Back to Journals » Cancer Management and Research » Volume 18

Early versus Long-Term Post-Prostatectomy Incontinence Recovery Among Three Robotic-Assisted Radical Prostatectomy Techniques: A Retrospective Cohort Study
Authors Lin SH ![]() , Lin PH, Chao DY, Wu CT, Shao IH
, Lin PH, Chao DY, Wu CT, Shao IH ![]()
Received 23 March 2026
Accepted for publication 12 June 2026
Published 18 June 2026 Volume 2026:18 604780
DOI https://doi.org/10.2147/CMAR.S604780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Shih-Hsuan Lin,1,* Po-Hung Lin,1,2,* Da-Yu Chao,1 Chun-Te Wu,1,3 I-Hung Shao1,2
1Department of Medicine, Chang Gung University, Taoyuan, Taiwan; 2Division of Urology, Department of Surgery, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan; 3Department of Urology, Chang Gung Memorial Hospital, Keelung Branch, Keelung, Taiwan
*These authors contributed equally to this article
Correspondence: I-Hung Shao, Division of Urology, Department of Surgery, Chang Gung Memorial Hospital, Linkou Branch, No. 5, Fusing Street,28 Gueishan District, Taoyuan City, 333, Taiwan, Email [email protected]
Objective: To compare the early and long-term recovery outcomes of post-prostatectomy incontinence (PPI) among patients undergoing Retzius-sparing robotic-assisted laparoscopic prostatectomy (RS-RARP), conventional 2-layer reconstruction, and conventional 3-layer total reconstruction.
Methods: We conducted a retrospective cohort study of 79 patients who underwent RARP by at a single tertiary center. Patients were grouped as RS-RARP (n=19), 2-layer RARP (n=30), and 3-layer RARP (n=30). The primary outcome was PPI recovery, defined as “pad-free”, which was evaluated at immediate, 1, 3, and 6 months after RARP to distinguish between early (immediate/1 month) and long-term (3/6 months) outcomes. Secondary outcomes included cystographic parameters like bladder neck (BN) angle and BN downward distance. Statistical analysis utilized ANOVA and Chi-square tests, with p< 0.05 considered significant.
Results: All three groups achieved excellent long-term continence rates (≥ 96.7% at 6 months, p=0.723). The RS-RARP group demonstrated a borderline statistical advantage of early PPI recovery at the immediate timepoint (89.5% vs. 60.0% in the other two groups, p=0.049). A similar favorable clinical trend was observed at the 1-month follow-up, though the difference did not reach statistical significance (p=0.251). Cystographic analysis revealed a significant difference in mean BN angle (p=0.001): 128.5∘for RS-RARP, 107.7∘for 2-layer RARP, and 120.1∘for 3-layer RARP.
Conclusion: All three RARP techniques yield excellent long-term continence rates. RS-RARP demonstrated a favorable advantage in immediate PPI recovery, which supports the benefit of anterior structure preservation. However, the observed significant anatomical difference in BN angle did not translate into a statistically significant functional difference in long-term PPI recovery, highlighting the multifactorial etiology of continence restoration.
Keywords: robotic assisted radical prostatectomy, RARP, urinary incontinence, post-prostatectomy incontinence, RS-RARP, posterior repair, 3-layer reconstruction
Introduction
Prostate cancer remains a formidable global health challenge, and radical prostatectomy (RP) is the established standard of care for localized disease. The evolution of robotic-assisted laparoscopic prostatectomy (RARP) has refined the surgical approach, offering demonstrable benefits such as reduced blood loss, shorter hospital stays, and accelerated convalescence compared to traditional open surgery. Despite these technical advancements, however, post-prostatectomy incontinence (PPI) persists as a significant complication that substantially compromises a patient’s quality of life (QoL). Although high long-term continence rates are generally achieved, the period of early PPI can be profoundly psychologically distressing for patients. Maximizing the preservation of urinary function remains a critical objective in modern urological surgery.1,2
In pursuit of this functional goal, numerous technical modifications and reconstruction methods have been developed to enhance continence outcomes.3 The Retzius-sparing RARP (RS-RARP) technique, first described by Galfano et al in 2010,4 represents a substantial methodological divergence from the conventional anterior approach. By avoiding dissection of the Retzius space, this technique is specifically designed to preserve the pubovesical complex and other critical anterior anatomical structures that support the bladder neck and urethra. Several studies have reported that RS-RARP is associated with a superior rate of early PPI recovery compared to conventional RARP, with some randomized controlled trials and meta-analyses demonstrating a significant short-term benefit, although long-term outcomes tend to converge.5,6
Conversely, conventional RARP techniques often prioritize meticulous reconstruction of the vesicourethral anastomosis to enhance PPI recovery [R4]. This encompasses sophisticated multi-layer reconstruction approaches aimed at supporting the residual urethral sphincter complex and mitigating anatomical distortion. For instance, conventional RARP with posterior wall repair or 3-layer reconstruction aims to provide robust support and re-establish the normal anatomical relationships of the pelvic floor.7–11 While these reconstruction techniques have proven effective, a direct head-to-head comparison evaluating the RS-RARP technique alongside 2-layer and 3-layer reconstructions within a single institution remains limited. Consequently, how these three distinct anatomical strategies differ in balancing early versus long-term functional recovery within the same clinical setting remains poorly defined.
To address this research gap, we conducted a retrospective cohort study to compare three distinct RARP techniques: RS-RARP, conventional 2-layer RARP (with posterior wall repair), and conventional 3-layer total reconstruction RARP (with posterior and anterior repair) within a single institutional context. The primary objective was to assess differences in PPI recovery rates at multiple post-operative time points and to investigate the role of post-operative cystography parameters, specifically the bladder neck (BN) angle and BN downward distance. These radiographic metrics provide an objective means to evaluate urinary tract restoration, as a wider BN angle reflects a more anatomically stable bladder base to withstand abdominal pressure, while a minimized downward distance indicates superior pelvic floor support.
Materials and Methods
This was a retrospective cohort study of 79 male patients who underwent RARP for localized prostate cancer at a single institution between 2015 and 2021. Prior to surgery, all patients were discussed within our institutional multidisciplinary team. Once RARP was confirmed as the recommended treatment option, patients underwent the procedure following thorough counseling. The specific surgical technique was selected based on the clinical judgment of the attending surgeon in alignment with the patient’s informed preference. The requirement for informed consent was waived by the Institutional Review Board (IRB) due to the retrospective nature of this case study. All surgical procedures were performed by two experienced surgeons (both with more than 200 cases before the cases enrolled in this study) to minimize inter-surgeon variability. Patients were categorized into three groups based on the surgical technique utilized: RS-RARP (n=19), conventional 2-layer RARP (n=30), and conventional 3-layer RARP (n=30).
Patient data were retrospectively collected from electronic medical records. The patient demographics and clinical characteristics were compiled for analysis, such as age, body mass index (BMI), initial PSA (iPSA), biopsy Gleason Score, and clinical T stage. Surgical and cystography parameters including BN sparing status, neurovascular bundle (NVB) preservation, BN angle and downward distance, and the presence of anastomotic leakage were also collected, while the cystographic parameters were measured on post-operative cystograms. Anastomotic leakage on cystography was indicated by contrast medium extravasation at the urethra-bladder neck junction. The BN angle was measured as the angle between the bladder neck and the bilateral bladder margins over the pelvic inlet, while the BN downward distance was defined as the length of the bladder neck below the lower margin of the pelvic inlet.
The primary outcome was PPI recovery, defined as a “pad-free” state (including the use of a pad for prevention only, but not actually needed). PPI recovery was assessed at immediate post-catheter removal and at 1-, 3-, and 6-months post-surgery.
All patients underwent a transperitoneal RARP using a 4-arm da Vinci Surgical System. For the 2-layer and 3-layer RARP groups, the extraperitoneal space was accessed, and the prostate was dissected using a standard anterior approach. Bladder neck sparing was performed whenever feasible. The 2-layer technique included a posterior wall repair with the musculofascial posterior plate, while the 3-layer technique involved additional anterior reconstruction to restore the previously dissected periurethral tissue, pubovesical ligaments, and endopelvic fascia. For the RS-RARP group, the procedure was performed through the posterior approach, without violating the Retzius space, to preserve the anterior anatomical attachments of the bladder neck and urethra. The three surgical techniques were illustrated in Figure 1.
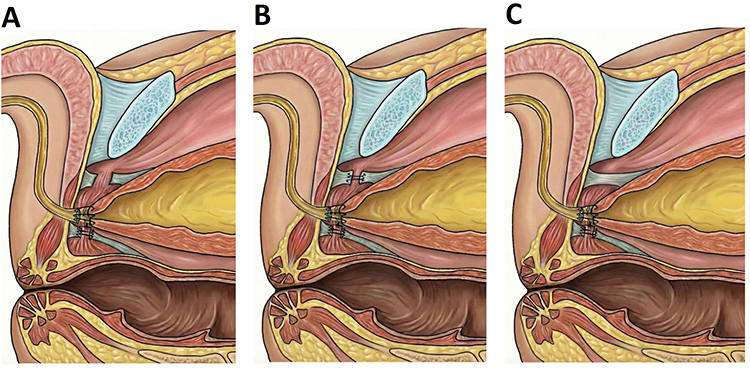 |
Figure 1 Illustration of 3 different surgical techniques. (A) 2-layer RARP, (B) 3-layer RARP, (C) RS-RARP. |
Univariate analysis was conducted to compare continuous and categorical variables among the three surgical groups. One-way ANOVA was used for continuous variables, and the Chi-square or Fisher’s exact test was applied for categorical variables. A p-value of less than 0.05 was considered statistically significant. Given the exploratory nature of this study, p-values were reported without formal adjustment for multiple time-point comparisons. A Bonferroni-corrected threshold of p< 0.0125 (0.05/4 time points) was utilized as a reference for strict statistical significance. Statistical analysis was performed using IBM SPSS version 22 (SPSS Inc).
Results
A total of 79 patients were included in the study cohort. The mean age was 66.5 ± 6.25 years, and the mean BMI was 25.8 ± 3.3 kg/m2. Baseline demographic and clinical characteristics, including age, iPSA, and prostate volume, were comparable across the RS-RARP (n=19), 2-layer RARP (n=30), and 3-layer RARP (n=30) groups, with no statistically significant differences observed (p>0.05). The detailed characteristics were listed in Table 1.
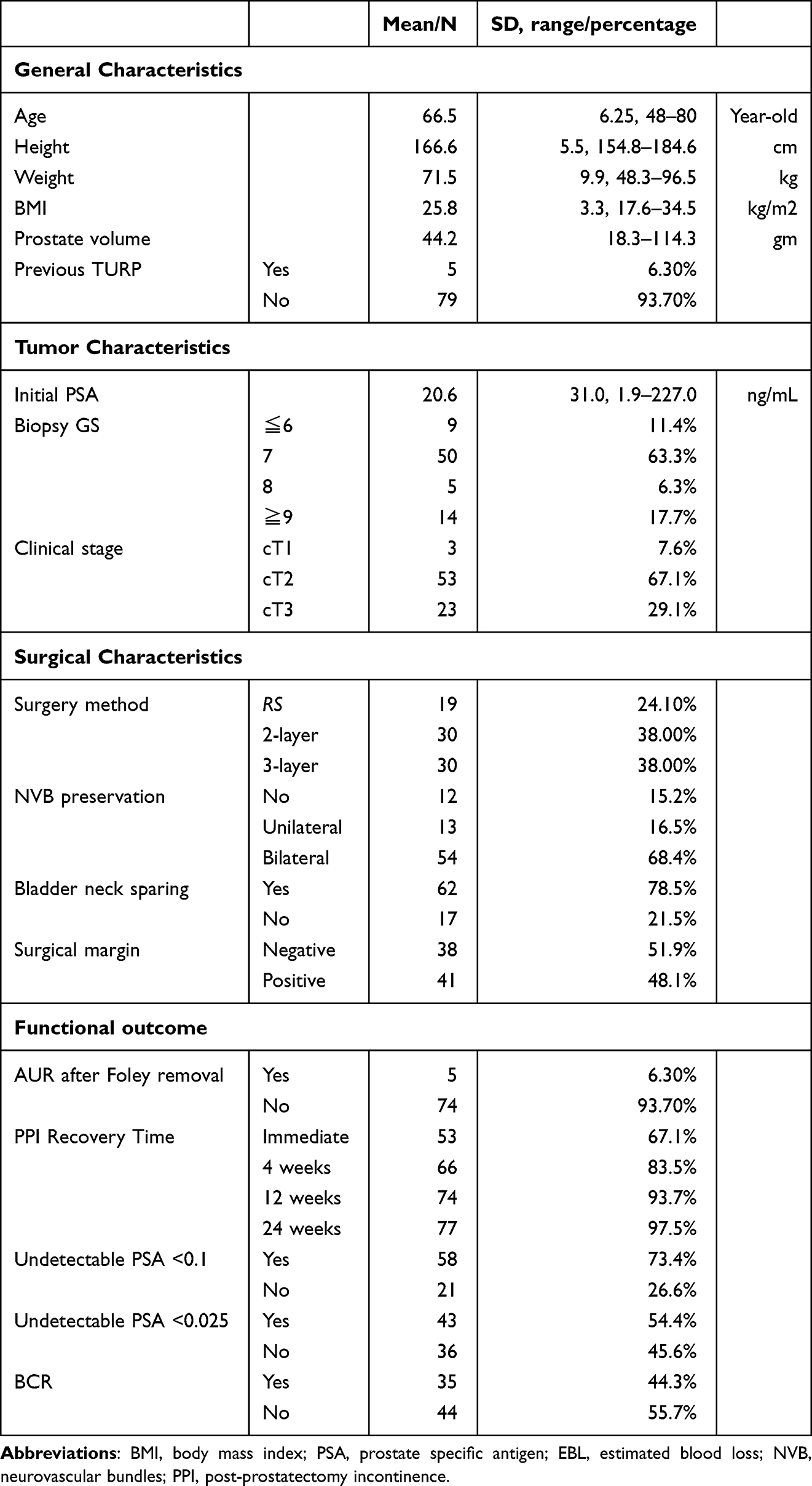 |
Table 1 Clinicopathological Patient Characteristics |
Surgical and cystographical parameters between the groups were compared and listed in Table 2. The rate of bladder neck (BN) sparing varied significantly (p=0.008), with 89.5% (17/19) of patients in the RS-RARP group, 60.0% (18/30) in the 2-layer RARP group, and 90.0% (27/30) in the 3-layer RARP group undergoing BN sparing. Furthermore, the bladder neck angle, as measured on cystography, was also significantly different among the groups (p=0.001), with mean angles of 128.5° ± 20.2°, 107.7° ± 17.5°, and 120.1° ± 16.7° for the RS-RARP, 2-layer RARP, and 3-layer RARP groups, respectively. Neurovascular bundle preservation rates were not significantly different between the groups (p=0.976).
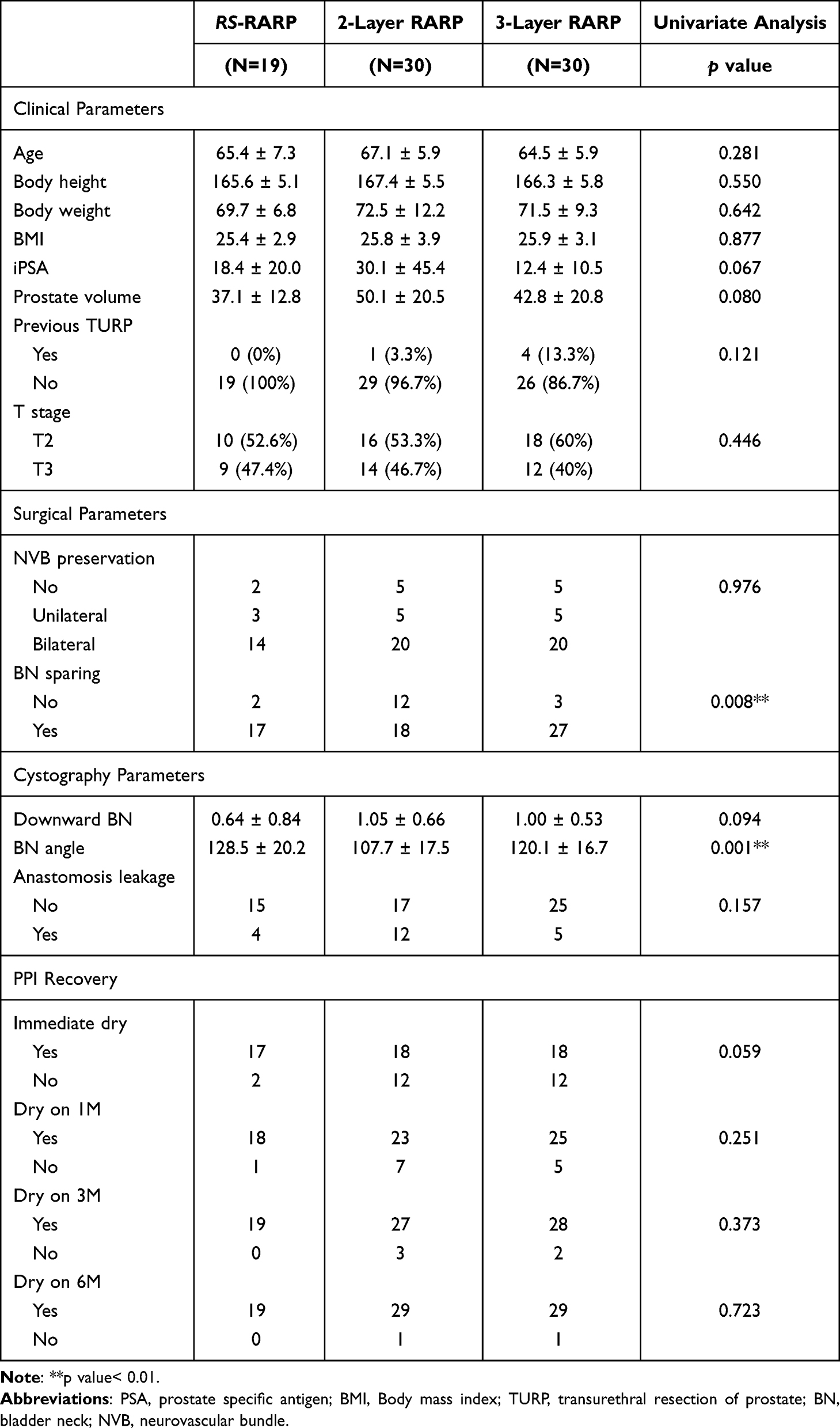 |
Table 2 Clinical Comparison Between Different Surgical Methods |
Regarding functional outcomes, PPI recovery rates were assessed at multiple time points. Although the RS-RARP group demonstrated numerically higher rates of continence recovery at immediate post-catheter removal (89.5% vs. 60.0% for the other two groups), 1 month (94.7% vs. 76.7% and 83.3%), and 3 months (100% vs. 90.0% and 93.3%), these differences did not achieve statistical significance (p=0.059, p=0.251, p=0.373, respectively). However, in pairwise comparisons, the RS-RARP group demonstrated a borderline statistical advantage in immediate dry rate when compared with the other two reconstruction groups (p=0.049). This difference did not retain strict significance after Bonferroni correction (p< 0.0125). Consequently, this finding should be interpreted cautiously as a favorable clinical trend. At 6 months post-surgery, all three groups achieved excellent continence rates (RS-RARP: 100.0%, 2-layer RARP: 96.7%, and 3-layer RARP: 96.7%), and the differences were not statistically significant (p=0.723). The detailed data and illustrated figure were shown as Table 2 and Figure 2.
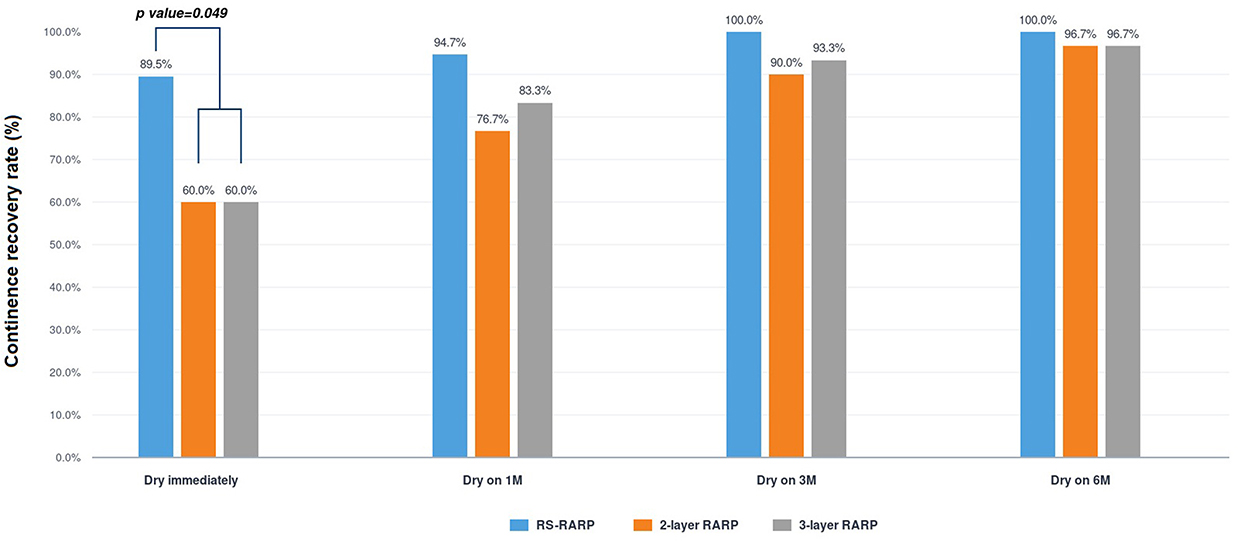 |
Figure 2 Comparison of PPI outcome between 3 different surgical techniques. |
Discussion
In the context of surgical anatomy, multiple factors have been identified to influence continence recovery.12 These include maximizing urethral length, careful management of the dorsal vein complex, intrafascial nerve-sparing techniques, BN sparing approaches, preservation of the puboprostatic ligaments, and restoration of urethral anatomical support. During the reconstructive phase, which aims to restore anatomy, three principal techniques have been developed for RARP beyond the standard urethro-vesical anastomosis: posterior repair (PR),7 anterior reconstruction (AR),8 and total reconstruction (TR).9,10 In contrast to these reconstruction methods, RS-RARP employs a preservation strategy, maintaining the pubovesical complex and other crucial anterior anatomical structures supporting the bladder neck and urethra to facilitate early PPI recovery. Both the reconstruction and preservation methods ultimately aim to enhance the recovery of PPI. Our previous research demonstrated that the recovery of PPI following RARP was correlated to preoperative patient status, intraoperative reconstructive techniques, and postoperative bladder neck position.10 In the current study, we further stratified patients by surgical approach to compare the impact of different pelvic floor preservation and reconstruction techniques on PPI recovery. Due to a paucity of direct comparisons between RS-RARP and conventional RARP with posterior repair or total reconstruction, most existing comparisons are based on systemic reviews and meta-analyses.
This retrospective cohort study compared the efficacy of three distinct RARP techniques on post-operative continence recovery. The primary findings indicate that all three techniques yield excellent long-term PPI recovery rates (over 96% at 6 months). Notably, intergroup analyses revealed that the RS-RARP group demonstrated a borderline statistical advantage in immediate PPI recovery (p=0.049), which should be interpreted cautiously as an encouraging clinical trend rather than a definitive conclusion. Although this significant superiority did not remain in PPI recovery at 1, 3, and 6 months. The advantage of the RS-RARP group in achieving early continence is consistent with findings from several other reports. A retrospective case series by Liao et al13 found that RS-RARP provided a significantly better immediate continence result compared to the retropubic approach (75.6% vs. 26.1%).13 Similarly, a large propensity score-matched analysis of 1863 patients by Lee et al14 demonstrated that RS-RARP was associated with a significantly superior PPI recovery rate over a 6-month period.14 Another comparative study found that RS-RARP resulted in a significantly higher proportion of continent patients at all time points up to 12 months, though it was concurrently associated with a higher positive surgical margin rate.15
The mechanism underlying the early continence benefit of the Retzius-sparing approach is widely believed to be the preservation of crucial anatomical structures within the anterior pelvic space.2 By leaving the pubovesical complex, detrusor apron, and other supporting ligaments intact, the bladder neck and urethra maintain their natural anatomical suspension. This preservation may prevent the downward displacement of the bladder neck and sustain the optimal vesicourethral junction angle, both of which are critical for immediate PPI recovery. Our study’s finding that the RS-RARP group had the largest mean BN angle (128.5∘) supports this hypothesis, suggesting a less distorted vesicourethral junction compared to the conventional groups.
In addition to the PPI recovery comparison, we performed an analysis of post-operative cystography patterns. Post-operative cystography has become a valuable modality for assessing the anatomical outcomes of surgery and predicting continence recovery. Features such as the BN angle, the position of the bladder neck relative to the pubic symphysis, and the presence of anastomotic leakage have been identified as key predictors of PPI recovery.16 A narrow vesical angle and a downward-positioned bladder neck are associated with a slower and less favorable recovery of urinary control.17,18 Therefore, analyzing these parameters alongside functional outcomes provides critical insight into the mechanisms by which different surgical techniques affect continence. Our study found a statistically significant difference in the BN angle among the three groups, with the 2-layer RARP group having the sharpest mean angle (107.7∘). However, this anatomical difference did not translate into a statistically significant difference in PPI recovery.
Our results, demonstrating a significant anatomical difference in the BN angle, yet lacking a corresponding significant functional difference in continence, may suggest that while the BN angle is an important factor, it is not the sole determinant of continence recovery. Other variables, such as the functional integrity of the urethral sphincter complex, the length of the membranous urethra, and overall pelvic floor muscle tone, are also crucial.5 Beyond these surgical factors, BMI and postoperative management play pivotal roles in functional outcomes. An increased BMI is frequently associated with a larger prostate volume and increased intrapelvic fat, which restricts the pelvic working space, thereby escalating the technical difficulty of apical dissection and subsequent reconstruction. Furthermore, post-operative interventions, ranging from early pelvic floor muscle training and medical therapies to subsequent anti-incontinence procedures, represent significant clinical confounders that can actively alter the observed long-term PPI recovery timeline. Accounting for these baseline characteristics and treatment modalities is essential for an accurate, multidimensional evaluation of continence rehabilitation.19,20 The anatomical reconstruction techniques, such as the 2-layer and 3-layer approaches, may potentially compensate for a sub-optimal BN angle through other mechanisms, such as increasing the functional urethral length or providing robust posterior support.21 This complexity underscores the multifactorial nature of post-operative continence and the imperative for a holistic view that considers both anatomical and functional factors.
This study is subject to several limitations. Its retrospective, single-center design limits the generalizability of the findings to other institutions. The relatively small sample size, particularly in the RS-RARP group (n=19), represents a significant limitation. To address this, a post-hoc power analysis was performed for the immediate PPI recovery rate (89.5% vs. 60.0%), yielding a statistical power of 67.6%. This indicates that while a favorable clinical trend is evident, the comparison was somewhat underpowered to establish an absolute functional superiority, leaving a small possibility of a Type II error. Based on our observed effect size (h = 0.71), a future balanced prospective study would require at least 32 patients per arm to achieve a standard statistical power of 80%. Therefore, the borderline p-value (p=0.049) should be interpreted with appropriate caution, serving as an encouraging signal for further large-scale validation. Furthermore, the definition of continence as a pad-free binary outcome does not fully capture the complete spectrum of urinary control, such as the use of one safety pad per day or occasional leakage. Future studies should adopt more objective and standardized measures of incontinence, including the 24-hour pad weight test and validated patient-reported outcome measures such as the I-QOL and IIQ-7 questionnaires, to provide a more precise and multidimensional assessment of functional recovery.22,23 Additionally, technique assignment was inherently surgeon-dependent, as each surgical technique was primarily performed by a specific experienced surgeon. Therefore, surgeon-related factors may have partially influenced the observed outcomes despite all surgeons having surpassed their learning curves. Future prospective studies utilizing a single-surgeon design across different technical arms are warranted to minimize this potential confounding effect. Ultimately, a larger randomized controlled or multi-center trial would be necessary to confirm the observed numerical trends and to establish the definitive clinical superiority regarding early PPI recovery.
Conclusion
In conclusion, this exploratory study suggests that all three RARP techniques examined in this study, including RS-RARP, 2-layer RARP, and 3-layer RARP, result in excellent long-term continence rates. The functional advantage of the RS-RARP technique was strictly limited to a favorable clinical trend benefit in the immediate dry rate, with no sustained statistical significance observed at the 1-, 3-, and 6-month follow-up. This observed pattern, supported by existing literature, highlights the potential benefit of preserving the anterior anatomical structures for short-term PPI recovery. While cystography revealed significant differences in bladder neck angles between the groups, this did not translate to a statistically significant difference in long-term continence, emphasizing that PPI recovery is a complex, multifactorial process. However, given the exploratory nature, small sample size, and lack of multivariate control in this series, these findings should be interpreted with caution as hypothesis-generating clinical trends. Future large-scale, prospective studies are warranted to further investigate the nuanced interplay between surgical technique, anatomical reconstruction, and the functional recovery of continence following RARP.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study has been conducted in accordance with the ethical principles mentioned in the Declaration of Helsinski (2013). This study was approved by Chang Gung Medical Foundation Institutional Review Board. (Number: 201504523B0C501) The requirement for informed consent was waived by IRB due to the retrospective nature of this case study. To ensure patient data confidentiality, all personal identifiers were fully anonymized, and strict privacy control was maintained during data extraction and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Di Mauro E, La Rocca R, Di Bello F, et al. Technical modifications employed in RARP to improve early continence recovery: a literature review. Life. 2025;15(3):415. doi:10.3390/life15030415
2. Arroyo C, Martini A, Wang J, Tewari AK. Anatomical, surgical and technical factors influencing continence after radical prostatectomy. Ther Adv Urol. 2019;11:1756287218813787. doi:10.1177/1756287218813787
3. Martini A, Tewari AK. Anatomic robotic prostatectomy: current best practice. Ther Adv Urol. 2019;11:1756287218813789. doi:10.1177/1756287218813789
4. Galfano A, Di Trapani D, Sozzi F, et al. Beyond the learning curve of the Retzius-sparing approach for robot-assisted laparoscopic radical prostatectomy: oncologic and functional results of the first 200 patients with ≥ 1 year of follow-up. Eur Urol. 2013;64(6):974–10. doi:10.1016/j.eururo.2013.06.046
5. Kumar S, Soni PK, Chandna A, Parmar K, Gupta PK. Mucosal coaptation technique for early urinary continence after robot-assisted radical prostatectomy: a comparative exploratory study. Central Eur J Urol. 2021;74(4):528–534. doi:10.5173/ceju.2021.R1.0050
6. Qian J, Fu Y, Marra G, et al. Modified Retzius-sparing robot-assisted radical prostatectomy for cases with anterior tumor: a propensity score-matched analysis. World J Urol. 2024;42(1):170. doi:10.1007/s00345-024-04807-7
7. Rocco F, Gadda F, Acquati P, et al. Ricerca personale: la ricostruzione dello sfintere striato uretrale [Personal research: reconstruction of the urethral striated sphincter]. Archivio italiano di urologia andrologia. 2001;73(3):127–137.
8. Patel VR, Coelho RF, Palmer KJ, Rocco B. Periurethral suspension stitch during robot-assisted laparoscopic radical prostatectomy: description of the technique and continence outcomes. Europ urol. 2009;56(3):472–478. doi:10.1016/j.eururo.2009.06.007
9. Tewari A, Jhaveri J, Rao S, et al. Total reconstruction of the vesico-urethral junction. BJU Int. 2008;101(7):871–877. doi:10.1111/j.1464-410X.2008.07424.x
10. Porpiglia F, Bertolo R, Manfredi M, et al. Total anatomical reconstruction during robot-assisted radical prostatectomy: implications on early recovery of urinary continence. Europ Urol. 2016;69(3):485–495. doi:10.1016/j.eururo.2015.08.005
11. Chen HY, Liu JM, Shao IH, et al. Modified three-layer vesicourethral reconstruction in robot-assisted radical prostatectomy can change cystography pattern and improve early recovery of continence. J Surg Oncol. 2024;129(7):1332–1340. doi:10.1002/jso.27636
12. Zattoni F, Artibani W, Patel V, et al. Technical innovations to optimize continence recovery after robotic assisted radical prostatectomy. Minerva urologica e nefrologica. 2019;71(4):324–338. doi:10.23736/s0393-2249.19.03395-2
13. Liao PC, Hung SC, Hu JC, Chiu KY. Retzius-sparing Robotic-assisted Radical Prostatectomy Facilitates Early Continence Regardless of Neurovascular Bundle Sparing. Anticancer Res. 2020;40(7):4075–4080. doi:10.21873/anticanres.14405
14. Lee J, Kim HY, Goh HJ, et al. Retzius sparing robot-assisted radical prostatectomy conveys early regain of continence over conventional robot-assisted radical prostatectomy: a propensity score matched analysis of 1863 patients. J Urol. 2020;203(1):137–144. doi:10.1097/ju.0000000000000461
15. Lambert E, Allaeys C, Berquin C, et al. Is it safe to switch from a standard anterior to Retzius-Sparing approach in robot-assisted radical prostatectomy? Current Oncol. 2023;30(3):3447–3460. doi:10.3390/curroncol30030261
16. Shao IH, Chou CY, Huang CC, et al. A specific cystography pattern can predict postprostatectomy incontinence. Ann Surg Oncol. 2015;22(Suppl 3):S1580–6. doi:10.1245/s10434-015-4847-y
17. Sugi M, Kinoshita H, Yoshida T, et al. The narrow vesicourethral angle measured on postoperative cystography can predict urinary incontinence after robot-assisted laparoscopic radical prostatectomy. Scand J Urol. 2018;52(2):151–156. doi:10.1080/21681805.2018.1428683
18. Shao IH, Kan HC, Chen HY, et al. Recognition of postoperative cystography features by artificial intelligence to predict recovery from postprostatectomy urinary incontinence: a rapid and easy way to predict functional outcome. J Personal Med. 2023;13(1):126. doi:10.3390/jpm13010126
19. Bada M, Crocetto F, Barone B, et al. ProACT in the management of stress urinary incontinence after radical prostatectomy. What happens after 8 years of follow up? Monocentric analysis in 42 patients. J Basic Clin Physiol Pharmacol. 2023;34(1):49–54. doi:10.1515/jbcpp-2021-0295
20. Barone B, Amicuzi U, Massanova M, et al. The correlation between body mass index and prostate volume: a retrospective analysis of pre and postoperative measurements in prostate cancer patients. Prostate. 2025;85(5):433–442. doi:10.1002/pros.24845
21. Yu Y, Reiter RE, Zhang M. Surgical techniques for enhancing postoperative urinary continence in robot-assisted radical prostatectomy: a comprehensive review. Int J Surg. 2025;111(6):3931–3941. doi:10.1097/js9.0000000000002414
22. Uebersax JS, Wyman JF, Shumaker SA, McClish DK, Fantl JA; Continence program for women research group. Short forms to assess life quality and symptom distress for urinary incontinence in women: the incontinence impact questionnaire and the urogenital distress inventory. Neurourol Urodyn. 1995;14(2):131–139. doi:10.1002/nau.1930140206
23. Wagner TH, Patrick DL, Bavendam TG, Martin ML, Buesching DP. Quality of life of persons with urinary incontinence: development of a new measure. Urology. 1996;47(1):
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.