")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Effect of Balneotherapy on Skin Lesion at Hot Springs in Southern Ethiopia: A Single-Arm Prospective Cohort Study
Authors Gebretsadik A
Received 23 March 2023
Accepted for publication 15 May 2023
Published 17 May 2023 Volume 2023:16 Pages 1259—1268
DOI https://doi.org/10.2147/CCID.S413926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Achamyelesh Gebretsadik
School of Public Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Southern Nation Nationalities People Region, Ethiopia
Correspondence: Achamyelesh Gebretsadik, School of Public Health, Hawassa University, P.O. Box 1466, Hawassa, Ethiopia, Tel +251 911303128, Email [email protected]
Background: Balneotherapy is the use of mineral water for the treatment of a wide range of diseases including skin lesions. Even though Ethiopia has a large number of places with natural hot springs, their therapeutic value has not been thoroughly studied. The aim of this study was to determine the effect of balneotherapy among patients with skin lesions at hot springs in southern Ethiopia.
Methods: A single-arm prospective cohort study design was used to assess patient’s progress from their skin lesion complaint after using the hot water for at least three consecutive days or more. An individual visiting the hot springs site and staying there for at least three days or more was included in the study. From four hot springs sites in Southern Ethiopia, 1320 study participants who were 18 years of age or older were enrolled. The data were gathered using a standardized questionnaire and a physical examination. A descriptive analysis was made.
Results: Of the total, 142 (10.8%) of them had various skin lesions. Flexural lesions accounted 87 (61.3%), non-specific skin conditions 51 (35.9%), co-lesions at the scalp, external ear canal, trunk, and various locations, and psoriatic lesions comprised 4.8%. There were 72 (82.8%) typical eczematous lesions among the total number of flexural lesions. After using balneotherapy for 3– 7 days once daily, 69 (95.2%) cases of eczematous dermatitis and 30 (58.8%) cases of non-specific skin issues showed improvement from the lesion. Additionally, after 30 days of bathing once daily, the PASI score of more than 90% of the psoriatic cases dropped to a score of one.
Conclusion: Patients with skin lesions benefit significantly from balneotherapy when it lasts for three or more days. In order to improve skin lesions, proper application for at least a week or longer is highly beneficial.
Keywords: balneotherapy, hot springs, skin lesion, southern Ethiopia
Background
A wide range of illnesses, including atopic dermatitis (AD), psoriasis, and all other dermatologic disorders, can be treated with balneotherapy, which uses mineral water. The world has been using it for a very long time. These disorders might vary in their nature and clinical symptoms. However, they are all chronic and inflammatory diseases.1
The widespread disease known as eczematous dermatitis can affect one’s ability to work, sleep, and interact with others in social situations. Atopic dermatitis, also known as eczema, contact dermatitis, dyshidrotic eczema, stasis dermatitis, and neurodermatitis are examples of prevalent forms. For patients, its persistence and accompanying pruritus can be distressing and irritating.2
A widespread chronic inflammatory skin disorder called psoriasis is characterized by periodic flare-ups and remissions of plaques that are thick, erythematous, and scaly. Due to the interaction between certain genetic predispositions and environmental circumstances, it is a complex disease.3 In terms of the therapy, it aims to normalize the skin by reducing or eliminating scales, papules, and erythema. Both pharmaceutical and non-pharmacologic treatments are used in the therapeutic strategies.4,5
Balneotherapeutic effects of mineral waters depend on their composition. Sulfur waters may contain various combinations of sulfur ions, water, and other ions. It has anti-inflammatory, keratoplasty, antipruritic, antibacterial and antifungal effects. The therapeutic action is related to sulfur’s keratolytic effect, resulting in peeling.6
The relapsing and remitting nature of the inflammation is an issue during treatment for both eczematous and psoriatic lesions. Therefore, evaluation of non-pharmacologic therapeutic modalities is required in order to carefully pick the therapy while taking into account potential long-term negative effects.3,7
Balneotherapy centers are promoted in a few select locations around the globe. These include the Dead Sea, the Blue Lagoon in Iceland, and the Kangal hot spring in Turkey. The dead sea is the only one of the three that contains salt, is below sea level, and can improve exposure to a natural light source.8 Even though Ethiopia has a large number of places with natural hot springs, their therapeutic value has not been thoroughly studied. Therefore, the aim of this study was to assess the effect of balneotherapy in treating skin lesions in southern Ethiopia.
Methods
This study is a portion of earlier studies that examined the effects of balneotherapy in treating persistent low back and musculoskeletal pain. Details of the procedure section were made available in that article.9,10
The study was carried out at the southern Ethiopian hot springs of Bersiso (Dilla woreda), Yirgalem (Yirgalem Town), Burkitu (Hawassa City), and Wondo (Wondo woreda). Because of this, the qualities of the hot spring water were first determined using physico-chemical tests. The medicinal element and ion composition of the hot springs were considered when choosing them. These hot springs were situated in East Africa’s Great Rift Valley.All those who sought balneotherapy in hot springs in southern Ethiopia during the study period were considered the source population. The study sample consisted of adults (18 years or older) who used balneotherapy in the chosen hot springs in southern Ethiopia between March and October 2019.
I have taken into account those people who wanted to stay in a hot spring for at least three consecutive days to track any improvements in their symptoms after seeking treatment there for a health issue. Under-age participants were prohibited for moral reasons. A further exclusion was made for guests who came to the hot springs in search of refreshments. A total of 1320 study participants who were 18 years of age or older were enrolled during the study period.
Data Collection and Analysis
The data were collected using a standardized questionary and physical examination. A questionnaire that covers the signs and symptoms required to diagnose dermatologic disorders along with sociodemographic information of the respondents were designed. A 5% of respondents from another hot spring (Alaba site) were used for pre-testing the tool, which was then changed as necessary. For each target site, three data collectors and one supervisor were assigned. The selection of the data collection team was based on their level of education (at least a medical degree by profession) and their understanding of the local Sidamu Afo and Amharic languages. Data collectors and supervisors received two days of training prior to the data collection. The doctors who gathered the data and performed the physical examination using the standard techniques then classified the dermatologic conditions. When being examined physically, if significant characteristics of typical eczematous lesions, such as pruritus, eczema, and a chronic or recurring history are present, flexural lesions present or past at any age, groin and axillary region were spared and are considered typical eczematous lesions. Psoriasis Area and Severity Index (PASI) score were used to determine the body surface area affected by psoriasis, severity of erythema, induration and scaling. The severity was consequently split into three categories: mild, moderate and severe. Other lesions were labeled as having a nonspecific dermatologic disorder.
Epi Data software version 3.1 was used to enter the data, which was then moved to SPSS software version 25 for analysis. SPSS was used for data cleaning, recoding, and analysis. Dermatological issues in patients receiving balneotherapy were evaluated using descriptive statistics, and the data were classified by identifying the symptoms that were or were not addressed by balneotherapy and taking the time that had passed into account.
Definitions
Balneotherapy (bathing in hot water): is a type of therapy that aims to reduce pain and improve daily functioning. Balneotherapy often takes place at centers with thermal baths or sea water baths.
Balneology: is the scientific study of the therapeutic benefits of naturally occurring mineral waters.
Skin lesions: are categorized as eczematous dermatitis, psoriasis, or nonspecific dermatologic lesions based on how they appear on the skin on any area of the body.
PASI: Psoriasis Area and severity index.
Results
Socio-Demographic Characteristics
Of the total, 1320 participants 142 (10.8%) patients who visited the hot springs had skin problems. The mean age of these patients were 44.1 years and ±16.5, with 63 (44.3%) of them being under 40. Among all patients with skin lesions, 96 (67.6%) were from rural areas, 73 (51.4%) were men, 115 (81%) were married, 56 (39.4%) were illiterate and 72 (50.7%) had an annual income of less than a thousand Ethiopian birrs. Table 1.
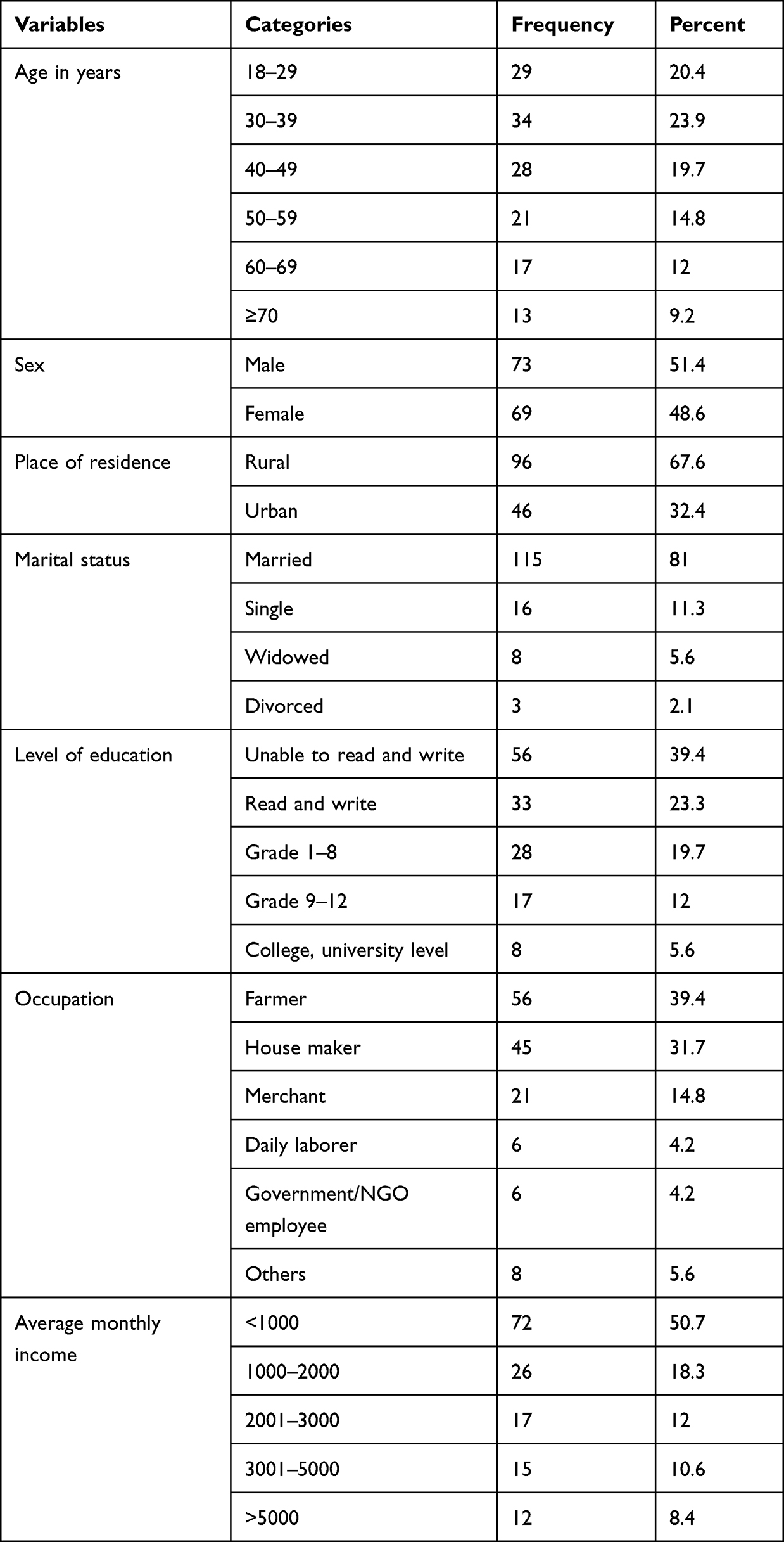 |
Table 1 Socio-Demographic Characteristics of Patients Who Used Balneotherapy in Southern Ethiopia 2019 N=142 |
Frequency of Visiting the Hot Springs and Duration of Use
The overall mean duration of stay at the site of the hot springs was 4 ±3 days. A total of 91 (64.1%) patients used the hot springs for three days and had plans to continue doing so for the next three days. Of all participants with skin lesions 53 (37.3%) visit the hot spring sites annually, while 38 (26.7%) participants only go when they need it. Table 2.
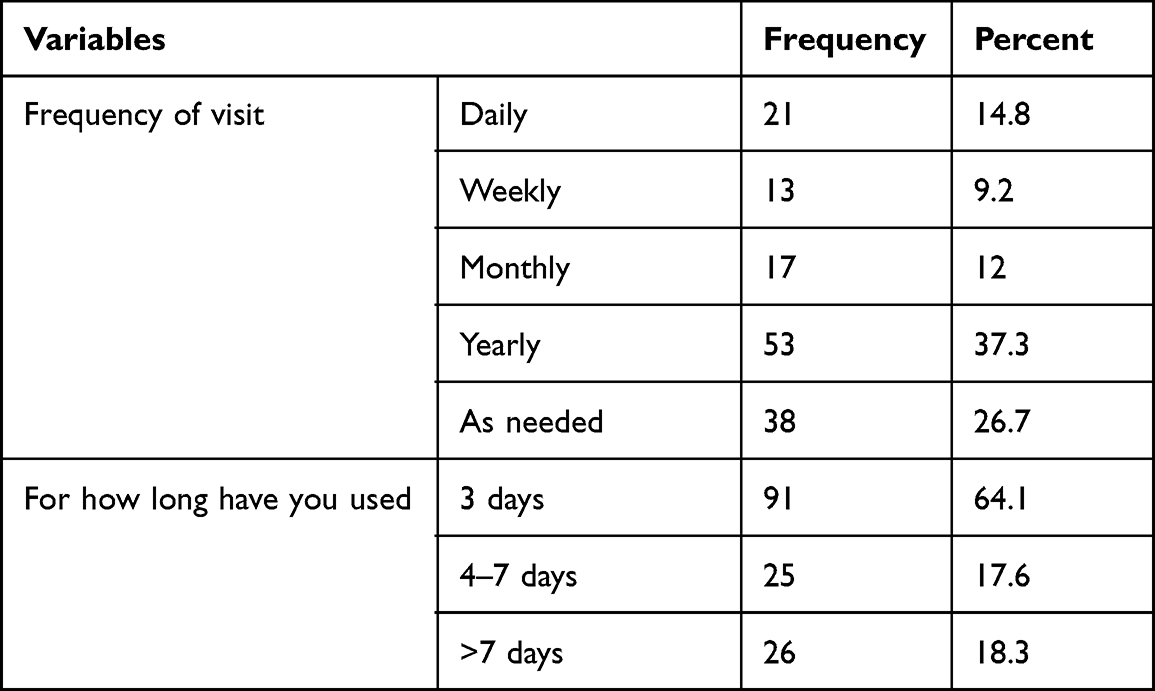 |
Table 2 Frequency of Visits and Duration of Stay Among Dermatologic Patients Who Use Balneotherapy in Southern Ethiopia 2019. N=142 |
Dermatologic Problems of Patients Who Used Balneotherapy
Of total, 142 (10.8%) patients who reported skin problems, flexural lesions accounted for 87 (61.3%), non-specific skin conditions 44 (31%), co-lesions at the scalp, external ear canal, trunk, and various locations, and psoriatic lesions comprised 11 (7.7%). These 108 (76.1%) people with pruritus are symmetrical in 88 (62%) cases, have lesions on their feet in 40 (28.2%), and have internal and exterior surfaces on their hands in 35 (24.6%) cases. Out of the total flexural lesions, there were 72 (82.8%) typical eczematous lesions. Table 3.
 |
Table 3 Characteristics of Skin Problems Among Patients Who Used Hot Springs in Southern Ethiopia 2019. N=142 |
Other Dermatologic Problem
Psoriasis Area and Severity Index (PASI), a numerical rating score for grading the severity of psoriatic lesions done based on the area covered and plaque appearance. The result revealed that a total of 11 (7.7%) individuals had psoriasis at the time of the initial examination. Both the lower 6/11 (54.5%) and upper 5/11 (45.5%) limbs of patients showed erythema with severe to very severe induration and scaling. Table 4.
 |
Table 4 Initial Assessment of Psoriasis Area and Severity Index (PASI) Among Patients Who Used Balneotherapy in Southern Ethiopia 2019. N=142 |
Follow-up assessments were done after three or more days of using the hot bath while the patients were ready to leave the hot springs site. Accordingly, the Erythematic, induration, and scaling characteristics of the lesion showed visible improvement to slight to a moderate level on the upper and lower limbs. Table 5.
 |
Table 5 Follow-Up Assessment of Psoriasis Area and Severity Index (PASI) Among Patients Who Used Balneotherapy in Southern Ethiopia in 2019. N=142 |
The majority of study participants who underwent balneotherapy reported complete relief from their problems in 104 (73.2%) cases, partially improved in 26 (18.3%), and no change in 12 (8.5%) cases. After three days of minimal usage, the patients were re-interviewed and monitored to determine the status of the hot bath’s beneficial effect. After using balneotherapy for 3–7 days once daily, 30 (68.2%) cases of non-specific skin problems and 62 (86.1%) cases of eczematous dermatitis showed improvement from the lesion. Additionally, more than 90% of the psoriatic cases’ PASI scores decreased to a score of one after 30 days of taking a once-daily bath. Table 6.
 |
Table 6 Duration of the Hot Bath and Therapeutics Effects Among Patients Who Used Balneotherapy in Southern Ethiopia, 2019. N=142 |
Discussion
Following balneotherapy, the symptoms of sixty-eight cases of eczematous dermatitis and thirty-four cases of nonspecific skin conditions were alleviated. This could be explained by the hot spring water’s chemical makeup and temperature, as it has been noted that mineral waters, particularly salty and sulfurous waters, are particularly beneficial for therapeutical dermatological applications because of their keratolytic, regenerative, and antioxidant effects.11,12 Additionally, taking mineral baths at various temperatures can eliminate microbial peptides that are the source of many skin conditions, reduce inflammation, enhance microcirculation, control immunological functions, and improve quality of life.13,14 These positive benefits of thermal waters, which have been supported by several clinical trials, are connected to either the regulation of skin temperature or the absorption of minerals by the skin.15
All eleven patients with psoriasis improved from a PASI of 4.4 to 0.4 after 30 days of taking a bath at the hot springs in southern Ethiopia. This is consistent with research done at Prolom Spa in Serbia, which revealed a decrease in PASI score after taking mineral water for a period of four weeks.16 In a different study, peloids, algae, and mineral baths were used to treat 55 psoriasis patients in Argentina at the Copahue thermal complex. For an average of 10 days, the patients bathed twice daily in mineral water. Their lessened erythema and desquamation indicated improvement.17
Limitations
Different skin conditions are included in the situations that we classify as eczematous dermatitis and non-specific skin diseases. It is therefore preferable to examine how balneotherapy affects each individual condition within this broad diagnosis.
The study included the use of the PASI score, which is intended to track changes in the components over the course of a week. But to evaluate the onset of the lesion and track change throughout the course of the study, I conducted an interview based on the skin’s current condition. Therefore, additional cohort studies with a longer data collecting time and patient recruitment from the healthcare facilities are needed.
Conclusion
The hot spring bath for three and more days has significant therapeutic effects among patients with dermatologic problems including psoriatic lesions.
Patients with eczematous dermatitis and nonspecific skin conditions need to consider hot spring bath therapy. Since soaking in a hot spring is a low-cost, all-natural treatment with no adverse effects. It would be wise to take additional research that takes into account more hot springs into consideration to help support the conclusion.
Ethical Consideration
Ethics were approved by the Institutional Review Board (IRB) of the College of Medicine and Health Sciences at Hawassa University. This item’s reference number is IRB/041/19. The respondents’ verbal consent was obtained prior to data collection. The owners of the hot springs then consented. Because there are no invasive procedures involved in this study, the Institutional Review Board of the College of Medicine and Health Sciences at Hawassa University acknowledged and approved verbal consent. Furthermore, this study is done in accordance with the Helsinki Declaration.
Acknowledgment
The author wishes to express thanks to Hawassa University, Research and technology transfer directorate office for the financial supportThe author is also extremely grateful to those patients who participated in this study for their willingness to share their health status.
Funding
The author received no specific funding for this study.
Disclosure
The author reports no conflict of interest in this work.
References
1. Routh HB, Bhowmik KR, Parish LC, Witkowski JA. Balneology, mineral water, and spas in historical perspective. Clin Dermatol. 1996;14:551–554. doi:10.1016/S0738-081X(96)00083-1
2. Zug KA, McKay M. Eczematous dermatitis: a practical review. Am Fam Physician. 1996;54(4):
3. Ghersetich I, Lotti T, Lotti T. Balneology today. J Eur Acad Dermatol Venereol. 2000;14:346–348. doi:10.1046/j.1468-3083.2000.00136.x
4. Lebwohl M, Ali S. Treatment of Psoriasis.Part 2, Systemic Therapies. J Am Acad Dermatol. 2001;45:649–661. doi:10.1067/mjd.2001.117047
5. Scott SA, Martin III RW. Scaly dermatoses. In: Berardi RR, McDermott J, Newton GD, editors. Handbook of Nonprescription Drugs.
6. Matz H, Orion E, Wolf R. Balneotherapy in dermatology. Dermatol Ther. 2003;16:132–140. doi:10.1046/j.1529-8019.2003.01622.x
7. Dennis P, Lee E, Scuderi L, Micali G. Psoriasis; dermatologic disorders in pharmacotherapy; 2020:1813–1827.
8. Hodak E, Segal T, Segal T, et al. Climatotherapy at the Dead Sea is a remittive therapy for psoriasis: combined effects on epidermal and immunologic activation. J Am Acad Dermatol. 2003;49:451–457. doi:10.1067/S0190-9622(03)00916-2
9. Yusuf H, Simegn S, Serka S, Gebretsadik A. Effect of balneotherapy on chronic low back pain at hot springs in southern Ethiopia: perceived improvements from pain. J Pain Res. 2021;14:2491–2500. doi:10.2147/JPR.S322603
10. Achamyelesh G, Fiker T, Nebiyu M, Yusuf H. Balneotherapy for musculoskeletal pain management of hot spring water in southern Ethiopia: perceived improvements. J Health Care Org Prov Financ. 2021;58:1–7.
11. Bacle I, Meges S, Lauze C, Macleod P, Dupuy P. Sensory analysis of four medical spa spring waters containing various mineral concentrations. Int J Dermatol. 1999;38:784–786. doi:10.1046/j.1365-4362.1999.00789.x
12. Soroka Y, Ma’or Z, Leshem Y, et al. Aged keratinocyte phenotyping: morphology, biochemical markers and effects of Dead Sea minerals. Exp Gerontol. 2008;43:947–957. doi:10.1016/j.exger.2008.08.003
13. Duvic M. Possible mechanisms of effectiveness of Dead Sea balneotherapy. J Am Acad Dermatol. 1986;15:1061. doi:10.1016/S0190-9622(86)80320-6
14. Bogdanov I, Kircheva K, Miteva L, Tsankov N. Quality of life in patients undergoing combined climatotherapy and phototherapy. Rom Med J. 2012;59:251–254.
15. Nunes S, Tamura BM. A historical review of mineral water. Surg Cosmet Dermatol. 2012;4:252–258.
16. Paravina M, Stepanovic M, Racic G. Balneotherapy effectively acts on symptoms of of psoriasis vulgaris. CEEDVA Bull. 2002;4:70–72.
17. Boros M, Kemeny A, Sebok B, et al. Sulphurous medicinal waters increase somatostatin release: it is a possible mechanism of anti-inflammatory effect of balneotherapy in psoriasis. Eur J Integr Med. 2013;5:109–118. doi:10.1016/j.eujim.2012.09.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.