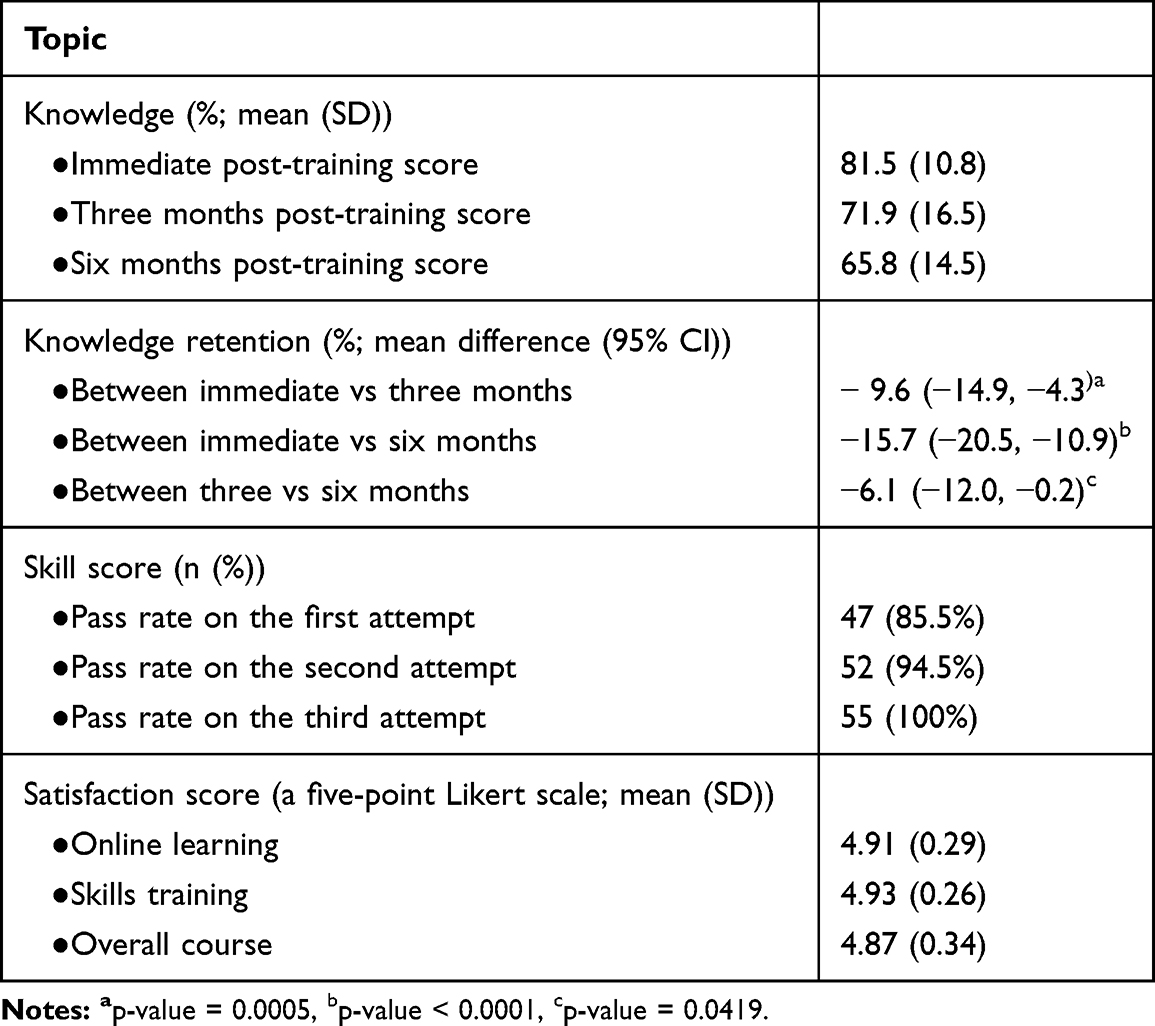 |
Table 1 Knowledge, Skills, and Course Satisfaction After BLS Training (N=55) |
Discussion
This study found that contact-restricted BLS learning, which was a combination of online learning along with automated real-time feedback skill training, had resulted in acceptable scores on the knowledge and skill tests, as well as on the course satisfaction of dental students. However, it was found that knowledge retention had reduced at three months and six months after the trainings. Although a descriptive study was conducted, this study’s method was similar to a previous study, which was conducted with 39 fifth-year dental students and had similar outcome measurements in a formal pre-pandemic BLS training.5 After making a comparison, the learning outcomes of the BLS training under the contact restrictions were comparable. The mean (SD) of the immediate post-training knowledge score for the contact restriction group and the formal group were 81.5 (10.8) vs 74.8 (7.8), respectively. The percentage of participants in the pandemic and formal groups, who passed their first and second attempts at skills testing, were 85.5% vs 53.8% and 94.5% vs 100%, respectively. At the same time, the mean (SD) of the knowledge retention score at the three-month point in the pandemic group and the formal group had been 71.9 (16.5) vs 65.2 (8.1), respectively. The mean (SD) of the satisfaction scores for the course in the pandemic group versus the formal group were 4.87 (0.34) vs 4.59 (0.55). Other comparable outcomes were also found in previous studies.6,7
Currently, the BLS training has been adjusted to account for the pandemic restrictions. During the pandemic, the training recommendations consisted of maintaining social distancing, reducing droplet diffusion, and alleviating learners’ fears of virus transmission.12 When it is not feasible to make direct contact, online learning is an alternative method of providing and evaluating knowledge that can be accessed outside of the classroom and can provide self-assessment before the formal class sessions.13 The International Liaison Committee on Resuscitation recommends using self-directed or digitally-based BLS education that can be implemented via any digital platform, such as videos, phone applications, the Internet, virtual reality, or augmented reality, which may serve as an alternative to training in the presence of a BLS instructor.4 Narrative reviews have been conducted regarding the effectiveness of online learning in improving CPR skills. However, these studies found that the method has limitations in the area of skills assessment.
Manikins, which are capable of automated real-time feedback, can effectively assist in improving skills and overall performance. The feedback, which these manikins can provide to participants during BLS trainings, has resulted in better compression performance than instructor feedback-based training.10,14,15 By using a manikin, which is equipped with a feedback device, it has been shown that self-directed learning is an effective method in gaining the knowledge and skills in trainings with lay adults, as is shown in this study.10 During the period of contact restrictions, this system was valuable.
In situations, such as in the current pandemic, in which there is an elevated risk for aerosol transmission of disease, contact restriction is necessary during BLS trainings for the safety of both instructors and learners. To facilitate adequate social distancing, each participant requires at least five square meters of space during skills training. Such restrictions limit the number of participants, who can make up each section, which necessitates an appointment-based management system for scheduling classes. Therefore, the participants are appointed a specific training time. In order to reduce contact, online learning (Google Classroom), knowledge testing (Google Forms®), and communication (Line®) methods were employed in this study. In addition, COVID-19 screening was conducted via mobile phones and near-infrared thermometers. Participants cleaned the training area and equipment before and after the training to reduce contamination. During the training, the participants did not make contact with one another. The manikins, which are capable of providing automated feedback, were also used to facilitate self-directed learning. BLS training by self-directed remote online-only learning and deliberate practice was reported to be comparable to the conventional classroom-based instructor-led method.16
Given that there are some limitations, the findings of this study should be interpreted with caution. Our study design was a prospective, descriptive study due to the limitations imposed by the pandemic. Given the ethical considerations, a formal course could not be performed, and a control group, could not, therefore, be included. However, the outcomes were compared with a pre-pandemic study, which reported comparable results with similar participants. The skills test was not repeated due to Thailand’s COVID-19 contact restriction policy. Since our participants were not randomly chosen, another limitation was selection bias. Therefore, caution must be exercised when generalizing these results to non-randomly selected participants. Finally, the study was exclusively conducted with Thai dental students during the COVID-19 pandemic, so these outcomes may not be applicable in other situations or for other populations.
It was found that contact-restricted BLS training with the contact restriction had yielded satisfactory knowledge, skills, and satisfaction outcomes. These outcomes were comparable to other formal pre-pandemic BLS trainings. This technique may be a viable option for BLS courses in situations in which there is an elevated risk for the aerosol transmission of diseases. Despite this, it was found that conducting BLS trainings under contact restrictions had provided satisfactory learning outcomes and that conducting trainings in this manner may be adopted for other populations during a pandemic. However, we recommend a further randomized controlled study to compare the two interventions during non-pandemic conditions. A larger sample size is required to ensure a distribution representative of general students or the entire population. A survey of the long-term outcomes of knowledge and skills retention, including willingness to perform CPR by this learning technique, needs to be conducted. Finally, the knowledge and skills acquired during training may not reflect the same during actual BLS performance. We recommend further study that focuses upon the willingness to perform BLS in the actual situation.
Conclusion
In terms of knowledge, skills, and course satisfaction among participants, the use of a contact-restricted BLS training yielded acceptable short-term outcomes. After the training, the knowledge and skills were also comparable to previous pre-pandemic studies conducted with similar outcomes. However, the assessment of the long-term effects, such as knowledge and skills retention, requires further study.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The institutional review board (Centre for Ethics in Human Research at the Khon Kaen University in Thailand) approved this study (Registration number: HE631380). Prior to beginning the study, all participants consented to participate.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding.
Disclosure
The authors declare that there were no conflicts of interest.
References
1. Olasveengen TM, Mancini ME, Perkins GD, et al.; Adult Basic Life Support Collaborators. Adult basic life support: international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2020;156:A35–A79. doi:10.1016/j.resuscitation.2020.09.010
2. Yan S, Gan Y, Jiang N, et al. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care. 2020;24:61. doi:10.1186/s13054-020-2773-2
3. American Heart Association (AHA). Basic life support (BLS) project team, editors. Basic life support (BLS): instructor manual. American Heart Association; 2016.
4. Cheng A, Magid DJ, Auerbach M, et al. Part 6: resuscitation education science: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(16 suppl 2):S551–S579. doi:10.1161/CIR.0000000000000903
5. Boonmak S, Plailaharn N, Sripadungkul D, Somjit M, Gaysonsiri D, Boonmak P. A randomized controlled, non-inferiority trial of Moodle online learning for basic life support training on learning outcomes among dental students. J Dent Educ. 2023;87(1):110–117. doi:10.1002/jdd.13089
6. Pande S, Pande S, Parate V, Pande S, Sukhsohale N. Evaluation of retention of knowledge and skills imparted to first-year medical students through basic life support training. Adv Physiol Educ. 2014;38(1):42–45. doi:10.1152/advan.00102.2013
7. Srivilaithon W, Amnuaypattanapon K, Limjindaporn C, Diskumpon N, Dasanadeba I, Daorattanachai K. Retention of Basic-life-support knowledge and skills in second-year medical students. Open Access Emerg Med. 2020;12:211–217. doi:10.2147/OAEM.S241598
8. Ali DM, Hisam B, Shaukat N, et al. Cardiopulmonary resuscitation (CPR) training strategies in the times of COVID-19: a systematic literature review comparing different training methodologies. Scand J Trauma Resusc Emerg Med. 2021;29(1):53. doi:10.1186/s13049-021-00869-3
9. Wyckoff MH, Singletary EM, Soar J, et al.; COVID-19 Working Group. 2021 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: summary from the basic life support; advanced life support; neonatal life support; education, implementation, and teams; first aid task forces; and the COVID-19 working group. Resuscitation. 2021;169:229–311. doi:10.1016/j.resuscitation.2021.10.040
10. Cortegiani A, Russotto V, Montalto F, et al. Use of a real-time training software (Laerdal QCPR®) compared to instructor-based feedback for high-quality chest compressions acquisition in secondary school students: a randomized trial. PLoS One. 2017;12(1):e0169591. doi:10.1371/journal.pone.0169591
11. Olaniran BA, Rodriguez NB, Williams IM. Cross-cultural challenges in web-based instruction. Knowl Manag ELearn. 2010;2:448–465. doi:10.34105/j.kmel.2010.02.032
12. Baldi E, Contri E, Savastano S, Cortegiani A. The challenge of laypeople cardio-pulmonary resuscitation training during and after COVID-19 pandemic. Resuscitation. 2020;152:3–4. doi:10.1016/j.resuscitation.2020.04.040
13. Lactona ID, Suryanto S. Efficacy and knowledge of conducting CPR through online learning during the COVID-19 pandemic: a literature review. J Public Health Res. 2021;10(2):2208. doi:10.4081/jphr.2021.2208
14. Kim Y, Han H, Lee S, Lee J. Effects of the non-contact cardiopulmonary resuscitation training using smart technology. Eur J Cardiovasc Nurs. 2021;20(8):760–766. doi:10.1093/eurjcn/zvaa030
15. Tanaka S, Tsukigase K, Hara T, et al. Effect of real-time visual feedback device ‘Quality Cardiopulmonary Resuscitation (QCPR) Classroom’ with a metronome sound on layperson CPR training in Japan: a cluster randomized control trial. BMJ Open. 2019;9(6):e026140. doi:10.1136/bmjopen-2018-026140
16. Chong KM, Yang HW, He HC, et al. The effectiveness of online-only blended cardiopulmonary resuscitation training: static-group comparison study. J Med Internet Res. 2023;25:e42325. doi:10.2196/42325
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.