Back to Journals » Infection and Drug Resistance » Volume 13
Echinocandins versus Amphotericin B Against Candida tropicalis Fungemia in Adult Hematological Patients with Neutropenia: A Multicenter Retrospective Cohort Study
Authors You L ![]() , Yao C, Yang F, Yang Q
, Yao C, Yang F, Yang Q ![]() , Lan J, Song X, Shen J, Sheng X, Chen X, Tang H
, Lan J, Song X, Shen J, Sheng X, Chen X, Tang H ![]() , Jiang H, Wu H, Qian S, Meng H
, Jiang H, Wu H, Qian S, Meng H
Received 18 April 2020
Accepted for publication 25 June 2020
Published 10 July 2020 Volume 2020:13 Pages 2229—2235
DOI https://doi.org/10.2147/IDR.S258744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Liangshun You,1,* Cunying Yao,1,2,* Fan Yang,3 Qing Yang,4 Jianping Lan,5 Xiaolu Song,5 Jianping Shen,6 Xianfu Sheng,6 Xiaohui Chen,7 Huifen Tang,7 Huifang Jiang,8 Haiying Wu,8 Shenxian Qian,3 Haitao Meng1
1Department of Hematology, The First Affiliated Hospital of Medical School of Zhejiang University, Hangzhou, People’s Republic of China; 2Department of Hematology, The Second Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Department of Hematology, Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 4State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital of Medical School of Zhejiang University, Hangzhou, People’s Republic of China; 5Department of Hematology, Zhejiang Provincial People’s Hospital, Hangzhou, People’s Republic of China; 6Department of Hematology, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 7Department of Hematology, The Affiliated Hospital, Hangzhou Normal University, Hangzhou, People’s Republic of China; 8Department of Hematology, Tongde Hospital of Zhejiang Province, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haitao Meng; Shenxian Qian Email [email protected]; [email protected]
Background: Candida tropicalis is the most common non-albicans Candida species identified in immunocompromised patients, which often appears with high mortality. However, data on the outcomes of treatment for Candida tropicalis fungemia in patients with neutropenia remain limited.
Methods: In the present study, 90 neutropenic adult patients with proven Candida tropicalis fungemia, who received initial antifungal therapy, were retrospectively analyzed.
Results: These results revealed that the overall 8-day and 30-day mortality among patients in the entire data set were 22.2% and 33.3%, respectively. However, there was no significant difference between the survival and death group, in terms of baseline characteristics. The univariate analysis of risk factors identified the treatment with azole as a predictor of mortality, while treatments that containing amphotericin B were associated with reduced mortality. In addition, the survival rate on day 30 was observed in 60.7% (17/28) of patients who were initially treated with echinocandins, while this was observed in 86.4% (19/22, P= 0.039) and 100% (13/13, P= 0.024) of patients treated with amphotericin B plus echinocandins and amphotericin B, respectively.
Conclusion: These data indicate for the first time that the initial therapy with amphotericin B-based agents was associated with a better survival rate and could be assessed as the optimal strategy for the treatment of Candida tropicalis fungemia in patients with neutropenia.
Keywords: Candida tropicalis, candidemia, hematological malignancy, neutropenia, amphotericin B, echinocandins
Introduction
Epidemiologic studies from the last two decades have identified that candidemia is the fourth most common nosocomial bloodstream infection worldwide.1–3 The proportion of non-albicans candidemia has been increasing in recent years, and often appears with antifungal resistance and poor outcomes.4–6 The occurrence of candidemia varies among different non-albicans Candida species, which is dependent on both underlying diseases and risk factors, such as neutropenia, immunosuppressive therapy, and so on.7–9 As a consequence, Candida tropicalis is one common Candida species, and candidemia due to Candida tropicalis has been characterized by high mortality in hematology patients with neutropenia or immunosuppression.10,11
Recently, for the treatment of candidemia in neutropenic patients, the Infectious Diseases Society of America (IDSA) guidelines first recommend either an echinocandins (Ech), or lipid formulation of amphotericin B (L-AmB).12 However, the optimal treatment for candidemia caused by Candida tropicalis in neutropenic patients remains unclear. A study performed by Koji et al revealed that L-AmB exhibited greater efficacy than Ech, in terms of prolonging the survival time in neutropenic murine systemic infections caused by Candida tropicalis.13 Unfortunately, at present, no study has directly compared the treatment outcomes of L-AmB and Ech for Candida tropicalis fungemia in patients with neutropenia. In addition, no differences in terms of efficacy were found between conventional AmB (c-AmB) and L-AmB in the treatment of invasive candidiasis.14 To this context, a multicenter retrospective cohort study was performed to provide better evidence for the efficacy of AmB (including c-AmB and L-AmB), when compared to Ech, in treating Candida tropicalis fungemia in hematological patients with neutropenia.
Patients and Methods
Patient Population and Inclusion Criteria
Electronic medical records of individuals diagnosed with Candida tropicalis fungemia between January 2011 and December 2018 at six hospitals in China were reviewed: the First Affiliated Hospital of Medical School of Zhejiang University; Affiliated Hangzhou first People’s Hospital, Zhejiang University School of Medicine; Zhejiang Provincial People’s Hospital; the First Affiliated Hospital of Zhejiang Chinese Medical University; the Affiliated Hospital, Hangzhou Normal University; Tongde Hospital of Zhejiang Province. All cohorts included adult patients (≥16 years old) with candidemia caused by Candida tropicalis treated with intravenous antifungal agents using the standard doses recommended by the IDSA for ≥3 days. Patients with HIV infection or those who suffered from any other severe infections were excluded from the analysis. Finally, 90 patients as well as 85 isolates from the first blood culture were analyzed in this study. The primary outcomes were 8-day and 30-day mortality. The study protocol was approved by the Ethics Committee of the participating hospitals. Given the retrospective nature of the study, the requirement for a written informed consent was waived. Patient confidentiality policy is based on local law of data protection in this study.
Definitions
Candidemia is defined as patients with at least one set of positive blood culture of Candida tropicalis with compatible clinical symptoms of infection, such as fever, chills, or blood pressure decline, and expelling other factors. Neutropenia is defined as an absolute neutrophil count of <500 cells/μL. Prior azoles exposure was recorded when patients were administered with a standard dosage of azoles prior to candidemia for at least three days. Colonization was defined as at least one positive culture of Candida tropicalis in the prior two weeks, which was collected from the following sites: the oropharynx, stomach, urine, tracheal secretion, drainage tube, and wound. Catheter-related candidemia is considered when the catheter tip was colonized with the same Candida tropicalis strain (showing the same antifungal susceptibility) from the blood culture or the quantitative blood sample culture from the central venous catheter (CVC) showed a ≥5-fold greater colony count than the concurrent peripheral venous quantitative blood culture. Azoles include fluconazole, itraconazole posaconazole and voriconazole. The Ech agents included caspofungin and micafungin, while AmB included c-AmB and L-AmB. The patients who were initially administered with adequate antifungal drugs for ≥3 days were included in the efficacy analysis of antifungal therapy. All dosages of antifungal agents were administered according to the IDSA guidelines. Candida tropicalis that exhibited resistance to one or more azoles was defined as azole resistance. The 8-day and 30-day mortality represent the time to death since the diagnosis of candidemia.
Identification and Antifungal Susceptibility
The identification and antifungal susceptibility test were described in the previous study of the investigators.15 Briefly, all Candida tropicalis isolates obtained from patients were identified using the CHROM Agar Candida API20C system. The antifungal susceptibility test of Candida tropicalis was confirmed by the E-TEST methodology according to the breakpoints of CLSI criteria.
Statistical Analysis
Continuous variables are presented as mean and standard deviation (SD), while categorical variables are reported in numbers and percentages. In order to evaluate the factors associated with mortality, the univariate analysis was performed using unpaired Student’s t-test or non-parametric (Mann–Whitney) test for continuous variables, while Chi-square test or Fisher’s exact test were used for categorical variables. The adjusted odds ratio (OR) and 95% confidence interval (CI) for factors associated with mortality were calculated. The Chi-square test or Fisher’s exact test was performed to compare the clinical outcomes between treatment groups. All tests were two-tailed, and a P-value of <0.05 was considered statistically significant. SPSS Statistics version 20.0 was used for all statistical analyses.
Results
Characteristics of the Clinical Data
A total of 182 consecutive patients, who were diagnosed with Candida tropicalis fungemia between January 2011 and December 2018 at six cohorts in China, were retrospectively included. Among these patients, 98 hematological patients were diagnosed with neutropenia. However, eight patients of these patients were excluded due to the following reasons: five patients received initial treatment with a lower than standard dose of antifungal agents, two patients had severe bacterial pneumonia, and one patient gave up any of the treatments. The remaining 90 patients were analyzed, and their baseline characteristics, clinical presentations and outcomes are summarized in Table 1.
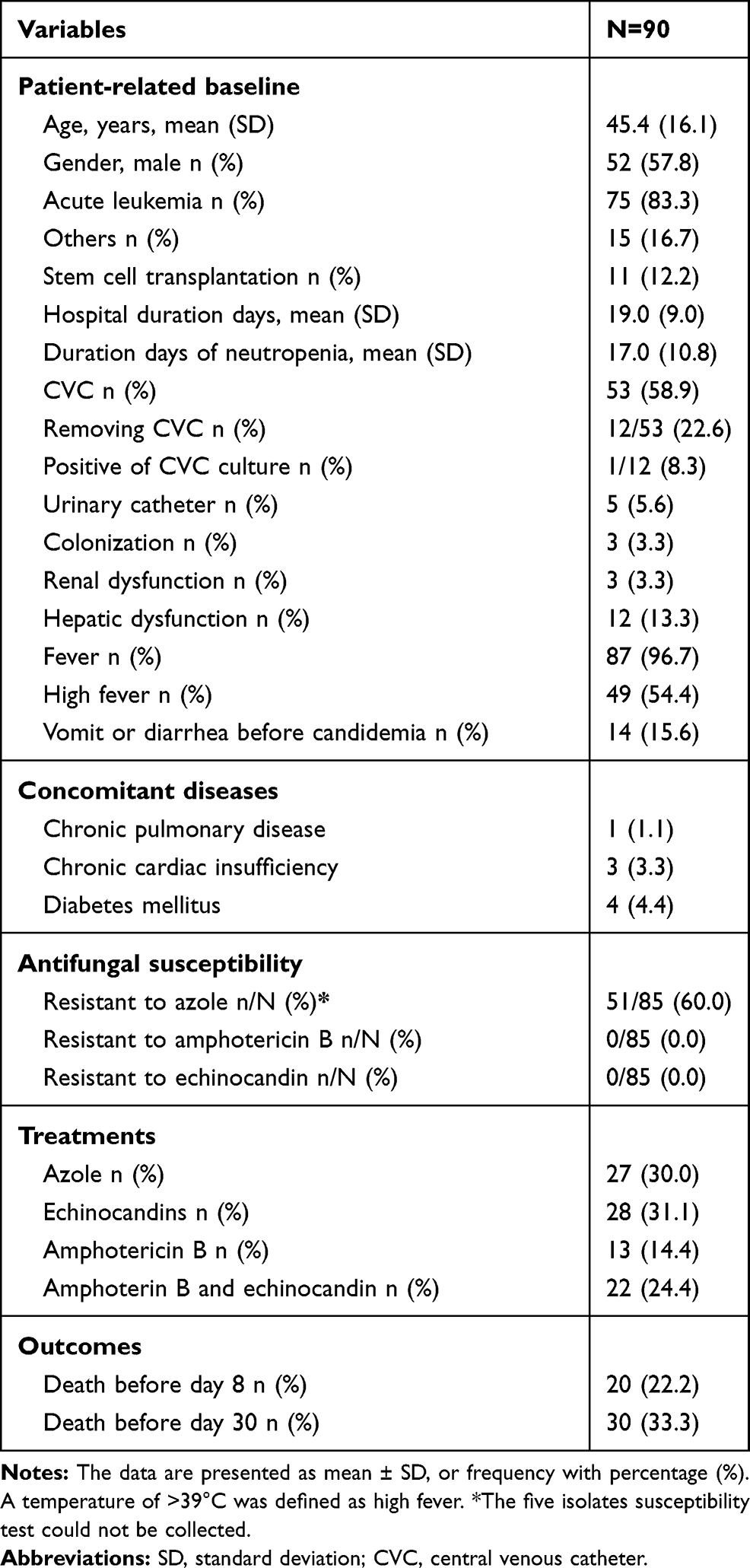 |
Table 1 Demographics, Clinical Characteristics, Antifungal Susceptibility, Treatment, and Outcome |
All patients were diagnosed with active hematological disease, and most of these patients had leukemia (83.3%). The mean age of these patients was 45.1±16.1 years old, and 57.8% of these patients were male. The duration of the neutropenia was 17.0±10.8 days. In this series, 53 patients (58.9%) had a central venous catheter (CVC) when they were diagnosed with candidemia. Among these patients, 12 patients received treatment for removing the CVC, and one catheter tip (8.3%) was identified with the same Candida tropicalis strain (showing the same antifungal susceptibility) from the blood culture.
These patients had a low proportion of concomitant diseases. Fever (96.7%), especially high fever (54.4%), was the main clinical presentation, followed by digestive manifestations (15.6%) and hyperbilirubin (13.3%). Eighty-five of 90 (94.0%) episodes of candidemia had antifungal susceptibility results. All isolates were susceptible to AmB and Ech, while up to 51 (60%) isolates were resistant to azole. The initial antifungal therapy consisted of triazole (n=27), AmB (n=13), Ech (n=28) and AmB plus Ech (n=22). The clinical outcomes revealed that the overall 8-day and 30-day mortality was 22.2% and 33.3%, respectively.
Factors Associated with Mortality and Treatment Response
Univariate analyses were performed to identify multiple factors significantly associated with the 8-day and 30-day mortality (Table 2). Based on the baseline characteristics (which included 16 predictors), there were no statistically significant differences between the survival and death groups. The treatment with different initial antifungal was the main prognosis factor. Patients with azole treatment were associated with 8-day (P=0.000) and 30-day (P=0.002) mortality. Conversely, survival was significantly better for those who initially received AmB-containing antifungal treatment, which included AmB (P=0.046 and P=0.025, respectively) and AmB plus Ech (P=0.018 and P=0.016, respectively).
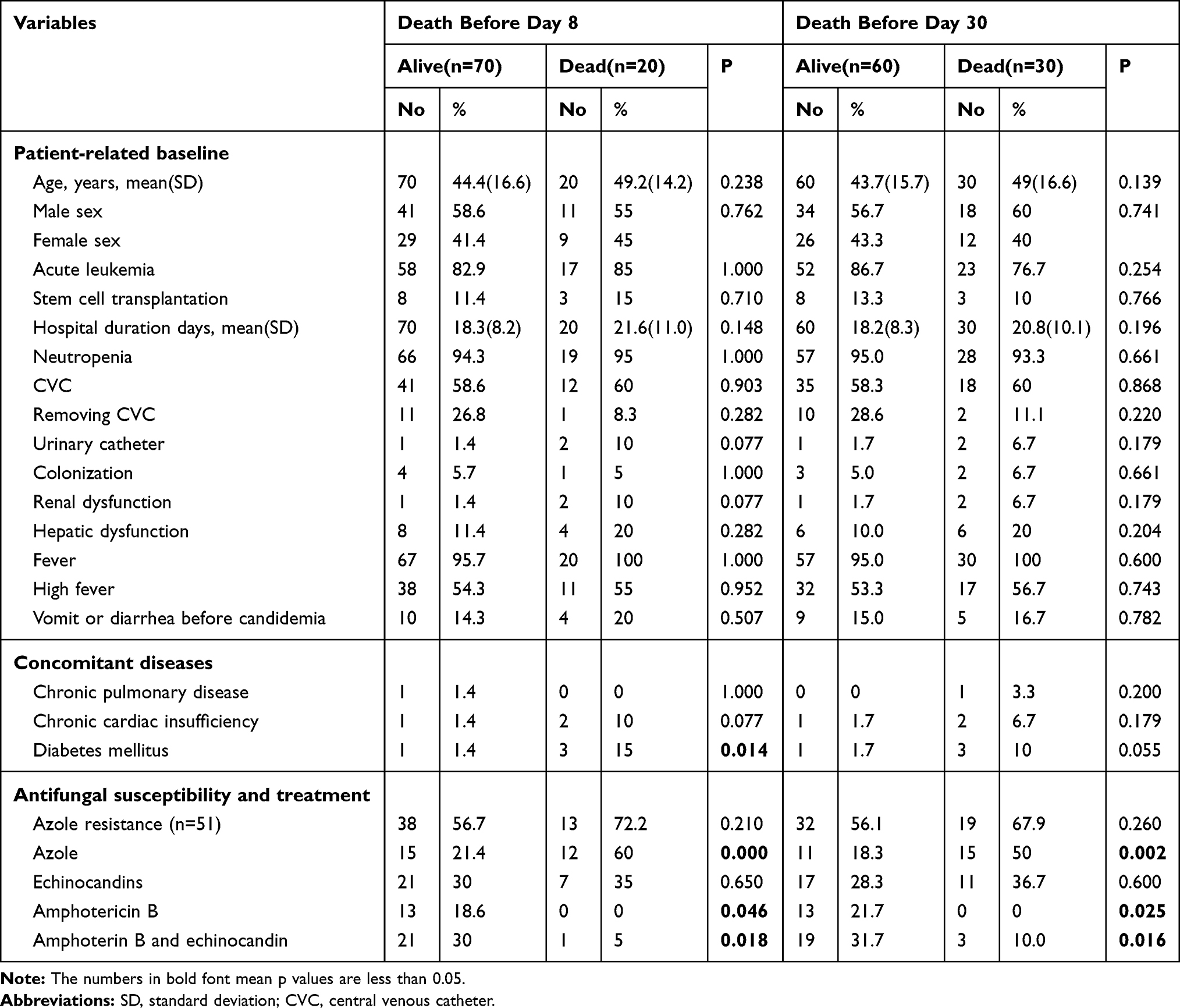 |
Table 2 Univariate Analysis of the Risk Factors and Outcomes |
Next, the clinical outcomes between the different treatment groups were compared. There were no differences in patient-related baseline and concomitant diseases among azole, Ech and AmB groups (data not shown). Compared to triazole group, a trend of superior survival could be observed in the Ech group on day 8 and 30. However, the difference between them was not statistically significant (75% vs 55.6% for 8-day with P=0.130; 60.7% vs 40.7% for 30-day with P=0.139) (Figure 1A), which may be attributed to small size sample. Notably, AmB-containing antifungal treatment could achieve satisfactory clinical efficacy, which had better survival rates than the treatment of Ech on day 30 (AmB vs Ech: 100% vs 60.7%, P=0.024; AmB plus Ech vs Ech: 86.4% vs 60.7%, P=0.039) (Figure 1B). These results indicate that AmB can be considered as the optimal initial treatment of Candida tropicalis fungemia in patients with neutropenia.
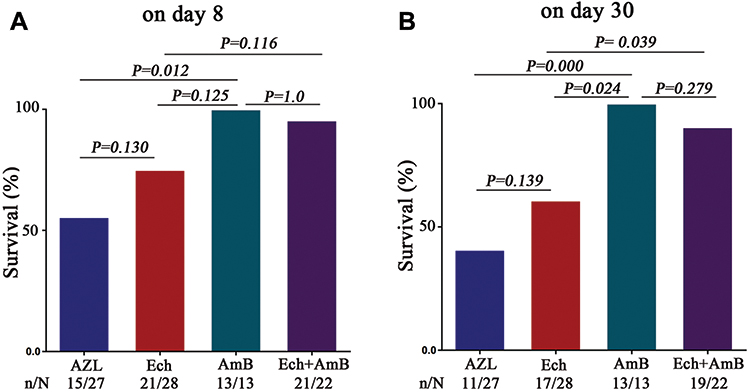 |
Figure 1 Comparison of clinical outcomes between different initial antifungal treatments. (A) The survival rates for day 8. Compared to the Ech group, a trend of superior survival could be observed in AmB-containing groups on day 8. (B) The survival rates for day 30. Patients who received AmB-containing antifungal treatment had a better survival rate than other patients on day 30 (AmB vs Ech: 100% vs 60.7%, P=0.024; AmB plus Ech vs Ech: 86.4% vs 60.7%, P=0.039; AmB vs AZL: 100% vs 40.7%, P=0.000). Abbreviations: AZL, azoles; Ech, echinocandins; AmB, amphotericin B. |
Azole Resistance and Treatment Outcome
Eight-five of 90 (90.4%) episodes of candidemia had antifungal susceptibility results. Fifty-one of 85 (60%) isolates were resistant to azole. Among these, one isolate was pan-azole resistant, which received Ech treatment. Forty-eight isolates were fluconazole resistant and two isolates were itraconazole resistant, all of these patients were received posaconazole or voriconazole treatment in azole treatment group. Furthermore, it was found that azoles exposure prior to candidemia could greatly increase the resistance rate of Candida tropicalis to azoles. Twenty-eight of 31 isolates with azole exposure prior to candidemia were resistant to azoles, which was significantly higher than those with no azole exposure before candidemia (90.3% vs 42.6%, P=0.000) (Figure 2A). Although a trend towards inferior survival could be observed in the azole-resistance group on day 8 and 30, the difference was not statistically significant (Figure 2B and C).
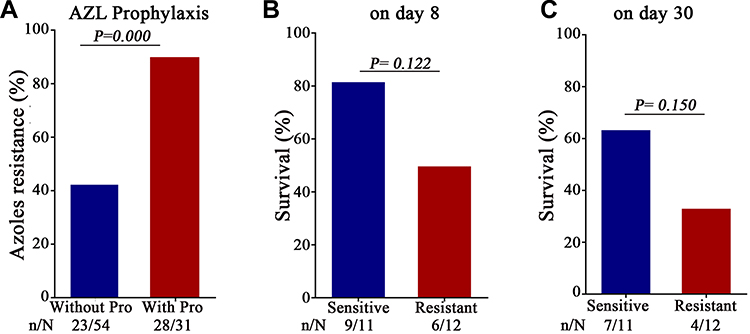 |
Figure 2 Azole resistance and outcomes. (A) The relationship between azole exposure and azole resistance. The azole resistance rate of isolates with azole exposure was significantly higher than those with no azole exposure before candidemia (90.3% vs 42.6%, P=0.000). (B and C) Comparison of clinical outcomes between azole-resistance and azole-sensitive groups on day 8 (B) and day 30 (C). Although a trend towards inferior survival could be observed in the azole-resistance group on day 8 and 30, the difference was not statistically significant. Abbreviations: AZL, azoles; Ech, echinocandins; AmB, amphotericin B; Pro, prophylaxis. |
Discussion
Candida tropicalis is the most commonly responsible for non-albicans candidemia in hematology patients with neutropenia, and is associated with high mortality.10,11 The primary objective of the present study was to add to the limited evidence base the treatment of Candida tropicalis fungemia in hematology patients with neutropenia, and compare clinical outcomes of AmB and Ech in these patients.
Similar to previous studies, the mortality at day 30 in the present study was 33.3%, which was significantly higher than that for patients with non-neutropenia, or with other non-albicans species-induced candidemia, suggesting that candidemia caused by Candida tropicalis and neutropenia are indeed risk factors for treatment failure.16–18 Some researchers have demonstrated that many factors affect the prognosis of patients with candidemia.18,19 Incompatibly, in the present study, no actual difference was found in the analysis of baseline characteristics between the survival and death groups. One possible reason is that the neutropenic patients included in the present analysis all had active blood cancers, and a younger average age with lower rates of concomitant diseases. The topic of CVC removal, regardless of whether this is associated with better prognosis for critical ill patients with candidemia, has been a matter of debate for years.16,20-24 As illustrated in the present study, although the recovery was not correlated to the treatment of removing CVC, positive culture of Candida tropicalis isolates from CVCs tends to argue for its removal, when possible, since CVC can be at high risk of fungal biofilm development.
The overall resistance rate of Candida tropicalis to azole was 60%, which was higher than that in some studies reported not only in China, but also in other countries.5,25,26 This may be mainly due to azoles commonly used as prophylaxis in hematology patients with neutropenia. More than 30% of patients received azoles prophylaxis in the present data, and 90.3% of isolates with azole prophylaxis acquired azoles resistance. These are in agreement with recent studies, in which azoles exposure is an independent risk factor for the development azole-resistant Candida species.27,28 Although no statistical significance was observed between azole-resistance and the overall mortality on day 8 and 30, there was a trend towards inferior survival in the azole-resistance group, which may due to the small sample size.
Considering that antifungal treatment is vital for critically ill patients who are unresponsive to antibiotics, the efficacy of these initial antifungal treatments was compared through the 8-day and 30-day mortality index. The univariate analysis revealed that patients with azole treatment were associated with inferior prognosis, while patients with AmB-containing antifungal treatment were associated with superior prognosis. Previous studies have confirmed that there are no differences between Ech and AmB, in terms of the efficacy in the treatment of invasive candidiasis.14 However, the proportion of candidemia caused by Candida tropicalis in patients with neutropenia was either too small, or not analyzed separately in these studies.19,23,28 To the best of our knowledge, the present study is the first to directly compare the treatment outcomes of AmB and Ech for Candida tropicalis fungemia in patients with neutropenia. It was found that AmB-containing antifungal was more effective than Ech, and had a better survival rate on day 30, indicating that AmB could be adopted as the optimal initial treatment for Candida tropicalis fungemia in the patients with neutropenia.
There were several limitations in the present study. First, the present study has a retrospective design based on pre-existing data, and is susceptible to bias. In addition, the present study was carried out in one city, which may be not applicable to other cities or countries. Furthermore, the samples that were included in this study had a modest size, although this already is the largest sample of Candida tropicalis fungemia with neutropenia at present. Lastly, there is lack of a case-control in the cohort study.
Conclusion
In summary, Candida tropicalis fungemia presents as an important cause of mortality in hematology patients with neutropenia. The present data demonstrate for the first time that the initial choice of antifungal agent is an independent predictor of mortality, and that AmB-containing agents may be assessed as the optimal initial treatment for these patients. A future randomized controlled trial is required to further confirm these present findings.
Data Sharing Statement
The datasets and material used and/or analyzed during the current study are available from the corresponding author upon request.
Ethics Approval
This experiment was approved by an independent ethics committee of The First Affiliated Hospital, College of Medicine, Zhejiang University (no.2018035).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Cleveland AA, Harrison LH, Farley MM, et al. Declining incidence of candidemia and the shifting epidemiology of Candida resistance in two US metropolitan areas, 2008–2013: results from population-based surveillance. PLoS One. 2015;10(3):e0120452. doi:10.1371/journal.pone.0120452
2. Wisplinghoff H, Bischoff T, Tallent SM, et al. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39(3):309–317. doi:10.1086/421946
3. Doi AM, Pignatari ACC, Edmond MB, et al. Epidemiology and microbiologic characterization of nosocomial candidemia from a Brazilian national surveillance program. PLoS One. 2016;11(1):e0146909. doi:10.1371/journal.pone.0146909
4. Kreusch A, Karstaedt AS. Candidemia among adults in Soweto, South Africa, 1990–2007. Int J Infect Dis. 2013;17(8):e621–23. doi:10.1016/j.ijid.2013.02.010
5. Tan TY, Hsu LY, Alejandria MM, et al. Antifungal susceptibility of invasive Candida bloodstream isolates from the Asia-Pacific region. Med Mycol. 2016;54(5):471–477. doi:10.1093/mmy/myv114
6. Hii IM, Chang HL, Lin LC, et al. Changing epidemiology of candidemia in a medical center in middle Taiwan. J Microbiol Immunol Infect. 2015;48(3):306–315. doi:10.1016/j.jmii.2013.08.017
7. Li D, Xia R, Zhang Q, et al. Evaluation of candidemia in epidemiology and risk factors among cancer patients in a cancer center of China: an 8-year case-control study. BMC Infect Dis. 2017;17(1):536. doi:10.1186/s12879-017-2636-x
8. Wu Z, Liu Y, Feng X, et al. Candidemia: incidence rates, type of species, and risk factors at a tertiary care academic hospital in China. Int J Infect Dis. 2014;22:4–8. doi:10.1016/j.ijid.2013.11.011
9. Yapar N. Epidemiology and risk factors for invasive candidiasis. Ther Clin Risk Manag. 2014;10:95–105. doi:10.2147/TCRM.S40160
10. Tan BH, Chakrabarti A, Li RY, et al. Incidence and species distribution of candidaemia in Asia: a laboratory-based surveillance study. Clin Microbiol Infect. 2015;21(10):946–953. doi:10.1016/j.cmi.2015.06.010
11. Puig-Asensio M, Ruiz-Camps I, Fernandez-Ruiz M, et al. Epidemiology and outcome of candidaemia in patients with oncological and haematological malignancies: results from a population-based surveillance in Spain. Clin Microbiol Infect. 2015;21(5):
12. Pappas PG, Kauffman CA, Andes DR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;62(4):e1–50. doi:10.1093/cid/civ1194
13. Takemoto K, Nakayama T, Kanazawa K, et al. Influence of fungicidal activity against Candida tropicalis on the efficacy of micafungin and liposomal amphotericin B in a neutropenic murine lethal infection model. Pharmacology. 2012;90(3–4):133–145. doi:10.1159/000341370
14. Hamill RJ. Amphotericin B formulations: a comparative review of efficacy and toxicity. Drugs. 2013;73(9):919–934. doi:10.1007/s40265-013-0069-4
15. You L, Qian W, Yang Q, et al. ERG11 gene mutations and MDR1 upregulation confer pan-azole resistance in candida tropicalis causing disseminated candidiasis in an acute lymphoblastic leukemia patient on posaconazole prophylaxis. Antimicrob Agents Chemother. 2017;61(7):e02496–16. doi:10.1128/AAC.02496-16
16. Andes DR, Safdar N, Baddley JW, et al. Impact of treatment strategy on outcomes in patients with candidemia and other forms of invasive candidiasis: a patient-level quantitative review of randomized trials. Clin Infect Dis. 2012;54(8):1110–1122. doi:10.1093/cid/cis021
17. Chandrasekar P, Sirohi B, Seibel NL, et al. Efficacy of micafungin for the treatment of invasive candidiasis and candidaemia in patients with neutropenia. Mycoses. 2018;61(5):331–336. doi:10.1111/myc.12748
18. Ko J-H, Jung DS, Lee JY, et al. Poor prognosis of Candida tropicalis among non-albicans candidemia: a retrospective multicenter cohort study, Korea. Diagn Microbiol Infect Dis. 2019;95(2):195–200. doi:10.1016/j.diagmicrobio.2019.05.017
19. Lortholary O, Renaudat C, Sitbon K, et al. The risk and clinical outcome of candidemia depending on underlying malignancy. Intensive Care Med. 2017;43(5):652–662. doi:10.1007/s00134-017-4743-y
20. Arias S, Denis O, Montesinos I, et al. Epidemiology and mortality of candidemia both related and unrelated to the central venous catheter: a retrospective cohort study. Eur J Clin Microbiol Infect Dis. 2017;36(3):501–507. doi:10.1007/s10096-016-2825-3
21. Liu CY, Huang LJ, Wang WS, et al. Candidemia in cancer patients: impact of early removal of non-tunneled central venous catheters on outcome. J Infect. 2009;58(2):154–160. doi:10.1016/j.jinf.2008.12.008
22. Rodriguez D, Park BJ, Almirante B, et al. Impact of early central venous catheter removal on outcome in patients with candidaemia. Clin Microbiol Infect. 2007;13(8):788–793. doi:10.1111/j.1469-0691.2007.01758.x
23. Chalmers C, Gaur S, Chew J, et al. Epidemiology and management of candidaemia - a retrospective, multicentre study in five hospitals in the UK. Mycoses. 2011;54(6):e795–800. doi:10.1111/j.1439-0507.2011.02027.x
24. Karadag-Oncel E, Kara A, Ozsurekci Y, et al. Candidaemia in a paediatric centre and importance of central venous catheter removal. Mycoses. 2015;58(3):140–148. doi:10.1111/myc.12288
25. Tadec L, Talarmin JP, Gastinne T, et al. Epidemiology, risk factor, species distribution, antifungal resistance and outcome of Candidemia at a single French hospital: a 7-year study. Mycoses. 2016;59(5):296–303. doi:10.1111/myc.12470
26. Fan X, Xiao M, Liao K, et al. Notable increasing trend in azole non-susceptible Candida tropicalis causing invasive candidiasis in China (august 2009 to july 2014): molecular epidemiology and clinical azole consumption. Front Microbiol. 2017;8:464. doi:10.3389/fmicb.2017.00464
27. Garnacho-Montero J, Diaz-Martin A, Garcia-Cabrera E, et al. Risk factors for fluconazole-resistant candidemia. Antimicrob Agents Chemother. 2010;54(8):3149–3154. doi:10.1128/AAC.00479-10
28. Goldani LZ, Mário PS. Candida tropicalis fungemia in a tertiary care hospital. J Infect. 2003;46(3):155–160. doi:10.1053/jinf.2002.1067
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.