Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 13
Ectopic Eruption of First Permanent Molars for Pediatric Patients Attended King Saud University, Riyadh, Saudi Arabia: A Radiographic Study
Authors Aldowsari MK ![]() , Alsaidan M
, Alsaidan M ![]() , Alaqil M, BinAjian A, Albeialy J, Alraawi M, Al Moaleem MM
, Alaqil M, BinAjian A, Albeialy J, Alraawi M, Al Moaleem MM
Received 16 May 2021
Accepted for publication 10 July 2021
Published 24 July 2021 Volume 2021:13 Pages 325—333
DOI https://doi.org/10.2147/CCIDE.S320441
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Mannaa K Aldowsari,1 Musab Alsaidan,2 Marshad Alaqil,2 Ali BinAjian,2 Jawad Albeialy,2 Mohammed Alraawi,3 Mohammed M Al Moaleem4
1Department of Pediatric Dentistry and Orthodontics, College of Dentistry, King Saud University, Riyadh, Saudi Arabia; 2College of Dentistry, King Saud University, Riyadh, Saudi Arabia; 3Department of Orthodontics, College of Dentistry, University of Hatay Mustafa Kemal, Antakya, Turkey; 4Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan, 45142, Saudi Arabia
Correspondence: Mohammed M Al Moaleem
Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan, 45142, Saudi Arabia
Email [email protected]
Background: Early diagnosis and intervention of ectopically erupting first permanent molars (FPMs) are vital to avoiding later complex surgical or/and orthodontic treatment. Selection of proper type of intervention and simple treatment is considered as more convenient to use with children.
Purpose: The aim of this retrospective radiographic cross-sectional study was to assess the prevalence and severity of ectopically erupting FPMs in children attending the Dental University Teaching Hospital (DUTH) at King Saud University, Riyadh, Saudi Arabia.
Methods: This retrospective study was conducted using panoramic radiographs (OPGs) of 2014 patients (973 females and 1041 males) aged from 5 to 8 years old who attended DUTH at King Saud University, Riyadh, Saudi Arabia. We assessed and recorded the age and gender of the subjects, the tooth number, arch, and location of the ectopic erupted FPMs, and the severity of resorption of the roots of the primary molars.
Results: Of 2014 reviewed OPGs, 45 (2.2%) cases were diagnosed with an ectopic eruption of the permanent first molar. The distribution of ectopic eruption based on gender showed that there was a higher prevalence in males 28 (2.9%) than in females 17 (1.6%). Of the 45 ectopic FPMs cases, 47 (78.33%) were detected in the maxilla, while 13 (21.66%) were seen in the mandible. Severe and moderate degrees of the ectopic eruption were found to be more common in the maxilla than in the mandible (p < 0.001).
Conclusion: Clinicians should be aware of such conditions, as early diagnosis is essential for providing optimum dental care. To our knowledge, this study is the first to assess the prevalence of ectopically erupting FPMs in a Saudi population.
Keywords: ectopic eruption, first permanent molars, resorption of primary second molars
Background
By the end of the eruption process, when the tooth is in its correct position, it will aid in function, esthetic, and phonetics. However, teeth do not always erupt where they are supposed to; sometimes deviation or drifting of a tooth from its path of eruption during the eruption process occurs, which is called ectopic eruption and is considered as an anomaly that causes malocclusion and might affect the function, appearance, and phonetics.1 Nikiforuk defined the ectopic eruption as
a condition in which the permanent teeth, because of deficiency of growth in the jaw or segment of the jaw, assumes a path of eruption that intercepts a primary tooth, causing its premature loss and producing a consequent malposition of the permanent tooth.1
Ectopic eruption of the PFM is a local disturbance characterized by the eruption of these teeth under the distal undercut of the second primary molars and failure of the first permanent molars (FPMs) to erupt to the normal occlusal plane.2 Absence of gubernacular canal may direct to a concerned eruption form of the tooth and may rise the danger of problems associated with an ectopic eruption subsequent to a tooth that is more probably to stayed as unerupted.3 Kaplan et al concluded that cone beam computed tomography (CBCT) is an effective technique for the assessment of the gubernacular tract in unerupted 1 ectopic eruption of the PFM.4
During daily dental practice, dental anomalies (developmental or acquired) are diagnosed in the pediatric clinics. Also, dental abnormalities in teeth number (congenitally missing teeth and supernumerary tooth), tooth size (macrodontia, microdontia, and fusion), tooth shape (dilaceration, dens evaginatus, and taurodontism), tooth structure (amelogenesis imperfecta and dentinogenesis imperfecta), and tooth position (ectopic eruption and rotation) are observed.1,3
Ectopic eruption of the PFM is mainly diagnosed by radiographs either as an incidental finding following radiographic examination for a different dental complaint or after the clinical suspicion when there is greater than 6 months delay of eruption or asymmetry in the eruption of FPM. Radiographically, it appears that the ectopically erupted PFM is “impacted” in the distobuccal root of the primary second molar.5–7 Early assessment of the proper type of radiographs for monitoring the FPMs eruption timing is important to detect the problem and proposal the opportunity to avoid possible disadvantages. If diagnosed at 5 to 6 years old, an observation approach of “watchful waiting” with appropriate follow-up may be indicated, where up to two-thirds would be expected to self-correct. Self-correction becomes more unlikely moving closer to the age of 7 years, where continued “locking” of the FPM with severely resorbed primary second molar usually requires intervention. Another important milestone is when the opposing molar reaches the level of the mandibular occlusal plane. At this time, an intervention is indicated to establish proper vertical control and prevent supra-eruption.8 So, the goal of treatment is to move the ectopically erupting tooth away from the tooth it is resorbing, allowing it to erupt, and retaining the primary second molar.6
Young classified ectopic eruption into two types: reversible and irreversible. In the reversible type, the molar frees itself from the ectopic position and erupts into normal alignment, with the second primary molar remaining in position. Most permanent molars in children with reversible patterns had freed themselves by 7 years old. In contrast, when irreversible, the maxillary FPM remains unerupted and in contact with the cervical root area of the second primary molar. So, through the age of 7 and 8 years, any ectopic eruption of FPM should be considered irreversibly locked.9 Bjerklin and Kurol reported that children with irreversible ectopic eruption patterns had significantly larger FPMs, a more pronounced mesial angle path of eruption, and a tendency toward a shorter maxilla in relation to the cranial base. If the irreversible ectopic molars remain locked and untreated, this might result in premature loss of the primary second molar with a deficiency in quadrant arch length, asymmetric shifting of the maxillary FPM toward class II positioning, and supra-eruption of the opposing molar with distortion of the mandibular curve of Spee and possible occlusal interferences.8
Quite a few local studies have investigated the ectopic eruption of FPMs teeth in different cities of Saudi Arabia. Yassin conducted a study in Abha, Saudi Arabia, concluding that the percentage of ectopic eruption was 2.3%, and more likely in males than females.10 Elsayed et al assessed the prevalence and distribution of rare ectopic impacted teeth at Al-Madinah Al-Munawwarah, Saudi Arabia. These authors describe 63 ectopically impacted teeth, with an incidence of 0.7% among older patients. The impacted teeth were higher in the mandible, with no difference between sides.11 A case reported for an ectopic eruption maxillary right FPM was published by Hafiz.12 However, to our knowledge, no studies to assess the prevalence of ectopic eruption of FPM have been carried out in Riyadh, Saudi Arabia. Thus, the aim of this retrospective radiographic study was to assess the prevalence and severity of the ectopic eruption of the FPM in Riyadh, Saudi Arabia accordingly.
Subjects and Methods
Study Sample and Patient Criteria
This was a retrospective cross-sectional, radiographic observational survey using dental panoramic x-ray of child patients who attended the Dental University Hospital at King Saud University in Riyadh, Saudi Arabia, between January 2014 and January 2020. The study was approved by the Institutional Review Board, King Saud University and Medical City (E-20-5033), and was performed in accordance with the Declaration of Helsinki. Patient parental consent was not required by Institutional Review Board as investigators did not access patient medical records nor physically examined the patients. We only view the radiographs. The case numbers were sent to us ready from IT department for patients who met study criteria only (5–8 years and medically fit and well). Radiographs were anonymized using serial number and no patient names were identified. Research protocol was done in compliance with Declaration of Helsinki.
Statistical advice was sought, and the sample size was calculated by using Cochran’s Formula and based on a previous study that was done by Güven.13 A sample size of 1695 was required. The inclusion criteria were healthy (absence of any relevant medical condition or history, mental illness, or syndromic patients) children (5 to 8 years old) who have good quality digital radiographs in their records. Children with no radiographs, low-quality radiographs, or not matching the selected age range were excluded from the study.
Training and Calibration
Four graduated dentists (dental interns) were trained by a radiographic and pediatric specialist. The training consisted of both theoretical lectures and workshops on how to diagnose and classify the ectopic eruption of the first permanent molars. Inter- and intra-observer reliability were assessed using a set of radiographs separate from the test sample and by reassessment after an interval of 2 weeks using the kappa test as a pilot study.
OPG Assessment
Radiographs were anonymized using serial number and no names were identified, then were collected from the X-ray machine (PLANMECA – ProMax machine, Helsinki, Finland) in an assigned radiographic reporting room in a dimmed light environment, using a graphic monitor and evaluated by the Planmeca Romexis (Helsinki, Finland) dental radiographic software by four trained dental interns. Simple image manipulation was used for more accurate image interpretation, such as contrast, brightness, and sharpness adjustments. A customized data collection sheet was used for data collection. The following relevant information on each patient included in this study was recorded: gender, date of birth, date of radiograph, ectopic tooth number site and arch, medical condition, and evidence of supernumerary teeth. FPMs with evidence of ectopic eruption were recorded. Also, the severity of the ectopic eruption was recorded based on the effect on the second primary molars as presented in Table 1.2,6
 |
Statistical Analysis
Descriptive statistics of parameters assessed in this study were performed using Statistical Package for the Social Science (SPSS) (version 23.0; IBM, Armonk, NY, USA). Statistical analysis included mean and standard deviation (SD). The frequency distribution between the ectopically erupted FPMs among age, gender, arch, site, and severity were tested using the chi-square analysis. Spearman correlation was applied to evaluate associations among age, gender, and severity of the ectopic eruption. The confidence level was set to 95%, and p-values less than 0.05 were considered significant.
Results
During the pilot study, we assessed the intra-clinical examiner reliability for the types of the severity of the ectopic eruption of PFMs using Kappa test scores for nominal data. The findings reveal the incidence of severity of the ectopic eruption of PFMs in this study, and the level of agreement was very high, reaching >95%, determined by the same clinical examiner in two separate examination times.
Of the 2014 reviewed cases, 45 subjects (28 males and 17 females) were diagnosed with an ectopic eruption of PFM. It was considered the absolute frequency of the ectopic erupted FPMs among all the examined cases with an overall or total prevalence of 2.2%. The mean age and standard deviation of the cases was 6.90 ± 0.985 years (6.91 ± 0.987 for female and 6.89 ± 0.984 for male). Although the distribution of ectopic eruption based on gender shows that there was a higher prevalence in males (2.9%) than in females (1.6%), the difference was not statistically significant (p = 0.59). The percentage of age shows that the highest groups were in age 8-years for both male and females with 33.7%, without any significance between the age group (Table 2). An example of the assessed and interpreted OPG is presented in Figure 1A–C.
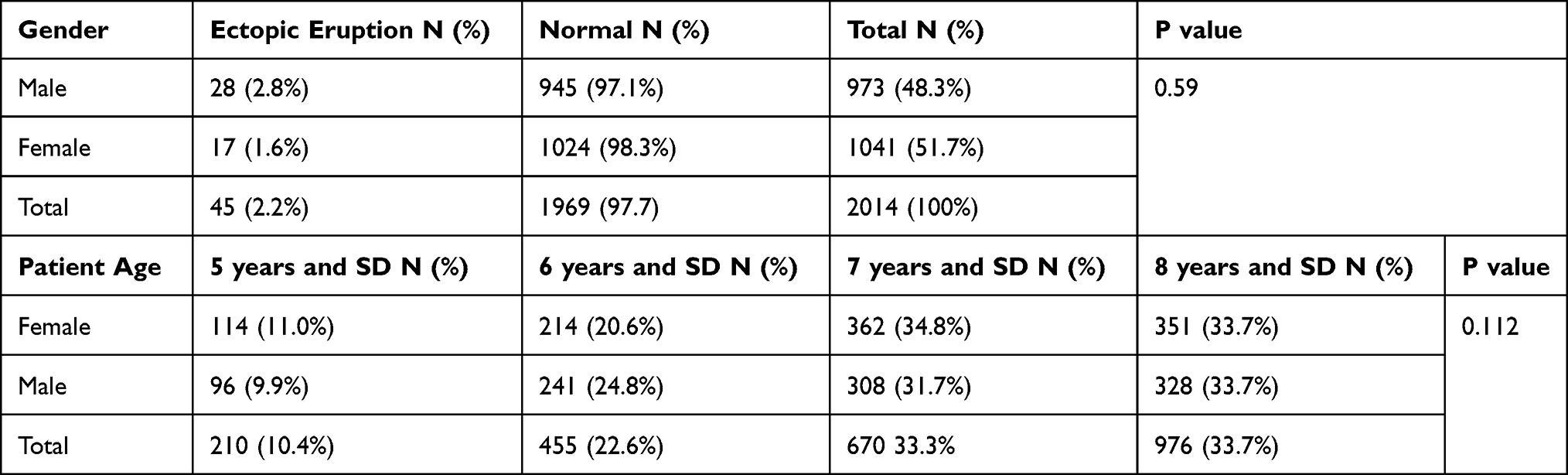 |
Table 2 Frequency Distribution of Ectopic Eruption PFM Cases Concerning Gender and Age |
The absolute frequency of teeth with ectopic eruption is 60 PFMs among 45 patients. There were 47 (78.4%) ectopic eruptions of FPM in the maxillary arch, which was much higher than the mandibular arch 13 (21.6%) with significant differences between the arches (p-value 0.000). In contrast, the rates of ectopic eruption of FPM were similar among the right and left sides (Table 3).
 |
Figure 1 Panoramic examples of all the severity of ectopic eruption (A) An example of severe ectopic eruption maxillary right first permanent molar causing severe resorption to maxillary right second primary molar. (B) An example of moderate ectopic eruption maxillary left first permanent molar causing resorption of the dentine without pulp exposure (C) An example of mild ectopic eruption maxillary right first permanent molar with limited resorption to the cementum to maxillary right second primary molar. |
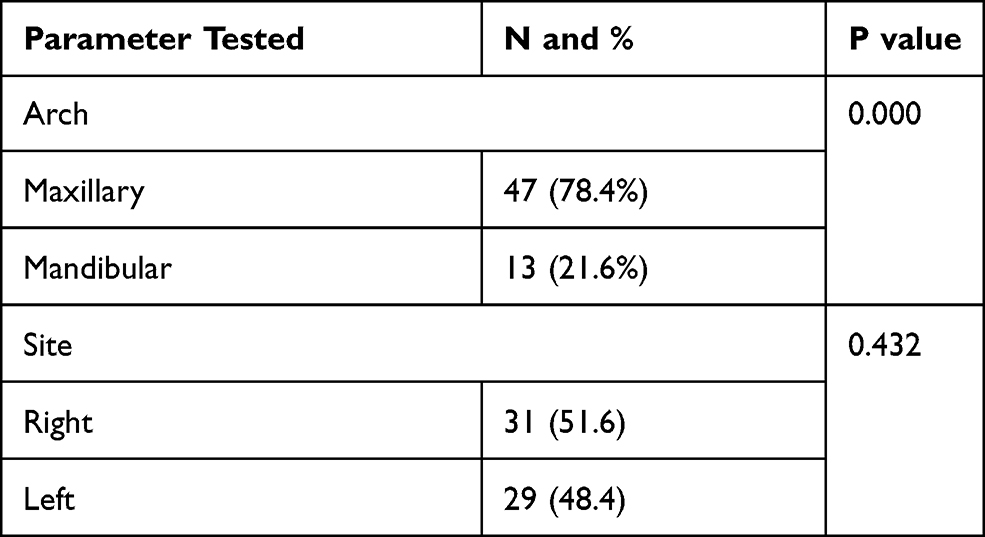 |
Table 3 Frequency Distribution of Ectopic Eruption of FPMs with Tooth Arch and Site |
The degree of severity distribution among the ectopically erupted FPMs recorded for these 60 teeth are presented in Table 4. The highest relative frequency of the cases was detected in the maxillary right FPM (41.65) first permanent molar, followed by maxillary left FPM with (n = 22, 36.6%), while the lowest relative index was mandibular right and left FPMs (0.11, 0.10, respectively). According to the severity of ectopic eruption for FPMs, the highest significant frequency was in the mild category with 33 (55%), followed by the moderate cases (n = 18, 30%), and severe cases (n = 9, 25%), respectively. There were statistically significant differences between the different types of the severity of ectopic eruption and the site of teeth (p = 0.001). All the severe cases were detected in the maxilla, with no severe instances recorded in the mandible (Table 4).
 |
Table 4 The Frequency Distribution of Ectopic Eruption of FPMs in Relation to Case Numbers with Severity |
The relation between ectodermal severity of permanent first molars and age and gender was measured using Spearman correlation in Table 5. The interrelation between ectopic PFMs and age showed a very weak relation in the four types of ectopic eruption of PFMs (−0.007–0.016). Similarly, there was a negative correlation between ectopic severity of PFMs and gender (0.002–0.035).
 |
Table 5 Spearman Correlations Between Severity of Ectopic Eruption of PFMs and Both of Age and Gender |
Discussion
To our knowledge, no previous study has investigated and assessed the ectopic eruption of the FPMs for pediatric Saudi patients attending King Saud University, Riyadh. Also, in this retrospective study, the severity of ectopically erupted FPMs was evaluated radiographically. The study is based on examining OPGs of 2014 patients aged from 5 to 8 years old who attended the Dental University Hospital. The sample size was calculated using data based on a study conducted among multiple populations.13,14 The radiographs were randomly selected by four general dentists. To minimize the risk of bias, the examiners were trained in assessing the ectopic eruption by a specialist in pediatric dentistry. In addition, inter- and intra-examiner tests to assess the ectopic eruption and the degree of severity were performed prior to conducting the main study. A recent image or modality is the CBCT to assess the ectopic eruption of the FPM, but in this current study it may not change any results, since we measured only number and did not evaluated or assessed and anatomical distances, it could do if the distance and the effects reach the erupted second primary molars were investigated .3,4
The overall percentage of the ectopic eruption of FPMs was 2.2% among the evaluated samples. Comparing our findings with some local studies, this value was similar to the percentages recorded by Yassin in Abha (2.3%),10 but higher than the percentage observed in Al-Madinah Al-Munawwarah for impacted teeth (0.7%).11 We compared the overall percentage of the ectopic eruption of the FPM recorded in the current study with other worldwide published studies. In a study conducted in Thailand in 1998 with a sample of 4232 Thai children (6–9 years old), the percentage of the ectopic eruption of the FPM was 0.75%.2 The finding of the present study was three times higher in comparison to the Thai children, and this can be explained by the differences in population genetic and ethnicity. Another retrospective study was completed in Spain with a sample of 509 children aged 6–9 years old, using radiographs to assess the prevalence of PFM in the maxillary arch and measure the resorption of the primary second molar. These authors also assessed the magnitude of impaction of the permanent molar in millimeters. These authors reported a prevalence of 4.3% in the ectopic eruption of the maxillary FPM,6 which was double the proportion detected in our study; this might be due to the differences in the numbers of the subject examined in each study.8 A recent retrospective study was carried among Turkish children to record the prevalence and severity of the ectopic eruption of the FPM. These authors screened 7649 OPGs of children aged 5–11 years old.13 This study reported a prevalence of ectopic eruption of FPM of 2.65%, which is similar to the percentage recorded in the present study.
Pulver summarized that a combination of factors contributed to the ectopic eruption of the maxillary FPM; those factors are categorized into five points: (1) larger than normal maxillary deciduous and permanent teeth; (2) smaller than normal length of the maxilla; (3) posterior position of the maxilla in relation to the cranial base; (4) abnormal angulation of eruption of the molars; and (5) delayed calcification of some affected FPM.15 In relation to the severity of the ectopic eruption of the PFMs, our results were in line with previous studies that showed that the highest type was the mild type; this was in parallel with the studies conducted in Spain and Turkish populations.6,13 The severity of ectopic eruption of FPM and the resorption degree of the second primary molar roots were equal between the arches. Severe and very severe degrees of ectopic eruption were found to be more common in the maxilla than in the mandible, whereas a mild degree of the ectopic eruption was more prevalent in the mandible which is consistant with previous published studies.5,13,16
Here we found that the percentage and frequency of ectopic eruption of FPMs were higher in males than females. This was in line with the findings of a local study by Yassin in Abha, Saudi Arabia,10 but did not agree with Hafiz,12 who published a case report among female Saudi patients with an ectopic eruption of FPM. Our data also coincide with a previous study that investigated the prevalence of ectopic eruption of PFM among Thai and Turkish populations.2,13 Other recent study conducted among Turkish population and published by Caliskan et al, 2021 found that the spreading of ectopic eruption rendering to gender shows a higher incidence in males in comparing to females.17
Ectopic eruption of PFMs is a serious abnormality in the teeth; it is the eruption of the tooth in an abnormal orientation or position; the most affected teeth are the maxillary canines and maxillary FPMs. The highest percentage (78.4%) was obtained in the maxillary arch (Table 3). This is totally consistent with results recorded in Thailand, England, Turkey, Germany, and Korea,2,5,13,17 in that the ectopic eruption of the FPM was higher in the maxillary arch. The disturbance between the required space of the eruption of the tooth and the available space results in the occurrence of ectopic eruption of the FPM (maxillary). Almost 66% of ectopic eruption occurs in the maxilla. The prevalence of FPM (maxillary first) is 0.75% to 6%.14,20 These percentages flank that reported in the present study, and were higher than the percentage obtain among patients in Abha,10 Saudi Arabia. Also, it was supported by the finding of a study conducted in England,5 which reported that maxillary ectopic eruption of FPMs was higher in the maxilla. These authors also found that maxillary FPM was more affected than mandibular FPM, with a prevalence of 0.39% and 0.36%, respectively. Totally agreed with the prevalence of ectopic eruption of FPM is higher in the maxillary arch in comparison to the mandibular one.2,13 Elsayed et al11 reported that the impacted teeth were higher in the mandible; this can be explained by the age of the examined subjects.7
A group of published radiographic studies carried out in Saudi Arabia, England, and Turkey have reported no differences in the percentage of the ectopic eruption of FPMs between the right and left sides.5,11,13 This is in agreement with our results, where no differences between both sides were detected. An Indian case report of a 13-year-old-male reported to the Department of Paediatric and Preventive Dentistry with a chief complaint of dental pain with an ectopic eruption of FPM in right mandibular posterior teeth21 while another case report for a Saudi male patient with ectopic maxillary right FPM.12
The ectopic eruption of the FPM can be classified into two types: reversible and irreversible. In the reversible type, most permanent molars in children free themselves from the ectopic position and erupt into normal alignment by 7 years old; by the age of 8 years, any ectopic eruption of FPM should be considered irreversibly locked. Early detection of ectopic eruption of the FPM is important to avoid unwanted consequences like continued “locking” of the first molar after the age of 7 years and if the opposing molar becomes supra-erupted, which all will require continuous intervention.8 Dabbagh et al stated that natural self-correction happened in 71% of permanent maxillary first molars with ectopic eruption; 33% of self-corrections arisen after nine years of age.22 That is why we investigated this issue to minimize the complication and the interceptive treatment times and avoid the possibility of surgical involvements later on. Children with ectopic molar eruption may be associated with another anomaly, such as hypodontia, cleft lip and/or palate, and supernumerary teeth;5 this was not recognized during interoperating of the OPG radiograph for our subjects.
Ectopic eruptions are a developmental disturbance in which the tooth fails to follow its normal eruption pathway, and it was relatively rare to occur in the second molar.7 Several management techniques have been discussed in the literature, including early interceptive treatment.12 Also, the importance of the early diagnosis could minimize the need for active interceptive treatment, even in moderate severity ectopic eruption cases, to reduce the resorption of the distal root and pulpal involving the primary second molar.12 Chen et al, 2021, recommended that continuous monitoring and early interference would assist 6–8-age children through increasing severity of distal unusual resorption in the second primary molar.16
Ectopic eruptions of the FPM can be successfully treated by extracting the primary second molar and guiding the eruption of the FPM using a space maintainer, which is considered simple, low-cost, and more convenient to use with children.20 Rajesh et al reported proper treatment for a 13-year-old male with an ectopic mandibular second permanent molar, which was corrected with surgical exposure and placement of elastic separators. This is one of the basic methods to obtain acceptable results rather than extensive surgical or orthodontic corrections. It is advised that ectopic eruption of FPM should not be neglected, especially when it concerns developing caries of adjacent teeth and malocclusion of both arches.21
From Table 5, it was clear that there was no relation between ectodermal severity of permanent FPM in neither maxillary nor mandibular arch as well as right or left, age, and gender of the participants. Similarities were recorded among samples screened by Salbach et al,18 but not agreed with Sun et al,19 and Caliskan et al.17
One of the drawbacks of the present study is that it was a retrospective design that may miss some information concerning dental history. Another limitation was that the study findings were based on a single tertiary hospital. So, further studies using recent types of x-rays should be considered crossing multicenter design in different cities of Saudi Arabia.
Conclusion
The following conclusions can be drawn from this retrospective cross-sectional, radiographic observational survey. Male children have a greater prevalence of ectopic eruption of FPMs than females, but without achieving a statistically significant difference. The prevalence and the severity of the ectopically erupted FPM was greater in the maxilla than in the mandible, with equal frequencies on the right and left side. Clinicians should be aware of such conditions as early diagnosis is essential for providing optimum dental care and minimizing the delayed clinical complications.
Acknowledgments
The authors would like to thank Dr Thiyezen A AlDhelai, Department of Orthodontic and Pediatric Dentistry, College of Dentistry, Qassim University, Buraydah, Saudi Arabia; Department of Orthodontics and Pediatric Dentistry, Faculty of Dentistry, Ibb University, Ibb, Yemen for his help in the statistical part of the research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nikiforuk G. Ectopic eruption: discussion and clinical report. J Ont Dent Assoc. 1948;25:243–246.
2. Chintakanon K, Boonpinon P. Ectopic eruption of the first permanent molars: prevalence and etiologic factors. Angle Orthod. 1998;68:153–160.
3. Koc N, Dogru HB, Cagirankaya B, Dural S, van der Stelt PF. CBCT assessment of gubernacular canals in relation to eruption disturbance and pathologic condition associated with impacted/unerupted teeth. Oral Maxillofac Radiol. 2019;127(2):175–184.
4. Kaplan FA, Bilgir E, Bayrakdar IŞ, Kılıç MÇ. Evaluation of gubernacular tract with cone beam computed tomography in impacted supernumerary teeth. Eur J Anat. 2020;24(6):485–490.
5. Barberia-Leache E, Suarez-Clúa MC, Saavedra-Ontiveros D. Ectopic eruption of the maxillary first permanent molar: characteristics and occurrence in growing children. Angle Orthod. 2005;75:610–615.
6. Proffit WR. Contemporary Orthodontics/Proffit WR, Fields Henry W, Sarver David M.
7. Bjerklin K, Kurol J. Ectopic eruption of the maxillary first permanent molar: etiologic factors. Am J Orthod. 1983;84:147–155. doi:10.1016/0002-9416(83)90179-3
8. Young D. Ectopic eruption of permanent first molar. J Dent Child. 1957;24:153–162.
9. Yassin SM. Prevalence and distribution of selected dental anomalies among Saudi children in Abha, Saudi Arabia. J Clin Exp Dent. 2016;8:e485.
10. Elsayed SA, Althagafi N, Bahabri R, Alshanqiti MM, Alrehaili AM, Alahmadi AS. Retrospective radiographic survey of unconventional ectopic impacted teeth in Al-Madinah Al-Munawwarah, Saudi Arabia. Open Access Maced J Med Sci. 2020;20:203–208. doi:10.3889/oamjms.2020.4533
11. Hafiz ZZ. Ectopic eruption of the maxillary first permanent molar: a review and case report. J Dent Health Oral Disord Ther. 2018;9:154–158. doi:10.15406/jdhodt.2018.09.00349
12. Güven Y. Prevalence of ectopic eruption of first permanent molars in a Turkish population. Eur Oral Res. 2018;52:1–5. doi:10.26650/eor.2018.45227
13. Mucedero M, Rozzi M, Cardoni G, Ricchiuti MR, Cozza P. Dentoskeletal features in individuals with ectopic eruption of the permanent maxillary first molar. Korean J Orthod. 2015;45:190–197. doi:10.4041/kjod.2015.45.4.190
14. Pulver F. The etiology and prevalence of ectopic eruption of the maxillary first permanent molar. J Dent Child. 1968;35:138–146.
15. Mooney GC, Morgan AG, Rodd HD, North S. Ectopic eruption of first permanent molars: a preliminary report of presenting features and associations. Eur Arch Paediatr Dent. 2007;8:153–157. doi:10.1007/BF03262586
16. Sun J, Nam O, Kim M, Lee H, Choi S. Predictive factors of ectopic eruption of the maxillary first permanent molar. J Korean Acad Pediatr Dent. 2016;43(3):284–291.
17. Chen X, Huo Y, Peng Y, Zhang Q. Ectopic eruption of the first permanent molar: predictive factors for irreversible outcome. Am J Orthod Dentofacial Orthop. 2021;159(2):E169–77. doi:10.1016/j.ajodo.2020.09.020
18. Caliskan S, Tuloglu N, Ozdemir C, Kizilaslan S, Bayrak S. Ectopic eruption of maxillary permanent first molars: predictive factors for self-corrected and impacted outcome. Int J Clin Pract. 2021;75(3):e13880. doi:10.1111/ijcp.13880
19. Salbach A, Schremmer B, Grabowski R, de Castrillon FS. Correlation between the frequency of eruption disorders for first permanent molars and the occurrence of malocclusions in early mixed dentition. J Orofac Orthop. 2012;4:298–306. doi:10.1007/s00056-012-0083-2
20. Zou J, Meng M, Law CS, Rao Y, Zhou X. Common dental diseases in children and malocclusion. Int J Oral Sci. 2018;10:1–7. doi:10.1038/s41368-018-0012-3
21. Rajesh R, Naveen V, Amit S, Baroudi K, Reddy S, Namineni S. Treatment of ectopic mandibular second permanent molar with elastic separators. Case Rep Dent. 2014:4. Article ID 621568. doi:10.1155/2014/621568
22. Dabbagh B, Sigal MJ, Tompson BD, Titley B, Andrews P. Ectopic eruption of the permanent maxillary first molar: predictive factors for irreversible outcome. Pediatr Dent. 2017;39(3):215–218.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.