Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Early Versus Late Tracheostomy in Stroke Patients: A Retrospective Analysis
Authors Shen Y ![]() , Cao Q
, Cao Q ![]() , Zhuo H, Hu M, Chen S
, Zhuo H, Hu M, Chen S ![]()
Received 30 August 2022
Accepted for publication 4 November 2022
Published 17 November 2022 Volume 2022:18 Pages 2713—2723
DOI https://doi.org/10.2147/NDT.S388062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Yu Shen,1,2,* Qian Cao,1,* Hou Zhuo,1 Mengyao Hu,3 Shenjian Chen1,4
1Department of Neurology, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2Department of Neurology, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 3The Medical Imaging Center, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 4Neurology Intensive Care Unit, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shenjian Chen, Department of Neurology, The Second Affiliated Hospital of Nanchang University, No. 1 Minde Road, Nanchang, Jiangxi, People’s Republic of China, Email [email protected]
Objective: The timing of tracheostomy (TR) in severe stroke patients receiving mechanical ventilation has not been determined. In this study, we compared some prognostic indicators of early tracheostomy (ET) and late tracheostomy (LT). A meta-analysis was performed to obtain a higher level of evidence of the timing of TR in patients with severe stroke receiving mechanical ventilation.
Methods: The study was a retrospective single-center study. We divided the severe stroke patients who received TR from June 2020 to June 2022 into the ET group and LT group. The demographic characteristics, clinical characteristics and prognostic indices were compared. For this meta-analysis, we systematically searched PubMed and other databases. The compared prognostic indicators included mechanical ventilation time, ICU length of stay (LOS), total LOS, ventilator-related pneumonia (VAP) incidence, and mortality.
Results: A total of 61 patients were included in our study, including 32 patients in the ET group and 29 patients in the LT group. Univariate and multivariate analyses showed that the NIHSS score in the ET group was higher than that in the LT group (P < 0.05). In terms of outcome indicators, compared with the LT group, the median mechanical ventilation time in the ET group was shortened by 5.5 days (P = 0.034). The ICU LOS and total LOS in the ET group were significantly lower than those in the LT group (median 14.5 days vs 22 days, P = 0.004; 21 days vs 27 days, P = 0.019). The meta-analysis showed that ET could significantly shorten the ICU LOS (MD − 3.89 [95% CI: − 6.86, − 0.92]) and the total LOS (MD − 7.70 [95% CI: − 8.57, − 6.83]) and significantly reduce the occurrence of VAP (OR 0.75 [95% CI: 0.64, 0.87]).
Conclusion: The results of our retrospective study and meta-analysis support that ET can shorten the ICU LOS and total LOS and reduce the occurrence of VAP. Therefore, it has a positive effect on the prognosis of patients with severe stroke who need mechanical ventilation support.
Keywords: tracheostomy, TR, tracheostomy timing, stroke, early tracheostomy, ET
Introduction
Stroke is an acute neurological deficit caused by arterial occlusion/stenosis or rupture.1,2 It has become the second most common cause of death worldwide, and the socioeconomic burden of surviving stroke patients is immeasurable.3 It is well known that severe ischemic or hemorrhagic stroke patients often require invasive mechanical ventilation for airway protection, aspiration, or respiratory failure.4 For patients requiring prolonged mechanical ventilation, tracheostomy (TR) has the natural advantage of reducing the use of sedative drugs and relieving patient rejection.5,6 TR can also shorten hospital stays, reduce the incidence of ventilator-associated pneumonia (VAP), reduce mortality, and improve outcomes.7–9 TR is performed in the general ICU in approximately 10–15% of patients and in the neurological ICU in 35% of patients.10,11
It is worth noting that while TR is important, it is still unclear when it should be performed. There is little evidence to guide the timing of TR in patients with massive cerebral infarction.12 For general ICU patients, previous studies have found that early tracheostomy (ET) can reduce the need for sedative drugs, speed up the removal of endotracheal intubation, shorten ICU stay, reduce death, and improve functional outcomes compared with late tracheostomy (LT).13–15 However, some studies did not report these potential benefits.5,16,17 There are relatively few TR studies in ischemic or hemorrhagic stroke patients. Although there have been previous meta-analyses with a small number of studies, ET was associated with fewer days in the hospital and fewer VAP but not with ICU LOS, duration of mechanical ventilation, or mortality compared with LT.18 In contrast, a recently published large randomized controlled trial (SETPOINT 2) found no difference in improved functional outcome.19 Therefore, we still want to conduct a comprehensive discussion of related issues because TR in severe stroke patients provides more comprehensive evidence.
This study includes severe ischemic or hemorrhagic stroke patients in the neurology ICU and comprehensively compared ET with LT. In addition, we conducted a meta-analysis of all previous related studies in the hope of obtaining higher-level evidence for the timing of TR in stroke patients.
Materials and Methods
Retrospective Study
Study Population
This study was a single-center, retrospective study. It was carried out in the Second Affiliated Hospital of Nanchang University, which is an advanced stroke center in Jiangxi Province. Patients admitted to the neurology or neurosurgery ICU due to severe ischemic or hemorrhagic stroke from June 2020 to June 2022 were included. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University.
According to the diagnostic criteria of the International Classification of Diseases, the types of strokes include acute cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage, and the diagnosis of the disease was performed by two experienced neurological ICU physicians who were blinded to the study. Notably, patients under the age of 18 and patients with traumatic intracerebral hemorrhage were not included in this study. TR was performed on the day of admission, and patients who died within 3 days were also excluded.
Percutaneous and surgical TR was performed by a specialized neurological ICU physician or an otolaryngologist. ET was defined as an operation occurring within 7 days of tracheal intubation, and LT was defined as occurring after 7 days. After the TR, patients were cared for by a professional specialist nurse. The intracranial pressure reduction of cerebral hemorrhage and the antiplatelet treatment of cerebral infarction were also carried out in accordance with the guidelines.20–22 Other treatments were performed according to disease guidelines, including management of blood pressure and blood sugar. This study defines VAP as pneumonia that occurs 48 hours after mechanical ventilation (tracheal or endotracheal intubation) or if the original pneumonia is aggravated 48 hours after mechanical ventilation. Diagnoses are based on symptoms, signs, routine blood tests, imaging examinations, and a simplified version of the Clinical Pulmonary Infection Score (CPIS). If the CPIS≥5, a VAP diagnosis is made.23 We extracted the demographic characteristics of the final included patient population, including age, sex, blood pressure, and history of smoking and alcohol use. Others include comorbidities, such as hypertension, diabetes, chronic obstructive pulmonary disease, and kidney disease. The National Institute of Health Stroke Scale (NHISS) score, disease diagnosis, and Glasgow Coma Scale (GCS) score were also recorded at admission. The primary outcomes observed in the study were the incidence of all-cause mortality, ICU and total LOS, incidence of VAP, and duration of mechanical ventilation. All-cause death refers only to ICU admission.
Statistical Analysis
According to the duration of TR, patients are divided into two groups. The chi-square test or Fisher’s exact test was used for single-factor classification data. For continuous variable data, the independent-sample t-test was used for normally distributed variables, and the Mann‒Whitney U-test was used for the nonnormally distributed variables. To assess the effect of all collected clinical data on the timing of TR, we performed multivariate logistic regression analysis. Variables with a P value less than 0.2 were also included in the regression model, and ORs and 95% CIs were calculated. P<0.05 was considered statistically significant. All tests were conducted by IBM SPSS Statistics 25.0 software (SPSS, Chicago, IL, USA).
Meta-Analysis
Search Strategy
The literature search was performed independently by 2 neurologists. We systematically searched PubMed, EMBASE, The Cochrane Library, and Web of Science databases. The search period was from database inception to March 2022. The search used the keywords “tracheostomy”, “stroke”, “early”, and “late”. The protocol has been registered in the International Prospective Register of Systematic Reviews (http://www.crd.york.ac.uk/prospero, CRD42022348602). The data were analyzed between March 2022 and June 2022.
Selection Criteria and Data Abstraction
Reviews, conference reports, case reports, and animal experiments were not included in this analysis. Duplicate data or duplicate publications were excluded. Literature with insufficient information was also excluded. Data extraction was performed independently by two reviewers. The following data were collected: (1) basic information, including authors, article titles, publication time, and study population; (2) definition of early or late TR, age and diagnosis of the study population, and GCS score. (3) ICU LOS, total LOS, number of deaths, number of mechanical pneumonias, and duration of mechanical ventilation. If there was any disagreement between the two reviewers during this process, a third expert decided the final result.
Quality Assessment and Statistical Method
Two reviewers independently assessed the quality of the studies using the Newcastle‒Ottawa quality assessment scale (NOS score). Scores ≥6 indicated that a study was of high quality, and scores of 4 or 5 points indicated moderate quality.24
Data were analyzed using a fixed-effect model if they were homogeneous (I2 < 25%) or of low heterogeneity (25% ≤ I2 < 50%), and a random-effect model was used if the data exhibited moderate (50% ≤ I2 < 75%) or substantial heterogeneity (I2 ≥ 75%).25,26 All analyses were conducted using Review Manager (RevMan) Version 5.3 software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
Retrospective Study
A total of 61 patients with poststroke TR were included in this study, including 32 patients (52.46%) in the ET group and 29 patients (47.54%) in the LT group. The median intubation time was 4 days (IQR, 3–5) in the ET group and 10 days (IQR, 8–13) in the LT group. The baseline characteristics of the two groups are shown in Table 1. In terms of age and sex, there was no significant difference between the ET group and the LT group, with an average age of 64.59 years vs 65.76 years and males comprised 65.63% vs 68.97%, respectively. The proportion of smoking in the two groups (ET Group 34.38% vs LT Group 41.38%, P = 0.573) was also similar. There was no significant difference in hypertension, diabetes, heart disease, kidney disease or chronic obstructive pulmonary disease (COPD) between the two groups. Stroke type distributions were 12 cases (37.5%) and 12 cases (41.38%) of acute ischemic stroke and 20 cases (62.5%) and 17 cases (58.62%) of hemorrhagic stroke in the ET and LT groups, respectively. There was no significant difference between the two groups. GCS scores were also similar between the two groups, with a median of 7.5 (IQR, 6–9) in the ET group and 8 (IQR, 7–10) in the LT group. The median NIHSS score in the ET group was 36 (IQR, 32.00–38.75), which was significantly higher than that in the LT group (median 26 [IQR, 20–35]).
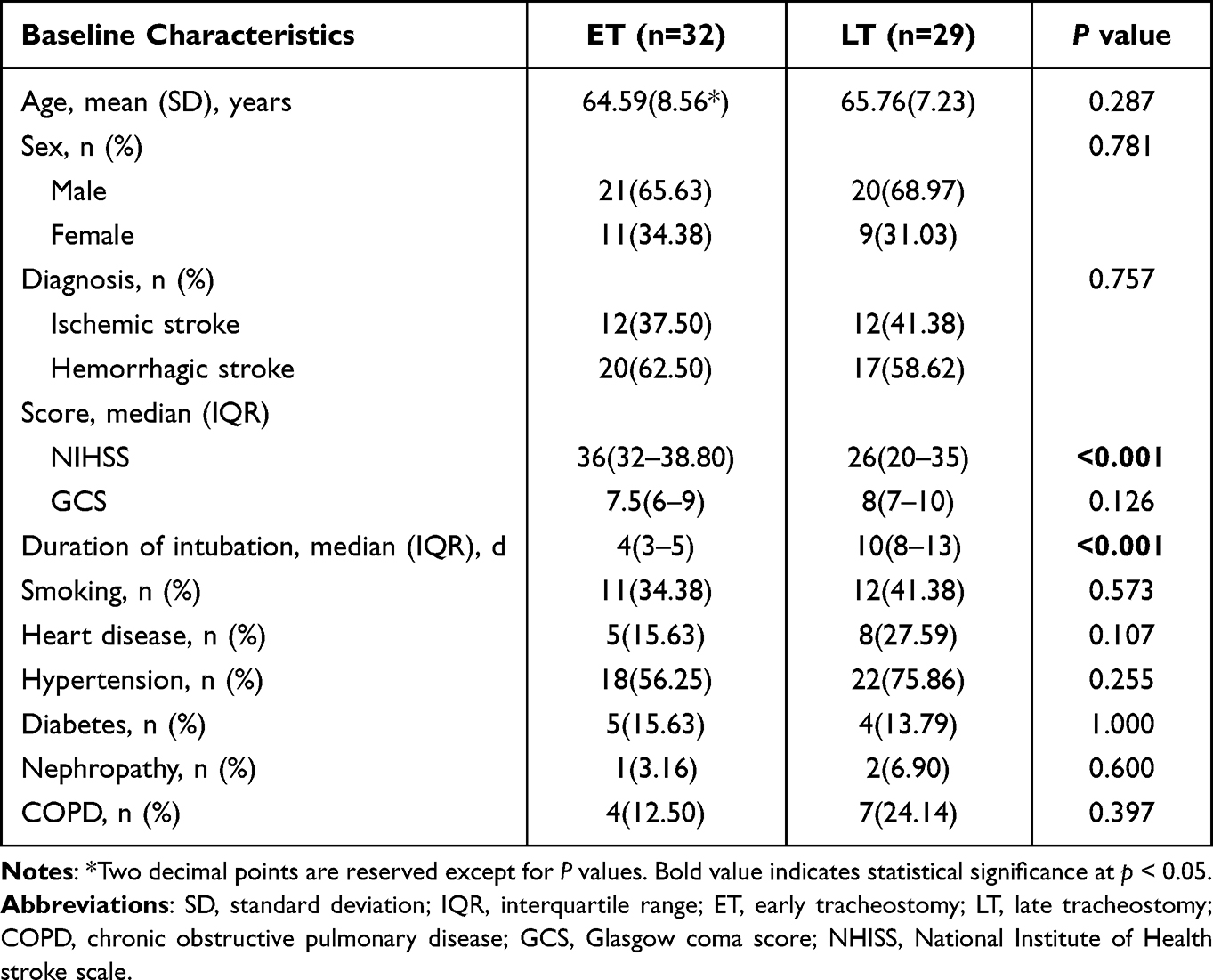 |
Table 1 The Baseline Characteristics of ET Group and LT Group |
In terms of outcome indicators, there was no significant difference in mortality (9.38% vs 20.69%) or VAP incidence (62.50% vs 62.07%) between the ET group and LT group. However, compared with LT, the median mechanical ventilation time in the ET group was shortened by 5.5 days (ET 8.5 days vs LT 14 days, P = 0.034). In terms of ICU LOS and total LOS, the ET group was significantly lower than the LT group (median: 14.5 days vs 22 days, P = 0.004; 21 days vs 27 days, P = 0.019). The outcome index results are shown in Table 2.
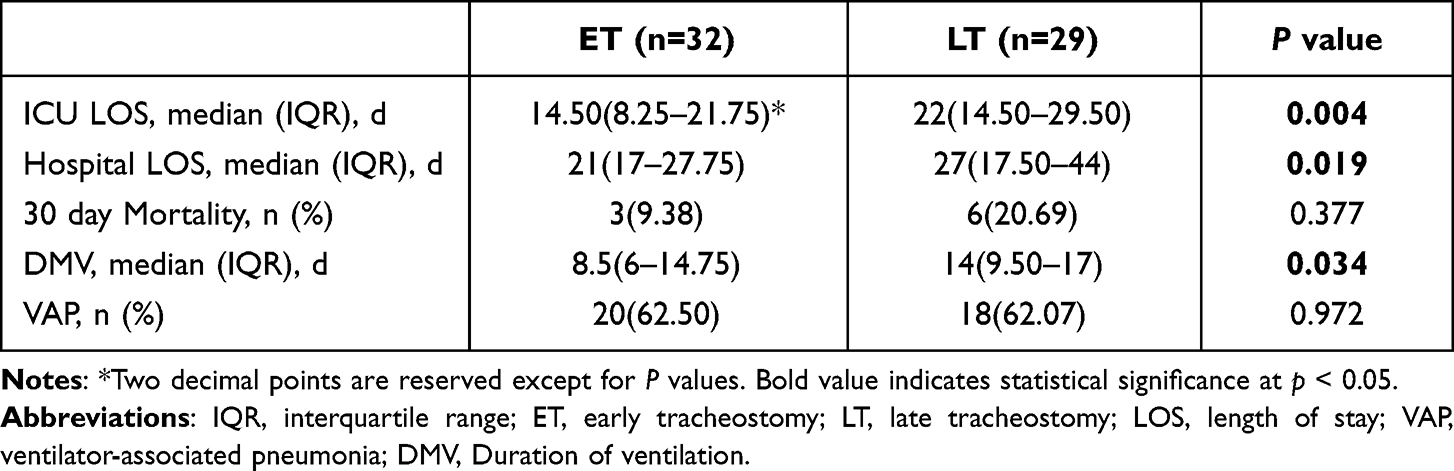 |
Table 2 Clinical Outcomes in Relation to Tracheostomy Timing |
In the binary logistic regression analysis, the NIHSS score was an independent factor (OR=0.859; 95% CI 0.774–0.952; p=0.004) affecting the choice of TR time, as shown in Supplementary Table S1. The results imply that the more severe the patient is, the more likely the clinicians are to prefer ET.
Meta-Analysis
A total of 834 articles were identified by searching PubMed, Medline, Embase, Web of Science and the Cochrane library databases. We screened the title and abstract, and 740 articles were excluded because they were obviously irrelevant. After careful review of articles by reading abstracts and full texts, 8 studies published between 2013 and 2022 were included in the analysis, with a total of 16,772 subjects identified.4,19,27–32 Supplementary Figure S1 shows the flow chart of the study.
The NOS score ranged from 6 to 9, indicating that the overall quality of the studies was good (Supplementary Table S2). The characteristics of the studies included in the meta-analysis are presented in Table 3 and Supplementary Table S3. Of note, among the 8 studies, various studies defined the time of ET as 3–10 days after endotracheal intubation, which was similar to our retrospective study criteria.
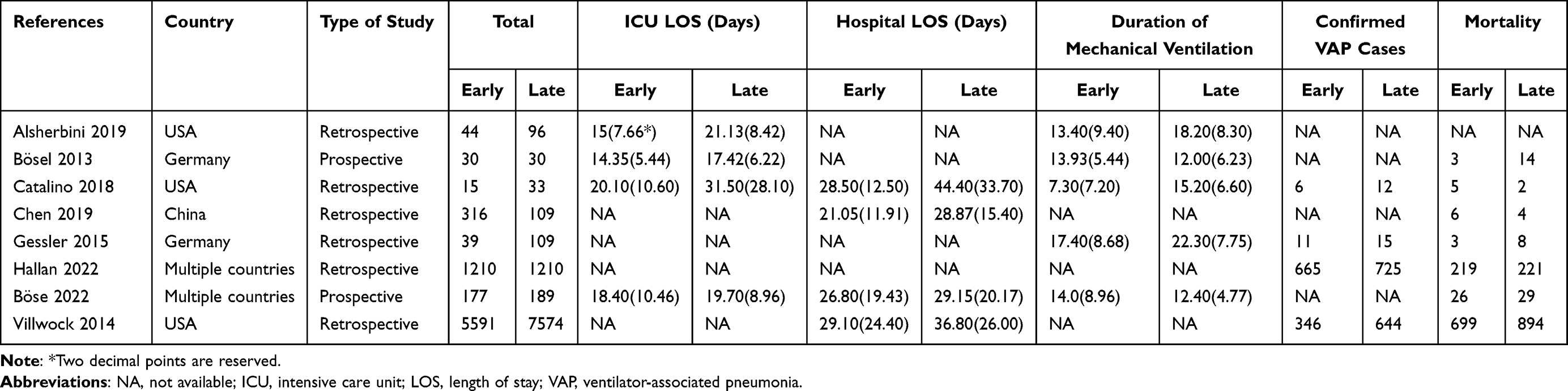 |
Table 3 Characteristics of Included Studies |
Among the 8 studies included in the meta-analysis, 5 of them enumerated the results of mechanical ventilation time, and a total of 762 subjects were included. Meta-analysis showed that there was no significant difference between ET and LT in ventilation time (MD −2.58 [95% CI −6.34,1.17], P = 0.18; Figure 1). A meta-analysis of 614 people included in 4 studies showed that ET could significantly shorten the ICU LOS (MD −3.89 [95% CI −6.86, −0.92], P = 0.01; Figure 2). In terms of total hospital LOS, the analysis of 14,004 persons included in 4 studies also showed that ET could significantly shorten the total hospital LOS (MD −7.70 [95% CI −8.57, −6.83], P < 0.001; Figure 3). In the analysis of VAP, a total of 15,772 subjects were included in 4 studies. The results showed that compared with LT, ET reduced the occurrence of VAP (OR 0.75 [95% CI 0.67, 0.83], P < 0.001; Figure 4). In terms of mortality, 7 studies were included, with a total of 16,632 subjects. The pooled results showed that ET had no significant effect on mortality (OR 0.96 [95% CI 0.72, 1.27], P = 0.76; Figure 5). Sensitivity analysis of all meta-analyses results indicated that the results were stable In addition, the analysis showed no significant risk of publication bias on funnel plots.
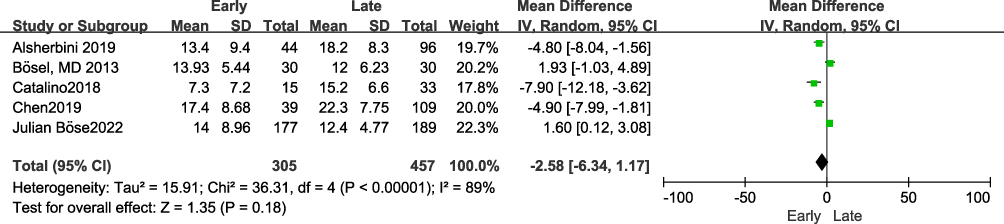 |
Figure 1 Forest plot of mechanical ventilation time. |
 |
Figure 2 Forest plot of ICU length of stay. |
 |
Figure 3 Forest plot of total hospital length of stay. |
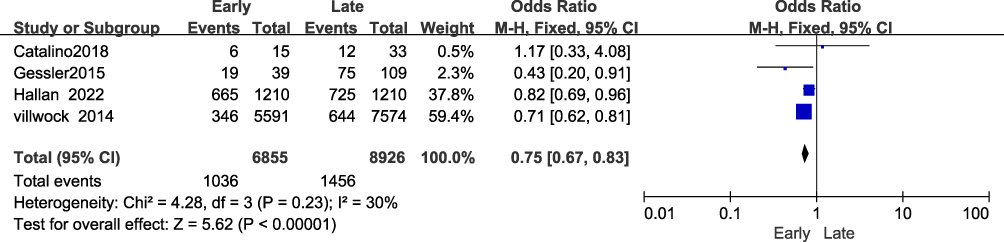 |
Figure 4 Forest plot of occurrence of ventilator-related pneumonia. |
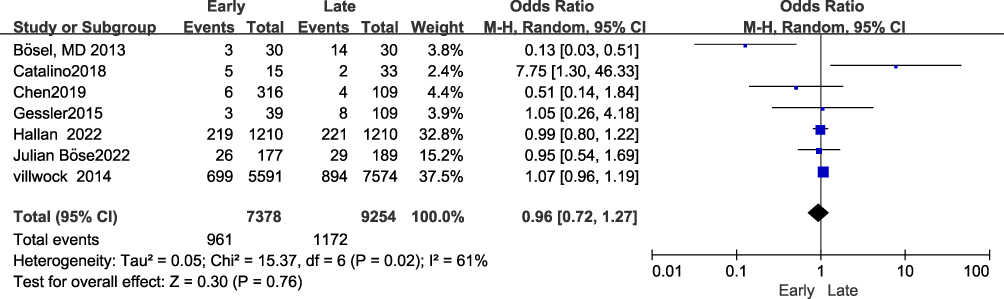 |
Figure 5 Forest plot of mortality. |
Discussion
It is generally accepted that mechanically assisted ventilation is required in critically ill neurological patients when they are unconscious or have bulbar dysfunction. Prolonged orotracheal intubation significantly increases the incidence of pulmonary infection and death.33–35 TR seems to solve this dilemma. However, when to perform TR is not settled. Compared to LT, this retrospective study and meta-analysis indicate that ET can shorten the ICU and hospital LOS but has no evident benefit for all-cause mortality. According to this retrospective study, ET significantly reduced mechanical ventilation time, but our meta-analysis did not fully support this conclusion and showed only relative trends. We found that ET significantly reduced the occurrence of VAP through meta-analysis; however, this retrospective study did not observe this phenomenon.
Univariate and logistic regression analyses indicated higher NIHSS scores in the ET group in this retrospective study. Although there was no significant difference in the GCS score between the two groups, it still suggested that the more serious the disease was, the more likely the patient was to receive ET. The severity of the disease and the state of consciousness are the factors that affect early extubation. A more serious disease reduces the chances of early extubation; ICU doctors may therefore make their clinical decisions more decisively in favor of ET, which may explain the higher NIHSS score of the ET group. Clinical practice and a variety of related studies have demonstrated that ET can reduce the need for sedatives and lead to removal of ventilator support more quickly.4,18,32,36–39 Our retrospective study also obtained a similar result showing that ET can shorten the mechanical ventilation time. However, our meta-analysis did not show that there was a significant difference in the mechanical ventilation time between the ET group and the LT group, which may be mainly affected by the results of the recently published SETPOINT2 randomized controlled trial.19 This large randomized controlled clinical trial showed that ET may help to start weaning from the ventilator earlier, but these differences did not reach statistical significance. The author’s explanation is that the potential benefits may be offset by longer off-line time and cannot be translated into shorter mechanical ventilation time or ICU LOS. Therefore, the study does not completely deny the possible benefits of ET in reducing mechanical ventilation time.
Regarding the LOS in the ICU and the total LOS, our retrospective study and meta-analysis showed that compared with LT, ET can significantly shorten the LOS in the ICU and the total LOS, which is consistent with the results of many previous clinical studies.39–43 This may be mainly related to ET reducing the time of mechanical ventilation, which means that ET patients can be transferred out of the ICU earlier and receive rehabilitation treatment earlier. However, the SETPOINT2 randomized clinical trial did not show that there was a significant difference between the ET group and LT group in the length of ICU stay and total LOS,19 but the study did not include patients with tracheal intubation 6–9 days after intubation, so the results may not fully reflect real clinical settings.
VAP incidence varies greatly among studies. Araujo et al reported 6.28% and 8.63% incidence rates for ET and LT groups, respectively, in their meta-analysis.18 However, the meta-analysis of ET in patients with severe acute brain injury performed by Mccredie found that the incidence of VAP in the ET group was as high as 54% and as high as 70% in the LT group.39 As seen in the retrospective study, VAP occurred in 62.5% of the ET group and 62.07% of the LT group, similar to the results of Mccredie et al.39 The high incidence of VAP in this study may be attributed to the serious disease and poor state of consciousness of the participants, which can be confirmed by the high NIHSS score and low GCS score of the study population. A low level of consciousness will lead to a worse cough response and a greater likelihood of microinhalation. In addition, the more serious the disease is, the longer the mechanical ventilation time will be, which will result in a decrease in mucociliary clearance capacity and a decline in local and systemic defense capacity, which may increase the incidence of VAP.23 In the population included in our meta-analysis, the incidence of VAP was 14.99% in the ET group and 15.64% in the LT group. In our clinical practice, we found that ET is helpful for airway management and reduces the occurrence of VAP. Most relevant clinical studies and our meta-analysis also support this view.31,32,44–46 Our retrospective study results showed that ET did not reduce the incidence of VAP. ET patients’ conditions are more severe than those of LT patients, their NIHSS scores are higher, and there is a higher probability of aspiration before intubation in ET patients. Some of these patients may have clinical and imaging manifestations of pneumonia after intubation or TR, and the more severe the condition is, the longer the mechanical ventilation time is. These may offset the potential benefits of ET, so the related benefits of ET on VAP cannot be ruled out.
ET has been shown to reduce mortality in SETPOINT research, primarily due to using less sedatives and shorter stays in the ICU.4 Surprisingly, the study of Catalino et al suggested that ET could increase mortality instead, and they explained this by early transition to comfort measures.29 The majority of clinical studies,19,30–32 including our retrospective studies and our meta-analysis, showed that ET had no significant effect on mortality. Since the ET group had a more severe condition than the control group in this retrospective study, the mortality analysis may have been affected. Unfortunately, we did not follow up on cases of death after discharge in this study.
Our study is based on our own retrospective studies and meta-analyses to explore the timing of tracheostomy, and the results are more credible. However, the study also has some limitations: 1. In our clinical study, we used a retrospective cohort study design, which inevitably contained confounding factors. For example, the control of blood pressure and blood glucose may not be the same for all patients, but these will also affect the prognosis. 2. This was a single-center study with a small sample size, and subgroup analysis was not conducted, so we should treat these results with caution. 3. Strokes of different subtypes, lesion locations, and ranges may affect respiration differently, as well as when tracheostomy is performed. For example, patients with posterior circulation stroke may not have serious clinical symptoms but may need longer respiratory support because the respiratory center is affected. 4. Finally, the definitions of ET in the studies included in our meta-analysis are not uniform and vary within 3–10 days after intubation. It is difficult to determine the optimal time of ET and its impact on patient prognosis. More studies may be needed in the future to determine the optimal time of ET.
Conclusion
Our retrospective study and meta-analysis results suggest that ET may shorten the ICU LOS and total hospital LOS and reduce the occurrence of VAP in severe stroke patients, but it has no significant effect on mechanical ventilation time or mortality. More research may be needed in the future to further evaluate the impact of ET on the prognosis of patients with severe stroke.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Statement of Ethics
The study protocol complied with the Declaration of Helsinki and was approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University. The procedures complied with institutional guidelines. Given the retrospective enrollment, patient consent for participation was waived by the Second Affiliated Hospital of Nanchang University. We promise that patient privacy data will not be available and published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. YS and QC contributed equally to this work and are co-first authors.
Funding
This research was supported by the Science and Technology Program of the Jiangxi Provincial Health Commission (funding number 202110056).
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
2. Gresham GE, Alexander D, Bishop DS, et al. American Heart Association prevention conference. IV. Prevention and rehabilitation of stroke. rehabilitation. Stroke. 1997;28(7):1522–1526. doi:10.1161/01.str.28.7.1522
3. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/s0140-6736(12)61728-0
4. Bösel J, Schiller P, Hook Y, et al. Stroke-related early tracheostomy versus prolonged orotracheal intubation in neurocritical care trial (SETPOINT): a randomized pilot trial. Stroke. 2013;44(1):21–28. doi:10.1161/strokeaha.112.669895
5. Young D, Harrison DA, Cuthbertson BH, Rowan K, TracMan Collaborators FT. Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA. 2013;309(20):2121–2129. doi:10.1001/jama.2013.5154
6. Cox CE, Carson SS, Holmes GM, Howard A, Carey TS. Increase in tracheostomy for prolonged mechanical ventilation in North Carolina, 1993–2002. Crit Care Med. 2004;32(11):2219–2226. doi:10.1097/01.ccm.0000145232.46143.40
7. Durbin CG
8. Freeman BD, Morris PE. Tracheostomy practice in adults with acute respiratory failure. Crit Care Med. 2012;40(10):2890–2896. doi:10.1097/CCM.0b013e31825bc948
9. Quinnell TG, Pilsworth S, Shneerson JM, Smith IE. Prolonged invasive ventilation following acute ventilatory failure in COPD: weaning results, survival, and the role of noninvasive ventilation. Chest. 2006;129(1):133–139. doi:10.1378/chest.129.1.133
10. Kurtz P, Fitts V, Sumer Z, et al. How does care differ for neurological patients admitted to a neurocritical care unit versus a general ICU? Neurocrit Care. 2011;15(3):477–480. doi:10.1007/s12028-011-9539-2
11. Groves DS, Durbin CG
12. Torbey MT, Bösel J, Rhoney DH, et al. Evidence-based guidelines for the management of large hemispheric infarction: a statement for health care professionals from the neurocritical care society and the German society for neuro-intensive care and emergency medicine. Neurocrit Care. 2015;22(1):146–164. doi:10.1007/s12028-014-0085-6
13. Rumbak MJ, Newton M, Truncale T, Schwartz SW, Adams JW, Hazard PB. A prospective, randomized, study comparing early percutaneous dilational tracheostomy to prolonged translaryngeal intubation (delayed tracheostomy) in critically ill medical patients. Crit Care Med. 2004;32(8):1689–1694. doi:10.1097/01.ccm.0000134835.05161.b6
14. Griffiths J, Barber VS, Morgan L, Young JD. Systematic review and meta-analysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation. BMJ. 2005;330(7502):1243. doi:10.1136/bmj.38467.485671.E0
15. Freeman BD, Borecki IB, Coopersmith CM, Buchman TG. Relationship between tracheostomy timing and duration of mechanical ventilation in critically ill patients. Crit Care Med. 2005;33(11):2513–2520. doi:10.1097/01.ccm.0000186369.91799.44
16. Blot F, Similowski T, Trouillet JL, et al. Early tracheostomy versus prolonged endotracheal intubation in unselected severely ill ICU patients. Intensive Care Med. 2008;34(10):1779–1787. doi:10.1007/s00134-008-1195-4
17. Terragni PP, Antonelli M, Fumagalli R, et al. Early vs late tracheostomy for prevention of pneumonia in mechanically ventilated adult ICU patients: a randomized controlled trial. JAMA. 2010;303(15):1483–1489. doi:10.1001/jama.2010.447
18. Araujo de Franca S, Tavares WM, Salinet ASM, Paiva WS, Teixeira MJ. Early tracheostomy in stroke patients: a meta-analysis and comparison with late tracheostomy. Clin Neurol Neurosurg. 2021;203:106554. doi:10.1016/j.clineuro.2021.106554
19. Bösel J, Niesen WD, Salih F, et al. Effect of early vs standard approach to tracheostomy on functional outcome at 6 months among patients with severe stroke receiving mechanical ventilation: the SETPOINT2 randomized clinical trial. JAMA. 2022;327(19):1899–1909. doi:10.1001/jama.2022.4798
20. Hemphill JC
21. Warner JJ, Harrington RA, Sacco RL, Elkind MSV. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke. Stroke. 2019;50(12):3331–3332. doi:10.1161/strokeaha.119.027708
22. Connolly ES
23. Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. 2020;46(5):888–906. doi:10.1007/s00134-020-05980-0
24. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-z
25. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
26. Yang X, Yang B, Wu M, et al. Association between serum uric acid levels and benign paroxysmal positional vertigo: a systematic review and meta-analysis of observational studies. Front Neurol. 2019;10:91. doi:10.3389/fneur.2019.00091
27. Hallan DR, Simion C, Rizk E. Early versus late tracheostomy in spontaneous intracerebral hemorrhage. Cureus. 2022;14(4):e24059. doi:10.7759/cureus.24059
28. Alsherbini K, Goyal N, Metter EJ, et al. Predictors for tracheostomy with external validation of the stroke-related early tracheostomy score (SETscore). Neurocrit Care. 2019;30(1):185–192. doi:10.1007/s12028-018-0596-7
29. Catalino MP, Lin FC, Davis N, Anderson K, Olm-Shipman C, Jordan JD. Early versus late tracheostomy after decompressive craniectomy for stroke. J Intensive Care. 2018;6:1. doi:10.1186/s40560-017-0269-1
30. Chen W, Liu F, Chen J, Ma L, Li G, Timing YC. Outcomes of tracheostomy in patients with hemorrhagic stroke. World Neurosurg. 2019;131:e606–e613. doi:10.1016/j.wneu.2019.08.013
31. Gessler F, Mutlak H, Lamb S, et al. The impact of tracheostomy timing on clinical outcome and adverse events in poor-grade subarachnoid hemorrhage. Crit Care Med. 2015;43(11):2429–2438. doi:10.1097/ccm.0000000000001195
32. Villwock JA, Villwock MR, Deshaies EM. Tracheostomy timing affects stroke recovery. J Stroke Cerebrovasc Dis. 2014;23(5):1069–1072. doi:10.1016/j.jstrokecerebrovasdis.2013.09.008
33. de Carvalho Baptista IM, Martinho FC, Nascimento GG, da Rocha Santos CE, Prado RFD, Valera MC. Colonization of oropharynx and lower respiratory tract in critical patients: risk of ventilator-associated pneumonia. Arch Oral Biol. 2018;85:64–69. doi:10.1016/j.archoralbio.2017.09.029
34. Kasuya Y, Hargett JL, Lenhardt R, et al. Ventilator-associated pneumonia in critically ill stroke patients: frequency, risk factors, and outcomes. J Crit Care. 2011;26(3):273–279. doi:10.1016/j.jcrc.2010.09.006
35. Upadya A, Thorevska N, Sena KN, Manthous C, Amoateng-Adjepong Y. Predictors and consequences of pneumonia in critically ill patients with stroke. J Crit Care. 2004;19(1):16–22. doi:10.1016/j.jcrc.2004.02.004
36. van der Lely AJ, Veelo DP, Dongelmans DA, Korevaar JC, Vroom MB, Schultz MJ. Time to wean after tracheostomy differs among subgroups of critically ill patients: retrospective analysis in a mixed medical/surgical intensive care unit. Respir Care. 2006;51(12):1408–1415.
37. Pinheiro Bdo V, Tostes Rde O, Brum CI, Carvalho EV, Pinto SP, Oliveira JC. Early versus late tracheostomy in patients with acute severe brain injury. J Bras Pneumol. 2010;36(1):84–91. doi:10.1590/s1806-37132010000100014
38. Bösel J. Use and timing of tracheostomy after severe stroke. Stroke. 2017;48(9):2638–2643. doi:10.1161/strokeaha.117.017794
39. McCredie VA, Alali AS, Scales DC, et al. Effect of early versus late tracheostomy or prolonged intubation in critically ill patients with acute brain injury: a systematic review and meta-analysis. Neurocrit Care. 2017;26(1):14–25. doi:10.1007/s12028-016-0297-z
40. Robba C, Galimberti S, Graziano F, et al. Tracheostomy practice and timing in traumatic brain-injured patients: a CENTER-TBI study. Intensive Care Med. 2020;46(5):983–994. doi:10.1007/s00134-020-05935-5
41. Qureshi AI, Suarez JI, Parekh PD, Bhardwaj A. Prediction and timing of tracheostomy in patients with infratentorial lesions requiring mechanical ventilatory support. Crit Care Med. 2000;28(5):1383–1387. doi:10.1097/00003246-200005000-00020
42. Rabinstein AA, Wijdicks EF. Outcome of survivors of acute stroke who require prolonged ventilatory assistance and tracheostomy. Cerebrovasc Dis. 2004;18(4):325–331. doi:10.1159/000080771
43. Koch T, Hecker B, Hecker A, et al. Early tracheostomy decreases ventilation time but has no impact on mortality of intensive care patients: a randomized study. Langenbecks Arch Surg. 2012;397(6):1001–1008. doi:10.1007/s00423-011-0873-9
44. Santoli F, De Jonghe B, Hayon J, et al. Mechanical ventilation in patients with acute ischemic stroke: survival and outcome at one year. Intensive Care Med. 2001;27(7):1141–1146. doi:10.1007/s001340100998
45. Lessire H, Denis B, Vankeerberghen L, Weyers P. Prognosis of stroke patients undergoing mechanical ventilation. Intensive Care Med. 1996;22(2):174–175. doi:10.1007/bf01720727
46. Berrouschot J, Rössler A, Köster J, Schneider D. Mechanical ventilation in patients with hemispheric ischemic stroke. Crit Care Med. 2000;28(8):2956–2961. doi:10.1097/00003246-200008000-00045
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.