")
Back to Journals » Clinical Interventions in Aging » Volume 18
Clinical Results of 10-mm Endoscopic Minimally Invasive Interlaminar Decompression in the Treatment of Lumbar Spinal Stenosis with Degenerative Lumbar Scoliosis and Simple Lumbar Spinal Stenosis
Authors Li P, Shi Z, Jiang Y, Peng Z, Wang Y
Received 28 March 2023
Accepted for publication 30 May 2023
Published 7 June 2023 Volume 2023:18 Pages 911—919
DOI https://doi.org/10.2147/CIA.S414559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Pengfei Li,1 Zhen Shi,1 Yunduo Jiang,1 Zhibin Peng,1 Yansong Wang1– 3
1Department of Orthopedic Surgery, the First Affiliated Hospital of Harbin Medical University, Harbin Medical University, Harbin, People’s Republic of China; 2NHC Key Laboratory of Cell Transplantation, Harbin Medical University, Harbin, People’s Republic of China; 3Heilongjiang Provincial Key Laboratory of Hard Tissue Development and Regeneration, Harbin Medical University, Harbin, People’s Republic of China
Correspondence: Yansong Wang, Department of Orthopedics, the First Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang Province, 150001, People’s Republic of China, Email [email protected]
Purpose: The number of patients with lumbar spinal stenosis (LSS) with degenerative lumbar scoliosis (DLS) is gradually increasing as the population ages. The purpose of this study was to evaluate the clinical outcomes of 10-mm endoscopic minimally invasive interlaminar decompression for LSS with DLS and simple LSS.
Material and Methods: The clinical data of 175 consecutive elderly patients with LSS were retrospectively analyzed. They were divided into LSS group and LSS with DLS group based on whether they were accompanied by DLS. Patient demographics, perioperative indicators, and clinical outcomes were recorded. Lumbar spine stability was assessed by imaging data. Meanwhile, visual analog scale (VAS) scores, Oswestry Disability Index (ODI) scores, and the modified Macnab criteria were used to assess clinical outcomes.
Results: There were 129 patients in the LSS group and 46 patients in the LSS with DLS group. Both groups had similar VAS and ODI scores preoperatively, and both were significantly lower postoperatively (P < 0.05). However, patients combined with DLS showed higher VAS scores for low back pain at 3 months and 1 year postoperatively (P < 0.05). In addition, postoperative LL and PI-LL were significantly improved in both groups (P < 0.05). However, patients in LSS with DLS group showed higher PT, PI and PI-LL before and after surgery. According to the modified Macnab criteria, the excellent and good rates were 92.25% and 89.13% in the LSS group and LSS with DLS group at the last follow-up, respectively.
Conclusion: 10-mm endoscopic minimally invasive interlaminar decompression for LSS with or without DLS has shown satisfactory clinical outcomes. However, patients with DLS may have higher residual low back pain after surgery.
Keywords: spinal stenosis, scoliosis, endoscope, minimally invasive, decompression, geriatric patients
Introduction
Degenerative lumbar scoliosis (DLS) is defined as a spinal deformity with a Cobb angle greater than 10° in the coronal plane that develops after skeletal maturation.1 This condition is characterized by mild lateral bending, loss of lumbar anterior convexity and multilevel instability.2 The etiology of DLS is complex and closely related to disc degeneration.3–5 The prevalence of DLS varies between 13% to 68% and increases with age.6 As a degenerative spine disease, DLS is often accompanied by the degeneration of intervertebral discs, ligaments, and facet joints. Therefore, the coexistence of lumbar scoliosis and lumbar spinal stenosis (LSS) is common in the elderly population.2 These patients often suffer from low back pain, radiculopathy and neurogenic claudication.7 This reduces the mobility and quality of life of patients to a great extent. As the population ages, the proportion of elderly will further increase, which poses a challenge to the management of DLS.
Conservative treatments such as medications, physical therapy, functional exercises, and epidural steroid injections are typically recommended as primary treatments for LSS.8,9 However, surgery may be necessary if conservative treatment fails to produce the desired results. For LSS patients with DLS, surgery can be complicated due to the potential impact of spinal deformity. While fixed fusion surgery can correct spinal imbalances and improve postoperative outcomes for DLS patients,10,11 it also has a high complication rate and mortality in a large elderly population.12 Decompression alone is considered to be a less invasive procedure that can significantly reduce the complication rate in patients with DLS.13 However, it is still unclear whether decompression without correction of the deformity will worsen its progression. The new 10-mm endoscope enables efficient decompression of spinal stenosis using specialized surgical instruments such as laminectomy rongeurs. This approach involves a small incision of approximately 10 mm, reducing bone destruction and protecting the paravertebral muscles, and further preserving spinal stability.14 This study reports the clinical outcomes of 10-mm endoscopic minimally invasive interlaminar decompression in the treatment of elderly LSS with or without DLS, with the aim of providing a reference for clinical practice.
Materials and Methods
Participants
This study was approved by our institutional review board, and all patients provided written consent. Between September 2019 and March 2022, a total of 175 elderly patients with LSS who underwent this procedure were consecutively enrolled (Figure 1). According to whether accompanied by DLS or not, they were divided into LSS group and LSS with DLS group. The procedures were all performed by the same surgeon. The inclusion criteria were as follows: (1) intermittent claudication or unilateral lower extremity radicular pain; (2) imaging manifestations consistent with symptoms; (3) LSS with or without DLS; (4) single-level lumbar spinal stenosis requiring treatment; and (5) ineffective conservative treatment for more than three months. The exclusion criteria were as follows: (1) age<60 years; (2) low back pain more severe than leg pain; (3) Cobb angle greater than 30° in the coronal plane; (4) patients with isthmic spondylolisthesis or dynamic X-ray showing motion greater than 3 mm; (5) pathological conditions such as tumor, trauma, and infection; and (6) lost to follow-up. Preoperative demographic characteristics, perioperative conditions, and clinical outcomes were recorded.
 |
Figure 1 Flowchart of patient eligibility screening. |
Surgical Procedure
Clarification of the Level of Responsibility
The level of responsibility is determined based on the patient’s physical examination and imaging findings. For patients with severe degeneration that makes it difficult to determine the responsible segment, a diagnostic nerve root block was performed prior to surgery. Using the G-arm as a guide, 1 mL of 2% lidocaine was injected transforaminally around the suspected nerve. If more than half of the pain in the lower extremity was relieved, the segment was considered responsible.
Surgical Procedure
The patient was placed in the prone position, and the procedure was completed under local infiltration anesthesia (Figure 2). The responsible segment was located using the G-arm X-ray machine, and the operative area was routinely disinfected. A surgical incision about 1 cm was made at the level of the responsible intervertebral space in line with the lateral edge of the vertebral body. The soft tissue dilators were used to dilate the vertebral plate space step by step, followed by placement of the working channel. A 10-mm endoscope (Spinendos GmbH, München, Germany) was then inserted. If necessary, the intervertebral space was enlarged by removing part of the bone using a burr and a laminectomy rongeur. The sublaminar ligamentum flavum was removed to expose the epidural space and the nerve root canal. After probing and releasing the nerve root and peridural sac adhesions, 3 ~ 5 mL of 2% lidocaine was injected into the epidural space. Shortly after induction of local anesthesia, the nerve root was gently pushed medially. Decompression of the spinal canal was then performed. When the endoscopic observation of the nerve root and dural sac compression was released, the procedure could be concluded.
 |
Figure 2 (A) Intraoperative anterior-posterior image. (B) Intraoperative lateral image. (C) Endoscope burr in use. (D) Removed compression-causing tissue. |
Measures
Evaluation of Imaging Parameters
The coronal Cobb angle was selected to evaluate coronal balance. Lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), and pelvic incidence-lumbar lordosis (PI-LL) were selected to measure the sagittal balance of the spinopelvic in patients with DLS.
Evaluation of Clinical Efficacy
Visual analog scale (VAS) and Oswestry Disability Index (ODI) were used to evaluate clinical outcomes before operation, 1 week after operation, 3 months after operation, and 12 months after operation. Furthermore, surgical satisfaction was assessed using the modified Macnab criteria at final follow-up.
Statistical Assessments
The statistical calculations were performed using the SPSS 26 program (IBM, Armonk, USA). The results are presented as mean and standard deviation (SD) values. The demographics, radiological values, and clinical outcomes of the two groups were analyzed by Student’s t test or Mann–Whitney U-test. The significance level was defined as p < 0.05.
Results
Preoperative Demographic Characteristics and Outcomes
Preoperative demographic characteristics are shown in Table 1. A total of 175 patients participated in this study. There were 129 patients in the LSS group with a mean age of 69.89±7.29 years. The LSS with DLS group had 46 patients with a mean age of 71.43±7.89 years. There were no statistical differences in age, gender, body mass index (BMI), disease duration, and surgical segment between the two groups.
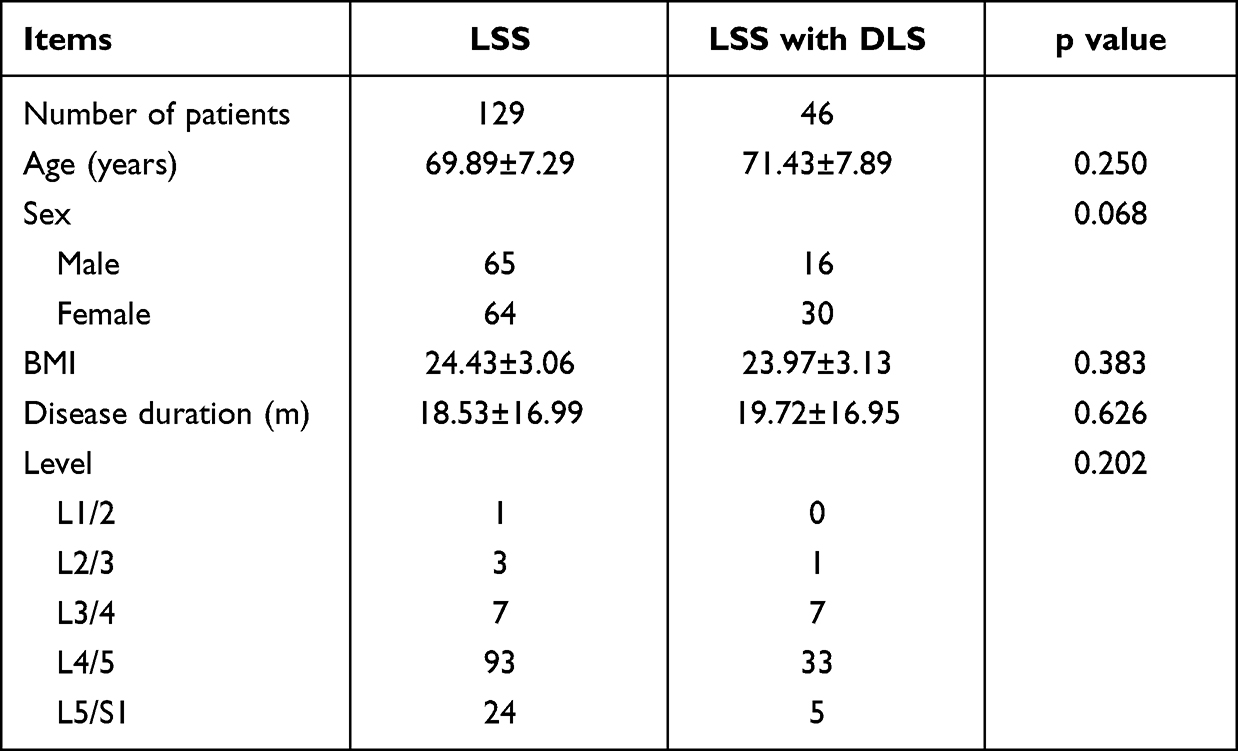 |
Table 1 Demographic Characteristics of the Two Groups |
Perioperative Indicators and Complications
As Table 2, there was no significant difference between the two groups in terms of operative time, postoperative hospital days and major complication rates (P > 0.05).
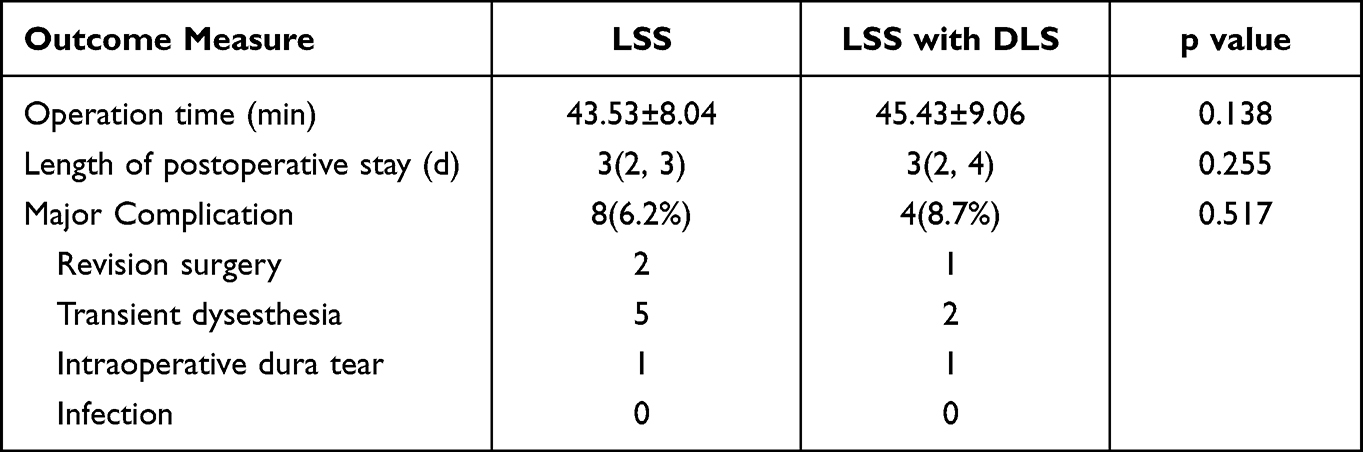 |
Table 2 Perioperative Indicators and Complications of the Two Groups |
Clinical Results
The improvement of patients’ clinical symptoms was assessed using the VAS score and ODI score (Figure 3). There was no significant difference in the preoperative VAS scores for low back pain between the two groups, and both groups improved significantly after surgery (P < 0.05). However, the LSS with DLS group exhibited higher low back pain VAS scores at 3 months and 1 year postoperatively. Both groups had similar improvements in VAS leg pain scores and ODI scores after surgery, with no statistically significant differences between the groups (P > 0.05). According to the modified MacNab criteria, the excellent and good rates at the final follow-up were 92.25% and 89.13% in the LSS group and the LSS with DLS group, respectively, with no statistically significant differences.
 |
Figure 3 Clinical outcomes of patients in both groups at different follow-up time points. (A) VAS-back pain score (☆: P < 0.05). (B) VAS-leg pain score. (C) Oswestry Disability Index. (D) the Modified Macnab criteria. |
Changes in radiographic parameters are presented in Table 3. Patients with simple LSS exhibited a loss of LL and imbalance of the spinopelvic region before the operation. However, their LL and PI-LL improved significantly postoperatively compared to preoperative values. Patients with DLS had similar changes in imaging parameters as those with simple LSS. However, DLS patients showed significantly higher PT, PI, and PI-LL before and after surgery, with statistically significant differences between the groups. Moreover, the coronal Cobb angles of DLS patients were 17.2±4.9° and 18.0±4.4° preoperatively and at 1 year postoperatively, respectively, with no statistically significant difference (P>0.05).
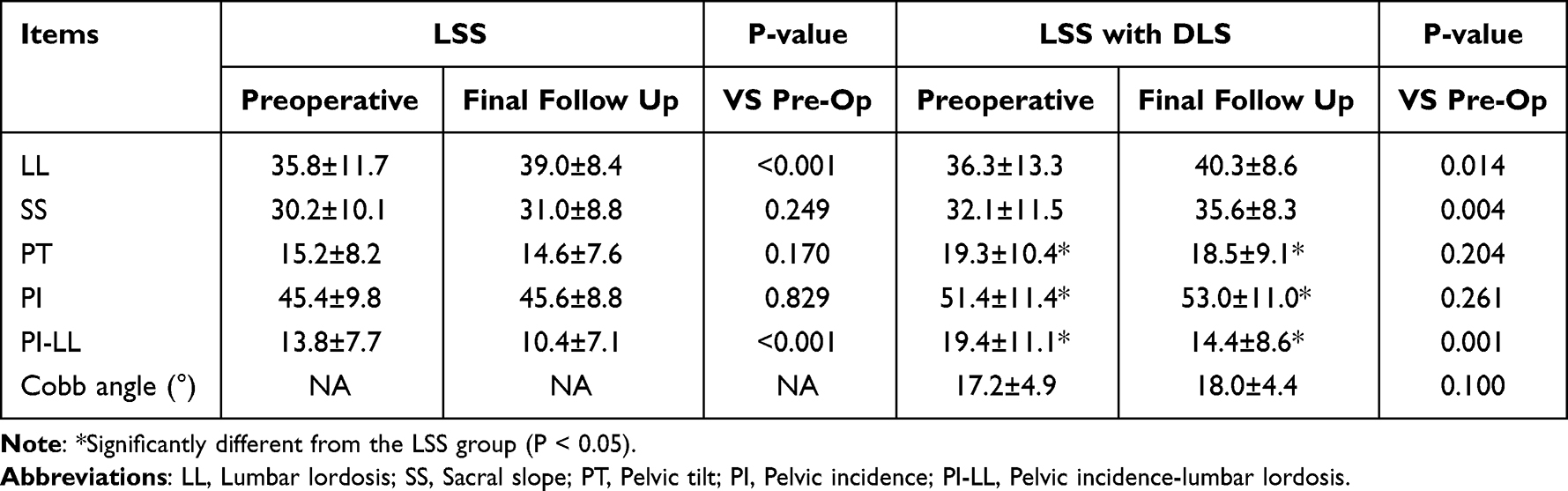 |
Table 3 Comparison of Imaging Parameters Between the Two Groups of Patients |
As in Figure 4, the 10-mm endoscopic technique achieves adequate decompression at the level of responsibility.
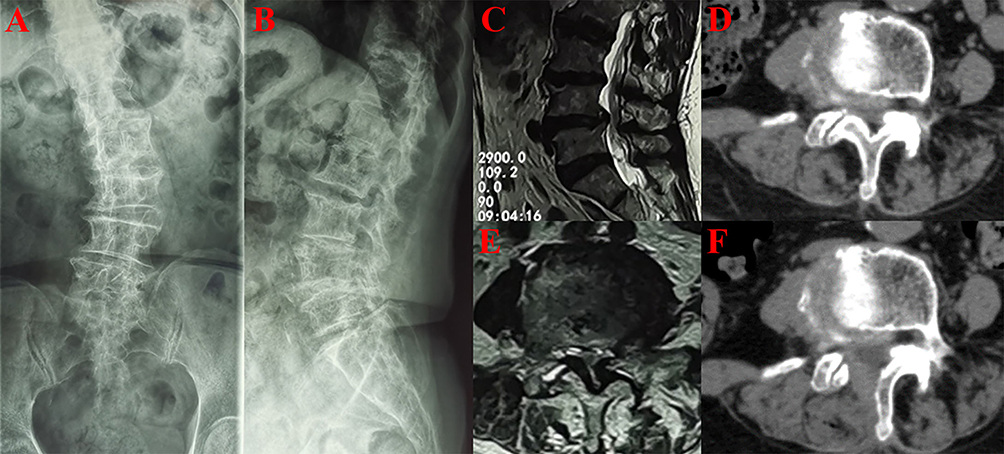 |
Figure 4 Imaging images of an 83-year-old DLS patient with L4/5 as the responsible segment. (A and B) X-rays showing degenerative deformity of the patient’s lumbar spine. (C and E) Preoperative lumbar MRI (Magnetic Resonance Imaging) showed severe spinal stenosis. (D and F) Axial CT (Computed Tomography) images of the lumbar spine show adequate decompression. |
Discussion
The ideal surgical approach for patients with DLS remains an intriguing topic. In this study, we observed the clinical outcomes of LSS with and without DLS. Both groups benefited from the 10-mm endoscopic procedure and showed responsive improvement in sagittal imbalance. However, patients with combined DLS may experience higher postoperative low back pain compared to those with simple LSS.
LSS is a very common degenerative disease of the spine, that affects millions of people worldwide.15 It is the fastest-growing disease in the United States among older adults who undergo lumbar spine surgery.16 As the population ages, more and more LSS patients are diagnosed with concomitant DLS.17,18 However, the management of DLS remains variable due to the lack of a clear evidence-based treatment approach. Surgical management of DLS includes decompression alone, short-segment fusion, and long-segment fusion, but there is conflicting evidence and wide variation in practice between them.1,19–21 Studies have shown that patients with DLS have similar imaging findings compared to those with simple LSS, including ligamentum flavum hypertrophy, bulging discs, and facet joint degeneration.22 Since LSS and DLS mainly affect an elderly population with poor surgical tolerance, less invasive decompression alone is an indispensable surgical option for elderly patients with DLS. Minimally invasive endoscopic decompression has been effectively used in elderly patients with LSS.23,24 But it has been less reported in the treatment of DLS. In the study, we used a 10-mm endoscope, which had a larger operating space and was more efficient in decompression operations. The advantages of local anesthesia and minimally invasive efficiency are particularly important for elderly patients with poor physical condition. Therefore, we believe that the application of this technique is appropriate for patients with DLS who require surgical intervention.
For patients with severe DLS, correcting the deformity may be crucial. However, for elderly patients with mild scoliosis and without significant back pain, the primary treatment goal should be alleviating the clinical symptoms caused by stenosis. In this study, the preoperative Cobb angle in DLS patients was 17.2 ± 4.9°. One year after surgery, the mean Cobb angle was 18.0±4.4°, which was not statistically significant compared to the preoperative period. The cobb angles of DLS patients in this group were maintained, which may benefit from the advantage of 10-mm endoscopic surgery. Because the function of the paravertebral muscles in the back has decreased in elderly patients with DLS.25 Compared to open surgery, endoscopic decompression is known to reduce the disruption of the back muscles. In addition, we have learned that the intervertebral disc can withstand up to 67% of the shear load, while the facet joints provide a maximum of approximately 49% stability during axial rotation.26 The interlaminar approach provides better protection of the disc and the facet joints compared to the posterolateral approach. Therefore, we recommend preserving these stability-maintaining structures in patients with DLS to avoid further disruption of the stabilizing structures.
Spinopelvic sagittal balance is another critical consideration following lumbar decompression surgery. Previous studies have shown that spinopelvic sagittal alignment plays a significant role in pain and functional decline in adult spinal deformities.27 Several radiological parameters, including LL, PI, PT, SS, and PI-LL, are essential to assess spinopelvic sagittal balance in patients with DLS. In particular, LL, PI, and PI-LL have been found to be closely associated with postoperative quality of life in patients with DLS.28–30 The elderly patients in this study had varying degrees of LL loss and PI-LL mismatch and were also faced with the challenges of advanced age and low surgical tolerance. Compared to the simple LSS group, DLS patients showed greater PI-LL both preoperatively and postoperatively. Fixed fusion surgery is more effective at correcting sagittal imbalance, but is also more risky, particularly for elderly patients with low surgical tolerance. In a previous study, nonfusion decompression surgery improved sagittal alignment in patients with spinal stenosis.31 The results of our study supported this idea. Both groups of patients demonstrated improved LL and PI-LL after surgery. However, DLS patients were more likely to have residual low back pain postoperatively, possibly due to a higher postoperative PI-LL. A study by Ogon I32 demonstrated that PI-LL was a significant predictor of low back pain in patients with LSS, while Gao A et al33 reported that DLS patients with PI-LL>20° had significantly higher dysfunction caused by low back pain than those with PI-LL<20°. In this study, postoperative PI-LL was significantly higher in patients with DLS than in those with simple LSS, which may account for the higher residual postoperative low back pain in DLS patients. It is important to clarify that although both groups achieved promising clinical outcomes at final follow-up, there is no evidence that minimally invasive endoscopic decompression is indicated for all types of DLS. In cases of severe scoliosis deformity, fixed fusion may still be necessary.
The current study still has some limitations. Firstly, the retrospective design may lead to potential selection bias, and the small sample size may reduce the rigor of our results. Secondly, the learning curve for endoscopic surgery is high, especially for elderly patients with spinal deformities. Finally, the short observation period of this study also requires long-term follow-up.
Conclusion
With an aging population, surgeons need to consider both surgical risks and healthcare costs. Compared with simple LSS, patients with DLS have achieved promising clinical outcomes. Therefore, 10-mm endoscopic interlaminar decompression under local anesthesia may be considered an effective alternative option for the treatment of patients combined with mild DLS.
Abbreviations
LSS, Lumbar spinal stenosis; DLS, Degenerative lumbar scoliosis; LL, Lumbar lordosis; PI, Pelvic incidence; PT, Pelvic tilt; SS, Sacral slope; PI-LL, Pelvic incidence-lumbar lordosis; VAS, Visual analog scale; ODI, Oswestry disability index.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
This retrospective study was approved by the Ethics Committee of the The First Affiliated Hospital of Harbin Medical University, and written informed consent was obtained from participants prior to data collection. This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
We have obtained the consent for publication from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have received no external funding in order to support this project.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Silva FE, Lenke LG. Adult degenerative scoliosis: evaluation and management. Neurosurg Focus. 2010;28(3):E1.
2. Ha KY, Kim YH, Kim SI, Park HY, Seo JH. Decompressive Laminectomy Alone for Degenerative Lumbar Scoliosis with Spinal Stenosis: incidence of Post-Laminectomy Instability in the Elderly. Clin Orthop Surg. 2020;12(4):493–502.
3. Bao H, Zhu F, Liu Z, et al. Coronal curvature and spinal imbalance in degenerative lumbar scoliosis: disc degeneration is associated. Spine. 2014;39(24):E1441–1447.
4. Aebi M. The adult scoliosis. Eur Spine J. 2005;14(10):925–948.
5. Kobayashi T, Atsuta Y, Takemitsu M, Matsuno T, Takeda N. A prospective study of de novo scoliosis in a community based cohort. Spine. 2006;31(2):178–182.
6. McAviney J, Roberts C, Sullivan B, Alevras AJ, Graham PL, Brown BT. The prevalence of adult de novo scoliosis: a systematic review and meta-analysis. Eur Spine J. 2020;29(12):2960–2969.
7. Xu F, Jiang S, Wang L, et al. Motion of Lumbar Endplate in Degenerative Lumbar Scoliosis Patients with Different Cobb Angle In Vivo: reflecting the Biomechanics of the Lumbar Disc. Biomed Res Int. 2022;2022:8745683.
8. Diebo BG, Shah NV, Boachie-Adjei O, et al. Adult spinal deformity. Lancet. 2019;394(10193):160–172.
9. Bussières A, Cancelliere C, Ammendolia C, et al. Non-Surgical Interventions for Lumbar Spinal Stenosis Leading To Neurogenic Claudication: a Clinical Practice Guideline. J Pain. 2021;22(9):1015–1039.
10. Liang Y, Tang X, Zhao Y, et al. Limited correction of lumbar lordosis in the treatment of degenerative scoliosis. Medicine. 2020;99(19):e19624.
11. Lak AM, Lamba N, Pompilus F, et al. Minimally invasive versus open surgery for the correction of adult degenerative scoliosis: a systematic review. Neurosurg Rev. 2021;44(2):659–668.
12. Acosta FL, McClendon J, O’Shaughnessy BA, et al. Morbidity and mortality after spinal deformity surgery in patients 75 years and older: complications and predictive factors. J Neurosurg Spine. 2011;15(6):667–674.
13. Transfeldt EE, Topp R, Mehbod AA, Winter RB. Surgical outcomes of decompression, decompression with limited fusion, and decompression with full curve fusion for degenerative scoliosis with radiculopathy. Spine. 2010;35(20):1872–1875.
14. Yang F, Chen R, Gu D, et al. Clinical Comparison of Full-Endoscopic and Microscopic Unilateral Laminotomy for Bilateral Decompression in the Treatment of Elderly Lumbar Spinal stenosis: a Retrospective Study with 12-Month Follow-Up. J Pain Res. 2020;13:1377–1384.
15. Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and Management of Lumbar Spinal Stenosis: a Review. JAMA. 2022;327(17):1688–1699.
16. Schneider MJ, Ammendolia C, Murphy DR, et al. Comparative Clinical Effectiveness of Nonsurgical Treatment Methods in Patients With Lumbar Spinal Stenosis: a Randomized Clinical Trial. JAMA Netw Open. 2019;2(1):e186828.
17. Hou Y, Shi H, Shi H, Zhao T, Shi J, Shi G. The clinical effectiveness and complications of lumbar selective fenestration and concave-side fusion (LSFCF) in degenerative lumbar scoliosis (DLS) combined with lumbar spinal stenosis (LSS). BMC Surg. 2022;22(1):405.
18. Lee SE, Jahng TA, Kim HJ. Decompression and nonfusion dynamic stabilization for spinal stenosis with degenerative lumbar scoliosis: clinical article. J Neurosurg Spine. 2014;21(4):585–594.
19. Gadiya AD, Borde MD, Kumar N, Patel PM, Nagad PB, Bhojraj SY. Analysis of the Functional and Radiological Outcomes of Lumbar Decompression without Fusion in Patients with Degenerative Lumbar Scoliosis. Asian Spine J. 2020;14(1):9–16.
20. Masuda K, Higashi T, Yamada K, Sekiya T, Saito T. The surgical outcome of decompression alone versus decompression with limited fusion for degenerative lumbar scoliosis. J Neurosurg Spine. 2018;29(3):259–264.
21. Echt M, De la Garza Ramos R, Geng E, et al. Decompression Alone in the Setting of Adult Degenerative Lumbar Scoliosis and Stenosis: a Systematic Review and Meta-Analysis. Global Spine J. 2022;21925682221127955.
22. Ploumis A, Transfledt EE, Denis F. Degenerative lumbar scoliosis associated with spinal stenosis. Spine J. 2007;7(4):428–436.
23. Ruetten S, Komp M. Endoscopic Lumbar Decompression. Neurosurg Clin N Am. 2020;31(1):25–32.
24. Fan N, Yuan S, Du P, et al. Complications and risk factors of percutaneous endoscopic transforaminal discectomy in the treatment of lumbar spinal stenosis. BMC Musculoskelet Disord. 2021;22(1):1041.
25. Kiram A, Hu Z, Man GC, et al. The role of paraspinal muscle degeneration in coronal imbalance in patients with degenerative scoliosis. Quant Imaging Med Surg. 2022;12(11):5101–5113.
26. Widmer J, Cornaz F, Scheibler G, Spirig JM, Snedeker JG, Farshad M. Biomechanical contribution of spinal structures to stability of the lumbar spine-novel biomechanical insights. Spine J. 2020;20(10):1705–1716.
27. Minamide A, Yoshida M, Iwahashi H, et al. Minimally invasive decompression surgery for lumbar spinal stenosis with degenerative scoliosis: predictive factors of radiographic and clinical outcomes. J Orthop Sci. 2017;22(3):377–383.
28. Chang HS. Influence of Lumbar Lordosis on the Outcome of Decompression Surgery for Lumbar Canal Stenosis. World Neurosurg. 2018;109:e684–e690.
29. Schwab FJ, Blondel B, Bess S, et al. Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine. 2013;38(13):E803–812.
30. Yoshihara H, Hasegawa K, Okamoto M, Hatsushikano S, Watanabe K. Relationship between sagittal radiographic parameters and disability in patients with spinal disease using 3D standing analysis. Orthop Traumatol Surg Res. 2018;104(7):1017–1023.
31. Fujii K, Kawamura N, Ikegami M, Niitsuma G, Kunogi J. Radiological improvements in global sagittal alignment after lumbar decompression without fusion. Spine. 2015;40(10):703–709.
32. Ogon I, Teramoto A, Takashima H, et al. Factors associated with low back pain in patients with lumbar spinal stenosis: a cross-sectional study. BMC Musculoskelet Disord. 2022;23(1):552.
33. Gao A, Wang Y, Yu M, et al. Association Between Radiographic Spinopelvic Parameters and Health-related Quality of Life in De Novo Degenerative Lumbar Scoliosis and Concomitant Lumbar Spinal Stenosis. Spine. 2020;45(16):E1013–e1019.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.