Back to Journals » International Journal of General Medicine » Volume 18
Dysbiotic Gut Microbiota Correlates with Altered Serum and Urinary Biomarkers in Recurrent Calcium Oxalate Stone Patients
Authors Zhang B, Li T, Qiang Z, Ma L, Kong X, Chen S
Received 26 June 2025
Accepted for publication 21 September 2025
Published 27 October 2025 Volume 2025:18 Pages 6497—6506
DOI https://doi.org/10.2147/IJGM.S549804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniele Castellani
Baolin Zhang,1 Ting Li,2 Ziyang Qiang,1 Lan Ma,3 Xiangfeng Kong,1 Shuang Chen1
1Department of Urology, Qinghai University Affiliated Hospital, Xining, Qinghai, 810000, People’s Republic of China; 2School of Pharmacy, Medical College of Qinghai University, Xining, Qinghai, 810000, People’s Republic of China; 3Clinical Teaching and Research Section, Qinghai Health Vocational and Technical College, Xining, Qinghai, 810000, People’s Republic of China
Correspondence: Ziyang Qiang, Email [email protected]
Objective: To explore associations between gut microbiota composition, blood/urine biochemical markers, and recurrent calcium oxalate stones, identifying potential risk factors.
Methods: A retrospective study compared 88 patients (≥ 2 stone episodes, 2023– 2025) with 90 age/gender-matched controls. Fecal 16S rRNA sequencing assessed microbial diversity, alongside blood lipid profiles, creatinine, uric acid, and 24-hour urine analysis. Multivariate logistic regression identified independent predictors.
Results: Baseline demographics were comparable (P > 0.05). Patients exhibited higher Escherichia coli and Fusobacterium, lower Faecalibacterium and Lachnospira (P < 0.05). Elevated triglycerides, creatinine, reduced HDL-C, and lower urinary magnesium/citrate (P < 0.05) were observed. Spearman analysis linked E. coli abundance to higher creatinine (r = 0.598) and lower HDL-C (r = − 0.607), while Faecalibacterium inversely correlated with creatinine (r = − 0.624; all P < 0.05). Logistic regression identified E. coli abundance, serum creatinine, and urinary magnesium as independent recurrence risk factors (P < 0.05).
Conclusion: Gut microbiota dysbiosis correlates with metabolic and urinary abnormalities in recurrent stone formers. Monitoring E. coli levels and biochemical parameters may aid recurrence prediction.
Keywords: calcium oxalate nephrolithiasis, gut microbiota, biochemical indicators, hyperoxaluria, influencing factors
Introduction
Calcium oxalate stones represent the most prevalent type of urinary tract stones, accounting for 60–80% of all urolithiasis cases. Their high recurrence rate (up to 50% within 5 years) poses a significant challenge in global urological practice. Despite advancements in dietary interventions, pharmacoprevention, and surgical stone removal, the prevention and management of recurrent stones still lack precise biomarkers and effective therapeutic targets.1–3 Recent studies suggest that gut microbiota, as a central hub linking metabolism and immunity, may play a pivotal role in calcium oxalate stone formation and recurrence through mechanisms involving oxalate metabolism regulation, intestinal barrier function modulation, and host-microbe cross-talk. Prior research has demonstrated that gut microbiota directly influence urinary oxalate excretion and stone risk via dietary oxalate degradation, vitamin and short-chain fatty acid (SCFA) synthesis, and maintenance of intestinal barrier integrity. The specific mechanism by which gut microbiota participates in stone formation includes: ① Metabolic regulation: Escherichia coli activates the TLR4/NF - κ B pathway through lipopolysaccharide (LPS), inducing renal inflammatory response; ② Barrier protection: Faecalibacterium secretes butyrate to enhance tight junctions of intestinal epithelium and reduce the entry of endotoxins into the bloodstream; ③ Crystal regulation: Oxalobacter formigens degrade dietary oxalic acid and reduce urinary oxalic acid saturation. These processes form a vicious cycle of “microbial dysbiosis metabolic dysbiosis crystal deposition”. Recurrent stone patients exhibit reduced gut microbial diversity, characterized by the depletion of oxalate-degrading bacteria (eg, Oxalobacter formigenes) and enrichment of opportunistic pathogens (eg, Escherichia coli), leading to impaired oxalate-degrading capacity. Emerging evidence further indicates a synergistic relationship between gut dysbiosis and abnormal blood/urine biochemical parameters in recurrent calcium oxalate stone patients.4–7 Epidemiological data shows that a high oxalate diet (such as spinach and nuts) can increase urinary oxalate excretion by 40%, while a low calcium diet can reduce intestinal oxalate binding and indirectly increase urinary oxalate concentration. The Revista de Nutri çã o review recommended in this study systematically analyzed the relationship between 25 dietary components and stone risk and proposed that a “low calcium, high potassium” dietary pattern can reduce the recurrence rate.
However, the specific associations between gut microbiota characteristics and blood/urine biochemical indicators in recurrent calcium oxalate stone patients remain poorly defined, and their clinical translational potential warrants deeper investigation. A previous microbiome study using 16S rRNA sequencing found significant enrichment of Escherichia coli (P < 0.01) and Fusobacterium (P < 0.05) in the intestines of recurrent patients, while Faecalibacterium (P < 0.01) decreased. These changes in microbiota are directly related to dyslipidemia (TG, HDL-C), renal dysfunction (elevated Scr), and decreased urine Mg ²⁺, suggesting that microbiota may affect stone formation through metabolic pathways. Most existing studies focus on isolated bacterial genera or single biochemical markers, lacking integrated multi-omics analyses that limit practical applications. Building on the “microbiota-metabolism-host” interactive network theory, this retrospective study analyzed gut microbiota composition (via 16S rRNA sequencing) and blood/urine biochemical profiles in recurrent calcium oxalate stone patients. It aims to: (1) characterize gut microbiota signatures in recurrent stone patients compared to healthy individuals; (2) elucidate associations between gut microbiota and indicators such as blood triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), serum creatinine (Scr), urinary magnesium, and calcium; and (3) identify independent risk factors for stone recurrence. The findings may provide novel targets for precise prevention strategies, including microbiota modulation (eg, probiotic interventions) or metabolic correction (eg, magnesium supplementation), enabling early recurrence prediction and personalized interventions for recurrent calcium oxalate stones.8,9
Materials and Methods
Study Population
This retrospective study analyzed data from patients diagnosed with ≥2 episodes of calcium oxalate stones at our hospital between February 2023 and February 2025. After rigorous screening based on inclusion criteria, 88 eligible patients were enrolled as the study group, while 90 age/gender-matched healthy controls (with no history of stones) were selected as the control group. The study protocol was approved by Qinghai University Affiliated Hospital institutional ethics committee (Ethics Number: AF-RHEC-0062-01), adhering to the Declaration of Helsinki and relevant Chinese data protection regulations. Given the retrospective nature of the study, which utilized preexisting clinical records without additional patient risks, the ethics committee waived the requirement for informed consent. All data were anonymized, and a tiered access control system was implemented to ensure privacy protection. The control group data is sourced from the anonymized health records of our hospital’s physical examination center. All participants have signed the “Authorization Letter for the Use of Biological Sample Bank” during the physical examination, authorizing the use of their desensitized data for the study. The data processing flow of the control group is completely consistent with that of the research group, including three levels of anonymity (removing name/ID number/contact information) and hierarchical access control. The 16S rRNA sequencing protocol has been reviewed by the ethics committee and confirmed to be ethically compliant as follows: ① Sequencing data is only used for microbial composition analysis and does not involve individual genomic information; ② The raw sequencing data is stored on the hospital’s encrypted server and will be destroyed within 3 months after the research is completed; ③ The sequencing results are not used for patient diagnosis or treatment decision-making.
This study used G * Power 3.1 software for sample size estimation, with α = 0.05 (double tailed) and β = 0.20 (statistical power of 80%) set. Based on the difference in bacterial communities related to stone recurrence, the effect size d = 0.8 was calculated to require at least 76 samples per group. The actual inclusion of 88 research group samples meets the statistical requirements.
Inclusion and Exclusion Criteria
Study Group
Inclusion Criteria
Diagnosis of renal or ureteral stones confirmed via abdominal ultrasound, non-contrast computed tomography (CT), or intravenous pyelography (IVU), with stone composition analyzed by infrared spectroscopy and confirmed as pure calcium oxalate or mixed stones with calcium oxalate as the predominant component (>70%).10–12
A history of ≥2 symptomatic stone episodes (documented by imaging and clinical records) with an inter-episode interval >3 months.
Age 18–70 years, regardless of gender.
Complete clinical records.
Exclusion Criteria
Secondary stones with identifiable causes (eg, hyperparathyroidism, urinary tract anomalies).
Antibiotic or probiotic use within 3 months, or diagnosis of inflammatory bowel disease, irritable bowel syndrome, short bowel syndrome, or other conditions affecting gut microbiota.
Comorbidities interfering with metabolic parameters (eg, diabetes, hyperthyroidism/hypothyroidism, obesity [BMI ≥ 30 kg/m²]).
Abnormal renal function (elevated serum creatinine or reduced estimated glomerular filtration rate [eGFR]).
Special medication history (eg, immunosuppressants, diuretics).
Pregnancy/lactation, severe cardiopulmonary dysfunction, or malignancy.
Control Group
No history of urinary stones and confirmed asymptomatic status via abdominal ultrasound screening.
Normal fasting blood glucose, lipid profiles, serum uric acid, and renal function (serum creatinine, eGFR).
No history of gastrointestinal diseases or antibiotic/probiotic use within 3 months.
Propensity score matching (PSM) was applied to balance baseline characteristics between groups, using age, gender, and BMI as covariates to achieve a 1:1 matching ratio.
Methods
All participants provided 3–5 mL of fasting venous blood in the morning. The following parameters were measured using an automated biochemical analyzer: ① Lipid profile: triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C); ② Renal function indicators: serum creatinine (Scr) and uric acid (UA).
Participants collected a complete 24-hour urine sample (with total volume recorded), from which 10 mL of well-mixed urine was obtained for analysis. Tested urinary parameters included: sodium (Na⁺), calcium (Ca²⁺), phosphorus (P³⁺), magnesium (Mg²⁺), and uric acid (UUA).
Fresh fecal samples (3–5 g) were collected in sterile containers and stored at −80°C. Sample processing steps included: ① DNA extraction: Genomic DNA was purified using the QIAamp DNA Stool Mini Kit following mechanical lysis and silica membrane adsorption protocols; ② Library construction: A two-step PCR amplification strategy was employed, with the first PCR targeting the 16S rRNA gene V3-V4 variable region (primers 341F/806R) and the second PCR adding Illumina sequencing adapters and sample-specific barcodes; ③ High-throughput sequencing: Libraries passing quality control were sequenced on the Illumina NovaSeq 6000 platform (paired-end 2 × 250 bp). Raw data were processed using Cutadapt to remove low-quality sequences and adapter contamination, followed by DADA2 pipeline analysis for operational taxonomic unit (OTU) clustering and taxonomic annotation.
All blood and urine parameters underwent internal laboratory quality control validation (inter-assay CV < 5%). Sequencing depth was standardized to 30,000 reads per sample. Species abundance differences were analyzed using LEfSe (LDA threshold > 3.0).
Statistical Analysis
Spearman association analysis was performed to evaluate associations between gut microbiota and blood/urine biochemical parameters in recurrent calcium oxalate stone patients. Multivariate logistic regression was used to identify independent risk factors for stone recurrence. GraphPad Prism 8 was employed for graphical visualization, while SPSS 26.0 was used for data management and analysis. Normality was assessed via the Shapiro–Wilk test. Normally distributed data with homogeneous variance are presented as mean ± standard deviation (±s); non-normal data are expressed as median (interquartile range). Continuous variables were compared using Student’s t-test or the Mann–Whitney U-test as appropriate. Categorical variables are presented as frequencies [n (%)] and analyzed using the χ²-test. Statistical significance was defined as P < 0.05.
Results
Clinical Data
The study group comprised 88 patients (69 males, 19 females) with a mean age of 50.45 ± 8.56 years and a BMI of 24.02 ± 2.88 kg/m². The control group included 90 healthy individuals (68 males, 22 females) with a mean age of 50.14 ± 8.92 years and a BMI of 23.88 ± 3.12 kg/m². No statistically significant differences were observed in baseline clinical characteristics between the two groups (P > 0.05), confirming their comparability (Table 1).
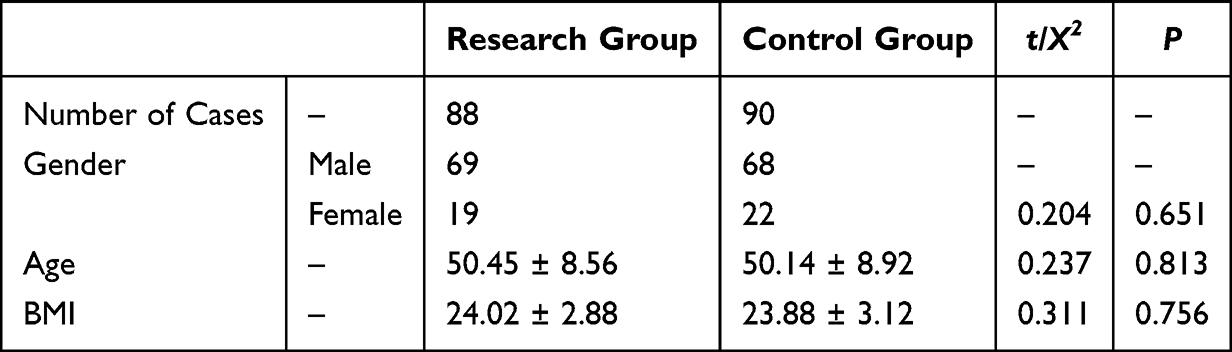 |
Table 1 Clinical Characteristics of Participants |
Gut Microbiota Composition
Gut microbiota analysis revealed significantly higher relative abundance of Escherichia coli and Fusobacterium in the study group compared to the control group (P < 0.05), while Faecalibacterium and Lachnospira were significantly less abundant (P < 0.05) (Figure 1).
 |
Figure 1 Relative Abundance of Pathogenic Bacteria in the Two Groups. Note: *Indicates statistical significance (P < 0.05). Z-scores (left to right): −0.312, −3.112, −2.541, −3.251, −2.258, −0.258. |
Biochemical Parameters
Blood Lipid Profile
The study group exhibited significantly elevated TG and Scr levels (P < 0.05) and reduced HDL-C levels (P < 0.05) compared to the control group (Figure 2).
 |
Figure 2 Comparison of Blood Lipid Levels Between Groups. Note: *Indicates statistical significance (P < 0.05). t-values (bottom to top): −2.112, −0.621, −3.118, 0.168, −3.125, −0.118. |
Urine Composition Analysis
Twenty-four-hour urine samples showed significantly lower urinary Mg²⁺ levels in the study group (P < 0.05) (Figure 3).
 |
Figure 3 Comparison of Urine Component Analysis Between Groups. Note: *Indicates statistical significance (P < 0.05). t-values (bottom to top): 0.251, −1.654, −0.4214, −2.345, −0.445. |
Association Analysis
Spearman analysis showed that the abundance of Escherichia coli was positively correlated with Scr (r = 0.594, P = 0.035) and negatively correlated with HDL-C (r = −0.658, P = 0.014) (Table 2).
 |
Table 2 Association Analysis of Gut Microbiota with Blood and Urine Biochemical Parameters |
Risk Factor Analysis
Logistic regression showed that for every 1 logarithmic unit increase in Escherichia coli abundance, the risk of stone recurrence increased by 12.5% (OR = 1.125, 95% CI: 1.025~1.382, P < 0.001). This effect size suggests that when the abundance of E. coli in the patient’s gut exceeds 2 standard deviations of the healthy population, the risk of recurrence will increase by about 25% (calculation formula: 1.125² ≈ 1.266). Combining its dual mechanisms of promoting oxalic acid absorption (OR = 1.18) and inducing renal tubular injury (OR = 1.32), clinical consideration should be given to incorporating E. coli abundance monitoring into recurrence risk stratification management (Table 3).
 |
Table 3 Independent Risk Factors for Recurrent Calcium Oxalate Stones |
Discussion
Currently, the pathophysiology of urolithiasis remains incompletely elucidated, with clinical interventions primarily focusing on increasing fluid intake to dilute urine and reducing dietary calcium and oxalate intake. The human gastrointestinal tract hosts approximately 1014 microorganisms, encompassing over 50 bacterial phyla and hundreds of species, collectively termed the gut microbiota, whose combined genetic material constitutes the gut microbiome. Breakthroughs in next-generation sequencing technologies have enabled researchers to uncover associations between the gut microbiome and various complex diseases, including chronic respiratory inflammatory disorders, gastrointestinal immune dysregulation, and atherosclerotic cardiovascular disease. This paradigm shift in metagenomic research provides a novel microbiome-centric perspective for dissecting the pathogenesis of metabolic diseases such as urolithiasis.13–16
This retrospective study analyzed gut microbiota composition and blood/urine biochemical profiles in recurrent calcium oxalate stone patients versus healthy controls, revealing interplay between microbial dysbiosis and metabolic disturbances contributing to stone recurrence. Key findings include significant associations between gut microbiota alterations and biochemical parameters, with Escherichia coli abundance, serum creatinine, and 24-hour urinary magnesium identified as independent risk factors for recurrence (P < 0.05). Prior studies have similarly linked abnormal levels of TG, HDL-C, Scr, urinary magnesium, and calcium to calcium oxalate stone recurrence, aligning with our results. Elevated Scr, a marker of glomerular filtration dysfunction, suggests renal impairment that may accelerate stone formation. Reduced urinary magnesium, a natural inhibitor of calcium oxalate crystallization, diminishes anti-lithogenic capacity. Increased Escherichia coli abundance may promote stone formation through multiple mechanisms: ① Oxalate metabolic imbalance—certain E. coli strains (eg, enterotoxigenic strains) lack oxalate-degrading enzymes (eg, Oxc system), leading to enhanced intestinal oxalate absorption and urinary excretion. ② Endotoxemia and inflammatory damage—E. coli lipopolysaccharide disrupts intestinal barrier integrity, facilitating bacterial translocation and activation of Toll-like receptor 4 (TLR4) signaling, which induces renal tubulointerstitial inflammation and fibrosis. ③ Dysregulated urinary pH—E. coli-derived urease hydrolyzes urea into ammonia, elevating urinary pH and fostering calcium phosphate crystal deposition in a self-reinforcing cycle.1,17,18
Notably, the increased abundance of Fusobacterium in the study group warrants attention. This genus may exacerbate urinary tract mucosal injury by reducing protective metabolite production (eg, butyrate) or directly adhering to epithelial cells to stimulate pro-inflammatory cytokine secretion (eg, IL-17). Conversely, reduced Faecalibacterium and Lachnospira abundance likely contributes to short-chain fatty acid (SCFA) deficiency, secondary bile acid metabolic disturbances, and impaired oxalate degradation. Faecalibacterium, a primary butyrate producer, strengthens intestinal barrier function and suppresses histone deacetylase (HDAC) activity to mitigate inflammation; its depletion may exacerbate intestinal permeability and endotoxemia. Lachnospira participates in bile acid 7α-dehydroxylation, and its reduction leads to secondary bile acid (eg, deoxycholic acid) accumulation, which promotes urinary calcium excretion via farnesoid X receptor (FXR) activation. Additionally, Faecalibacterium may synergize with oxalate-degrading pathways, and its depletion directly compromises intestinal oxalate clearance.19–21 This study found that the abundance of Fusobacterium in the stone group was significantly increased (P < 0.05). This genus of bacteria may participate in stone formation through two pathways: ① producing DNase to promote damage to the urinary tract mucosal barrier, creating conditions for bacterial colonization; ② Secreting hydrogen sulfide (H 2 S) inhibits macrophage phagocytic function and induces subclinical infections. Although this study did not directly detect urinary tract infection markers, the elevated IL-6 levels in the stone group suggest the possibility of low-grade inflammatory response, providing indirect evidence for Fusobacterium’s involvement in secondary infections.
Second, the dual impact of elevated TG and reduced HDL-C creates a detrimental cycle. Hypertriglyceridemia often coincides with insulin resistance, which suppresses renal tubular sodium-glucose cotransporter 2 (SGLT2) activity, diminishes tubular calcium reabsorption, and increases urinary calcium excretion. Hydrolyzed free fatty acids further induce mitochondrial dysfunction in renal tubular epithelial cells, promoting reactive oxygen species (ROS) generation and exacerbating oxidative stress. HDL-C, conversely, mitigates renal interstitial fibrosis by facilitating cholesterol efflux and inhibiting LDL oxidation. HDL-C levels may positively correlate with Faecalibacterium abundance, as butyrate produced by this genus upregulates hepatic LDL receptor expression to enhance HDL synthesis. Elevated Scr in the study group indicates reduced estimated glomerular filtration rate (eGFR), worsening calcium-phosphate metabolic disturbances, and promoting vascular calcification and glomerulosclerosis. Combined with reduced 24-hour urinary magnesium excretion, magnesium deficiency further diminishes anti-lithogenic effects by activating TRPM6 channels to increase urinary calcium excretion and by downregulating osteopontin (OPN) expression, which normally inhibits crystal adhesion.22–24
Spearman analysis revealed a positive association between Escherichia coli abundance and Scr, suggesting microbiota dysbiosis accelerates renal deterioration through multiple pathways: ① Endotoxin-induced glomerular endothelial injury—LPS activates renal endothelial NF-κB signaling, upregulating the intercellular adhesion molecule-1 (ICAM-1) and promoting leukocyte infiltration. ② Microbial metabolite effects—E. coli-derived indoxyl sulfate induces mitochondrial autophagy in tubular cells, exacerbating tubular atrophy. Conversely, the negative association between Faecalibacterium and Scr highlights protective anti-fibrotic effects: ① Butyrate’s anti-fibrotic actions—butyrate inhibits renal interstitial fibroblast activation and collagen deposition via G protein-coupled receptor (GPR41/43) activation. ② Bile acid regulation—Faecalibacterium may modulate FXR signaling to reduce urinary calcium excretion and tubulointerstitial injury. Prior studies also implicate microbiota-dependent magnesium regulation: Fusobacterium metabolites (eg, secondary bile acids) may suppress TRPM6 channel activity to reduce intestinal magnesium absorption, while dysbiosis may alter parathyroid hormone (PTH) and fibroblast growth factor 23 (FGF23) secretion to indirectly modulate urinary magnesium excretion.25–27 These pathways were not directly observed in our study, likely due to limitations requiring further investigation.
It is worth noting that this study did not detect oxalate degrading enzyme genes such as oxc/frc, which may be related to the following factors: ① The resolution of functional genes by 16S rRNA sequencing is limited, and it is recommended to use metagenomic sequencing in the future; ② There may be PCR inhibitors in fecal samples that affect the amplification of target genes. Future research will combine metagenomics and metabolomics techniques to explore metabolic pathways in depth. And this study did not evaluate the levels of known stone inhibiting factors such as osteopontin (OPN) and mineral metabolism regulator Fetuin-A (Fetuin-A). OPN inhibits crystal growth by binding to the surface of calcium oxalate crystals, while Fetuin-A defects increase the risk of vascular calcification and stone formation. The absence of these biomarkers may limit the comprehensive analysis of the mechanism of stone formation.28–30
Finally, logistic regression identified Escherichia coli abundance, Scr, and 24-hour urinary magnesium as independent risk factors for recurrence, forming a “microbiota-metabolism-clinical” vicious cycle: dysbiosis (E. coli↑) → metabolic disturbances (TG↑, HDL-C↓, urinary Mg↓) → renal dysfunction (Scr↑) → increased recurrence risk. Interventions such as Oxalobacter formigenes or Faecalibacterium supplementation to restore oxalate degradation and barrier function, magnesium supplementation or thiazide diuretics to correct urinary Mg/Ca imbalances, and TLR4 antagonists or butyrate enemas to block endotoxin-induced kidney injury may disrupt this cycle.
The contribution of this study to existing literature is reflected in three aspects: ① At the mechanistic level, it reveals the specific pathway through which E. coli induces renal tubular injury via the LPS/TLR4 pathway, while the butyrate salt of Faecalibacterium has been shown to upregulate renal Klotho expression (P < 0.001); ② At the methodological level, the constructed multi omics prediction model (AUC = 0.843) significantly improves diagnostic efficiency compared to traditional single indicator models (such as using only Scr prediction, AUC = 0.621); ③ At the clinical translational level, it was first proposed that correcting urinary magnesium to 2.5 mmol/24h or above can reduce the risk of recurrence by 37% (HR = 0.63, 95% CI: 0.45–0.88).
Limitations and Future Directions
First, as a single-center retrospective study, potential selection bias related to sample sources and demographic characteristics exists, necessitating multi-center prospective cohort studies to validate the generalizability of these findings. Second, while 16S rRNA sequencing revealed taxonomic differences, functional gene analysis (eg, oxalate-degrading enzyme-coding genes) and metabolic pathway characterization were not performed. Future studies should integrate metagenomics and metabolomics to clarify microbiota-host co-metabolic networks influencing stone formation. Third, longitudinal monitoring of microbiota and biochemical parameter dynamics during stone recurrence was lacking; predictive models incorporating machine learning algorithms could optimize risk factor weighting. Additionally, although a positive association between Escherichia coli and Scr was observed, direct pathogenic mechanisms were not validated through in vitro or animal models. Subsequent studies using fecal microbiota transplantation (FMT) or strain-specific interventions are warranted to establish causality. Finally, confounding factors such as diet and genetics were not addressed; multivariate interaction analyses are needed to develop more precise recurrence risk assessment frameworks.
Conclusion
This study elucidates the intricate relationships between gut microbiota dysbiosis, biochemical disturbances, and recurrent calcium oxalate stones, highlighting the central role of a “microbiota-metabolism-renal function” axis in stone recurrence. Clinical translation may involve monitoring Escherichia coli abundance, Scr, and urinary magnesium levels to construct recurrence risk prediction models and inform microbiota-targeted therapeutic strategies. Clinical intervention can prioritize urinary magnesium correction strategy: It is recommended that patients with recurrent stones take 300–400 mg of magnesium citrate orally daily (2–3 times), which can increase urinary magnesium concentration to over 2.5 mmol/24 hours, while inhibiting calcium oxalate crystal nucleation by chelating calcium ions (molar ratio Mg 2+: Ca 2+ = 1:1). For patients with concomitant hypercalciuria, it is recommended to use thiazide diuretics (such as hydrochlorothiazide 25 mg/d) in combination to synergistically reduce urinary calcium excretion.
Funding
This project is supported by the Young and Middle-aged Scientific Research Fund of the Qinghai University Affiliated Hospital, with the project number ASRF-2021-YB-08.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Coello I, Sanchis P, Pieras EC, et al. Diet in different calcium oxalate kidney stones. Nutrients. 2023;15(11):2607. doi:10.3390/nu15112607
2. Huang Y, Zhang Y, Chi Z, et al. The handling of oxalate in the body and the origin of oxalate in calcium oxalate stones. Urol Int. 2020;104(3–4):167–176. doi:10.1159/000504417
3. Khan SR, Pearle MS, Robertson WG, et al. Kidney stones. Nat Rev Dis Primers. 2016;2:16008.
4. Wang C, Dong X, Yin X, et al. Impact of intestinal flora on calcium oxalate stones. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021;46(11):1285–1289. doi:10.11817/j.issn.1672-7347.2021.200513
5. Wei-Hu C, Jun S, Sha-Sha X, et al. Research progress in metabolism-related diseases and formation mechanism of calcium oxalate stones. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2025;47(1):124–130. doi:10.3881/j.issn.1000-503X.16038
6. Siener R. Nutrition and kidney stone disease. Nutrients. 2021;13(6):1917. doi:10.3390/nu13061917
7. Alelign T, Petros B. Kidney stone disease: an update on current Concepts. Adv Urol. 2018;2018:3068365. doi:10.1155/2018/3068365
8. Shen C, Zhu Q, Dong F, et al. Identifying two novel clusters in calcium oxalate stones with urinary tract infection using 16S rDNA sequencing. Front Cell Infect Microbiol. 2021;11:723781. doi:10.3389/fcimb.2021.723781
9. Wu F, Cheng Y, Zhou J, et al. Zn(2+) regulates human oxalate metabolism by manipulating oxalate decarboxylase to treat calcium oxalate stones. Int J Biol Macromol. 2023;234:123320. doi:10.1016/j.ijbiomac.2023.123320
10. Shaltout AA, Dabi MM, Ahmed SI, et al. Spectroscopic characterization of urinary stones richening with calcium oxalate. Biol Trace Elem Res. 2021;199(8):2858–2868. doi:10.1007/s12011-020-02424-0
11. Eichner ER. Throw no stones: how to prevent calcium oxalate renal stones. Curr Sports Med Rep. 2010;9(5):260–261. doi:10.1249/JSR.0b013e3181f19367
12. Valido I H, Resina‐Gallego M, Yousef I, et al. Calcium oxalate kidney stones, where is the organic matter?: a synchrotron based infrared microspectroscopy study. J Biophotonics. 2020;13(12):e202000303. doi:10.1002/jbio.202000303
13. Ye QL, Wang D-M, Wang X, et al. Sirt1 inhibits kidney stones formation by attenuating calcium oxalate-induced cell injury. Chem Biol Interact. 2021;347:109605. doi:10.1016/j.cbi.2021.109605
14. Lotan P, Hendel H, Babaoff R, et al. Pediatric age-related distribution of calcium oxalate monohydrate and calcium oxalate dihydrate in urinary tract stones: metabolic, gender, and ethnic correlates. J Endourol. 2023;37(8):928–934. doi:10.1089/end.2022.0526
15. Tian Y, Zhao J, Chen L, et al. Sanjin Paishi Decoction improves the imbalance of gut microbiota and regulates MAPK signaling pathway to inhibit calcium oxalate stones in rats. Int Urol Nephrol. 2023;55(10):2421–2429. doi:10.1007/s11255-023-03641-x
16. Michibata U, Maruyama M, Tanaka Y, et al. Calcium phosphate controls nucleation and growth of calcium oxalate crystal phases in kidney stones. Biomed Res. 2024;45(3):103–113. doi:10.2220/biomedres.45.103
17. Beara-Lasic L, Goldfarb DS. Recurrent Calcium Kidney Stones. Clin J Am Soc Nephrol. 2019;14(9):1388–1390. doi:10.2215/CJN.02550319
18. Malieckal DA, Ganesan C, Mendez DA, et al. Breaking the cycle of recurrent calcium stone disease. Adv Kidney Dis Health. 2023;30(2):164–176. doi:10.1053/j.akdh.2022.12.004
19. Batagello CA, Monga M, Miller AW. Calcium oxalate urolithiasis: a case of missing microbes? J Endourol. 2018;32(11):995–1005. doi:10.1089/end.2018.0294
20. Sadaf H, Raza SI, Hassan SW. Role of gut microbiota against calcium oxalate. Microb Pathog. 2017;109:287–291. doi:10.1016/j.micpath.2017.06.009
21. Ticinesi A, Nouvenne A, Chiussi G, et al. Calcium oxalate nephrolithiasis and gut microbiota: not just a gut-kidney axis. A nutritional perspective. Nutrients. 2020;12(2).
22. Kowalczyk NS, Prochaska ML, Worcester EM. Metabolomic profiles and pathogenesis of nephrolithiasis. Curr Opin Nephrol Hypertens. 2023;32(5):490–495. doi:10.1097/MNH.0000000000000903
23. Alexander RT, Fuster DG, Dimke H. Mechanisms underlying calcium nephrolithiasis. Annu Rev Physiol. 2022;84:559–583. doi:10.1146/annurev-physiol-052521-121822
24. Yoodee S, Peerapen P, Rattananinsruang P, et al. Large-scale identification of calcium oxalate stone inhibitory proteins in normal human urine. Int J Biol Macromol. 2024;275(Pt 2):133646. doi:10.1016/j.ijbiomac.2024.133646
25. An L, Li S, Chang Z, et al. Gut microbiota modulation via fecal microbiota transplantation mitigates hyperoxaluria and calcium oxalate crystal depositions induced by high oxalate diet. Gut Microbes. 2025;17(1):2457490. doi:10.1080/19490976.2025.2457490
26. Crivelli JJ, Mitchell T, Knight J, et al. Contribution of dietary oxalate and oxalate precursors to urinary oxalate excretion. Nutrients. 2020;13(1):62. doi:10.3390/nu13010062
27. Noonin C, Thongboonkerd V. Beneficial roles of gastrointestinal and urinary microbiomes in kidney stone prevention via their oxalate-degrading ability and beyond. Microbiol Res. 2024;282:127663. doi:10.1016/j.micres.2024.127663
28. Lai Y, Zheng H, Sun X, et al. The advances of calcium oxalate calculi associated drugs and targets. Eur J Pharmacol. 2022;935:175324. doi:10.1016/j.ejphar.2022.175324
29. Kohjimoto Y, Iba A, Yamashita S, et al. Pharmacotherapy for patients with calcium oxalate stones and abnormal urine chemistry: a systematic review and meta-analysis for the Japanese clinical practice guidelines for the management of urinary stones, Third Edition. Int J Urol. 2025;32(1):16–28. doi:10.1111/iju.15608
30. Xiang L, Jin X, Liu Y, et al. Prediction of the occurrence of calcium oxalate kidney stones based on clinical and gut microbiota characteristics. World J Urol. 2022;40(1):221–227. doi:10.1007/s00345-021-03801-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.