Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Dynamic Observation of Atypical Sporotrichosis Before and After Itraconazole Treatment by Dermoscopy
Authors Tang Q, Zhou Y, Chen Y ![]() , Chen J, Xiong X
, Chen J, Xiong X
Received 6 December 2022
Accepted for publication 26 January 2023
Published 3 February 2023 Volume 2023:16 Pages 339—343
DOI https://doi.org/10.2147/CCID.S400302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Qinqin Tang, Yanjun Zhou, Yujuan Chen, Jie Chen, Xincai Xiong
Department of Dermatology, Affiliated Hospital of North Sichuan Medical College, Nanchong, People’s Republic of China
Correspondence: Xincai Xiong, Department of Dermatology, Affiliated Hospital of North Sichuan Medical College, No. 1 Maoyuan South Road, Shunqing District, Nanchong City, Sichuan Province, 637000, People’s Republic of China, Tel +86 13551686620, Email [email protected]
Abstract: Sporotrichosis is a deep fungus infection caused by the Sporothrix. In China, the most common species is Sporothrix globosa which is difficult to treat with most antifungal drugs. Atypical clinical forms of sporotrichosis can be a hinder to clinicians for an early diagnosis and treatment. We report a case of fixed cutaneous sporotrichosis of the face caused by S. globosa in a healthy adult that was initially misdiagnosed as rosacea due to its unusual clinical features. We made an effort to dermoscopically track changes in skin lesions both before and after treatment, confirming that itraconazole was effective in the treatment of sporotrichosis.
Keywords: skin disease, dermatology, sporotrichosis, fixed cutaneous sporotrichosis, dermoscopy, Sporothrix globosa, fungus infection
Introduction
Sporotrichosis usually appears as a cutaneous mycotic infection illness after organism injection through a puncture or small skin trauma site contaminated with vegetation or another environmental source.1 It was reported by Schenck in 1898,2 and sporotrichosis is hyperendemic in Latin American nations, followed by South Africa, Japan, and other countries.3–5 Previously, S. schenckii was assumed to be the only pathogen causing sporotrichosis.6 Six new genotypes have been found as a result of breakthroughs in genotyping technology. Sporotrichosis is classified into four forms, with fixed cutaneous sporotrichosis being the least prevalent. It typically manifests as a localized erythematous, papulo-plaque, or nodule at the site of inoculation.7 Clinical suspicion is essential for early diagnosis; nevertheless, some diseases with distinctive clinical features are more prone to be misinterpreted as other diseases. We herein present a case of atypical fixed sporotrichosis initially misdiagnosed as Rosaceae. The dermoscopic observations prompted us to suspect fungal infection, and the efficacy of itraconazole in the treatment of sporotrichosis was verified in our investigation by dynamic dermoscopy monitoring of changes before and after therapy.
Case Presentation
A 46-year-old female was admitted to our hospital in March 2021 with a nonhealing lesion on the right side of her face that appeared one year and six months prior. Sixteen months prior, the patient developed erythema and papules at the tip of the nose for no apparent reason, and the skin lesions gradually expanded into infiltrating red patches. A large number of papules and pustules were scattered and distributed on top of the infiltrating erythema. Some papules had an umbilical concave shape. The lesions gradually spread to the right nasal root, alar, and right cheek. There were red patches overlaid with numerous papules and pustules, some of which had crusted. In another hospital, she was diagnosed with “rosacea” and treated with topical tacrolimus, mucopolysaccharide polysulfate cream, and fusidic acid and internal administration of hydroxychloroquine tablets and ebastine tablets, but no improvement was observed, after which she came to our clinic. Her past medical history was unremarkable.
Physical examination revealed multiple papules and pustules of different sizes on the infiltrating erythema on the right cheek and nose. Some papules were umbilical concave, with local necrosis and crusting, and the skin lesions were well-defined (Figure 1A). There were no signs of organomegaly, visible lymph nodes, unusual auscultatory sounds, or indications of brain dysfunction. Unpolarized contact dermoscopy at x20 magnification revealed generalized dark erythema, yellowish, structureless areas (Figure 1B, dark arrow), and clustered pustules (Figure 1C, blue arrow), which resembled fried eggs on a dark red background. Vellus hair loss was noted in some lesions (Figure 1C, dark circle).
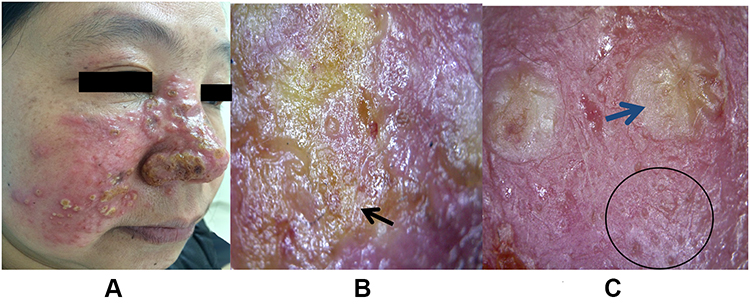 |
Figure 1 Prior treatment: picture taken at the clinic shows nonhealing, infiltrating erythema, umbilical concave papules and pustules on the right side of the face and nose (A); dermoscopy revealed generalized erythema, a yellowish, structureless area ((B), dark arrow), clustered pustules ((C), blue arrow), which resemble fried eggs on a dark red background, and vellus hair loss ((C), dark circle). |
Routine biochemical and hematological testing revealed nothing remarkable. Both the HIV ELISA test and the syphilis serology test came out negative. Bacteria were not discovered in a culture of the lesion’s secretions. Histopathology revealed lymphocyte, histocytes, and neutrophil infiltration (hematoxylin and eosin, original magnification x200), and periodic acid-Schiff (PAS) staining confirmed the presence of spherical, aubergine, and double-countered yeast cells (PAS stain, original magnification x400).
Fungal cultures were obtained by surgically removing skin lesions. Moist membranous fawn-colored colonies could be seen around the sample fifteen days after incubation at room temperature on Sabouraud’s dextrose agar (SDA) slants supplemented with cycloheximide (500 mg/l) and chloramphenicol (50 mg/l). The DNA of the isolated strain was extracted using the method outlined by Makimura.8 For amplification, we utilized the universal fungal primers ITS 1 (5′-TCCGTAGGTGAACCTGCGG) and ITS4 (5′-TCCTCCGCTTATTGA TATGC) (Chengdu Feiteng Bochuan Biotechnology Co. Ltd, China). Each 20 L reaction mixture included 10 L of PCR pfu Mix (dATP, dCTP, dGTP, dTTP, and pfu DNA Taq polymerase; Chengdu Feiteng Bochuan Biotechnology Co., Ltd., China), 1 L of each primer, 2 L of DNA sample, and 6 L of ddH2O. The PCR mixture was denatured at 94°C for 90 seconds, followed by 30 cycles of denaturation at 94°C for 30 seconds, annealing at 55°C for 30 seconds, extension at 72°C for 1 minute, and final extension at 72°C for 5 minutes. Agarose gel electrophoresis (1.5%) followed by UV irradiation identified the amplification products as a single band. Next, the gel was transferred to Dufeiteng Bochuan Biotechnology Co., Ltd. for DNA purification and bidirectional sequencing. The sequences were aligned using BIOEDIT (http://www.mbio.ncsu.edu/) and submitted to GenBank as accession No. GR3V2CT7013. Furthermore, we discovered that the DNA sequences of the isolated fungi’s nuclear ribosomal ITS region had 100% homology with S. globosa ON092639.1 (GenBank accession No. ON092639.1).
We established that the etiologic agent was S. globosa based on molecular methods. The patient was diagnosed with fixed cutaneous sporotrichosis and started oral itraconazole (200 mg/day) therapy in March 2021.
The red swellings and papules started gradually subsiding, and the pustules disappeared (Figure 2A) after two weeks of treatment. Dermoscopy showed yellow dots (Figure 2B, black arrow) on a bright red background, “fried eggs” had disappeared, but vellus hair loss was still noted in some lesions (Figure 2C, dark circle). Three months later, the infiltrating erythema and papules had mostly subsided, and after six months, the lesions had significantly resolved (Figure 3A). Dermoscopy revealed linear and dendritic vessels (Figure 3B, dark arrow) on a pink background, yellow dots had disappeared, and the vellus hair had returned (Figure 3C). The patient was cured clinically and mycologically 6 months after initiation of treatment without adverse drug-related events.
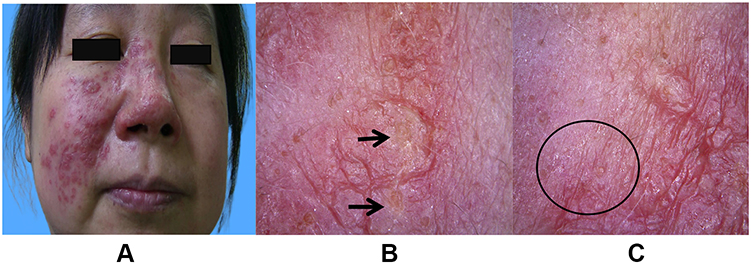 |
Figure 2 Two weeks of treatment: the red swellings and papules started gradually subsiding, and the pustules had disappeared (A); dermoscopy showed yellowish, structureless areas turned into yellow dots ((B), black arrow) on a bright red background, and “fried eggs” had disappeared; vellus hair loss persisted in some lesions ((C), black circle). |
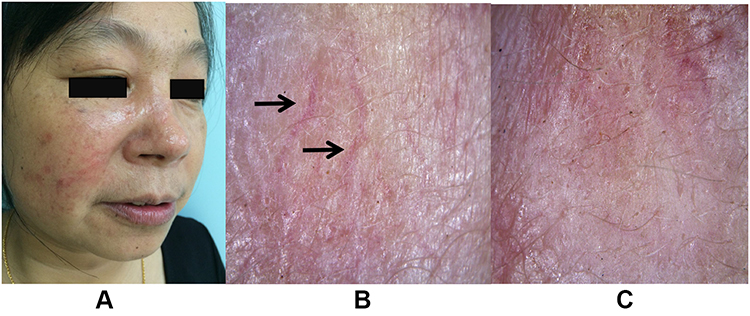 |
Figure 3 Six months of treatment: the lesions had significantly resolved (A); dermoscopy revealed linear and dendritic vessels ((B), dark arrow) on a pink background, and yellow dots have disappeared; vellus hair had returned (C). |
Discussion
Fixed cutaneous sporotrichosis less frequently presents as a cutaneous form (approximately 25%) than as a lymphocutaneous form; overall, it occurs more frequently in infants than in adults.9 The lesion at the inoculation site can be numerous, and the aberrant appearance may be mistaken for other illnesses such as prurigo nodularin,7 bacterial cellulitis,10 and TB verrucous cutis.11 In our case, the atypical and complex clinical picture leads to misdiagnosis as rosacea. Long-term treatment failure and dermoscopy examination led us to the suspicion of fungus infection. The diagnosis was finally confirmed by pathological examination and fungal culture.
Dermoscopy is a noninvasive diagnostic technique that allows the in vivo examination of skin micro-structures that are not visible to the naked eye, from the epidermis to the superficial dermis.12 Generalized erythema, yellowish structureless patches, arborizing telangiectasias, and white scar-like areas appear to be typical dermoscopic hallmarks of neutrophilic-rich granulomatous inflammation, including leishmaniasis and deep mycosis.13 In our study, dermoscopy reveals generalized erythema, clustered pustules, a yellowish structureless area, and vellus hair loss. The granulomatous components of the disease are represented by generalized erythema and yellowish structureless areas, whereas clustered pustules, which resembled a fried egg on a dark red background, indicate neutrophilic microabscesses.13 Vellus hair loss can be noted in many cases of fungal infection.
Itraconazole is indicated in a healthy or immunocompromised patient with limited cutaneous involvement and is considered the drug of choice given its efficacy, relative safety profile and oral route of administration and the treatment duration is between 3 and 6 months, given the possibility of recurrence.3 After 2 weeks of oral itraconazole therapy, clinical pictures showed early efficacy and dermoscopy showed the yellow nonstructural areas turned into yellow dots and clustered pustules had disappeared which corresponds to the pustules disappearing. Dermoscopy after 6 months of therapy revealed that vellus hair had returned, indicating that fungus had been eliminated from the hair follicles; linear and dendritic vessels could be observed on a pink background, indicating new skin; and the yellow spots had vanished. During treatment, the red background gradually fades from deep red to light red to normal pink. Our investigation proved itraconazole’s effectiveness in the treatment of sporotrichosis on a micro-scale.
Despite the presence of publications on the dermoscopic symptoms of fungal infection, no data on the changes in each dermoscopic feature before and after medication are available. By dynamically studying the dermoscopic characteristics of sporotrichosis, we discovered that the yellow unstructured area is related to the yellow dot sign and hair growth tends to occur later in the treatment, in addition to verifying and supplementing the dermoscopic features of the deep fungus.
In conclusion, we reported a case of fixed cutaneous sporotrichosis mimicking rosacea, and dermoscopic features of deep cutaneous mycosis, including generalized erythema, clustered pustules, a yellowish structureless area, and vellus hair loss, were confirmed. At the same time, the changes in each of the above features before and after treatment were dynamically observed, from dark red background to pink background, from yellow nonstructural areas to yellow dots until they disappeared, from hair loss to hair growth, and hair growth was only seen in the final stage of recovery. Dermoscopy can help doctors not only diagnose deep cutaneous mycosis early on, but it can also help doctors evaluate the efficacy of antifungal drugs by dynamically observing each dermoscopic feature.
Ethics
The need for ethics committee approval was waived, as this is a case report.
Consent for Publication
The images and patient data have been published with the consent of the patient.
Acknowledgments
The authors are grateful to the patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This article has no funding support.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Kauffman CA, Bustamante B, Chapman SW, et al. Clinical practice guidelines for the management of sporotrichosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis. 2007;45(10):1255–1265. doi:10.1086/522765
2. Schenck BR. On refractory subcutaneous abscesses caused by a fungus possibly related to the sporotricha. Bull Johns Hopkins Hosp. 1898;9:286–290.
3. Orofino-Costa R, De Macedo PM, Rodrigues AM, et al. Sporotrichosis: an update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics. An Bras Dermatol. 2017;92:606–618. doi:10.1590/abd1806-4841.2017279
4. Rabello VBS, Almeida MA, Bernardes-Engemann AR, et al. The historical burden of sporotrichosis in Brazil: a systematic review of cases reported from 1907 to 2020. Braz J Microbiol. 2021;53:231–244. doi:10.1007/s42770-021-00658-1
5. Toriello C, Brunner-Mendoza C, Ruiz-Baca E, et al. Sporotrichosis in Mexico. Braz J Microbiol. 2021;52(1):49–62. doi:10.1007/s42770-020-00387-x
6. Yao L, Song Y, Cui Y, et al. Pediatric sporotrichosis in Jilin Province of China (2010–2016): a retrospective study of 704 cases. J Pediatric Infect Dis Soc. 2020;9(3):342–348. doi:10.1093/jpids/piz052
7. Mahajan VK, Sharma NL, Shanker V, et al. Cutaneous sporotrichosis: unusual clinical presentations. Indian J Dermatol Venereol Leprol. 2010;76(3):276–280. doi:10.4103/0378-6323.62974
8. Makimura K, Murayama SY, Yamaguchi H. Detection of a wide range 4 of medically important fungi by the polymerase chain reaction. J Med Microbiol. 1994;40:358–364. doi:10.1099/00222615-40-5-358
9. Queiroz-Telles F, Fahal AH, Falci DR, et al. Neglected endemic mycoses. Lancet Infect Dis. 2017;17(11):e367–e377. doi:10.1016/S1473-3099(17)30306-7
10. Ochoa-Reyes J, Ramos-Martínez E, Treviño-Rangel R, González GM, Bonifaz A. Auricular sporotrichosis. Atypical case report simulating bacterial cellulitis. Revista Chilena de Infectología. 2018;35(1):83–87. doi:10.4067/s0716-10182018000100083
11. Martínez-Herrera E, Arenas R, Hernández-Castro R, et al. Uncommon clinical presentations of sporotrichosis: a two-case report. Pathogens. 2021;10(10):1249. doi:10.3390/pathogens10101249
12. Chen X, Lu Q, Chen C, et al. Recent developments in dermoscopy for dermatology. J Cosmet Dermatol. 2021;20(6):1611–1617. doi:10.1111/jocd.13846
13. Dabas G, Kaur H, Vinay K, et al. Dermoscopy in disseminated sporotrichosis. J Eur Acad Dermatol Venereol. 2019;33(1):e33–e35. doi:10.1111/jdv.15152
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Are Systemic Drug Choices for Psoriasis by Dermatologists Compatible with Psoriatic Arthritis? Data from the German National Psoriasis Registry PsoBest
Sorbe C, Kargin S, von Kiedrowski R, Thaci D, Weyergraf A, Blome C, Augustin M, Stephan B
Psoriasis: Targets and Therapy 2025, 15:197-207
Published Date: 30 May 2025
The Prevalence, Knowledge, and Awareness Level of Atopic Dermatitis Among a Sample of Adult Jordanian Population
Saleh MM, Al-Qerem W, Karaki LA, Al-Zayadneh A, Al-Awawdeh A
Clinical, Cosmetic and Investigational Dermatology 2026, 19:624003
Published Date: 10 July 2026