Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Economic Impact of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in Italy. Analysis and Perspectives
Authors Torre E ![]() , Di Matteo S, Martinotti C
, Di Matteo S, Martinotti C ![]() , Bruno GM
, Bruno GM ![]() , Goglia U, Testino G, Rebora A, Bottaro LC, Colombo GL
, Goglia U, Testino G, Rebora A, Bottaro LC, Colombo GL ![]()
Received 10 April 2024
Accepted for publication 4 October 2024
Published 24 October 2024 Volume 2024:16 Pages 773—784
DOI https://doi.org/10.2147/CEOR.S472446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dean Smith
Enrico Torre,1 Sergio Di Matteo,2 Chiara Martinotti,2 Giacomo Matteo Bruno,3 Umberto Goglia,4 Gianni Testino,5 Alberto Rebora,1 Luigi Carlo Bottaro,6 Giorgio Lorenzo Colombo3
1Diabetology and Metabolic Diseases Unit - ASL3, Genoa, Italy; 2Center of Research, SAVE Studi - Health Economics and Outcomes Research, Milan, Italy; 3Department of Drug Sciences, University of Pavia, Pavia, Italy; 4Territorial Diabetology Unit, ASLCN1, Cuneo, Italy; 5Units of Addiction and Hepatology, ASL3, Genoa, Italy; 6General Direction, ASL3, Genoa, Italy
Correspondence: Giorgio Lorenzo Colombo, Email [email protected]
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD) is a multisystem condition destined to become pandemic in the coming decades. This study aimed at evaluating the economic impact of MASLD in the Italian population from the Italian National Healthcare Service (NHS) perspective.
Methods: The economic impact of the MASLD was assessed by developing a calculation model in Microsoft Excel® from the Italian NHS perspective, considering healthcare resources and direct costs. The target population was based on the prevalence data. Through a literature search, complications of MASLD were identified, including MASH, with relative risk of evolution into CC, DCC, HCC, T2DM, cardiovascular diseases, in particular AMI and stroke, CKD, and CRC. The differential impact between complication development in the population with MASLD and the same sample size population without-MASLD was evaluated. Differential risk data, mortality rates, and event unit costs were drawn from the published international literature. Frequency and cost data were applied to the total target population, the total annual costs and mortality data, referring to the two arms, were then calculated, and the differential value was obtained.
Results: Based on an estimated 11,546,370 MASLD target population, an annual illness impact of € 12,251,631,822 was calculated, corresponding to a difference of € 7,731,674,054 compared with the same sample size without MASLD. Moreover, the MASLD population is expected to experience 13,438 additional deaths annually.
Conclusion: The growing epidemiological impact of MASLD and its complications represent a huge economic burden for healthcare services worldwide. An integrated approach, including changes in lifestyle behaviors, will be the first step. Specific drugs for MASLD are not yet available; however, studies are underway, and combined pharmaceutical therapies may be an inevitable choice to achieve adequate control of MASLD and its complications.
Keywords: metabolic associated fatty liver disease MASLD, complications, MASLD burden in Italy, healthcare costs, treatment and perspectives
Introduction
The term MASLD (Metabolic Dysfunction-Associated Steatotic Liver disease) was proposed in 2023 to better define the disease characterized by hepatic steatosis (verified through imaging techniques or liver biopsy) and at least one of the following conditions: obesity, metabolic dysregulation, or type 2 diabetes mellitus (T2DM).1 Metabolic dysregulation refers to the presence of at least two of the following conditions: waist circumference above 102/88 cm for Caucasian males/females, blood pressure above 130/85 mmHg or antihypertensive medication, plasma triglycerides above 150 mg/dl or related medication, HDL cholesterol < 40 mg/dl for men and 50 mg/dl for women, prediabetic condition (fasting plasma glucose between 100–125 mg/dl or 2 h post load between 140–199 mg/dl or glycosylated haemoglobin between 5.7%–6.4%), homeostasis model assessment (HOMA) score > 2.5, and high-sensitivity C-reactive protein levels above 2 mg/L.2 The old term NAFLD (Non-Alcoholic Fatty Liver Disease) remains confined to forms of steatosis (more than 5% of hepatocytes) unrelated to alcohol (less than 20/10 grams per day for males/females), viruses, genetic diseases, or toxic medications.2,3 Therefore MASLD does not just represent the new term for NAFLD, but, together with its more aggressive form named MASH (Metabolic dysfunction-Associated Steato-Hepatitis, definition that, in turn, replaces NASH), involves the manifold ensemble of metabolic disorders and is steadily increasing worldwide and will be the main cause of chronic liver diseases in the coming decades. In USA only, the prevalence of MASLD increased from 28.4% in 1999–2002 to 35.8% in 2011–2016.4,5 Moreover, compared to the diagnosis by exclusion in NAFLD, MASLD is a diagnosis of inclusion. Studies have shown that a portion of the NAFLD population is included under the proposed MASLD definition.6
A team from the University of Singapore elaborated a meta-analysis and systematic review of over 10 million individuals, documenting for the first time that global prevalence and clinical features of MASLD are very impressive. In a pooled analysis of over 3.3 million individuals, the overall prevalence of MASLD was found to be 38.77%, with significant differences in geographical regions: highest in Europe (55.33%), followed by Asia (36.31%), and the lowest in North America (35.99%, 95% CI 30.68% to 41.66%).7 In the same study, in a pooled analysis of 4.09 million patients with MASLD, the mean age of patients was 51.99 years, with an average Body Mass Index (BMI) and waist circumference of 27.71 kg/m2 and 92.91 cm, respectively; 41.38% had hypertriglyceridemia, 43.72% had hypertension, and 22.79% (95% CI 19.42% to 26.55%) were diabetic. In the analysis of MASLD demographics, 27.51% were smokers, and 19.28% had excessive alcohol consumption. A pooled mean liver function test revealed that the average aspartate aminotransferase (AST), alanine transaminase (ALT), and gamma-glutamyl transferase (GGT) levels were 35.08 U/L, 43.71 U/L, and 60.47 U/L, respectively.
In Italy, the Diabetes Barometer Report 2023 documented a self-reported prevalence of diabetes of 3.9 million (6.6% in the general population), with an evident age-correlated gradient, achieving a prevalence of 18.7% in subjects over 65 years of age.8 The prevalence of MASLD in patients with diabetes in Italy was 67.97%.9 Therefore, the estimated prevalence of MASLD in Italy, calculated considering the presence of the disease in the T2DM population (2.6 million T2DM patients have MASLD) and applying the previously reported prevalence of 22.79% of T2DM among the MASLD population,7 amounts to approximately 11.6 million out of a population of 58.85 million in January 2023 (19.62%) (as shown in Methods).10
Thus, MASLD is a multisystem disease presenting an increased risk of developing diabetes as well as cardiovascular diseases (CVD), renal impairment (CKD), extrahepatic cancers (mainly colorectal), obvious liver-related complications leading towards MASH, cirrhosis (compensated, CC, and decompensated, DCC), and hepatocellular carcinoma (HCC), requiring a liver transplant in case of end-stage disease.
In recent years the role of the inflammatory status on the development of the MASLD-MASH has been highlighted: hypertension and obesity, as well as pre-diabetes, were correlated to an inflammation increase associated with elevated serum uric acid to HDL-cholesterol ratio.11–13 Moreover, sarcopenia in individuals with MASLD portends increase mortality and significant liver fibrosis, so that new therapeutic strategies targeting at increasing skeletal muscle mass should be explored for these patients.14
Not being available data about the incidence of diabetes in MASLD population, the risk of developing T2DM among subjects with MASLD can be estimated starting from the annual incidence of T2DM among Italian population: 350,000 new diagnosis per year.15 Knowing that the prevalence of MASLD among diabetic patients is 68%, as reported above, we can deduce that about 238,000 new T2DM are diagnosed per year among non-diabetic MASLD subjects, thus determining an annual incidence of 2.66%.
If we also consider T2DM related events, among MASLD complications, the most common as well as the major cause of death is CVD, representing advanced liver disease, the second item in order of relevance.
A 2013 meta-analysis reported several studies demonstrating an increased risk of CVD among patients with NAFLD,16 and a paper published in 2021 quantified the prevalence of acute myocardial infarction (AMI) and stroke in USA adults, expressed as a percentage of 10-year risk, for MASLD compared to non-MASLD subjects.5 In the above-cited study, that analyzed data from 19617 adults aged ≥20 years from the cross-sectional US National Health and Nutrition Examinations Survey periods ranging from 1999 to 2016, the estimated 10-year risk of AMI and stroke ranged from 10.8% to 13.2% in MASLD subjects and from 6.6% to 7.1% in non-MASLD population; therefore, the highest prevalence presented by MASLD subjects ranged from 5.2% to 6.1% over a 10 years period. Applying these data to the Italian population, we deduce that in MASLD individuals, apart from T2DM-related complications (included in the computation of its global costs), we can estimate a population with AMI or stroke over a 10-year period, ranging from 465,000 to 545,000.
Chronic kidney disease (CKD) is another important and recognized complication of MASLD.17 In the main institutional document of the Italian Ministry of Health regarding the management of CKD, defined as an estimated glomerular filtration rate (eGFR) <60 mL/min 1.73 m2 and/or urinary albumin-to-creatinine ratio (ACR) ≥3 mg/mmol, the prevalence, based principally on the STUDIO CHARES, is 7.1% (7.5% in men and 6.5% in women), including 2.6% in stage 3 (eGFR 30–59 mL/min 1.73 m2) and 0.3% in stage 4–5 (eGFR <30 mL/min/ 1.73 m2).18 Considering these epidemiological data, we can calculate renal impairment in the general population, amounting to approximately 4.18 million subjects, including 177,000 affected by stage 4–5 CKD. Another review reported that NAFLD patients presented a higher risk of incident CKD than those without NAFLD over a median follow-up of nearly 5 years (HR 1.37, 95% CI 1.20–1.50).19 So, considering that MASLD individuals have a lower glomerular filtration rate and a greater prevalence of CKD than NAFLD individuals (29.6% vs 25.56%, P<0.05),20 even when applying the previous and more conservative rate of 1.37 to the Italian MASLD population, we can estimate at least 1.13 million subjects with CKD, of which 47,600 presenting stage 4–5 CKD. Therefore, excluding MASLD patients with T2DM, which represent two-thirds of all diabetic patients, and considering that T2DM accounts for approximately 20% of all cases of CKD,21 we can deduce about 590,000 not-T2DM MASLD subjects presenting CKD and 24,600 with stage 4–5 CKD.
Another important epidemiological association presented by MASLD subjects is an increased risk of colorectal cancer (CRC). A study starting from a nationwide health screening database including more than 8.9 million participants demonstrated that MASLD, more than NAFLD, was associated with a higher CRC risk, that, after multivariable adjustment for age, sex, household income quartile, residential area, CCI index (Charlson Comorbidity Index, which predicts 10-year survival in patients with multiple comorbidities), aspirin use, nonsteroidal anti-inflammatory drug use, tobacco smoke, exercise frequency, alcohol intake and concomitant liver diseases, was expressed as an HR of 1.16 (95% CI, 1.13–1.18).22 The study also found that patients with fatty liver disease and advanced liver fibrosis had a higher CRC risk than those with simple steatosis, suggesting that adequate intervention on the disease could reduce the overall risk. Considering that the incidence rate detected in individuals without MASLD was 57.5 per 100,000 person-years, the additional incidence attributable to MASLD can be quantified as 9.2 per 100,000 person-years. Applying this to the above-defined Italian MASLD population (11.6 million), we can consider an additional incidence of CRC in MASLD subjects of approximately 1067 patients per year.
Last but not least, MASLD presents a higher risk of hepatic events, whose incidence is related to the stage of fibrosis detected (F0-F2 versus F3 versus F4) as follows: variceal hemorrhage (0.00 versus 0.06 versus 0.70), ascites (0.04 versus 0.52 versus 1.20), encephalopathy (0.02 versus 0.75 versus 2.39), and hepatocellular carcinoma (HCC) (0.04 versus 0.34 versus 0.14) per 100 persons-year.23 Considering that the annual incidence of HCC in NAFLD (and moreover MASLD) patients is 0.44 per 1000 person-years (95% CI: 0.29–0.66) whereas for MASH is 5.29 per 1000 person-years and approximately 41% (95% CI: 34.69–47.13) of MASH patients present a worsening of fibrosis with an annual progression rate of 0.09% (95% CI: 0.06–0.12), the development of HCC and mortality has been stratified by NAFLD/MASLD or MASH status, as shown in Methods.24
Considering the constant growth of MASLD in terms of the percentage of population concerned,25 our study aimed at evaluating the economic impact of MASLD among the Italian population from the Italian National Healthcare Service (NHS) perspective.
Methods
Study Design
The economic impact of MASLD was assessed by developing a calculation model using Microsoft Excel®. The analysis was conducted from the Italian NHS perspective, considering the healthcare resources and direct costs related to the management of clinical conditions in the Italian setting. The target population was defined based on the prevalence data to provide a snapshot of the current situation. Prior to the analysis, a literature search was conducted to examine the MASLD clinical background and gather evidence regarding complications and the possible evolution of specific clinical conditions. Following the review, the main MASLD-related complications were identified, corresponding to MASH, with a relative risk of evolution into CC, DCC, HCC, T2DM, cardiovascular diseases, in particular AMI and stroke, CKD, and CRC. As these complications, in turn, represent significant chronic, metabolic, and worsening diseases, the differential impact between their development in the population with MASLD and in the same sample size without-MASLD was evaluated while highlighting the negative impact of MASLD, still largely overlooked today. T2DM cardiovascular related events were included in the cost of the disease. Furthermore, liver transplantation-related costs were taken into consideration. Differential risk data, referring to the development of these conditions between the populations affected by MASLD and non-MASLD, were drawn from published international literature. Mortality rates associated with complications were also investigated to estimate the differential impact on patients destined to die between the two groups. Once the estimated event rates for the groups were obtained, the annual unit cost of each event was applied. In addition, the annual unit costs per event were obtained from the literature, adopting specific data for the Italian healthcare context. Frequency and cost data were applied to the total target population, the total annual costs and mortality data referring to the two arms were then calculated, and the differential value was obtained.
Target Population
The MASLD target population was estimated by applying prevalence data and clinical characteristics obtained from the international literature7,9 to the Italian epidemiological context.8,10 Since no Italian studies on specific MASLD populations are available, the target population was obtained by extrapolation, starting from international data on the share of patients affected by MASLD among diabetics (67.75%) and the estimate of diabetic patients among all patients with MASLD (22.79%).7,9 Based on a total Italian population of 58,850,000 and 6.6% diabetes prevalence,8,10 a target population of 11,546,370 subjects in Italy was estimated, corresponding to approximately 19.6% of the total population (Table 1). Our estimate of prevalence must be considered conservative, as it presents international literature with higher estimates worldwide.
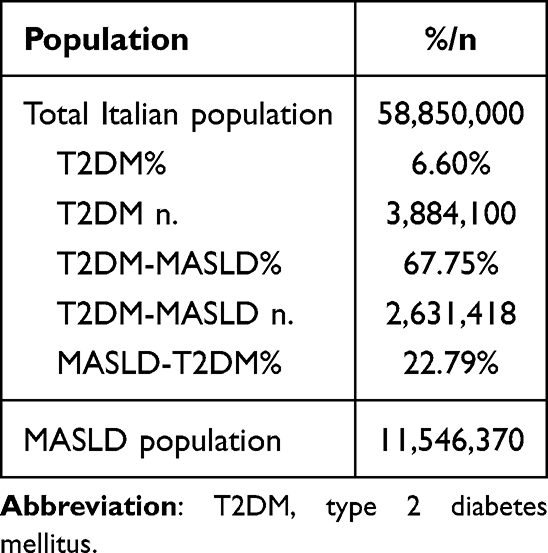 |
Table 1 Target Population |
Event Rate and Unit Costs
The differential rates of complications in the MASLD target population and in the same sample size not affected by MASLD were obtained from a literature search regarding the main complications of MASLD (MASH and advanced stages of liver damage (CC, DCC, HCC), also considering liver transplant cases, diabetes, cardiovascular diseases, including myocardial infarction and stroke, CKD, and colorectal cancer).5,7,15–17,19,22–24,26–28
For each complication, the unit cost was determined by referring to the relevant Italian literature.29–33 For steatosis evaluation, an outpatient services tariff was adopted.34 Table 2 lists the event occurrence rates and the related costs for each event.
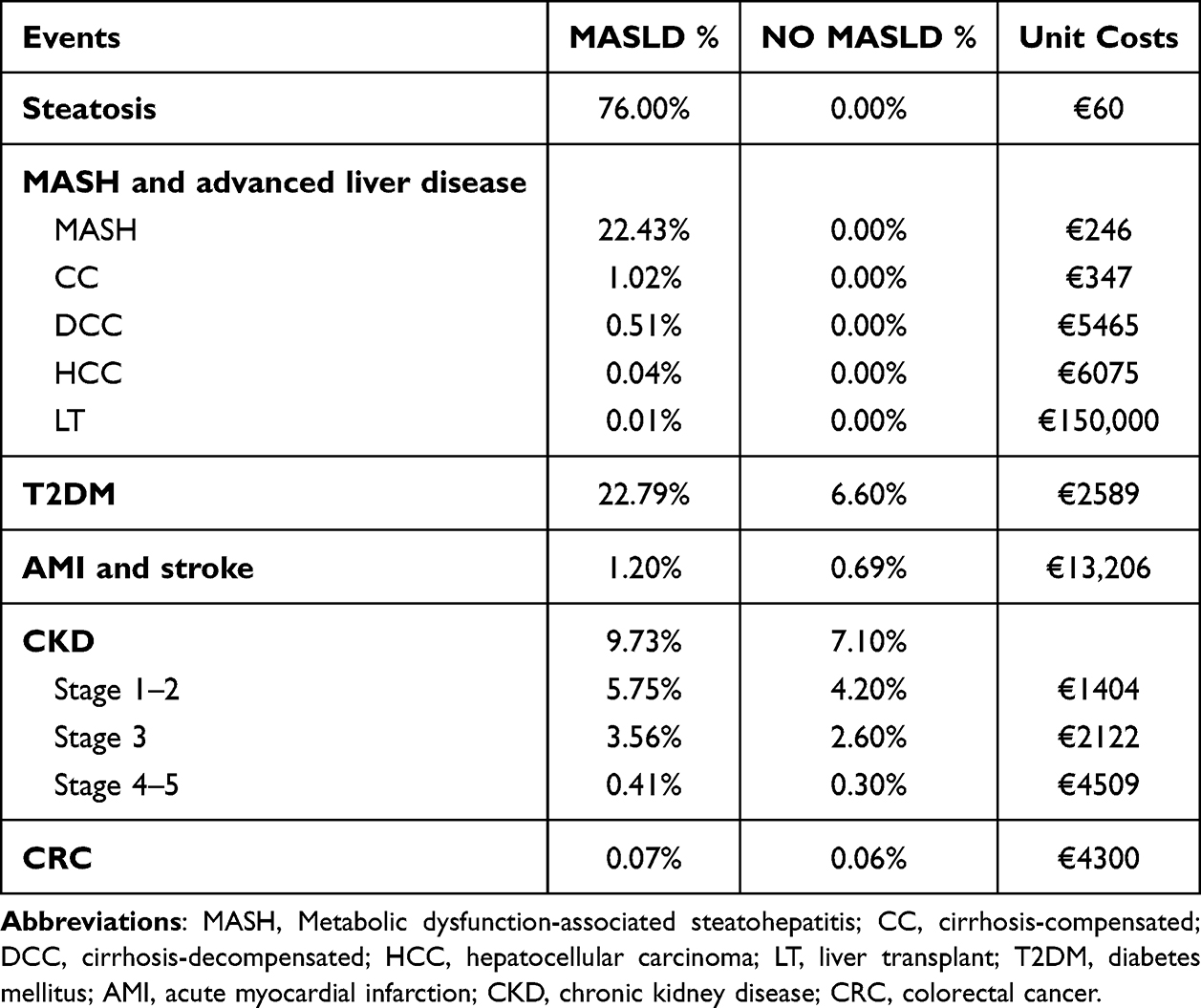 |
Table 2 Event Rate and Unit Cost |
Mortality
To estimate the impact of complications on life expectancy, the mortality rate associated with each complication has been investigated.27,35–37
This analysis was conducted to evaluate the differential impact between populations on deaths associated with the clinical condition of MASLD and related complications compared with the population without MASLD. Table 3 lists the adopted mortality rates.
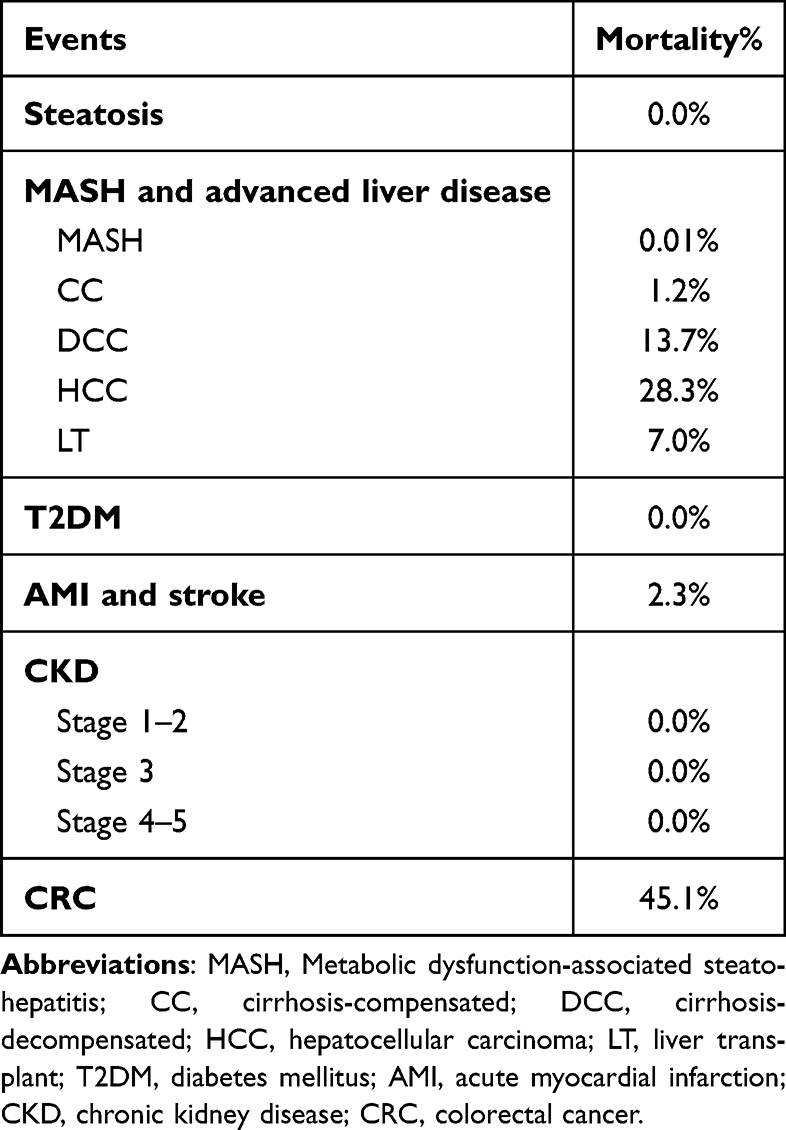 |
Table 3 Mortality Rates |
Sensitivity Analysis
One-way sensitivity analysis (OWSA) and probabilistic sensitivity analysis (PSA) were performed to assess the robustness of the results related to the main input adopted and assumptions considered. The OWSA has been used to assess parameter uncertainty by increasing and decreasing the base case value of each parameter and plotting the impact on the outcome in a tornado chart, thereby providing information regarding which parameters are most influential. In the OWSA have been considered a ±5% epidemiological data variation and a ±10% event rate and cost input data variation. The simulation scenarios were developed and compared with the base case, adopting as reference parameter the difference in total expenditure reported in the MASLD population and in the same sample without MASLD. Probabilistic sensitivity analysis (PSA) demonstrated parameter uncertainty; again, the difference in total spending reported in the two compared populations was used as a reference for the base case. A total of 1000 simulations were performed to establish the base-case probabilistic results. The gamma distribution was considered as the sampling variable.
Results
The results highlight the differential impact between the populations with and without MASLD on event occurrence, corresponding to the complications and disease evolutions to advanced stages, allowing the relative economic impact to be assessed (Table 4).
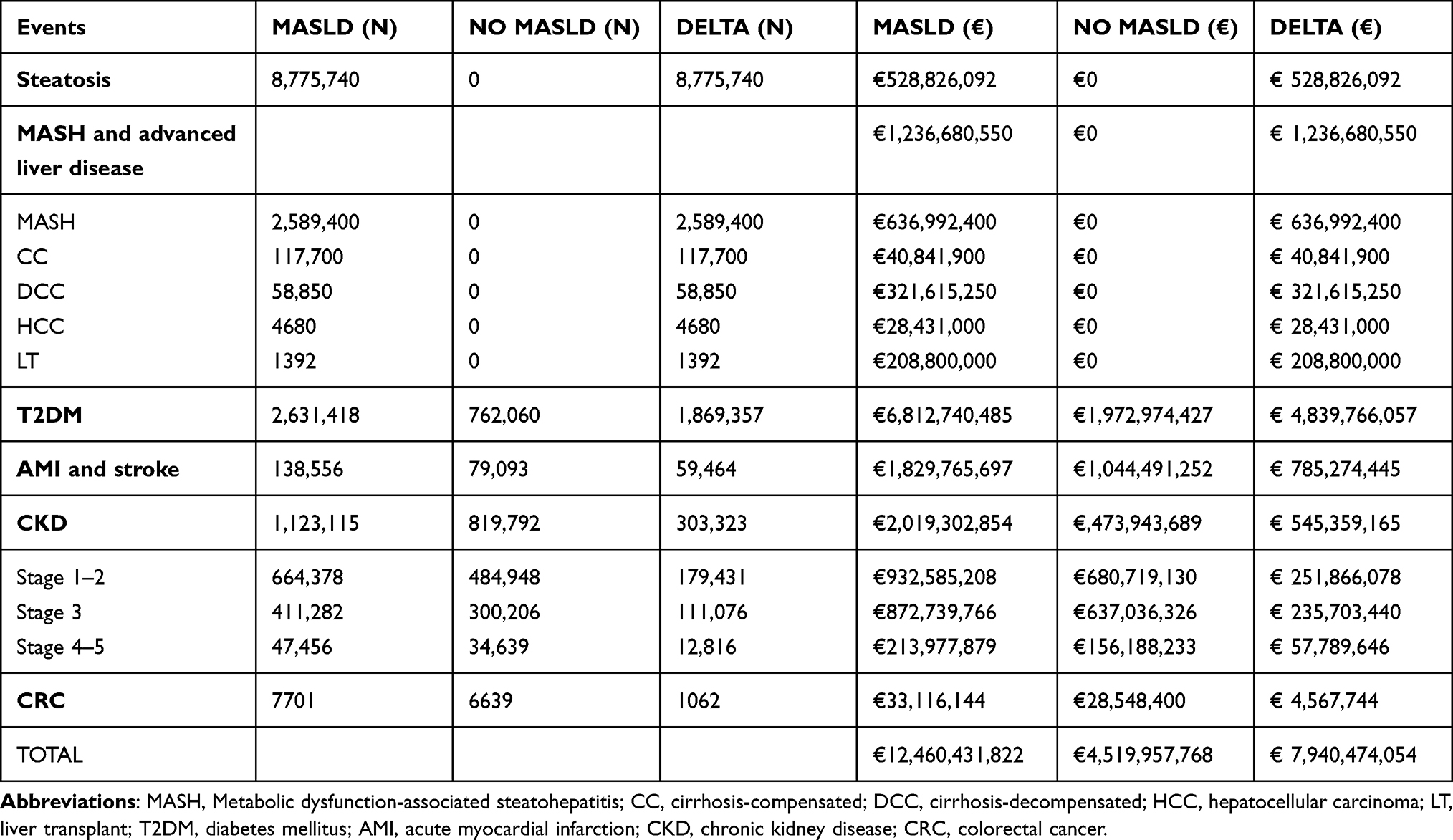 |
Table 4 Total Events and Related Cost Compared: MASLD versus Without MASLD Population |
Comparing the two arms, based on the disease prevalence data application, it is possible to grasp the significant impact related to the presence of steatosis and advanced stages of liver disease as a basic distinctive element between the two groups, resulting in an increase in costs of €528,826,092 for steatosis and €1,236,680,550 for the advanced stages of liver disease (MASH, CC, DCC, HCC). In the advanced stages of liver disease economic evaluation, liver transplant annual estimates (n. 1392) were included, corresponding to a cost of €208,800,000.
The impact of diabetes was particularly significant, resulting in an increase in expenditure of €4,839,766,057, corresponding to the largest cost item given the high prevalence within the population with MASLD, considering the elevated rate of cardiovascular events.
Moreover, to these major items, we have added the costs related to cardiovascular diseases (AMI, stoke), CKD and colorectal cancer with an expense of €785,274,445, €545,359,165, and €4,567,744, respectively.
Overall, considering a MASLD population estimate of 11,546,370, an annual illness impact of €12,460,431,822 was calculated, corresponding to a difference of €7,940,474,054 compared with the same sample without MASLD.
The different impacts in terms of costs of diabetes, MASH, AMI and stroke, CKD, steatosis, and colorectal cancer in the MASLD and non-MASLD groups are shown in Figure 1.
 |
Figure 1 Overall difference in total costs: MASLD versus without MASLD population. Abbreviations: T2DM, diabetes mellitus; MASH, Metabolic dysfunction-associated steatosis Hepatitis (including advanced liver disease and liver transplant costs related to end-stage liver disease management); AMI, acute myocardial infarction; CKD, chronic kidney disease; CRC, colorectal cancer. |
The analysis also estimated the number of deaths attributable to the two populations and their relative differences (Table 5). The presence of MASLD resulted in a greater number of deaths, particularly due to advanced liver disease (DCC, CC, HCC, LT), colorectal cancer, and cardiovascular diseases (Table 5).
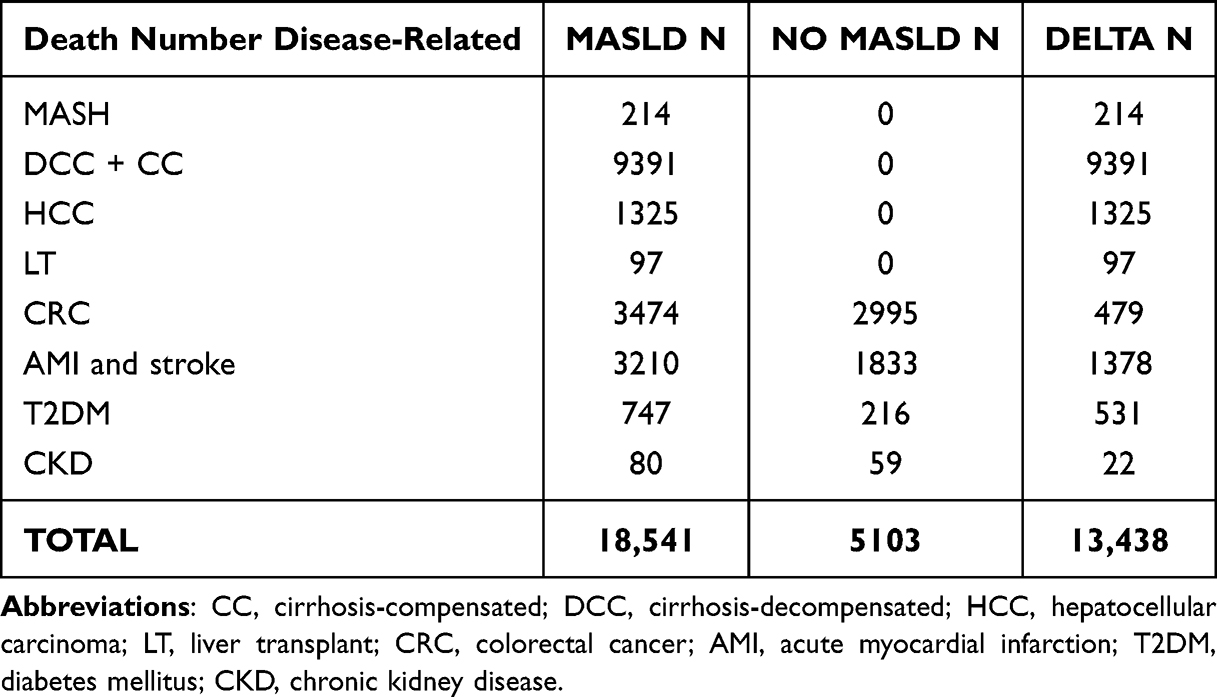 |
Table 5 Impact of Disease on Mortality: MASLD versus Without MASLD Population |
Overall, the MASLD population is expected to experience 13,438 additional deaths annually (Figure 2).
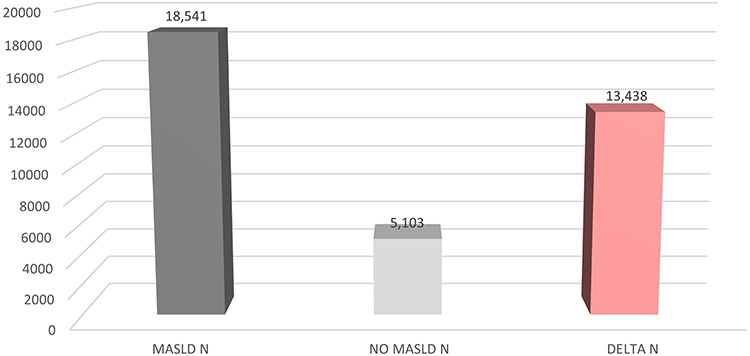 |
Figure 2 Total deaths: MASLD versus without MASLD population. |
The OWSAs demonstrated the robustness of the results. The main input data and assumption variation did not result in significant deviations from the base case findings, as shown in Figure 3. Compared to an increase in cost for MASLD versus non-MASLD population reported for the base case equal to €7.9 million, the sensitivity analysis documented a maximum value corresponding to 10% costs increase, with a result equal to €8.7 million and a minimum value corresponding to a 10% costs reduction equal to €7.1 million.
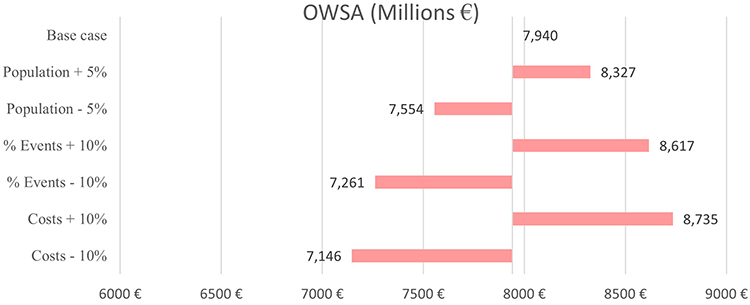 |
Figure 3 Deterministic one-way sensitivity analysis results. |
Probabilistic analysis also confirmed the robustness of the results by evaluating the uncertainty of the cost parameter; 90% of the values were between €7.2 billion and €8.8 billion, (Figure 4).
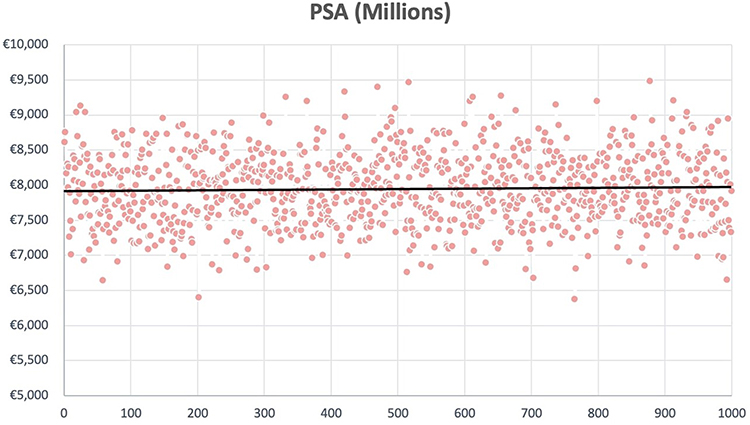 |
Figure 4 Probabilistic sensitivity analysis results. |
Discussion
In a previous study, we evaluated the epidemiologic and economic burden of NAFLD/MASH among the T2DM population,38 while in this study, we have further expanded the magnifying glass on the huge social issue of MASLD in the Italian general population, a condition involving multi-organ impairment that is strictly associated with individual behaviors. From this point of view, T2DM represents the main complication and cost item of MASLD, accounting for approximately two-thirds of all cases of diabetes.
In Italy, the estimated population suffering from MASLD is 11,546,370, corresponding to 19.6% of the general population. The annual burden of MASLD disease in terms of mortality and healthcare expenses, as resulting from the Italian NHS perspective adoption, is very impressive: total direct healthcare costs amount to €7,940,474,054, which correspond to about 6% of national healthcare expenditure for 2023; in addition, MASLD accounts for 13,438 deaths per year.
Among the estimated population suffering from MASLD in Italy, we counted 22.79% of subjects with T2DM. Considering the annual incidence of T2DM (350,000 new diagnoses per year) and the prevalence of MASLD among T2DM, we can deduce that 238,000 patients shift from MASLD to T2DM every year.10
T2DM represents the first and preponderant cost item among MASLD (€4,839,766,057/year), producing 62.6% of the total expenditure for this metabolic disease; therefore, interventions aimed at reducing the economic burden of MASLD must be targeted mainly to prevent its development towards diabetes.
Considering the overall MASLD individuals, 72.37% were affected by hepatic steatosis, 22.43% had MASH, and a minimal share of subjects suffered from HCC (0.80%), severe chronic kidney disease (stage IV–V: 0.41%), and colorectal cancer (0.07%). Liver impairment represents a lower burden in terms of costs (overall €1,765,506,642, 22.2% of total costs, adding steatosis and MASH, including liver transplantation costs), but the highest in terms of lethality, accounting for 11,028 deaths per year, equal to 82.1% of the annual MASLD-related mortality.
Cardiovascular complications (AMI and stroke), accounting for €785,274,445 and 1378 deaths per year, ranked third considering the combinations of cost and lethality. However, they would probably come first if we also considered the CV events already included among the complications of T2DM-MASLD subjects. In addition, CV-related mortality could increase if we consider also T2DM related CV deaths, which are often not attributed to diabetes in Italian death statistical reports.8
The annual cost of chronic kidney disease remains above half a billion (€545,359,165), and MASLD-related colorectal cancer is responsible for 479 deaths per year (3.6% of total MASLD-related deaths).
Therefore, cost analysis of MASLD complications showed a frank predominant burden of chronic metabolic and hepatic illnesses: in fact T2DM and steatosis-MASH produce 62.5% and 22.2% of overall health spending, respectively, whereas acute cardiovascular complications (AMI and stroke) and renal impairment are separately responsible of 10.16% and 7.05% of cost weight; last but not least, minor cost is associated to colorectal cancer (0.06%), due to lower incidence and higher mortality. Beyond the evaluation of the global economic burden of the disease, it is interesting to highlight that the differential per capita cost related to MASLD subjects amounts to €688 per year. Therefore, this figure could be used as a reference for assessing the cost-effectiveness of treatments aimed at stopping the evolution of the MASLD.
Sensitivity analysis showed that hypothetical variation of ±5% regarding population data input and ±10% regarding costs and MASLD related events could result in a range of global direct cost varying from €7.1 billion to €8.7 billion, corresponding respectively to 5.4% and 6.6% of annual global sanitary expenditure.
The time lag necessary to achieve an effective reduction in the incidence of MASLD-related complications after starting an effective therapeutic measure remains to be evaluated. During this period, the costs of treatment will be superimposed on the costs of the disease. Nevertheless, our study did not include an estimate of indirect costs or its impact in terms of the impairment of national GDP.
Moreover, the early role of inflammation in the development of the disease should be considered as a target to treat. Clinical investigation of the presence of sarcopenia as well as the detection of inflammation PCR ratio should be performed and monitored after early clinical intervention (lifestyle changes, drug treatment).14,39
Clinical implications of MASLD are very relevant: an early detection of the disease among unaware population as well as a consequent intervention (lifestyle, drugs) aimed at improving body weight and reducing liver fat accumulation could consent to delay, if not to avoid, the development of all the MASLD related complications (diabetes, MI, stroke, CKD, liver cirrhosis, and so on). The limitations of our study lie in the lack of a direct estimate of the real prevalence of MASLD among the Italian population; therefore, we preferred to underestimate the possible prevalence and maximize the simplicity of our model.
Finally, our study adopted international data when national data were not available. The point of strength of our work is that it is the first study to have evaluated the economic burden of MASLD among the Italian population, as well as to have analyzed MASLD-related diseases in an innovative way, so that T2DM can be, at least partially, seen as a complication of hepatic disease.
Conclusion
If obesity and diabetes mellitus represent a pandemic giant worldwide for the next few decades, MASLD will provide their ominous shadow. The data emerging from our study are impressive, both in terms of the number of subjects involved, amounting to approximately one-fifth of the Italian population, and the economic burden (€7.94 billion per year). A recent study evaluating the economic burden of obesity in Italy documented a similar direct cost profile (€7.89 billion) with a higher impact on cardiovascular diseases (€6.66 billion).40 Even if the two populations are largely overlapping, we believe that the basic behavioral and pharmacological treatment could be the same, reserving more targeted interventions, to prevent new cases of T2DM and to provide an early treatment of MASH.
Therefore, the growing epidemiological impact of MASLD, obesity and its complications, associated with the related cardiovascular diseases, will represent a huge economic burden for healthcare services worldwide for the next decades, and a holistic approach to the person (mainly behaviors lifestyle changes) to control the dramatic health and economic impact will be the first step to take.
Specific drugs for MASLD are not yet available. However, studies are underway on many molecules, and meanwhile combination pharmaceutical therapies can provide an adequate control of MASLD and its complications.
Data Sharing Statement
The original contributions of this study are included in the article, and further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
For the development of this study, it was not necessary to proceed with the request for ethical approval and consent to participate, and previously published and validated literature sources were adopted.
Acknowledgment
This paper has been uploaded to Research Square as a preprint: https://www.researchsquare.com/article/rs-3755157/v1
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by an unconditional grant and exclusive grant from Novo Nordisk. The sponsors had no role in the design, execution, interpretation, or writing of the study.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. De A, Bhagat N, Mehta M, Taneja S, Duseja A. Metabolic dysfunction-associated steatotic liver disease (MASLD) definition is better than MAFLD criteria for lean patients with NAFLD. J Hepatol. 2023;S0168-8278(23):5044
2. Boccatonda A, Andreetto L, D’Ardes D, et al. From NAFLD to MAFLD: definition, pathophysiological basis, and cardiovascular implications. Biomedicines. 2023;11:883. doi:10.3390/biomedicines11030883
3. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018;67:328–357. doi:10.1002/hep.29367
4. Eslam M, Sanyal AJ, George J. MAFLD: a consensus-driven proposed nomenclature for metabolic-associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014.e1991. doi:10.1053/j.gastro.2019.11.312
5. Zhang HJ, Wang YY, Chen C, Lu YL, Wang NJ. Cardiovascular and renal burdens of metabolic-associated fatty liver disease from serial US national surveys, 1999-2016. Chin Med J. 2021;134(13):1593–1601. doi:10.1097/CM9.0000000000001513
6. Lim GEH, Tang A, Ng CH, et al. An observational data meta-analysis on the differences in prevalence and risk factors between MAFLD vs NAFLD. Clin Gastroenterol Hepatol. 2023;21(3):619–629.e7. doi:10.1016/j.cgh.2021.11.038
7. Chan KE, Koh TJL, Tang ASP, et al. Global prevalence and clinical characteristics of metabolic-associated fatty liver disease: a meta-analysis and systematic review of 10 739 607 individuals. J Clin Endocrinol Metab. 2022;107:2691–2700. doi:10.1210/clinem/dgac321
8. 16th Italian barometer diabetes report, diabetes monitor journal, IBDO Foundation. 2023:67–72
9. Younossi ZM, Golabi P, De Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71:793–801. doi:10.1016/j.jhep.2019.06.021
10. ISTAT. Popolazione residente 1° gennaio 2023. Available from: https://demo.istat.it/app/?i=POS&l=it.
11. Aktas G, Khalid A, Kurtkulagi O, et al. Poorly controlled hypertension is associated with elevated serum uric acid to HDL-cholesterol ratio: a cross-sectional cohort study. Postgrad Med. 2022;134(3):297–302. PMID: 35142235. doi:10.1080/00325481.2022.2039007
12. Aktas G, Zahid Kocak M, Taslamacioglu Duman T, Erkus E. Mean Platelet Volume (MPV) as an inflammatory marker in type 2 diabetes mellitus and obesity. Bali Medl J. 2018;7(3):650–953. doi:10.15562/bmj.v7i3.806
13. Aktas G, Yilmaz S, Kantarci DB, et al. Is serum uric acid-to-HDL cholesterol ratio elevation associated with diabetic kidney injury? Postgraduate Med. 2023;135(5):519–523. doi:10.1080/00325481.2023.2214058
14. Zhao Q, Yin Y, Deng Y. Metabolic associated fatty liver disease and sarcopenia additively increase mortality: a real-world study. Nutr Diabetes. 2023;13:21. doi:10.1038/s41387-023-00250-6
15. Bonora E. La pandemia di diabete in Italia. L’Endocrinologo. 2022;23:337–344. Italian
16. Anstee QM, Targher G, Day CP. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat Rev Gastroenterol Hepatol. 2013;10:330–344. doi:10.1038/nrgastro.2013.41
17. Mantovani A, Lombardi R, Cattazzo F, et al. MAFLD and CKD: an updated narrative review. Int J Mol Sci. 2022;23:7007. doi:10.3390/ijms23137007
18. De Nicola L, Donfrancesco C, Minutolo R, et al. Epidemiologia della MRC in Italia: stato dell’arte e contributo dello studio CHARES. G Ital Nefrol. 2011;28(4):401–407. Italian
19. Mantovani A, Zaza G, Byrne CD, et al. Nonalcoholic fatty liver disease increases risk of incident chronic kidney disease: a systematic review and meta-analysis. Metabolism. 2018;79:64–76. doi:10.1016/j.metabol.2017.11.003
20. Sun DQ, Jin Y, Wang T, et al. MAFLD and risk of CKD. Metabolism. 2021;115:154433. doi:10.1016/j.metabol.2020.154433
21. SNLG-Regioni. La nefropatia diabetica: linee guida diagnostiche e terapeutiche Zadig- Milano. 2016:23. Italian
22. Lee H, Lee HW, Kim SU, Kim HC. Metabolic dysfunction–associated fatty liver disease increases colon cancer risk: a nationwide cohort study. Clin Transl Gastroenterol. 2022;13(1):e00435. doi:10.14309/ctg.0000000000000435
23. Pipitone RM, Ciccioli C, Infantino G, et al. MAFLD: a multisystem disease. Ther Adv Endocrinol Metab. 2023;14:1–23. doi:10.1177/20420188221145549
24. Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease—meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. doi:10.1002/hep.28431
25. Ferrarese A, Battistella S, Germani G, et al. Nash up, virus down: how the waiting list is changing for liver transplantation: a single center experience from Italy. Medicina. 2022;58(290):1–8. doi:10.3390/medicina58020290
26. Estes C, Anstee QM, Arias-Loste MT, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016-2030. J Hepatol. 2018;69(4):896–904. doi:10.1016/j.jhep.2018.05.036
27. AIOM. I numeri del cancro in Italia 2022. Intermedia Editore. Italian. Available from: https://www.aiom.it/wp-content/uploads/2022/12/2022_AIOM_NDC-web.pdf.
28. Gallo M, Colandrea C, Ceccolini C, et al. Rapporto annuale sull’attività di ricovero ospedaliero - DATI SDO 2022. Ministero della Salute, ex Direzione generale della programmazione sanitaria - Ufficio 6 Viale Giorgio Ribotta, 5 – 00144 Roma. ISBN: 9791280892072. Italian. Available from https://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=3441.
29. AISF. Libro bianco AISF 2011. Proposta per un piano nazionale per il controllo delle malattie epatiche. Italian. Available from: https://www.webaisf.org/wp-content/uploads/2019/01/libro-bianco-aisf-2011.pdf.
30. Lucioni C, Mazzi S, Rossi S, et al. Percorsi terapeutici e costi sanitari di pazienti ricoverati per un evento cardiovascolare in Italia. Glob Reg Health Technol Assess. 2016;3(2):80–91. Italian.
31. Pagano E, De Rosa M, Rossi E, et al. The relative burden of diabetes complications on healthcare costs: the population-based CINECA-SID ARNO diabetes observatory. Nutr Metab Cardiovasc Dis. 2016;26(10):944–950. doi:10.1016/j.numecd.2016.05.002
32. Jommi C, Armeni P, Battista M, et al. IRIDE Study Group. The cost of patients with chronic kidney failure before dialysis: results from the IRIDE observational study. Pharmacoecon Open. 2018;2(4):459–467. doi:10.1007/s41669-017-0062-z
33. Francisci S, Guzzinati S, Mezzetti M, et al. Cost profiles of colorectal cancer patients in Italy based on individual patterns of care. BMC Cancer. 2013;13:329. doi:10.1186/1471-2407-13-329
34. Tariffe delle prestazioni di assistenza specialistica ambulatoriale. 2013 Allegato 3 ministero della Salute - Direzione generale della programmazione sanitaria. Supplemento ordinario n. 8 alla Gazzetta Ufficiale. Serie generale - n. 23. Italian.
35. ISTAT. Il diabete in Italia. Italian. Available from: https://www.istat.it/it/files/2017/07/REPORT_DIABETE.pdf.
36. Saglietto A, Manfredi R, Elia E, et al. Cardiovascular disease burden: Italian and global perspectives. Minerva Cardiol Angiol. 2021;69(3):231–240. PMID: 33703858. doi:10.23736/S2724-5683.21.05538-9
37. Mortalità per insufficienza renale cronica. Italian. Available from: https://www.ars.toscana.it/banche-dati/dettaglio_indicatore-1329-mortalita-insufficienza-renale-cronica?provenienza=dettaglio_indicatore_consigliati&par_top_geografia=090&dettaglio=ric_anno_geo_ausl.
38. Torre E, Di Matteo S, Bruno GM, et al. Economic Burden of Non-Alcoholic Steatohepatitis (NASH) among diabetic population in Italy: analysis and perspectives. Clinicoecon Outcomes Res. 2022;14:607–618. doi:10.2147/CEOR.S371778
39. Tarantino G, Sinatti G, Citro V, Santini SJ, Balsano C. Sarcopenia, a condition shared by various diseases: can we alleviate or delay the progression? Intern Emerg Med. 2023;18(7):1887–1895. PMID: 37490203; PMCID: PMC10543607. doi:10.1007/s11739-023-03339-z
40. D’Errico M, Pavlova M, Spandonaro F. The economic burden of obesity in Italy: a cost-of-illness study. Eur J Health Econ. 2022;23:177–192. doi:10.1007/s10198-021-01358-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.