Back to Journals » ClinicoEconomics and Outcomes Research » Volume 8
Economic analysis of empiric versus diagnostic-driven strategies for immunocompromised patients with suspected fungal infections in the People's Republic of China
Authors Mao N, Lesher B, Liu Q, Qin L, Chen Y, Gao X ![]() , Earnshaw S, McDade C, Charbonneau C
, Earnshaw S, McDade C, Charbonneau C
Received 21 November 2015
Accepted for publication 9 February 2016
Published 14 June 2016 Volume 2016:8 Pages 275—285
DOI https://doi.org/10.2147/CEOR.S101015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Ningying Mao,1 Beth Lesher,2 Qifa Liu,3 Lei Qin,2 Yixi Chen,4 Xin Gao,2 Stephanie R Earnshaw,5 Cheryl L McDade,5 Claudie Charbonneau,6
1School of International Pharmaceutical Business, China Pharmaceutical University, Nanjing, People's Republic of China; 2Pharmerit International, Bethesda, MD, USA; 3Hematology Department, Nanfang Hospital, Southern Medical University, Guangzhou, 4Pfizer Investment Co. Ltd., Beijing, People's Republic of China; 5RTI Health Solutions, Research Triangle Park, NC, USA; 6Pfizer International Operations, Paris, France
Abstract: Invasive fungal infections (IFIs) require rapid diagnosis and treatment. A decision-analytic model was used to estimate total costs and survival associated with a diagnostic-driven (DD) or an empiric treatment approach in neutropenic patients with hematological malignancies receiving chemotherapy or autologous/allogeneic stem cell transplants in Shanghai, Beijing, Chengdu, and Guangzhou, the People's Republic of China. Treatment initiation for the empiric approach occurred after clinical suspicion of an IFI; treatment initiation for the DD approach occurred after clinical suspicion and a positive IFI diagnostic test result. Model inputs were obtained from the literature; treatment patterns and resource use were based on clinical opinion. Total costs were lower for the DD versus the empiric approach in Shanghai (¥3,232 vs ¥4,331), Beijing (¥3,894 vs ¥4,864), Chengdu, (¥4,632 vs ¥5,795), and Guangzhou (¥8,489 vs ¥9,795). Antifungal administration was lower using the DD (5.7%) than empiric (9.8%) approach, with similar survival rates. Results from one-way and probabilistic sensitivity analyses were most sensitive to changes in diagnostic test sensitivity and IFI incidence; the DD approach dominated the empiric approach in 88% of scenarios. These results suggest that a DD compared to an empiric treatment approach in the People’s Republic of China may be cost saving, with similar overall survival in immunocompromised patients with suspected IFIs.
Keywords: aspergillosis, cost-effectiveness analysis, voriconazole, caspofungin, itraconazole
Introduction
Invasive fungal infections (IFIs) are deadly infections requiring rapid diagnosis and treatment. In the People’s Republic of China, the IFI incidence ranges from 4% to 41% depending on patient population and underlying conditions.1 Candida spp. are the predominant organisms identified in patients with IFIs in the People’s Republic of China; however, the incidence of Aspergillus infections is increasing.1 Patients at risk for IFIs include transplant recipients and those with hematological malignancies or human immunodeficiency virus.2
Empiric antifungal therapy is often initiated in patients with persistent and/or recurrent fevers unresponsive to broad-spectrum antibacterial therapy for 72 hours. Early use of companion diagnostics, or a diagnostic-driven (DD) approach, can potentially identify IFIs prior to antifungal treatment initiation. Patients treated using a DD treatment approach are initiated on antifungal therapy based not only on clinical suspicion but also on a positive diagnostic evaluation. A benefit of a DD treatment approach is lower costs due to reduction of unnecessary antifungal treatment. Results from several studies suggest that a DD or preemptive approach compared to an empiric approach may be beneficial in patients with suspected IFIs.3–7
Given the high mortality reported for IFIs, specifically invasive aspergillosis, and the increasing incidence of aspergillosis in the People’s Republic of China, we adapted a pharmacoeconomic model to assess the impact of a DD compared to an empiric approach on costs and outcomes in neutropenic patients with suspected IFIs in the following four geographically representative Chinese cities: Beijing, Chengdu, Guangzhou, and Shanghai.
Methods
A previously published decision-analytic model8 was adapted to reflect costs and resource utilization in Beijing, Chengdu, Guangzhou, and Shanghai, the People’s Republic of China. A DD or an empiric approach was used to treat patients with persistent or recurrent febrile neutropenia. Patients treated using a DD approach following clinical suspicion of an IFI underwent galactomannan (GM) testing and/or a computed tomography (CT) scan to direct initiation of antifungal therapy. Patients treated using an empiric approach were initiated on antifungal therapy based on clinical suspicion alone. Antifungal treatment was assumed initiated at the same time regardless of approach.8
Model structure
The previously published decision model (UK perspective) that we adapted was designed as a simple decision tree over a time horizon of 5 months.8 In this adapted model, a hypothetical cohort of 1,000 neutropenic patients at risk of IFIs entered the decision tree and were treated using either a DD or an empiric approach (Figure 1). Patients treated using a DD approach received antifungal therapy following both clinical suspicion and a positive diagnostic test result suggestive of an IFI. Patients treated using an empiric approach received antifungal therapy following clinical suspicion of an IFI alone. Patients treated using an empiric approach could ultimately have a proven, probable, or no fungal infection. Following initiation of antifungal therapy regardless of approach, patients survived or died based on epidemiological and clinical data obtained from published literature.9 Antifungal therapies evaluated in both the DD and empiric branches included caspofungin, itraconazole, and voriconazole; therapies evaluated were recommended by the Chinese clinical experts interviewed for this study.
 | Figure 1 Model structure. (A) Diagnostic-driven treatment approach. (B) Empiric treatment approach. |
Patient population
The hypothetical study population for this model adaptation included patients older than 18 years with a hematological malignancy scheduled for chemotherapy or autologous/allogeneic stem cell transplantation with an expected neutrophil count <500 cells/mm3 for at least 10 days.3–7 We assumed that all patients entering the model were not previously diagnosed with a proven or probable IFI or treated with an antifungal therapy within the last 6 months.
Clinical variables
Overall mortality, IFI incidence, IFI identification by the empiric approach, and IFI-related mortality data were incorporated from the global model.8 Survival rates were generated based on the proportion of patients with identified and appropriately treated IFIs. Treatment patterns and therapy duration for both approaches were based on the opinion of three to five renowned clinicians practicing at top hospitals in each Chinese city.
The primary clinical measure required to estimate the costs and outcomes associated with each treatment approach was IFI incidence within a particular clinical setting. An IFI incidence of 10.9% (95% confidence interval [CI]: 9%–13%) was assumed based on a patient population treated with myelosuppressive chemotherapy for hematological malignancies or following autologous stem cell transplant in a German tertiary care center9 and confirmed by our Chinese clinical experts.
Predicted survival following a DD or an empiric approach was the primary clinical outcome of interest. Mortality inputs were obtained from epidemiological and clinical studies due to a lack of data from head-to-head comparative antifungal treatment studies.9,10 Specifically, overall mortality during the years 2002–2006 was reported as 10.7% (95% CI: 9%–13%) and IFI-related mortality as 28.6% (95% CI: 19%–39%) in a population of patients treated with myelosuppressive chemotherapy for hematological malignancies or following autologous stem cell transplantation.9 A 28.6% increase in mortality was assumed for patients with IFIs since IFI deaths would only occur in patients with IFIs. Given this assumption, the overall mortality was adjusted to be specific to patients with and without IFIs (Table 1).
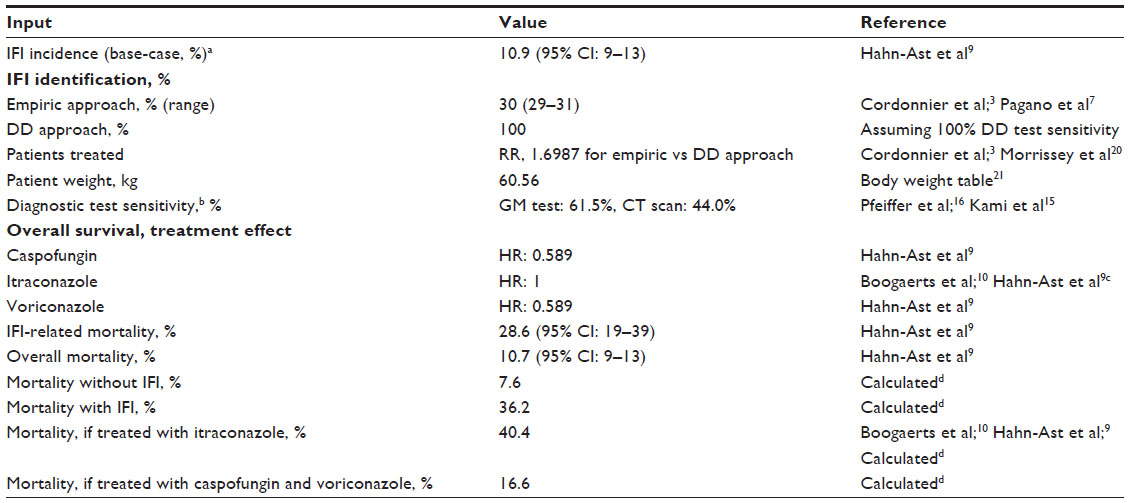 | Table 1 Clinical variables and data source of model inputs |
Additionally, the model examined the treatment effect of itraconazole, caspofungin, or voriconazole administration on overall survival. Results from a multivariable analysis in patients with IFIs showed a significant improvement in overall survival with voriconazole and caspofungin compared to amphotericin (hazard ratio: 0.589; 95% CI: 0.362–0.959; P=0.033).9 Results from a separate analysis showed similar mortality rates for itraconazole and amphotericin.10 Therefore, specific morality values for itraconazole, caspofungin, and voriconazole were calculated using amphotericin-based agents as a reference comparator (Table 1).
Costs and health care resource use
Health care resource unit costs in 2014 Chinese Yuan (¥; July 2014: 1 Chinese Yuan =0.1612 US dollars) were collected for each Chinese city evaluated. Three to five clinical experts on IFI treatment at major tier-3A hospitals from the four representative cities were recruited and surveyed through a series of face-to-face interviews to determine actual resource utilization. Per-patient antifungal therapy costs were estimated by multiplying the daily drug acquisition costs by treatment duration (Table 2). The model incorporated additional resources utilized in IFI patient management as determined through the physician surveys (Table 3). Analysis of survey results showed a lack of differentiation in laboratory test utilization between the DD and the empiric approaches. This lack of differentiation between treatment approaches was previously reported.11 Hepatotoxicity was identified as the only adverse event requiring intensive treatment and resource use and therefore included in the model. Antifungal hepatotoxicity rates were obtained from the drug labels.12–14 The estimated cost to treat one case of hepatotoxicity was ¥400.
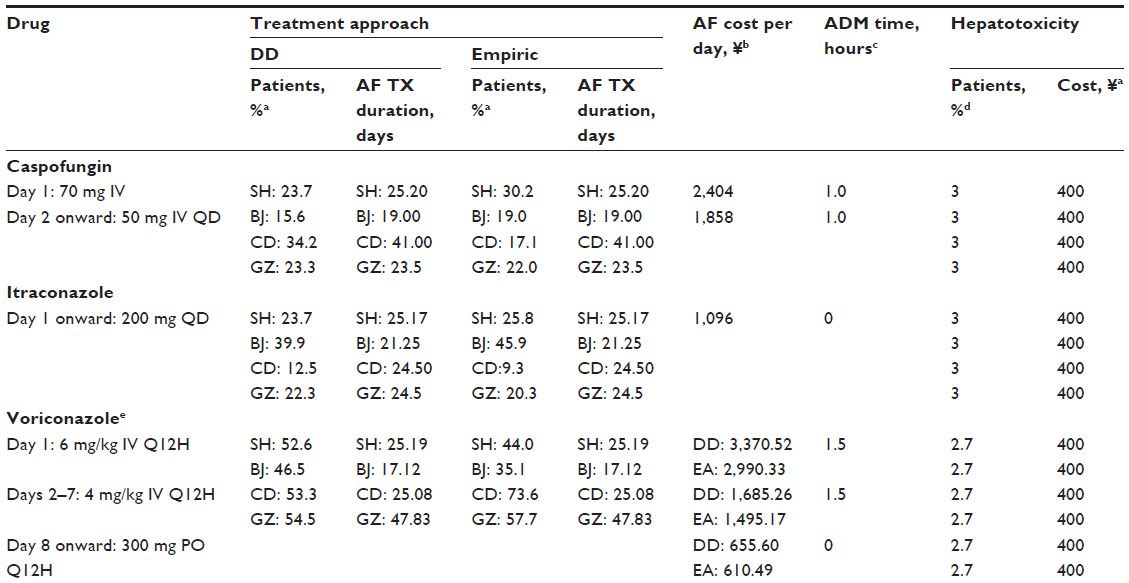 | Table 2 Antifungal therapy and adverse event model inputs |
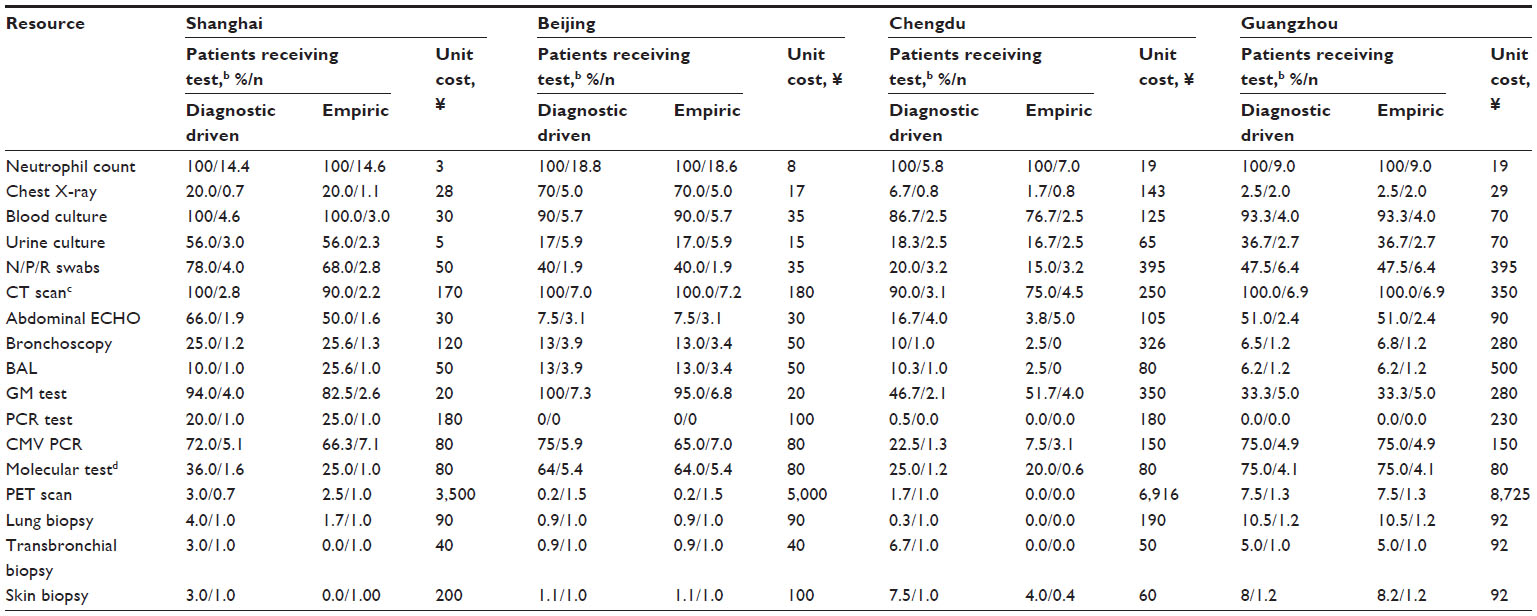 | Table 3 Model inputs for resource usea in Shanghai, Beijing, Chengdu, and Guangzhou |
Model analyses
The model estimates total costs, death avoided, and incremental cost-effectiveness ratios per death avoided for the DD and the empiric approaches from a third-party payer perspective in 2014 Chinese ¥. The base-case scenario incorporates real-world GM test and CT scan utilization rates. The CT scan and GM test sensitivity was averaged and applied to the DD treatment arm.15,16 A scenario analysis was conducted utilizing a GM test rate of 100% for the DD arm only, consistent with a recently published guideline.17
One-way sensitivity analyses were performed to assess the impact of each parameter on the incremental cost per death avoided. Second-order Monte Carlo simulations were also conducted to examine the robustness of model results and the effects of parameter uncertainty on study findings.
Results
Cost-effectiveness analysis (base-case results)
Cost results obtained from our model varied from ¥3,232 in Shanghai to ¥8,489 in Guangzhou for the DD and from ¥4,331 in Shanghai to ¥9,795 in Guangzhou for the empiric approach (Table 4). Fewer patients in the DD (5.7%) than empiric (9.8%) arm received antifungal treatment, although the number of patients diagnosed with IFIs was higher in the DD (5.7%) than empiric (3.3%) arm. Estimated survival rates ranged from 91.38% to 91.72% in the DD and 90.24% to 91.19% in the empiric treatment arms. As a result, the DD compared to empiric approach was cost saving (ie, cost less with similar mortality) to health care payers in the People’s Republic of China.
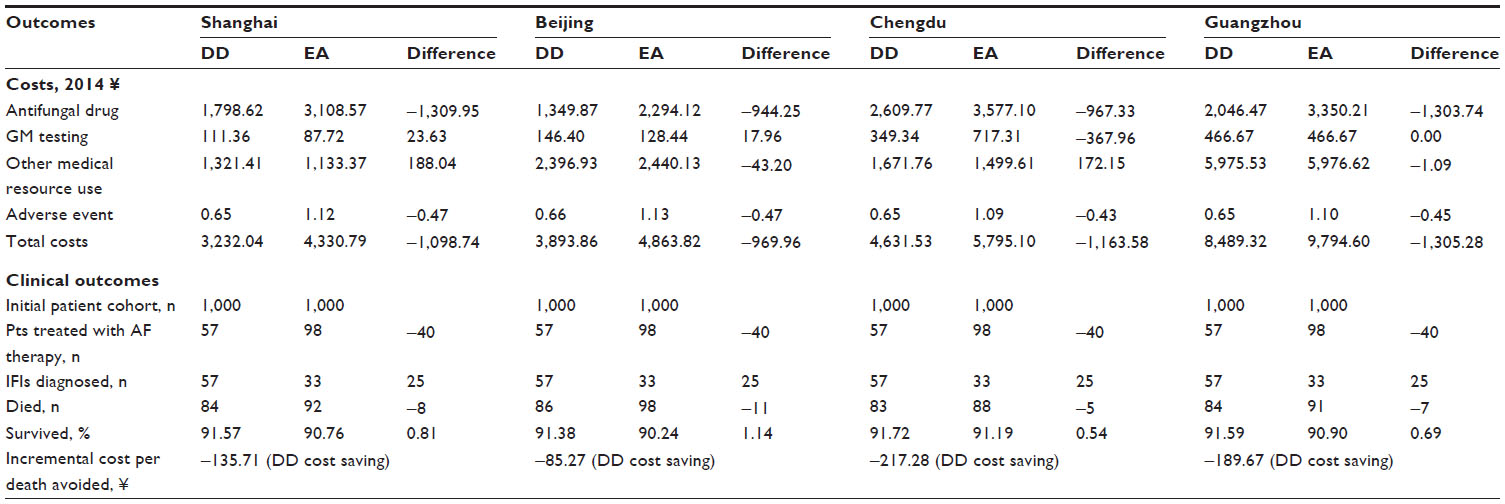 | Table 4 Modeled outcome results for DD and empiric IFI treatment strategies for four Chinese cities |
Scenario analysis
Results from the scenario analysis, in which GM test utilization was assumed to be 100%, show higher total costs per patient for both the DD and the empiric approaches compared to the base-case analysis, reflecting an increase in GM testing costs and number of IFIs diagnosed. For this scenario, total treatment costs per patient for the DD compared to the empiric approach, respectively, were ¥3,535 and ¥4,847 in Shanghai, ¥4,118 and ¥5,245 in Beijing, ¥5,463 and ¥6,389 in Chengdu, and ¥9,762 and ¥10,351 in Guangzhou. The number of diagnosed IFIs was higher in this scenario analysis (6.7%) than the base-case scenario (5.7%) for all four cities as a result of the higher diagnostic test sensitivity with 100% GM test utilization. Thus, more patients received antifungal treatment in this scenario (DD, 6.7% vs empiric approach, 11.4%) than the base-case (DD, 5.7% vs empiric approach, 9.8%).
One-way sensitivity analysis
Univariate one-way sensitivity analysis was conducted in the adapted Shanghai model to test the impact of parameter variations on the cost-effectiveness of a DD approach. The incremental cost per death avoided was most sensitive to changes in diagnostic test sensitivity, followed by IFI-related mortality (Figure 2). Cost savings per death avoided increased from ¥108 to ¥1,599 as the diagnostic test sensitivity increased from 47.5% to 95%. The DD approach remained dominant, regardless of variables changed. Dominance of the DD over the empiric approach was observed from the negative incremental cost-effectiveness ratios in terms of per death avoided in all cases. Results were similar for the other three cities (data not shown).
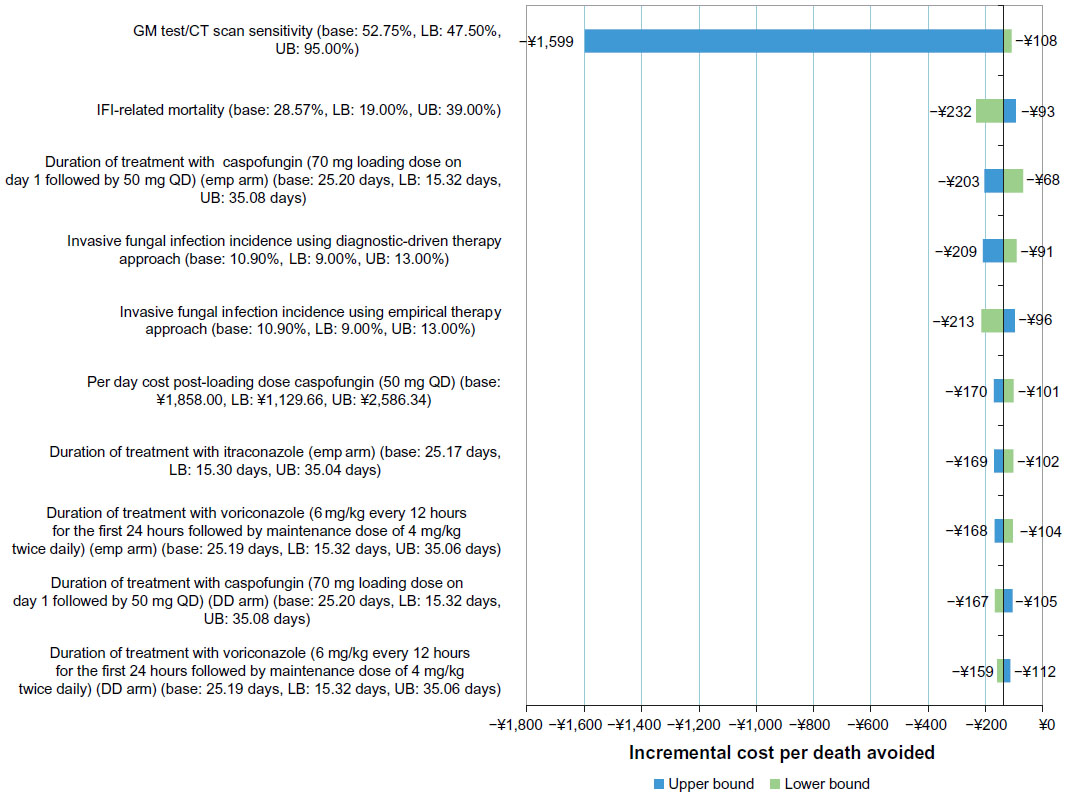 | Figure 2 One-way sensitivity analyses on incremental cost per death avoided comparing DD and empiric treatment approaches in Shanghai, the People’s Republic of China. |
Probabilistic sensitivity analysis
Second-order Monte Carlo simulations, in which all model parameters were varied, were run 10,000 times in order to capture stability in the results and the effects of parameter uncertainty on study findings for Shanghai. Results from this analysis showed that a DD approach was cost saving in 88.45% and an empiric approach in 0.06% of simulations (Figure 3).
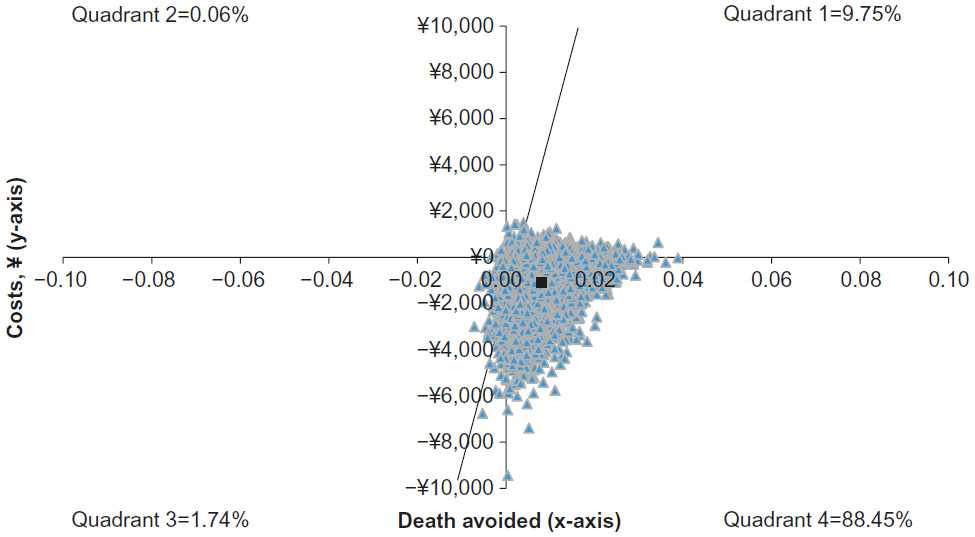 | Figure 3 Probabilistic sensitivity analysis scatter plot showing the incremental costs (in Chinese ¥) per death avoided for a DD compared to an empiric treatment approach in Shanghai, the People’s Republic of China. |
Discussion
Neutropenic patients with persistent fever following 72 hours of empiric antibiotic therapy are typically treated empirically for IFIs. Not all of these empirically treated patients will have IFIs, resulting in unnecessary administration of antifungal therapies and an increased risk of developing serious adverse events. Patients treated using a DD approach receive antifungal therapy following not only clinical suspicion but also diagnostic confirmation of fungal infections.
Results from our analyses found that a DD compared to an empiric treatment approach is cost saving (ie, cost less with similar mortality) from the point of view of the third-party payer (eg, Bureau of Human Resources and Social Security) in four Chinese cities (Beijing, Chengdu, Guangzhou, and Shanghai). In general, the increase in diagnostic test costs incurred was offset by a decrease in antifungal therapy costs due to identification of a more targeted treatment population in the DD (5.7%) than the empiric (9.8%) arm. Cost savings ranged from a low of ¥969.96 per patient in Beijing to a high of ¥1,305.28 per patient in Guangzhou. Results from one-way sensitivity analyses were most sensitive to changes in diagnostic test sensitivity followed by IFI-related mortality.
Differences in GM test utilization were evident among the four cities evaluated, potentially reflecting differences in test availability and acceptance. In Shanghai and Beijing, use of GM testing was high with 94% or more of patients treated using a DD approach receiving four to seven GM tests. In Chengdu and Guangzhou, <50% of patients received one to two GM tests. The lower use of GM testing in Chengdu and Guangzhou compared to Beijing and Shanghai is potentially reflective of test availability. Although GM testing is used in clinical practice in large cities, it is not yet available in many provinces.
Use of CT scans in a DD approach in the People’s Republic of China was common with 100% of patients in Shanghai, Beijing, and Guangzhou and 90% in Chengdu undergoing at least one CT scan. Combined use of GM tests and CT scans is consistent with recent guideline recommendations and should improve overall test sensitivity.18 However, until GM testing becomes universally available throughout the People’s Republic of China, CT scans will be the predominant test utilized in a DD approach. To reflect the differences in resource utilization among these four cities, we conducted sensitivity analyses to assess the impact of varying the percentages of patients receiving these two tests on our model results, which appeared robust to the change.
We found that the use of diagnostic tests to aid in the diagnosis of IFI in the People’s Republic of China varied widely and at times blurred the distinction between the DD and the empiric treatment approaches. Based on results obtained from the Chinese clinical expert interviews, we opted to only include GM testing and CT scans in our model. Although other biomarker screening tests such as beta-d-glucan and polymerase chain reaction tests are used to identify patients with invasive aspergillosis in other parts of the world, these tests are rarely utilized in the People’s Republic of China and therefore were not incorporated into the model.
Results from this Chinese pharmacoeconomic model adaptation are similar to those reported for the UK8 and Spain.19 Lower total costs were reported for patients treated using a DD (£1,561) compared to an empiric (£2,302) approach in the UK. Although per-patient medical costs were higher for the cohort treated using a DD compared to an empiric approach (£734 vs £623, respectively), these costs were offset by lower per-patient antifungal treatment costs (£799 vs £1,678, respectively). In the Spanish model, the DD approach was dominant with an average cost-effectiveness per persistent febrile episode of €32,671 versus €52,479 for the empiric approach.
Our modeled results are similar to those reported from clinical studies. Results from our study predict that fewer patients treated using a DD than an empiric approach would receive antifungal therapy. Similarly, Maertens et al found a decrease in antifungal administration using a preemptive compared to an empiric treatment approach. In this study, antifungal drug administration was reduced by 78% in patients treated using a preemptive compared to an empiric treatment approach.6 Results reported by Girmenia et al4 were also similar with a 43% decrease in antifungal drug administration with a DD (48 cases) compared to an empiric (84 cases) treatment approach.
The results of our analysis should be evaluated with the following limitations. First, a decision model was used to extrapolate and compile data in a mathematical and systematic manner to enable a comparative analysis because of limited published head-to-head clinical data comparing a DD versus an empiric treatment approach. Although a real-world analysis may more accurately reflect IFI incidence and mortality at a hospital in the People’s Republic of China, the resources required to abstract real-world data from several hospitals located in different regions of the People’s Republic of China was prohibitive. We therefore opted to construct a decision model incorporating data obtained from interviews of experts practicing at tier-3A hospitals located in four Chinese cities, representing geographically different locations and addressing variability in inputs such as IFI incidence, mortality, and duration of treatment in the sensitivity analyses. As we observed, there was considerable heterogeneity in physicians’ treatment habits and considerable variability in resource utilization was noted for the four cities evaluated. Second, the clinical data used in the model were obtained from the published literature and supplemented with resource use and cost data obtained from top clinicians located at tier-3A hospitals in the People’s Republic of China. These results may not be generalizable to a broader population. However, results from our analysis were consistent with published clinical studies, suggesting that a DD compared to an empiric treatment approach is cost saving for neutropenic fever in the People’s Republic of China. Third, the incidence data incorporated into the model were for IFIs, not specifically invasive aspergillosis. Real-world incidence data for invasive aspergillosis within a particular clinical setting such as patients treated with myelosuppressive chemotherapy are scarce in the published literature. Therefore, our model was propagated using the IFI incidence reported by Hahn-Ast for patients with IFIs and neutropenia after myelosuppressive chemotherapy.9 Although this may be an overestimate of the true incidence of invasive aspergillosis in this population, additional cost savings could be realized if the true incidence of invasive aspergillosis was lower than the IFI incidence incorporated into the model. Finally, we did not account for patients empirically initiated on antifungal therapy having their antifungal therapy discontinued early as a result of negative biomarker test and/or CT scan results. Although this would decrease the overall costs associated with the empiric approach, these patients would still be unnecessarily exposed to antifungal therapy and the risks associated with antifungal administration.
Conclusion
Results from our model incorporating real-world data support a change in the treatment paradigm for IFIs from an empiric to a DD approach in the People’s Republic of China for neutropenic patients with persistent fever unresponsive to broad-spectrum antibiotic therapy. Total costs were lower with similar survival for the cohort of neutropenic patients treated with a DD compared to an empiric approach, despite the additional costs of GM antigen and CT scan testing. Additional benefits could potentially be realized through standardization of a DD treatment protocol as collected data showed considerable variability in both DD and empiric treatment strategies throughout the People’s Republic of China.
Acknowledgments
Interim findings for the Shanghai analyses were presented at the ISPOR 17th Annual European Congress, November 8–12, 2014, in Amsterdam, the Netherlands, as a poster presentation. The abstract for this presentation is available on http://www.valueinhealthjournal.com/article/S1098-3015(14)04409-X/pdf. Interim findings for the Beijing, Chengdu, and Guangzhou analyses were presented at the 2015 ISPOR Annual International Meeting, May 16–20, 2015, in Philadelphia, PA, USA, as a poster presentation. The abstract of this poster is available on https://www.rti.org/publications/abstract.cfm?pubid=24212.
Disclosure
Financial support for this study was provided through a grant from Pfizer Investment Co. Ltd., Beijing, People’s Republic of China. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, and writing and publishing the report. Yixi Chen and Claudie Charbonneau are employed by the sponsor. The authors report no other conflicts of interest in this work.
References
Liao Y, Chen M, Hartmann T, Yang RY, Liao WQ. Epidemiology of opportunistic invasive fungal infections in China: review of literature. Chin Med J (Engl). 2013;126(2):361–368. | |
Warnock DW. Trends in the epidemiology of invasive fungal infections. Nippon Ishinkin Gakkai Zasshi. 2007;48(1):1–12. | |
Cordonnier C, Pautas C, Maury S, et al. Empirical versus preemptive antifungal therapy for high-risk, febrile, neutropenic patients: a randomized, controlled trial. Clin Infect Dis. 2009;48(8):1042–1051. | |
Girmenia C, Micozzi A, Gentile G, et al. Clinically driven diagnostic antifungal approach in neutropenic patients: a prospective feasibility study. J Clin Oncol. 2010;28(4):667–674. | |
Hebart H, Klingspor L, Klingebiel T, et al. A prospective randomized controlled trial comparing PCR-based and empirical treatment with liposomal amphotericin B in patients after allo-SCT. Bone Marrow Transplant. 2009;43(7):553–561. | |
Maertens J, Theunissen K, Verhoef G, et al. Galactomannan and computed tomography-based preemptive antifungal therapy in neutropenic patients at high risk for invasive fungal infection: a prospective feasibility study. Clin Infect Dis. 2005;41(9):1242–1250. | |
Pagano L, Caira M, Nosari A, et al. The use and efficacy of empirical versus pre-emptive therapy in the management of fungal infections: the HEMA e-Chart Project. Haematologica. 2011;96(9):1366–1370. | |
Barnes R, Earnshaw S, Herbrecht R, et al. Economic comparison of an empirical versus diagnostic-driven strategy for treating invasive fungal disease in immunocompromised patients. Clin Ther. 2015;37(6):1317–1328.e2. | |
Hahn-Ast C, Glasmacher A, Muckter S, et al. Overall survival and fungal infection-related mortality in patients with invasive fungal infection and neutropenia after myelosuppressive chemotherapy in a tertiary care centre from 1995 to 2006. J Antimicrob Chemother. 2010;65(4):761–768. | |
Boogaerts M, Winston DJ, Bow EJ, et al. Intravenous and oral itraconazole versus intravenous amphotericin B deoxycholate as empirical antifungal therapy for persistent fever in neutropenic patients with cancer who are receiving broad-spectrum antibacterial therapy. A randomized, controlled trial. Ann Intern Med. 2001;135(6):412–422. | |
Tan BH, Low JG, Chlebicka NL, et al. Galactomannan-guided preemptive vs empirical antifungals in the persistently febrile neutropenic patient: a prospective randomized study. Int J Infect Dis. 2011;15(5):e350–e356. | |
VFEND [package insert]. New York, NY: Roerig; 2014. | |
Cancidas [package insert]. Whitehouse Station, NJ: Merck and Co., Inc; 2014. | |
Sporanox [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 2014. | |
Kami M, Kishi Y, Hamaki T, et al. The value of the chest computed tomography halo sign in the diagnosis of invasive pulmonary aspergillosis. An autopsy-based retrospective study of 48 patients. Mycoses. 2002;45(8):287–294. | |
Pfeiffer CD, Fine JP, Safdar N. Diagnosis of invasive aspergillosis using a galactomannan assay: a meta-analysis. Clin Infect Dis. 2006;42(10):1417–1427. | |
Morrissey CO, Gilroy NM, Macesic N, et al. Consensus guidelines for the use of empiric and diagnostic-driven antifungal treatment strategies in haematological malignancy, 2014. Intern Med J. 2014;44(12b):1298–1314. | |
Marchetti O, Lamoth F, Mikulska M, et al. ECIL recommendations for the use of biological markers for the diagnosis of invasive fungal diseases in leukemic patients and hematopoietic SCT recipients. Bone Marrow Transplant. 2012;47(6):846–854. | |
Martin-Pena A, Gil-Navarro MV, Aguilar-Guisado M, et al. Cost-effectiveness analysis comparing two approaches for empirical antifungal therapy in hematological patients with persistent febrile neutropenia. Antimicrob Agents Chemother. 2013;57(10):4664–4672. | |
Morrissey CO, Chen SC, Sorrell TC, et al. Galactomannan and PCR versus culture and histology for directing use of antifungal treatment for invasive aspergillosis in high-risk haematology patients: a randomised controlled trial. Lancet Infect Dis. 2013;13(6):519–528. | |
Body weight [webpage on the Internet]. Human Body Weight; 2014. Available from: http://en.wikipedia.org/wiki/Body_weight. Accessed March 24, 2016. | |
Ascioglu S, Rex JH, de Pauw B, et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis. 2002;34(1):7–14. | |
Cao J, Ye W, Zhang L, Lu X, Sun Y. Clinical nursing system and staff composition in Shanghai. J Nurs Adm. 2009;39(3):113–114. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.