")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Economic Evaluation of the Use of FeNO for the Diagnosis and Management of Asthma Patients in Primary Care in Sweden
Authors Darbà J , Ascanio M, Syk J , Alving K
Received 15 February 2021
Accepted for publication 25 March 2021
Published 23 April 2021 Volume 2021:13 Pages 289—297
DOI https://doi.org/10.2147/CEOR.S306389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samer Hamidi
Josep Darbà,1 Meritxell Ascanio,2 Jörgen Syk,3– 5 Kjell Alving4
1Department of Economics, Universitat de Barcelona, Barcelona, Spain; 2BCN Health Economics & Outcomes Research, S.L., Barcelona, Spain; 3Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden; 4Department of Women’s and Children’s Health, Uppsala University, Uppsala, Sweden; 5Academic Primary Health Care Centre, Stockholm, Sweden
Correspondence: Josep Darbà
Department of Economics, Universitat de Barcelona, Diagonal 696, Barcelona, 08034, Spain
Tel +34 934020110
Fax +34 934039082
Email [email protected]
Objective: To determine the economic impact of the fraction of exhaled nitric oxide (FeNO) in asthma diagnosis and management in primary care in Sweden.
Methods: An economic model has been developed to determine the economic impact of the fraction of exhaled nitric oxide (FeNO) in asthma diagnosis and management in primary care in Sweden. The model includes the use and cost of commonly used tests, the associated outcomes and diagnostic accuracy. We compared FeNO with spirometry and reversibility testing, methacholine challenge test, allergy testing, and blood eosinophil count. One-way sensitivity analyses were performed to confirm the robustness of results.
Results: Adding FeNO measurement in asthma diagnosis resulted in cost savings of SEK 672 per patient by the fourth year. The use of FeNO testing in asthma management proved to be a dominant strategy when compared with each other test except methacholine challenge test. Sensitivity analyses confirmed the robustness of the results.
Conclusion: Introducing FeNO testing in clinical practice for the diagnosis and management of asthma in primary care in Sweden is less costly than standard methods while providing similar health benefits.
Keywords: asthma, management, diagnosis, FeNO, exhaled nitric oxide, health economy
Introduction
According to the Global Initiative for Asthma (GINA) description, asthma is
a heterogeneous disease, usually characterised by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation.1
In Europe, about 30 million children and adults under 45 years of age have asthma.2 In most European countries, the prevalence of asthma increased substantially but in Western Europe the increase has stabilized in the past decade.2 The rates of disease tend to be higher in northern and Western Europe where the prevalence may be higher than 10%.2
In 2009, the first systematic review of the literature about the economic burden of asthma was published.3 The authors found that hospitalization and medications were the most important drivers of direct costs; work and school absence accounted for the greatest percentage of indirect costs. Globally, asthma costs were increasing, closely correlated with comorbidities, age and asthma severity.
In Sweden, a study conducted in 352 subjects surveyed about asthma-specific resource use concluded that the total costs of asthma for the society could be estimated to SEK 3.7 billion in the age range of 25–56 years, and approximately SEK 7.4 billion in the whole Swedish population.4 Disease severity and increasing age were the main cost drivers.
According to the national guidelines,5 a diagnosis of asthma in Sweden is mainly based on the use of family and medical history for finding out symptoms and symptom-triggering factors, and by performing spirometry with reversibility test.
However, in mild and moderate asthma, lung function can be normal at rest and in quieter periods of illness. Normal results from a spirometry cannot therefore exclude asthma. In those cases where the history indicates asthma disease, the health care system therefore uses other complementary diagnostic methods, such as measurement of peak expiratory flow rate (PEFR) variability, allergy investigation, measurement of the fraction of nitric oxide in exhaled air (FeNO), and methacholine challenge test.5
Spirometry with reversibility testing, allergy assessment and history finding can be performed in both primary care and in specialist asthma clinics.5 The same applies to the measurement of PEFR variability. However, methacholine challenge test and FeNO tests are still mainly used at specialist clinics.5
The objective of this study was to estimate the economic consequences of introducing FeNO testing in clinical practice for diagnosis and management of asthma patients in primary care in Sweden.
Methods
Economic Models
An economic model has been developed for asthma diagnosis and management in primary health care in Sweden, using Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA, USA). The use and cost of each standard test, as well as associated outcomes, such as diagnostic accuracy, were derived from the medical literature appropriate for the country under study, for incorporation into the model and subsequent calculation of cost data. For each test included in this model, the cost of the diagnostic test, diagnosis and control visits and exacerbations are calculated. Test and exacerbations costs were obtained from the literature. The cost of the diagnosis and control visits was calculated multiplying the number of visits by the cost of each visit.
For asthma diagnosis, we compared FeNO measurement with standard diagnostic tests used in Swedish primary care clinical practice, including spirometry and reversibility testing, methacholine challenge test (after referral to secondary care), allergy testing, and blood eosinophil count. In the base-case analysis, FeNO measurement was compared individually with each test.
For asthma management, we assessed the impact on asthma outcomes of monitoring with FeNO measurement versus the tests used in the diagnosis analysis during 2020–2023. This model assessed the impact of an incremental use of FeNO, not a replacement of the standard tests by FeNO use.
We have used conservative assumptions and sought to include all relevant data from clinical studies and asthma guidelines. Where evidence was not yet fully available, we have used data collected by using a questionnaire from two Swedish specialists of asthma, a Swedish primary care clinical expert and a Swedish academic expert.
Study Population
In the base case, the cohort comprised 10,421,400 residents in Sweden in 2020. The populations for 2020–2023 were obtained from the Central Bureau of Statistics of Sweden (SCB).6 The target prevalence was obtained by dividing the population in adults and children (obtained from SCB)6 and then applying the prevalence of asthma in each patient population (Figure 1). As no updated asthma prevalence for the Swedish population was available, we obtained asthma prevalence for adults and children from the Swedish asthma experts.
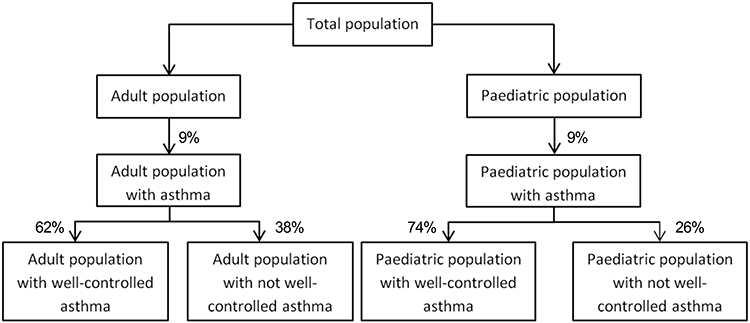 |
Figure 1 Study population. |
Data Sources
The selection of diagnostic tests for comparison with FeNO measurement was based on information about daily use in clinical practice from the two Swedish asthma experts. To avoid making assumptions about the frequency of use for each test in clinical practice, as these data are not available partly due to lack of a definite gold standard, we estimated frequency weights for each test according to the information provided by the Swedish experts.
The sensitivity and specificity of each diagnostic test were obtained from five different published articles7–11 (Table 1). Karrasch et al7 assessed FeNO accuracy for making the diagnosis of asthma by conducting a systematic review and diagnostic meta-analysis of 26 different studies, which account for a total of 4518 participants. Smith et al8 evaluated the diagnostic utility of FeNO testing and conventional test of lung function in 47 patients with symptoms suggestive of asthma. Berkman et al9 assessed the diagnostic utility of FeNO compared with conventional bronchial provocation tests in a prospective study with a group of 85 patients using a clinical follow up of 24 months to define asthma. The sensitivity and specificity of blood eosinophil count were derived from the observational study by Hunter et al10 that compared tests accuracy in 21 controls, 69 patients with asthma and 20 patients with an asthma diagnosis with an alternative explanation for their symptoms. Finally, Gallmeier et al11 evaluated the diagnostic utility of skin prick tests (SPTs) and radioallergosorbent tests (RASTs) in 1185 patients during 20 years.
 |
Table 1 Sensitivity and Specificity of Diagnostic Tests for Asthma |
The type of drugs used in asthma management was obtained from our Swedish experts, as there were no published evidence available. The evidence on the reduction of the use of inhaled corticosteroids (ICS) is based on a systematic review that found an approximately 27% average reduction of ICS when FeNO monitoring was used in adult patients.12
Finally, data about the number of exacerbations per test used were obtained from Syk et al.13 This study registered the number of exacerbations in the FeNO group and in the control group, obtaining the proportion of patients experiencing moderate or severe exacerbations with and without the use of FeNO measurement.
Costs and Use of Resources
The economic assessments were conducted from a Swedish health-care payer perspective (Swedish crowns [SEK] 2019), taking into account the cost for the health-care system, and included changes in resource use, namely the direct medical costs, including costs of diagnostic tests, primary care GP visits, primary care nurse visits, laboratory visits, and treatment, as available from published data (Table 2). Drug costs were obtained from TLV, the Swedish drug price database.14 The cost related to the use of each test included the test cost, the number of primary care GP visits, the number of primary nurse visits, and the laboratory visits. The drug doses and use were derived from Ställberg et al,15 a study that compared the asthma control in 2001 and 2005 in the primary care setting in Sweden. The number of diagnostic and control visits were derived from the National guidelines for the treatment of asthma and COPD. The cost of a FeNO test was based on the figures provided by Intramedic AB,16 the Swedish distributor of NIOX VERO®,17 a device for monitoring FeNO. Exacerbations costs in the primary care setting were obtained from Lane et al.18 In this study, the authors conducted a prospective study that assessed the local cost of asthma exacerbations managed in either primary or secondary care.
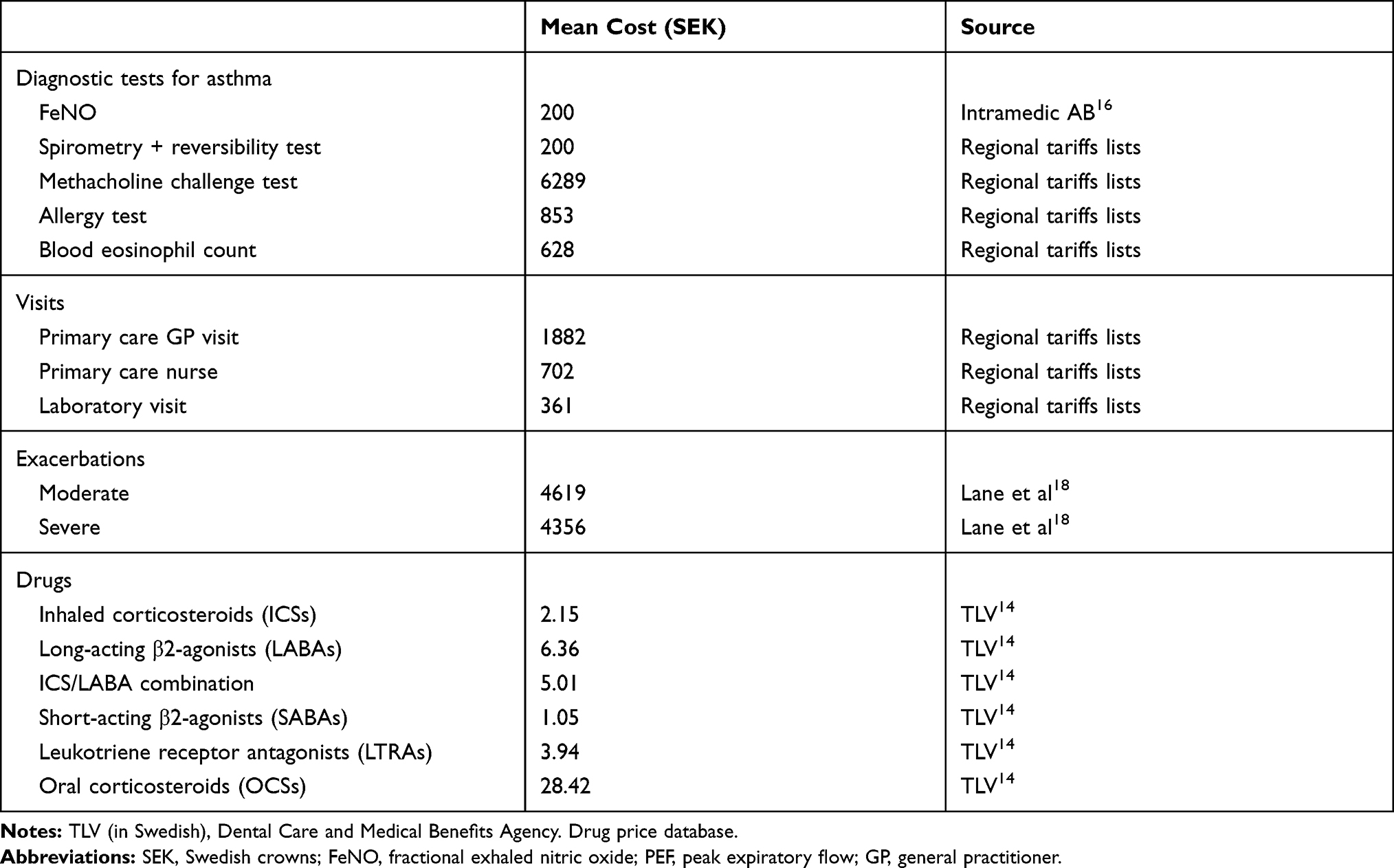 |
Table 2 Unit Costs (SEK 2019) Used in the Model, from a Swedish Health-Care Payer Perspective |
According to the experts’ opinion, the commonly used diagnostic methods in Swedish primary health care were weighted as follows:
- Fractional exhaled nitric oxide (FeNO): relative frequency weight in adult population <1%; in paediatric population <1%.
- Spirometry and reversibility testing: relative frequency weight in adult population 75%; in paediatric population 50%.
- Methacholine challenge test: relative frequency weight in adult population 10%; in paediatric population 10% (after referral to a specialist clinic).
- Allergy testing, including skin prick test and serum IgE: relative frequency weight in adult population 50%; in paediatric population 75%.
- Blood eosinophil count: relative frequency weight in adult population <1%; in paediatric population <1%.
Sensitivity Analyses
We performed numerous one-way sensitivity analyses to examine the robustness of both diagnostic and management models. The parameters assessed in the one-way sensitivity analysis for both asthma management and diagnosis were:
Ethics
No patient data have been analysed and no patients were involved in this study.
Data Availability
No datasets were generated or analysed during the current study.
Results
Base Case
The use of FeNO tests in asthma management resulted in savings ranging from SEK 2181 to SEK 7842 per patient when compared to the standard tests included in this study (Table 3). The use of FeNO monitoring in asthma management improved asthma care and generated savings for the Swedish health care system. FeNO was related to cost savings due to its lesser use of resources represented by fewer visits to the primary care GP when compared to the standard tests.
 |
Table 3 Base Case Results: Management of Asthma |
In this study, the efficacy is strongly associated with the test’s sensitivity, which allows for better management of asthma. Methacholine challenge test showed the higher sensitivity (88%), which means that this test is the most effective tests for asthma management. The least effective standard test was the blood eosinophil count, with a sensitivity of 21%, followed by the combination of spirometry and reversibility test, with a sensitivity of 35% (Table 3). So, the combination of less costs and better efficacy when compared with standard tests, made FeNO testing a dominant option over all the standard tests except methacholine challenge test. FeNO showed to be less effective but also less costly than methacholine challenge test.
The progressive introduction of FeNO testing in asthma diagnosis resulted in increasing savings during the 2021–2023 period (Table 4). In the last year of study, the adding of FeNO testing resulted in total savings of SEK 128,429,100 in adult patients (SEK 495 per patient), and SEK 99,147,258 in paediatric patients (SEK 1679 per patient). Both patient populations taken together, the savings were SEK 227,576,358 (SEK 672 per patient).
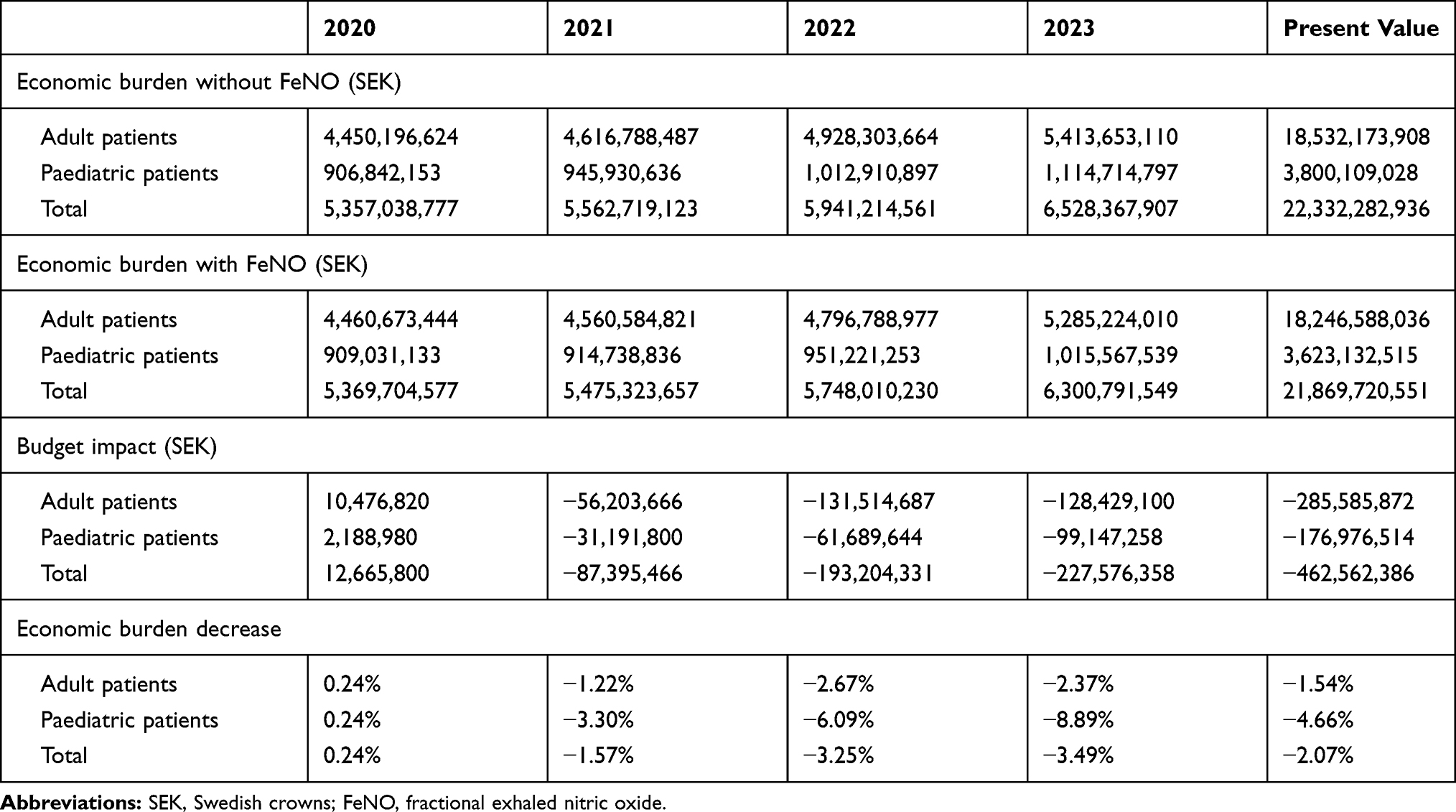 |
Table 4 Base Case Results: Diagnosis of Asthma |
Sensitivity Analyses
The one-way sensitivity analysis (Table 5) showed that the introduction of FeNO in asthma management was dominant for all parameter changes. Regarding FeNO diagnosis, savings per patient were most sensitive to asthma prevalence and cost of standard tests but also to FeNO cost. Assuming an asthma prevalence from 8% to 35%, savings ranged from SEK 411,166,565 to SEK 1,850,249,543. When increasing the standard tests cost from 50% to 150%, savings varied from SEK 537,335,517 to SEK 686,881,781. Finally, the variation of FeNO cost, considering an increment from 10% to 20%, resulted in a variation of savings from SEK 460,297,825 to SEK 461,430,105. In all the other parameter changes, savings per patient remained stable.
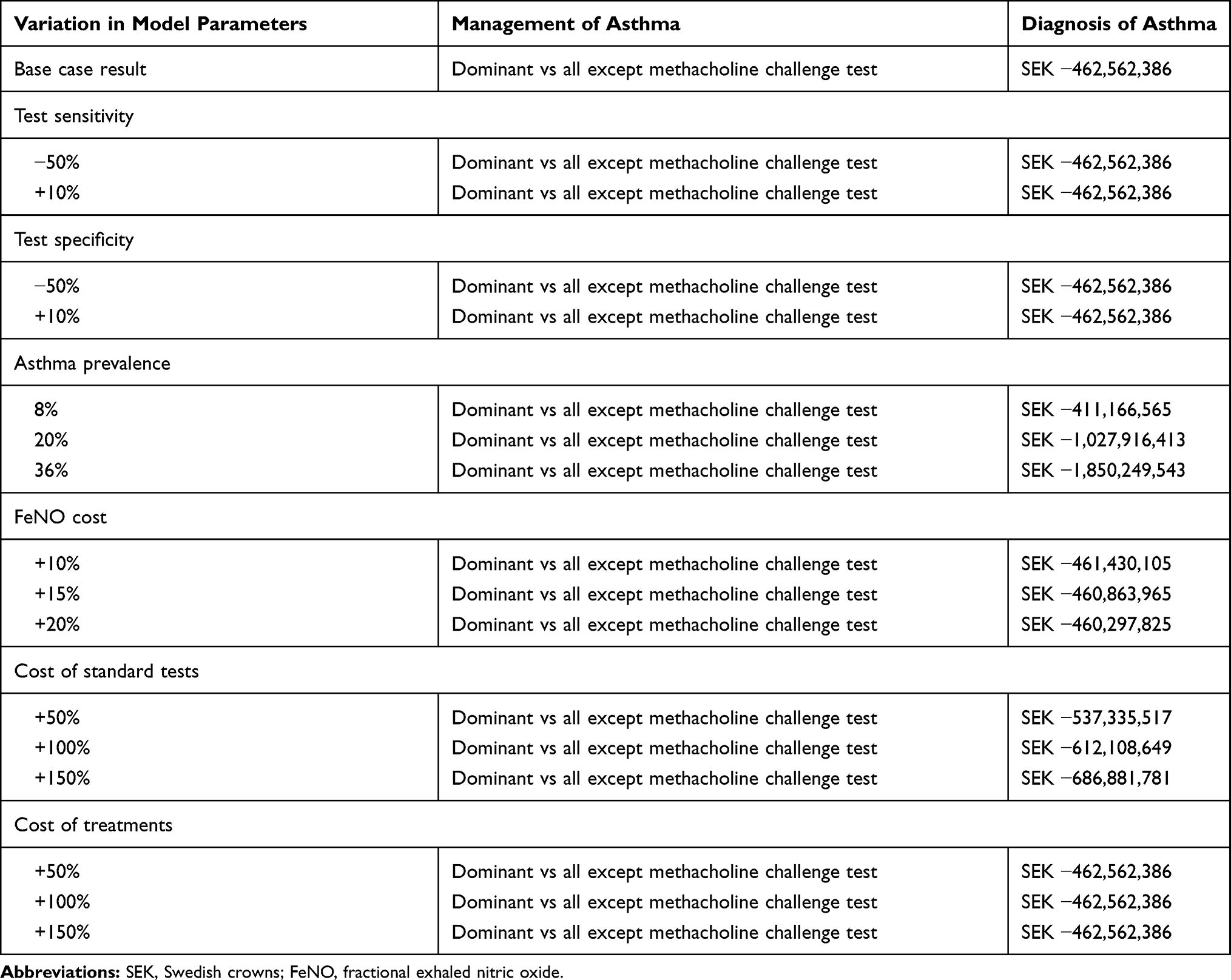 |
Table 5 Sensitivity Analysis Results |
Discussion
This study has evaluated the economic consequences of introducing FeNO testing in clinical practice for diagnosis and management of asthma patients in primary health care in Sweden. At a reimbursement price of SEK 200, asthma diagnosis with the progressive introduction of FeNO testing in clinical practice costs SEK 672 less per patient by the fourth year as compared with standard diagnostic tests. Asthma management using FeNO testing instead of standard tests resulted in a dominant strategy when compared with each test. FeNO testing resulted in savings ranging from SEK 2181 to SEK 7842 per patient and a specificity difference ranging from 45% to 67% when compared to the standard tests included in this study. The savings related to the use of FeNO can be due to different reasons related to the reduction of asthma exacerbation, hospitalized stay, and cost of treatment.
The results of the sensitivity analyses were consistent with the base-case analysis for both asthma management and diagnosis, showing that the base-case models are robust. For asthma management, FeNO testing remained the dominant strategy in all cases. Similarly, for asthma diagnosis, savings per patient were most sensitive to asthma prevalence and cost of standard tests but also to FeNO cost.
In clinical practice, a diagnosis of asthma in Sweden is mainly based on the use of family and medical history for finding out symptoms and symptom-triggering factors, and by performing spirometry with reversibility test.5 For that reason and due to experts’ suggestion, we analysed the use of FeNO in conjunction with other diagnostic tests. This approach is also supported by the results obtained in a recent study in which the use of FeNO testing together with spirometry improved diagnostic confidence and therapeutic decision-making regarding more than 90% of patients with nonspecific respiratory symptoms managed in primary care.22 In addition the use of FeNO has been considered as adjuvant tool for diagnosis of type 2 asthma,1 so it could not replace spirometry of methacholine challenge test. Hence, the cost of diagnosis of asthma with FeNO might be higher than standard diagnosis. In the case of non-type 2 asthma, FeNO can provide a more effective approach for asthma in monitoring of airway inflammation to determine risk for future impairment or loss of asthma control during reduction/cessation of ICS treatment, in unmasking non-adherence to corticosteroid therapy and in severe asthma cases tailoring treatment with biological drugs.23
The direct costs obtained for the adult and paediatric populations together (about SEK 6.5 billion) is higher than those reported by Jansson et al.4 That study estimated the societal costs for subjects with asthma by using telephone interviews to 115 randomly selected patients with asthma. The total societal costs of asthma were estimated to SEK 3.7 billion in the age range of 25–56 years, and were considered to be approximately twice as high in the whole population of Sweden, with the direct costs constituting about 31% of total costs (about SEK 2.3 billion). However, that report is approximately 15 years old, and we know that the prevalence of paediatric asthma has increased in Sweden during this time period.
Regarding the cost of asthma treatment by using FeNO for the titration of the ICS dose, some previous studies have been published.24–26 Truong-Thanh et al24 conducted a prospective and randomized study to demonstrate the role of FeNO in association with GINA guidelines for treatment of adult patients with asthma. The study involved 176 patients followed up 9 months. At the end of the study, the FeNO associated to GINA group showed higher reduction of FeNO levels, less moderate asthma patients and lower daily dose of ICS. Dinh-Thi-Dieu et al25 conducted a prospective and descriptive study to evaluate the beneficial role of FENO in combination with GINA guidelines for titration of ICS in asthmatic children. A total of 204 patients were included in this study, and were followed-up to 12 months. This study concluded that the use of FENO in combination with GINA guidelines for ICS titration is useful in reducing the daily ICS dose and treatment cost. Finally, Duong-Quy et al26 conducted a prospective study to analyse the role of FENO measurement for categorizing asthma phenotype and treatment in children. A total of 187 asthmatic children were included and were followed up to 3 months. The level of FENO was significantly reduced after 1 month and normalized at 3 months, and the dose of ICS was significant reduced after 3 months. FeNO has also showed to be a useful biomarker to categorize asthma phenotypes in children.
This is the first economic evaluation of the use of FeNO testing in asthma management and diagnosis in Sweden, but some previous economic studies have been carried out in other European countries and in the US, and in all of them FeNO was related to savings and the same or better health outcomes. Sabatelli et al27 evaluated the cost-effectiveness and budget impact of FeNO monitoring for the management of adult asthma in Spain, with both the cost-effectiveness and budget impact analyses showing savings for the healthcare system when considering the use of FeNO monitoring in primary health care. In other study, Brooks et al28 examined the impact of FeNO monitoring on the cost-effectiveness of asthma management, with FeNO monitoring being cost effective, and related to increased QALYs and decreased health care costs. LaForce et al29 conducted an observational study to determine whether the use of FeNO in the management of asthma is related to more effective and cost-effective treatment decisions, with results showing that the addition of FeNO to standard of care was estimated to save USD 629 per patient per year. Bukstein et al30 assessed the potential US payer cost savings due to the incorporation of FeNO in management or monitoring of difficult-to-treat asthma patients, with all scenarios showing cost and use reduction across all medical resource use parameters. Price et al20 determined the cost-effectiveness of FeNO measurement for asthma diagnosis and management in the UK, with FeNO being less costly and more accurate than standard diagnostic methods and providing similar health benefits. Finally, Berg et al21 assessed the cost-effectiveness of FeNO measurement in asthma diagnosis and management in Germany, showing that the use of FeNO measurement is less costly than asthma management based on standard guidelines and provides similar health benefits.
Although this study is similar to the previously conducted economic evaluations described above, it presents some possible limitations. Indirect costs such as loss of productivity due to disability pensions and absence from work or school due to sick leave were not included in this study since there is no available data on the direct impact of FeNO management. However, inclusion of indirect costs would likely improve the results further, since it has been shown that exacerbations lead to several days off work: on average, 3 days for mild exacerbations and 7 days for moderate and severe exacerbations.27 In the study of Jansson et al,4 indirect costs, including loss of productivity and absence from work due to sick leave, accounted for the 69% of total reported costs.
Conclusion
This study has shown that from the Swedish healthcare payer perspective, introducing FeNO testing in clinical practice for the diagnosis and management of asthma patients in primary care is less costly than standard methods while providing similar health benefits.
The cost savings were seen both in asthma management and diagnosis and were driven mainly by less use of healthcare resources in comparison with standard methods. The clinical benefits were seen in asthma management and were mainly related to the higher sensitivity for FeNO.
Including FeNO to the current set of available diagnostic tests available provides a unique way of detecting airway inflammation, which will complement pulmonary function tests in a cost-effective way. Similarly, adding FeNO testing into asthma management may facilitate the identification of patients at risk for future exacerbations and would therefore be related to cost savings in both adult and paediatric patients. FeNO use could also be potentially cost-effective in reducing medication consumption. Moreover, due to the increasing use of new biological therapies in asthma treatment, there will be a growing need for clinically relevant biomarkers to facilitate the identification of appropriate candidates for treatment and to monitor the response to treatment in a cost-effective way.
Acknowledgment
BCN Health Economics and Outcomes Research S.L. provided statistical analysis and editorial support. BCN Health Economics & Outcomes Research services have been funded by Circassia Ltd.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
J Darbà is employed by the University of Barcelona. M Ascanio is an employee of BCN Health Economics & Outcomes Research S.L., Barcelona, Spain, an independent contract health economic organization. K Alving and J Syk are affiliated with Uppsala University. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. K Alving has received a consultancy fee from Intramedic AB. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2019. Available from: https://ginasthma.org/wp-content/uploads/2019/06/GINA-2019-main-report-June-2019-wms.pdf.
2. Gibson GJ, Loddenkemper R, Sibille Y, Lundbäck B, Fletcher M. Lung health in Europe – facts and figures: a better understanding of lung disease and respiratory care in Europe. European Lung Foundation (ELF); 2013. Available from: https://www.europeanlung.org/assets/files/publications/lung_health_in_europe_facts_and_figures_web.pdf.
3. Bahadori K, Doyle-Waters MM, Marra C, et al. Economic burden of asthma: a systematic review. BMC Pulm Med. 2009;9(1). doi:10.1186/1471-2466-9-24
4. Jansson SA, Rönmark E, Forsberg B, et al. The economic consequences of asthma among adults in Sweden. Respir Med. 2007;101(11):2263–2270. doi:10.1016/j.rmed.2007.06.029
5. Socialstyrelsen. Nationella riktlinjer för vård vid astma och KOL. [National guidelines for the treatment of asthma and COPD]. Swedish; 2018. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2018-1-36.pdf.
6. Statistiska centralbyrån (SCB). Sveriges framtida befolkning 2018–2070. [The future population of Sweden 2018–2070]. Swedish; 2018. Available from: https://www.scb.se/contentassets/b3973c6465b446a690aec868d8b67473/be0401_2018i70_br_be51br1801.pdf.
7. Karrasch S, Linde K, Rücker G, et al. Accuracy of FENO for diagnosing asthma: a systematic review. Thorax. 2017;72(2):109–116. doi:10.1136/thoraxjnl-2016-208704
8. Smith AD, Cowan JO, Filsell S, et al. Diagnosing asthma: comparisons between exhaled nitric oxide measurements and conventional tests. Am J Respir Crit Care Med. 2004;169(4):473–478. doi:10.1164/rccm.200310-1376OC
9. Berkman N, Avital A, Breuer R, Bardach E, Springer C, Godfrey S. Exhaled nitric oxide in the diagnosis of asthma: comparison with bronchial provocation tests. Thorax. 2005;60(5):383–388. doi:10.1136/thx.2004.031104
10. Hunter CJ, Brightling CE, Woltmann G, Wardlaw AJ, Pavord ID. A comparison of the validity of different diagnostic tests in adults with asthma. Chest. 2002;121(4):1051–1057. doi:10.1378/chest.121.4.1051
11. Gallmeier K, Becker E, Kirsten A, et al. Prediction of new-onset asthma and nasal allergy by skin prick test and RAST in a cohort of adults. Eur Respir J. 2014;43(1):92–102. doi:10.1183/09031936.00012813
12. Donohue JF, Jain N. Exhaled nitric oxide to predict corticosteroid responsiveness and reduce asthma exacerbation rates. Respir Med. 2013;107(7):943–952. doi:10.1016/j.rmed.2013.02.018
13. Syk J, Malinovschi A, Johansson G, et al. Anti-inflammatory treatment of atopic asthma guided by exhaled nitric oxide: a randomized, controlled trial. J Allergy Clin Immunol Pract. 2013;1(6):639–648. doi:10.1016/j.jaip.2013.07.013
14. Tandvårds- och läkemedelsförmånsverket (TLV). Drug price database. Available from: https://www.tlv.se/beslut/sok-i-databasen.html.
15. Ställberg B, Lisspers K, Hasselgren M, et al. Asthma control in primary care in Sweden: a comparison between 2001 and 2005. Prim Care Respir J. 2009;18(4):279–286. doi:10.4104/pcrj.2009.00024
16. Intramedic AB. Intramedic AB web page. Available from: https://www.intramedic.se/about-us/.
17. NIOX VERO®. NIOX web page. Available from: https://www.niox.com/en/niox-vero/about-niox-vero/.
18. Lane S, Molina J, Plusa T. An international observational prospective study to determine the cost of asthma exacerbations (COAX). Respir Med. 2006;100(3):434–450. doi:10.1016/j.rmed.2005.06.012
19. Enilari O, Sinha S. The global impact of asthma in adult populations. Ann Glob Health. 2019;85(1):2. doi:10.5334/aogh.2412
20. Price D, Berg J, Lindgren P. An economic evaluation of NIOX MINO airway inflammation monitor in the United Kingdom. Allergy. 2009;64(3):431–438. doi:10.1111/j.1398-9995.2008.01855.x
21. Berg J, Lindgren P. Economic evaluation of FE(NO) measurement in diagnosis and 1-year management of asthma in Germany. Respir Med. 2008;102(2):219–231. doi:10.1016/j.rmed.2007.09.008
22. Harnan SE, Tappenden P, Essat M, et al. Measurement of exhaled nitric oxide concentration in asthma: a systematic review and economic evaluation of NIOX MINO, NIOX VERO and NObreath. Health Technol Assess. 2015;19(82):1–330. doi:10.3310/hta19820
23. Mgaloblishvili N, Gotua M. Modern approaches to fractional exhaled nitric oxide as a useful biomarker for allergic asthma phenotyping and management. Georgian Med News. 2017;273:51–55.
24. Truong-Thanh T, Vo-Thi-Kim A, Vu-Minh T, Truong-Viet D, Tran-van H, Duong-Quy S. The beneficial role of FeNO in association with GINA guidelines for titration of inhaled corticosteroids in adult asthma: a Randomized Study. Adv Med Sci. 2020;65(2):244–251. doi:10.1016/j.advms.2020.03.001
25. Dinh-Thi-Dieu H, Vo-Thi-Kim A, Tran-van H, Tang-Thi-Thao T, Duong-Quy S. Study of the beneficial role of exhaled nitric oxide in combination with GINA guidelines for titration of inhaled corticosteroids in children with asthma. J Breath Res. 2020;14(2):026014. doi:10.1088/1752-7163/ab6809
26. Duong-Quy S, Nguyen-Thi-Bich H, Le-thi-minh H, Timothy C. The use of exhaled nitric oxide (NO) to categorize asthma phenotype and treatment in children - results from national hospital of pediatrics. Eur Respir J. 2018;52(suppl 62):PA1315.
27. Sabatelli L, Seppälä U, Sastre J, Crater G. Cost-effectiveness and budget impact of routine use of fractional exhaled nitric oxide monitoring for the management of adult asthma patients in Spain. J Investig Allergol Clin Immunol. 2017;27(2):89–97. doi:10.18176/jiaci.0103
28. Brooks EA, Massanari M. Cost-effectiveness analysis of monitoring fractional exhaled nitric oxide (FeNO) in the management of asthma. Manag Care. 2018;27(7):42–48.
29. LaForce C, Brooks E, Herje N, Dorinsky P, Rickard K. Impact of exhaled nitric oxide measurements on treatment decisions in an asthma specialty clinic. Ann Allergy Asthma Immunol. 2014;113(6):619–623. doi:10.1016/j.anai.2014.06.013
30. Bukstein D, Luskin AT, Brooks EA. Exhaled nitric oxide as a tool in managing and monitoring difficult-to-treat asthma. Allergy Asthma Proc. 2011;32(3):185–192. doi:10.2500/aap.2011.32.3449
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.