Back to Journals » Risk Management and Healthcare Policy » Volume 15
Early Readmission and Reoperation After Percutaneous Transforaminal Endoscopic Decompression for Degenerative Lumbar Spinal Stenosis: Incidence and Risk Factors
Authors Wang A, Si F, Wang T, Yuan S ![]() , Fan N, Du P, Wang L, Zang L
, Fan N, Du P, Wang L, Zang L ![]()
Received 30 August 2022
Accepted for publication 16 November 2022
Published 25 November 2022 Volume 2022:15 Pages 2233—2242
DOI https://doi.org/10.2147/RMHP.S388020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Aobo Wang,* Fangda Si,* Tianyi Wang, Shuo Yuan, Ning Fan, Peng Du, Lei Wang, Lei Zang
Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Zang, Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, 5 JingYuan Road, Shijingshan District, Beijing, 100043, People’s Republic of China, Tel +86 13601252787, Email [email protected]
Purpose: To identify the incidence rates and risk factors for early readmission and reoperation after percutaneous transforaminal endoscopic decompression (PTED) for degenerative lumbar spinal stenosis (DLSS).
Patients and Methods: A total of 1011 DLSS patients who underwent PTED were retrospectively evaluated. Of them, 58 were readmitted, and 31 underwent reoperation. The patients were matched with 174 control patients to perform case-control analyses. The clinical and preoperative imaging data of each patient were recorded. Univariate analyses were performed using independent sample t-tests and Fisher’s exact tests. Furthermore, the risk factors for early readmission and reoperation were analyzed using multivariate logistic regression analyses.
Results: The incidence rates of readmission and reoperation within 90 days after PTED were 5.7% and 3.1%, respectively. Age (odds ratio [OR]=1.054, p=0.001), BMI (OR=1.104, p=0.041), a history of lumbar surgery (OR=3.260, p=0.014), and the number of levels with radiological lumbar foraminal stenosis (LFS, OR=2.533, p< 0.001) were independent risk factors for early readmission. The number of levels with radiological LFS (OR=5.049, p< 0.001), the grade of surgical-level facet joint degeneration (OR=2.010, p=0.023), and a history of lumbar surgery (OR=10.091, p< 0.001) were independent risk factors for early reoperation.
Conclusion: This study confirmed that aging, a higher BMI, a history of lumbar surgery, and more levels with radiological LFS were associated with a higher risk of early readmission. More levels with radiological LFS, a higher grade of surgical-level facet joint degeneration, and a history of lumbar surgery were predictors of early reoperation. These results are helpful in patient counseling and perioperative evaluation of PTED.
Keywords: spinal stenosis, minimally invasive, readmission, reoperation, risk factor
Introduction
Degenerative lumbar spinal stenosis (DLSS) is a medical condition characterized by a diminished space available for neural and vascular elements in the lumbar spine secondary to degenerative changes.1 It is one of the main causes of low back and leg pain in geriatric patients. Approximately 10–20% of DLSS patients need surgical decompression after failed conservative treatment.2,3 In recent years, with the development of minimally invasive concepts, percutaneous transforaminal endoscopic decompression (PTED) has been considered as a surgical option for DLSS.4,5 Previous studies have demonstrated that PTED is an effective technique for treating DLSS.6,7 Compared with traditional posterior lumbar interbody fusion, it has the advantages of less trauma and faster rehabilitation.
Owing to the irreversibility of the disease and the complexity of the operation, reoperation and readmission are very common after spine surgery,8,9 increasing the physical and economic burden on patients. Early reoperation and readmission are particularly unacceptable.10,11 Thus, they have become important measures of quality of care.12,13 Many studies have investigated early reoperation and readmission rates after elective lumbar surgery. Identifying their incidence rates and risk factors is important in predicting patient prognosis and optimizing perioperative management.10,14
However, many previous studies aimed to reduce the financial penalty associated with readmission rates. Therefore, there are still some limitations. First, most previous studies did not stratify the different types of lumbar surgery. There are many differences in anesthesia, approach, surgical area, and trauma between different types of lumbar surgery. Thus, the incidence rates and risk factors for readmission and reoperation can be quite different among these techniques.10,11 Second, previous studies investigated demographic data and comorbidity conditions as potential risk factors; however, few of them reported radiological risk factors. Most early readmissions and reoperations are attributed to spine-related indications.13,15 Thus, preoperative evaluation of imaging parameters is valuable for predicting early adverse outcomes.16
In this study, we retrospectively reviewed the medical records and imaging data of patients with DLSS who underwent PTED at our institution. A case-control study was designed to investigate the incidence rates, reasons and risk factors for early readmission and reoperation after PTED.
Materials and Methods
Patient Selection
This study retrospectively evaluated 1011 consecutive patients with lateral recess or foraminal stenosis who underwent unilateral and single-level PTED at our institution between January 2016 and December 2021. The inclusion criteria were as follows: (1) age >40 years; (2) unilateral lateral recess or foraminal stenosis diagnosed on the basis of clinical symptoms and physical examination and imaging findings; and (3) symptoms with no relief after at least 3 months of conservative treatment. The exclusion criteria were as follows: (1) symptoms caused only by disc herniation; (2) instability or higher than grade I spondylolisthesis at the responsible level; (3) insufficient clinical or imaging data; and (4) concomitant conditions affecting the lumbar spine, including fractures, infections, and tumors. After reviewing the medical and follow-up data, we identified a group of patients with an unplanned readmission or reoperation within 90 days postoperatively. Thus, 58 and 31 patients were finally enrolled in the readmission and reoperation groups, respectively. To identify the risk factors for readmission and reoperation, we matched the patients with 174 control patients in a 1:3 ratio according to the date of operation (Figure 1). This study was performed in accordance with the Declaration of Helsinki and was approved by our institutional ethics committee.
 |
Figure 1 Flow chart of patient inclusion and exclusion. The exclusion criteria 1 and 2 are not shown in this figure, since patients with only lumbar disc herniation were excluded previously according to preoperative images, while patients with severe instability were excluded from the indications for lumbar endoscopy. |
Surgical Technique
The PTEDs were performed by a senior surgeon with an experience of more than 100 lumbar endoscopic procedures. In the patients with multilevel radiographic stenoses, local blocking was performed to identify the level of responsibility.
PTED was performed as follows: The patients were placed in the prone position, and the entire procedure was performed under local anesthesia. The entry point was set at 10–14 cm lateral to the midline at the index intervertebral level. A puncture needle was inserted into the superior articular process (SAP). The surgical approach was progressively expanded to 8 mm using a hollow -tapered cannula. A trepan was then used to remove the capsule and ventral side of the SAP to perform foraminoplasty. Decompression was performed using continuous irrigation under direct vision. The osteophytes, thickened ligament flavum, perineural fat, degenerated annulus fibrosus, and nucleus pulposus were removed. The traversing nerve root and dural sac were exposed with adequate mobility and good pulse to ensure complete decompression.
Data Collection
The clinical and radiological parameters of all the enrolled patients were collected. The preoperative clinical parameters included age, gender, body mass index (BMI), duration of symptoms, hypertension, diabetes mellitus, heart disease, cerebrovascular disease, chronic respiratory disease, chronic renal disease, current smoking, and alcohol consumption. The surgical level, duration of operation, and intraoperative blood loss (IBL) were recorded as the intraoperative parameters. The preoperative radiological parameters included lumbar lordosis and scoliosis, disc wedge,17 disc height index,18 Modic changes,19 Wildermuth grading of lumbar foraminal stenosis (LFS),20 Pfirrmann grading of disc degeneration,21 and Weishaupt grading of facet joint osteoarthritis.22 The above-mentioned degenerative grading systems were used at the surgical level. The number of levels with severe disc degeneration (higher than Pfirrmann grade 3) and radiological LFS (higher than Wildermuth grade 0) were also recorded.
The radiological measurements were performed as follows: All measurements were performed using the DICOM (version 3.1) viewer software (Neusoft PACS/RIS) by two experienced clinicians in a blinded fashion. For the quantitative measurements, the mean results were calculated. For the qualitative assessments, the results were recorded when the results obtained by the two clinicians were consistent. The remaining atypical cases were reassessed together by these clinicians.
The reasons, treatment, and days to readmission or reoperation were also collected for the patients who experienced readmissions and reoperations.
Statistical Analysis
For statistical analyses, data were analyzed using a statistical software (SPSS version 23.0 for Windows, IBM). Continuous variables were presented as means ± standard deviations. A univariate analysis was performed using independent sample t-tests for continuous variables and Fisher’s exact tests for categorical variables. The parameters with p-values of <0.10 in the univariate analysis were considered as potential risk factors and were included in the multivariate logistic regression analysis. The variance inflation factor (VIF) was used to determine collinearity. The Hosmer–Lemeshow (HL) goodness-of-fit and C-statistic tests were used to evaluate the fitness of the data and predictive power of the logistic regression model. Statistical significance was set at p<0.05.
Results
We retrospectively reviewed the medical records of 1011 patients. Among the patients, 58 were readmitted, and 31 underwent reoperation within 90 days postoperatively. The early readmission and reoperation rates were 5.7% and 3.1%, respectively. The mean times of readmission and reoperation were 35.7 and 33.7 days, respectively. Table 1 provides the indications for readmission and reoperation. Among the readmissions, 63.8% (37/58) were attributed to significant back or leg pain. The specific reasons included nerve root injury or edema, recurrent disc herniation, incomplete decompression, and adjacent segment stenosis. Non-spine-related admissions accounted for 25.9% (15/58) of all readmissions. The readmission times are summarized in Table 2. Most readmissions (31/58, 53.4%) occurred within 30 days postoperatively.
 |
Table 1 Indications for Reoperation and Readmission |
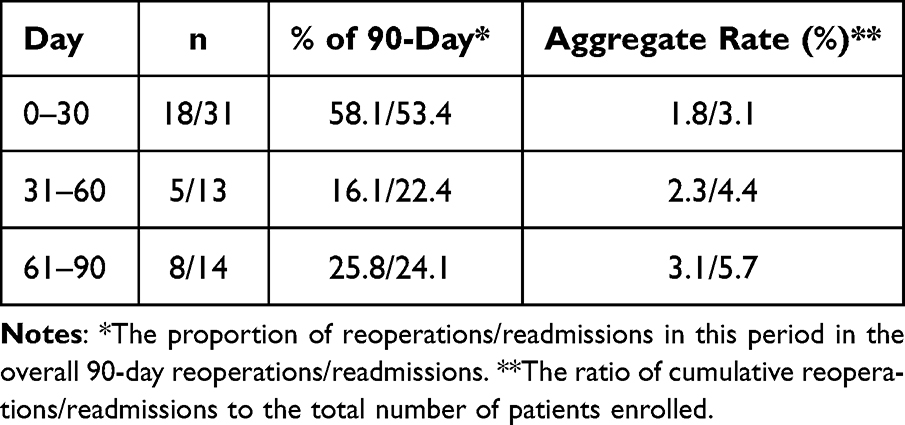 |
Table 2 Early Reoperation/Readmission Rates Stratified by the Time of Occurrence |
The clinical and imaging data of the patients in the readmission and control groups are shown in Table 3. The mean age (68.5 vs 61.4 years, p<0.001) and BMI (26.2 vs 25.1 kg/m2, p=0.032) were higher in the readmission group than in the control group. More patients in the readmission group had cerebrovascular disease (36.2% vs 19.0%, p=0.011), chronic respiratory disease (17.2% vs 7.5%, p=0.002), and a history of lumbar surgery (22.4% vs 7.5%, p=0.003) than those in the control group. There were no differences in gender (p=1.000), duration of symptoms (p=0.153), smoking status (p=0.732), drinking status (p=0.251), other comorbidities (p>0.05), surgical level (p=0.529), duration of operation (p=0.807), and IBL (p=0.239) between the two groups. The readmission group had a higher grade of surgical-level facet joint degeneration (1.6 vs 1.3, p=0.045) and a larger number of levels with radiological LFS (1.7 vs 1.2, p<0.001) than the control group. No significant differences were found in the other imaging parameters between the two groups (p>0.05).
 |
Table 3 Comparison of the Clinical and Imaging Parameters Between the Readmission and Control Groups |
Age, BMI, history of lumbar surgery, cerebrovascular disease, chronic respiratory disease, the grade of surgical-level facet joint degeneration, and the number of levels with radiological LFS were included in further multivariate logistic regression analyses (Table 4). There was no collinearity among the variables (VIFs<10). The multivariate logistic regression analysis demonstrated that age (odds ratio [OR]=1.054, 95% confidence interval [CI]=1.021–1.088, p=0.001), BMI (OR=1.104, 95% CI=1.004–1.214, p=0.041), history of lumbar surgery (OR=3.260, 95% CI=1.270–8.365, p=0.014), and the number of levels with radiological LFS (OR=2.533, 95% CI=1.552–4.134, p<0.001) were independent risk factors for early readmission (HL test, p=0.577; C-statistic=0.763). The number of levels with radiological LFS (OR=5.049, 95% CI=2.754–9.255, p<0.001), the grade of surgical-level facet joint degeneration (OR=2.010, 95% CI=1.100–3.674, p=0.023), and a history of lumbar surgery (OR=10.091, 95% CI=3.162–32.207, p<0.001) were independent risk factors for early reoperation (HL test, p=0.207; C-statistic =0.853).
 |
Table 4 Multivariate Regression Model of the Predictors for Early Readmission and Reoperation |
Discussion
Although many studies have described early readmission and reoperation after lumbar surgery, to the best of our knowledge, no previous study has specifically investigated PTED. This study retrospectively analyzed the readmission and reoperation risks after PTED for the treatment of DLSS. The 90-day readmission and reoperation rates were 5.7% and 3.1%, respectively. More than half of the readmitted patients experienced significant back or leg pain. Age, BMI, a history of lumbar surgery, and the number of levels with radiological LFS were independent risk factors for early readmission. The number of levels with radiological LFS, the grade of surgical-level facet joint degeneration, and a history of lumbar surgery were associated with a higher risk of early reoperation.
The reported 90-day readmission and reoperation rates after lumbar surgery were 2.5–24.8%10−13,23,24 and 2.0–7.1%,14,15,25 respectively. Some studies have investigated reoperation and readmission rates after certain surgical procedures. Kohls13 focused on microscopic discectomy and found a 90-day readmission rate of 5.3%. Patients who underwent spinal fusion seem to be more likely to be readmitted (9.7–24.8%).11,12,26 In this study, the 90-day reoperation and readmission rates after PTED were 3.1% and 5.7%, respectively, which are similar to those reported by Kohl. Thus, we cautiously speculate that the reoperation and readmission rates after minimally invasive procedures are lower than those after traditional spinal fusion. However, notably, previous studies have reported varying rates, although they were all based on large samples.10,11,23 A horizontal comparison is required in the future to determine whether there is a difference in the reoperation and readmission rates among different surgical indications and procedures.
Akamnonu15 investigated readmissions after open decompression with or without fusion and found that the most common causes of readmission were surgical site infection and other wound complications. Ilyas14 arrived at a similar conclusion that the most common indications for reoperation were surgical site infection, dural tear, and hematoma. In this study, we found that the most common reason for readmission and reoperation was persistent or recurrent pain, which accounted for 52.5% of all readmissions and 73.5% of all reoperations. This result differs from the previous findings. Unlike traditional open surgeries, PTED has a smaller incision, and the entire procedure is performed with continuous irrigation. Thus, the postoperative infection rate of PTED is significantly lower than that of open surgery. In addition, although dural tear is also a common complication of PTED, the injuries are usually not severe and can be treated conservatively.27 However, PTED cannot achieve thorough removal of compressive factors, resulting in the potential risk of incomplete decompression and postoperative recurrence.
Aging and a higher BMI often indicate a poor general condition. Thus, they are recognized predictors for readmission after lumbar surgery.24,28 However, the relationship between age and reoperations is complex. In this study, aging was significantly associated with readmission, but was not a risk factor for reoperation. We believe that many geriatric patients may refuse surgical treatment despite unsatisfactory outcomes after PTED. In a study based on data from the Spine Patient Outcomes Research Trial, Abdu29 proposed a similar opinion. In addition, we found differences in cerebrovascular and respiratory conditions between the patients in the readmission and control groups. These findings may be attributed to non-operative-related deterioration of the underlying diseases. This is supported by our results that comorbidities are not risk factors for readmission or reoperation. Previous studies have also concluded that comorbidities may be associated with non-operative readmission rather than all-cause readmission.14,24 To the best of our knowledge, there is no clear evidence that PTED, which is performed under local anesthesia, has a significant impact on diseases in other systems. Nonetheless, perioperative management remains important for improving postoperative recovery.30
In this study, 90.3% of the reoperations (28/31) were attributed to spine-related indications. Thus, we believe that imaging data, which are important in preoperative evaluation, may be helpful in predicting early readmission and reoperation. The multivariate analysis showed that the number of levels with radiological LFS was an independent risk factor for early reoperations. Multilevel degeneration often indicates an increased segmental stress force, a long disease course, an unclear spinal structure, and a severe adhesion, all of which increase the difficulty and risk of the operation.31,32 On the other hand, despite one of the stenotic levels being confirmed to be the responsible level in patients with multilevel stenoses, lesions at other levels may also lead to residual symptoms, which is necessary to be treated operatively. For patients who refuse or do not tolerate open decompression, a detailed perioperative assessment and notification of the possibility of further treatment are very important. We also found that a higher grade of surgical-level facet joint degeneration was associated with an early reoperation. Hypertrophy of the articular process leads not only to severe bony foraminal or lateral recess stenosis but also to difficulties in establishing a surgical approach.33 Our experience showed that insufficient foraminoplasty was common in the patients with severe facet joint degeneration, and residual osteophytes could be the cause of postoperative radicular symptoms. However, there was no significant association between the other imaging parameters and early readmission or reoperation. Many clinicians believe that disc degeneration is the initial factor of spinal stenosis.34,35 Severe disc degeneration and collapse can lead to restenosis. However, this process usually takes months to years.36 Early reoperation is mainly attributed to surgical complications or untreated pre-existing degeneration, which may explain why the disc degeneration grade was not associated with early reoperation in this study.
Notably, no significant difference was found in the intraoperative parameters, including the surgical level, duration of operation, and IBL, between the readmitted and control patients. The surgical procedure is still considered an important contributing factor.37 Our experience showed that significant adhesions and severe ossification during intraoperative exploration may be related to early surgical complications. In patients with a history of lumbar surgery, perineural adhesions and scars are particularly troublesome, resulting in a higher risk of complications and repeated revision.38,39 Placing the end of the working cannula at the lateral edge of the articular process, careful dissection of the disc and ligament flavum, detailed hemostasis, decompression of the nerve root to free pulsation instead of full exposure, and postoperative functional exercises are recommended to improve postoperative symptoms. Further studies are required to confirm these theories.
Based on the results, we believe that there are several things worth noting in clinical practice. First, the selection of surgical indication according to a thorough evaluation is very important. Classical theory holds that geriatric patients without poor physical conditions and patients with multilevel lumbar stenosis are more suitable for open decompression or spinal fusion.40,41 Because the lumbar degeneration is more severe in them, and a complete decompression and fusion is required. Although with the development of minimally invasive techniques, PTED can deal with complex degeneration and achieve satisfactory outcomes in geriatric patients,42 a comparative study is needed in the future to determine the optimal surgical choice. Second, for high-risk patients, clinicians should inform them of the possibility of surgical complications and recurrence after the treatment modality is determined. This helps in adjusting their psychological expectations and improving adherence in lifestyle modification. Third, for patients with severe facet joint osteoarthritis, a detailed surgical planning and careful intraoperative manipulation are helpful to establish an appropriate range of foraminoplasty, as is discussed above.
This study had several limitations. First, this was a retrospective study based on a relatively small sample size. However, some scholars believe that the records of single-center analyses are more detailed and accurate than those of multicenter or nationwide analyses.13,24 Second, socioeconomic factors were not considered in this study because the coverage rate of social medical insurance in the area where our institution is located has reached >95%. However, additional factors, such as commercial insurance, deserve further investigation. Third, the early reoperation and readmission rates of different surgical procedures were not compared in this study.
Conclusion
The early readmission and reoperation rates were 5.7% and 3.1%, respectively, after PTED for DLSS. Age, BMI, a history of lumbar surgery, and the number of levels with radiological LFS were independent risk factors for early readmission. The number of levels with radiological LFS, the grade of surgical-level facet joint degeneration, and a history of lumbar surgery were risk factors for early reoperation. A comprehensive evaluation and communication are required for patients with these characteristics during the perioperative period.
Data Sharing Statement
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study design was approved by the Ethics Review Committee of Beijing Chaoyang Hospital (Registration number: 2021-8-5-5), and no administrative permission was required to access the raw data for this study. In addition, all subjects provided informed consent prior to participation. All methods in the study were carried out in accordance with the Helsinki guidelines and declaration.
Funding
There is no funding that supported this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kreiner DS, Shaffer WO, Baisden JL, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J. 2013;13(7):734–743. doi:10.1016/j.spinee.2012.11.059
2. Choi WS, Oh CH, Ji GY, et al. Spinal canal morphology and clinical outcomes of microsurgical bilateral decompression via a unilateral approach for lumbar spinal canal stenosis. Eur Spine J. 2014;23(5):991–998. doi:10.1007/s00586-013-3116-7
3. Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol. 2010;24(2):253–265. doi:10.1016/j.berh.2009.11.001
4. Pan M, Li Q, Li S, et al. Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician. 2020;23(1):49–56.
5. Ahn Y. Percutaneous endoscopic decompression for lumbar spinal stenosis. Expert Rev Med Devices. 2014;11(6):605–616. doi:10.1586/17434440.2014.940314
6. Lee CW, Yoon KJ, Kim SW. Percutaneous endoscopic decompression in lumbar canal and lateral recess stenosis - the surgical learning curve. Neurospine. 2019;16(1):63–71. doi:10.14245/ns.1938048.024
7. Li P, Tong Y, Chen Y, Zhang Z, Song Y. Comparison of percutaneous transforaminal endoscopic decompression and short-segment fusion in the treatment of elderly degenerative lumbar scoliosis with spinal stenosis. BMC Musculoskelet Disord. 2021;22(1):906. doi:10.1186/s12891-021-04804-6
8. Park MS, Ju YS, Moon SH, et al. Reoperation rates after posterior lumbar spinal fusion surgery according to preoperative diagnoses: a national population-based cohort study. Clin Neurol Neurosurg. 2019;184:105408. doi:10.1016/j.clineuro.2019.105408
9. Weir S, Kuo TC, Samnaliev M, et al. Reoperation following lumbar spinal surgery: costs and outcomes in a UK population cohort study using the Clinical Practice Research Datalink (CPRD) and Hospital Episode Statistics (HES). Eur Spine J. 2019;28(4):863–871. doi:10.1007/s00586-018-05871-5
10. Wadhwa RK, Ohya J, Vogel TD, et al. Risk factors for 30-day reoperation and 3-month readmission: analysis from the quality and outcomes database lumbar spine registry. J Neurosurg Spine. 2017;27(2):131–136. doi:10.3171/2016.12.SPINE16714
11. Baaj AA, Lang G, Hsu WC, Avila MJ, Mao J, Sedrakyan A. 90-day readmission after lumbar spinal fusion surgery in new york state between 2005 and 2014: a 10-year analysis of a statewide cohort. Spine. 2017;42(22):1706–1716. doi:10.1097/BRS.0000000000002208
12. Chen SA, White RS, Tangel V, Nachamie AS, Witkin LR. Sociodemographic characteristics predict readmission rates after lumbar spinal fusion surgery. Pain Med. 2020;21(2):364–377. doi:10.1093/pm/pny316
13. Kohls MR, Jain N, Khan SN. What are the rates, reasons, and risk factors of 90-day hospital readmission after lumbar discectomy?: An institutional experience. Clin Spine Surg. 2018;31(8):E375–E380. doi:10.1097/BSD.0000000000000672
14. Ilyas H, Golubovsky JL, Chen J, Winkelman RD, Mroz TE, Steinmetz MP. Risk factors for 90-day reoperation and readmission after lumbar surgery for lumbar spinal stenosis. J Neurosurg Spine. 2019;31(1):20–26. doi:10.3171/2019.1.SPINE18878
15. Akamnonu C, Cheriyan T, Goldstein JA, Lafage V, Errico TJ, Bendo JA. Unplanned hospital readmission after surgical treatment of common lumbar pathologies: rates and causes. Spine. 2015;40(6):423–428. doi:10.1097/BRS.0000000000000759
16. Shi H, Zhu L, Jiang ZL, Wu XT. Radiological risk factors for recurrent lumbar disc herniation after percutaneous transforaminal endoscopic discectomy: a retrospective matched case-control study. Eur Spine J. 2021;30(4):886–892. doi:10.1007/s00586-020-06674-3
17. Cho JH, Lee CS, Lee DH, et al. Disc wedge and vertebral body tilt angle below lower instrumented vertebra after posterior correction and fusion in patients with a structural thoracolumbar/lumbar curve: a minimum 5-year follow-up. Spine. 2019;44(24):E1436–E1442. doi:10.1097/BRS.0000000000003164
18. Akeda K, Yamada T, Inoue N, Nishimura A, Sudo A. Risk factors for lumbar intervertebral disc height narrowing: a population-based longitudinal study in the elderly. BMC Musculoskelet Disord. 2015;16:344. doi:10.1186/s12891-015-0798-5
19. Braithwaite I, White J, Saifuddin A, Renton P, Taylor BA. Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lumbar discography. Eur Spine J. 1998;7(5):363–368. doi:10.1007/s005860050091
20. Wildermuth S, Zanetti M, Duewell S, et al. Lumbar spine: quantitative and qualitative assessment of positional (upright flexion and extension) MR imaging and myelography. Radiology. 1998;207(2):391–398. doi:10.1148/radiology.207.2.9577486
21. Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine. 2001;26(17):1873–1878. doi:10.1097/00007632-200109010-00011
22. Weishaupt D, Zanetti M, Boos N, Hodler J. MR imaging and CT in osteoarthritis of the lumbar facet joints. Skeletal Radiol. 1999;28(4):215–219. doi:10.1007/s002560050503
23. Rubel NC, Chung AS, Wong M, et al. 90-day readmission in elective primary lumbar spine surgery in the inpatient setting: a nationwide readmissions database sample analysis. Spine. 2019;44(14):E857–E864. doi:10.1097/BRS.0000000000002995
24. Canseco JA, Karamian BA, Minetos PD, et al. Risk factors for 30-day and 90-day readmission after lumbar decompression. Spine. 2022;47(9):672–679. doi:10.1097/BRS.0000000000004325
25. Leven D, Passias PG, Errico TJ, et al. Risk factors for reoperation in patients treated surgically for intervertebral disc herniation: a subanalysis of eight-year SPORT data. J Bone Joint Surg Am. 2015;97(16):1316–1325. doi:10.2106/JBJS.N.01287
26. Cui JJ, Gala RJ, Ondeck NT, et al. Incidence and considerations of 90-day readmissions following posterior lumbar fusion. Spine J. 2019;19(4):631–636. doi:10.1016/j.spinee.2018.09.004
27. Fan N, Yuan S, Du P, et al. Complications and risk factors of percutaneous endoscopic transforaminal discectomy in the treatment of lumbar spinal stenosis. BMC Musculoskelet Disord. 2021;22(1):1041. doi:10.1186/s12891-021-04940-z
28. Kim JM, Lee SH, Ahn Y, Yoon DH, Lee CD, Lim ST. Recurrence after successful percutaneous endoscopic lumbar discectomy. Minim Invasive Neurosurg. 2007;50(2):82–85. doi:10.1055/s-2007-982504
29. Abdu RW, Abdu WA, Pearson AM, Zhao W, Lurie JD, Weinstein JN. Reoperation for recurrent intervertebral disc herniation in the spine patient outcomes research trial: analysis of rate, risk factors, and outcome. Spine. 2017;42(14):1106–1114. doi:10.1097/BRS.0000000000002088
30. Chapin L, Ward K, Ryken T. Preoperative depression, smoking, and employment status are significant factors in patient satisfaction after lumbar spine surgery. Clin Spine Surg. 2017;30(6):E725–E732. doi:10.1097/BSD.0000000000000331
31. Cai XY, Sun MS, Huang YP, et al. Biomechanical effect of L4 -L5 intervertebral disc degeneration on the lower lumbar Spine: a finite element study. Orthop Surg. 2020;12(3):917–930. doi:10.1111/os.12703
32. Chen X, Qin R, Hao J, et al. Percutaneous endoscopic decompression via transforaminal approach for lumbar lateral recess stenosis in geriatric patients. Int Orthop. 2019;43(5):1263–1269. doi:10.1007/s00264-018-4051-3
33. O’Leary SA, Paschos NK, Link JM, Klineberg EO, Hu JC, Athanasiou KA. Facet joints of the spine: structure-function relationships, problems and treatments, and the potential for regeneration. Annu Rev Biomed Eng. 2018;20:145–170. doi:10.1146/annurev-bioeng-062117-120924
34. Haimoto S, Nishimura Y, Hara M, et al. Clinical and radiological outcomes of microscopic lumbar foraminal decompression: a pilot analysis of possible risk factors for restenosis. Neurol Med Chir (Tokyo). 2018;58(1):49–58. doi:10.2176/nmc.oa.2017-0121
35. Blumenthal C, Curran J, Benzel EC, et al. Radiographic predictors of delayed instability following decompression without fusion for degenerative grade I lumbar spondylolisthesis. J Neurosurg Spine. 2013;18(4):340–346. doi:10.3171/2013.1.SPINE12537
36. Miyahara J, Yoshida Y, Nishizawa M, et al. Treatment of restenosis after lumbar decompression surgery: decompression versus decompression and fusion. J Neurosurg Spine;2022. 1–8. doi:10.3171/2021.10.SPINE21728
37. Scholler K, Steingruber T, Stein M, et al. Microsurgical unilateral laminotomy for decompression of lumbar spinal stenosis: long-term results and predictive factors. Acta Neurochir. 2016;158(6):1103–1113. doi:10.1007/s00701-016-2804-6
38. Liang JQ, Chen C, Zhao H. Revision surgery after percutaneous endoscopic transforaminal discectomy compared with primary open surgery for symptomatic lumbar degenerative disease. Orthop Surg. 2019;11(4):620–627. doi:10.1111/os.12507
39. Yao Y, Zhang H, Wu J, et al. Comparison of three minimally invasive spine surgery methods for revision surgery for recurrent herniation after percutaneous endoscopic lumbar discectomy. World Neurosurg. 2017;100:641–647. doi:10.1016/j.wneu.2017.01.089
40. Kim CH, Chung CK, Choi Y, et al. The selection of open or percutaneous endoscopic lumbar discectomy according to an age cut-off point: nationwide cohort study. Spine. 2015;40(19):E1063–E1070. doi:10.1097/BRS.0000000000001053
41. Lee JK, Amorosa L, Cho SK, Weidenbaum M, Kim Y. Recurrent lumbar disk herniation. J Am Acad Orthop Surg. 2010;18(6):327–337. doi:10.5435/00124635-201006000-00005
42. Cheng XK, Chen B. Percutaneous transforaminal endoscopic decompression for geriatric patients with central spinal stenosis and degenerative lumbar spondylolisthesis: a novel surgical technique and clinical outcomes. Clin Interv Aging. 2020;15:1213–1219. doi:10.2147/CIA.S258702
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Results of 10-mm Endoscopic Minimally Invasive Interlaminar Decompression in the Treatment of Lumbar Spinal Stenosis with Degenerative Lumbar Scoliosis and Simple Lumbar Spinal Stenosis
Li P, Shi Z, Jiang Y, Peng Z, Wang Y
Clinical Interventions in Aging 2023, 18:911-919
Published Date: 7 June 2023