Back to Journals » Patient Preference and Adherence » Volume 17
Educational Interventions in Immigrants for Asthma and COPD: A Systematic Review
Authors Al-Juhaishi M ![]() , Lim CX
, Lim CX ![]() , Chan V
, Chan V ![]() , Stupans I
, Stupans I ![]() , Thrimawithana TR
, Thrimawithana TR ![]()
Received 11 August 2023
Accepted for publication 2 November 2023
Published 11 December 2023 Volume 2023:17 Pages 3245—3257
DOI https://doi.org/10.2147/PPA.S431224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Malath Al-Juhaishi, Chiao Xin Lim, Vincent Chan, Ieva Stupans, Thilini R Thrimawithana
Discipline of Pharmacy, School of Health and Biomedical Sciences, RMIT University, Melbourne, VIC, 3083, Australia
Correspondence: Malath Al-Juhaishi, Email [email protected]
Objective: Asthma and COPD are prevalent respiratory conditions among immigrants, yet many individuals in this population do not effectively utilize available therapies, resulting in exacerbations and limitations in their daily lives. This systematic review seeks to describe asthma/COPD educational interventions specifically tailored for immigrant patients and assess their variability and outcomes, with the ultimate goal of improving self-management and achieving better asthma or COPD control in this population.
Design: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. A comprehensive literature search was conducted using four electronic databases (CINAHL, PubMed, Embase and PsycInfo). Articles were included if they focused on asthma or COPD interventions conducted in immigrant populations. The Mixed Methods Appraisal Tool was used to assess the quality of included articles.
Results: Out of the initial 1173 articles identified, 812 were assessed for eligibility. Six articles met the inclusion criteria for educational interventions targeting immigrants with asthma or COPD. These studies explored the effectiveness of interventions on various immigrant populations using different methodologies including group discussion of photographs and classroom-based interventions. The interventions varied in terms of settings, educational materials, and delivery methods. Positive outcomes were observed in areas such as knowledge, understanding of instructions, and inhaler technique. However, the included studies had limitations in assessing the impact on asthma and COPD self-management and sustainability.
Conclusion: More research is needed on asthma and COPD management in immigrants. The interventions included in this review had positive effects on outcomes like inhaler technique and asthma knowledge. However, due to variability in outcome measures, it is difficult to directly compare the interventions. Future studies should include diverse immigrant populations, consider the specific migration status of the immigrants, long-term sustainability of the intervention and use culturally tailored approaches to improve respiratory health in this population.
Keywords: asthma, COPD, immigrants, refugees, asylum seekers, self-care, intervention
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are widely recognized as the most prevalent non-communicable respiratory chronic diseases.1,2 Asthma is a common non-communicable chronic disease, with over 300 million people diagnosed with asthma worldwide.3 Asthma is defined as a chronic inflammatory disorder of the airways.4 It involves widespread obstruction of the airways causing episodes of breathlessness, wheezing, coughing, and chest tightness that becomes worse at night and in the mornings.4 Chronic obstructive pulmonary disease (COPD) is also a significant health issue worldwide.5 It affects around 10% of the adult population, and its incidence is increasing, partly due to the aging population. COPD is characterized by persistent airflow obstruction and associated respiratory symptoms such as dyspnea, coughing and production of excess sputum.5–7
Treatments for people with asthma and COPD are guided by their lung function as well as the severity of symptoms.8,9 Various clinical guidelines are available for managing these respiratory conditions, aiming to prevent exacerbations and improve quality of life.9,10 Pharmacological therapies for asthma and COPD encompass the utilization of short-acting bronchodilators for rapid relief; and long-acting bronchodilators, inhaled corticosteroids (ICS), and combination therapies involving ICS for ongoing maintenance.9,10 Recent research has strongly emphasized the effectiveness of long-acting bronchodilators, including both long-acting muscarinic antagonists and long-acting β2-agonists, as the preferred choice for alleviating symptoms, reducing exacerbations and improving quality of life in patients with COPD.11–13 Inhalation therapy is the primary treatment method, but up to 90% of individuals demonstrate incorrect inhaler techniques.12 This issue is partially attributed to the diverse array of inhaler types and their technical complexities, which pose significant barriers to the management of asthma and COPD.12
In addition to pharmacological treatments, self-management has been identified as an effective approach to controlling asthma and COPD; however, it requires patients to have a good understanding of the condition, know what happens to their airways, understand the differences between their medications, and most importantly, use the prescribed medication as advised by a healthcare professional.14,15
Numerous meta-analyses of randomized controlled trials have demonstrated the beneficial effects of asthma educational interventions on various aspects of asthma and COPD management. These interventions have been shown to have a positive impact on improving inhaler technique, asthma/COPD control, reducing hospital admissions, and enhancing overall quality of life.16–19 Despite these findings, the frequency of inhaler technique errors remains unacceptably high and has only demonstrated marginal improvements over the past four decades.20 This persistent issue can be attributed to the inherent complexity of asthma as a chronic condition, necessitating ongoing education and support for patients.16,21 While community-based asthma educational interventions have primarily focused on patient education, follow-up, and monitoring programs, they have often been of limited duration, typically ranging from immediate to six months post-intervention, and have targeted only a select number of individuals with asthma.16,21,22 There is a need for improved asthma educational interventions to address high rates of inhaler technique errors and limited sustainability over time. Comprehensive, accessible, and sustained programs, incorporating technology-based solutions, can provide ongoing support and enhance asthma self-management for better patient outcomes.
Recent literature highlights that ethnic minority groups, including immigrants, endure a disproportionate burden of asthma.23 In contrast, these populations exhibit a lower likelihood of developing chronic obstructive pulmonary disease (COPD), prompting investigations into potential factors like underdiagnosis or reduced susceptibility to the disease.6,24 A direct link has been established in the literature between asthma management in these populations and barriers to accessing the healthcare system.25 Barriers encompass factors such as limited health literacy, financial challenges, and cultural beliefs, which significantly impact health management and medication adherence.25 The significance of these findings underscores the need for focused attention on addressing the specific healthcare needs of ethnic minority groups, particularly immigrants. It is imperative to develop and assess targeted interventions that address access barriers, improve health literacy, and account for cultural nuances; and by doing so enhance asthma and COPD management outcomes and promote equitable health care for these vulnerable populations.
This systematic review focuses on immigrants, including refugees, asylum seekers, and migrants. Although there are differences between the terms “refugee”, “asylum seeker”, and “migrant”, for the purposes of this review, they have been grouped together as immigrants. According to the 1951 Refugee Convention, a “refugee” is defined as someone who flees their homeland due to war or violence, leaving behind their family, friends, and belongings, and is unable to return to their country.26 “Asylum seekers” are individuals who seek sanctuary in another country due to war or life-threatening risks, hoping for protection from another government.26 Some define a “migrant” as a person who voluntarily leaves their country in search of a better life in another country and has the ability to return home.26 Differences in medication adherence have been observed between migrants and refugees, potentially attributed to variations in health beliefs, medication beliefs, cultural beliefs, and levels of acculturation.27 This underscores the importance of clearly identifying participant demographics in studies.27
Knowledge and self-management have a crucial influence on asthma/COPD clinical outcomes. For instance, low levels of asthma knowledge are associated with poor asthma control.28 Knowledge about asthma/COPD is positively linked to improved medication adherence.14,15 Educating immigrants in their native language has also been found to be more effective than using the language of the host population.29 Overall, current educational health information often lacks the involvement of the community’s views and perspectives, as these are frequently written in English and then translated into the community’s language.29,30 Ethnic minorities may have additional factors that can affect their medication adherence, such as their perception of the disease and medications, as well as levels of acculturation.31,32
Several systematic reviews on asthma and/or COPD interventions have been previously conducted and reported.16,17,30,33,34 These reviews have examined the effectiveness of interventions; however, none of them have specifically focused on immigrants. While several studies have implemented educational interventions within the host population to improve asthma management and reduce hospital admissions, there remains a notable gap in providing similar educational programs tailored to the immigrant population.19,30,35 This review aims to fill that gap by focusing on assessing the effectiveness of asthma educational interventions in immigrant patients. The objectives of this systematic review are to systematically evaluate the existing body of evidence, identify the key components of interventions, and determine their effectiveness in improving inhaler technique, asthma and/or COPD knowledge, and self-efficacy in immigrants with asthma or COPD.
Methods
The literature search for this systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.36 A comprehensive search was performed in four electronic databases, namely CINAHL, PubMed, Embase, and PsycInfo, to retrieve relevant articles addressing asthma or COPD management in migrant, refugee, and asylum seeker populations. The search was limited to articles published from inception to April 2023.
The search strategy involved using combinations of relevant search terms, including (education OR intervention OR clinical trial OR randomized controlled trial OR controlled trial OR behavior) AND (asthma OR bronchial asthma OR chronic obstructive pulmonary disease OR COPD OR chronic obstructive airway disease OR COAD) AND (refugee OR asylum seeker OR migrant OR emigrant OR immigrant). These search terms were used to identify papers that focused on interventions, education, clinical trials, and behaviour related to asthma and COPD in the specified populations.
In addition to the electronic database search, the reference lists of identified articles were screened to identify any additional relevant studies that might not have been captured through the initial database search. This step was taken to ensure the inclusion of all relevant studies in the systematic review.
Inclusion Criteria
The criteria used for article inclusion in this systematic review were as follows: (1) must be published in English; (2) report on asthma and/or COPD intervention studies specifically conducted in immigrant populations, including refugees, migrants, and asylum seekers; (3) published in peer-reviewed journals; and (4) published before April 30, 2023, to capture relevant studies conducted within the specified timeframe.
Exclusion Criteria
Articles were excluded from this systematic review if they met any of the following criteria: (1) asthma or COPD non-intervention studies conducted in the target populations of immigrants, including refugees, migrants, and asylum seekers; (2) focused on asthma or COPD intervention studies specifically targeting immigrant healthcare workers; (3) the interventions examined in the studies were primarily focused on chronic conditions other than asthma or COPD in the target population; (4) discussed asthma self-management in ethnic groups without explicitly specifying if the participants were migrants, refugees, or asylum seekers; and (5) the asthma or COPD intervention studies specifically focused on children or individuals younger than 18 years of age.
Selection of Studies
Two authors independently conducted database searches using the same search terms to ensure robustness of the search strategy. After exporting the search results to EndNote version 20, duplicates were removed. Both title and abstract screening phases were performed by two researchers (MA and CL). Following this, one researcher (MA) conducted the full-text screening, and the included articles were later reviewed by four additional researchers (TT, VC, IS, and CL). In cases of discrepancies regarding article inclusion or exclusion, discussions among the researchers took place until consensus was reached.
Data Extraction
Data were extracted from selected articles and tabulated. The categories of data extracted included a brief description of the intervention, study population (participants’ country of origin and country of residency, age range, sample size and gender), comparison tools used pre- and post-intervention to evaluate the intervention and summary of findings. The findings were further categorized under three subheadings: (1) inhaler technique; (2) asthma knowledge; and (3) self-efficacy. Findings were reviewed by all authors.
Assessment of Quality
The Mixed Methods Appraisal Tool (MMAT) version 2018 was used to assess the quality of included articles.37 MMAT is a quality appraisal tool that assesses different methodologies including qualitative, quantitative, and mixed methods studies. Each included paper was independently assessed by four investigators to appraise the quality (TT, VC, IS and CL). In cases of discrepancies, a discussion took place until a consensus could be reached.
Results
Article Selection
A comprehensive search yielded a total of 1173 articles, including 1161 articles from the database search and 12 articles from the hand search of reference lists. After removing duplicates (312 records) and articles published in languages other than English, the title and abstract screening were conducted on 812 articles. Of these, 788 articles were excluded as they did not meet the inclusion criteria. Thirty-six articles remained and were considered potentially relevant for this systematic review.
A subsequent review of the full text of the selected papers resulted in the inclusion of six articles that met the inclusion criteria (Figure 1). These six articles form the basis of the analysis and findings presented in this systematic review.
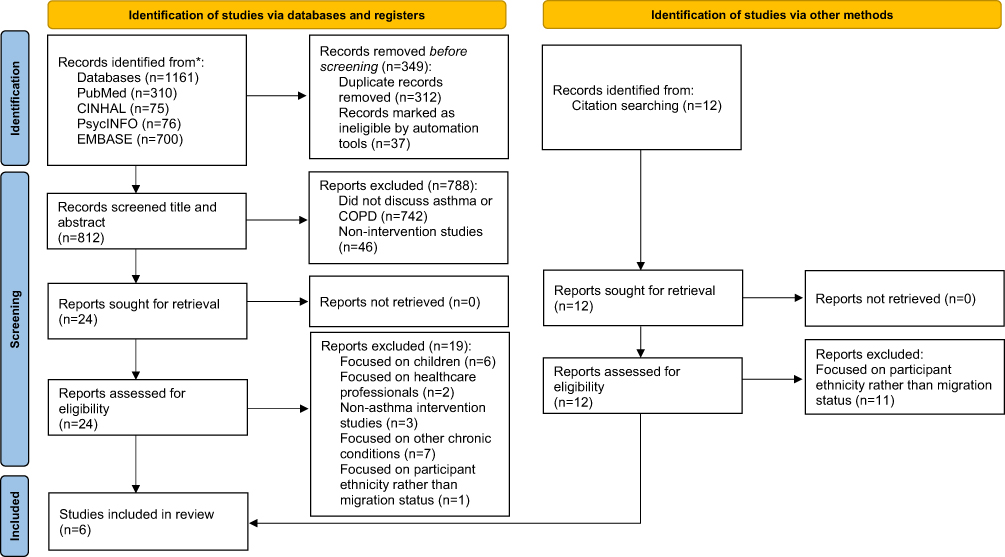 |
Figure 1 PRISMA flow diagram outlining the literature search and study selection process. |
Assessment of Quality
All studies were assessed using the MMAT tool. Categories of study assessed included quantitative randomised controlled trial (2/6), quantitative non-randomized controlled trials (2/6) and mixed methods studies (2/6).
Among the papers included in the review, one study38 fulfilled 80% of the MMAT criteria, while two studies39,40 met 60% of the inclusion criteria (Appendix 1). Both non-randomized studies41,42 scored 40% on the MMAT criteria (Appendix 1). Notably, one study43 did not meet any of the MMAT criteria (Appendix 1). Given the limited availability of literature on the topic, all papers were included in this review.
Characteristics of Selected Studies
All of the included interventions in this systematic review used the term “immigrants” to describe their participants.39–43 However, none of the included articles specified the migration status of their participants, such as refugees, migrants, or asylum seekers, according to the definitions provided by World Health Organization.26
Regarding participants’ characteristics, three interventions focused on Latino immigrants in the United States of America,41–43 two interventions discussed Punjabi and Chinese immigrants in Canada39,40 and one intervention focused on Chinese immigrants in Canada.38 Three studies were conducted in the United States of America41–43 and three were conducted in Canada.38–40
Design of Interventions
The study settings varied, with three interventions being conducted at home or in a medical clinic depending on participant’s preference,38–40 while the other three studies were conducted in an English as a second language centre.41–43
In terms of intervention characteristics, five of the selected interventions focused on asthma and its management,39–43 while one intervention study discussed the management of COPD.38
Among the included interventions, four studies included both an intervention group and a control group.38–40,42 One of the interventions was a pilot study,43 and the educational material used in two interventions was pilot tested prior to conducting the intervention to evaluate its effectiveness.39,40
Material and Delivery of Education
The educational material of three interventions was co-developed with members of the target community.38–40 Two studies used asthma educational material developed by other organizations,41,42 and the research team of one intervention created specific educational material for their target population.43
These studies used a variety of methods to deliver the educational material to the participants. Three studies used audio-visual as well as written educational materials,38–40 two interventions used video-based education only,41,42 and one study used a group discussion using photovoice cards.43 Three interventions were delivered by healthcare providers as well as community members and it was consistently reported that participants who viewed the videos delivered by healthcare providers achieved the most significant improvements in both their inhaler technique and knowledge.38–40 Meanwhile, the remaining interventions were administered by research facilitators.41–43
Sample demographics varied considerably between the included studies, ranging from 19 to 152 adults, aged 21–87 years. Five out of six studies specified the language used to deliver the interventions, with two studies delivering the educational intervention in Punjabi or Mandarin,39,40 a study using Mandarin or Cantonese,38 a study using Spanish or English,43 and with one study only using English language.42
Five studies specified the duration of the educational session and the duration varied considerably between studies with short educational videos that last 12 minutes to 25 minutes,38,40 to 60-minute group educational programs,42,43 or interactive videoconferences that last 60 to 90 minutes.41 Only three studies specified the intervention duration, with the interventions ranging from 4 to 10 months. The intervention duration included a baseline assessment and post-intervention assessment to determine sustainability.38–40
As shown in Table 1, the intervention components of each program were different. However, education on basic asthma knowledge and self-management skills, as well as care coordination to connect patients/families with relevant primary care health professionals, were common intervention elements.
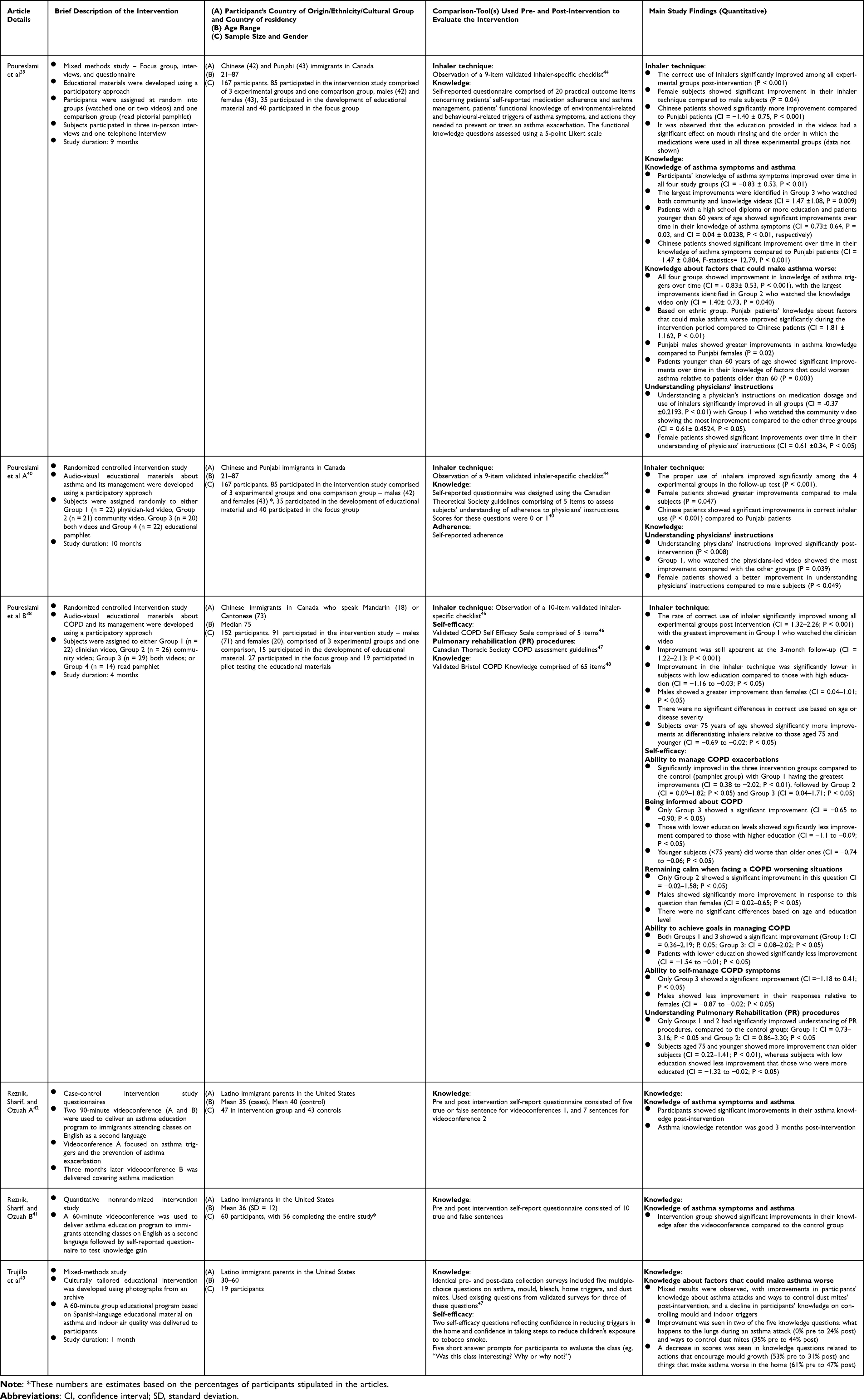 |
Table 1 Study Characteristics and Outcomes |
Two of the included studies39,40 appeared to be derived from the same study data, as they had identical study designs, materials and methods, study subjects, educational material, and measurement tools.
Regarding the evaluation of interventions, different pre- and post-intervention tools were used. Three interventions out of six discussed inhaler technique.38–40 Two of these interventions used a validated checklist with 9 items to assess inhaler technique39,40 and one used a 10-item checklist.38
Evaluation of Interventions
To evaluate asthma/COPD knowledge, only one intervention used a validated Bristol COPD Knowledge questionnaire comprised 65 items,38 the other five studies developed questionnaires specific for the study.39–43
Self-efficacy was assessed in two interventions.39,43 The validated COPD Self Efficacy Scale was used in patients with COPD,38 while the researchers designed a questionnaire for the other intervention.43
The interventions included in our review demonstrated positive outcomes in various areas, including improved knowledge about asthma,39,41,42 COPD38, triggers,41–43 understanding physicians’ instructions,40 and inhaler technique.38,39 However, it is worth noting that these positive outcomes were not measured using objective assessments such as spirometry to evaluate lung function or electronic monitoring of medication adherence. Additionally, it is also worth noting that none of the reviewed studies assessed the impact of improving these specific aspects, such as knowledge, understanding physicians’ instructions, and inhaler technique, on asthma self-management and overall asthma control. The absence of such measurements limits our understanding of how these improvements may directly influence the management and control of asthma.
Discussion
There is a lack of knowledge on how tailored educational interventions influence chronic disease management of immigrant populations. This systematic review on asthma and COPD educational interventions in immigrants appears to be the first review conducted on this specific topic. Six studies met the criteria for inclusion, with five focusing on asthma educational interventions and one addressing COPD education. The term “immigrant” was used as an umbrella term to describe the participants in these studies, without specifying their migration status as refugees, migrants or asylum seekers.
It is important to recognize that there may be variations among immigrant populations in terms of their migration journey and health status. Even within the same ethnic group, refugees and migrants may have distinct health beliefs and perceptions of illness.49 Therefore, it is crucial for future studies to not only consider participants’ ethnicity but also specify their migration status. This additional information can help to better understand the unique challenges, facilitators, and barriers to chronic disease management within each immigrant group.
By acknowledging the diversity within immigrant populations and considering specific migration status, researchers and healthcare providers can gain deeper insights into the factors influencing the management of chronic diseases among different immigrant groups. This knowledge can contribute to the development of more effective interventions to support the health and well-being of immigrants with asthma and COPD.
This review identified that only a limited number of intervention papers targeting immigrant populations with asthma/COPD, specifically six, have been published before April 30th, 2023. Notably, three of these papers were authored by the same group of researchers. This indicates a scarcity of research focusing on interventions for immigrants with asthma/COPD.
All of the included papers in this review reported positive impacts of the educational interventions on various outcomes such as inhaler technique, asthma knowledge, and self-efficacy.38–43 Moreover, previous studies have demonstrated that educational interventions in asthma management can yield favourable effects on a range of significant patient outcomes.17 These outcomes extend beyond the specific ones previously mentioned and include vital aspects such as mortality rates, daily activities, quality of life, and satisfaction with care.17,22 Incorporating these additional patient outcomes in future educational intervention studies would contribute to a more comprehensive understanding of the impact and benefits of such interventions in improving overall asthma management.
It is worth mentioning that in the included papers, educational materials that were co-developed with members of the community showed significant effectiveness in educating the participants. This highlights the importance of involving the target population in the development of educational materials to ensure their cultural relevance and appropriateness.39,40 Additionally, the delivery of educational materials by healthcare providers from the same cultural background to the participants was found to be more effective compared to delivery by non-healthcare providers. This finding aligns with existing literature and emphasizes the significance of having trusted professionals present relevant and useful information to the target population.39,40
Based on our review, interventions employing a blend of written and video-based materials indicated that individuals who received asthma and COPD education through video-based materials demonstrated more significant improvements in knowledge compared to those who solely received written information. These results align with existing evidence highlighting the advantages of video-based content for asthma and COPD education. Videos can provide visual demonstrations of proper inhaler techniques, trigger identification, and asthma management strategies, which are crucial for individuals to effectively manage their condition.50 The dynamic and interactive nature of videos can capture attention and facilitate better understanding and retention of asthma-related information.50 Therefore, incorporating video-based educational resources in asthma and COPD education programs may enhance knowledge acquisition and empower individuals to better manage their asthma and COPD symptoms and improve their overall asthma and COPD control.50
In the assessment of inhaler technique, the studies included in this review predominantly employed observational tools, utilizing 9 or 10-item checklists.38–40 These checklists were designed to observe and evaluate specific steps and skills related to proper inhaler use.20 Similarly, other studies examining inhaler technique also utilized either observational methods or questionnaires as assessment tools.20,51 It is important to note that the reliance on self-reported measures, such as questionnaires, may introduce potential limitations, as they rely on participants’ subjective perceptions and recall. The use of objective measures, such as direct observation by trained assessors, could provide more accurate and reliable assessments of inhaler technique.20 Future research should consider incorporating a combination of objective and self-reported measures to comprehensively evaluate inhaler technique and its impact on asthma and COPD management. By employing a multimodal approach to assessment, a more comprehensive understanding of inhaler technique proficiency can be achieved, leading to more targeted interventions and improved asthma and COPD care. Our findings have highlighted the research gaps in identifying the impact of these interventions on asthma and COPD management and patient’s daily life. In comparison to the current literature on asthma and COPD educational interventions, the reviewed papers in this study did not report the impact of the interventions on asthma and COPD management, patient’s quality of life, and hospital admissions.16 One explanation for the lack of reported outcomes related to asthma and COPD management, quality of life, and hospital admissions could be the relatively short duration of the interventions and the follow-up periods, which ranged from one day to six months post-intervention. These outcomes may require longer-term follow-up to accurately assess their impact.
Strengths and Limitations
The key strengths of this review are the use of rigorous search strategy to search various databases and the quality assessment of included studies. Importantly, our study fills a notable gap as there has been a lack of systematic reviews specifically addressing asthma and COPD in the immigrant population. Therefore, this review stands as the pioneering systematic review on this topic within the immigrant population.
The limitations of this study are the relatively small number of studies that met the inclusion criteria and the risk of selection bias. The search was limited to English language articles published before April 30th, 2023, and retrieved from four electronic databases.
Furthermore, a variety of comparison tools were used to assess inhaler technique, asthma knowledge, and self-efficacy before and after the interventions. However, none of the asthma intervention studies utilized a validated tool for assessment, mainly due to a lack of available validated tools for these specific outcomes.
Similarly, for assessing self-efficacy and asthma knowledge, the researchers in all of the studies designed their own assessment tools. While these tools may have been tailored to the specific interventions and populations, the lack of validation raises concerns about their reliability and validity.
The absence of validated tools in the reviewed studies highlights the need for the development and utilization of standardized and validated instruments for assessing important outcomes such as inhaler technique, asthma knowledge, and self-efficacy. The use of validated tools would enhance the rigor and comparability of future studies in this field, allowing for more robust conclusions and facilitating the identification of effective interventions for asthma and COPD management in immigrant populations.
Conclusion
In conclusion, the findings of this systematic review highlight the limited number of studies conducted in this specific population, indicating a gap in research on asthma and COPD management among immigrants. Despite the scarcity of studies, the included interventions demonstrated positive impacts on outcomes such as inhaler technique, asthma knowledge and self-efficacy. Given the paucity of the literature and the limitations identified, this review underscores the need for further research in this area. Future studies should aim to specify the migration status of participants and include diverse immigrant populations, including refugees and asylum seekers, to better understand the unique enablers and barriers to chronic disease management within each group. By addressing these gaps, healthcare providers can better support immigrant populations in managing their asthma or COPD and improving their overall health outcomes.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This project did not receive any funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Labaki WW, Han MK. Chronic respiratory diseases: a global view. Lancet Respir Med. 2020;8(6):531–533. doi:10.1016/S2213-2600(20)30157-0
2. Australian Institute of Health and Welfare. Chronic respiratory conditions; 2023. Available from: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/chronic-respiratory-conditions.
3. Dharmage SC, Perret JL, Custovic A. Epidemiology of asthma in children and adults. Front Pediatr. 2019;7:246. doi:10.3389/fped.2019.00246
4. Wu TD, Brigham EP, McCormack MC. Asthma in the primary care setting. Med Clin North Am. 2019;103(3):435–452. doi:10.1016/j.mcna.2018.12.004
5. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
6. Agusti A, Vogelmeier C, Faner R. COPD 2020: changes and challenges. Am J Physiol Lung Cell Mol Physiol. 2020;319(5):L879–L883. doi:10.1152/ajplung.00429.2020
7. Agarwal AK, Raja A, Brown BD. Chronic obstructive pulmonary disease. In: StatPearls. StatPearls Publishing; 2023.
8. Papi A, Blasi F, Canonica GW, Morandi L, Richeldi L, Rossi A. Treatment strategies for asthma: reshaping the concept of asthma management. Allergy Asthma Clin Immunol. 2020;16:75. doi:10.1186/s13223-020-00472-8
9. Gupta N, Agrawal S, Chakrabarti S, Ish P. COPD 2020 Guidelines - what is new and why? Adv Respir Med. 2020;88(1):38–40. doi:10.5603/ARM.2020.0080
10. Reddel HK, Bacharier LB, Bateman ED, et al. global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
11. Pires N, Pinto P, Marcal N, et al. Pharmacological treatment of COPD - New evidence. Pulmonology. 2019;25(2):90–96. doi:10.1016/j.pulmoe.2018.10.005
12. Bollmeier SG, Hartmann AP. Management of chronic obstructive pulmonary disease: a review focusing on exacerbations. Am J Health Syst Pharm. 2020;77(4):259–268. doi:10.1093/ajhp/zxz306
13. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
14. Khalid AN. Stepwise management of asthma. Int Forum Allergy Rhinol. 2015;5:S41–4. doi:10.1002/alr.21606
15. Miles C, Arden-Close E, Thomas M, et al. Barriers and facilitators of effective self-management in asthma: systematic review and thematic synthesis of patient and healthcare professional views. NPJ Prim Care Respir Med. 2017;27(1):57. doi:10.1038/s41533-017-0056-4
16. Mahdavi H, Esmaily H. Impact of educational intervention by community pharmacists on asthma clinical outcomes, quality of life and medication adherence: a systematic review and meta-analysis. J Clin Pharm Ther. 2021;46(5):1254–1262. doi:10.1111/jcpt.13419
17. Chongmelaxme B, Lee S, Dhippayom T, Saokaew S, Chaiyakunapruk N, Dilokthornsakul P. The effects of telemedicine on asthma control and patients’ quality of life in adults: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2019;7(1):199–216 e11. doi:10.1016/j.jaip.2018.07.015
18. Jia X, Zhou S, Luo D, Zhao X, Zhou Y, Cui YM. Effect of pharmacist-led interventions on medication adherence and inhalation technique in adult patients with asthma or COPD: a systematic review and meta-analysis. J Clin Pharm Ther. 2020;45(5):904–917. doi:10.1111/jcpt.13126
19. Abdulsalim S, Unnikrishnan MK, Manu MK, Alrasheedy AA, Godman B, Morisky DE. Structured pharmacist-led intervention programme to improve medication adherence in COPD patients: a randomized controlled study. Res Social Adm Pharm. 2018;14(10):909–914. doi:10.1016/j.sapharm.2017.10.008
20. Sanchis J, Gich I, Pedersen S. Aerosol drug management improvement T. Systematic review of errors in inhaler use: has patient technique improved over time? Chest. 2016;150(2):394–406. doi:10.1016/j.chest.2016.03.041
21. Maricoto T, Monteiro L, Gama JMR, Correia-de-Sousa J, Taborda-Barata L. Inhaler technique education and exacerbation risk in older adults with asthma or chronic obstructive pulmonary disease: a meta-analysis. J Am Geriatr Soc. 2019;67(1):57–66. doi:10.1111/jgs.15602
22. Kneale D, Harris K, McDonald VM, Thomas J, Grigg J. Effectiveness of school-based self-management interventions for asthma among children and adolescents: findings from a Cochrane systematic review and meta-analysis. Thorax. 2019;74(5):432–438. doi:10.1136/thoraxjnl-2018-211909
23. Jones JA, Wahlgren DR, Meltzer SB, Meltzer EO, Clark NM, Hovell MF. Increasing asthma knowledge and changing home environments for Latino families with asthmatic children. Patient Educ Couns. 2001;42(1):67–79. doi:10.1016/s0738-3991(00)00102-6
24. Gilkes A, Ashworth M, Schofield P, et al. Does COPD risk vary by ethnicity? A retrospective cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2016;11:739–746. doi:10.2147/COPD.S96391
25. Patel D, Jalal Z, Guo P. Medicine adherence and associated factors in immigrants and refugees: a systematic review. Int J Clin Pract. 2022;2022:1993066. doi:10.1155/2022/1993066
26. World Health Organization. Refugee and migrant health. Available from: https://www.who.int/news-room/questions-and-answers/item/refugee-and-migrant-health.
27. Shahin W, Kennedy GA, Cockshaw W, Stupans I. The effect of acculturation and harm beliefs on medication adherence on Middle Eastern hypertensive refugees and migrants in Australia. Int J Clin Pharm. 2021;43(5):1283–1292. doi:10.1007/s11096-021-01248-9
28. Mancuso CA, Rincon M. Impact of health literacy on longitudinal asthma outcomes. J Gen Intern Med. 2006;21(8):813–817. doi:10.1111/j.1525-1497.2006.00528.x
29. Netto G, Bhopal R, Lederle N, Khatoon J, Jackson A. How can health promotion interventions be adapted for minority ethnic communities? Five principles for guiding the development of behavioural interventions. Health Promot Int. 2010;25(2):248–257. doi:10.1093/heapro/daq012
30. Salim H, Ramdzan SN, Ghazali SS, et al. A systematic review of interventions addressing limited health literacy to improve asthma self-management. J Glob Health. 2020;10(1):010427. doi:10.7189/jogh.10.010428
31. Mathes T, Jaschinski T, Pieper D. Adherence influencing factors - a systematic review of systematic reviews. Arch Public Health. 2014;72(1):37. doi:10.1186/2049-3258-72-37
32. Shahin W, Kennedy GA, Cockshaw W, Stupans I. The association between social support and medication adherence in patients with hypertension: a systematic review. Pharm Pract. 2021;19(2):2300. doi:10.18549/PharmPract.2021.2.2300
33. Gill I, Shah A, Lee EK, et al. Community interventions for childhood asthma ED visits and hospitalizations: a systematic review. Pediatrics. 2022;150(4). doi:10.1542/peds.2021-054825
34. Cross AJ, Thomas D, Liang J, Abramson MJ, George J, Zairina E. Educational interventions for health professionals managing chronic obstructive pulmonary disease in primary care. Cochrane Database Syst Rev. 2022;5(5):CD012652. doi:10.1002/14651858.CD012652.pub2
35. Castro M, Zimmermann NA, Crocker S, Bradley J, Leven C, Schechtman KB. Asthma intervention program prevents readmissions in high healthcare users. Am J Respir Crit Care Med. 2003;168(9):1095–1099. doi:10.1164/rccm.200208-877OC
36. Wang X, Chen Y, Liu Y, et al. Reporting items for systematic reviews and meta-analyses of acupuncture: the PRISMA for acupuncture checklist. BMC Complement Altern Med. 2019;19(1):208. doi:10.1186/s12906-019-2624-3
37. Hong QN, Fàbregues S, Bartlett G, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34:285–291. doi:10.3233/EFI-180221
38. Poureslami IKS, Lam S, Khan NA, FitzGerald JM, Fitzgerald JM. Assessing the effect of culturally specific audiovisual educational interventions on attaining self-management skills for chronic obstructive pulmonary disease in Mandarin- and Cantonese-speaking patients: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2016b;11:1811–1822. doi:10.2147/COPD.S105408
39. Poureslami I, Nimmon L, Doyle-Waters M, et al. Effectiveness of educational interventions on asthma self-management in Punjabi and Chinese asthma patients: a randomized controlled trial. J Asthma. 2012;49(5):542–551. doi:10.3109/02770903.2012.682125
40. Poureslami I, Shum J, Nimmon L, FitzGerald JM. Culturally specific evaluation of inhaler techniques in asthma. Respir Care. 2016a;61(12):1588–1596. doi:10.4187/respcare.04853
41. Reznik M, Sharif I, Ozuah PO. Use of interactive videoconferencing to deliver asthma education to inner-city immigrants. J Telemed Telecare. 2004;10(2):118–120. doi:10.1258/135763304773391585
42. Reznik M, Ozuah PO. Asthma educational videoconferencing for parents: a case-control study. J Telemed Telecare. 2004;10:83–85. doi:10.1258/1357633042614447
43. Trujillo A, Evans-Agnew R, Tinajera M, Alonso S, Postma JM. Measuring our success in teaching latinos about asthma and home environments: lessons learned from an intervention developed through photovoice. Prog Community Health Partnersh. 2020;14(3):381–392. doi:10.1353/cpr.2020.0043
44. Asthma Canada. How to use your Medication. Available from: https://asthma.ca/get-help/treatment/controllers/#:~:text=Asthma%20Canada%20recommends%20using%20a%20spacer%20with%20your,breath%20for%20about%2010%20seconds%2C%20then%20breathe%20out.
45. Rootmensen GN, van Keimpema ARJ, Jansen HM, de Haan RJ. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010;23(5):323–328. doi:10.1089/jamp.2009.0785
46. Zhang C, Wang W, Li J, et al. Development and Validation of a COPD Self-Management Scale. Respiratory Care. 2013;58(11):1931–1936. doi:10.4187/respcare.02269
47. O’Donnell DE, Aaron S, Bourbeau J, et al. State of the Art Compendium: Canadian Thoracic Society recommendations for the management of chronic obstructive pulmonary disease. Can Respir J. 2004;11:7B–59B. doi:10.1155/2004/946769
48. White R, Walker P, Roberts S, Kalisky S, White P. Bristol COPD Knowledge Questionnaire (BCKQ): testing what we teach patients about COPD. Chron Respir Dis. 2006;3(3):123–131. doi:10.1191/1479972306cd117oa
49. Shahin W, Kennedy GA, Cockshaw W, Stupans I. The role of refugee and migrant migration status on medication adherence: mediation through illness perceptions. PLoS One. 2020;15(1):e0227326. doi:10.1371/journal.pone.0227326
50. Wilson EA, Park DC, Curtis LM, et al. Media and memory: the efficacy of video and print materials for promoting patient education about asthma. Patient Educ Couns. 2010;80(3):393–398. doi:10.1016/j.pec.2010.07.011
51. Ndukwe HC, Shaul D, Shin J, et al. Assessment of inhaler technique among fourth-year pharmacy students: implications for the use of entrustable professional activities. Curr Pharm Teach Learn. 2020;12(3):281–286. doi:10.1016/j.cptl.2019.12.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patients’ Expectations of Evidence-Based Service at the Pharmacy Regarding Information on Self-Care of the Feet for Persons with Diabetes at Risk of Developing Foot Ulcers – A Cross-Sectional Observational Study in Sweden
Hellstrand Tang U, Scandurra I, Sundberg L, Annersten Gershater M, Zügner R
Patient Preference and Adherence 2023, 17:3557-3576
Published Date: 27 December 2023
Development and Implementation of a Self-Management Intervention Program for Patients with Esophageal and Gastric Varices Secondary to Liver Cirrhosis Under Collaborative Care
Li M, Xie XE, Qin X, Wu T, Bian ZL
International Journal of General Medicine 2025, 18:2673-2686
Published Date: 22 May 2025
The Impact of Self-Management Interventions on Behavioral and Clinical Outcomes in Individuals with Systemic Lupus Erythematosus: A Systematic Review of Empirical Evidence From 2003-2024
Hanrop S, Narupan N, Praha N, Phianhasin L, Ruksakulpiwat S
Patient Preference and Adherence 2025, 19:1763-1779
Published Date: 17 June 2025
The Existing Interventions to Promote Self-Care and Self-Monitoring Preventing Hypertension Among Thai Risk People: A Scoping Review
Banharak S, Potempa K, Limpawattana P, Pamungkas RA, Mahikul W, Jeamjitvibool T, Karaket A, Siriprathum S, Ransinyo K
Vascular Health and Risk Management 2025, 21:519-544
Published Date: 9 July 2025
Anticipations and Requirements of Individuals with Long-Term Health Conditions Regarding Self-Management and Digital Health Support Tools
Alessa T
Patient Preference and Adherence 2025, 19:2901-2918
Published Date: 13 September 2025