Back to Journals » Clinical Ophthalmology » Volume 17
Early Experience with the Paul Glaucoma Implant in Childhood Glaucoma: A Case Series
Authors Elhusseiny AM ![]() , Khodeiry MM, Lee RK, Shaarawy T, Waqar S, Sayed MS
, Khodeiry MM, Lee RK, Shaarawy T, Waqar S, Sayed MS
Received 7 April 2023
Accepted for publication 26 June 2023
Published 6 July 2023 Volume 2023:17 Pages 1939—1944
DOI https://doi.org/10.2147/OPTH.S414183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Paul glaucoma implant (PGI) in childhood glaucoma" [ID 414183].
Views: 490
Abdelrahman M Elhusseiny,1,2,* Mohamed M Khodeiry,3,4,* Richard K Lee,4 Tarek Shaarawy,5 Salman Waqar,6 Mohamed S Sayed6
1Department of Ophthalmology, Harvey and Bernice Jones Eye Institute, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 2Department of Ophthalmology, Boston Children’s Hospital, Boston, MA, USA; 3Department of Ophthalmology, UPMC Children’s Hospital of Pittsburgh, Pittsburgh, PA, USA; 4Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA; 5Department of Ophthalmology, Hôpitaux Universitaires de Genève, University of Geneva, Geneva, Switzerland; 6Glaucoma Division, Moorfields Eye Hospitals, Dubai, United Arab Emirates
*These authors contributed equally to this work
Correspondence: Mohamed S Sayed, Glaucoma Division, Moorfields Eye Hospitals, Dubai, United Arab Emirates, Tel +97144297888, Email [email protected]
Purpose: The Paul glaucoma implant (PGI, Advanced Ophthalmic Innovations, Singapore, Republic of Singapore) is a recently developed novel non-valved glaucoma drainage device (GDD) designed to effectively reduce the intraocular pressure (IOP) in glaucoma patients with a theoretically reduced risk of postoperative complications such as hypotony, endothelial cell loss, strabismus, and diplopia. Limited literature has evaluated its use in adult glaucoma; however, its use in pediatric glaucoma has not been reported to date. We present our early experience with PGI in refractory childhood glaucoma.
Patients and Methods: This study was retrospective single-surgeon case series in a single tertiary center.
Results: Three eyes of 3 patients with childhood glaucoma were enrolled in the study. During nine months of follow-up, postoperative IOP and number of glaucoma medications were significantly lower than preoperative values in all the enrolled patients. None of the patients developed postoperative complications including postoperative hypotony, choroidal detachment, endophthalmitis, or corneal decompensation.
Conclusion: PGI is an efficient and relatively safe surgical treatment option in patients with refractory childhood glaucoma. Further studies with larger number of participants and longer follow-up period are required to confirm our encouraging results.
Keywords: glaucoma, pediatric, intraocular pressure, tube, Paul glaucoma implant
Introduction
Childhood glaucoma is a heterogeneous group of ocular disorders characterized by increased IOP, which leads to glaucomatous optic neuropathy.1,2 GDDs are usually used in refractory cases or as a first-line surgery in select secondary glaucoma cases. The most used GDDs are the Ahmed glaucoma valve (AGV, New World Medical Inc., Rancho Cucamonga, CA) and the Baerveldt glaucoma implant (BGI, Abbott Medical Optics Inc., Santa Ana, CA).3 Recently, several GDDs have been introduced to the market, such as the Ahmed ClearPath (ACP, New World Medical, Rancho Cucamonga, CA) and the Paul glaucoma implant (PGI, Advanced Ophthalmic Innovations, Singapore, Republic of Singapore), with limited literature evaluating their efficacy and safety in the pediatric population.4,5
The PGI is a valveless device made of medical-grade silicone making its implantation easier due to pliability. The internal tube diameter is 0.127 mm and external tube diameter is 0.467 mm. Both are smaller than those of AGV and BGV which might decrease corneal endothelial loss and decrease the risks of tube erosion and exposure. The breadth of the PGI endplate is 21.9 mm, the width is 16.11 mm, and the surface area is 342.1 mm2.
In this case series, we evaluated the efficacy and safety of PGI in 3 childhood glaucoma eyes with at least 9 months of follow-up.
Materials and Methods
The study adhered to the tenants of the Declaration of Helsinki. Due to the case series nature of our study, it was exempted from ethical approval by the ethical committee of Moorfields Eye Hospital Dubai. Written informed consent was obtained from all subjects and their legal guardians to publish the case details and any accompanying images. This study included patients with diagnosis of refractory childhood glaucoma with uncontrolled IOP on maximal medical treatment or after failure of previous glaucoma procedures. All patients underwent full ophthalmological examination preoperatively and at 1 week, 1 month, 3 months, 6 months and 9 months postoperatively. At each visit, clinical parameters including IOP, using Tono-Pen (Reichert, Inc, Depew, NY) at all the visits, number of glaucoma medications, Snellen’s visual acuity, slit-lamp examination, dilated fundus exam using 28 diopter lens, and postoperative complications were collected. Humphrey visual field (HVF) 24–2 (Carl Zeiss Meditec Dublin, CA) was performed in patient 2.
Surgery (Figure 1 and Supplementary Video) was performed by a single surgeon (MSS) in the supertemporal quadrant in all 3 cases. After creating a peritomy and cauterizing bleeding points, the superior and lateral rectus muscles were isolated. A 6-0 prolene ripcord intraluminal stent was placed. The PGI wings were tucked under the muscles, and the plate was secured to the sclera using 8-0 nylon sutures. The opposite end of the ripcord was tucked under the temporal conjunctiva. The tube was cut to an appropriate length, inserted into the anterior chamber with the bevel directed away from the iris. In cases #1 and 3, tube coverage was achieved by creating a partial thickness scleral flap. In case #2, a half-thickness corneal patch graft was used to cover the tube. The conjunctival peritomy was then closed.
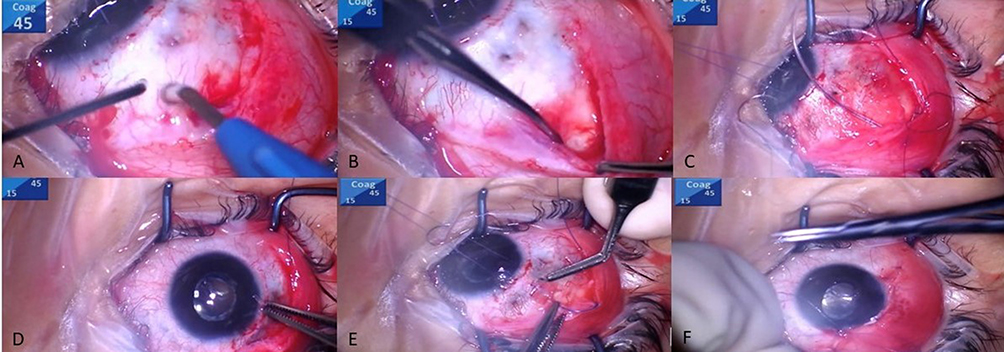 |
Figure 1 Surgical steps of Paul glaucoma implant (PGI) insertion. (A) Fornix-based peritomy was performed, and bleeding points were cauterized, (B) The rectus muscles were isolated, (C) The PGI was inserted (note the ripcord inside the tube lumen), (D) Holding the tube end before inserting it into the anterior chamber, (E) The tube is secured underneath a scleral flap, (F) The conjunctiva was closed. |
Results
We included 3 eyes of 3 patients who underwent PGI surgeries. The main clinical findings in our case series are presented in Table 1.
 |
Table 1 Baseline and Postoperative Clinical Information of the Whole Cohort |
Case 1
A 6-year-old girl presented with bilateral glaucoma following cataract surgery (GFCS) for congenital cataracts in both eyes. She had a history of 360-degree-trabeculotomy - once in the right eye (RE) and twice in the left eye (LE). Her best corrected visual acuity (BCVA) was 20/50 in the RE and 20/200 in the LE. The slit-lamp exam showed bilateral pseudophakia. IOP was 24 mmHg and 5 mmHg in the RE and LE, respectively, on dorzolamide-timolol twice daily, travoprost once daily, and apraclonidine three times daily, all in the RE only. Fundus examination revealed cup-to-disc (C/D) asymmetry (0.4 RE and 0.7 LE). The patient underwent PGI in the RE. On postoperative week 1 (POW-1), the IOP was 12 mmHg on no glaucoma medications. At postoperative month-1 (POM-1), IOP was 16 mmHg RE, and she was restarted on a dorzolamide-timolol twice daily. The ripcord was removed on POM-2, leading to an IOP of 13 mmHg RE. Nine months postoperatively, her IOP was 14 mmHg in the RE and 20 mmHg in the LE on dorzolamide-timolol twice daily in both eyes with a best corrected visual acuity (BCVA) 20/50 and 20/100 in the RE and LE, respectively.
Case 2
A 15-year-old girl with a history of bilateral primary congenital glaucoma (PCG) with prior bilateral trabeculectomies presented with a BCVA of no light perception in the RE and 20/25 in the LE. IOP was 24 mmHg and 46 mmHg in the RE and LE, respectively, on maximal medical therapy (oral acetazolamide, brimonidine-timolol, brinzolamide, latanoprost). Slit-lamp examination disclosed enlarged corneal diameter with old Haab’s striae in both eyes. C/D ratios were 1.0 in the RE and 0.8 in the LE on fundus exam. Humphrey visual field testing (HVF) of the LE demonstrated inferior arcuate and superior and inferior nasal scotomas. PGI was performed in the LE. IOP in the LE was 20 mmHg on POW-1, 12 mmHg on POM-2, 10 mmHg on POM-6, and 10 mmHg on POM-9 on no antiglaucoma medications during any of the postoperative visits. The ripcord intraluminal stent did not need to be removed in this patient, and IOP was adequately controlled without any medications.
Case 3
A 7-year-old boy was referred for management of uncontrolled glaucoma in the LE due to PCG and traumatic glaucoma. He had a history of goniotomy in the LE at the age of 8 months. At presentation, IOP was 12 mmHg in the RE and 28 mmHg in the LE on a combination of brinzolamide-timolol twice daily in both eyes, latanoprost once daily in the LE, and oral acetazolamide. The C/D ratios were 0.4 and 0.9 in the RE and LE, respectively. The BCVA was 20/40 in the RE and 20/300 in the LE. Enlarged corneal diameter and Haab’s Striae were noted in the LE. After PGI implantation in the LE, IOP was 36 mmHg on POW-1, which dropped after ripcord removal to 11 mmHg without any IOP-lowering agents on POM-2. On the POM 9 visit, his IOP in the LE continued to be controlled off-medications (11 mmHg).
Discussion
Paul glaucoma implant was developed by Professor Paul Chew (National Institute of Singapore) to control IOP with a theoretically higher safety profile compared to other GDDs (Figure 2). The outer tube diameter is significantly smaller compared to the AGV and BGI, which may theoretically reduce the effect of the implant on corneal endothelial cell density (ECD). However, long-term studies are needed to confirm this hypothesis. Although the inner tube diameter is smaller than other GDDs, resistance to aqueous outflow is theoretically mildly elevated while simultaneously reducing the risk of hypotony. In our series, none of the patients had postoperative hypotony. The device was designed to increase the surface area of aqueous drainage while reducing the area tucked under the muscles, theoretically reducing the risk of diplopia and strabismus.
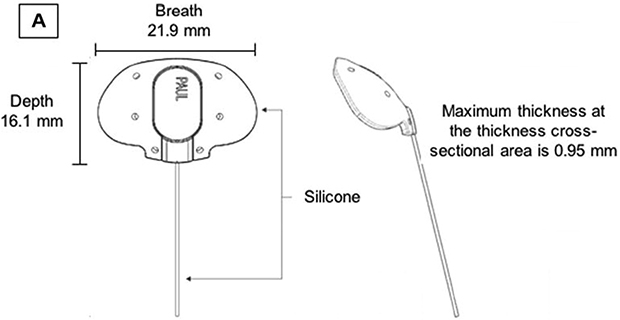 |
Figure 2 (A) Design of Paul glaucoma implant. Courtesy of advanced ophthalmic innovations. |
Limited literature evaluated the efficacy of PGI in adult glaucoma.6–10 Tan et al6 studied 45 eyes with refractory glaucoma or patients who had previously failed glaucoma surgery. The mean follow-up duration was 25 months. They reported a complete success rate, defined as IOP between 6 and 18 mmHg without glaucoma medications or development of vision-threatening complications or re-operation, of 71.1.%. The mean IOP was significantly reduced from a baseline of 19.8±6.3 mmHg on 3.2±0.8 medications to 13.9±3.7 mmHg on 0.2±0.6 at the 2-year follow-up visit. In a retrospective study that included 99 eyes who underwent PGI surgeries by Vallabh et al,8 the failure rate (postoperative IOP of >21 mmHg, <20% IOP reduction from baseline values, loss of light perception, need for further glaucoma surgeries, or PGI removal) was 9.3%. There was a statistically significant reduction in the mean preoperative IOP decreased from 28.1±9.0 mmHg to 13.6±4.7 mmHg at 6-months and 13.3±4.4 mmHg at 12-months. Similarly, the mean number of glaucoma medications was significantly reduced from 3.61±1.09 at baseline to 1.22±1.21 at 6-months and 1.25±1.28 at the 12-month follow-up visit. Four eyes developed hyphema, two eyes had postoperative hypotony, and cystoid macular edema was reported in the early postoperative period.
In a recent study9 that evaluated the outcomes of PGI outcomes in 45 eyes of 41 patients during one-year follow-up period, the mean percentage of IOP reduction was 48.83% at 12 months form preoperative values. The mean number of preoperative glaucoma medications was 3.44 that decreased to 0.47 at 12 months (p < 0.05). In this cohort, 4 eyes (8.9%) developed choroidal detachments due to hypotony which resolved without further interventions after 6 weeks, but one eye (2.2%) needed an injection of viscoelastic due to persistent hypotony. In our series, the PGI was effective in reducing the IOP and the number of glaucoma medications in all 3 eyes without any cases of postoperative hypotony or vision-threatening complications. Our series highlights the potential role of PGI in childhood glaucoma management.
The PGI with its plates surface area has been useful in our limited series of children aged between 6 and 15 years. It remains to be seen if this device’s volume would be safely implantable in younger children and newly born with smaller globe size.
The current study is limited by its small sample size, retrospective nature, and short follow-up. Future studies with larger cohorts and longer follow-up periods are needed to evaluate the efficacy and safety of PGI.
Abbreviations
AGV, Ahmed glaucoma valve; BCVA, best-corrected visual acuity; BGI, Baerveldt glaucoma implant; C/D, cup-to-disc; ECD, endothelial cell density; GDD, glaucoma drainage devices; IOP, intraocular pressure; LE, left eye; PGI, Paul glaucoma implant; RE, right eye.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Due to the case series nature of our study, it was exempted from ethical approval by the ethical committee of Moorfields Eye Hospital Dubai. Written informed consent was obtained from all subjects and their legal guardians to publish the case details and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosures
The authors report no relevant financial disclosures.
References
1. Tam EK, Elhusseiny AM, Shah AS, et al. Etiology and outcomes of childhood glaucoma at a tertiary referral center. J AAPOS. 2022;26(3):117.e1–117.e6.
2. Thau A, Lloyd M, Freedman S, Beck A, Grajewski A, Levin AV. New classification system for pediatric glaucoma: implications for clinical care and a research registry. Curr Opin Ophthalmol. 2018;29(5):385–394.
3. Elhusseiny AM, VanderVeen DK. Outcomes of glaucoma drainage devices in childhood glaucoma. Semin Ophthalmol. 2020;35(3):194–204. doi:10.1080/08820538.2020.1781906
4. Khodeiry M, Sayed MS. New glaucoma drainage implants available to glaucoma surgeons. Curr Opin Ophthalmol. 2023;34(2):176–180. doi:10.1097/ICU.0000000000000936
5. Elhusseiny AM, VanderVeen DK. Early experience with Ahmed clear path glaucoma drainage device in childhood glaucoma. J Glaucoma. 2021;30(7):575–578. doi:10.1097/IJG.0000000000001855
6. Tan MCJ, Choy HYC, Koh Teck Chang V, et al. Two-year outcomes of the Paul glaucoma implant for treatment of glaucoma. J Glaucoma. 2022;31(6):449–455. doi:10.1097/IJG.0000000000001998
7. Koh V, Chew P, Triolo G, et al. Treatment outcomes using the PAUL glaucoma implant to control intraocular pressure in eyes with refractory glaucoma. Ophthalmol Glaucoma. 2020;3(5):350–359. doi:10.1016/j.ogla.2020.05.001
8. Vallabh NA, Mason F, Yu JTS, et al. Surgical technique, perioperative management and early outcome data of the PAUL® glaucoma drainage device. Eye. 2022;36(10):1905–1910. doi:10.1038/s41433-021-01737-1
9. Weber C, Hundertmark S, Liegl R, et al. Clinical outcomes of the PAUL® glaucoma implant: one-year results. Clin Experiment Ophthalmol. 2023. doi:10.1111/ceo.14235
10. Elhusseiny AM, Hassan AK, Azhari JO, et al. Ahmed and Baerveldt glaucoma drainage devices in childhood glaucoma: a meta-analysis. J Glaucoma. 2023. doi:10.1097/IJG.0000000000002235
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.