Back to Journals » Journal of Inflammation Research » Volume 16
Dynamic Change of Novel Systemic Inflammation Markers to Predict Maternal-Neonatal Prognosis After Cervical Cerclage
Authors Lin Y, Fang J, Ni R, Zhang L, Zhao J, Jiang X, Lin Y, Pan M ![]()
Received 14 March 2023
Accepted for publication 19 April 2023
Published 21 April 2023 Volume 2023:16 Pages 1745—1756
DOI https://doi.org/10.2147/JIR.S410211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yan Lin,1,* Jiaoning Fang,1,* Ruilan Ni,1,* Li Zhang,1 Jie Zhao,1 Xiumin Jiang,2 Yuping Lin,2 Mian Pan1
1Department of Obstetrics, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, People’s Republic of China; 2Department of Nurse, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mian Pan, Department of Obstetrics, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, 18 Daoshan Road, Fuzhou, Fujian, 350001, People’s Republic of China, Tel +86-13178031273 ; +86-591-86329321, Email [email protected] Xiumin Jiang, Department of Nurse, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, 18 Daoshan Road, Fuzhou, Fujian, 350001, People’s Republic of China, Email [email protected]
Objective: Cervical cerclage is an effective method to prevent preterm birth. However, the clinical indicators that can predict cervical cerclage remain limited. This study aimed to explore whether dynamically inflammatory markers are valuable biomarkers for the prognosis of cervical cerclage.
Methods: This study included 328 participants. Inflammatory markers were calculated using maternal peripheral blood before and after the cervical cerclage procedure. The Chi-square test, linear regression, and logistic regression were performed to evaluate the dynamic change of inflammatory markers with the prognosis of cervical cerclage. And the optimal cut-off values of inflammatory markers were calculated.
Results: Totally 328 pregnant women were analyzed in the study. 223 (67.99%) participants obtained successful cervical cerclage. This study revealed that the maternal age, the baseline BMI (cm2/kg), the times of gravida, the rate of recurrent abortion, the PPROM, cervical length shorter (< 1.5cm), cervical dilation (≥ 2cm), the bulging membrane, the Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, and the ΔSII were significantly associated with outcomes after cervical cerclage (all P< 0.05). Pre-SII, Pre-SIRI, Post-SII, Post-SIRI, and ΔSII levels were mainly related to maternal-neonatal outcomes. Furthermore, the results demonstrated that the ΔSII level had the highest OR (OR=14.560; 95% CI (4.461– 47.518)). In addition, we revealed that Post-SII and ΔSII levels had the highest AUC (0.845/0.840) and relatively higher sensitivity/specificity (68.57/92.83% and 71.43/90.58%) and PPV/ NPV (81.82/86.25% and 78.13/87.07%) compared with other indicators.
Conclusion: This study suggested that the dynamic change of SII level and SIRI level are important biochemical markers to predict the prognosis of cervical cerclage and maternal-neonatal prognosis, especially the Post-SII and ΔSII levels. They can help to determine candidates for cervical cerclage before surgical procedure and enhance postoperative surveillance.
Keywords: cervical cerclage, maternal-neonatal, outcome, inflammatory markers, peripheral blood
Introduction
Globally, it is reported that the preterm birth rate is nearly 11%.1 Preterm birth significantly increases neonatal mortality and morbidity. Approximately 1 million infants died from preterm birth,1 severely threatening families and public health. Cervical insufficiency (CI), with an incidence of 0.1–2%, is the main factor causing fetal late pregnancy abortion and premature birth, generally occurring at 18–24 weeks.2 The clinical manifestation of cervical insufficiency is painless progressive cervical shortening and dilation in the middle and late pregnancy. It accounts for 15% of recurrent abortions at 16–28 weeks and is essential to neonatal mortality.3 The most common surgical treatment for cervical insufficiency is cervical cerclage. It is reported that cervical cerclage effectively prolongs the number of weeks gestation in patients with cervical insufficiency.4 With the increase of gestational age, the pressure of the intrauterine fetus and its appendages on the cervical cervix gradually increases. Cervical cerclage strengthens the cervix through sutures and provides mechanical support to prevent the extension of the lower uterine segment in the middle of pregnancy and reduce the rate of preterm birth.5,6 This surgical method becomes more mature. Unfortunately, abortion and premature birth still occur after cervical cerclage, and the mechanism remains unknown.
Generally, cervical cerclage is the only hope for prolonging pregnancy in patients with cervical insufficiency, with a fetal salvage rate reaching 46–100%.7,8 However, despite the clinical significance of this method, information on the biomarkers to predict pregnancy outcomes after cervical cerclage, especially using suitable and non-invasive procedures, remains limited. Several studies have revealed that increased levels of pro-inflammatory cytokines and chemokines in amniotic fluid are associated with poor prognosis after cervical cerclage.9,10 Similarly, numerous studies have revealed that the levels of interleukin (IL)-1, IL-6, and IL-8 in the amniotic fluid can be used to evaluate the outcomes of cervical cerclage.11–13 However, the clinical utility of these predictors remains limited in prognostic assessment and treatment guidance because their diagnostic sensitivity, specificity, and cut-off values have not been evaluated. Moreover, these test indicators require clinically invasive manipulation that significantly limits their application. Therefore, it is urgent to find novel and reliable noninvasive indicators to predict the pregnancy outcomes of cervical cerclage.
Our research group has long been dedicated to studying noninvasive predictors of the outcome of cervical cerclage. Our previous study14 demonstrated that a higher grade of vaginal cleanliness, a higher pH, a lower abundance of Lactobacillus spp., a higher sialidase positive percentage, a higher positive percentage of clue cells, a higher lactobacillus grade, a higher Nugent score and a higher rate of microecological dysbiosis are potential risk factors that predict subsequent cerclage failure. Importantly, recent studies have revealed the systemic immune-inflammation index (SII) and systemic inflammation response index (SIRI) are novel and comprehensive inflammatory biomarkers to suitably reflect the local immune status and the systemic immune response throughout the human body with noninvasive methods.15–17 Furthermore, current studies have revealed that SII and SIRI can be better biomarkers to reflect the chronic inflammatory state than other inflammatory indicators.18,19 Based on the above conclusions, our previous study found that the baseline SII and SIRI levels are important biochemical markers for predicting the outcome of cervical cerclage and maternal-neonatal results.20 However, the body’s inflammatory response is a complex and changeable process. Therefore, a single test can only reflect the body’s inflammatory response at a point in time.
In this study, we dynamically compare the relationship between inflammatory markers in the peripheral blood of pregnant women before and after cervical cerclage and prognosis. We aimed to explore whether dynamically inflammatory markers in maternal blood are valuable biomarkers that can more accurately and objectively predict clinical outcomes after cervical cerclage.
Materials and Methods
Participants
This study included 328 pregnant women with cervical cerclage from Fujian Provincial Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University (FMCH) from March 1, 2018, to November 31, 2022. Women needing to have cervical cerclage should meet some indications, which have been detailed and described in our previous study.14 Participants were recruited to the study according to the following criteria: (1) received cervical cerclage; (2) single pregnancies; (3) patients with complete clinical data; (4) patients with complete laboratory data before and after cervical cerclage. Detailed data about the clinical characteristic of participants and maternal-neonatal outcomes were collected from computerized obstetric records, neonatal databases, and handwritten records. This study was approved by the Hospital Ethics Committee (2021KLR601), and all individuals signed informed consent.
The Procedure of Cervical Cerclage
Cervical cerclage was offered to those pregnant women with cervical insufficiency and was performed using the McDonald technique under spinal anesthesia. Prophylactic antibiotics (intravenous Cefmetazole 1g) were performed routinely before cerclage. Our previous study described the specific surgical procedures in detail.14 The same team performed all cervical cerclages by a standardized technique. Cervical cerclage was only taken without surgical contraindications: heavy vaginal bleeding and signs of maternal infection (temperature >37.5°C, purulent discharge, and tachycardia >110 bpm). There is no different progesterone administration after the cerclage procedure. Antibiotics were given based on the suggestions of the American College of Obstetricians and Gynecologists.21 Immediate termination of pregnancy is recommended in case of chorioamnionitis, fetal distress, persistent preterm birth, or other emergency conditions.
Definition
Successful cervical cerclage is a practical extension of gestational age, and the newborns are discharged from the hospital without identifiable complications. And then, the unsuccessful cervical cerclage included miscarriage, intrauterine death, neonatal death, or neonatal morbidity. And significant neonatal morbidity was defined as the presence of any of the following: respiratory distress syndrome (RDS), intro-ventricular hemorrhage (VIH), sepsis, necrotic enterocolitis (NEC), retinopathy of prematurity, and patent ductus arteriosus (PDA).
Blood Cell Count Assay
The collection of blood samples was performed in two time periods. The first time was completed within three days before the cervical cerclage procedure, and the second time within three days after the process. The blood samples were collected through face-to-face interviews. The samples were sent to the laboratory for the test immediately. The white blood cell (WBC) counts, neutrophil counts, lymphocyte counts, monocyte counts, and platelet counts were detected with flow cytometry (XE-3000, SYSMES, Kobe, Japan). According to the calculation formula, the SII (platelet count×neutrophil count/lymphocyte count) and SIRI (monocyte count×neutrophil count/lymphocyte count) were calculated with absolute neutrophil count (×109 /L), monocyte count (×109 /L), lymphocyte count (×109 /L) and platelet count (×109 /L).22,23 In addition, ΔSII is defined as Pre-SII minus Post-SII. Similarly, ΔSIRI means Pre-SIRI minus Post-SIRI.
Statistical Analysis
The counting data were analyzed with t-tests, and the measurement data were calculated by chi-square tests using SPSS version 26.0 (IBM, Armonk, NY, USA). And then, the Spearman rank correlation coefficient was performed to determine relationships between novel systemic inflammation markers (Pre-SII, Pre-SIRI, Post-SII, Post-SIRI, ΔSII, and ΔSIRII) and maternal-neonatal outcomes. Diagnostic accuracy of novel systemic inflammation markers for outcomes of cervical cerclage was expressed as the area under the receiver operating characteristic (ROC) curve (AUC). Multiple logistic regression analysis was used to assess the risk factors associated with the prognosis of the cervical cerclage. The results were presented as odds ratio (OR) and 95% confidence interval (CI). A P value less than 0.05 was defined as statistically significant in all statistical tests.
Results
The Baseline Characteristics
Finally, 328 pregnant women enrolled in the study. The detailed characteristics of pregnant women and pregnancy outcomes are shown in Table 1. The mean age of the study subjects was 31.0±4.4 years, and the mean body mass index (BMI) was 22.8±3.3 (cm2/kg). The median times of gravida and parity were 2 (0–8) times and 0 (0–3) times. Some pregnancy-specific symptoms and diseases are described in the following. There are 126 (28.4%) women with gestational diabetes (GDM), 22 (6.7%) with gestational hypertension, and 30 (9.1%) with recurrent abortion. Also, there are 117 (35.7%) women with shorter cervical lengths (≤1.5cm), 60 (18.3%) with cervical dilation (≧2cm), and 96 (29.3%) with bulging membranes. And then, the median gestational age (GA) at the time of cerclage was 22+3 (12+5- 27+4), PPROM 33+3 (22+3- 41+4), and delivery 34+3 (17+3- 41+1). Furthermore, the mean interval between cervical cerclage and delivery was 82.1±43.3 days. Regarding the adverse pregnancy complications, there were 77 (23.5%) women with preterm premature rupture of membranes (PPROM), 9 (2.7%) with postpartum hemorrhage, 8 (2.4%) with intrapartum fever, and 130 (39.6%) with cesarean delivery. As for neonatal outcomes, 36 (11.0%) newborns died, and the mean birth weight was 2491.2±1019.5g. Most babies have a good prognosis delivered after 28 weeks. However, there were some severe neonatal outcomes such as RDS 59 (20.1%), IVH 25 (8.5%), sepsis 16 (5.5%), NEC 14 (4.2%), retinopathy of prematurity 19 (6.5%) and PDA 24 (8.2%).
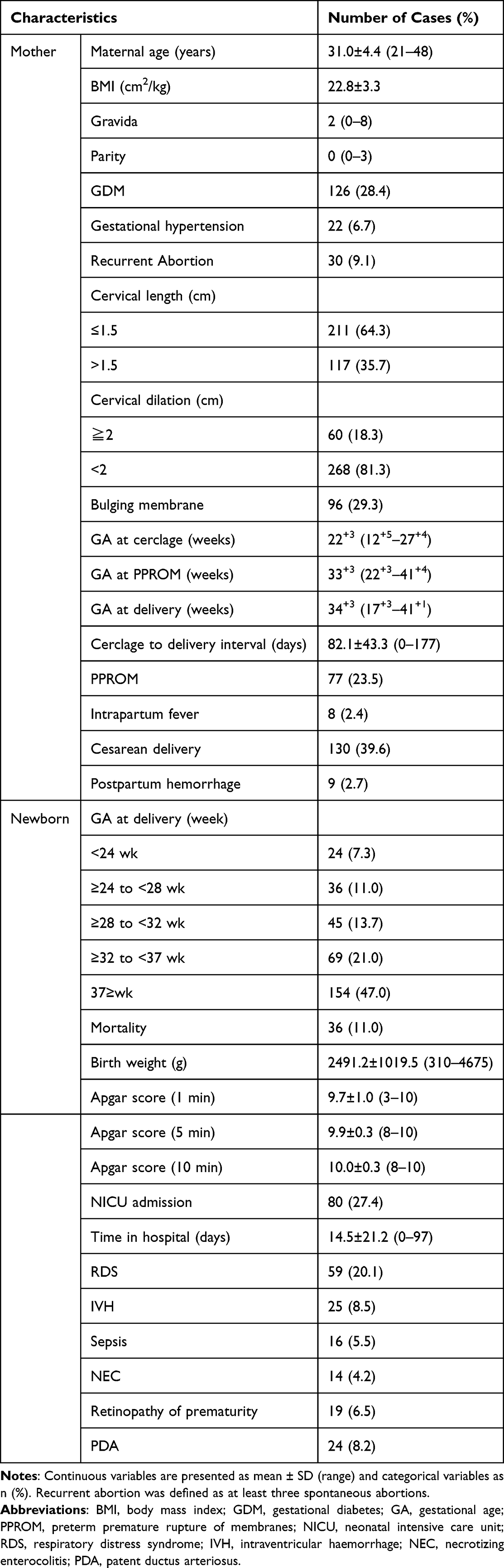 |
Table 1 Clinical Characteristics of the Study Population |
The Predictive Risk Factors for Cervical Cerclage Outcomes
Finally, 223 (67.99%) pregnant women obtained successful cervical cerclage. As shown in Table 2, the maternal age, the baseline BMI (cm2/kg), the times of gravida, the rate of recurrent abortion, the PPROM, cervical length shorter (<1.5cm), cervical dilation (≥2cm), the bulging membrane, the Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, and the ΔSII were significantly different between the successful and unsuccessful outcomes (all P<0.05). In addition, the times of parity, GDM, gestational hypertension, and the ΔSIRI were not significantly different.
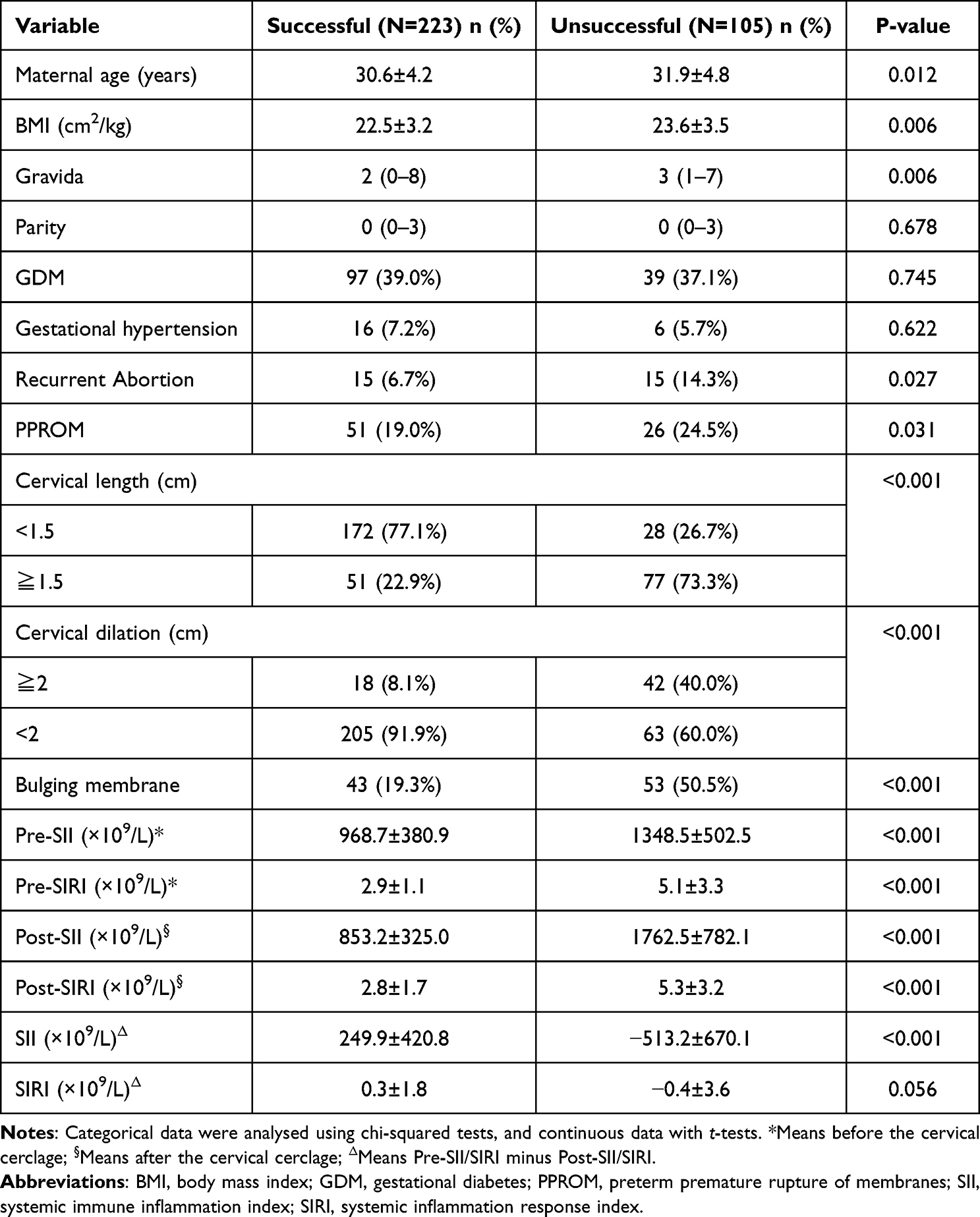 |
Table 2 The Association Between Inflammatory Markers and Cervical Cerclage Outcomes |
The Relationships Between the Dynamic Change of Novel Systemic Inflammation Markers and Maternal-Neonatal Outcomes
Table 3 shows that maternal blood novel systemic inflammation markers, such as Pre-SII, the Pre-SIRI, Post-SII, Post-SIRI, and the ΔSII, were significantly related to maternal outcomes. It suggested that a lower Pre-SII, a lower Pre-SIRI, a lower Post-SII, a lower Post-SIRI, and a higher ΔSII level associated with a longer cerclage to delivery interval times (r =−0.360, P<0.001; r =−0.372, P<0.001; r =−0.495, P<0.001; r =−0.363, P<0.001; r =−355, P<0.001).
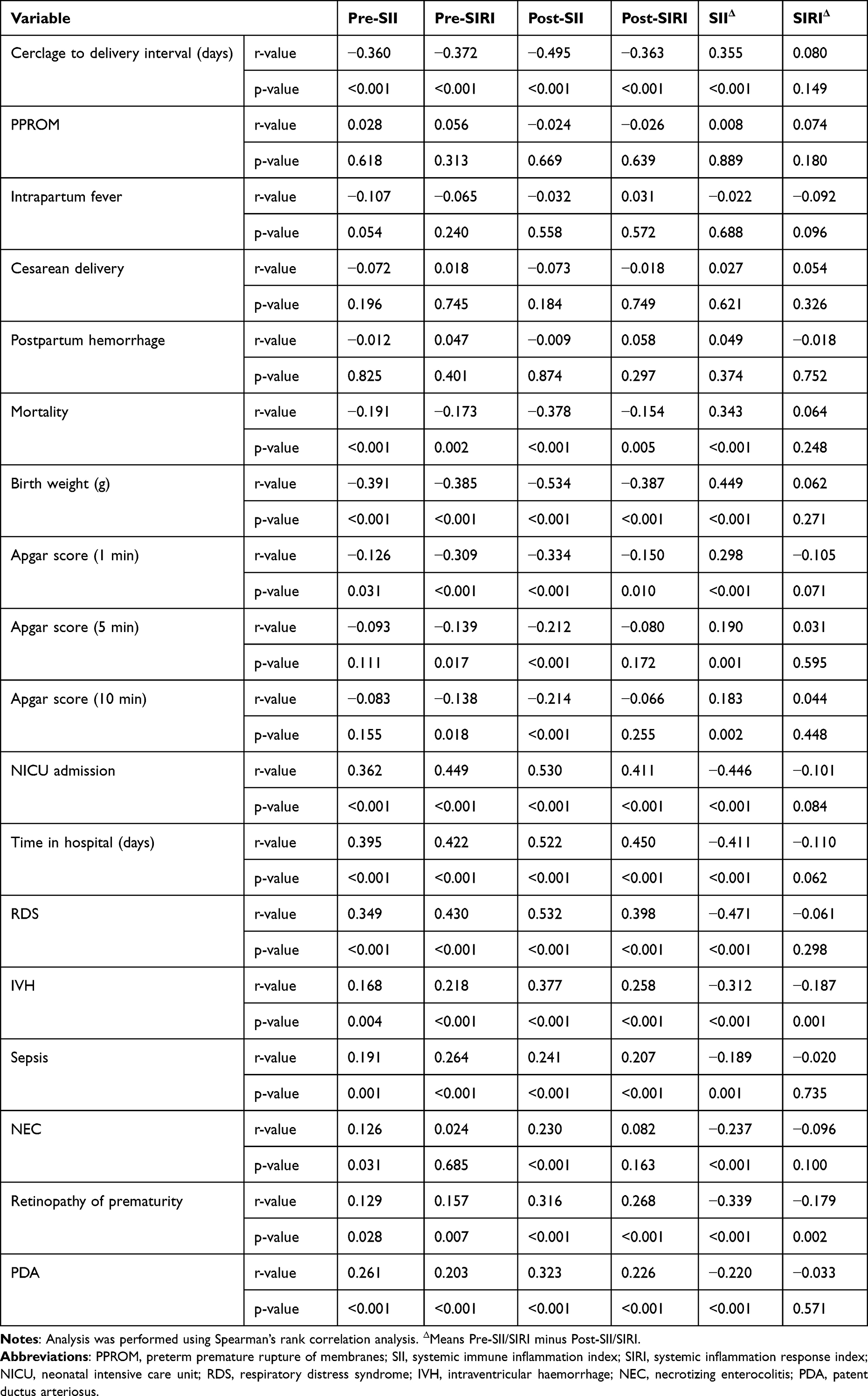 |
Table 3 Relationships Between the Inflammatory Markers and Maternal-Neonatal Outcomes |
In addition, there are relationships between maternal blood novel systemic inflammation markers and neonatal outcomes. Significant associations were revealed between mothers with a higher Pre-SII, a higher Pre-SIRI, a higher Post-SII, a higher Post-SIRI, and a lower ΔSII levels with a higher mortality rate (r =−0.191, P<0.001; r =−0.173, P=0.002; r =−0.378, P<0.001; r =−0.154, P=0.005; r =0.343, P<0.001), lower birth weight (r =−0.391, P<0.001; r =−0.385, P<0.001; r =−0.534, P<0.001; r =−0.387, P<0.001; r =0.449 P<0.001), a lower neonatal Apgar score (1 min) (r =−0.126, P=0.031; r =0.309, P<0.001; r =−0.334, P<0.001; r =−0.150 P=0.010; r =0.298, P<0.001), a lower neonatal Apgar score (5 min) (r =−0.139, P=0.017; r =−0.212, P<0.001; r =0.190, P=0.001), a lower neonatal Apgar score (10 min)(r =−0.138, P=0.018; r =−0.214, P<0.001; r =0.183, P=0.002), a higher rate of NICU admission (r =0.362, P<0.001; r=0.449, P<0.001; r =0.530, P<0.001; r =0.411, P<0.001; r =−0.446, P<0.001), an longer times in hospital (r =0.395, P<0.001; r=0.422, P<0.001; r =0.522, P<0.001; r =0.450, P<0.001; r =−0.411, P<0.001), an higher rate of RDS (r =0.349, P<0.001; r=0.430, P<0.001; r =0.532, P<0.001; r =0.398, P<0.001; r =−0.471, P<0.001), an higher rate of IVH (r =0.168, P<0.001; r=0.218, P<0.001; r =0.377, P<0.001; r =0.258, P<0.001; r =−0.471, P<0.001), an higher rate of sepsis (r =0.191, P=0.001; r=0.264, P<0.001; r =0.241, P<0.001; r =0.207, P<0.001; r =−0.189, P=0.001), an higher rate of NEC (r =0.126, P=0.031; r=0.230, P<0.001; r =−0.237, P<0.001), an higher rate of retinopathy of prematurity (r =0.129, P=0.028; r=0.157, P=0.007; r =0.316, P<0.001; r =0.268, P<0.001; r =−0.339, P<0.001), and an higher rate of PDA (r =0.261, P<0.001; r=0.203, P<0.001; r =0.323, P<0.001; r =0.226, P<0.001; r =−0.220, P<0.001).
Predictive Value of Dynamic Change of Novel Systemic Inflammation Markers for Outcomes After Cervical Cerclage
ROC analyses of maternal blood novel systemic inflammation markers, such as Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, the ΔSII, and ΔSIRI, were performed to predict the outcomes after cervical cerclage. We revealed that the Post-SII level had the highest AUC (0.845), followed by ΔSII (0.840), Post-SIRI (0.807), the Pre-SIRI (0.771), Pre-SII (0.733), and ΔSIRI (0.585). Also, an optimal cut-off of Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, the ΔSII, and ΔSIRI levels was 1225.7, 4.1803, 1328.9, 3.1684, −204.35 and −0.9015, respectively (Figure 1).
 |
Figure 1 Cut-off, the optimal novel systemic inflammation markers level is used to predict the outcome of cervical cerclage according to the ROC curve. (A) Pre-SII level; (B) Pre-SIRI level; (C) Post-SII level; (D) Post-SIRI level; (E) ΔSII level; (F) ΔSIRI levels. Abbreviations: SII, systemic immune inflammation index; SIRI, systemic inflammation response index; AUC, the area under the ROC curve; CI, confidence interval. Note: ΔMeans Pre-SII/SIRI minus Post-SII/SIRI. |
The sensitivity and specificity of Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, the ΔSII, and ΔSIRI were 56.19/88.79%, 59.05/80.27%, 68.57/92.83%, 75.24/74.89%,71.43/90.58%, and 43.81/86.65%. In addition, the PPV and NPV of the Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, the ΔSII, and ΔSIRI were 70.24/81.15%, 58.49/80.63%, 81.82/86.25%, 58.52/86.53%, 78.13/87.07%, and 58.97/76.40% (Table 4).
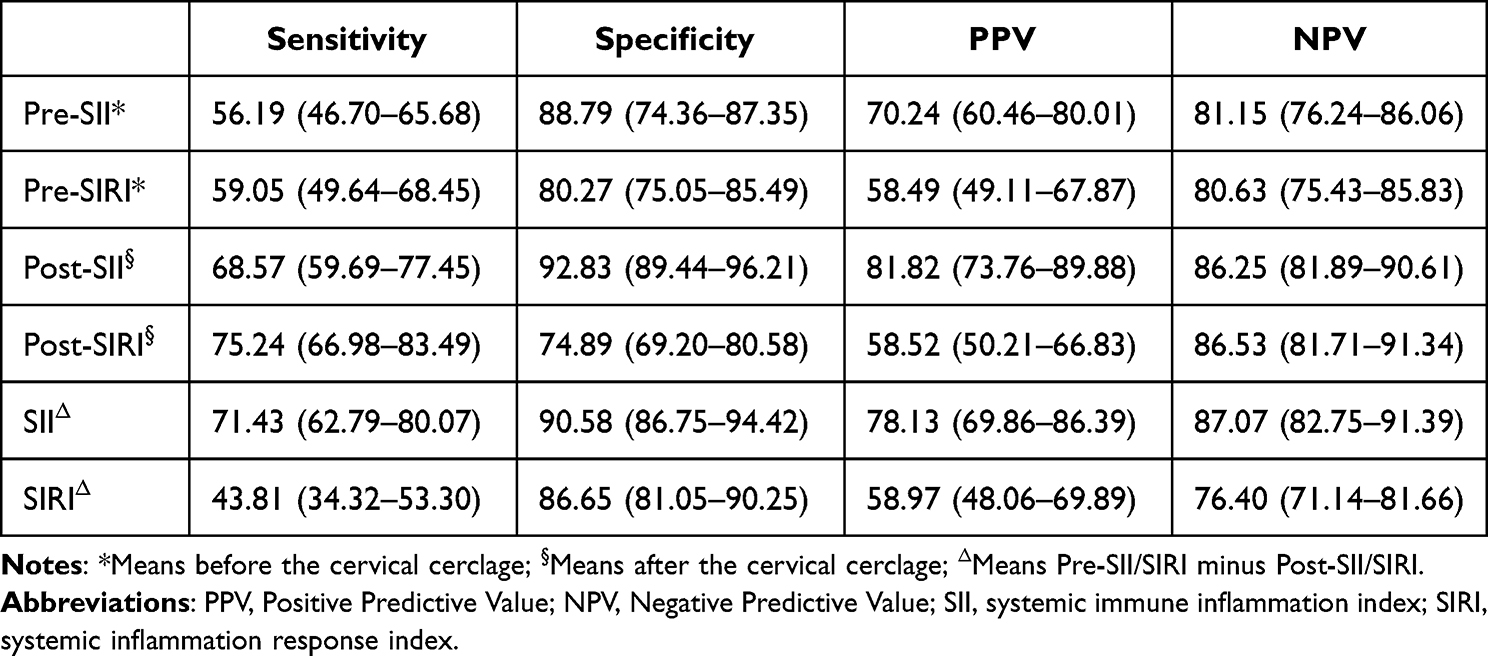 |
Table 4 Diagnostic Accuracy of the Inflammatory Markers for the Outcomes of Cervical Cerclage |
The independent risk factors associated with prognosis after cervical cerclage by multi-variable logistic regression analysis were presented in Figure 2. The results demonstrated that the ΔSII level had the highest odds ratio (OR) (OR=14.560; 95% CI (4.461–47.518)), followed by short cervical length (<1.5cm)(OR = 1.796; 95% (0.473–4.975)), short cervical length (<1.5cm)(OR = 14.256; 95% (4.766–42.645)), Post-SII level (OR =9.200; 95% (4.142–25.949)), bulging membrane (OR =6.800; 95% (2.141–21.600)), Pre-SII level (OR =6.212; 95% (4.117–18.237)), cervical dilation (≥2cm) (OR =5.546; 95% (0.864–23.924)), 95% (4.117–18.237)), Pre-SIRI level (OR =5.436; 95% (3.104–15.696)) and Post-SIRI level (OR =4.941; 95% (2.971–15.904)).
 |
Figure 2 Independent risk factors for predicting the unsuccessful cervical cerclage. Abbreviations: SII, systemic immune inflammation index; SIRI, systemic inflammation response index; BMI, body mass index; PPROM, preterm premature rupture of membranes; OR, odds ratio, CI, confidence interval. Note: ΔMeans Pre-SII/SIRI minus Post-SII/SIRI. |
Discussion
Cervical insufficiency is the main factor causing fetal late pregnancy abortion and premature birth. It has increased yearly, causing a higher perinatal mortality rate and severely harming individuals and families. Cervical cerclage is the most valuable surgical treatment for cervical insufficiency. It is widely used in clinical practice. Unfortunately, some adverse pregnancy outcomes, such as PPROM, chorioamnionitis, and cervical laceration, occurred, and the mechanism remains unknown.24,25 Therefore, it is urgent to find novel and reliable non-invasive indicators to predict the pregnancy outcomes of cervical cerclage.
In the present study, 223 (67.99%) pregnant women obtained successful cervical cerclage, suggesting that the method of cervical cerclage can effectively reduce the rate of preterm birth. It is similar to our previous studies.14,20 In addition, 36 (11.0%) newborns died in the study. Similarly, other studies reported the neonatal mortality rate ranging from 12.7–47.5%.26,27 What is more, our results revealed that the maternal age, the baseline BMI (cm2/kg), the times of gravida, the rate of recurrent abortion, the PPROM, cervical length shorter (<1.5cm), cervical dilation (≥2cm), the bulging membrane are risk factors for subsequent adverse cervical cerclage outcome. It is consistent with another study. Wei et al28 revealed that pregnancies with women with cervical dilatation (≥2cm) indicated a higher rate of preterm birth and an average delivered age before 27 weeks. In addition, Ito et al29 also revealed the influence of bulging membranes on pregnancy outcomes.
Importantly, our study demonstrated that the Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, and the ΔSII significantly differed between the successful and unsuccessful outcomes. In addition, the ΔSII level had the highest OR to predict the prognosis of cervical cerclage. Moreover, the maternal blood novel systemic inflammation markers (a higher Pre-SII, a higher Pre-SIRI, a higher Post-SII, a higher Post-SIRI, and lower ΔSII levels) were related to shorter cerclage to delivery interval times. Furthermore, a higher Pre-SII, a higher Pre-SIRI, a higher Post-SII, a higher Post-SIRI, and a lower ΔSII level significantly suggested poor prognostic neonatal outcome, with a higher neonatal mortality, a lower neonatal Apgar score (1min), a lower neonatal Apgar score (5 min), a lower neonatal Apgar score (10 min), a higher rate of NICU admission, a long times in hospital and a higher rate of complications (RDS, IVH, sepsis, NEC, retinopathy of prematurity and PDA). Our previous study found that the baseline SII level and SIRI level are important biochemical markers for predicting the outcome of cervical cerclage and maternal-neonatal outcomes.20 Recently, It has been demonstrated that inflammatory indicators may predict pregnancy prognosis after cervical cerclage.30 Because cervical dilatation usually increases the risk of infection, it may lead to poor outcomes after cervical insufficiency. It is reported that nearly 40% of preterm birth had inflammation of the uterine cavity or membranes, which is considered to be the occurrence of preterm birth.31 Some studies have demonstrated that SII and SIRI are comprehensive indicators that can fully reflect local immunity and systemic inflammatory response.15–17 SII and SIRI are new prognostic indicators of systemic immune inflammation. Its ability to predict prognosis has certain advantages over a traditional inflammatory index. Moreover, SII and SIRI are easy to obtain and less cost-effective, so they are gradually applied to clinical research.
Interestingly, this study found that the Post-SII level had the highest AUC (0.845), followed by ΔSII (0.840), Post-SIRI (0.807), the Pre-SIRI (0.771), Pre-SII (0.733), and ΔSIRI (0.585), respectively. The sensitivity and specificity of Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, the ΔSII, and ΔSIRI were 56.19/88.79%, 59.05/80.27%, 68.57/92.83%, 75.24/74.89%,71.43/90.58%, and 43.81/86.65%. In addition, the PPV and NPV of the Pre-SII, the Pre-SIRI, the Post-SII, the Post-SIRI, the ΔSII, and ΔSIRI were 70.24/81.15%, 58.49/80.63%, 81.82/86.25%, 58.52/86.53%, 78.13/87.07%, and 58.97/76.40%. Comparing the different indicators, we suggested that Post-SII and ΔSII are more suitable predictors for outcome after cervical cerclage due to higher sensitivity, specificity, PPV, and NPV.
There are some limitations to this study. Firstly, this study did not explore twin and multiple pregnancies because the surgical indications for twin and multiple pregnancies are unclear. So the conclusions in this study do not apply to twin and multiple pregnancies. Secondly, this is a retrospective study, so temporality cannot be ascertained. Therefore, a prospective study and a randomized controlled trial are necessary.
In conclusion, this study demonstrated that the Pre-SII, the Post-SII, the Post-SIRI, and the ΔSII level in maternal peripheral blood could be valuable biomarkers to predict the prognosis of the cervical cerclage, especially the Post-SII and ΔSII level. Furthermore, the dynamic Change of the novel systemic inflammation markers (SII and SIRI) can more accurately and objectively predict clinical outcomes after cervical cerclage. In addition, our results suggested that they are significantly associated with maternal-neonatal outcomes. We advocate dynamic Change of SII level and SIRI level from maternal peripheral blood with noninvasive procedures as a suitable and practical method to predict the prognosis of cervical cerclage. Our results may offer additional clinical prognostic information, which helps provide personalized treatment before surgery and enhance postoperative surveillance.
Patient Consent for Publication
The Hospital Ethics Committee of Fujian Provincial Maternity and Children’s Hospital, an affiliated hospital of Fujian Medical University, approved the study (2021KLR601) and complied with the Declaration of Helsinki. And all individuals participating in this study signed written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the report has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by grants from the Fujian Science and Technology Innovation Joint Fund Project (2020Y9148) and Natural Science Foundation of Fujian Province (No.2021J01406).
Disclosure
All authors declare that they have no competing interests.
References
1. Walani SR. Global burden of preterm birth. Int J Gynaecol Obstet. 2020;150(1):31–33. doi:10.1002/ijgo.13195
2. Alfirevic Z, Stampalija T, Medley N. Cervical stitch (cerclage) for preventing preterm birth in singleton pregnancy. Cochrane Database Syst Rev. 2017;6(6):CD008991. doi:10.1002/14651858.CD008991.pub3
3. Wang SW, Ma LL, Huang S, Liang L, Zhang JR. Role of cervical cerclage and vaginal progesterone in the treatment of cervical incompetence with/without preterm birth history. Chin Med J. 2016;129(22):2670–2675. doi:10.4103/0366-6999.193451
4. American College of Obstetricians and Gynecologists. ACOG practice bulletin No.142: cerclage for managing cervical insufficiency. Obstet Gynecol. 2014;123:372–379. doi:10.1097/01.AOG.0000443276.68274.cc
5. Gonzales SK, Adair CD, Torres C, et al. Robotic-assisted laparoscopic abdominal cerclage placement during pregnancy. J Minim Invasive Gynecol. 2018;25(5):832–835. doi:10.1016/j.jmig.2017.12.014
6. Basbug A, Bayrak M, Doğan O, Ellibeş Kaya A, Goynumer G. McDonald versus modified Shirodkar rescue cerclage in women with prolapsed fetal membranes. J Matern Fetal Neonatal Med. 2020;33(7):1075–1079. doi:10.1080/14767058.2018.1514378
7. Namouz S, Porat S, Okun N, Windrim R, Farine D. Emergency cerclage: literature re- 335 336 view. Obstet Gynecol Surv. 2013;68(5):379–388. doi:10.1097/OGX.0b013e31828737c7
8. Brown R, Gagnon R, Delisle MF, et al. Cervical insuffificiency and cervical cerclage. J Obstet Gynaecol Can. 2013;35(12):1115–1127. doi:10.1016/S1701-2163(15)30764-7
9. Jung EY, Park KH, Lee SY, Ryu A, Joo JK, Park JW. Predicting outcomes of emergency cerclage in women with cervical insufficiency using inflammatory markers in maternal blood and amniotic fluid. Int J Gynaecol Obstet. 2016;132(2):165–169. doi:10.1016/j.ijgo.2015.07.011
10. Son GH, You YA, Kwon EJ, Lee KY, Kim YJ. Comparative analysis of midtrimester amniotic fluid cytokine levels to predict spontaneous very pre-term birth in patients with cervical insufficiency. Am J Reprod Immunol. 2016;75(2):155–161. doi:10.1111/aji.12451
11. Again E, Aguin T, Cordoba M, et al. Amniotic fluid inflammation with negative culture and outcome after cervical cerclage. J Matern Fetal Neonatal Med. 2012;25(10):1990–1994. doi:10.3109/14767058.2012.667177
12. Lee KY, Jun HA, Kim HB, Kang SW. Interleukin-6, but not relaxin, predicts the outcome of rescue cerclage in women with cervical incompetence. Am J Obstet Gynecol. 2004;191(3):784–789. doi:10.1016/j.ajog.2004.04.019
13. Park JC, Kim DJ, Kwak-Kim J. Upregulated amniotic fluid cytokines and chemokines in emergency cerclage with protruding membranes. Am J Reprod Immunol. 2011;66(4):310–319. doi:10.1111/j.1600-0897.2011.00991.x
14. Fang J, Chen L, Chen Z, Jiang X, Pan M. Association of the vaginal microbiota with pregnancy outcomes in Chinese women after cervical cerclage. Reprod Biomed Online. 2020;41(4):698–706. doi:10.1016/j.rbmo.2020.06.016
15. Wang J, Zhou D, Dai Z, Li X. Association between systemic immune inflammation index and diabetic depression. Clin Interv Aging. 2021;16:97–105. doi:10.2147/CIA.S285000
16. Zhang F, Niu M, Wang L, et al. Systemic-immuneInflammation index as a promising biomarker for predicting perioperative ischemic stroke in older patients who underwent non-cardiac surgery. Front Aging Neurosci. 2022;14:865244. doi:10.3389/fnagi.2022.865244
17. Tian T, Lu J, Zhao W, et al. Associations of systemic inflammation markers with identification of pulmonary nodule and incident lung cancer in Chinese population. Cancer Med. 2022;11:2482–2491. doi:10.1002/cam4.4606
18. Goyal N, Tsivgoulis G, Chang JJ, et al. Admission neutrophil-to-lymphocyte ratio as a prognostic biomarker of outcomes in large vessel occlusion strokes. Stroke. 2018;49(8):1985–1987. doi:10.1161/STROKEAHA.118.021477
19. Weng Y, Zeng T, Huang H, et al. Systemic immune inflammation index predicts 3-month functional outcome in acute ischemic stroke patients treated with intravenous thrombolysis. Clin Interv Aging. 2021;16:877–886. doi:10.2147/CIA.S311047
20. Fang J, Lin Y, Chen Z, Lin Y, Pan M. The association of inflammatory markers with maternal-neonatal outcome after cervical cerclage. J Inflamm Res. 2023;19(16):245–255. doi:10.2147/JIR.S393666
21. American College of Obstetricians and Gynecologists. Prelabor rupture of membranes: practice bulletin no. 188. Obstet Gynecol. 2018;131:e1–e14. doi:10.1097/AOG.0000000000002455
22. Nam KW, Kwon HM, Jeong HY, et al. High neutrophil to lymphocyte ratio is associated with white matter hyperintensity in a healthy population. J Neurol Sci. 2017;380:128–131. doi:10.1016/j.jns.2017.07.024
23. Benedetti F, Palladini M, Paolini M, et al. Brain correlates of depression, post-traumatic distress, and inflammatory biomarkers in COVID-19 survivors: a multimodal magnetic resonance imaging study. Brain Behav Immun Health. 2021;18:100387. doi:10.1016/j.bbih.2021.100387
24. Wu Y, Liang X, Cai M, Gao L, Lan J, Yang X. Development and validation of a model for individualized prediction of cervical insufficiency risks in patients undergoing IVF/ICSI treatment. Reprod Biol Endocrinol. 2021;19(1):6. doi:10.1186/s12958-020-00693-x
25. Kassanos D, Salamalekis E, Vitoratos N, Panayotopoulos N, Loghis C, Creatsas C. The value of transvaginal ultrasonography in diagnosis and management of cervical incompetence. Clin Exp Obstet Gynecol. 2001;28(4):266–268.
26. Kurup M, Goldkrand JW. Cervical incompetence: elective, emergent, or urgent cerclage. Am J Obstet Gynecol. 1999;181(2):240–246. doi:10.1016/S0002-9378(99)70542-9
27. Galyean A, Garite TJ, Maurel K, et al. Removal versus retention of cerclage in preterm premature rupture of membranes: a randomized controlled trial. Am J Obstet Gynecol. 2014;211:399.e1–399.e7. doi:10.1016/j.ajog.2014.04.009
28. Wei L, Xie H, Yan P. Prognostic value of the systemic inflammation response index in human malignancy: a meta-analysis. Medicine. 2020;99(50):e23486–e23486. doi:10.1097/MD.0000000000023486
29. Ito A, Maseki Y, Ikeda S, Tezuka A, Kuribayashi M, Furuhashi M. Factors associated with delivery at or after 28 weeks gestation in women with bulging fetal membranes before 26 weeks gestation. J Matern Fetal Neonatal Med. 2017;30(17):2046–2050. doi:10.1080/14767058.2016.1236247
30. Gülücü S, Neşet G. The role of inflammatory markers in the evaluation of cerclage success. Chron Precis Med Res. 2022;3(3):174–179.
31. Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet. 2008;371:75–84. doi:10.1016/S0140-6736(08)60074-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association of Inflammatory Markers with Maternal-Neonatal Outcome After Cervical Cerclage
Fang J, Lin Y, Chen Z, Lin Y, Pan M
Journal of Inflammation Research 2023, 16:245-255
Published Date: 19 January 2023