Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Economic Evaluation of Ready-to-Dilute Thiotepa (Tepylute®): Institutional Cost Offsets and Time Savings Compared to Lyophilized Thiotepa in a United States Hospital Pharmacy
Authors Ryan O, Clancy M, MacDonald A, Pastor L, Bourque M
Received 17 September 2025
Accepted for publication 1 December 2025
Published 13 January 2026 Volume 2026:18 559251
DOI https://doi.org/10.2147/CEOR.S559251
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Giorgio Colombo
Orlaith Ryan,1 Maurice Clancy,1 Alanna MacDonald,2 Laura Pastor,2 Megan Bourque2
1Shorla Oncology, Clonmel, Co., Tipperary, Ireland; 2Value and Evidence Department, EVERSANA, Burlington, ON, Canada
Correspondence: Orlaith Ryan, Shorla Oncology, Questum Acceleration Centre Ballingarrane Science and Technology Park, Clonmel, Co., Tipperary, E91 V329, Ireland, Tel +353 87 950 9534, Email [email protected]
Purpose: Thiotepa is an intravenous alkylating agent used with other chemotherapy drugs to treat several forms of cancers. Preparation of thiotepa requires reconstitution of powder in sterile water, followed by dilution of the solution with sodium chloride 0.9% solution for injection. The reconstitution of lyophilized powdered drug formulations may pose challenges as it can increase the risk of preparation errors, leading to wastage or potential clinical consequences, and extend preparation time compared to ready-to-dilute formulations; one study found that 15% of thiotepa doses were made out-of-tolerance. Tepylute® is a ready-to-dilute formulation of thiotepa and has been approved by the United States Food and Drug Administration for the treatment of breast and ovarian adenocarcinoma. The objective of this study was to explore the economic impact to a hospital pharmacy of using ready-to-dilute Tepylute® versus a lyophilized powdered formulation of thiotepa.
Patients and Methods: A cost offset model was created in Microsoft Excel™, the analysis compared a current scenario (thiotepa: 100% market share) with a future scenario (Tepylute®: 100% market share) for a hospital pharmacy treating 96 cancer patients annually. Costs (2024 USD) included drug acquisition, compounding time, drug wastage, and clinical consequences due to reconstitution errors. Incremental costs, cost offsets, and pharmacy time saved were evaluated.
Results: For a hypothetical hospital pharmacy, use of Tepylute® versus a lyophilized powdered formulation of thiotepa resulted in savings of $339,777 over 1-year ($3539 per patient), primarily from reduced drug acquisition costs, as well as a reduction in drug wastage, clinical consequences due to reconstitution errors, and compounding time. Results were consistent across sensitivity and scenario analyses.
Conclusion: Modeled results demonstrate that ready-to-dilute Tepylute® may save time, reduce acquisition and preparation costs, and lower clinical risks from preparation errors. This study is among the first to quantify potential savings from switching to a ready-to-dilute formulation.
Keywords: costs and cost analysis, pharmacy administration, drug costs, thiotepa, cost savings, drug compounding
Introduction
Alkylating agents are widely used in cancer treatment and function by acting on the DNA of tumor cells, leading to cell death.1 Thiotepa is an alkylating drug used in combination with other chemotherapy drugs to treat several forms of cancers and is considered a hazardous drug by the United States (US) Centers for Disease Control and Prevention (CDC).2,3 In the US, thiotepa is currently approved for the treatment of breast or ovarian adenocarcinoma.3 Thiotepa is also approved for use in the US as a preparative regimen for the treatment of allogeneic hematopoietic progenitor (stem) cell transplantation (HSCT) for pediatric patients with class 3 beta-thalassemia, for treatment of superficial papillary carcinoma of the urinary bladder, and for controlling intracavitary effusions secondary to diffuse or localized neoplastic diseases of various serosal cavities.3 Thiotepa is available as a generic formulation and a branded version, Tepadina®, and comes in vial sizes of 15 mg or 100 mg.
Thiotepa is available as a lyophilized powder, and the preparation of thiotepa is a two-step process consisting of reconstitution (manual mixing of thiotepa with sterile water) and dilution (dilution of the hypotonic reconstituted solution in saline prior to patient administration).3 In clinical practice, thiotepa is commonly used in oncology and transplant settings,4–7 where compounding complexity and drug wastage are persistent issues.8,9 These settings demand precise dosing and timely administration, and the manual preparation of thiotepa can introduce risks of error, inefficiency, and occupational exposure.
Terkola et al9 reported a high rate of inappropriate preparation for thiotepa, with 15% of thiotepa formulations being made out-of-tolerance, defined as a dose outside each center’s preset tolerance limits for their gravimetric software systems (ranging from 2.5% to 6%). Previous studies have reported that 0.3–0.4% of oncology and non-oncology drugs have preparation errors due to inappropriate reconstitution.10,11 These findings highlight the vulnerability of manual compounding processes to error, particularly for complex or high-risk medications like thiotepa.
Compounding inefficiencies and errors have broader health and economic implications, including clinical consequences for patients, increased workload for pharmacy staff, drug wastage from preparation errors, and associated costs. For patients, preparation errors can lead to reduced therapeutic efficacy, prolonged hospital stays, and increased monitoring requirements.12 This may translate to additional healthcare costs and burden, such as increased monitoring with clinic visits or prolonged inpatient stays.12 Not all medication errors result in clinical harm, but even minor deviations can disrupt workflow and increase operational costs.13,14 Terkola et al9 also reported that among 759,060 doses of antineoplastic drugs prepared at participating centers between 2011 and 2015, 13.77% of preparations required more than one attempt. Minimizing the rates of preparation errors could have additional benefits of improved efficiency, increased safety and accuracy, and reduced drug wastage. Given that thiotepa is a cytotoxic agent,3 transitioning to a ready-to-dilute formulation may also reduce occupational exposure risks by simplifying handling procedures.15,16 The desirability for de-risking of product preparation through simplification has commonly understood benefits, and are well documented by the National Institute for Occupational Safety and Health (NIOSH) and are in accordance with the guidance from “Preventing Occupational Exposures to Antineoplastic Drugs in Health Care Settings”.2,17
Tepylute®, approved for the treatment of breast and ovarian adenocarcinoma, is an intravenous ready-to-dilute formulation of thiotepa which can be readily diluted in sodium chloride (NaCl).18,19 Ready-to-dilute formulations remove the necessity to reconstitute drugs, simplifying preparation. In the US, Tepylute® 100 mg vials can be used for up to 28 days after opening,19 unlike the lyophilized powder formulation of thiotepa, which is recommended to be used within 24 hours of reconstitution.3 After preparing thiotepa, the remainder of the vial is wasted if not used immediately, whereas Tepylute® 100mg vials can be used for multiple doses.19 Vial sharing results in fewer vials being needed, reducing acquisition costs for an institution. The Hematology/Oncology Pharmacy Association (HOPA) convened a diverse group of stakeholders, who noted that multi-dose vials can minimize or eliminate waste, compared to single-dose vials and should be promoted whenever possible.20
Tepylute® offers a streamlined alternative to traditional thiotepa preparation, addressing several key challenges associated with the lyophilized formulation. As the preparation of Tepylute® is simplified by removing the step of reconstitution, the risk of drug preparation errors may be lowered.21 Fewer errors during preparation can, in turn, lower the risk of clinical consequences for patients and minimize drug wastage, both of which are important considerations in high-risk oncology and transplant settings. Adopting ready-to-dilute Tepylute® would also result in improved efficiencies by reducing compounding time for pharmacists. Currently, pharmacists must prepare thiotepa, which can include manual or robotic compounding. Despite attempts to reduce preparation time with robotic compounding, preparation of thiotepa can still be time-consuming for pharmacists. As ready-to-dilute products do not need to be reconstituted prior to dilution, they have been reported to significantly reduce preparation time compared to the lyophilized powder products.22 By reducing preparation time, adoption of Tepylute® may result in cost offsets, due to decreased demand on pharmacist time, facilitating the reallocation of pharmacist time to other crucial priorities. Importantly, transitioning to a ready-to-dilute formulation may also enhance occupational safety. Thiotepa is a cytotoxic agent,3 and its manual handling during reconstitution poses exposure risks to healthcare workers. Simplifying the preparation process with Tepylute® may reduce the potential for spills, contamination, and exposure incidents. These safety benefits align with guidance from the NIOSH, which advocates for minimizing exposure to antineoplastic drugs through safer handling practices.2,17
Healthcare institutions are continually seeking methods to reduce costs and improve efficiency without compromising the quality of patient care.23 As Tepylute® may reduce time requirements and provide economic benefits, while maintaining quality of care, it would be valuable to examine the potential effects of introducing Tepylute® to an institution. This study adopts a hospital pharmacy economic perspective, focusing on direct costs incurred by hospital pharmacies. The time horizon for the analysis reflects a one-year operational period, aligning with typical budget cycles and procurement planning in hospital settings. The objective of this study was to explore potential cost-offsets resulting from the use of ready-to-dilute Tepylute® versus a lyophilized powdered formulation of thiotepa.
Materials and Methods
Model Framework
A cost-calculator model was developed to estimate the current costs associated with the usage of thiotepa in a theoretical hospital pharmacy and to compare with costs from a future scenario where Tepylute® is integrated into the market from a US hospital pharmacy perspective (Figure 1). The model was constructed in Microsoft Excel™. The base case parameters were sourced from US Food and Drug Administration (FDA) product labels, IQVIA,14 administrative open claims data from Symphony Integrated Dataverse (IDV™),24 the NAVLIN by EVERSANA database on drug costs,25 and published scientific literature. All costs are reported in USD and inflated to 2024 values.
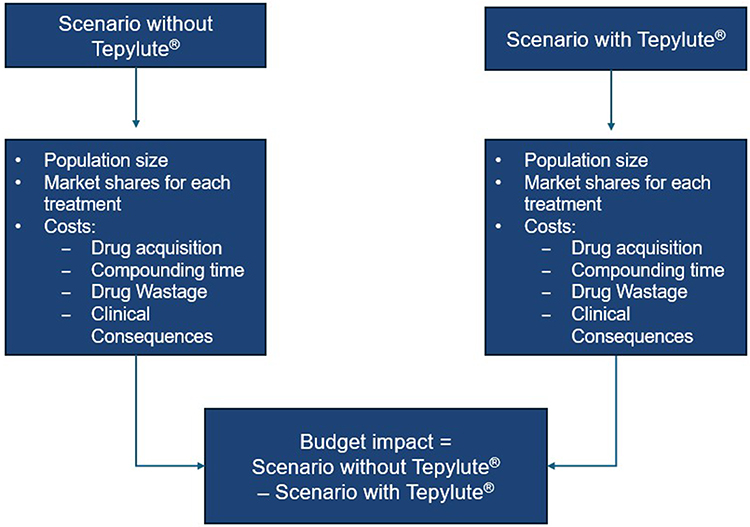 |
Figure 1 Model Structure. |
The model incorporates drug acquisition costs, costs for pharmacist compounding time, drug wastage costs due to remade doses as a result of reconstitution errors, and healthcare costs due to clinical consequences resulting from preparation errors. An overview of model inputs is presented in Table 1. Model outcomes include annual costs for the hypothetical hospital pharmacy and annual costs per patient.
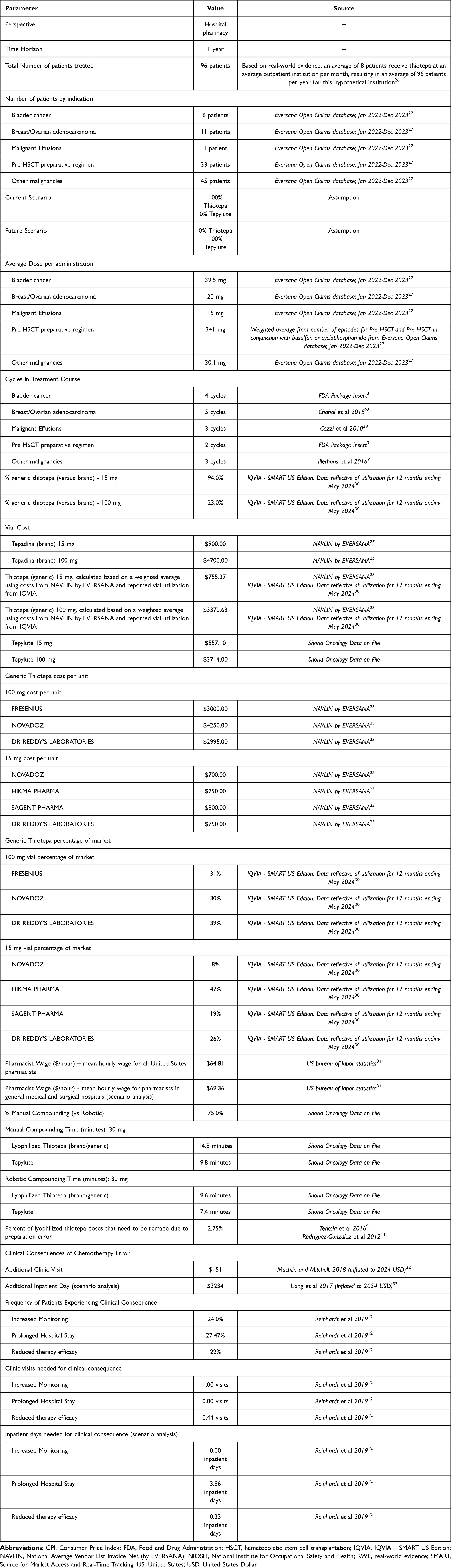 |
Table 1 Model Parameters |
Population
A double-blinded market research survey was conducted in February 2024 among 20 pharmacy directors in the US, across a variety of institution sizes and types, and found that an average of 8 patients receive thiotepa at an average outpatient institution per month, resulting in an average of 96 patients per year per institution.26 The population in this model therefore included 96 patients, and leveraged administrative open claims data from the IDV™ from 2022 to 2023 to inform the distribution of indications for patients receiving thiotepa in the mo categorized as bladder cancer, breast/ovarian adenocarcinoma, a preparative regimen for HSCT, malignant effusion and other cancers.24 The IDV™ contains data from 307 million patients in the US, representing data from pharmacies, prescription claims and medical transactions.24 The population of 96 patients was weighted to the distribution of claims data to determine the estimated number of patients with each indication in the hypothetical hospital pharmacy (Table 1). The number of modeled patients was tested in one-way sensitivity analyses. Another scenario analysis was included to evaluate only on-label indications of thiotepa.
Market Share
The base case analysis assumed the most extreme market share shift: where the current scenario considered a market with 100% utilization of brand or generic thiotepa and the future scenario considered a market with 100% utilization of Tepylute®, to evaluate the largest possible economic impact associated with the introduction of Tepylute®. This assumption has been evaluated in a scenario analysis.
Costs
Acquisition Costs
Wholesale acquisition costs (WAC) were sourced from the NAVLIN by EVERSANA database.25 For Tepadina®, one WAC price is available, but for the generic thiotepa, there are multiple prices on the market. The price of generic thiotepa was calculated as a weighted average price considering the number of units of each generic option sold, and the price for each generic.25,30 The costs by vial size for each generic and brand thiotepa, as well as Tepylute®, are presented in Table 1. The model calculated an average price of thiotepa to account for the respective market utilization of brand and generic thiotepa. IQVIA data reported that branded utilization varies depending on dose size, where 94% of 15 mg vial use is generic, compared to 23% of 100 mg vials.30 Discounts, rebates, and tender prices were not included in the analysis as these data are not publicly available; and the use of wholesale acquisition costs may overestimate actual prices paid for all products in the analysis, including Tepylute®. Scenario analyses were conducted to compare against only generic or only brand options, based on real-world market share mix of these products.
To calculate the acquisition costs for a course of treatment for both lyophilized thiotepa and Tepylute®, the number of vials required by indication was calculated based on the average dose and cycles in a treatment course (assuming the most efficient dosing, with minimum drug wastage). The model leveraged IDV™ data to estimate the average dose for each indication in the model.24 The average dose by indication is presented in Table 1. The FDA Package insert was leveraged to inform the number of administrations per treatment course for bladder cancer and the pre- hematopoietic stem cell transplantation (HSCT) preparative regimen.3 The number of administrations for other indications were sourced from the literature.7,28,29 Dosing assumptions for each indication are summarized in Table 1.
From these assumptions and pricing, the cost per treatment course across all patients, and the cost per treatment course per patient, were calculated for lyophilized thiotepa (brand/generic) and Tepylute® (Table 2).
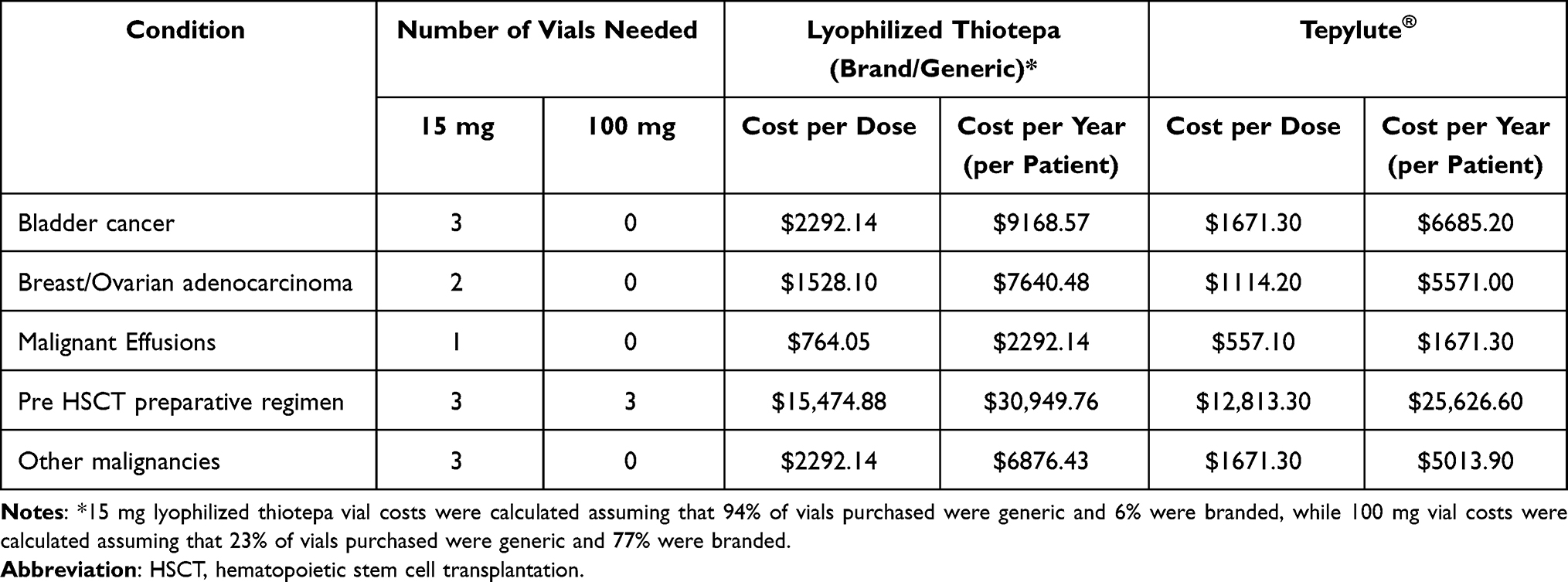 |
Table 2 Calculated Costs for Thiotepa and Tepylute® |
Compounding Time Costs
In a nationwide survey of pharmacists, pharmacy managers, and directors conducted in 2019, 17.1% of participants reported using robotic technologies to compound chemotherapies.34 Internal data has indicated that thiotepa may have higher rates of robotic preparation, where 25% of pharmacists use robotic compounding to prepare thiotepa.26 The thiotepa market research described previously reported that 30 mg of lyophilized thiotepa requires 14.8 minutes to prepare with manual compounding, while Tepylute® requires 9.8 minutes. If robotic compounding is used, 30 mg of thiotepa requires 9.6 minutes to prepare versus 7.4 minutes for Tepylute®.26 Total compounding times were estimated by applying the total manual and robotic compounding time per dose for the respective therapies, assuming 25.0% robotic compounding, and the number of administrations per treatment course for each indication. In the absence of data for other doses, the model assumed compounding time per dose was equivalent to that for 30 mg. Total costs for compounding were calculated by applying a pharmacist wage of $64.81 per hour, based on the US bureau of labor statistics reported average hourly wage for all pharmacists.31 This is a conservative assumption, so as to not to overestimate the cost for compounding time, as it is likely that the wage for a pharmacist qualified to prepare cytotoxic agents is higher than the average hourly wage for all pharmacists. To address this, a scenario analysis was conducted using the hourly wage of $69.36 per hour, based on the wage for a pharmacist working in “General Medical and Surgical Hospitals” (Table 3).31
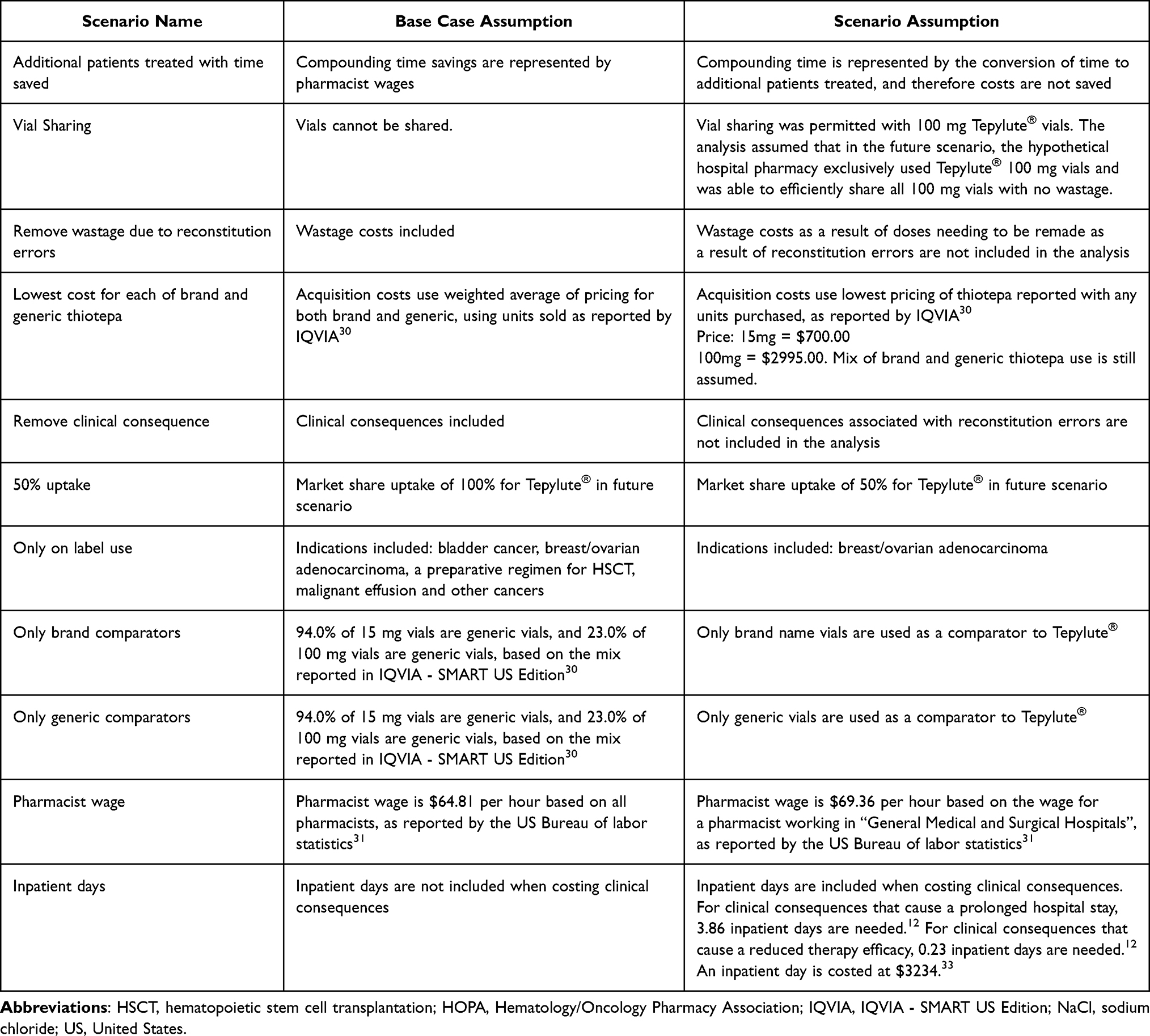 |
Table 3 Scenario Analyses |
Drug Wastage from Preparation Errors
Costs associated with drug wastage due to reconstitution error were estimated in the model. It was assumed that 13.77% of lyophilized thiotepa preparations require an additional attempt to prepare, and doses are remade.9 Rodriguez-Gonzalez et al11 reported that for 40 medication preparation errors, 8 were due to reconstitution and 32 were due to dilution. The proportion of remade lyophilized thiotepa doses due to reconstitution error was estimated to be 2.75%, based on the ratio of reconstitution errors to total preparation errors, and additional drug acquisition costs for these remade doses were considered. It was assumed that there are no costs associated with wastage due to reconstitution errors for Tepylute®, as Tepylute® preparation does not require a reconstitution step. All wastage not related to reconstitution errors, such as wrong dilution volume, wrong dilution solvent, spillage, etc., were assumed to be equivalent between lyophilized thiotepa and Tepylute®. Compounding time for remaking doses after drug wastage errors was not considered in the analysis. A scenario analysis was included which removed drug wastage due to reconstitution errors from the analysis.
Healthcare Costs
Healthcare costs associated with clinical consequences due to reconstitution errors were considered for patients receiving thiotepa. The model assumed that 15.09% of patients receiving thiotepa had a clinical consequence resulting from inaccurate dosing, as per the findings from Terkola et al9 and that 20% of these errors were due to reconstitution as per the findings from Rodriguez-Gonzalez et al.11 Therefore, 3.02% of patients receiving lyophilized thiotepa were assumed in the model to have received an inaccurate thiotepa dose due to a reconstitution-related dosing error, and to have a clinical consequence as a result, based on modeled estimates extrapolated from preparation deviation data.9 The model assumed that patients receiving Tepylute® would not experience any clinical consequences from inaccurate dosing due to reconstitution as this step is not necessary for Tepylute® preparation.
Reinhardt et al12 noted that 24% of patients experiencing a clinical consequence due to an error would require increased monitoring and 22% would have reduced therapy efficacy, and further reported that increased monitoring was associated with an additional clinic visit per error and reduced therapy efficacy was associated with an average of 0.44 clinic visits per error. The cost of additional clinic visits was sourced from Machlin and Mitchell32 and inflated to 2024 USD, at $151 per additional clinic visit. The model took a conservative approach in determining which clinical consequences to include, and did not consider the cost of inpatient days associated with prolonged hospital stays and reduced therapy efficacy.12 Two scenario analyses were included to test these assumptions, one which removed the impact of clinical consequences due to reconstitution errors, and one which also considered inpatient days associated with the clinical consequences.
Sensitivity Analyses
To characterize uncertainty in the analysis, various one-way sensitivity analyses were conducted by varying key parameters by ±20% to investigate their impact. Key parameters included: total population size, number of patients treated for each indication, dose for treatment of each indication, percentage of generic thiotepa use, manual versus robotic compounding time, percentage of thiotepa doses resulting in remade doses, and number of clinical consequences associated with reconstitution errors.
Scenario Analyses
A number of scenario analyses were conducted to test the assumptions in the model, as described in Table 3. The first scenario analysis was a time-saved analysis that considered pharmacist time saved due to reduced compounding time with Tepylute® and estimated the number of additional patients that pharmacists could prepare medication for with the time saved. While this may not translate into full operationalization of time savings in practice, it is realistic that there would be improved efficiency, and additional opportunity costs should be considered. The next scenario evaluated the impact of vial-sharing, assessing potential cost savings when vials are permitted to be shared across patients. As previously noted, reconstituted thiotepa must be used within 24 hours, and any unused portion is discarded if not immediately administered. In contrast, Tepylute® 100 mg vials remain usable for up to 28 days after opening, allowing for multiple doses to be drawn from a single vial when clinically appropriate. This extended usability enables vial sharing, which can reduce the total number of vials required, and lowers acquisition costs for institutions. The scenario assumes exclusive use of 100 mg Tepylute® vials with no wastage, as once opened, the vial could be used for multiple patients and doses. Other scenarios included removing wastage costs due to the need to remake doses due to reconstitution errors in the model, using the lowest reported thiotepa acquisition costs for brand and generic comparators, exclusion of clinical consequences due to reconstitution errors, reduced market uptake of Tepylute® (to 50%), restriction of the analysis to on-label indications only, exclusive use of either brand or generic thiotepa vials in the current scenario, variation in pharmacist wage assumptions, and inclusion of inpatient days when costing clinical consequences due to reconstitution errors.
Results
Base Case Scenario
In a hypothetical hospital pharmacy consisting of 96 treated patients, the analysis predicted there would be 6 bladder cancer patients, 11 breast/ovarian adenocarcinoma patients, 33 pre-HSCT patients, 1 malignant effusion patient, and 45 patients with various other cancers treated with thiotepa over the course of 1-year. The use of Tepylute® versus a lyophilized powdered formulation of thiotepa in this analysis resulted in net savings of $339,777 over 1-year for a US hospital pharmacy, or $3539 per patient (Table 4). Acquisition costs were projected to decrease by $297,547 in the future scenario. Additional potential cost offsets of $42,229 were predicted due to reduced drug wastage and clinical consequences from reduced drug reconstitution errors, and reduced compounding time for pharmacists.
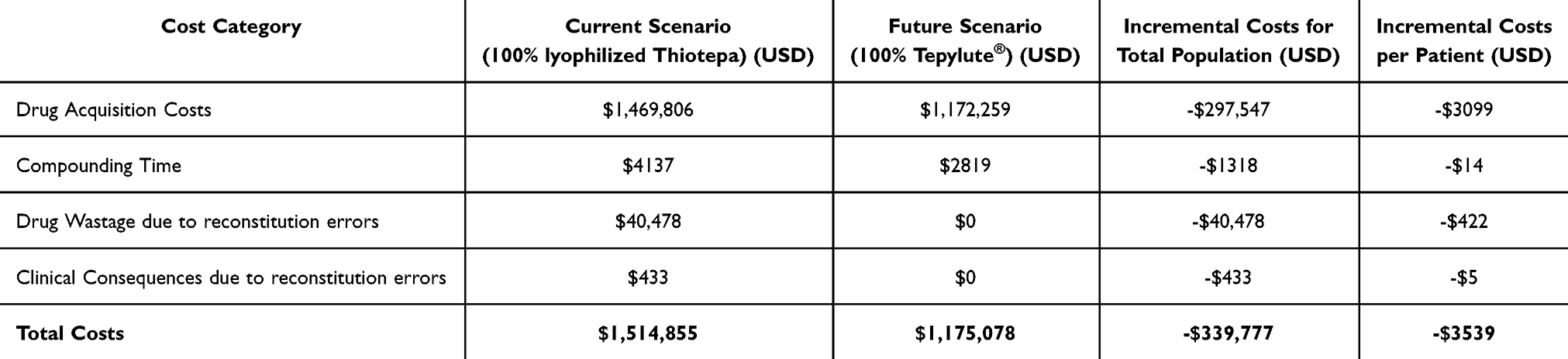 |
Table 4 Base Case Analysis: Total Annual Costs for the Hypothetical Hospital Pharmacy |
Sensitivity Analyses
One-way sensitivity analyses demonstrated which key parameters in the model drove the results (Figure 2). One-way sensitivity analyses confirmed the robustness of the model, with all scenarios demonstrating cost savings associated with the adoption of ready-to-dilute Tepylute®. The most influential parameter was the total population size, with cost savings ranging from $271,821 to $407,732 for the cohort (or $2831 to $4247 per patient) compared with the current scenario. The number of pre-HSCT patients was the second most influential parameter tested, with cost savings ranging from $299,104 to $380,449. Other variables, including the rate of dose re-preparation due to compounding errors and manual compounding time, had smaller effects but still resulted in cost savings. Across all ranges tested, scenarios evaluating the impact of adopting Tepylute® consistently resulted in cost savings compared with the current scenario, with savings exceeding $271,000 annually.
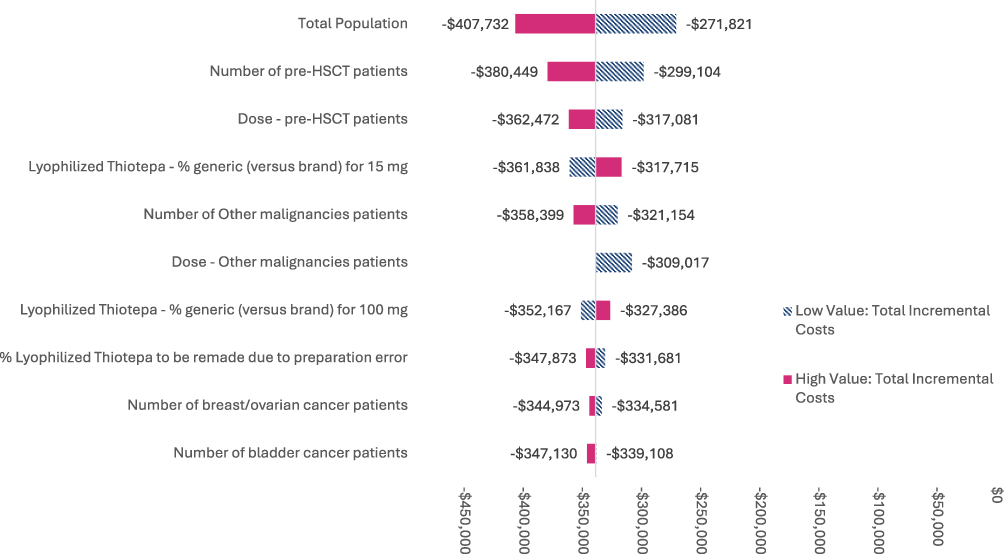 |
Figure 2 One-way sensitivity analysis tornado diagram. |
Scenario Analyses
A time-saved analysis found notable time savings when switching from lyophilized thiotepa to Tepylute® (Table 5). An average of 12.7 minutes of pharmacist time was saved per treatment cycle, resulting in a total of 1219.8 saved minutes across 96 patients, representing a 32% decrease in compounding time. Applying the total time saved for the hypothetical hospital pharmacy due to using Tepylute® (1219.8 minutes) and the total compounding time per Tepylute® administration (27.2 minutes), medication for an additional 44 patients could be prepared in a year at a given hypothetical hospital pharmacy. This estimate assumes that all saved compounding time is fully reallocated to patient care, which may overstate real-world productivity gains, particularly given the mix of manual and robotic preparation methods.
 |
Table 5 Results from the Time Saved Analysis |
A second scenario analysis considered the economic impact if vial sharing was permitted for 100 mg Tepylute® vials, where all doses for all indications were prepared with 100 mg vials only. In the future scenario, vial sharing of 100 mg Tepylute® vials resulted in additional cost savings where acquisition costs decreased by an additional $106,341 compared with the base case analysis, totaling cost savings of $446,118 for the hypothetical hospital pharmacy.
Additional scenario analyses were conducted to test the robustness of the model assumptions. These included removing wastage costs due to reconstitution errors, using the lowest reported thiotepa prices for generic and branded comparators, excluding clinical consequences associated with reconstitution errors, assuming 50% market uptake of Tepylute®, restricting to on-label indications only, using only brand or only generic comparator vials, adjusting pharmacist wage assumptions, and including inpatient days in the cost of clinical consequences due to reconstitution errors. Results varied across scenarios, with total cost savings ranging from $125,331 to $512,036 for the population, or $1306 to $5334 per patient (Table 6).
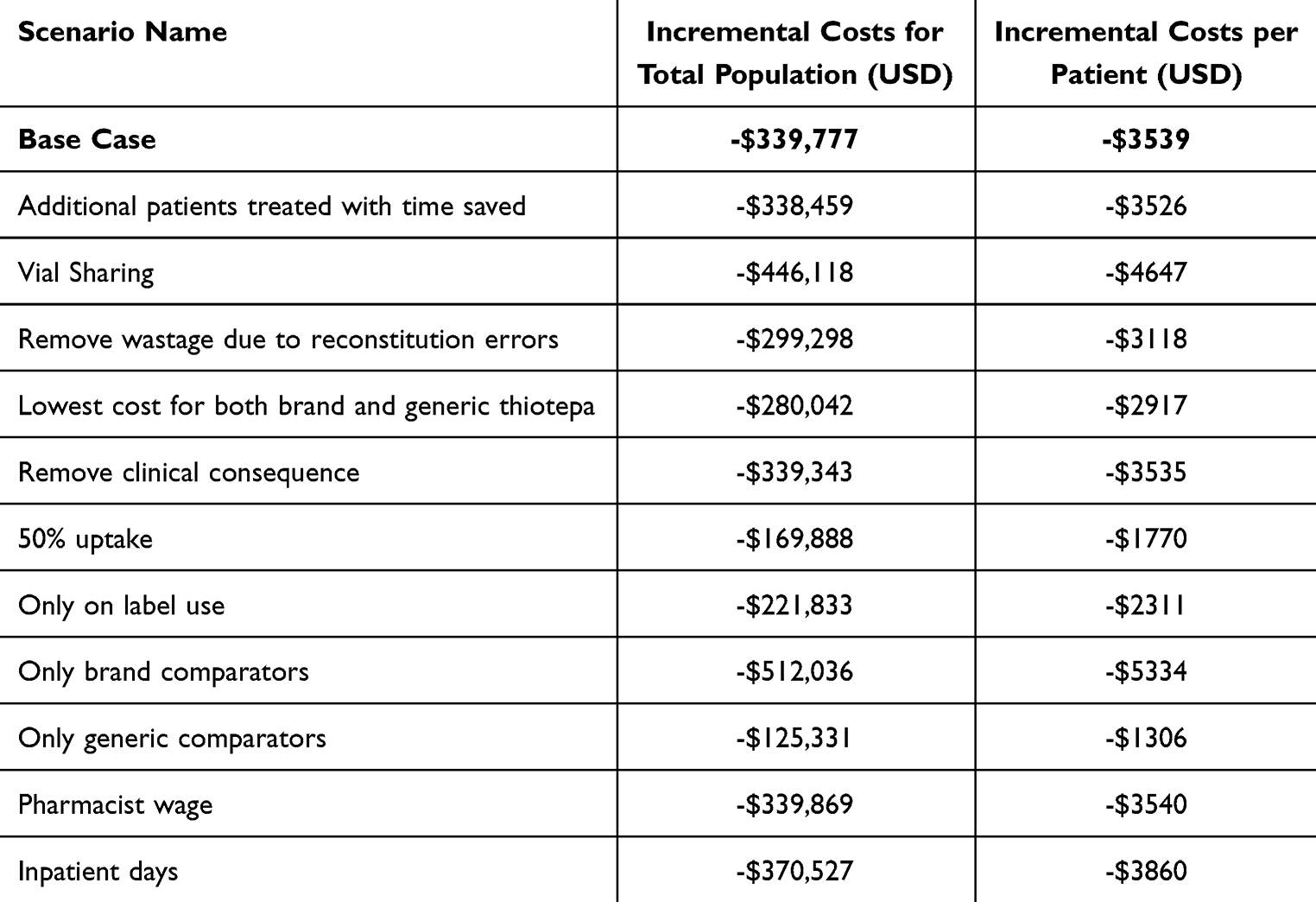 |
Table 6 Scenario Analyses Results |
Discussion
This cost offset model compared the current costs associated with treating patients with thiotepa at a hypothetical hospital pharmacy with a future scenario after adopting Tepylute®. The model results suggest that using Tepylute® instead of lyophilized thiotepa can result in potential cost savings for a US hospital pharmacy. The model predicted cost savings as compared with the current scenario, resulting from reduced acquisition costs, saved compounding time, reduced drug wastage, and lower frequency of clinical consequences. There were several parameters that had a significant impact on this result, including the proportion of pre-HSCT patients and the dose of thiotepa by indication.
Key factors of the analysis were the percent of branded versus generic thiotepa and the cost of generic thiotepa, which was determined by a weighted average cost of the available formulations using current utilization based on claims. While Tepadina® is the more costly formulation, 15 mg vials of generic thiotepa cost more than 15 mg vials of Tepylute® (a pattern not observed with 100 mg vials). Due to the competitive pricing of Tepylute® and the market purchase patterns of generic versus branded thiotepa, the model estimates that a future scenario with 100% Tepylute® use would result in lower total acquisition costs compared to a scenario with 100% lyophilized thiotepa. While all cost categories indicated that Tepylute® would result in cost savings compared with the current scenario, acquisition costs contributed the largest share of savings. This finding was consistent across scenario analyses that considered uncertainty around pricing and proportion of brand usage, still showing savings of more than $125,331 compared with the current scenario.
There are also additional sources of value associated with ready-to-dilute thiotepa that this model did not consider but would bring advantages for an institution, such as opportunity costs associated with pharmacists preparing medications for additional patients. Another potential source of value would be the reduction of time spent by employees handling thiotepa, as it is designated as a hazardous drug.2,3 As a hazardous drug, special handling, disposal procedures and personal protective equipment (PPE) is required for employees involved in thiotepa’s administration. Using the ready-to-dilute formulation circumvents the need to handle thiotepa in the powder format, increasing worker safety and reducing their exposure to a cytotoxic and carcinogenic drug.3,15 This could result in further cost offsets, potentially reducing worker injury and saving costs on PPE.
There is a paucity of data on ready-to-dilute products to inform specific inputs in the model. One previous study on vaccine preparation time with fully-liquid hexavalent vaccine versus non-fully liquid hexavalent vaccine requiring reconstitution found that removing the step of reconstitution is associated with a reduction of errors in drug preparations.21 Another study compared economic outcomes of two ready-to-dilute solutions, one with a short-duration infusion, and found that increasing adoption of short-duration infusion was associated with lower acquisition costs and reduced administration costs.35 There was a lack of literature on the likelihood of preparation errors with a ready-to-dilute formula. In oncology, only one article has been published on the budget impact on a ready-to-dilute formula, where bendamustine RTD use was considered at US infusion facilities, which estimated a $1808 per patient cost saving per year, assuming utilization shift from 50% to 100%, which was driven by lower acquisition costs and lower labor costs.35 This result was in line with the magnitude of the cost saving found in this current study – when looking at a 50% utilization shift scenario, this study estimates $169,888 in cost-savings, or $1770 in cost savings per patient for the 96 patient cohort. Other products, such as ready-to-administer medications like prefilled syringes, have investigated the potential benefits associated with drug formulations that are easier and faster to use. Previous work has also reported reductions in preparation errors associated with simplifying medication preparation, including removing reconstitution.21,36–39 Due to a lack of data on switching to ready-to-dilute formulations, our study has made the assumption that switching to ready-to-dilute formulations decreases drug preparation errors and would be associated with a reduction in drug wastage and clinical consequences. Economic evaluations on other products that simplify drug preparation have also found reductions in medication errors and adverse drug events can result in cost offsets, due to a reduction in hospital admissions and length of stay.38
In addition to the paucity of data in this area, there are potential limitations to this study. A potential limitation is the chosen indications for the hypothetical hospital pharmacy. Tepylute® is currently approved for breast and ovarian adenocarcinoma, but the model included off-label indications to reflect the real-world usage of thiotepa.3,19,27,30 This limitation was addressed by conducting a scenario analysis, only considering breast and ovarian adenocarcinoma. Another limitation was that the analysis relied on wholesale acquisition costs, as discounts, rebates, and tender prices are not publicly available; this may overestimate actual prices paid for all modeled products in practice, or reflect outdated costs, and is acknowledged as a limitation. Another limitation was that the model excludes potential costs associated with capital investments or infrastructure changes required for ready-to-dilute product adoption, such as cold storage or equipment upgrades. However, Tepylute® is stored between 36°F to 46°F, so specialized equipment is not required.
A strength in this model was the use of conservative assumptions to avoid overestimating the cost offsets of Tepylute®. The model assumed the most efficient use of vials by the hypothetical hospital pharmacy, which is likely unrealistic, as pharmacists may not always optimize vial usage to decrease wastage or have optimal vial sizes available. If the model reflected more realistic wastage patterns, the results would likely have shown higher cost savings associated with the future scenario, after adoption of Tepylute®, due to its overall lower acquisition costs. Vial sharing for Tepylute® was excluded in the base case analysis as another conservative assumption, which would have also resulted in more cost offsets when adopting Tepylute®. The model also assumed that all doses had the same compounding time as a 30 mg dose (two 15 mg vials), which would have underestimated the reduced incremental compounding time between Tepylute® and lyophilized thiotepa, as the majority of patients are modeled to require more than two vials per dose. The analysis also excluded the cost of inpatient days when considering healthcare costs due to preparation errors, which would have increased the healthcare costs of thiotepa. By applying conservative assumptions in the model, the results likely underestimate the cost offsets associated with adopting Tepylute®.
Beyond the use of conservative assumptions, this model had several other notable strengths. This study used real-world data to inform inputs on dosage, proportion of patients by indication and the market shares of thiotepa and Tepadina®. By using real-world data, the study could more accurately predict the results of adopting Tepylute® into a hypothetical hospital pharmacy. Another strength is despite a scarcity of data on the potential benefits of ready-to-dilute formulations, this study is one of the first to attempt to quantify the potential cost savings associated with switching to a new formulation.
The findings of this study highlight the potential of Tepylute®, potentially providing significant economic benefits to a hypothetical hospital pharmacy, while providing equivalent efficacy to thiotepa. As Tepylute® is a ready-to-dilute formulation of thiotepa, institutions can reduce time needed for compounding by pharmacists, saving time and improving efficiency, without compromising the care of patients. By eliminating the need for reconstitution, Tepylute® may provide more consistent and accurate dosing than thiotepa, potentially reducing preparation errors and clinical consequences. Further, the acquisition costs of drugs would be predicted to decrease due to the pricing of Tepylute® compared to thiotepa and Tepadina®. Overall, incorporating Tepylute® could save an institution time and money, and reduce preparation errors, while still as effective as alternatives.
Conclusion
Thiotepa is an intravenous alkylating agent that requires reconstitution and dilution to prepare and is used in combination with other chemotherapy drugs to treat several forms of cancers. The process of reconstitution can be time-consuming and may increase the chance of preparation errors. The model suggests that Tepylute® may offer cost savings driven by acquisition costs, particularly for the 15 mg vial, as well as potential reductions in pharmacy compounding time and reconstitution-related errors. These findings are based on modeled assumptions and extrapolated data and should be interpreted as hypothetical estimates rather than observed outcomes. In the base case analysis, the use of Tepylute® versus a lyophilized powdered formulation of thiotepa was modeled to result in cost savings of $339,777 over 1-year for a US hospital pharmacy, or $3539 per patient. One-way sensitivity analyses found that these results ranged from $271,821 to $407,732 in cost savings for the population ($2831 to $4247 per patient), and scenario analyses demonstrated that testing uncertainty in model inputs varied model results from $125,331 to $512,036 for the population ($1306 to $5334 per patient). While the model consistently predicted cost savings across analyses, the results are sensitive to pricing and utilization inputs. In a future study, it would be valuable to compare cost-savings against real-world outcomes for validation. Ready-to-dilute formulations like Tepylute® may offer practical advantages in oncology care, particularly in larger institutions or settings with high compounding demands. Future studies could explore the broader applicability of these findings to other ready-to-dilute oncology products and assess their impact on workflow efficiency, safety, and cost-effectiveness in clinical practice. Introducing Tepylute® to a US hospital pharmacy is predicted to reduce costs and increase efficiency for pharmacists while maintaining quality of care for patients.
Acknowledgments
We thank Parash Bhandari for his helpful input on this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, including the conception, study design, execution, acquisition of data, analysis, and interpretation, and in drafting, revising, critically reviewing, and approving the final version to be published.
Funding
This work was funded by Shorla Oncology.
Disclosure
At the time this work was conducted, OR and MC were paid employees and shareholders of Shorla Oncology. AM, LP, and MB are employees of Eversana and members of the Value and Evidence team and hired by Shorla Oncology to provide health economic consulting services for this project, and were contracted to build the model, run the analyses, and write the manuscript. OR has a patent US-11975013-B2 issued to Shorla Oncology, a patent US-20230041156-A1 pending to Shorla Oncology, a patent US-20230017521-A1 pending to Shorla Oncology. The authors report no other conflicts of interest in this work.
References
1. National Institute of Diabetes and Digestive and Kidney Diseases. LiverTox: clinical and research information on drug-induced liver injury: alkylating agents. Bethesda (MD). Available from: https://www.ncbi.nlm.nih.gov/books/NBK547849/.
2. US Centers for Disease Control and Prevention. NIOSH list of hazardous drugs in healthcare setting, 2024. 2024. Available from: https://www.cdc.gov/niosh/docs/2025-103/pdfs/2025-103.pdf?id=10.26616/NIOSHPUB2025103.
3. ADIENNE pharma and biotech. In: thiotepa, editor. Zurigo, Switzerland. 2017.
4. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. THIOTEPA. Pharmaceuticals. Lyon (FR): International Agency for Research on Cancer; 2012. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 100A).
5. Chen YB, Batchelor T, Li S, et al. Phase 2 trial of high‐dose rituximab with high‐dose cytarabine mobilization therapy and high‐dose thiotepa, busulfan, and cyclophosphamide autologous stem cell transplantation in patients with central nervous system involvement by non‐Hodgkin lymphoma. Cancer. 2015;121(2):226–16. doi:10.1002/cncr.29023
6. Ferreri AJ, Illerhaus G. The role of autologous stem cell transplantation in primary central nervous system lymphoma. Blood J Am Soc Hematol. 2016;127(13):1642–1649.
7. Illerhaus G, Kasenda B, Ihorst G, et al. High-dose chemotherapy with autologous haemopoietic stem cell transplantation for newly diagnosed primary CNS lymphoma: a prospective, single-arm, phase 2 trial. Lancet Haematol. 2016;3(8):e388–e397. doi:10.1016/S2352-3026(16)30050-3
8. Hess LM, Cui ZL, Li XI, Oton AB, Shortenhaus S, Watson IA. Drug wastage and costs to the healthcare system in the care of patients with non-small cell lung cancer in the United States. J Med Econ. 2018;21(8):755–761. doi:10.1080/13696998.2018.1467918
9. Terkola R, Czejka M, Bérubé J. Evaluation of real‐time data obtained from gravimetric preparation of antineoplastic agents shows medication errors with possible critical therapeutic impact: results of a large‐scale, multicentre, multinational, retrospective study. J Clin Pharm Therapeutics. 2017;42(4):446–453. doi:10.1111/jcpt.12529
10. Chaudhari A, Mule A, Dhande P. Medication errors in an oncology inpatient setting in India—Audit by clinical pharmacists. J Oncol Pharm Pract. 2023;29(7):1667–1672. doi:10.1177/10781552221146529
11. Rodriguez-Gonzalez CG, Herranz-Alonso A, Martin-Barbero ML, et al. Prevalence of medication administration errors in two medical units with automated prescription and dispensing. J Am Med Inf Assoc. 2012;19(1):72–78. doi:10.1136/amiajnl-2011-000332
12. Reinhardt H, Otte P, Eggleton AG, et al. Avoiding chemotherapy prescribing errors: analysis and innovative strategies. Cancer. 2019;125(9):1547–1557. doi:10.1002/cncr.31950
13. Castro R, Aguiar LB, Volpe CRG, et al. Determining medication errors in an adult intensive care unit. Int J Environ Res Public Health. 2023;20(18):6788. doi:10.3390/ijerph20186788
14. Gallina M, Testagrossa M, Provenzani A. Unit dose drug dispensing systems in hospitals: a systematic review of medication error reduction and cost-effectiveness. Eur J Hosp Pharm. 2025;ejhpharm–2024–004444. doi:10.1136/ejhpharm-2024-004444
15. National Toxicology Program. Thiotepa 15th report on carcinogens. No. 52-24-4. ed. Research triangle park (NC). 2021.
16. Gonçalves A, de Oliveira RA, Fernandes PO. The occupational risks and health effects resulting from exposition to cytotoxic drugs preparation. Procedia Comput Sci. 2023;219:1420–1429. doi:10.1016/j.procs.2023.01.431
17. Connor TH, McDiarmid MA. Preventing occupational exposures to antineoplastic drugs in health care settings. Ca a Cancer J Clinicians. 2006;56(6):354–365. doi:10.3322/canjclin.56.6.354
18. Shorla Oncology. SH-105 A treatment for breast & ovarian cancer. Available from: https://shorlaoncology.com/pipeline/sh-105/.
19. Shorla Oncology. In: TEPYLUTE (thiotepa), editor. Cambridge, MA. 2025.
20. HOPA. Intravenous cancer drug waste issue brief. 2022. Available from: https://www.hoparx.org/documents/65/HOPA_Drug_Waste_Issue_Brief_-_Updated_01.19.22_FINAL.pdf.
21. De Coster I, Fournie X, Faure C, et al. Assessment of preparation time with fully-liquid versus non-fully liquid paediatric hexavalent vaccines. A time and motion study. Vaccine. 2015;33(32):3976–3982. doi:10.1016/j.vaccine.2015.06.030
22. Business Wire. Eagle pharmaceuticals announces TREAKISYM (bendamustine) ready-to-dilute (“RTD”) formulation, in combination with rituximab for treatment of relapsed or refractory diffuse large B-cell lymphoma receives PMDA approval in Japan. 2021. Available from: https://www.businesswire.com/news/home/20210430005136/en.
23. Medicine E, National Academies of Sciences. Medications in Single-Dose Vials: Implications of Discarded Drugs. 2021.
24. Symphony Integrated Dataverse. Administrative open claims data from symphony integrated dataverse, Jan 2022-Dec 2023 Accessed October 2023.
25. NAVLIN by EVERSANA. NAVLIN price & access data tool. Available from: https://www.eversana.com/ko/products/pricentric-one/.
26. EVERSANA Custom Insights. Final report: opportunities and barriers for SH105. 2024.
27. Eversana open claims database. Jan 2022-Dec 2023 Accessed October, 2023.
28. Chahal J, Stopeck A, Clarke K, Livingston RB, Chalasani P. Intravenous thiotepa for treatment of breast cancer-related leptomeningeal carcinomatosis: case series. Neurol Sci. 2015;36(9):1691–1693. doi:10.1007/s10072-015-2259-1
29. Cozzi S, Montanara S, Luraschi A, et al. Management of neoplastic pericardial effusions. Tumori J. 2010;96(6):926–929. doi:10.1177/548.6510
30. IQVIA - SMART US Edition. Data reflective of utilization for 12 months ending May 2024. Accessed June 2024.
31. Occupational employment and wages, May 2023 (2023).
32. Machlin SR, Mitchell EM. Expenses for office-based physician visits by specialty and insurance type, 2016. 2018.
33. Liang L, Moore B, Soni A. National inpatient hospital costs: the most expensive conditions by payer, 2017. 2020.
34. Boyd A, Sue C, Khandoobhai A, et al. Evaluation of oncology infusion pharmacy practices: a nationwide survey. J Oncol Pharm Pract. 2024;30(1):127–141. doi:10.1177/10781552231170358
35. James E, Trautman H, Thompson S, Ribalov R, Choudhry A. Budgetary impact of bendamustine ready-to-dilute products in chronic lymphocytic leukemia and non-hodgkin lymphoma to a United States infusion facility. Clinicoecon Outcomes Res. 2021;Volume 13:201–211. doi:10.2147/CEOR.S297284
36. Arora P, Muehrcke M, Hertig J. A cost-effectiveness study comparing ready-to-administer and traditional vial-and-syringe method for opioids. Pain Ther. 2022;11(3):937–950. doi:10.1007/s40122-022-00402-z
37. Larmené-Beld K, Frijlink HW, Taxis K. Ready to administer parenteral medication produced by the hospital pharmacy. Eur J Clin Pharmacol. 2019;75(5):609–617. doi:10.1007/s00228-019-02631-2
38. Benhamou D, Weiss M, Borms M, et al. Assessing the clinical, economic, and health resource utilization impacts of prefilled syringes versus conventional medication administration methods: results from a systematic literature review. Ann Pharmacother. 2023:10600280231212890.
39. Tu H-N, Shan T-H, Wu Y-C, et al. Reducing medication errors by adopting automatic dispensing cabinets in critical care units. J Med Systems. 2023;47(1):52. doi:10.1007/s10916-023-01953-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.