Back to Journals » Journal of Pain Research » Volume 19
Early Postoperative Pain and Its Risk Factors in Patients Undergoing Total Knee Arthroplasty Under the ERAS Protocol
Authors Wu L, Sun S, Kan Y, Liu X, Wu Q
Received 26 June 2025
Accepted for publication 26 November 2025
Published 8 January 2026 Volume 2026:19 549841
DOI https://doi.org/10.2147/JPR.S549841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Liming Wu,1,* Shiyu Sun,2,* Yanpeng Kan,2,* Xing Liu,1 Qiong Wu3
1Department of Pain Medicine, The Fifth People’s Hospital of Wujiang Area, Suzhou, Jiangsu, 215200, People’s Republic of China; 2Department of Pain Medicine, Shanghai Tenth People’s Hospital, Tongji University, Shanghai, 200072, People’s Republic of China; 3Department of Rehabilitation Medicine, The Ninth People’s Hospital of Suzhou, Suzhou, Jiangsu, 215000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiong Wu, Email [email protected] Xing Liu, Email [email protected]
Background: Enhanced Recovery After Surgery (ERAS) is a multidisciplinary, evidence-based protocol designed to accelerate patient recovery after surgery. While applied to total knee arthroplasty (TKA) to optimize perioperative care, a significant risk of early postoperative pain persists. This study aims to investigate the current status and identify key high-risk factors for early pain in TKA patients under ERAS, facilitating the development of targeted strategies to alleviate pain and enhance recovery.
Methods: We conducted a retrospective analysis of 183 patients who underwent TKA under the ERAS protocol at our hospital. On postoperative day 3, patients were categorized using the Numerical Rating Scale (NRS): those with NRS scores ≤ 3 formed the mild pain group (n=132), and those with scores > 3 constituted the moderate-to-severe pain group (n=51). Clinical data were compared, and univariate along with multivariate logistic regression analyses were employed to identify independent risk factors for early postoperative pain.
Results: Of the 183 patients, 51 (27.87%) experienced moderate-to-severe pain. Comparative analysis revealed significant differences between the two groups in intraoperative tourniquet time, preoperative Hamilton Anxiety Scale (HAMA) score, preoperative quadriceps thickness, and preoperative Knee Society Score (KSS). Multivariate analysis confirmed these four factors as independent risk factors. A predictive nomogram model built on these factors demonstrated good calibration and a high predictive value, with an Area Under the Curve (AUC) of 0.892. Furthermore, NRS scores showed a positive correlation with tourniquet time and HAMA scores, and a negative correlation with quadriceps thickness and KSS scores.
Conclusion: A notable proportion of TKA patients under ERAS still experience moderate-to-severe early postoperative pain. This pain is independently associated with longer tourniquet time, higher preoperative anxiety, thinner quadriceps, and lower preoperative KSS. These factors are valuable for predicting pain, enabling early targeted interventions to minimize its occurrence and promote recovery.
Keywords: total knee arthroplasty, enhanced recovery after surgery, early postoperative pain, knee osteoarthritis
Introduction
Osteoarthritis (OA) is a chronic degenerative joint disease, with knee osteoarthritis (KOA) being one of the most common subtypes. It is primarily characterized by knee pain, swelling, stiffness, and restricted mobility, and is a leading cause of knee pain and functional impairment in the elderly population. With the global trend of population aging, the incidence of KOA has been increasing annually. Total knee arthroplasty (TKA) is a widely adopted clinical intervention for knee joint diseases, effectively relieving knee pain and restoring joint function. Numerous studies have confirmed its favorable mid- and long-term outcomes. According to statistics,1 the number of patients undergoing TKA globally is increasing at an annual rate of 5.3%–17.0%. In China, data from Beijing show an average annual growth rate of 9.73% in TKA procedures, with the number reaching 12,000 cases in 2019.2 This growing demand highlights TKA as an effective and increasingly preferred treatment for knee joint disorders. The Enhanced Recovery After Surgery (ERAS) protocol is a perioperative management concept based on evidence-based medicine. It emphasizes multidisciplinary collaboration and the optimization of perioperative care. Preoperatively, patients’ physical condition is optimized through health education, psychological intervention, fasting and fluid restriction management, as well as optimization of comorbidities and nutritional status, thereby reducing stress reserves. Intraoperatively, precise minimally invasive techniques, optimized anesthesia and analgesia management, and restrictive fluid infusion are employed to achieve targeted tissue protection and minimize physiological stress. Postoperatively, multimodal analgesia, early mobilization and rehabilitation training, complication prevention, and follow-up management are implemented to enhance pain control and early recovery, thereby accelerating functional restoration.3 Previous reports have shown that in recent years, the application rate of ERAS protocols in TKA both domestically and internationally has exceeded 60%, and the ERAS model can shorten the total hospital stay by approximately 27.5%.4 However, studies have reported that 10%–34% of patients still experience pain within the first three days following TKA.5 Clinically, early postoperative pain may be attributed to the extensive distribution of nerves around the knee and the widespread soft tissue dissection during surgery. Without timely and effective interventions, such pain may hinder functional rehabilitation, delay ambulation, slow knee function recovery, prolong hospital stay, and increase the patient’s financial burden.6 Therefore, managing early postoperative pain remains a critical concern in clinical practice.
A nomogram-based study involving 100 KOA patients indicated that age, diabetes, preoperative pain severity, and postoperative wound infection are significant risk factors for pain following TKA.7 Other research has shown that while most patients are satisfied with pain control under the ERAS protocol, a subset still experiences peak pain during the night of the first postoperative day and the second day, which may be influenced by sleep quality, disease severity, caregiver type, and depression scores.8 Predictive interventions targeting these factors could effectively alleviate early postoperative pain and enhance recovery. Furthermore, a non-randomized controlled trial demonstrated that a 3-week rehabilitation program significantly improved patients’ physical endurance and lower limb muscle strength, indicating that effective rehabilitation strategies play a vital role in postoperative recovery after TKA.9 These findings suggest that early identification of factors associated with early postoperative pain under the ERAS protocol, followed by personalized interventions, could significantly improve pain outcomes and functional recovery.
However, there is still a lack of systematic research on the current status and high-risk factors of early postoperative pain following TKA under the ERAS protocol. This study aims to fill this gap by analyzing relevant risk factors, emphasizing the timely identification of early postoperative pain, enabling the prompt initiation of rehabilitation measures to promote faster recovery and restore patients’ health.
Methods
Study Subjects
A total of 183 patients who underwent TKA at our hospital between May 2021 and September 2024 were retrospectively analyzed. All patients received surgery under the ERAS protocol. On postoperative day 3, the Numerical Rating Scale (NRS) was used to assess early pain levels. Patients scoring ≤3 were categorized into the mild pain group, and those scoring >3 were categorized into the moderate-to-severe pain group. This study was approved by the hospital ethics committee and conducted in accordance with the principles of the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Inclusion criteria: ① Diagnosed with KOA by imaging and met the indications for TKA;10 ② Undergoing primary surgery; ③ Normal mental and cognitive status with the ability to communicate; ④ Complete clinical data and relevant information; ⑤ Preoperative American Society of Anesthesiologists (ASA) physical status classification of I or II.
Exclusion criteria: ① Underwent bilateral TKA; ② Coagulopathy; ③ History of knee trauma or surgery; ④ History of chronic pain disorders; ⑤ Severe cardiopulmonary insufficiency making surgery intolerable.
Baseline Characteristics
Clinical data of patients meeting the inclusion and exclusion criteria were obtained from the hospital information system, including age, sex, body mass index (BMI), disease duration, educational level, presence of diabetes (based on the diagnostic criteria in the consensus statement for type 2 diabetes in adults11), presence of hypertension (based on diagnostic criteria from the European Society of Hypertension guidelines12), monthly household income, surgical duration, intraoperative blood loss, ASA classification (Grade I: healthy, good surgical tolerance; Grade II: mild systemic disease with preserved compensatory function), surgical site, preoperative opioid use, intraoperative tourniquet time (During surgery, a specialized surgical timer was operated by the circulating nurse to record the entire duration. The timing started when the tourniquet was inflated to achieve effective hemostatic pressure and ended when the tourniquet was completely deflated. The duration of tourniquet use was calculated as the end time minus the start time. If the tourniquet was intermittently released during the procedure due to surgical requirements, each inflation and release duration was recorded separately, and the total tourniquet time was determined by summing all inflation periods), and postoperative hospital stay.
TKA Procedure Based on the ERAS Protocol
TKA procedures followed the ERAS protocol described in the Expert Consensus on Outpatient Rehabilitation After Total Knee Arthroplasty.13 The protocol included preoperative education, fasting strategies, prehabilitation, assessment and management of comorbidities, pain control, complication prevention, nutritional support, and fluid management. All patients were eligible for surgery and received spinal anesthesia. With the patient in the supine position, a midline anterior incision was made, followed by a medial parapatellar approach. Intramedullary alignment was used for femoral osteotomy, and extramedullary alignment for tibial osteotomy. After trial prosthesis fitting, local “cocktail” analgesia was administered. Cemented, posterior-stabilized prostheses were used. Tranexamic acid was injected after capsular closure. Minimally invasive surgical principles were followed throughout.
Hamilton Anxiety Rating Scale (HAMA)14
The HAMA was developed by British psychologist Hamilton to assess the severity of anxiety symptoms. After the patients completed the basic examinations upon admission and before preoperative education, assessments were conducted by trained professionals. It includes 14 items scored on a 5-point Likert scale from 0 (no symptoms) to 4 (very severe symptoms). A total score <7 indicates no anxiety, 7–20 mild anxiety, 21–29 moderate anxiety, and >29 severe anxiety. The scale has excellent reliability, with an internal consistency coefficient of 0.934 and test–retest reliability of 0.848.
Knee Surgery Score (KSS)15
This scale was developed by the American Knee Society. Before formulating the preoperative rehabilitation plan, assessments were conducted by trained professionals. This scale mainly evaluates knee joint function across four dimensions: pain (50 points), function (25 points), range of motion (20 points), and stability (10 points), for a total of 100 points. Scores are interpreted as: 85–100 excellent, 70–84 good, 60–69 fair, and <60 poor. The internal consistency coefficient of the scale is 0.921, and the test-retest reliability is 0.873, which has good reliability and validity.
Ultrasound Examination
Ultrasound was performed preoperative 1–2 days using the Venue 50 diagnostic system (GE Healthcare) with a 12L-SC high-frequency linear probe. The “MSK” mode was selected with a frequency of 10 MHz, gain of 70 dB, and depth of 6 cm. A single focus point was placed at the top of the image. With the patient supine, they were instructed to straighten the operated knee and relax the lower limb muscles, coupling gel was applied, and the probe was placed perpendicular to the skin at the midpoint between the greater trochanter and lateral femoral condyle of the operative side. The probe position was adjusted to clearly visualize the rectus femoris and vastus intermedius muscles. Images of the rectus femoris and vastus intermedius muscles were collected. Image J software (version 1.53c, NIH, USA) was used to process 8-bit grayscale images. The region of interest was selected at the point of the muscle’s maximum cross-sectional area, and the total thickness of the rectus femoris and vastus intermedius was recorded as the quadriceps thickness.
X-Ray Examination
On postoperative day 1, before the patient got out of bed, anteroposterior and lateral X-rays of the knee were obtained. The patient was positioned supine with the knee fully extended, toes pointing upward and perpendicular to the bed, and the patella facing the bed surface. The X-ray central beam was directed perpendicular to the midpoint of the knee joint space. The tube voltage was set at 65–70 kV, tube current at 30–35 mA, and exposure time at 0.03–0.05 s. The acquired X-ray images were imported into medical image analysis software for preprocessing. Using the anterior tibial cortex line as a reference, the angle formed between the perpendicular to the tibial shaft axis at the upper-middle segment and the line connecting the anterior and posterior edges of the medial tibial plateau was measured as the posterior tibial slope.
Postoperative C-Reactive Protein
On the morning of postoperative day 1, fasting venous blood (3 mL) was collected and placed in a non-anticoagulant tube, centrifuged at 3000 rpm for 10 minutes with a radius of 10 cm to separate the serum. C-reactive protein levels were measured using an automatic biochemical analyzer (YDA-330, Shanghai Jumu Medical) based on the enzyme-linked immunosorbent assay (ELISA) method. For each batch of tests, blank controls and standard controls were included to ensure a measurement error of less than 5%. Any abnormal values were verified by recollecting and retesting the sample.
Note: The above clinical scales, imaging, and serum indicators were all part of the routine preoperative assessments for patients undergoing TKA at our hospital. Ultrasound and X-ray examinations, as well as their interpretations, were independently performed by two experienced physicians of intermediate or higher professional titles. The physicians were only aware of the examination site and timing, and were blinded to the patients’ postoperative pain grouping and the study objectives. A single-blind method was used to measure quadriceps thickness and posterior tibial slope, and the average of the two physicians’ measurements was taken as the final value.
Observation Indicators
Patients were grouped based on early postoperative pain severity after TKA. Clinical data were compared between groups. Univariate and multivariate logistic regression analyses were performed to identify risk factors associated with early postoperative pain under the ERAS protocol.
Statistical Analysis
All statistical analyses were performed using SPSS version 25.0. Categorical variables were expressed as n (%) and compared using χ2 test. The Shapiro–Wilk test was used to assess normality of continuous variables. Normally distributed data were presented as ( ±s) and analyzed using independent or paired t-tests. Non-normally distributed data were expressed as [M (P25, P75)] and analyzed using the Mann–Whitney U-test. A p-value <0.05 was considered statistically significant.
±s) and analyzed using independent or paired t-tests. Non-normally distributed data were expressed as [M (P25, P75)] and analyzed using the Mann–Whitney U-test. A p-value <0.05 was considered statistically significant.
Results
Early Postoperative Pain Status Following TKA
A total of 183 patients who underwent TKA under the ERAS protocol were included in this study. The NRS was used to assess early postoperative pain on postoperative day 3. The mean NRS score was 2.74 ± 0.90. Among them, 132 patients (72.13%) had NRS scores ≤3 and were categorized into the mild pain group, while the remaining 51 patients (27.87%) with scores >3 were classified into the moderate-to-severe pain group.
Comparison of Clinical Characteristics Between the Two Groups
To preliminarily screen potential factors affecting early postoperative pain in patients undergoing TKA under the ERAS protocol, this study grouped patients based on early pain severity assessed using the NRS scale on postoperative day 3, and compared the clinical characteristics between the two groups. The result revealed statistically significant differences in intraoperative tourniquet time, preoperative HAMA score, preoperative quadriceps thickness, and preoperative KSS score (P < 0.05). However, there were no significant differences between the moderate-to-severe pain group and the mild pain group in terms of operative time, intraoperative blood loss, postoperative length of stay, postoperative posterior tibial slope, or C-reactive protein levels (P > 0.05, Table 1).
 |
Table 1 Comparison of Clinical Characteristics Between the Two Groups (N= 183) |
Study Variable Assignment
The level of early postoperative pain after TKA was used as the dependent variable. The intraoperative tourniquet time, preoperative HAMA score, preoperative quadriceps thickness, and preoperative KSS score were used as independent variables X1, X2, X3, and X4, respectively (Table 2).
 |
Table 2 Assignment of Study Variables |
Multivariate Analysis of Early Pain After Total Knee Replacement
Based on the intergroup comparison results, indicators showing statistically significant differences were selected: intraoperative tourniquet time, preoperative HAMA score, preoperative quadriceps thickness, and preoperative KSS score. A logistic regression model was constructed, and the results showed that intraoperative tourniquet time (OR = 1.092, 95% CI: 1.046–1.139), preoperative HAMA score (OR = 1.123, 95% CI: 1.037–1.217), preoperative quadriceps thickness (OR = 0.393, 95% CI: 0.246–0.629), and preoperative KSS score (OR = 0.770, 95% CI: 0.708–0.838) were all significant factors influencing early postoperative pain after TKA (Table 3).
 |
Table 3 Multivariate Analysis of Early Postoperative Pain After TKA |
A Nomogram Prediction Model for Early Postoperative Pain After TKA Was Constructed
To translate the independent risk factors into a clinically actionable risk prediction tool, this study constructed a nomogram for predicting the risk of early postoperative pain after TKA based on the results of multivariate logistic regression analysis. The intraoperative tourniquet time, preoperative HAMA score, preoperative quadriceps thickness, and preoperative KSS score were used as predictive variables, while the occurrence of early postoperative pain after TKA was used as the dependent variable. Each variable corresponds to a specific point score, and the total score maps to a predicted probability of pain shown at the bottom of the nomogram (Figure 1).
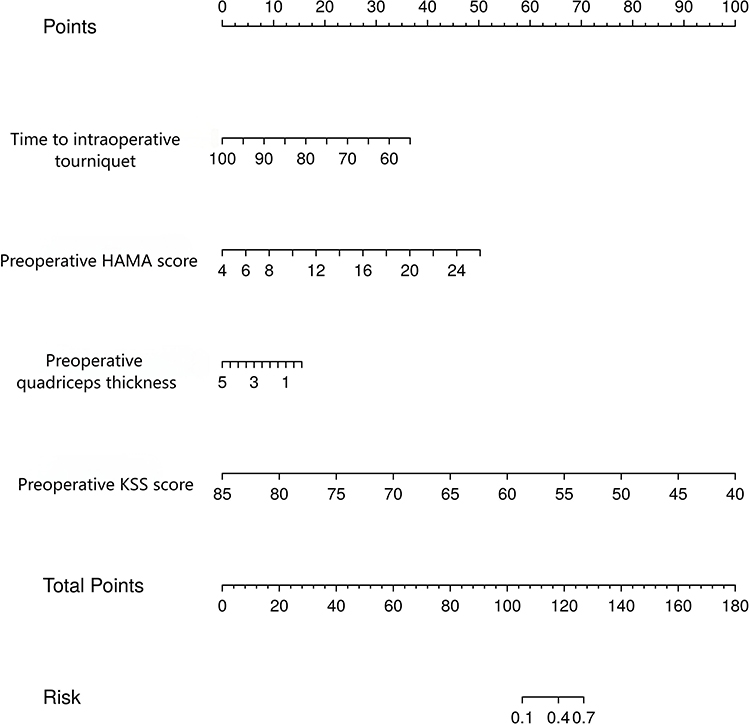 |
Figure 1 Nomogram model for predicting early postoperative pain after TKA. |
Calibration and Validation of the Prediction Model
The performance of the nomogram prediction model was validated using calibration and ROC curves. Bootstrap validation was adapted and the result showed that the calibration curve closely aligned with the reference curve, indicating that the nomogram model was reliable. Meanwhile, the area under the ROC curve (AUC) for predicting early postoperative pain after TKA was 0.892 (95% CI: 0.844–0.939), suggesting good discriminative ability. The nomogram has certain predictive value for early postoperative pain following TKA (Figure 2).
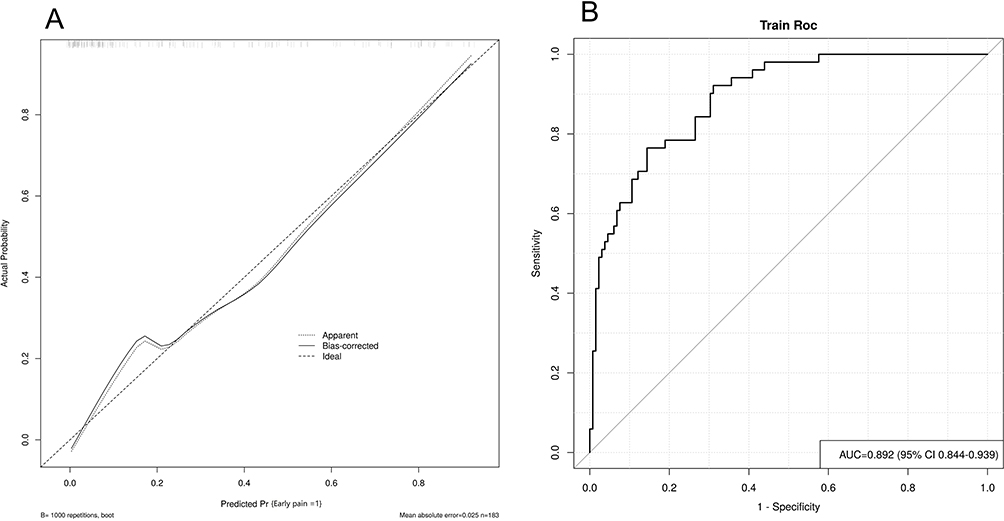 |
Figure 2 Calibration curve and ROC curve (A) calibration curve of the nomogram mo (B) ROC curve of the nomogram model for predicting early postoperative pain). |
Correlation Analysis Between Pain Severity and Influencing Factors
In this study, patients were divided into mild pain and moderate-to-severe pain groups to compare differences in pain levels. Further analyses were conducted to examine the correlations between various factors and pain, aiming to provide a basis for targeted interventions. The results showed that the NRS score in the moderate-to-severe pain group was 3.12 ± 1.01, while in the mild pain group it was 2.36 ± 0.68. Based on this, a Pearson correlation analysis was conducted. In the mild pain group, NRS scores were positively correlated with intraoperative tourniquet time and preoperative HAMA scores, and negatively correlated with preoperative quadriceps thickness and preoperative KSS scores (r = 0.492, 0.433, –0.341, –0.561; P < 0.05). In the moderate-to-severe pain group, NRS scores also showed positive correlations with intraoperative tourniquet time and preoperative HAMA scores, and negative correlations with preoperative quadriceps thickness and preoperative KSS scores (r = 0.682, 0.670, –0.667, –0.634; P < 0.05). These results suggest a close association between the degree of early postoperative pain and the identified influencing factors, with stronger correlations observed in the moderate-to-severe pain group (Figure 3).
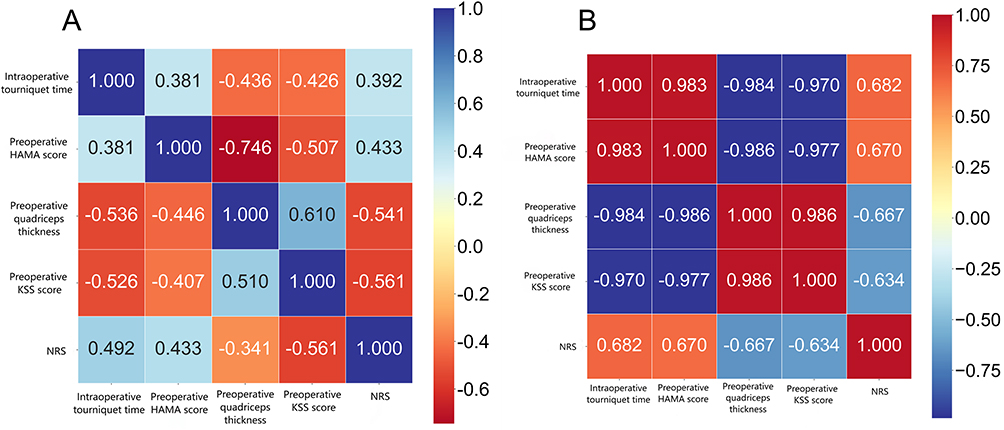 |
Figure 3 Correlation between Early Postoperative Pain Severity and Influencing Factors. (A) Correlation between NRS scores and intraoperative tourniquet time, preoperative HAMA scores, quadriceps thickness, and preoperative KSS scores in the mild pain group; (B) Correlation between NRS scores and intraoperative tourniquet time, preoperative HAMA scores, quadriceps thickness, and preoperative KSS scores in the moderate-to-severe pain group. |
Discussion
In recent years, the ERAS protocol has been widely promoted and extensively studied in the field of joint replacement. Its goal is to implement evidence-based perioperative strategies to reduce surgical stress, minimize complications, improve surgical safety and patient satisfaction, and ultimately accelerate recovery.16 However, even under the ERAS model, some patients undergoing TKA still experience early postoperative pain. According to relevant data, the incidence of moderate-to-severe acute pain after TKA is approximately 30% to 58%.17 The findings of this study are consistent with clinical data: among the 183 patients who underwent TKA, 132 (72.13%) experienced mild pain on postoperative day 3, while 51 (27.87%) experienced moderate-to-severe pain. The occurrence of early pain may be associated with factors such as intraoperative tourniquet time, preoperative HAMA score, quadriceps thickness, and preoperative KSS score. Therefore, identifying the impact of these factors on early postoperative pain is of great clinical significance.
Previous clinical studies under the ERAS protocol for TKA often considered abnormal posterior tibial slope and elevated C-reactive protein (CRP) levels as important contributors to postoperative pain. Abnormal posterior tibial slope can lead to uneven load distribution across the knee joint and reduce the congruence between the prosthesis and surrounding soft tissues, resulting in soft tissue damage around the implant, a marked decline in joint stability, and ultimately increased pain.18 Postoperative CRP reflects the inflammatory response following surgical trauma and is positively correlated with pain severity. However, in the present study, no significant differences in posterior tibial slope or CRP levels were observed between the mild pain and moderate-to-severe pain groups. This may be attributed to the ERAS protocol, which employs standardized surgical techniques and multidimensional analgesia management, effectively mitigating abnormal posterior tibial slope and elevated CRP levels, thereby eliminating significant differences between the groups.
The tourniquet is a standard tool used during TKA to reduce intraoperative bleeding, improve the surgical field, and facilitate cement fixation. However, complications related to tourniquet use—such as thigh pain, ischemia-reperfusion injury, tourniquet paralysis, and delayed wound healing—can significantly affect early functional rehabilitation and rapid recovery.19 Prolonged tourniquet time may lead to ischemia-reperfusion injury and activate the fibrinolytic system, inducing stress responses that reduce muscle strength and stimulate the release of inflammatory mediators, thereby increasing the risk of postoperative pain.20 Our findings show that the moderate-to-severe pain group had longer tourniquet times compared to the mild pain group, and a significant correlation was observed between tourniquet duration and pain intensity. While tourniquets provide a bloodless operative field and improve prosthesis implantation conditions, prolonged use can result in local tissue ischemia and hypoxia, tissue damage, and accumulation of metabolic byproducts. Once the tourniquet is released, these byproducts rapidly enter the bloodstream, exacerbating the inflammatory response and triggering postoperative pain. Thus, these pathological changes can exacerbate patients’ perception of postoperative pain. However, in those with shorter tourniquet application times, the associated tissue damage and inflammatory response are relatively milder, resulting in significantly lower pain levels. Additionally, ischemia-reperfusion injury activates various intracellular signaling pathways that heighten neural sensitivity, which becomes a major factor contributing to increased pain intensity and prolonged pain duration.21,22
Patients undergoing TKA often experience preoperative anxiety due to concerns about the surgery, fear of pain, and uncertainty about postoperative outcomes. This anxiety can exacerbate postoperative pain and delay recovery.23 In our study, the moderate-to-severe pain group had significantly higher preoperative HAMA scores than the mild pain group. Preoperative anxiety not only serves as a risk factor for early postoperative pain but also has predictive value. Anxiety may suppress immune function, impairing the body’s ability to respond to surgical trauma and increasing susceptibility to infection. Stress-induced hormonal fluctuations can further exacerbate the inflammatory response and increase the sensitivity of patients’ nociceptive nerve endings, leading to a heightened subjective perception of pain in response to stimuli of the same intensity.24 Moreover, anxiety can increase pain sensitivity and reduce compliance with postoperative rehabilitation due to fear of surgical failure, leading to complications such as joint stiffness and muscle atrophy, which in turn aggravate pain, further amplifying the pain difference compared with the mild pain group.
Quadriceps femoris is a key muscle group involved in knee joint movement. It plays a vital role in knee extension and buffering mechanical impacts during activity.25 In TKA patients, reduced activity due to pain and joint inflammation often leads to arthrogenic muscle inhibition and quadriceps atrophy, resulting in decreased muscle thickness.26 In this study, the moderate-to-severe pain group had significantly thinner preoperative quadriceps compared to the mild pain group, and quadriceps thickness was negatively correlated with pain severity, suggesting its potential as a predictor of early postoperative pain. Psychological factors such as anxiety, depression, and catastrophizing pain beliefs often reduce patients’ activity levels and nutritional intake, leading to muscle wasting and decreased quadriceps thickness.27 Thinner quadriceps muscle correlates with diminished strength and endurance, reduced knee stability, and impaired soft tissue balance, all of which contribute to increased pain and poor gait function.28,29 In contrast, the mild pain group had relatively greater preoperative quadriceps thickness, with stronger knee joint stability and compensatory capacity, resulting in significantly reduced postoperative pain.
Previous studies have shown that preoperative knee joint function is closely associated with postoperative recovery outcomes.30 In this study, the moderate-to-severe pain group had lower preoperative KSS scores compared to the mild pain group, and pain intensity increased as KSS scores decreased. This finding confirms the strong link between early postoperative pain and preoperative knee function. Patients with poor preoperative joint function may already have damaged or degenerated periarticular soft tissues, which take longer to heal postoperatively and are often accompanied by more severe pain.31 Additionally, these patients often have limited mobility and joint stiffness, which, combined with surgical trauma, reduce compliance with rehabilitation training, further exacerbating stiffness and pain. Malalignment of the knee joint in patients with poor preoperative function may also lead to uneven stress distribution on joint surfaces postoperatively, thereby increasing local pressure and pain, in stark contrast to the mild pain group, which benefits from better preoperative functional baseline and faster postoperative recovery.32
To address these high-risk factors, the following clinical interventions are recommended: (1) Assess patients’ psychological status preoperatively. Provide counseling for those with anxiety, educate them about the surgical process, and use relaxation techniques such as meditation and breathing exercises to reduce anxiety. (2) Evaluate physical condition and motor function, implement personalized quadriceps strengthening programs, and regularly assess outcomes to adjust the plan accordingly. (3) Focus on patients with poor preoperative knee function, and improve range of motion through targeted physical and pharmacological therapy before surgery. (4) Use the tourniquet judiciously during surgery based on procedural needs. Intermittent use may help minimize its adverse effects on blood circulation.
Conclusion
In conclusion, despite the implementation of ERAS protocols, some patients still experience early postoperative pain after TKA. This pain is significantly associated with intraoperative tourniquet time, preoperative HAMA scores, quadriceps muscle thickness, and preoperative KSS scores. These factors hold significant predictive value for early postoperative pain, and timely implementation of targeted interventions can effectively reduce its incidence. However, this study has certain limitations. The sample size was relatively small and drawn from a single institution, which may limit its generalizability. Pain is inherently subjective, and this study assessed patients’ pain only on postoperative day 3, which may not fully capture the dynamic changes in pain over time. Furthermore, although key risk factors for early postoperative pain were identified, the complex nature of pain suggests that other unexamined or unknown factors may also be involved. In the multivariate logistic regression analysis conducted in this study, collinearity among key variables (eg, the potential association between preoperative KSS score and quadriceps thickness) was not specifically assessed. Although univariate analysis was used to select variables with significant differences to reduce potential confounding, the degree of intervariable influence was not quantified, which may have affected the stability of the regression coefficients. Future research should aim to expand sample sizes, include multicenter data, and explore more objective and accurate pain assessment tools. Multiple pain assessment time points should be established to more comprehensively analyze the trajectory of postoperative pain and the time-dependent nature of its risk factors. Additionally, incorporating collinearity tests such as the variance inflation factor in multivariate analyses would further enhance the statistical rigor of the results. Additionally, further investigation is needed to identify more potential risk factors. Ultimately, this provides strong support for developing more personalized pain management strategies for patients undergoing TKA.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Informed Consent
This study was reviewed and approved by the Ethics Committee of The Fifth People’s Hospital of Wujiang Area (Approval Number: Not applicable). Written informed consent was obtained from all participants, and all procedures followed the principles of the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
Liming Wu, Shiyu Sun and Yanpeng Kan contributed equally to this work and share first authorship. No potential conflict of interest was reported by the authors.
References
1. Aalders MB, Van Der List JP, Keijser LCM, et al. Anxiety and depression prior to total knee arthroplasty are associated with worse pain and subjective function: a prospective comparative study. Knee Surg Sports Traumatol Arthrosc. 2025;33(1):308–12. doi:10.1002/ksa.12336
2. Yang J, Gao H, Wang C, et al. Related factors and risk prediction of chronic pain after knee replacement. Ann Ital Chir. 2024;95(5):934–943. doi:10.62713/aic.3593
3. Gerow DE, Small SR, Lackey WG, et al. Incidence of anterior knee pain and functional difficulty in a prospectively recruited cohort following total knee arthroplasty with selective patellar resurfacing. J Arthroplasty. 2024;39(1):81–86. doi:10.1016/j.arth.2023.06.029
4. Jiao S, Feng Z, Huang J, et al. Enhanced recovery after surgery combined with quantitative rehabilitation training in early rehabilitation after total knee replacement: a randomized controlled trial. Eur J Phys Rehabil Med. 2024;60(1):74–83. doi:10.23736/S1973-9087.23.07899-1
5. Chodor P, Kruczynski J, Badicu G. Preoperative risk factors of persistent pain following total knee arthroplasty. Biomed Res Int. 2022;2022(1):4958089. doi:10.1155/2022/4958089
6. Feng H, Feng ML, Cheng JB, et al. Meta-analysis of factors influencing anterior knee pain after total knee arthroplasty. World J Orthop. 2024;15(2):180–191. doi:10.5312/wjo.v15.i2.180
7. Zhang B, Meng H, Zhang H, et al. Influencing factors of chronic pain after total knee replacement in osteoarthritis patients: a nomogram prediction model. Am J Transl Res. 2024;16(9):4479–4491. doi:10.62347/ZMMD4239
8. Garval M, Runge C, Holm CF, et al. Prognostic factors of knee pain and function 12 months after total knee arthroplasty: a prospective cohort study of 798 patients. Knee. 2023;44:201–210. doi:10.1016/j.knee.2023.08.013
9. An S, Zheng Q, Wang K, et al. Characteristics and influencing factors of early pain in patients after total knee arthroplasty]. Beijing Da Xue Xue Bao Yi Xue Ban. 2024;56(1):167–173. doi:10.19723/j.issn.1671-167X.2024.01.026
10. Hashizaki T, Nishimura Y, Ogawa T, et al. Effectiveness of a 3-week rehabilitation program combining muscle strengthening and endurance exercises prior to total knee arthroplasty: a non-randomized controlled trial. J Clin Med. 2023;12(4):1523. doi:10.3390/jcm12041523
11. Haase E, Lange T, Lutzner J, et al. Indication for total knee arthroplasty: evidence mapping] [J. Z Evid Fortbild Qual Gesundhwes. 2015;109(8):605–614. doi:10.1016/j.zefq.2015.09.029
12. Abusaib M, Ahmed M, Nwayyir HA, et al. Iraqi experts consensus on the management of type 2 diabetes/prediabetes in adults. Clin Med Insights Endocrinol Diabetes. 2020;13:1179551420942232. doi:10.1177/1179551420942232
13. Graber J, Churchill L, Struessel T, et al. Expert consensus for the use of outpatient rehabilitation visits after total knee arthroplasty: a delphi study. J Orthop Sports Phys Ther. 2023;53(9):566–574. doi:10.2519/jospt.2023.11840
14. Grassi G, Kreutz R, Mancia G. The 2023 European society of hypertension guidelines for high blood pressure - what’s new on diagnostic and therapeutic approaches. Pharmacol Res. 2024;199:107003. doi:10.1016/j.phrs.2023.107003
15. Kurien T, Kerslake RW, Graven-Nielsen T, et al. Chronic postoperative pain after total knee arthroplasty: the potential contributions of synovitis, pain sensitization and pain catastrophizing-An explorative study. Eur J Pain. 2022;26(9):1979–1989. doi:10.1002/ejp.2018
16. Lawrence KW, Buehring W, Habibi AA, et al. The influence of tourniquet and adductor canal block use on pain and opioid consumption after total knee arthroplasty. Orthop Clin North Am. 2023;54(4):383–396. doi:10.1016/j.ocl.2023.05.005
17. Li J, Guan T, Zhai Y, et al. Risk factors of chronic postoperative pain after total knee arthroplasty: a systematic review. J Orthop Surg Res. 2024;19(1):320. doi:10.1186/s13018-024-04778-w
18. Cheng YH, Yang CP, Chang SS, et al. Arthroscopic-assisted reduction and internal fixation for complex tibial plateau fracture: radiographic and clinical outcomes with 2- to 15-year follow-up. J Orthop Surg Res. 2023;18(1):448. doi:10.1186/s13018-023-03938-8
19. Nishimoto J, Shiraoka T, Takiguchi Y, et al. Derivation of a clinical prediction rule for chronic post-surgical pain after total knee arthroplasty considering biopsychosocial factors: a prospective cohort study. Knee. 2023;42:364–372. doi:10.1016/j.knee.2023.04.015
20. O’brien-Horgan A, Woodhouse E, Mannion S. Incidence and risk factors for chronic pain following primary total knee arthroplasty in an Irish surgical population. Ir J Med Sci. 2024;193(6):2983–2988. doi:10.1007/s11845-024-03817-z
21. Olsen U, Lindberg MF, Rose C, et al. Factors correlated with pain after total knee arthroplasty: a systematic review and meta-analysis. PLoS One. 2023;18(3):e0283446. doi:10.1371/journal.pone.0283446
22. Olsen U, Sellevold VB, Gay CL, et al. Factors associated with pain and functional impairment five years after total knee arthroplasty: a prospective observational study. BMC Musculoskelet Disord. 2024;25(1):22. doi:10.1186/s12891-023-07125-y
23. Palanne R, Rantasalo M, Vakkuri A, et al. Testing of a predictive risk index for persistent postsurgical pain on patients undergoing total knee arthroplasty: a prospective cohort study. Eur J Pain. 2023;27(8):961–972. doi:10.1002/ejp.2138
24. Paredes AC, Costa P, Costa M, et al. Differences in the relationship between pain and anxiety in total knee and Hip arthroplasty: a longitudinal cross-lagged analysis mediated by depression and pain catastrophizing. Br J Pain. 2024;18:20494637241273905.
25. Pei J, Chen H, Ma T, et al. Pain catastrophizing and associated factors in preoperative total knee arthroplasty in Lanzhou, China: a cross-sectional study. BMC Musculoskelet Disord. 2022;23(1):507. doi:10.1186/s12891-022-05435-1
26. Qian J, Wang X. Construction and validation of chronic pain prediction model after total knee arthroplasty. Pak J Med Sci. 2024;40(4):657–662. doi:10.12669/pjms.40.4.8979
27. Sciberras SC, Vella AP, Vella B, et al. A randomized, controlled trial on the effect of anesthesia on chronic pain after total knee arthroplasty. Pain Manag. 2022;12(6):711–723. doi:10.2217/pmt-2021-0081
28. Sideris A, Malahias MA, Birch G, et al. Identification of biological risk factors for persistent postoperative pain after total knee arthroplasty. Reg Anesth Pain Med. 2022;47(3):161–166. doi:10.1136/rapm-2021-102953
29. Springborg AH, Kehlet H, Nielsen NI, et al. Predictors of subacute postoperative pain after total knee arthroplasty: a secondary analysis of two randomized trials. Eur J Pain. 2025;29(1):e4703. doi:10.1002/ejp.4703
30. Tang S, Jin Y, Hou Y, et al. Predictors of chronic pain in elderly patients undergoing total knee and hip arthroplasty: a prospective observational study. J Arthroplasty. 2023;38(9):1693–1699. doi:10.1016/j.arth.2023.04.055
31. Terradas-Monllor M, Ochandorena-Acha M, Beltran-Alacreu H, et al. A feasibility study of home-based preoperative multimodal physiotherapy for patients scheduled for a total knee arthroplasty who catastrophize about their pain. Physiother Theory Pract. 2023;39(8):1606–1625. doi:10.1080/09593985.2022.2044423
32. Tian M, Li Z, Chen X, et al. Prevalence and predictors of chronic pain with two-year follow-up after knee arthroplasty. J Pain Res. 2022;15:1091–1105. doi:10.2147/JPR.S345496
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
High Pain Self-Efficacy Reduces the Use of Analgesics in the Early Postoperative Period After Total Knee Arthroplasty: A Retrospective Cohort Study
Sonobe T, Nikaido T, Sekiguchi M, Kaneuchi Y, Kikuchi T, Matsumoto Y
Journal of Pain Research 2025, 18:1407-1415
Published Date: 19 March 2025
Application of Perioperative Nursing Based on Enhanced Recovery After Surgery (ERAS) Principles in Patients Undergoing Total Knee Arthroplasty
Huang J, Wu G, Li X
Therapeutics and Clinical Risk Management 2025, 21:829-839
Published Date: 31 May 2025