Back to Journals » International Journal of Women's Health » Volume 17
Eating Amidst Concerns: A Qualitative Study on the Experiences of Disordered Eating in Women with Gestational Diabetes Mellitus
Authors Sun D, Weng X ![]() , Xu J, Luo D
, Xu J, Luo D
Received 9 August 2025
Accepted for publication 17 October 2025
Published 30 October 2025 Volume 2025:17 Pages 4019—4032
DOI https://doi.org/10.2147/IJWH.S559665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Dandan Sun,1,* Xinyi Weng,2,* Jingjing Xu,3,4 Dan Luo2
1Department of Obstetrics, the First Affiliated Hospital with Nanjing Medical University, Nanjing, People’s Republic of China; 2School of Nursing, Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China; 3Department of Nursing, the First Affiliated Hospital with Nanjing Medical University, Nanjing, People’s Republic of China; 4School of Public Health, Nanjing Medical University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dan Luo, School of Nursing, Nanjing University of Chinese Medicine, No. 138 Xianlin Dadao, Qixia District, Nanjing City, Jiangsu Province, 210023, People’s Republic of China, Tel +8615720800662, Email [email protected]
Purpose: Women with gestational diabetes mellitus (GDM) may experience disordered eating (DE), leading to adverse pregnancy outcomes and compromised mental health. However, in-depth studies in this field are lacking. This study explored the DE experiences among women with GDM, focusing on behavioral characteristics and potential risk factors.
Patients and Methods: This study was a descriptive qualitative study. Using purposive sampling, 23 pregnant women with GDM who had exhibited DE behaviors within the past month were recruited from a maternal and child health hospital in Nanjing, China. Semi-structured interviews were conducted with the participants. Data were analyzed using conventional content analysis.
Results: Three categories of DE experiences among women with GDM were identified: (1) behavioral characteristics; (2) internal drivers; (3) external enablers. DE behaviors in women with GDM primarily included restrictive eating, binge eating, and inappropriate insulin use. These behaviors often formed a vicious cycle: initial excessive restrictive eating led to binge eating due to intense hunger and food cravings, which in turn caused elevated glycemia and prompted impromptu restrictive eating, restarting the cycle. Inappropriate insulin use aimed at maintaining glycemic stability further perpetuated DE. Additionally, the study identified three internal drivers and three external enablers. Excessive risk perception mainly drove restrictive eating, insufficient internal motivation triggered binge eating, and low self-efficacy exacerbated both. Perceived pressure from dietary norms was a key external risk factor for the development of restrictive eating. Permissive messages from family members and disruptions from unexpected social events induced binge eating.
Conclusion: Internal and external factors led to a restrictive-binge eating cycle in women with GDM, sustained by inappropriate insulin use. Excessive risk perception about hyperglycemia and fetal health existed as unique risk factors. Future studies should be conducted across diverse cultural and geographical contexts to enhance the generalizability of our findings.
Keywords: pregnant women, perinatal mental health, dietary management, risk factors
Introduction
Gestational diabetes mellitus (GDM) refers to the first manifestation of glucose intolerance during pregnancy.1 As one of the most common pregnancy complications, GDM affects approximately one in seven women worldwide.1 Evidence confirms that dietary management, being fundamental to GDM treatment, can effectively achieve glycemic control and improve pregnancy outcomes when properly implemented.2 However, in real-world settings, translating complex dietary guidelines into daily practice poses a significant challenge for women with GDM. This population continues to exhibit suboptimal dietary adherence, inadequate micronutrient intake, and excessive sugar consumption, with limited improvement even after receiving medical nutrition therapy.3–5 Women with GDM report that the highly medicalized dietary management may provoke negative pregnancy experiences, which in turn can trigger disordered eating (DE).6
As defined by the National Eating Disorders Collaboration, DE represents a subthreshold condition between normal eating and eating disorders (EDs), characterized by less frequent and severe restrictive eating, binge eating, and compensatory behaviors (such as use of diuretics, laxatives, or self-induced vomiting).7 By simultaneously embodying the dual identities of both pregnant women and people with diabetes, women with GDM may constitute a group at higher risk for DE. Specifically, most women with GDM present with high BMI and excessive gestational weight gain,8 factors known to increase susceptibility to DE during pregnancy.9 Beyond demographic risks, this population frequently faces more psychosocial challenges, including insufficient social support, anxiety, depression, and difficulties in adapting to the maternal role.10 Multiple studies have confirmed that these psychosocial factors are well-established contributors to the development of DE.11,12 Moreover, the disease-specific management burden introduces additional DE triggers for women with GDM. Key diabetes-related factors - such as strict dietary regimens, insulin therapy, and elevated glycated hemoglobin levels - have been empirically shown to promote the emergence or exacerbation of DE behaviors.13,14 Currently, a multicenter cohort study has provided epidemiological data on DE in women with GDM, in which binge eating was the most common DE behavior, with a prevalence as high as 31.6%, while restrictive eating (3.7%) and compensatory behaviors (0.8%) were less prevalent.15 This DE pattern not only leads to fluctuations in glycemia,16 weight,15 and emotions6 during pregnancy, but may also cause adverse pregnancy outcomes, such as small- or large-for-gestational-age infants.15
Nevertheless, quantitative research on DE among women with GDM remains scarce. Several qualitative studies on the dietary experiences of women with GDM have touched upon DE in this population. Benton et al6 noted that women with GDM exhibit distinct DE-related cognitions. Unlike the DE cognitive focus on food, body shape, and weight commonly seen in general pregnant women9 and people with diabetes,17 women with GDM appear to shift their attention towards glycemic control, fetal health, and reproductive choices.6 Some other studies have mentioned that a subset of women with GDM reported adopting highly restrictive dietary strategies (such as severe carbohydrate avoidance or prolonged fasting) due to fears of hyperglycemia, insulin use, or postpartum complications.16,18 Other women with GDM may exhibit rebellious attitudes toward dietary management, engaging in binge eating followed by secretive compensatory behaviors or falsified glycemia records.19,20 A qualitative study of Aboriginal Canadians has also reported that over half of women with GDM experienced overeating episodes, with two resorting to extreme binge eating and self-induced vomiting.21 However, no qualitative study has comprehensively explored the behavioral spectrum of DE in women with GDM, and the interrelationships between these behaviors remain unclear. Moreover, to our knowledge, only one quantitative study has explored demographic risk factors for binge eating in women with GDM, such as young age, low level of education, and pre-pregnancy BMI < 25 kg/m2.15 The psychosocial factors associated with DE in this population also remain poorly understood.
Therefore, this study aims to conduct a qualitative study to explore the behavioral characteristics and risk factors of DE in women with GDM. This will help bridge existing knowledge gaps and raise awareness among healthcare professionals.
Material and Methods
Study Design
This study employed a descriptive qualitative approach, grounded in the general principles of naturalistic inquiry.22 By emphasizing direct description (low-inference interpretation) of phenomena within their natural context,23 this methodology is appropriate for capturing the authentic and objective DE experiences of women with GDM. The consolidated criteria for reporting qualitative research checklist (COREQ) was adhered to for accurate reporting.24
Participants
Purposive sampling was used to recruit women with GDM from the departments of obstetrics and nutrition at a major maternal and child health hospital in Nanjing, China, seeking maximum variation in age, gestational weeks, and parity. Recruitment was conducted by DDS. Inclusion criteria were: (1) age 18–50 years; (2) diagnosed with GDM25 for more than one month during the current pregnancy; (3) presence of any DE behaviors within the past month, encompassing restrictive eating, binge eating, and compensatory behaviors. Exclusion criteria included pre-existing type 1/2 diabetes, psychiatric disorders (including EDs), or other pregnancy complications requiring dietary control.
Previous practice has successfully utilized structured clinical interview-related questions for the Diagnostic and Statistical Manual of Mental Disorders (DSM) in identifying specific DE behaviors among women with GDM.15 Building upon this, the present study established operational definitions and identification criteria for three primary DE behaviors in this population by referencing the DSM-526 and Chinese GDM guidelines.27 Restrictive eating was operationalized as excessive restriction of energy, nutrients, or eating frequency for non-medical purposes. Binge eating referred to consuming large amounts of food in a discrete period with a sense of loss of control, echoing prior research.15 Compensatory behaviors were considered strategies aimed at offsetting excessive food intake like self-induced vomiting and excessive exercise. All behaviors required a minimum frequency of once weekly over the past month, with detailed criteria provided in Table S1. Researchers explained these criteria to participants, with self-reported adherence to any of the three DE behavior criteria being considered potential candidates. Subsequently, the mapping questions from the NEDC-recommended pregnancy-adapted SCOFF questionnaire (Table S2)28 were used as an auxiliary, with scores ≥2 indicating high risk for DE. Ultimately, only participants who met both the self-developed identification criteria and the SCOFF high-risk threshold were deemed eligible.
Of the 30 eligible women with GDM contacted, three discontinued due to examination interruptions, four expressed no interest, and ultimately, 23 women with GDM completed the interviews.
Data Collection
Through a comprehensive literature review, XYW developed a semi-structured interview guide, which was reviewed by a maternal mental health specialist (DDS) and a qualitative study expert (DL). To further validate the guide’s applicability, pilot interviews were conducted with two women with GDM. Based on participant feedback, the term “disordered eating” was replaced with “unhealthy eating behaviors” to avoid unfamiliarity. The final guide covered three topics: (1) disease feelings; (2) dietary changes; and (3) DE experiences (Box 1).
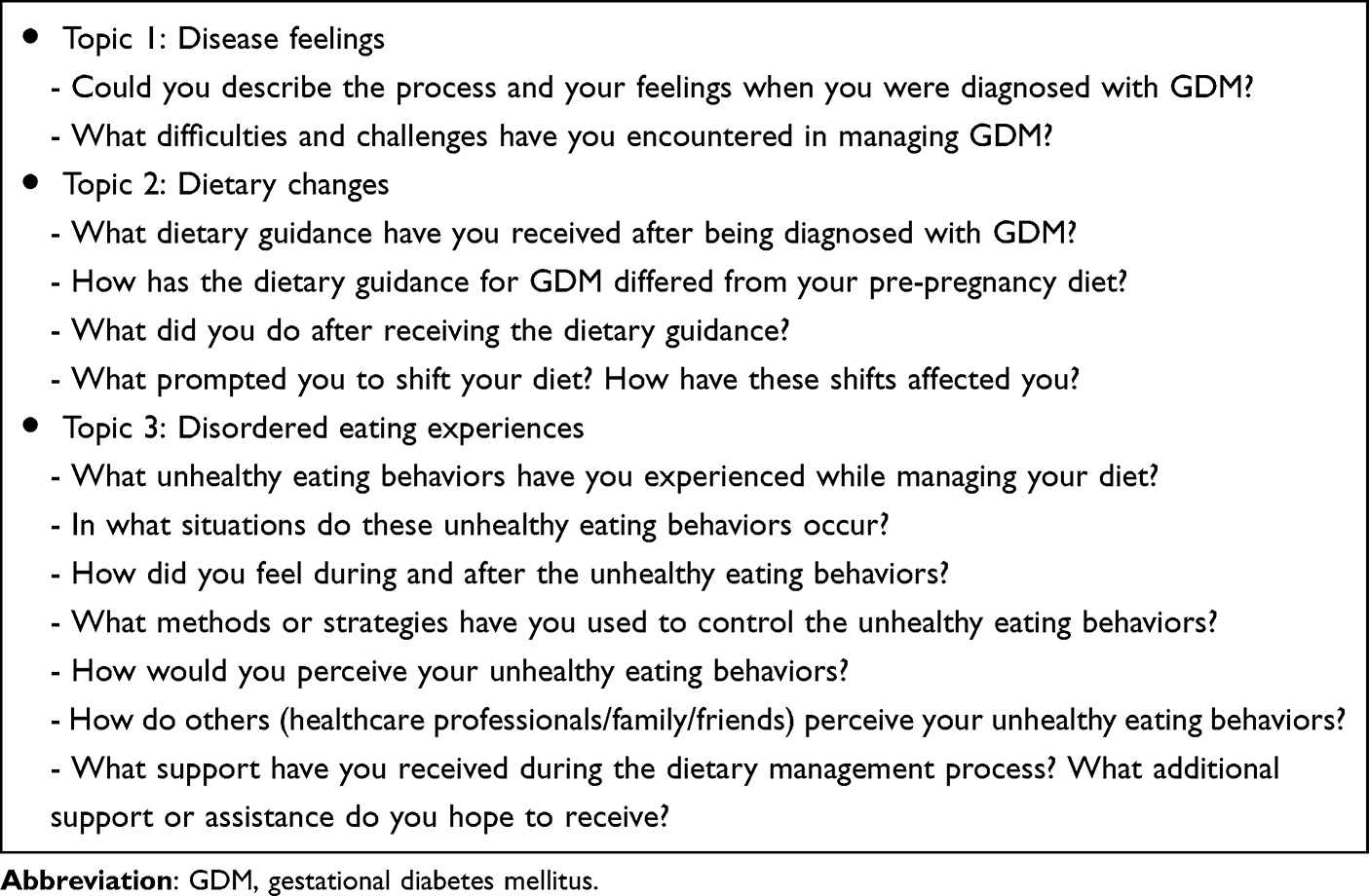 |
Box 1 Interview Guide |
The interviews were hosted by DDS and XYW. Before starting, XYW explained the study’s purpose, data management, confidentiality, and anonymity, and promised participants that they could withdraw consent at any time without consequence. The interviews were held in pre-reserved private rooms within the obstetrics outpatient department (n = 9) or the ward (n = 14) to ensure quiet and security. Participants were first invited to describe the process and feelings of being diagnosed with GDM to build rapport. Subsequent questions evolved naturally based on participants’ narratives, with probing for clarification when needed. For instance, a multiparous woman with a history of GDM maintained a normal diet during her previous pregnancy but began to binge during this pregnancy. DDS then asked further: “Please share more about your experiences of adopting different eating behaviors in the two pregnancies”. Demographic information was collected by XYW at the interview’s conclusion. All interviews were audio-recorded, with each session lasting 20 to 60 minutes. DDS transcribed these recordings verbatim into Mandarin within 24 hours. After interviewing 21 women with GDM, no new codes or categories emerged, as subsequent responses only repeated prior data, confirming code saturation. Following two additional interviews, the research team reviewed and found that the identified categories had been sufficiently elaborated, with no new insights emerging, thus confirming meaning saturation. The saturation grid is shown in Table S3.
Data Analysis
Data analysis commenced following the first interview and proceeded in tandem with data collection using NVivo 11.0. Two researchers (DDS and XYW) performed conventional content analysis29 in Chinese. During preparation, each transcribed interview was considered a unit of analysis and read repeatedly and carefully for overall impression. In organization, both researchers highlighted the words, sentences, and paragraphs that mapped DE as meaning units, respectively, and then condensed and coded them. Comparisons were made after coding was completed. Afterwards, the coding was iteratively compared and assigned to more abstract subcategories and higher-order categories. The final categorization results were confirmed through collective discussion by the research team. For accurate dissemination, representative Chinese quotes were translated into English by one bilingual translator (XYW), then back-translated into Chinese by another bilingual translator (DDS). Both carefully compared the two versions of the Chinese quotes to avoid translation errors. For quotes rich in metaphorical expressions, XYW independently translated them into English and presented the contextual connotations of the quote in a collective meeting. Two researchers with cross-cultural backgrounds (JJX and DL) were then introduced to adjudicate on the English versions of the metaphors, aiming to ensure a faithful representation of the meaning, context, and cultural specificities inherent in the original data.30
Reflexivity Statement
The research team consisted of four female researchers dedicated to the psychological health of high-risk pregnant women in the perinatal period. The first author (DDS) is an expert with 15 years of experience in maternal mental health nursing, possessing extensive expertise in GDM care. As a mother of two, her personal pregnancy experiences helped build rapport with participants, encouraging them to share sensitive information about DE. However, having never experienced GDM herself, she remained aware of the differences between general pregnancy experiences and the specific challenges of GDM. The second author (XYW) is a graduate student specializing in diabetes-related DE, possessing a solid theoretical foundation in DE research. Being unmarried, nulliparous, and likely younger than most participants, she adopted a learner-oriented stance during interviews to understand DE behaviors objectively. The third author (JJX) is the Director of Nursing at the study hospital. The fourth author (DL) has a PhD in Nursing and focuses on obstetrical nursing research and teaching at a university.
The study was led by DDS and XYW, with JJX and DL serving as consultants. Based on literature review and clinical experience, the research team hypothesized that strict GDM management might trigger negative emotions and subsequent DE behaviors. DDS, responsible for subject recruitment, had no direct clinical care relationship with them. XYW, a non-clinical researcher, had no prior contact with participants. Interviews followed naturalistic principles: no interviewer manipulation and no a priori outcomes.31 Researchers bracketed assumptions, used techniques like clarification and summarization to minimize bias. XYW documented field notes and reflections on participants, which were used in collective meetings to refine category development.
Rigor
Lincoln and Guba’s criteria were applied to ensure trustworthiness.32 Codes were compared with raw data and shared with participants for reflection. Participants of different gestational weeks, parity, and glycemic control methods (data-source triangulation), along with the research team (researcher triangulation),33 reviewed the data to enhance the credibility. Furthermore, peer check was conducted throughout the data analysis process, and an out-of-field researcher was involved for external validation to ensure confirmability and dependability. Regarding transferability, the context of the study and direct quotes from the participants were described thoroughly.
Results
The study included 23 women with GDM (Table 1). Most participants were primiparous, had junior college education or higher, without diabetes family history or prior GDM diagnosis. Data analysis revealed three categories and nine subcategories of DE experience in women with GDM (Figure 1), with typical quotes displayed in detail (Table 2).
 |
Table 1 The Characteristics of the Participants |
 |
Table 2 Categories and Subcategories Associated with the Experience of Disordered Eating in Pregnant Women with Gestational Diabetes Mellitus |
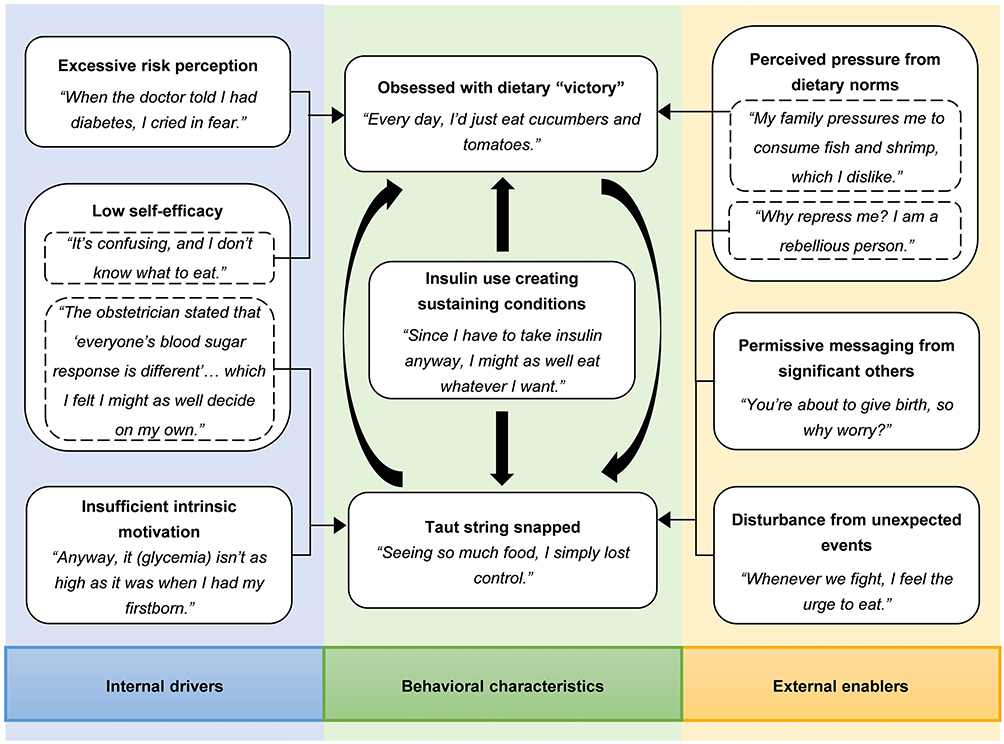 |
Figure 1 A map of disordered eating experiences in women with gestational diabetes mellitus. |
Behavioral Characteristics
This category described three DE behavioral characteristics in women with GDM. “Obsessed with dietary ‘victory’” reflected extreme sugar and carbohydrate restriction. “Taut string snapped” depicted binge eating and then compensated by impromptu dieting or excessive exercise. “Insulin use creating sustaining conditions” highlighted the role of inappropriate insulin use in maintaining restrictive eating and binge eating.
Obsessed with Dietary “Victory”
The determination to manage the diet began almost simultaneously with the abnormal oral glucose tolerance test (OGTT) results; however, the approach went to extremes to achieve victory in the diet. Initially, low-sugar vegetables were chosen as the food of choice,
Every day, I’d just eat cucumbers and tomatoes; that’s all I had (Participant 7).
Extreme “veggie patterns” usually gave way to more sustainable low-sugar and low-carb diets within a week, although this still fell significantly short of the nutritional requirements for pregnant women. Alternatively, this conservative approach was chosen from the outset. Participant 2 described her typical diet,I only eat two meals a day. I eat very little now… I eat salad bowls from the grocery store that are 348 calories each, with my sugar-free dressing, and only eat those two meals, nothing more.
This pattern of enduring hunger was perceived by participants as being associated with subsequent maternal-fetal health issues, exemplified by Participant 8’s “blood sugar level once of 2.6” and Participant 11’s fetal condition of “small size”.
Taut String Snapped
When restrictive eating exceeded tolerable limits, the dietary management of women with GDM began to go unchecked. Participant 1 stated,
A string always snaps when it’s taut for too long. I can’t take it anymore.
Despite distraction attempts, binge urges persisted,I try to keep busy, but I still crave bread desperately. I always feel like something is missing (Participant 17).
At this point, satisfying appetite took precedence over glycemic management. Participant 13 confessed,After learning to control my sugar intake, I craved sweets for days. Yesterday, I devoured a whole six-inch cream cake in half an hour!
As the pregnancy progressed, women reported that cravings intensified, making the period near childbirth a high-risk time for binge eating. Some participants hoped their baby would be born early to end their feeling of loss of control.Subsequently, participants reported negative emotions such as guilt and regret following binge eating, as well as alleviating elevated glycemia and bloating discomfort through diverse compensatory behaviors. Participant 1 shared her experience of exercising after binge eating during her second trimester,
I found an online prenatal workout, did it, and checked my blood sugar hourly until it decreased.
Additionally, dietary adjustments were common, typically manifesting as impromptu dieting. Participant 19 consumed only two cherry tomatoes for the rest of the day after her “overindulgence” at lunch.Insulin Use Creating Sustaining Conditions
Insulin therapy became the necessary intervention for women with GDM who had uncontrolled glycemia. Nevertheless, when DE was already present, insulin’s efficacy in stabilizing glycemia may create conditions that sustain such behaviors. Participant 2 refused to increase food intake despite hypoglycemia, instead discontinuing insulin independently. Participant 10, hospitalized for insulin treatment, abandoned her vegan diet and rationalized binge eating with,
Since I have to take insulin anyway, I might as well eat whatever I want. Now, I’m going to give up on myself.
Unexpectedly, among those not using insulin, Participant 14 proactively expressed a desire to initiate insulin therapy to maintain her current fruit addiction,
Can I just use insulin? I want to eat, and I really love fruit. Before I was pregnant, I had to eat fruit every night. If I don’t eat it, I feel bad, kind of down.
Internal Drivers
From the perspective of women with GDM, three personal DE risk factors emerged: “excessive risk perception” fostered restrictive eating, “insufficient intrinsic motivation” predominantly caused binge eating, and “low self-efficacy” potentially induced both DE behaviors.
Excessive Risk Perception
Irrational perception of GDM fueled DE, with glycemic control being a primary concern. Some women were devastated by their OGTT results, “When the doctor told me I had diabetes, I cried in fear. I could no longer dare to eat what I liked” (Participant 8). Daily glycemia monitoring further exacerbated these fears, with cases like Participant 14 fasting all day after post-breakfast hyperglycemia (9.2 mmol/L) and Participant 12 who “barely ate rice” due to “constant anxiety about high blood sugar.” Insulin avoidance also motivated restrictive behaviors, with Participant 23 dieting to avoid potential “pain and hassle”. Additional triggers included pregnancy outcome worries and weight gain concerns, expressed as “eating less to gain less” (Participant 7).
In addition to the challenges faced by women with GDM themselves, concerns about fetal growth and prognosis also occupied a prominent place, such as concerns about macrosomia. Participant 2 acknowledged restrictive eating for fetal weight,
Even with the salad, my baby is still much bigger than the last checkup. I’m worried that if I eat more, he’ll be bigger.
Other reasons for excessive restrictive eating stemmed from worries about the child’s future metabolic disease, obesity, and mental deficiency.Insufficient Intrinsic Motivation
Strict GDM diets proved challenging for women with intense food cravings, despite understanding the guidelines. As Participant 19 stated,
I’m clear on how to eat to keep my blood sugar normal, but I’ve always been very fanatical about food. Sometimes I just want to indulge.
On the other hand, women with GDM following regulated diets felt “starving all day long” and developed thoughts likeThe blander the food I eat, the more nauseous I’ll get (Participant 4).
Once this physical response became unbearable, they were unwilling to stick to dietary rules, as Participant 18 explained,I was so hungry that I just binged.
Successful pregnancy experiences also undermined intrinsic motivation. Participants with a history of GDM and favorable perinatal outcomes were less concerned about current hyperglycemia, as Participant 5 said,
I can’t control my mouth. I think, anyway, it (glycemia) isn’t as high as it was when I had my firstborn.
Primiparous women, like Participant 15, might be influenced by others’ success stories and develop a false sense of security thatEverything will be fine after delivery.
Low Self-Efficacy
Women with GDM struggled to balance glycemic control with fetal nutrition, experiencing frustration when regular diets failed to yield predictable results. Participant 9 lamented,
Even drinking water doesn’t control my blood sugar,
while Participant 12 described confusion over food choices:I usually eat mixed grains or quinoa with rice, but I feel like my sugar rises faster when I eat mixed grains instead. I don’t know if it’s because black rice, oats, and other stuff are in there. It’s confusing, and I don’t know what to eat.
Additionally, inconsistent advice from healthcare professionals further confused women with GDM and eroded their confidence in dietary management. Participant 16 linked her binge eating to dissatisfaction with conflicting glycemic control recommendations,
The outpatient doctor recommended hospitalization, but another physician said I could adjust my insulin dosage at home. Later, when I visited this hospital, the obstetrician stated that ‘everyone’s blood sugar response is different’ and suggested that my situation be discussed with an endocrinologist.
External Enablers
This category identified three subcategories of external risk factors that exacerbate DE: “perceived pressure from dietary norms” primarily drove restrictive eating (though occasionally triggered bingeing), while “permissive messaging from significant others” and “disturbance from unexpected events” emerged as predominant binge-eating triggers.
Perceived Pressure from Dietary Norms
The management of GDM often involves both family members and the healthcare system. While essential, this external support could sometimes be perceived as controlling by the pregnant women. For instance, when families overlooked the women’s own dietary preferences, it could exacerbate psychological distress and increase the risk of DE. Participant 10 described how being pressured to eat disliked foods intensified her restrictive eating,
My family pressures me to consume fish and shrimp, which I dislike. This has caused significant conflict, as they believe I’m shortchanging the baby.
Conversely, Participant 20 admitted her spouse’s strict dietary supervision had the opposite effect, contributing to her binge eating in private,My husband cares about me, but he’s too strict. Why repress me? I am a rebellious person.
In addition, some women with GDM felt pressured by healthcare professionals to demonstrate excellent glycemic control. Participant 23 intentionally restricted her food intake before appointments to avoid blame from her nutritionist,
Before each appointment, I reduce my food intake for a few days in advance due to anxiety about possible hospitalization for high blood sugar.
Permissive Messaging from Significant Others
Not all DE happened automatically, and women with GDM often faced challenges related to it. However, family support occasionally rationalized or inadvertently reinforced such behaviors, particularly as childbirth approached. Participant 5 recalled being reassured by relatives after an episode of binge eating,
A few nights ago, I ate almost out of control. But my relatives were all telling me, ‘It’s okay, you’re about to give birth, so why worry?’
Moreover, some participants’ spouses appeared to acquiesce to the onset of DE, prioritizing emotional well-being. Participant 14 explained,Ever since we got married, I’ve been particularly fond of fruits, and I have to eat them every night or else I’ll be sad. My husband knows me well, so he doesn’t bother me about it. Like yesterday, I even ate durian.
Disturbance from Unexpected Events
Some women described turning to DE behaviors as a way to manage unexpected stressful events. Participant 3 reported habitually indulging in “McDonald’s and coffee” during periods of work-related stress. Participant 18, whose episodes were characterized by binge eating following marital conflicts, stated,
Whenever we fight, I feel the urge to eat. Once, after an argument, I drove out to a hot pot buffet.
Surprisingly, DE behaviors were also reported in specific social or cultural contexts, such as the celebration of traditional festivals. As Participant 21 recounted,
During the Mid-Autumn Festival, everyone was eating mooncakes. I couldn’t help myself and ate five consecutively.
Similar episodes occurred at social gatherings,Recently, a friend got married. Normally, I would never dare to eat them. But we were eating at the restaurant, and that table of food looked all incredibly tempting. It’s unreasonable not to eat. (Participant 15)
Discussion
The study specifically explores the experiences of DE among women with GDM. Compared with prior research that only sporadically mentioned DE within the broader context of dietary experiences, this study systematically describes the behavioral characteristics and risk factors of DE in women with GDM, constructing an explicit DE framework. Restrictive eating (Obsessed with dietary “victory”) and binge eating (Taut string snapped) served as the prominent behavioral characteristics that hinder self-management in women with GDM. Inappropriate insulin use (Insulin use creating sustaining conditions) emerged as a novel category in this study, playing a unique role in maintaining these extreme dietary patterns. Meanwhile, by establishing a typology of internal and external risk factors, this study identified multi-source risks (spanning individual, family, medical, and societal) and demonstrated how DE performs differently across various risk contexts. These insights may raise awareness among obstetric healthcare professionals and nutritionists about this overlooked DE population, while providing new perspectives for improving dietary self-management and maternal mental health.
Restrictive eating became the initial form of DE in most women with GDM, primarily driven by excessive risk perception regarding glycemia. This aligned with previous qualitative studies reporting behaviors such as meal-skipping, carbohydrate avoidance, and exclusive water intake to manage extreme hyperglycemia anxiety in women with GDM.18,19,34 Distinctively, concerns about fetal health became a specific risk factor for restrictive eating in women with GDM, unlike in general individuals with diabetes, where body dissatisfaction was more prevalent.17 This may be attributed to the potential adverse outcomes of GDM, such as macrosomia, neonatal hypoglycemia, and respiratory distress,35 leading our sample to prioritize fetal health over appearance. Nevertheless, prolonged restrictive eating may lead to maternal malnutrition. Deficiencies in critical micronutrients like folate, iron, and zinc may have lasting effects on the offspring’s body composition and brain function.36 Hence, for individuals overly focused on glycemic control, continuous glucose monitoring systems may be considered to reduce glycemic fluctuations effectively.37 Simultaneously, virtual reality simulations of fetal development during prenatal visits could help alleviate anxiety related to fetal health.38 Additionally, perceived pressure to comply with dietary norms is a key external factor driving restrictive eating, a finding similar to that of Neumark-Sztainer reported in adolescents.39 In China, the ideas of filial piety and responsibility emphasized by traditional Confucianism have a profound influence.40 Under this culture, a pregnant woman’s bearing of a healthy child is regarded as a priority that impacts the well-being of the entire family.41 Consequently, when families assist with dietary management for GDM, they may overlook the woman’s own food preferences, thereby exacerbating her psychological distress and increasing the risk of DE. This underscores the importance of obstetricians and midwives collaborating with both patients and their families to develop personalized dietary plans, rather than focusing solely on emphasizing prohibited foods. Also, family members should shift from verbal supervision to practical nudging strategies, such as modifying meal sequencing and using quantified trays,42 to facilitate sustainable dietary management in home settings.
From participants’ narratives, extremely restrictive eating proved unsustainable over time, eventually leading to a vicious restrictive-binge eating cycle. This reflected the “abstinence violation effect” in DE,43 where even minor deviations from restrictions lead to perceived failure and subsequent binge eating. Among these women with GDM, poor glycemic control despite restrictive dieting led to low self-efficacy, which in turn triggered binge eating. Emerging digital health solutions, particularly artificial intelligence-based nutrition guidance systems,44 can support informed dietary decision-making while enhancing self-management achievement in this population. Notably, inconsistent dietary management advice from healthcare professionals was also identified as a significant contributor to low self-efficacy, echoing previous findings.45 Within the current Chinese healthcare system, although the density of maternal and child health workers far exceeds internationally recommended standards, their professional education levels remain uneven.46 This is particularly evident in primary care institutions, where only 1% of personnel hold a bachelor’s degree or higher.46 A separate survey involving healthcare providers from 68 Chinese obstetric and gynecological hospitals revealed that the overall awareness rate of GDM remains below 60%.47 This highlights the urgency of establishing a standardized GDM training system and improving continuous treatment/care procedures. Interestingly, this study also found that some participants experienced binge eating without actual energy deficiency, with insufficient intrinsic motivation being the main internal driving factor. According to Colton’s research, lower health motivation significantly mediated the link between rapid appetite gratification and binge eating.48 For these cases, using ecological momentary assessment49 to monitor the recurrence of binge eating and combining it with regular motivational interviewing50 to assist in transforming an ambivalent mindset towards eating may represent a promising intervention approach.
No typical compensatory behaviors, such as self-induced vomiting or laxative use, were observed in this study - a finding consistent with previous reports of their low prevalence in GDM populations.15 However, several population-based differences in compensatory behaviors were identified. Specifically, women with GDM reported employing mild over-exercise, avoiding glycemic testing, and impromptu dieting as coping strategies after binge episodes. Although these behaviors have been documented in DE among other diabetes populations,51 the primary motivation in our sample was glycemic control rather than weight reduction. Of particular concern, insulin-treated women reported self-adjusting their insulin dosage to compensate for glycemic fluctuations following binge eating. Reliance on such inappropriate insulin use to maintain glycemic stability may foster conditions that perpetuate DE. This means that, among those who intend to binge eat, insulin might be overused. This practice stands in stark contrast to the insulin restriction commonly adopted by individuals with type 1 diabetes and comorbid DE for the purpose of purging calories.52 These nuances complicate the identification of DE in women with GDM by healthcare professionals. Developing a specific tool is warranted, as existing generic tools have shown limited applicability for pregnant women,53 and no instrument covers glycemia, insulin, and fetal-related factors.
Limitations
Several limitations must be acknowledged. First, the sample was composed solely of Asian women recruited from a single well-known maternal and child health hospital in China. Although the institution serves a national population, this ethnic and institutional homogeneity may limit the generalizability of the findings to other cultural contexts or healthcare settings, such as community hospitals. Future research conducted across diverse geographic and ethnic backgrounds is needed to validate and extend these results. Second, participant screening relied on self-developed criteria for identifying DE behaviors, supplemented by the NEDC-recommended pregnancy-adapted SCOFF questionnaire. However, DE in women with GDM often involves unique factors, such as concerns about glycemic control and fetal health.6 Consequently, some high-risk individuals who conceal their DE behaviors may have been missed. This emphasizes the significance of developing reliable screening tools for DE in women with GDM. Lastly, the cross-sectional design limited our ability to examine the postpartum persistence of GDM effects. Future longitudinal studies are needed to elucidate the long-term impact of GDM on DE.
Conclusion
As a preliminary qualitative inquiry, this study explored the experiences of DE in women with GDM, identifying three core behavioral characteristics of DE and six categories of risk factors. The findings indicate that restrictive eating and binge eating represent significant yet underrecognized challenges in GDM dietary management, while insulin therapy may create unexpected conditions that perpetuate these DE behaviors. Additionally, concerns about glycemic control and fetal health are unique risk factors for DE in this population. Although these insights enhance healthcare professionals’ and researchers’ comprehension of DE in women with GDM, they are constrained by the study’s qualitative design and homogeneous sample. Further research should seek validation in larger, geographically diverse populations to improve generalizability.
Data Sharing Statement
Due to ethical constraints, participants’ raw data will not be shared. The processed data supporting this study’s findings are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Nanjing University of Chinese Medicine (January 15, 2025/2025NZY-2-01). Written informed consent was obtained from all participants, which included permission for the publication of anonymized responses and direct quotes.
Acknowledgments
Sincere thanks to all the participants who took part in the interviews.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (grant number 72204125); the Philosophy and Social Sciences Project of Nanjing University of Chinese Medicine (grant number 24XRC001); the Postgraduate Research & Practice Innovation Program of Jiangsu Province (grant number KYCX25_2383).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sweeting A, Hannah W, Backman H, et al. Epidemiology and management of gestational diabetes. Lancet. 2024;404(10448):175–192. doi:10.1016/S0140-6736(24)00825-0
2. Yamamoto JM, Kellett JE, Balsells M, et al. Gestational diabetes mellitus and diet: a systematic review and meta-analysis of randomized controlled trials examining the impact of modified dietary interventions on maternal glucose control and neonatal birth weight. Diabetes Care. 2018;41(7):1346–1361. doi:10.2337/dc18-0102
3. Sousa AM, Fiuza D, Mikami FC, et al. Evaluation of information retention and adherence to treatment in patients with gestational diabetes mellitus after multidisciplinary group. Rev Assoc Med Bras. 2016;62(3):212–217. doi:10.1590/1806-9282.62.03.212
4. Lawrence RL, Wall CR, Bloomfield FH. Adherence to dietary guidelines among women with and without gestational diabetes: evidence from the growing up in New Zealand study. Nutrients. 2022;14(10):2145. doi:10.3390/nu14102145
5. Krige SM, Booley S, Levitt NS, Chivese T, Murphy K, Harbron J. Dietary intake and beliefs of pregnant women with gestational diabetes in Cape Town, South Africa. Nutrients. 2018;10(9):1183. doi:10.3390/nu10091183
6. Benton M, Silverio SA, Ismail K. “It feels like medically promoted disordered eating”: the psychosocial impact of gestational diabetes mellitus in the perinatal period. PLoS One. 2023;18(7):e0288395. doi:10.1371/journal.pone.0288395
7. Disordered eating & dieting [homepage on the Internet]. Australia: National Eating Disorders Collaboration; 2017. Available from: https://nedc.com.au/eating-disorders/eating-disorders-explained/disordered-eating-and-dieting.
8. Zhang S, Wang J, Xu F, et al. Sex-specific mediating effect of gestational weight gain between pre-pregnancy body mass index and gestational diabetes mellitus. Nutr Diabetes. 2022;12(1):1–8. doi:10.1038/s41387-022-00203-5
9. Gerges S, Obeid S, Hallit S. Pregnancy through the looking-glass: correlates of disordered eating attitudes among a sample of Lebanese pregnant women. BMC Psychiatry. 2023;23(1):699. doi:10.1186/s12888-023-05205-w
10. Craig L, Sims R, Glasziou P, Thomas R. Women’s experiences of a diagnosis of gestational diabetes mellitus: a systematic review. BMC Pregnancy Childbirth. 2020;20(1):76. doi:10.1186/s12884-020-2745-1
11. Baskin R, Meyer D, Galligan R. Psychosocial factors, mental health symptoms, and disordered eating during pregnancy. Int J Eat Disord. 2020;53(6):873–882. doi:10.1002/eat.23264
12. Chan CY, Lee AM, Koh YW, et al. Course, risk factors, and adverse outcomes of disordered eating in pregnancy. Int J Eat Disord. 2019;52(6):652–658. doi:10.1002/eat.23065
13. Rancourt D, Foster N, Bollepalli S, et al. Test of the modified dual pathway model of eating disorders in individuals with type 1 diabetes. Int J Eat Disord. 2019;52(6):630–642. doi:10.1002/eat.23054
14. Propper-Lewinsohn T, Shalitin S, Gillon-Keren M, et al. Glycemic variability and disordered eating among adolescents and young adults with type 1 diabetes: the role of disinhibited eating. Diabetes Technol Ther. 2025;27(2):113–120. doi:10.1089/dia.2024.0267
15. Silvani J, Schmidt MI, Zajdenverg L, Galliano LM, Antunes Nunes MA. Impact of binge eating during pregnancy on gestational weight gain and postpartum weight retention among women with gestational diabetes mellitus: LINDA-Brasil. Int J Eat Disord. 2020;53(11):1818–1825. doi:10.1002/eat.23361
16. Sandsæter HL, Horn J, Rich-Edwards JW, Haugdahl HS. Preeclampsia, gestational diabetes and later risk of cardiovascular disease: women’s experiences and motivation for lifestyle changes explored in focus group interviews. BMC Pregnancy Childbirth. 2019;19(1):448. doi:10.1186/s12884-019-2591-1
17. De Paoli T, Rogers PJ. Disordered eating and insulin restriction in type 1 diabetes: a systematic review and testable model. Eat Disord. 2018;26(4):343–360. doi:10.1080/10640266.2017.1405651
18. Hui AL, Sevenhuysen G, Harvey D, Salamon E. Barriers and coping strategies of women with gestational diabetes to follow dietary advice. Women Birth. 2014;27(4):292–297. doi:10.1016/j.wombi.2014.07.001
19. Neufeld HT. Food perceptions and concerns of aboriginal women coping with gestational diabetes in Winnipeg, Manitoba. J Nutr Educ Behav. 2011;43(6):482–491. doi:10.1016/j.jneb.2011.05.017
20. Draffin CR, Alderdice FA, McCance DR, et al. Exploring the needs, concerns and knowledge of women diagnosed with gestational diabetes: a qualitative study. Midwifery. 2016;40:141–147. doi:10.1016/j.midw.2016.06.019
21. Neufeld HT. Food perceptions and concerns of aboriginal women coping with gestational diabetes in Winnipeg, Manitoba. J Nutr Educ Behav. 2011;43(6):482–491. doi:10.1016/j.jneb.2011.05.017
22. Lincoln YS, Guba EG. Naturalistic Inquiry. California: SAGE Publications Ltd; 1985.
23. Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Health. 2010;33(1):77–84. doi:10.1002/nur.20362
24. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
25. Metzger BE, Gabbe SG, Persson B, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi:10.2337/dc09-1848
26. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
27. Chinese Society of Obstetrics and Gynecology, Obstetrics Subgroup; Chinese Society of Perinatal Medicine; Chinese Maternal and Child Health Association. Diabetes in pregnancy committee. Guidelines for the diagnosis and treatment of hyperglycemia in pregnancy (2022) [part 1]. Chin J Obstet Gynecol. 2022;57(01):3–12. doi:10.3760/cma.j.cn112141-20210917-00528
28. Pregnancy and eating disorders: a professional guide to assessment and referral [homepage on the Internet]. Australia: National Eating Disorders Collaboration; 2017. Available from: https://nedc.com.au/eating-disorder-resources/find-resources.
29. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
30. Larkin PJ, Dierckx de Casterlé B, Schotsmans P. Multilingual translation issues in qualitative research: reflections on a metaphorical process. Qual Health Res. 2007;17(4):468–476. doi:10.1177/1049732307299258
31. McInnes S, Peters K, Bonney A, Halcomb E. An exemplar of naturalistic inquiry in general practice research. Nurse Res. 2017;24(3):36–41. doi:10.7748/nr.2017.e1509
32. Lincoln and Guba’s evaluative criteria [homepage on the Internet]. Princeton: Qualitative Research Guidelines Project; 2006. Available from: http://www.qualres.org/HomeLinc-3684.html.
33. Santos KD, Ribeiro MC, Queiroga DE, et al. The use of multiple triangulations as a validation strategy in a qualitative study. Cien Saude Colet. 2020;25(2):655–664. doi:10.1590/1413-81232020252.12302018
34. Khooshehchin TE, Keshavarz Z, Afrakhteh M, Shakibazadeh E, Faghihzadeh S. Perceived needs in women with gestational diabetes: a qualitative study. Electron Physician. 2016;8(12):3412–3420. doi:10.19082/3412
35. Johns EC, Denison FC, Norman JE, Reynolds RM. Gestational diabetes mellitus: mechanisms, treatment, and complications. Trends Endocrinol Metab. 2018;29(11):743–754. doi:10.1016/j.tem.2018.09.004
36. Young MF, Ramakrishnan U. Maternal undernutrition before and during pregnancy and offspring health and development. Ann Nutr Metab. 2021;1–13. doi:10.1159/000510595
37. Majewska A, Stanirowski PJ, Wielgoś M, Bomba-Opoń D. Efficacy of continuous glucose monitoring on glycaemic control in pregnant women with gestational diabetes mellitus—a systematic review. J Clin Med. 2022;11(10):2932. doi:10.3390/jcm11102932
38. Estrella-Juarez F, Requena-Mullor M, Garcia-Gonzalez J, Lopez-Villen A, Alarcon-Rodriguez R. Effect of virtual reality and music therapy on the physiologic parameters of pregnant women and fetuses and on anxiety levels: a randomized controlled trial. J Midwifery Womens Health. 2023;68(1):35–43. doi:10.1111/jmwh.13413
39. Neumark-Sztainer D, Wall MM, Story M, Perry CL. Correlates of unhealthy weight-control behaviors among adolescents: implications for prevention programs. Health Psychol. 2003;22(1):88–98. doi:10.1037//0278-6133.22.1.88
40. Tang Y. Confucianism, Buddhism, Daoism, Christianity and Chinese Culture. Berlin: Springer; 2015.
41. Luo X, Pan J, Jiang C, Li X, Li P. The influence of Chinese culture and customs on the beliefs and health-related behaviours of Chinese women with gestational diabetes mellitus: a qualitative study. Int J Nurs Pract. 2024;30(1):e13234. doi:10.1111/ijn.13234
42. Park Y, Kim J. Development and effect of child obesity management program by applied nudge. Int J Environ Res Public Health. 2022;19(19):12692. doi:10.3390/ijerph191912692
43. Fairburn CG, Cooper Z, Shafran R. Cognitive behaviour therapy for eating disorders: a “transdiagnostic” theory and treatment. Behav Res Ther. 2003;41(5):509–528. doi:10.1016/s0005-7967(02)00088-8
44. Guan Z, Li H, Liu R, et al. Artificial intelligence in diabetes management: advancements, opportunities, and challenges. Cell Rep Med. 2023;4(10):101213. doi:10.1016/j.xcrm.2023.101213
45. Kokanovic R, Manderson L. Exploring doctor–patient communication in immigrant Australians with type 2 diabetes: a qualitative study. J Gen Intern Med. 2007;22(4):459–463. doi:10.1007/s11606-007-0143-2
46. Zhang H, Liu X, Penn-Kekana L, Ronsmans C. A systematic review of the profile and density of the maternal and child health workforce in China. Hum Resour Health. 2021;19(1):125. doi:10.1186/s12960-021-00662-4
47. Wang L, Wang Y, Chen H, Liu L, Chen X, Gan Q. Knowledge, attitudes and practices towards gestational diabetes mellitus among obstetric and gynaecological healthcare workers: a cross-sectional study of 68 hospitals in Hubei Province, China. BMJ Open. 2025;15(9):e101475. doi:10.1136/bmjopen-2025-101475
48. Colton E, Mahlberg J, Chong TTJ, Verdejo-Garcia A. Food choice motives mediate the relationship between delay discounting and binge eating: a structural equation modelling approach. Appetite. 2025;206:107834. doi:10.1016/j.appet.2024.107834
49. Schaefer LM, Engel SG, Wonderlich SA. Ecological momentary assessment in eating disorders research: recent findings and promising new directions. Curr Opin Psychiatry. 2020;33(6):528–533. doi:10.1097/YCO.0000000000000639
50. Fetahi E, Søgaard AS, Sjögren M. Estimating the effect of motivational interventions in patients with eating disorders: a systematic review and meta-analysis. J Pers Med. 2022;12(4):577. doi:10.3390/jpm12040577
51. De Paoli T, Rogers PJ. Disordered eating and insulin restriction in type 1 diabetes: a systematic review and testable model. Eat Disord. 2018;26(4):343–360. doi:10.1080/10640266.2017.1405651
52. Coleman SE, Caswell N. Diabetes and eating disorders: an exploration of ‘Diabulimia. BMC Psychol. 2020;8(1):101. doi:10.1186/s40359-020-00468-4
53. Stephens J, Ellis A, Roberts S, Gillespie K, Bannatyne A, Branjerdporn G. Disordered eating instruments in the pregnancy cohort: a systematic review update. Eat Disord. 2025;33(4):512–536. doi:10.1080/10640266.2024.2386469
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Toxoplasma gondii Infection and ABO Blood Group Association Among Pregnant Sudanese Women: A Case Study
Magboul AM, Elamin E, Tamomh AG, Mohammed HY, Suliman MA, Ibrahim RM, Hassan IM, Mohammed SM, Albashir AA, Mhmoud MM, Abakar FS, Ahmed RA
International Journal of Women's Health 2023, 15:1375-1381
Published Date: 31 August 2023
HIV Infection Among Pregnant Women in a Vietnamese Population: Prevalence and Associated Factors

Ho HTT, Nguyen TH, Nguyen HH, Nguyen SPH, Nguyen KT
HIV/AIDS - Research and Palliative Care 2025, 17:195-202
Published Date: 11 July 2025