Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Early Detection of Iron Overload Cardiomyopathy in Transfusion Dependent Thalassemia Patients in Sulaimaniyah City, Iraq
Authors Ahmed RA ![]() , Salih AF
, Salih AF ![]() , Omer SH, Rahman HS
, Omer SH, Rahman HS ![]() , Rasool LK
, Rasool LK
Received 19 December 2021
Accepted for publication 8 March 2022
Published 22 March 2022 Volume 2022:18 Pages 259—271
DOI https://doi.org/10.2147/TCRM.S354574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Rana Adnan Ahmed,1 Aso Faeq Salih,2 Shirwan Hamasalih Omer,1 Heshu Sulaiman Rahman,1,3 Luqman Khalid Rasool4
1Department of Physiology, College of Medicine, University of Sulaimani, Sulaimaniyah, Republic of Iraq; 2Department of Pediatrics, College of Medicine, University of Sulaimani, Sulaimaniyah, Republic of Iraq; 3Department of Medical Laboratory Sciences, Komar University of Science and Technology, Sulaimaniyah, Republic of Iraq; 4Hiwa Hematology/Oncology Hospital and Sulaimaniyah Thalassemia and Congenital Blood Disorders Center, Sulaimaniyah, Republic of Iraq
Correspondence: Rana Adnan Ahmed; Heshu Sulaiman Rahman, Department of Physiology, College of Medicine, University of Sulaimani, Sulaimaniyah, Republic of Iraq, Tel +964 7703665588 ; +964 7726159598, Email [email protected]; [email protected]
Background: Lifelong blood transfusion is recommended for patients with transfusion-dependent thalassemia (TDT) that lead to iron overload and results in cardiomyopathy (CM).
Aim: To assess the accuracy of several electrocardiographic (ECG) data in patients at high risk of arrhythmia, early detection of structural and functional changes in left atrium and ventricle using ECG and echocardiography (two dimensional, M-mode echocardiography along with Doppler studies), and to observe the correlations between plasma B-type atrial natriuretic peptide (BNP)/serum ferritin and ECG with Doppler as well as echocardiographic changes in patients with TDT.
Methods: The current prospective case-control study included 75 TDT patients and 74 control subjects with the mean age of 9.55 and 9.93 years, respectively. Participants were assessed for the socio-demographic, physical examinations, serum ferritin, plasma BNP, ECG, 2D echocardiography, and tissue/pulse wave Doppler.
Results: The mean of serum ferritin and plasma BNP were significantly (p< 0.001) higher in the cases (1475.19 ng/mL and 47.63 pg/mL, respectively) than controls (41.3 ng/mL and BNP 23.37 pg/mL, respectively). ECG findings showed significant higher P-wave dispersion, QRS duration, QT duration and dispersion, and JTc dispersion in cases than controls. Echocardiography findings revealed diastolic dysfunction with preserved ejection fraction (EF) in thalassemia cases, as well as significant higher left ventricular (LV) mass, LV internal diameters during systole and diastole (LVIDs and d) and LV posterior wall thickness during diastole (LVPWd) in cases than controls (p< 0.05). Also, a significant (p< 0.05) correlation between BNP and QT dispersion was found in patients.
Conclusion: These findings suggest the usefulness of ECG, 2D echocardiographic, Doppler studies and plasma BNP, with no significant beneficial effect of serum ferritin level in detecting early cardiac changes in patients with TDT.
Keywords: hereditary disease, blood transfusion, iron overload, thalassemia complications, case-control study
Introduction
β-Thalassemia is a common hereditary blood disease in the Middle East and other developing countries,1 in which there is a reduction or absence in the synthesis of the β-globin chain leading to ineffective erythropoiesis and malfunctioning hemoglobin A (HbA).2,3 Patients with β-Thalassemia require frequent blood transfusion based on the clinical severity, whether it is major on intermedia, or they may not need any of the minor types.4
All thalassemia patients are susceptible to iron overload, and those who are transfusion-dependent thalassemia (TDT) are at higher risk of developing cardiac complications as a result of iron deposition in the cardiac-myocyte due to parenteral iron induction.5,6
However, the pathophysiology of heart disease in β-thalassemia is multifactorial, with inflammation and immunogenic factors playing a significant role.7,8 The iron deposition could adversely affect the heart’s structure and function, producing ventricular diastolic and systolic dysfunction, often in conjunction with cardiac rhythm disturbances including slowed electrical conduction, heart-block, increased susceptibility to atrial fibrillation, and frequent premature ventricular contraction and eventually sudden death.5 Although the heart is not the first target organ; cardiac siderosis is important since it contributes to high morbidity and mortality rates, accounting for >60% of deaths in thalassemia.9,10
With increased life expectancy to those patients after the commencing of iron chelation therapy,5 the need for evaluating cardiac iron-overload emerged, especially it’s a slowly progressive, dose-dependent process and may take decades to be detectable by the conventional laboratory and clinical measures.10 Also, it can be reversed by mono or combined chelation therapy, particularly in the case of early diagnosis that provides a better life quality and prevents severe complications to patients with thalassemia.4,11
Dilated CM is a progressive ventricular wall thinning accompanied by gradual functional impairment12 in which its echocardiographic diagnostic criteria are LVIDd of >117%, left ventricular ejection fraction (LVEF) of <45% and/or fractional shortening (FS) of <25%.13
In TDT patients, the cause of CM is infiltration of iron inside the cardiac myocyte, causing prominent diastolic dysfunction and increased wall thickness.13 Generally, CM starts with iron-mediated cardiovascular injury that leads to altered excitation-contraction coupling and electrophysiology followed by diastolic dysfunction and finalized with dilated biventricular CM.14
Serum ferritin level is used along with Hb level routinely to assess the need for the burden of blood transfusion in these patients.5 Hb levels should be kept around 10 g/dL to suppress ineffective erythropoiesis and its complications. At the same time, serum ferritin should not exceed 300 ng/mL, along with echocardiography assessment to keep the balance between the effect of anemia on the heart and the burden of cardiac hemosiderosis.15 Routine echocardiography measures the systolic function of the heart, EF, LV chamber dimensions and correlate results with serum ferritin and Hb.16
BNP is used to detect early cardiac iron overload, even when EF is reserved.17 It is released from the cardiac myocyte in response to stretching due to volume overload.18 It has both diagnostic and prognostic values for detecting cardiac function and the effectiveness of chelating therapy, especially in congestive heart failure.19
ECG changes such as P-wave abnormalities, P-wave dispersion, QT interval prolongation and dispersion, QRS widening and T-wave abnormality; were found to proceed with echocardiographic abnormalities.20 Patients with iron-overload cardiomyopathy (IOC) can be asymptomatic, have diastolic dysfunction, systolic dysfunction, congestive heart failure, pulmonary hypertension and arrhythmia, which may lead to sudden death.21,22
Although most thalassemia centers routinely assess the cardiac function by echocardiography, these assessments usually measure the systolic function, which occurs at the late course of the disease. Due to pulmonary hypertension, the impaired left diastolic function is mostly seen with higher serum ferritin that indicates high iron deposition in the cardiac myocyte.3
Although iron is essential for multiple cellular activities, but is highly toxic, forming oxidative reactions and free oxygen radicals; thus, its intracellular/extracellular concentrations should be kept in balance. Therefore, this study aimed to assess the accuracy of several electrocardiographic data in predicting patients risk of arrhythmia, early detection of structural and functional changes in left atrium/ventricle and to observe correlations between BNP, serum ferritin and ECG with echocardiographic, as well as Doppler changes in patients with TDT.
Methods
Study Setting and Participants
This case-control study was conducted on 75 patients with TDT and 75 healthy subjects at the Department of Cardiology, Dr. Jamal Ahmed Rashid’s Pediatric Teaching Hospital, with the cooperation of Sulaimaniyah Thalassemia and Congenital Blood Disorders Center, Sulaimaniyah City, Republic of Iraq from September 2019 till September 2021. Written informed consent was taken from all study participants’ parents or guardians. However, one healthy subject was excluded from the control group due to cardiac disease that was discovered accidentally by an echocardiographic assessment during the study.
Ethical Approval
The study was performed following the Declaration of Helsinki and approved by the ethical committee of College of Medicine, University of Sulaimani, Sulaimaniyah, Republic of Iraq, with COM/UNIVSUL/24/2852019.
Inclusion Criteria
Patients with TDT (major/intermedia) who received >15 units of blood with no cardiac symptoms aged 2.5–18 years of both genders were included in this study.
Exclusion Criteria
Patients with thalassemia major or intermedia not received 15 units of blood, those who already had cardiac complications and were on treatment for it, and patients with an EF of <60% were not enrolled in this study. Additionally, patients and controls with acute illnesses such as flu or other sensitive conditions that may affect serum ferritin levels were excluded from this study.
Questionnaire
A detailed questionnaire for the collection of socio-demographic data (age, sex, and residency) and anthropometric measures (height and weight to determine body surface area using the Dubois formula)23 was filled out for each participant. The subjects and their parents/guardians were asked about age, age at which thalassemia has been diagnosed, type of thalassemia, age at which blood transfusion started, number of units of blood received by the patient per year, iron chelation therapy, and adherence to the therapy. In addition, the entire cardiovascular history was covered to find any symptoms of cardiac complications, including dyspnea, orthopnea and syncope. It also includes questions about the history of splenectomy and any other surgeries.
Assessment of Participants for Cardiovascular Diseases
All participants were evaluated for cardiovascular diseases by general examination and a detailed cardiovascular examination to ensure they did not have any obvious cardiac complications; otherwise, patients were excluded from the study.
Electrocardiographic Assessment
Twelve leads electrocardiography was conducted on all participants under standard measures with a speed of 50 mm/sec and 10 mm/millivolt amplitude using a portable ECG device of ASPEL (AsCARD ORANGE). Heart rate, rhythm, cardiac axis, P-wave amplitude, duration and dispersion, QRS duration, JT, QT and QTc with QT dispersion were manually calculated for all participants. P-wave dispersion was calculated manually in milliseconds (ms) by measuring the difference between the widest P-wave and the narrowest one in all leads of the same record. QT interval was also manually measured from the beginning of the Q-wave till the end of the T-wave using the tangent method to locate its end. Then, the reading was corrected to obtain QTc using the Frederica correction for regular heart rate and the Bazett formula for irregular heart rate.
Echocardiographic Assessment
A detailed echocardiographic study was performed on all participants using the Vivid E9 device and 3000 MHz transducers. In this regard, a standard two-dimensional (2D) echocardiography and M-mode was used to measure chamber size, EF, and wall thickness of the LV, as well as tricuspid annular plane systolic excursion (TAPSE) and mitral annular plane systolic excursion (MAPSE). In addition, the heart chamber dimensions and wall thickness had been corrected by the Z-score system to the body surface area (BSA). Then, pulse wave Doppler and tissue Doppler were used to measure the peak mitral inflow velocities at early (E) and late (A) diastole, and their ratio (E/A) was determined. Finally, mitral annular early diastolic velocity (e^) and the left atrial pressure were estimated through the ratio of E/e^ along with pulmonary venous flow velocity in systolic (S) and diastolic (D) components with their ratio (S/D).
Biochemical Parameters
Blood samples were collected from TDT patients before blood transfusion, while blood samples were collected from the controls after the clinical assessment. Serum ferritin was measured using chemiluminescence immunoassay, while BNP was determined using a fluorescent nanoparticle immunoassay designed to measure the BNP in vitro human plasma.
Statistical Analysis
The statistical computation was enhanced using the statistical method (SPSS, version 25.0) to determine descriptive statistical data analysis (frequency, percentage, minimum, maximum, mean, and standard deviation) and inferential data analysis using Chi-square, independent samples t-test and one-way ANOVA (F-test). Correlations between variables were found using Pearson’s correlation. The criteria for the probability (p-value) level of significance were shown as; a. high significance (p<0.001), b. Significant (p<0.05), c. Non-significant (p>0.05), and d. very highly significant (p<0.000).
Results
Socio-Demographic and Clinical Characteristics of Studied Participants
After applying exclusion criteria, 75 thalassemia cases with a mean age of 9.55 ± 3.83 and 74 age and sex-matched control subjects with a mean age of 9.93 ± 3.66 were included in this study (Table 1). There were no significant differences (p>0.05) in the gender between cases and controls. Among the patients, 18.7% had major thalassemia, while 81.3% had intermedia. On the other hand, 90.7% of cases had facial disfigurement, and the percentage of splenomegaly, hepatomegaly, and jaundice were 88%, 26.7%, and 96%, respectively, with none of these findings in control subjects (p<0.05). Splenectomy was present in 5.3% of thalassemia patients. Neither basal crepitation nor cardiac murmur was present in cases and the controls (Table 1).
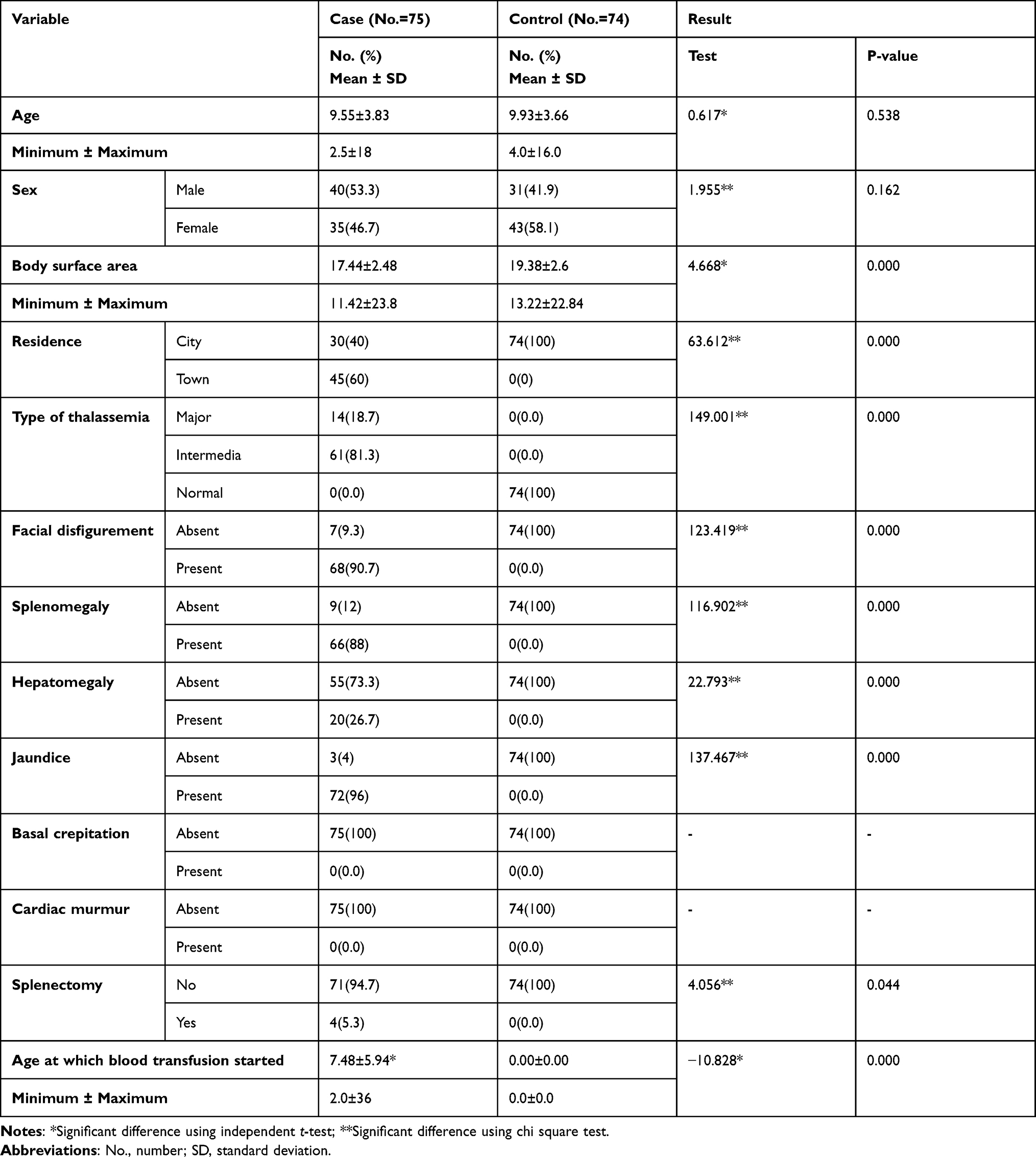 |
Table 1 The Association Between Case and Control Groups in Relation to Socio-Demographic Data |
ECG Measurements
There were no significant differences in heart rate, rhythm disturbances and cardiac axis deviations between thalassemia cases and controls (p>0.05). P-wave dispersion and QT dispersion were significantly higher in cases compared to the controls (p<0.05). The duration of QRS, QT and JTc in patients was higher than in the controls (p<0.05). At the same time, QTc duration between cases and controls was not significant (p>0.05) (Table 2).
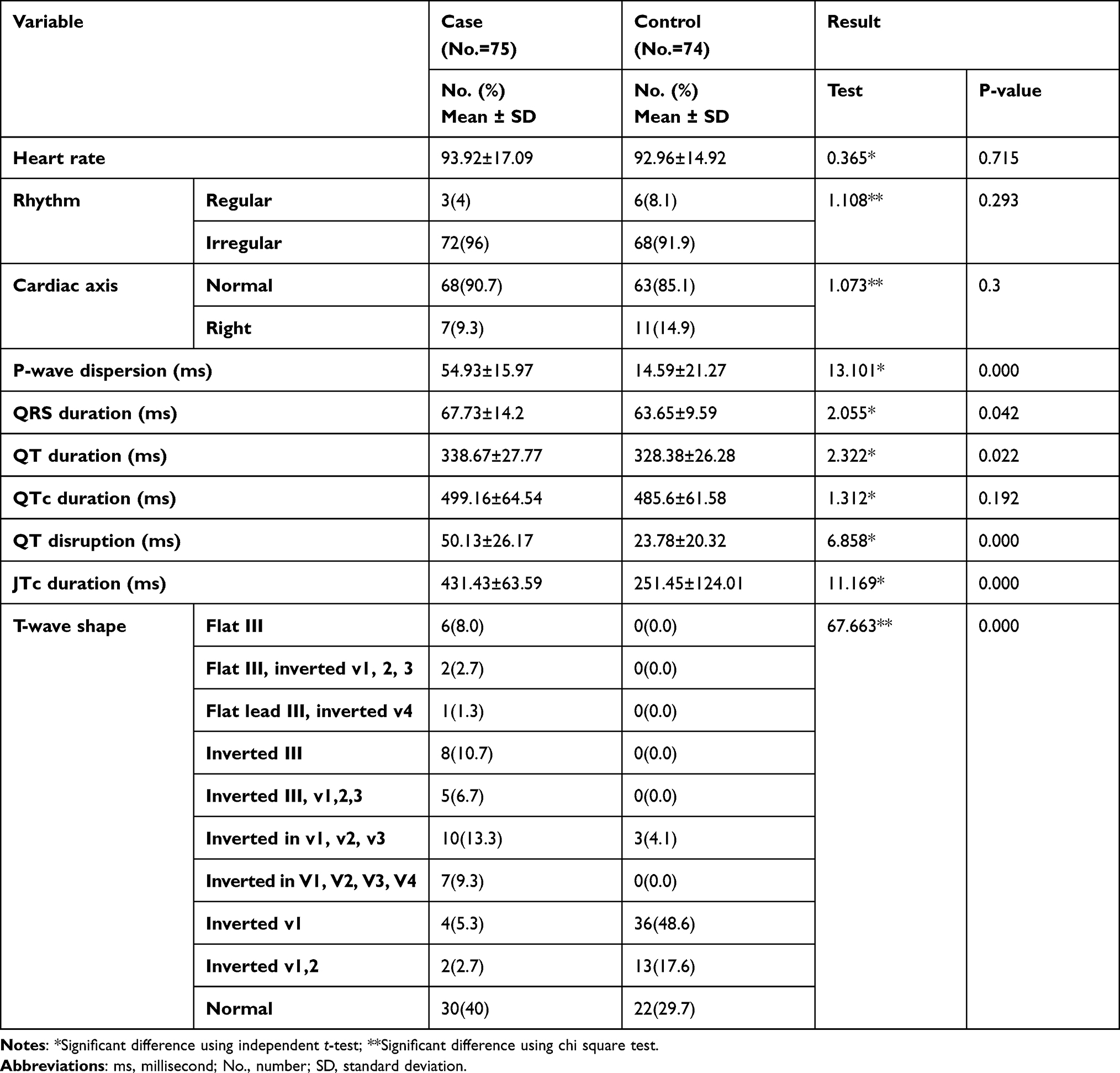 |
Table 2 The Association Between Case and Control Group in Relation to Electrocardiogram Measurement |
Two-Dimensional Echo Parameters
There was a very highly significant difference between cases and controls in left ventricular mass, left ventricular internal diameter in diastole and systole (p<0.000). Left posterior wall thickness in diastole was significant (p<0.05), while systole was not significant. MAPSE also significantly differed between both groups. Interventricular septal had no significance in systole or diastole (p>0.05). There was no significant difference for TAPSE, EF and FS of the LV (Table 3).
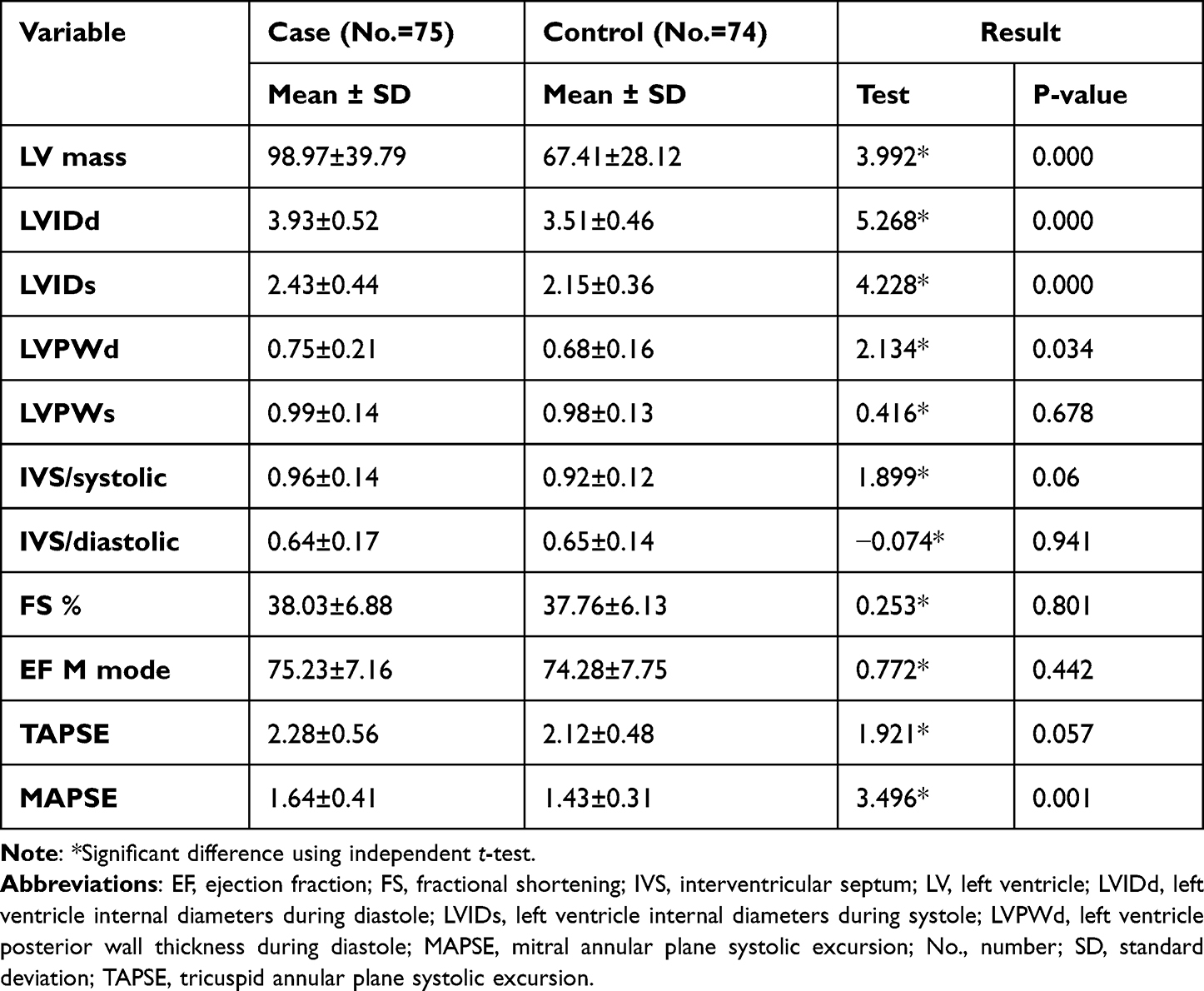 |
Table 3 The Association Between Case and Control Groups in Relation to 2-Dimension-Echo Measurement |
Pulse-Doppler Velocities
LV in diastole Doppler wave showed significantly higher E wave and E/A ratio (p<0.025 and p<0.000, respectively) in cases than controls. The ratio of trans-mitral (E/e^) was very highly significant (p<0.000), whereas the early diastolic velocity (e^) showed a significant difference. Peak flow pulmonary velocities during ventricular diastole (D) and S/D ratio expressed a highly significant difference. Elevation flow pulmonary velocities during ventricular systole (S) had no significant difference (Table 4).
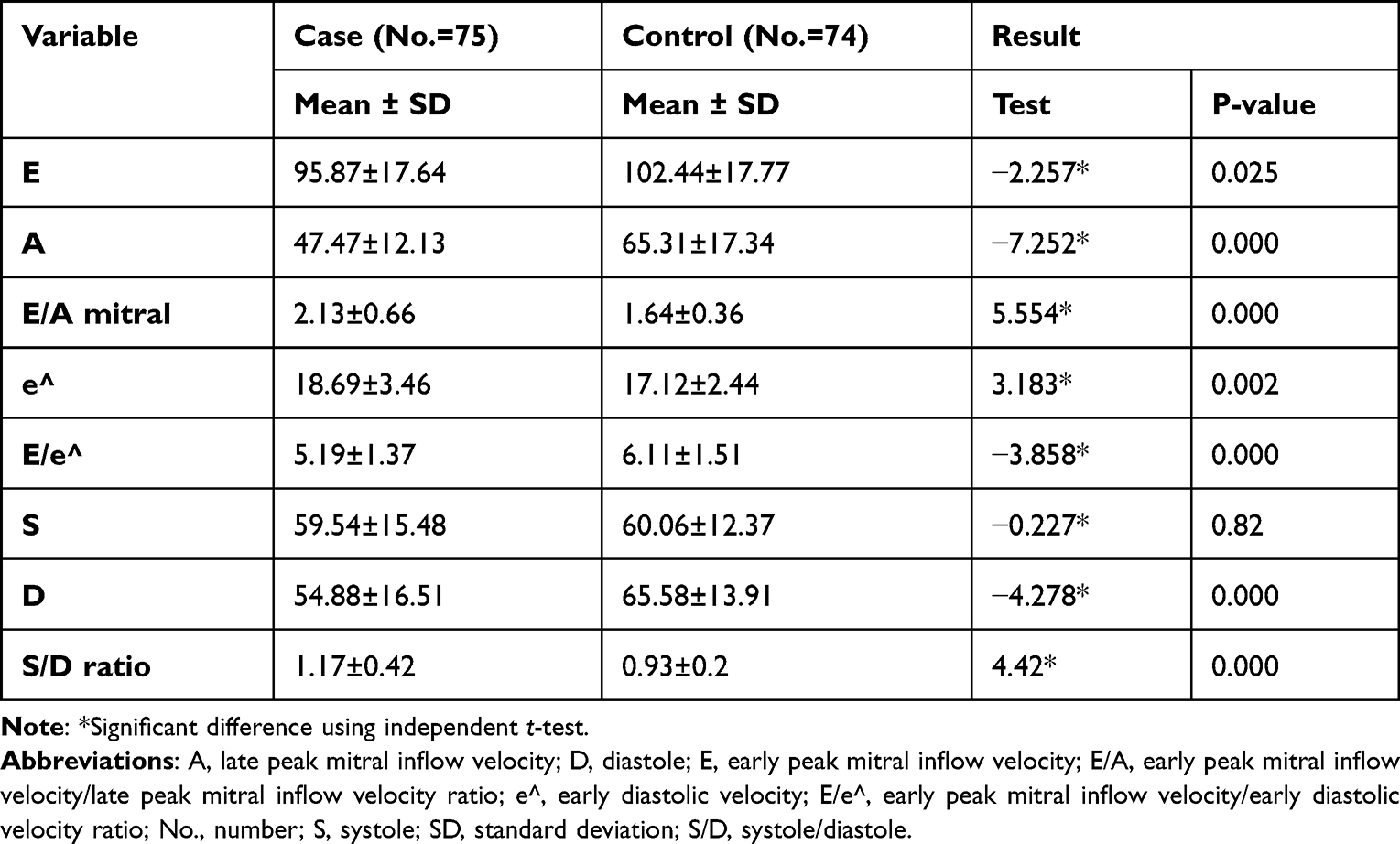 |
Table 4 The Association Between Case and Control Groups in Relation to Doppler Study |
The Z-score correction of LV wall thickness between both groups showed a highly significant difference in the LV posterior wall in both systole and diastole and a highly significant difference in interventricular septa in systole (p<0.000). While interventricular septum (IVS) diastolic thickness showed no significance, BSA showed a significant reduction in the cases (Table 5).
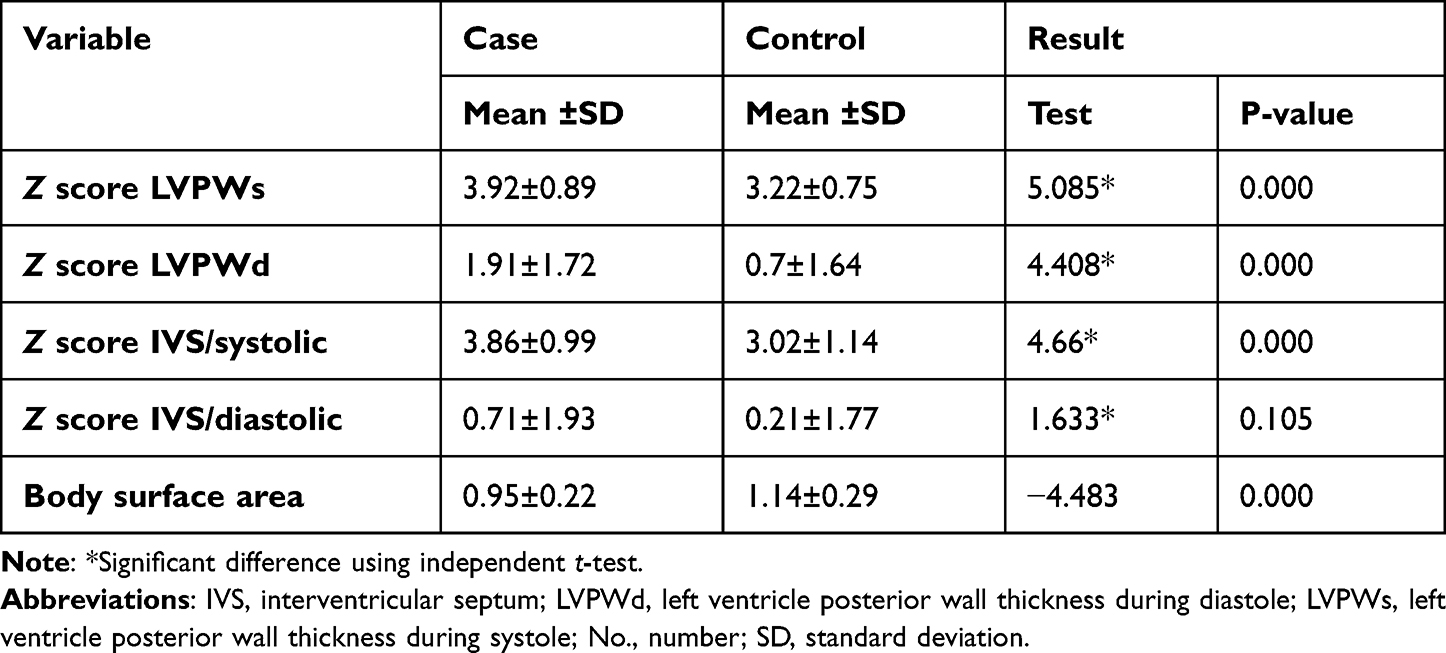 |
Table 5 Z-Score of Left Ventricular Wall Thickness and Interventricular Septa in Systole and Diastole Between the Two Study Groups |
Biochemical Tests
There was high serum ferritin and plasma BNP in the cases with a meagre amount for both tests in the controls. Thus, there was a highly significant association in the mean of serum ferritin (1475.19 ng/mL) and plasma BNP (47.63 pg/mL) in cases than controls (41.3 ng/mL and 23.37 pg/mL for both serum ferritin and plasma BNP, respectively) (Figure 1). In addition, there was a very high significant difference between serum ferritin levels in both groups (p<0.000) (Table 6). However, there was no significant correlation between serum ferritin and all echocardiographic parameters (p>0.05) and between serum ferritin and ECG parameters, except for the T-wave abnormalities.
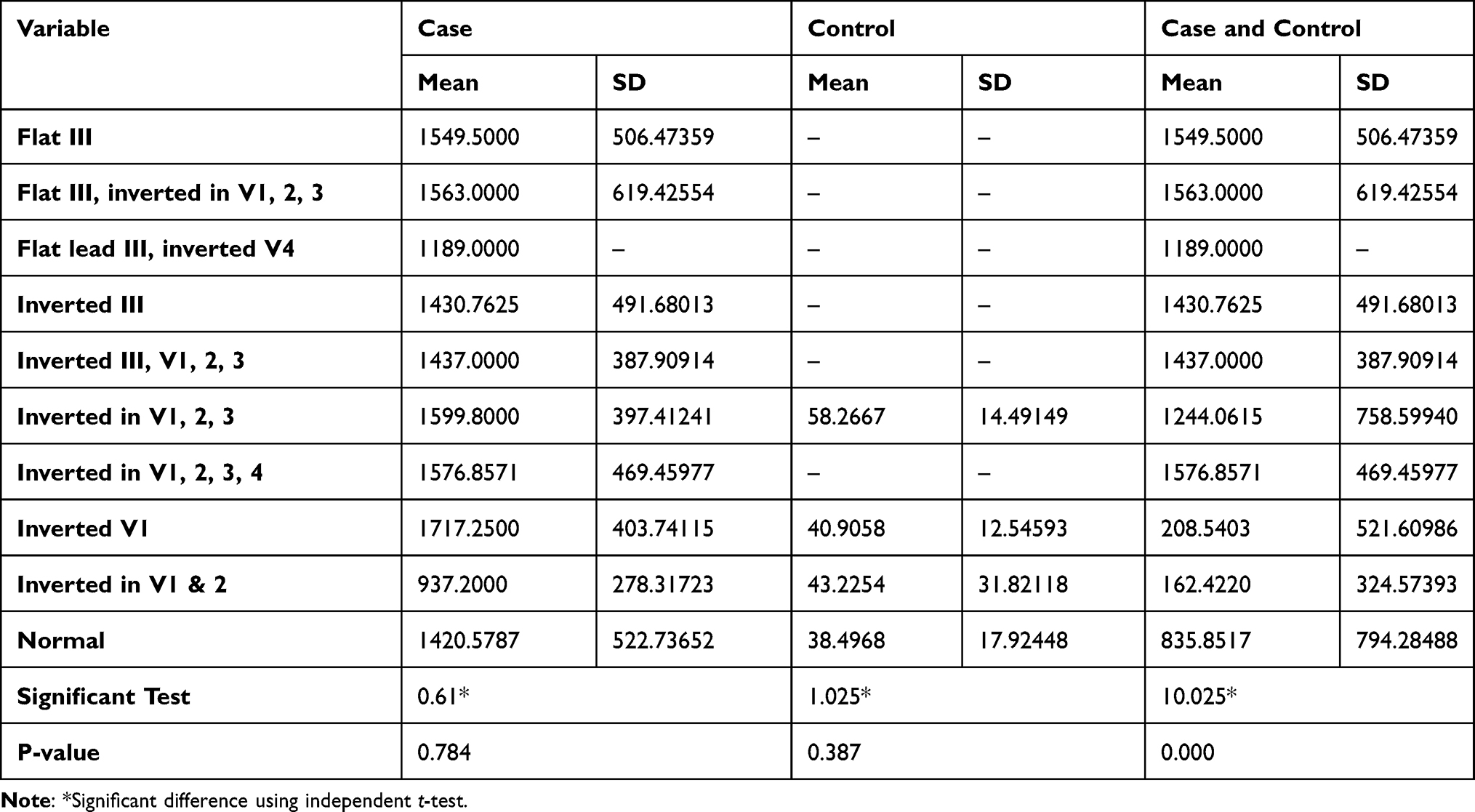 |
Table 6 Comparison the Means of Serum Ferritin and T-Wave Abnormality |
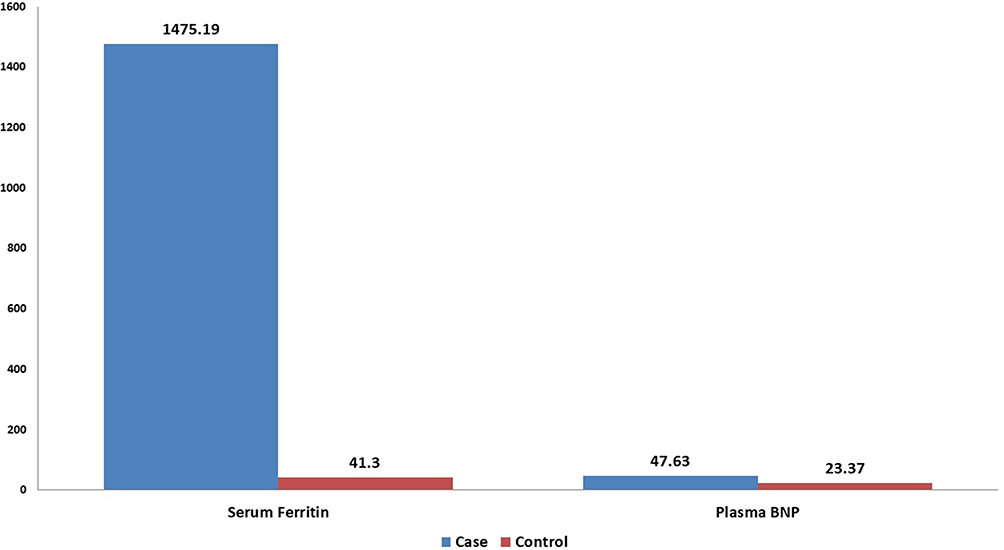 |
Figure 1 The levels of serum ferritin and plasma B-type atrial natriuretic peptide (BNP) in studied groups. |
Correlation Between Different Variables
Plasma BNP showed a significant correlation with LV mass, LVPWd, IVSd, TAPSE and QT dispersion (p<0.05). There was no significant correlation between serum ferritin and LVmass, IVS in systole and diastole in the controls. BNP levels also had no significant correlation with TAPSE in the controls. In both groups, the age was significantly correlated with LV wall thickness in systole and diastole and with IVS (p<0.05), except for the control LVPWd and IVSd (p>0.05) (Table 7).
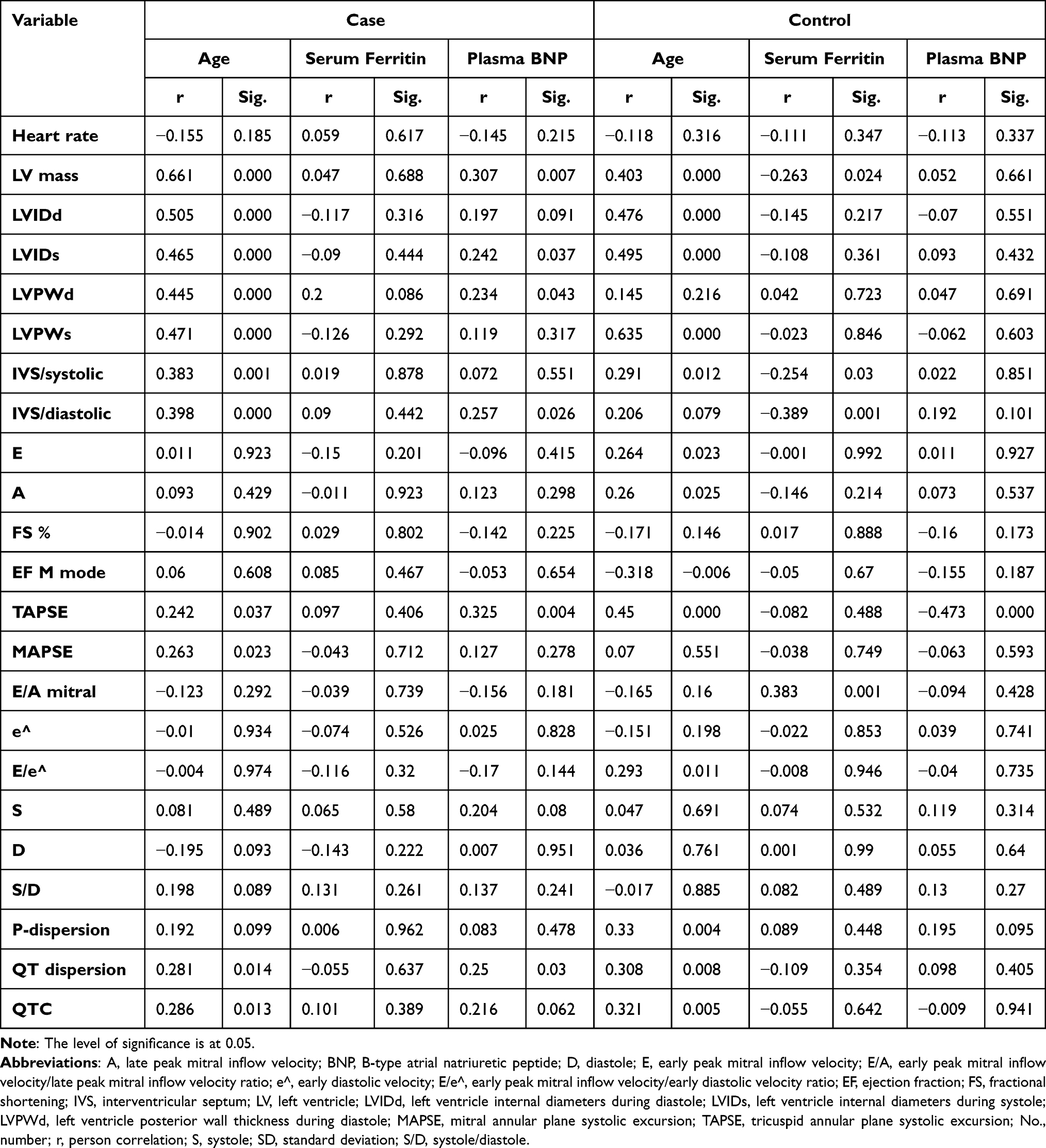 |
Table 7 Correlations Between Age, Serum Ferritin, Plasma BNP and Characteristics in Case and Control Groups |
Discussion
Heart complications represent CM due to increased body iron is characterized by early diastolic dysfunction that develops before systolic dysfunction, in which cardiac iron toxicity is the leading cause of diastolic dysfunction in TDT.24
Regarding ECG findings, no significant differences (p>0.05) in heart rate and rhythm disturbances between thalassemia cases and control groups were found in the current study. These findings align with Patsourakos et al 202025 and Ghandi et al 201815 results that a significant association between heart rate and ECG abnormality did not exist. While these outcomes were inconsistent with Detterich et al 2012 findings, who found heart rate abnormalities in thalassemia major patients, not correlated tachycardia with cardiac iron overload and significantly correlated sinus bradycardia with cardiac iron overload.26
Cardiac axis deviations comparisons between thalassemia and the control group were not significant (p>0.05) in the current study in which 9.3% of TDT had right axis deviation. In this regard, Ramazzotti et al 2008 found right axis deviation as a common finding in 12% of thalassemia major patients.27
Also, we found that P-wave dispersion and QT dispersion were significantly (p<0.05) higher in thalassemia cases than in controls. Similar to our findings, P-wave dispersion was significantly (p<0.05) higher in patients with major thalassemia than controls in studies conducted in Iran by Ghadiri et al 201228 and in Turkey by Nisli et al 2010.29
Additionally, we found significantly (p<0.05) higher duration of QRS, QT and JTc in cases than in controls. Similarly, Patsourakos et al 2020, revealed a significant (p<0.05) longer QRS duration in cases versus control.25 At the same time, QTc duration between patients and controls did not show significant results, similar to other studies’ effects. However, Garadah et al 201030 and Detterich et al 201226 showed significantly (p<0.05) higher QTc and QTc duration in thalassemia subjects than controls. These differences might be due to higher serum ferritin in thalassemia major patients, although we included both thalassemia major and intermedia in this study.
In the current study, repolarization abnormalities and non-specific ECG changes were significantly (p<0.05) associated with thalassemia patients. In addition, T-wave inversion and flat T-wave were higher in cases versus control, whereas, Detterich et al 2012, showed prolonged QT/QTc in thalassemia cases.26
The general finding of this study revealed that the P-wave dispersion, QT dispersion and prolongation, and repolarization abnormality, especially in terms of T-wave changes, were significantly (p<0.05) associated with thalassemia patients. However, the differences in other ECG parameters such as QTc could be due to the population, ethnicity, age group, types of thalassemia, duration of chelation therapy, serum ferritin, and cardiac iron overload. This can be explained as cardiac iron toxicity delays and blocks electrical conduction, which occurs earlier than impaired contractility and subject the patient to re-entry arrhythmia. This phenomenon is considered one of the complications of iron-induced CM that is responsible for atrial fibrillation and sudden death.
BNP is released from cardiac myocytes to the circulation in response to volume overload and stretching. There was a significant (p<0.05) increase in plasma BNP levels in TDT patients than controls with normal EF in the current study. These results are also reported by Kremastinos et al 200731 and Deraz et al 2021,32 who found significantly (p<0.05) high levels of BNP with no clinical presentation of heart failure (HF) nor abnormal EF.
BNP was also found to be correlated with echocardiography findings such as LV mass, LVID s, LVPWd, and IVSd. Same outcomes also were explained by Bosi et al 2003.33 Also, Kremastinos et al 200731 and Huttin et al 202134 found that circulating BNP was higher in patients with isolated diastolic dysfunction, while Kautsar et al 2019 found no correlation.24
Moreover, BSA was significantly (p<0.05) lower in patients than controls. In this respect, Garadah et al 2010 reported the same result and also, they found significant (p<0.05) correlations between BNP and TAPSE, which is inconsistent with our finding of higher MPSE levels.30
The echocardiography measures are the gold standard for evaluating cardiac chambers and function. Tissue and pulse Doppler studies are of great value in assessing diastolic dysfunction in most patients before the impairment of systolic function. Transmitral flow velocity to annular flow velocity ratio (E/e^) is the best Doppler predictor of diastolic dysfunction because it combines transmural pressure and myocardial relaxation.35 In this regard, in our study, the flow velocity transmitral valve (E) was significantly lower in patients than in controls. At the same time, relaxation time was significantly prolonged, and the E/e^ ratio was significantly low between both groups that representing impaired LV relaxation.
Furthermore, Pulse wave Doppler velocity of the LV showed a high E/A (2.13) ratio in this study, indicating reversible restrictive diastolic function. The same result was reported by Garadah et al 2010 but with higher early filling.7 However, we found lower E in patients than controls reported by Kremastinos et al 1993.6
On the other hand, the LVEF% and FS% in the mid cavity sector were normal, indicating that β-TM patients had a preserved systolic function. MAPSE was significantly (p<0.05) higher in the patients, which means impaired longitudinal LV function. These findings were similar to another study that found an increased pulmonary vein S/D ratio was significantly (p<0.05) increased in thalassemia patients.36
Consequently, we assessed serum ferritin level to determine iron overload, and we found that mean serum ferritin was significantly (p<0.05) higher in TDT than the controls. These findings are also reported by Majd et al 2015 who found a significant (p<0.05) correlation between serum ferritin with heart and liver MRI in patients with TDT.37 Although high serum ferritin levels were found in these patients; there was no correlation with other parameters in this current study. Another study found the same result but significantly correlated serum ferritin and tissue iron deposition using CMRI and liver tissue biopsies.38 A significant correlation (p<0.05) was found between plasma BNP and QT dispersion, which probably occurred due to the concurrent effect of iron deposition in the cardiac myocytes that impairs the conductive function and its secretion of the BNP. However, currently, there is no conducted study for comparing these two parameters.
In conclusion, we realized that most ECG parameters, especially P-wave dispersion, QT prolongation and dispersion and repolarization abnormalities (T-wave inversion in chest leads), Doppler finding of early diastolic dysfunction and impaired relaxation were significantly higher in TDT patients than healthy individuals. Echocardiographic findings of LV wall thickness and increased chamber dimension; LV enlargement was significantly high in thalassemia patients with normal systolic function than normal subjects. Plasma BNP was associated with diastolic dysfunction in TDT patients. These findings suggest the usefulness of ECG, 2D-echocardiographic, Doppler studies and plasma BNP, with no significant beneficial effect of serum ferritin level in detecting early cardiac damage in TDT patients.
Acknowledgments
We acknowledge the staff and healthcare workers at the Department of Cardiology, Dr. Jamal Ahmed Rashid’s Pediatric Teaching Hospital, Sulaimaniyah Thalassemia and Congenital Blood Disorders Center, Department of Physiology, University of Sulaimani, Sulaimaniyah City, Republic of Iraq for their kind efforts and support for this work.
Funding
No funding was received.
Disclosure
None of the authors has a potential conflict of interest for this work to be disclosed.
References
1. Wood JC, Enriquez C, Ghugre N, et al. Physiology and pathophysiology of iron cardiomyopathy in thalassemia. Ann N Y Acad Sci. 2009;1054:386–395. doi:10.1196/annals.1345.047
2. Kremastinos DT, Farmakis D, Aessopos A, et al. β-thalassemia cardiomyopathy: history, present considerations, and future perspectives. Circ Heart Fail. 2010;3(3):451–458. doi:10.1161/CIRCHEARTFAILURE.109.913863
3. Pennell DJ, Udelson JE, Arai AE, et al. Cardiovascular function and treatment in β-thalassemia major: a consensus statement from the American Heart Association. Circulation. 2013;128(3):281–308. doi:10.1161/CIR.0b013e31829b2be6
4. Kontoghiorghe CN, Kontoghiorghes GJ. Efficacy and safety of iron-chelation therapy with deferoxamine, deferiprone, and deferasirox for the treatment of iron-loaded patients with non-transfusion-dependent thalassemia syndromes. Drug Des Devel Ther. 2016;10:465–481. doi:10.2147/DDDT.S79458
5. Kremastinos DT, Farmakis D. Iron overload cardiomyopathy in clinical practice. Circulation. 2011;124(20):2253–2263. doi:10.1161/CIRCULATIONAHA.111.050773
6. Kremastinos DT, Tsiapras DP, Tsetsos GA, Rentoukas EI, Vretou HP, Toutouzas PK. Left ventricular diastolic Doppler characteristics in beta-thalassemia major. Circulation. 1993;88(3):1127–1135. doi:10.1161/01.CIR.88.3.1127
7. Garadah TS, Kassab S, Mahdi N, Abu-Taleb A, Jamsheer A. QTc interval and QT dispersion in patients with thalassemia major: electrocardiographic (EKG) and echocardiographic evaluation. Clin Med Insights Cardiol. 2010;4:31–37. doi:10.4137/cmc.s4472
8. Rose RA, Sellan M, Simpson JA, et al. Iron overload decreases CaV1. 3-dependent L-type Ca2+ currents leading to bradycardia, altered electrical conduction, and atrial fibrillation. Circ Arrhythm Electrophysiol. 2011;4(5):733–742. doi:10.1161/CIRCEP.110.960401
9. Ghanavat M, Haybar H, Pezeshki SMS, et al. Cardiomyopathy in thalassemia: quick review from cellular aspects to diagnosis and current treatments. Lab Med. 2020;51(2):143–150. doi:10.1093/labmed/lmz052
10. Lekawanvijit S, Chattipakorn N. Iron overload thalassemic cardiomyopathy: iron status assessment and mechanisms of mechanical and electrical disturbance due to iron toxicity. Can J Cardiol. 2009;25(4):213–218. doi:10.1016/S0828-282X(09)70064-9
11. Russo V, Melillo E, Papa AA, Rago A, Chamberland C, Nigro G. Arrhythmias and sudden cardiac death in beta-thalassemia major patients: noninvasive diagnostic tools and early markers. Cardiol Res Pract. 2019;2019:1–8. doi:10.1155/2019/9319832
12. McMurray JJV, Adamopoulos S, Anker SD, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33(14):1787–1847. doi:10.1093/eurheartj/ehs104
13. Rubis P. The diagnostic work up of genetic and inflammatory dilated cardiomyopathy. E-J Cardiol Pract. 2015;13(19):1–11.
14. Murphy CJ, Oudit GY. Iron-overload cardiomyopathy: pathophysiology, diagnosis, and treatment. J Card Fail. 2010;16(11):888–900. doi:10.1016/j.cardfail.2010.05.009
15. Ghandi Y, Eghbali A, Rafie F. Correlation between mean serum ferritin levels and atrial electrocardiographic markers in beta-thalassemia major. Iran J Blood Cancer. 2018;10(3):76–81.
16. Wood JC. Cardiac complications in thalassemia major. Hemoglobin. 2009;33(sup1):S81–S86. doi:10.3109/03630260903347526
17. Kirillova VV, Sokolova LA, Meshchaninov VN, Pershanova VI. The level of NT-proBNP in ambulatory patients with chronic heart failure with preserved ejection fraction of the left ventricle. Ter Arkh. 2018;90(9):68–72. doi:10.26442/terarkh201890968-72
18. Fan S, Huang H, Zhang D, et al. The dynamic change of serum cTnT and NT-ProBNP during the intervention therapy for congenital heart disease and the value for prognosis prediction. Int J Clin Exp Med. 2016;9(3):5842–5847.
19. Vlachou M, Kamperidis V, Giannakoulas G, Karamitsos T, Vlachaki E, Karvounis H. Biochemical and imaging markers in patients with thalassaemia. Hellenic J Cardiol. 2021;62(1):4–12. doi:10.1016/j.hjc.2020.04.012
20. Mozos I. Ventricular Arrhythmia Risk in Noncardiac Diseases. In Tech; 2014:89–109.
21. Rago A, Russo V, Papa AA, et al. The role of the atrial electromechanical delay in predicting atrial fibrillation in beta-thalassemia major patients. J Interv Card Electrophysiol. 2017;48(2):147–157. doi:10.1007/s10840-016-0201-y
22. Siri-Angkul N, Xie L, Chattipakorn SC, Chattipakorn N. Cellular electrophysiology of iron-overloaded cardiomyocytes. Front Physiol. 2018;9:1–7. doi:10.3389/fphys.2018.01615
23. Yu CY, Lin CH, Yang YH. Human body surface area database and estimation formula. Burns. 2010;36(5):616–629. doi:10.1016/j.burns.2009.05.013
24. Kautsar A, Advani N, Andriastuti M. N-terminal-pro-b-type natriuretic peptide levels and cardiac hemosiderosis in adolescent β-thalassemia major patients. Ann Pediatr Cardiol. 2019;12(1):32. doi:10.4103/apc.APC_49_18
25. Patsourakos D, Gatzoulis KA, Aggeli C, et al. Twelve‐lead and signal‐averaged electrocardiographic parameters among beta‐thalassemia major patients. J Arrhythm. 2020;36(5):920–928. doi:10.1002/joa3.12412
26. Detterich J, Noetzli L, Dorey F, et al. Electrocardiographic consequences of cardiac iron overload in thalassemia major. Am J Hematol. 2012;87(2):139–144. doi:10.1002/ajh.22205
27. Ramazzotti A, Pepe A, Positano V, et al. Standardized T2* map of a normal human heart to correct T2* segmental artefacts; myocardial iron overload and fibrosis in thalassemia intermedia versus thalassemia major patients and electrocardiogram changes in thalassemia major patients. Hemoglobin. 2008;32(1–2):97–107. doi:10.1080/03630260701879514
28. Ghadiri Anari A, Ghiliyan R, Rezaeian G. P-wave Dispersion in patients with major Thalassemia. Iran J Pediatr Hematol Oncol. 2012;2(2):67–71.
29. Nisli K, Taner Y, Naci O, et al. Electrocardiographic markers for the early detection of cardiac disease in patients with beta-thalassemia major. J Pediatr. 2010;86:159–162. doi:10.2223/JPED.1982
30. Garadah TS, Mahdi N, Kassab S, Shoroqi IA, Abu-Taleb A, Jamsheer A. The pro-BNP serum level and echocardiographic tissue Doppler abnormalities in patients with beta thalassemia major. Clin Med Insights Cardiol. 2010;4:135–141. doi:10.4137/CMC.S6452
31. Kremastinos DT, Tsiapras DP, Kostopoulou AG, Hamodraka ES, Chaidaroglou AS, Kapsali ED. NT‐proBNP levels and diastolic dysfunction in β‐Thalassaemia major patients. Eur J Heart Fail. 2007;9(5):531–536. doi:10.1016/j.ejheart.2006.11.004
32. Deraz SE, Abd El Naby SA, Mahmoud AA. Assessment of ventricular dysfunction in Egyptian children with Beta-thalassemia major. Hematol Oncol Stem Cell Ther. 2021;14(3):206–213. doi:10.1016/j.hemonc.2020.07.003
33. Bosi G, Crepaz R, Gamberini MR, et al. Left ventricular remodelling, and systolic and diastolic function in young adults with β thalassaemia major: a Doppler echocardiographic assessment and correlation with haematological data. Heart. 2003;89(7):762–766. doi:10.1136/heart.89.7.762
34. Huttin O, Kobayashi M, Ferreira JP, et al. Circulating multimarker approach to identify patients with preclinical left ventricular remodelling and/or diastolic dysfunction. ESC Heart Failure. 2021;8(2):1700–1705. doi:10.1002/ehf2.13203
35. Nagueh SF. Left ventricular diastolic function: understanding pathophysiology, diagnosis, and prognosis with echocardiography. JACC Cardiovasc Imaging. 2020;13(1Part 2):228–244. doi:10.1016/j.jcmg.2018.10.038
36. Sahin C, Basaran O, Altun I, et al. Assessment of myocardial performance index and aortic elasticity in patients with beta-thalassemia major. J Clin Med Res. 2015;7(10):795–801. doi:10.14740/jocmr2293w
37. Majd Z, Haghpanah S, Ajami GH, et al. Serum ferritin levels correlation with heart and liver MRI and LIC in patients with transfusion-dependent thalassemia. Iran Red Crescent Med J. 2015;17(4):e24959. doi:10.5812/ircmj.17(4)2015.24959
38. Eghbali A, Taherahmadi H, Shahbazi M, Bagheri B, Ebrahimi L. Association between serum ferritin level, cardiac and hepatic T2-star MRI in patients with major β-thalassemia. Iran J Pediatr Hematol Oncol. 2014;4(1):17–21.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.