Back to Journals » Patient Preference and Adherence » Volume 16
Early Postnatal Care: Exploring Primary Caregivers’ Experiences of Continuity of Care After Discharge at Selected Districts in Limpopo Province South Africa
Authors Shirindza KJ, Malwela T ![]() , Maputle MS
, Maputle MS ![]()
Received 30 March 2022
Accepted for publication 18 June 2022
Published 8 August 2022 Volume 2022:16 Pages 2009—2020
DOI https://doi.org/10.2147/PPA.S366948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Katekani Joyce Shirindza, Thivhulawi Malwela, Maria Sonto Maputle
University of Venda, Faculty of Health Sciences, Department of Advanced Nursing, Thohoyandou, South Africa
Correspondence: Maria Sonto Maputle, University of Venda, Faculty of Health Sciences, Department of Advanced Nursing, Private Bag X 5050, Thohoyandou, South Africa, Tel +271 5 962 8125, Email [email protected]
Background: Early postnatal discharge is perceived as a factor that contributes to possible maternal, neonatal complications and deaths during the first week of delivery. Continuing with provision of home-based postnatal care by the primary caregivers is crucial to prevent morbidity and mortality.
Purpose: The purpose was to explore the experiences of primary caregivers of continuing with the provision of early postnatal care at home.
Method: A qualitative research approach, which was explorative, descriptive, and contextual was conducted in the three selected districts of different ethnic groups at Limpopo Province in October 2019. A non-probability, purposive sampling was used to conveniently sample 20 primary caregivers of postnatal women. Data were collected during the first 2 weeks of delivery through in-depth individual semi-structured interviews until data saturation was reached. Data were analysed through a thematic analysis framework applying Tesch’s open coding method. The study was done in Limpopo district, South Africa.
Findings: The findings revealed a theme, namely, knowledge and skills of providing community-based postnatal care and three sub-themes; early postnatal care to detect and prevent possible complications to the mother; general postnatal care, and early neonatal care to detect and prevent possible complications.
Conclusion: Primary caregivers displayed acceptable indigenous skills and knowledge of providing early postnatal care. However, the skills of detecting potential danger signs were not adequately displayed. It was recommended that midwives need to create awareness to primary caregivers from the antenatal through postnatal care period. Community Health Workers to assist during immediate postnatal check-ups (mother and neonate) which is done within 72hours of delivery. The health education, counseling, and community-based awareness campaigns are to be done with a focus on the detection and prevention of possible complications to mother and baby.
Keywords: early postpartum discharge, maternal and neonatal complications, postnatal care, primary caregivers
Introduction
The first six weeks of the postnatal period is the most critical period for the survival of both the mother and a baby.1 This was corroborated by Afolaranmi et al2 and Akin-Otiko and Bhengu3 that the burden of maternal and neonatal complications and deaths is highest in the first few days of delivery. It was estimated that globally every year 3 million babies die in the first 28 days of life.4 According to UNICEF5 in developing countries, 55% of babies die at home. Whereas, 45% of maternal deaths occur within 48 hours. Lassi and Bhutta6 pointed that more than 66% of women die in a week and 80% of women die in 2 weeks. The findings were supported by another study where it was found that the limited continuity of postnatal care resulted in more deaths at home.7 According to UNICEF,5 the possible causes of death for newborns are infections, asphyxia, preterm births, and low birth weights. Similar findings by Butta et al8 reflected that the immediate deaths are related to the lack of proper postnatal care during this period. Once the woman is discharged from the health facility, the primary caregivers are responsible to continue with the provision of postnatal and neonatal care at home.8 Primary caregivers are females, especially the woman’s mother-in-law or family relatives, who assist with domestic duties to maintain daily life of postnatal woman and her baby from discharge until the six-week period. They are not government employees or private ones, but someone who is naturally very easy going and flexible, empathetic and caring during the postnatal period.
The life-saving support systems within the health facilities can save lives; however, more postnatal deaths that occurred to the mother and baby are associated with the care that is provided at home.9 The findings in UNICEF5 indicated that the survival of the mother and the baby at the health facility depends on the life-saving devices. The discharge of the pair only happens if there are no complications within the 6 hours of delivery, which means that the primary caregivers should be knowledgeable about the provision of early postnatal care, to be able to continue with postnatal care at home. However, the primary caregivers were not included in the maternal health-care guidelines for the early discharge postnatal care. This puts the women and the babies at risk of developing postnatal and neonatal complications, thus leading to deaths. The authors10 confirmed that continuity of care saved lives of mother and baby, at developed countries like New Zealand where there is a dedicated community midwife who often visit the family as part of continuity of care. The midwife also teach the family members on how to pick up common complications and report to her.11,12 However, in developing and underdeveloped African states the practice is that the in-laws, spouses and elder daughter in the family are the ones continuing with care. This family members use their previous experience to assist women during this critical period. No midwife is allocated to teach and assist them on the daily care of mother and baby in their first 42 days hence increases neonatal and maternal complications and death.13
When women and babies are faced with postnatal and neonatal complications at home; the primary caregivers would resort to practice their indigenous postnatal care. Provision and continuing with community-based care could prevent morbidities and mortalities. Warren11 corroborated that early postnatal discharge contributes to the lack of conducive postnatal care at home. Cognizant of the above statement, the developing countries have established community-based postnatal care to improve the lives of both mother and baby.14 Despite the critical importance of the postnatal period to promote optimal essential neonatal and maternal care practices as well as to save both lives, it is evident that many women and their newborns do not have access to health care during the early postnatal period.14,15 According to the South African Nursing Council (SANC) Regulation (R.2598), registered midwives are given directives on how to provide postnatal care; however, the primary caregivers are not included.16 Primary caregivers used the indigenous understanding and practices based on their cultural background to provide postpartum care and some of the practices could be harmful.17
Limpopo is a rural province and primary caregivers were still employing the indigenous practices such as introducing the infant to the ancestors by making it to inhale mixed herbs. This was a handing over of the newborn and to ensure that it is connected to the spiritual ancestors. Some would even make superficial incision on frontal fontanelle and rub in the burned herbs (ashes) which is believed to provide immunity and protection. Other primary caregivers boil the herbs and make watery soft porridge to assist it to adjust to solid food early. These practices were dangerous and were discouraged as they could contribute to sepsis, tetanus, transmission of HIV, and meningitis leading to neonatal mortality.22
Community and home-based postnatal care are effective if provided by the trained community health worker.15 The findings in WHO15 reflected that home-based postnatal care increases newborn survival and reduces maternal morbidity. Community/home-based care includes promotion of exclusive breastfeeding, helping to keep the newborn warm through the promotion of skin-to-skin contact, instructing mothers on hand hygiene, counseling on umbilical cord care, delaying the first bath and assessing the danger signs, and counseling on the problems that are recognized initially such as baby not feeding well. Advising the primary caregivers on how to assess and diagnose difficulty in breathing, fever, fits, and convulsions. To the mother, they must observe the general condition of the mother regarding urination and urinary incontinence, bowel function, healing of any perineal wound, headache, fatigue, back pain, perineal pain, perineal hygiene, uterine tenderness, and lochia discharges. They also need to observe, and report swollen, red, and tender breasts or nipples and the management of breastfeeding problems. To report changes in the moods as well as any changes in maternal behaviour. The primary caregivers should be equipped with skills to provide community/home-based postnatal care to achieve the quality of life for both the mother and the baby.14 In the context of this study, it was noted that women were discharged within six hours after delivery whereas some primary caregivers were not adequately equipped to continue with the provision of postnatal care. The importance of the study was to determine the continuity of postnatal care by primary caregivers immediately after the early discharge period. The purpose was to explore the experiences of primary caregivers of continuing with the provision of early postnatal care at home.
Materials and Methods
The study was conducted at ten health centres of the three districts with different ethnic groups in Limpopo Province namely; (4) Mopani, (4) Vhembe, and (2) Sekhukhune. A qualitative explorative, descriptive contextual research design was used.16
Population and Sampling
The population comprised all primary caregivers who accompanied the woman and the new-born for postnatal assessment. These primary caregivers were from the three selected districts Vhembe, Mopani and Greater Sekhukhune as they were having different ethnic groups. The researchers arranged to visit the facilities based on the dates with more visits and conveniently select those bringing babies for two (2) weeks after delivery. Non-probability purposive sampling was used to recruit a total of twenty (20) participants who volunteered to participate in the study. The inclusion criteria were those who accompanied the postnatal women at 2 days, and/or 2 weeks; cultural diversity; namely, Xitsonga, Venda, and Northern Sotho. Those who were not meeting the inclusion criteria were excluded from participating.
Ethical Considerations
Ethical standards were ensured by obtaining the ethical clearance (Ref: SHS/19/PDC/07/2904), from the University of Venda Ethics Committee, permission to conduct the study from the Limpopo Provincial Department of Health, the District Managers and the hospital Chief Executive Officer, responsible for taking managerial decisions, and the primary caregivers, who were very crucial in following instructions of midwives. Participants were coded as Participant number from a specific ethnic group, to maintain anonymity. Participants gave verbal and written, informed consent, and were informed of their right to withdraw from the study without any penalty. Ethical principles of fairness, privacy, confidentiality as well as participants’ rights to voluntarily participate in the study were adhered to.
Data Collection
In-depth individual unstructured face-to-face interviews were used to collect data on primary caregivers’ experiences regarding continuing with early postnatal care as well as their interpretations on experiences.18 Data were collected from September 2019 to January 2020. The researcher used the private quiet room of the facility as arranged with the manager for data collection. The question asked was “Can you share with me as to how do you continue with the provision of early postnatal and neonatal care at home”? Probing was done focusing on observations that were done to detect possible complications and early care provided to the mother and a neonate. The interviews were conducted by researchers in participants’ local language (Tshivenda, Sepedi, and/or Xitsonga), and each lasted between 30 and 45 minutes. Permission to use the voice recorder was obtained from participants.
Data Analysis
The narrative data from the in-depth individual interviews were analyzed qualitatively using the framework of Tesch’s open coding. The researcher examines data to identify common themes, topics, ideas and patterns of meaning that came up repeatedly. The seven-step process included transcription, reading and familiarization, coding, searching for themes, reviewing themes, defining, and naming themes and finalizing the analysis. Tesch’s open coding method as postulated by Creswell was applied.19 The recorded interviews were translated into English by the language expert, transcribed word by word, and the nonverbal cues (for example, silence/sigh, frowns, and lean back) were included in the transcripts. All transcripts were read to give meaning, and a list of similar topics clustered. Data were grouped according to themes and sub-themes and field notes were also coded and categorized. A literature control was integrated into the discussion to validate the findings in order to gain a better understanding about the early postnatal care period.
Trustworthiness
The criteria for ensuring trustworthiness as outlined in Polit, Beck and Hungler20 were adhered to. Credibility was ensured through prolonged engagement during data collection. The researcher met with the participant at the hospital after delivery to establish rapport and to make an appointment. During the interviews, the researcher spent time with the participants listening and observing them as they were interviewed. Confidentiality was ensured by not including the participant names in all the transcripts and recordings, only code was assigned from participants 1 to 20. The participants were interviewed to the point at which there was data saturation. A member check was also conducted to validate the truth and to confirm the findings. The voice recorder was used to ensure credibility. Transferability was ensured by thick descriptions of the research methodology. The recorded interviews were transcribed verbatim and the nonverbal cues (for example, silence/sigh, frowns, and lean back) were included in brackets of the transcripts to ensure authenticity. Peer review was done by promoters and the independent coder to critique the study methods and validation of the conclusions as a thorough check on research bias.
Presentation of Findings
Demographic Profile of Participants
Twenty (20) participants agreed to participate and the breakdown was; Xitsonga speaking 12, 4 Venda-speaking, and 4 Northern Sotho. Their age ranged from 30 to 68 years. Most participants were unemployed and had provided indigenous care to postnatal women and their babies. Most primary caregivers were single as well as married and the least were divorced and some widowed (Table 1).
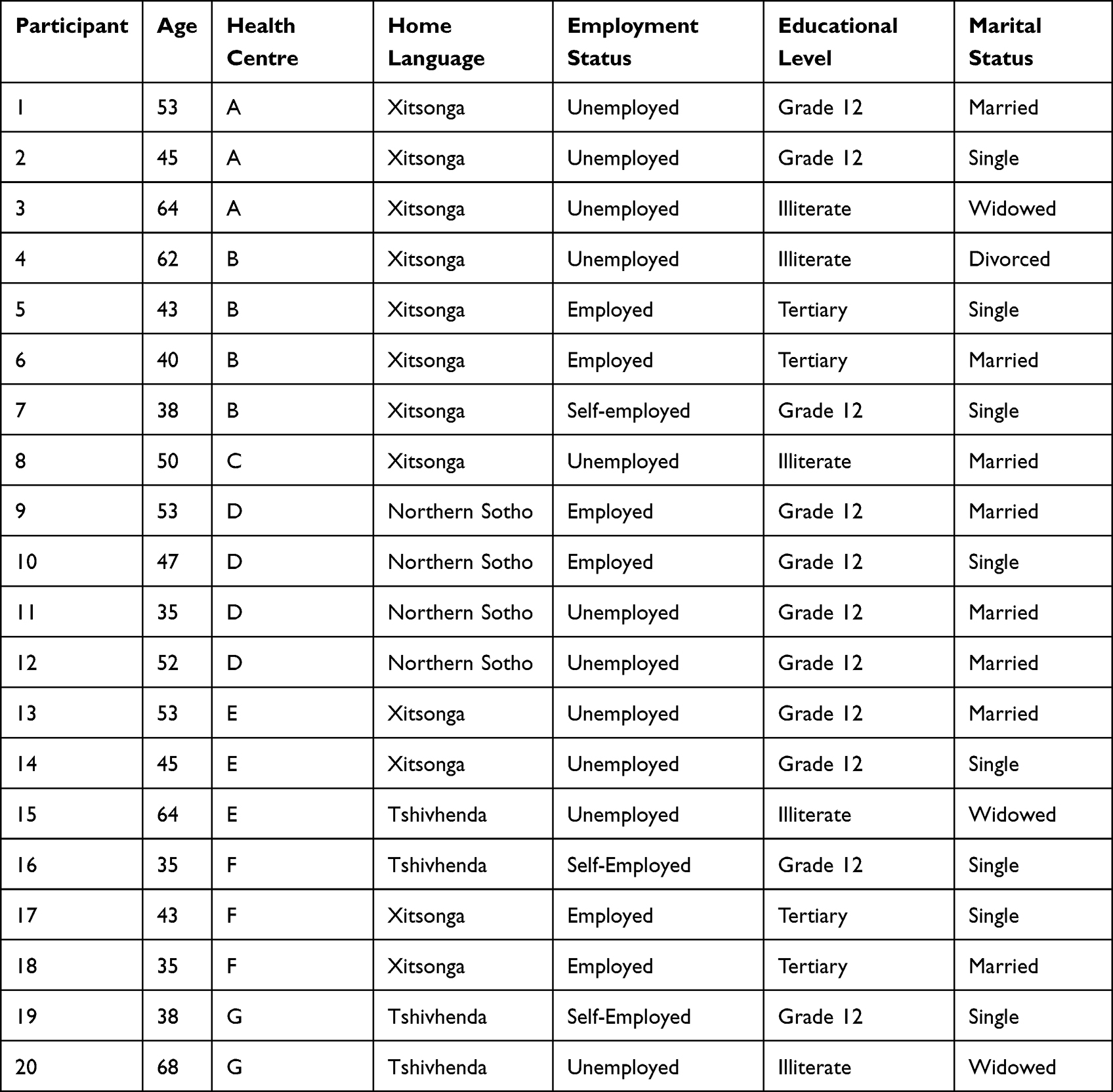 |
Table 1 Demographic Profile of Primary Caregivers (No 20) |
Theme and Sub-Themes Reflecting the Primary Caregivers’ Knowledge and Skills of Early Postnatal Care
The findings were generated from the initial 20 transcripts and grouped to form three sub-themes which was merged to one theme as knowledge and skills of providing early postnatal community/home-based care. These are presented in Table 2 and findings are discussed and based on excerpts from participants’ responses.
 |
Table 2 The Theme and Sub-Themes Reflecting the Primary Caregivers’ Knowledge and Skills of Early Postnatal Care |
Theme: Knowledge and Skills of Providing Community-Based Postnatal Care
The purpose of providing optimal postnatal care is to avert maternal and neonatal deaths, as well as long-term complications. Midwives were expected to build the capacity of primary caregivers, as they are expected to continue with the provision of postnatal care at home. The study findings revealed that primary caregivers displayed indigenous skills and knowledge of when providing postnatal care. The early postnatal care focused on the reproductive system which included perineal hygiene for episiotomy care, uterine involution and lochia assessment, breastfeeding, breast care, and development of sudden headache. Primary caregivers further provided general physical care which included early ambulation and exercises, maternal nutrition, rest and sleep, and family planning. To the neonate, they were supposed to check for breathing, temperature, skin colour, feeding and to prevent infection. However, the skills of detecting potential danger signs were not adequately displayed. The sub-themes that emerged included (1.1) Early postnatal care on detection and prevention of possible complications to the mother, (1.2) Provision of general postnatal care, and (1.3) Early neonatal care to detect and prevent possible complications.
Sub-Theme 1.1: Early Postnatal Care on Detection and Prevention of Possible Complications to the Mother
Early postnatal care is critical for early detection of complications, to manage or refer the client to the relevant health facility. The findings showed that primary caregivers had basic indigenous knowledge regarding the management of hygiene measures to prevent possible infections. Participants reflected that they adhered to measures of infection control by hand washing. Participant 02 (XiT), aged 45, single and unemployed with grade 12 certificate said,
I wash my hands before I touch the mother and the baby and encourage the mother to wash her hands too.
The participant further said, “the room of the postnatal woman should always be clean and not to have an offensive smell. The environment should be well ventilated”.
Participants from all different ethnic groups indicated that the mother and the neonate were secluded from other family members and strangers. This was supported by participant 07 (SeP), 38 years, single and self-employed with grade 12 certificate when saying
I was a caretaker I ensured that they stay in the room and strangers not allowed in to prevent infections. They will stay in the room until the stump of the cord falls off, even the husband is not allowed inside (laughing).
To further emphasise the issue of hygiene maintenance participant 10 (SeP), 47 years old, single and employed with grade 12 said,
The perineal area of the mother must be kept clean by using salty water and with the changing of the pad as soon as it is full. If the condition of the baby is good, it must also be bath and kept warm especially covering the head.
Post-delivery, the woman will be having lochia, so primary caregivers were asked as to how they provide for perineal hygiene. Participant 03 (TshiV), aged 64, unemployed, illiterate and widowed said;
When the mother is having the stitches when bathing, we use a Dettol (antiseptic) and salt with little warm water, I encourage them to look for the cloth to compress on the wound to prevent sepsis and gaping of sutures.
However, the quantity of how much Dettol or salt is added in water was not mentioned and how often is the perineal care did was not indicated.
To encourage airflow participant 05 (SeP), aged 43, employed, single and at tertiary level said:
During breastfeeding, I advised … .eeh … I advised the woman to sit down with legs straight to avoiding stretching the perineal muscles and to ensure the proper healing of the area that was cut to extend to path.
Most women are dying due to secondary postpartum haemorrhage. So primary caregivers expressed their basic understanding of the uterine involution process and the assessment of lochia concerning amount, contents, colour, and smell. The following quote to support this by participant 01 (TshiV), aged 53, unemployed, married with grade 12 was
As I have learned previously from my pregnancies, I observe the amount of bleeding from the vaginal area and the state of the uterus. I encouraged her to apply pressure around the umbilical region with a cloth around the waist to promote the contraction of the uterus and to lie on the abdomen to relieve abdominal pains as well as to ease the drainage of blood.
This was supported by participant 09 (XiT), aged 53, employed, married with grade 12 certificate who said, “I encourage the woman to rub the abdomen to facilitate the contraction of the uterus to prevent the excessive bleeding”.
Participant 04 (SeP), aged 62, unemployed, illiterate and divorced said that:
I advised the mother to observe the bleeding by the number of pads changed and the colour so that when it seems profuse; they must report this to the health facility.
Concerning breastfeeding and breast care: The findings revealed that primary caregivers had basic knowledge regarding breastfeeding and the care of the breasts. However, they were not assessing whether the baby was having a good attachment. This was confirmed by participants 06 (SeP) aged 40, employed, married and at tertiary level and participant 18 (TshiV), aged 35, employed, married and at tertiary level who said:
I prepare soft porridge and tea for the woman to have sufficient breastmilk because if she doesn’t eat home-made food, the breastmilk will be insufficient and the baby won’t be satisfied and start crying.
One participant 11 (SeP), aged 35, unemployed, married and in grade 12, said:
At the clinic, they told us that the child should be breastfed exclusively, thus not mixing the breastmilk with some formula. The baby must be fed on breastmilk only and no traditional medicines.
Whereas participant 08 (XiT), 50 years, married, illiterate and unemployed said “I advise the mother on how to put the baby on or off the breast to encourage the emptying and to prevent too much fullness that is painful (breast engorgement)”.
Some women may develop severe headaches followed by eclampsia postnatally. The primary caregivers when asked about how they exclude signs for imminent eclampsia, they failed to provide any care or ask any questions regarding the signs of headache with visual disturbances or vomiting.
Sub-Theme 1.2: Provision of General Postnatal Care
Maternal Nutrition
Nutrition plays an important role for both the mother and the baby during the postnatal period. Participants displayed general knowledge regarding maternal diet during the early postnatal period. This was confirmed by participants 14 (TshiV), aged 45, unemployed, single with grade 12 certificate 03 (TshiV), aged 64, unemployed, illiterate and widowed and 09 (XiT) aged 53, employed, married with grade 12 certificate who said:
I prepare soft porridge and tea for the woman to have sufficient breastmilk because if she doesn’t eat home-made food, the breastmilk will be insufficient and the baby won’t be satisfied and start crying.
When asked about the food classification related and its importance, participant 15 (XiT), aged 64, unemployed, illiterate and widowed said:
To make sure that the baby is satisfied the mother must eat warm food. The baby is exclusively breastfed for six months because the stomach is not well developed.
Concerning early ambulation and exercises, participants from all different ethnic groups indicated that they understand the importance of resumption of daily activities to promote circulation to all parts of the body. This was echoed by participant 01 (TshiV) 53 years old, unemployed, married with grade 12 who said:
I encourage her to move around in the house and bath herself. This is done so that she can regain her bodily movements, strengthening the body muscles that were affected or traumatised during normal delivery or operation.
Participant 15 (XiT) aged 64, unemployed, illiterate and widowed concurred by saying, “I encourage the mother to walk in the house and to do postnatal exercises that I was shown at the clinic to promote circulation”.
The findings related to rest and sleep revealed that primary caregivers were aware of the comfort of the postnatal woman after delivery. This was echoed by participant 13 (XiT), 53 years old, married, married with grade 12 who said
On the maternal part, the mother will be assessed for tiredness and relieved as she will be neglecting the baby.
Yet, participant 12 (XiT) 52 years old, unemployed, married with grade 12 shared the same view and said:
The mother is tired from the day of giving birth, then I prepare warm water to the bath so that she can position and bond with the child. I put the baby on her lap so that she relaxes and feeds the baby. I told her to sleep when the baby also is asleep for her to rest.
Sub-Theme 1.3: Early Neonatal Care to Detect and Prevent Possible Complications
Participants were asked as to how they assess and prevent the possible danger signs of the neonate through the observation. It was noted that no participant mentioned breathing problems like fast breathing or chest in-drawings, very high or very low temperature.
The interviews with the primary caregivers indicated the knowledge they have regarding breastfeeding was stated based on their cultural beliefs. The following are some of the direct quotes from the participants. Participant 17 (TshiV) aged 43, employed, single and at tertiary level said
I observe as to how the mother is putting the baby on the breast and whether the baby can suckle from the breast, whether the baby is not drowsy (lethargic) during feeding.
Participant 08 (TshiV) aged 50 years, unemployed, married and illiterate echoed the same sentiments by saying
The child should be breastfed exclusively, thus not mixing the breastmilk with some formulas.
Whereas, participant 09 (XiT), aged 53, employed, married with grade 12 noted her observation when saying:
During the initiation of breastfeeding, the baby was sucking with difficulties, and the milk was not swallowed but coming out from the mouth. I then decided to send the child to the hospital for further management. The baby was operated on inside the mouth and the midwives said that the tongue was not moving but attached to the mouth.
Relating the skin colour with feeding participant 19 (TshiV) aged 38, self-employed, single with grade 12 said:
I check the baby while bathing, looking at the skin colour and the colour of the eyes. If the eyes are yellow, I encourage the mother to breastfeed the baby because the yellow colour indicates that the baby is not getting enough milk from the breast.
It is always important to keep the baby warm. Participant 04 (SeP) aged 62, unemployed, illiterate, and divorced mentioned that “I use warm water and bath the baby to keep it clean and to keep warm”. The question on the delay of bathing or skin-to-skin practice there was nothing mentioned on this aspect.
The findings on questions related to umbilical cord care showed that some primary caregivers were performing cultural practices that were harmful to the baby. This was confirmed by participant 20 (XiT) aged 68, unemployed, illiterate and widowed who said:
Eish, although there are no medications to clean the cord provided by nurses, we use a white spirit three times a day to keep the cord clean so that it can dry and fell off.
Participant 11 (SeP), aged 35 years, unemployed, married with grade 12 mentioned the method used to clean the cord by saying
I did what I was taught. Before I clean the cord, I wash my hands and clean the cord from the base of the stump, and then I put the napkin … .eeh … . I sometimes … I sprinkle breast milk into the eyes and cord to hasten the healing of the cord and to prevent eye problems as breast milk can prevent bacteria through it.
Participant 16 (TshiV) aged 35, self-employed, single and with grade 12 said:
At 3 days period after birth, I go with her for check-up … the umbilical cord is kept clean always for faster healing … . using white spirit or Dettol and even Savlon.
However; participant 20 (XiT) aged 68, unemployed, illiterate and widowed mentioned how they used to treat the umbilical cord when saying
In the olden days chicken faeces and used motor oil was applied on the stump to keep flies away from the cord … but since we are nearer hospitals we no longer use it.
Primary caregivers revealed that they know the care of the eyes of the neonate. This was reflected by participant 11 (SeP), aged 35, unemployed, married with grade 12 who said:
Sometimes I sprinkle breast milk into the eyes and cord to hasten the healing of the cord and prevent eye problems as the breast milk can prevent bacteria through it.
Participant 10 (SeP), aged 47, employed, single with grade 12 said:
I observe the colour of the eyes and the whole skin areas observing the ears for growth, abnormal folds and some cracks in the skin area. I report it to the nurses at the clinic if the problem takes a long time.
Some of the primary caregivers were using traditional practices when caring for the eyes of a new-born.
Discussion of Findings
Early Postnatal Care on Detection and Prevention of Possible Complications to the Mother
The researcher employed the step by step thematic analysis framework of Tech’s steps of open coding. From the 20 transcripts, similarities were grouped and merged to form three sub-themes and one theme. The theme reflected primary caregivers’ knowledge deficit and skills of early postnatal care to enhance continuity of care. All twenty primary caregivers from diverse ethnic groups who were interviewed displayed limited differences in cultural practices and beliefs when providing early postnatal care. The participants cited the prevention of infection by hand washing before touching the baby or before breastfeeding. Ngunyulu et al22 pointed that postnatal women were put in a clean house and encouraged to bathe daily to prevent the spread of infections. To further prevent infection and promote healing, participants showed they provided care related to perineum and episiotomy wounds. They mentioned the use of a sitz bath using salt and warm water. However, the frequency and exactly as to what should be observed on the tear or episiotomy were not mentioned. This showed that midwives and community health workers need to create opportunities for information giving to reduce conflicting messages from indigenous practice that retards the continuity of care. The study conducted by Asgharikhatooni21 confirmed that salty warm water was best for the postnatal woman as it brings a soothing effect on the perineum. This was also supported by the guidelines that it helps with the aspects of positioning and movements in a postnatal woman.21 Okeke et al23 revealed that primary caregivers who are providing perineal hygiene to postnatal women feel attached to the woman and are fearful that complications such as sepsis might occur while under their care. According to Sellers,24 the infection from unhygienic perineum may predispose the woman to the risk of dehiscence due to a faulty healing technique. The perineal trauma and the episiotomy that are unhygienic contribute to the decreased level of daily activities to the postnatal woman, hence, to also neglect to care for the baby.25 The discomfort caused by perineal lacerations, episiotomy, and caesarean section wounds resulted in insomnia that also disrupts the postnatal woman’s ability to interact easily with the baby in the early weeks and thus interfere with breastfeeding.26,27
The seclusion of the mother from the male partner and strangers was practiced until the stump of the umbilical cord falls off. Personal and environmental hygiene was cited as a very important aspect that promotes healing. This was supported by Sharma et al28 who cited that women are housebound for several days after birth and the length of seclusion varies by ethnic groups. The findings further confirmed that postnatal woman was prohibited to prepare for household chores until after six weeks.
Postpartum haemorrhage (PPH) is the leading cause of maternal mortality, accounting for about 35% of all maternal deaths.29 To prevent secondary postpartum haemorrhage, participants displayed knowledge of rubbing the uterus to stimulate the uterine contraction. They indicated that they monitor the bleeding by checking the fullness of the sanitary pad, however, ensuring that the bladder should be kept empty was not emphasised. Another study emphasise that educating the woman, relative, or neighbour regarding the early detection and seeking medical assistance for complications such as postpartum haemorrhage that can be detected through uterine involution and lochia assessment is very important to monitor the health of a postnatal woman. Adequate nutrition during infancy is essential to ensure the growth, health, and development of babies to their full potential.30
Participants were encouraged to initiate and maintain breastfeeding. Breastfeeding and breast care were supported by Ngunyulu et al22 who indicated that the initiation and maintenance of exclusive breastfeeding, is an important strategy in the reduction of child mortality rates in developing countries. The main reason was that breastfeeding provides all nutrients to the baby with no infections. The study conducted by WHO15 shows that exclusively breastfed babies are referred to as healthy baby with a healthy weight. Primary caregivers were aware of the importance of breastfeeding; however, the need to teach on good attachment need to be emphasised so that infant get sufficient milk and to prevent mixed feeding. The study was confirmed by Nkala and Msuya31 that breastfeeding should not be mixed with water, other liquids, tea, herbal preparations, or food in the first six months of life, except for vitamins, mineral supplements, or medicines. Fraser and Cooper26 reflected that it is very important to reassure and teach the postnatal woman the care of breasts and breastfeeding to reduce pain. Emphasis on how to prevent breast engorgement should be taught to mothers. Ngunyulu et al22 confirmed that advising on breast care by placing cabbage leaves helped with the secretion of milk, thus preventing infection to the breasts. De Jager32 indicated that there is an association between breastfeeding and breastfeeding difficulties.
Provision of General Postnatal Care
Primary caregivers displayed basic knowledge regarding the nutritional status of postnatal women. The idea was supported by Ngunyulu et al22 who stated that the woman is encouraged to eat a well-balanced diet and increase fluid intake to improve the skin integrity, gastro-intestinal activity, and the absorption of iron and minerals, as well as to reduce the potential for constipation and the feelings of fatigue. The early ambulation and exercises were encouraged for postnatal women, to promote blood circulation by all participants of diverse ethnic groups. The WHO15 supported that more than 500,000 women die each year due to complications related to lack of early ambulation and exercises. The findings revealed that postnatal women were encouraged to walk around the house and to perform light exercises that were taught to them during their antenatal care sessions.33,34
With related to rest and sleep, findings indicated that postnatal women were encouraged, and opportunities were created. A study by Dorheim35 reflected that a woman with poor sleep quality had a chance of depression than a woman with adequate sleep. Postpartum depression has serious consequences on the quality of life of the mother and her child. The findings were confirmed by a study which stated that inadequate sleep also disrupts the relationship of both the mother and her baby, thus damaging the emotional, cognitive, motor, and behavioural development of the growing baby.35
Early Neonatal Care to Detect Possible Complications
Primary caregivers displayed limited knowledge regarding the care of the newborn at home, and they did not display skills on how to assess for possible danger signs. Participants did not mention any observations to be made to detect breathing problems like fast breathing or chest in-drawings, very high or very low temperature. No mention or understanding of the basic neurobehavioral assessment. Neonatal neurobehavioral assessment is one key mechanism by which neonates with the central nervous system and neurobehavioral disturbances are identified, Lean et al36 which was contrary to the findings by Awoyal37 who found that defects were observed during the home-based care services. The mixed or contradictory and imbalanced understanding amongst primary caregivers may again be due to a lapse of consistency in the inclusion of the support system including the primary caregivers to the women during the postnatal period
In the care of the umbilical cord, participants displayed the accurate practices of using surgical spirit to clean and not cover the cord stump with the bandage. The findings are supported by Ngunyulu et al22 in which infection control is strictly adhered to by using different basins for the mother and the baby. Similar findings by Afolaranimi et al2 confirmed that the application of methylated/surgical spirits is used for fasting drying and healing of the cord, thus avoiding sepsis of the umbilical region. However, one participant mentioned the use of Dettol or Savlon disinfectant; this misinformation needs to be corrected.
Regarding eye care participants were using clear water, although one participant indicated to be sprinkling breast milk in the eyes of the newborn. The study by Dougherty and Lister38 showed that the use of breastmilk is also a cultural medication that can keep the eyes of a newborn clean. They also acknowledged the use of warm water every morning as an indication of preventing eye conditions more especially if the mother might have encountered sexually transmitted diseases. Emphasis is to be made on maintaining strict hygiene when doing eye care.39
Limitations
The study was conducted in three selected districts of the Limpopo Province. The findings cannot be generalised to the entire province because the cultures and traditions of the ethnic groups are not the same.
Conclusion
Findings revealed that the primary caregivers were experiencing knowledge deficit and displayed limited confidence when continuing with early postnatal care provision. Some indigenous practices by primary caregivers were not adhering to hygienic principles. The discharge plan and information need to be emphasised the promotion and maintenance of hygiene. It was recommended that midwives should involve primary caregivers from the antenatal to postnatal care period. The midwives and community health-care workers should provide primary caregivers with health education emphasizing community-based awareness, and counselling programmes. The focus should be on possible early danger signs to mother and baby. Where the community health workers are used to providing community-based care, their capacity must be upscaled on possible risks of postnatal care. Postnatal check-ups (mother and neonate) to be done within 72 hours of delivery. The findings of the study may be used to bridge the gap between the postnatal care provided by midwives at the hospital and home-based/community-based care to be provided by primary caregivers.
Implications for Practice
Provision and continuing with community-based postnatal care could promote health and prevent maternal and neonatal morbidities and mortalities.
Data Sharing Statement
Most of the raw data used to support the findings are included in the article and can be made available from the corresponding author upon request.
Acknowledgments
Researchers would like to acknowledge all primary caregivers of postnatal mothers who participated in this study, Limpopo Provincial Department of Health, and the District managers who granted permission to conduct the study.
Author Contributions
The authors were K.J.S, T.M and M.S.M. All authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data. They took part in drafting the article and revising it critically for important intellectual content; agreed to submit to the current journal; they further gave final approval of this version to be published and agree to be accountable for all aspects of the work.
Funding
The project was funded by University of Venda Research and Publication Committee.
Disclosure
The authors report no conflicts of interest in relation to this work and declare that they had no financial or personal relationship(s) which may have inappropriately influenced them in writing this article.
References
1. Forster DA, McLachlan HL, Rayner J, Yelland J, Gold L, Rayner S. The early postnatal period: exploring women’s views, expectations and experiences of care using focus groups in Victoria, Australia. BMC Pregnancy Childbirth. 2008;8(1):1. doi:10.1186/1471-2393-8-27
2. Afolaranmi TO, Hassan ZI, Akinyemi OO, et al. Cord care practices: a perspective of contemporary African setting. Front Public Health. 2018;6:10. doi:10.3389/fpubh.2018.00010
3. Akin-Otiko BO, Bhengu BR. Client education experiences and expectations of women at the first level of maternal and childcare in Kaduna state, Nigeria. Midwifery. 2012;28(6):e893–9. doi:10.1016/j.midw.2011.11.011
4. World Health Organization. Guidelines on optimal feeding of low birth-weight infants in low- and middle-income countries. World Health Organization; 2011. Available from: https://apps.who.int/iris/handle/10665/85670.
5. World Health Organization. Infant and young child feeding; 2021. Available from: www.int/newsroom/fact-shhets/detail/infant-and-young-child-feeding.
6. Lassi ZS, Bhutta ZA. Community‐based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Syst Rev. 2015;CD007754. doi:10.1002/14651858.CD007754.pub3
7. Benova L, Owolabi O, Radovich E, et al. Provision of postpartum care to women giving birth in health facilities in sub-Saharan Africa: a cross-sectional study using Demographic and Health Survey from 33 countries. PLoS Med. 2019;16(10):e1002943. doi:10.1371/journal.pmed.1002943
8. Bhutta ZA, Das JK, Bahl R, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. 2014;384(9940):347–370. doi:10.1016/S0140-6736(14)60792-3
9. Baqui AH, Williams E, El-Arifeen S, et al. Effect of community-based new-born care on cause-specific neonatal mortality in Sylhet district, Bangladesh: findings of a cluster-randomized controlled trial. J Perinatol. 2016;36:71–76. PMID: 26540248. doi:10.1038/jp.2015.139
10. Limenih MA, Endale ZM, Dachew BA. Postnatal care service utilization and associated factors among women who gave birth in the last 12 months prior to the study in Debre Markos town, north-western Ethiopia: a community-based cross-sectional study. Int J Reprod Med. 2016;2016:7095352. PMID: 27433481; PMCID: PMC4940555. doi:10.1155/2016/7095352
11. McAra-Couper J, Gilkison A, Crowther S, Hunter M, Hotchin C, Gunn J. Partnership and reciprocity with women sustain Lead Maternity Carer midwives in practice. New Zealand Coll Midwives J. 2014;49:23–33. doi:10.12784/nzcomjnl49.2014.5.29-33
12. Bowers J, Cheyne H, Mould G, Page M. Continuity of care in community midwifery. Health Care Manag Sci. 2015;18(2):195–204. doi:10.1007/s10729-014-9285-z
13. Warren C, Daly P, Toure L, Mongi P. Opportunities for Africa’s new-borns: practical data policy and programmatic support for new-born care in Africa. Partnership Mater, Newborn Child Health. 2006;32:79–90.
14. Burnett-Zieman B, Abuya T, Wanyugu J, Warren CE, Sripad P. Community-based postnatal care services for women and new-borns Kenya: an opportunity to improve quality and access? J Glob Health. 2021;11:07006. doi:10.7189/jogh.11.07006
15. World Health Organization. WHO recommendations on postnatal care of the mother and newborn. World Health Organization; 2014. Available from: https://apps.who.int/iris/handle/10665/97603.
16. South African Nursing Council. Regulations relating to the scope of practice of persons who are registered or enrolled under the Nursing Act, 1978; 1984: 2598. Available from: www.sanc.co.za.
17. Dahiru T, Oche OM. Determinants of antenatal care, institutional delivery and postnatal care services utilization in Nigeria. Pan Afr Med J. 2015;22(1). PMID: 26587168; PMCID: PMC4633744. doi:10.11604/pamj.2015.21.321.6527
18. Brink H, Van der Walt C, Van Rensburg G. Fundamentals of Research Methodology for Health Care Professionals. Juta and Company Ltd; 2018.
19. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Sage Publications; 2017.
20. Polit D, Beck CT. Essentials of Nursing Research. Appraising Evidence for Nursing Practice. Philadelphia: Wolters Kluwer/ Lippincott Williams & Wilkins; 2014:8.
21. Asgharikhatooni A, Bani S, Hasanpoor S, Alizade SM, Javadzadeh Y. The effect of equisetum arvense (horse tail) ointment on wound healing and pain intensity after episiotomy: a randomized placebo-controlled trial. Iran Red Crescent Med J. 2015;17(3):e25637. doi:10.5812/ircmj.25637
22. Ngunyulu RN, Mulaudzi FM, Peu MD. Comparison between indigenous and Western postnatal care practices in Mopani District, Limpopo Province, South Africa. Curationis. 2015;38(1):1–9. doi:10.4102/curationis.v38i1.1252
23. Okeke E, Glick P, Chari A, et al. The effect of increasing the supply of skilled health providers on pregnancy and birth outcomes: evidence from the midwives’ service scheme in Nigeria. BMC Health Serv Res. 2016;16(1):1–9. doi:10.1186/s12913-016-1688-8
24. Sellers PM. Midwifery.
25. Fenwick J, Toohill J, Gamble J, et al. Effects of a midwife psycho-education intervention to reduce childbirth fear on women’s birth outcomes and postpartum psychological wellbeing. BMC Pregnancy Childbirth. 2015;(1):1–8. doi:10.1186/s12884-015-0721-y
26. Fraser D, Cooper M. Survival Guide to Midwifery, Physiology and Care in the Puerperium. Edinburgh: Churchill Livingstone El Sevier; 2014:411–414.
27. Pound CM, Unger SL. The baby-friendly initiative: protecting, promoting and supporting breastfeeding. Paediatr Child Health. 2012;17(6):317–321. PMID: 23730170; PMCID: PMC3380749.
28. Sharma S, Van Teijlingen E, Hundley V, Angell C, Simkhada P. Dirty and 40 days in the wilderness: eliciting childbirth and postnatal cultural practices and beliefs in Nepal. BMC Pregnancy Childbirth. 2016;16(1):1–2. doi:10.1186/s12884-016-0938-4
29. Sentilhes L, Lasocki S, Ducloy-Bouthors AS, et al. Tranexamic acid for the prevention and treatment of postpartum haemorrhage. Br J Anaesth. 2015;114(4):576–587. PMID: 25571934. doi:10.1093/bja/aeu448
30. Mumtaz Z, Salway S, Nyagero J, Osur J, Chirwa Ekachale F, Saunders D. Improving the standards -based management: recognition initiative to provide high quality, equitable maternal health services in Malawi. An implementation research protocol. BMJ Global Health. 2016;1:e000022. doi:10.1136/bmjgh-2015-000022
31. Nkala TE, Msuya SE. Prevalence and predictors of exclusive breastfeeding among women in Kigoma region, Western Tanzania: a community based cross-sectional study. Int Breastfeed J. 2011;1:1–7. doi:10.1186/1746-4358-6-17
32. De Jager E, Broadbent J, Fuller-Tyszkiewicz M, Skouteris H. The role of psychosocial factors in exclusive breastfeeding to six months postpartum. Midwifery. 2014;30(6):657–666. doi:10.1016/j.midw.2013.07.008
33. Tiwari S, Bharadva K, Yadav B, et al. Infant and young child feeding guidelines, 2016. Indian Paediatr. 2016;53(8):703–713. doi:10.1007/s13312-016-0914-0
34. Caughey AB, Cahill AG, Guise JM, Rouse DJ. Safe prevention of the primary caesarean delivery. Am J Obstet Gynaecol. 2014;210(3):179–193. doi:10.1016/j.ajog.2014.01.026
35. Dørheim SK, Bjorvatn B, Eberhard-Gran M. Can insomnia in pregnancy predict postpartum depression? A longitudinal, population-based study. PLoS One. 2014;9(4):e94674. doi:10.1371/journal.pone.0094674
36. Lean RE, Smyser CD, Rogers CE. Assessment: the newborn. Child Adolesc Psychiatry Clinics. 2017;26(3):427–440. doi:10.1016/j.chc.2017.02.002
37. Awoyale T, Onajole AT, Ogunnowo BE, Adeyemo WL, Wanyonyi KL, Butali A. Quality of life of family caregivers of children with orofacial clefts in Nigeria: a mixed‐method study. Oral Dis. 2016;22(2):116–122. doi:10.1111/odi.12379
38. Dougherty L, Lister S, editors. The Royal Marsden Manual of Clinical Nursing Procedures. John Wiley & Sons; 2015:Wiley–Blackwell.
39. McLeish J, Redshaw M. Maternity experiences of mothers with multiple disadvantages in England: a qualitative study. Women Birth. 2019;32(2):178–184. doi:10.1016/j.wombi.2018.05.009
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.