Back to Journals » International Journal of General Medicine » Volume 15
Duplex Hemodynamic Parameters of Both Superior and Inferior Thyroid Arteries in Evaluation of Thyroid Hyperfunction Disorders
Authors Assem Hussein M, Abdel Hamid A, M Abdel Samie R ![]() , Hussein E, Sadik Elsawy S
, Hussein E, Sadik Elsawy S
Received 17 May 2022
Accepted for publication 29 August 2022
Published 9 September 2022 Volume 2022:15 Pages 7131—7144
DOI https://doi.org/10.2147/IJGM.S375016
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Maha Assem Hussein,1 Alaa Abdel Hamid,2 Rasha M Abdel Samie,1 Elshaymaa Hussein,3 Shereen Sadik Elsawy1
1Internal Medicine Department, Faculty of Medicine, Kasr El-Ainy Hospital, Cairo University, Cairo, Egypt; 2Kasr El-Ainy Vascular Laboratory, Cairo University, Cairo, Egypt; 3Nuclear Medicine Department, Faculty of Medicine, Kasr El-Ainy Hospital, Cairo University, Cairo, Egypt
Correspondence: Rasha M Abdel Samie, Email [email protected]
Background: Thyrotoxicosis may be caused by Graves’ disease or destructive thyroiditis. Differentiation between causes of thyrotoxicosis is crucial as management will differ. 99mTechnetium (Tc)-pertechnetate thyroid scintigraphy is currently the gold standard for this purpose, however, is expensive and uses ionizing radiation.
Objective: To evaluate the role of color flow Doppler Ultrasound (CDU) of the superior thyroid (STA) and inferior thyroid arteries (ITA) as an inexpensive, non-invasive tool that can aid in differentiating between Graves’ disease and thyroiditis and compare it with thyroid scintigraphy.
Methods: Sixty-nine patients with newly-diagnosed thyrotoxicosis and 30 controls were enrolled. Thyroid functions, thyroid scintigraphy, and CDU of STA and ITA with measurements of peak systolic velocity (PSV) and end diastolic velocity (EDV), were performed. According to thyroid scintigraphy results, patients were divided into two groups: 42 patients with Graves’ disease and 27 patients with thyroiditis.
Results: PSV and EDV of both STA and ITA were significantly higher in patients with Graves’ disease than thyroiditis (p-values < 0.001). The STA-PSV had an equal sensitivity and specificity of 66.7%; cut-off value 76.57 cm/s, while those of STA-EDV were 73.8%, and 77.8% respectively; cut-off value 28.22 cm/s. ITA-PSV had a sensitivity and specificity of 76.2% and 77.8%, respectively; cut-off value 62.12 cm/s), while those of ITA-EDV were 78.6% and 77.8%, respectively; cut-off value 5.22 cm/s.
Conclusion: CDU parameters of the STA and ITA could be used as an alternative to thyroid scintigraphy for discriminating between Graves’ disease and thyroiditis.
Keywords: Color Doppler Flow Ultrasound, peak systolic velocity, end-diastolic velocity, Graves’ disease, thyroiditis
Introduction
Two of the common causes of thyrotoxicosis are hyperthyroidism due to Graves’ disease and destructive thyroiditis. It is crucial to differentiate between them as managing each one will differ.1 Thyroid scintigraphy using Technetium 99 99mTc-pertechnetate or iodine 123 radioisotopes is a sensitive method used to differentiate between Graves’ disease and thyroiditis,2 with a considerably low effective radiation dose (to the whole body) of around 3.2 millisieverts (mSv) being delivered to adults for conventional activities of thyroid scan.3 However, it is costly and may be contraindicated in some cases, as in pregnant or lactating female patients.4
It has been established that measurement of thyrotropin receptor antibodies (TRAb) is greatly efficacious in rapid diagnosis of Graves’ disease,5 particularly with the emergence of new-generation TRAb immunoassays demonstrating high sensitivity and specificity.6 Thyroid-stimulating immunoglobulins (TSI), although characteristic of Graves’ disease, are not integrated in recent algorithms for diagnosis of hyperthyroidism as they are evaluated by costly and clinically unpractical bioassays. Few studies employed an entirely automated chemiluminescent bioassay (Immulite) for the direct detection of TSI but concluded that TRAb and TSI assays had the same diagnostic performance in detection of Graves’ hyperthyroidism.6
Most of the diffuse pathological involvement of the thyroid gland is coupled with impaired vascularity.7,8 High systolic velocities on Doppler ultrasound have been reported in cases with thyrotoxicosis.9–11
Color Doppler Flow Ultrasound (CDU) has emerged as an easier, inexpensive and a more convenient method for investigating the cause of thyrotoxicosis.12–16 It has also been applied clinically in discriminating between benign and malignant thyroid nodules17 because of its high sensitivity and specificity and has shown diagnostic utility in the prediction and grading of malignant thyroid follicular neoplasms.18,19 Moreover, CDU may be a useful tool in timely identification of asymptomatic, incidental diffuse parenchymal thyroid disease;20 evaluation of functional status of thyroid gland as well as disease activity, remission, or recurrence in case of Graves’ disease or thyroiditis;19 and clinical value in monitoring response to therapy.21,22
Different parameters can be evaluated by CDU including vascular pattern in thyroid parenchyma and blood flow as well as quantitative assessment of blood flow velocities in thyroid arteries.23–25
Several studies have assessed the mean peak systolic velocity (PSV) and end-diastolic velocity (EDV) in the superior and inferior thyroid arteries using color flow Doppler ultrasound for differentiating between patients with Graves’ disease and those with destructive thyroiditis.1,4,22,26,27 The sensitivity and specificity have differed among various studies and no cut-off values have yet been validated.11,28,29
Measurement of mean peak systolic velocity (PSV) in the inferior thyroid artery (ITA) has been widely employed in previous studies1,30,31 to assess its ability in distinguishing the causes of thyrotoxicosis. There are some limitations, however, to its utility in clinical practice such as the anatomic variation of the lumen size, accurate positioning due to its deep location,25,32 and interference with detection of blood flow velocity owing to variation in ITA spectral flow directions.33
Superior thyroid artery (STA) being more superficially located is more accurately positioned,34 thereby facilitating its clinical utility for measurement of PSV in multiple retrospective and prospective studies and evaluating its diagnostic accuracy in discriminating between Graves’ disease and destructive thyroiditis.11,27
The aim of the study was to assess the role of color Doppler sonography of the superior (STA) and inferior (ITA) thyroid arteries as a sensitive, non-invasive tool in differentiating between Graves’ disease and thyroiditis as compared to 99mTc-pertechnetate thyroid scintigraphy and to assess the difference in CDU parameters between the right and left thyroid arteries and their diagnostic accuracy. We also aimed to compare and assess the sensitivity and specificity of the mean PSV and EDV of both the inferior and superior thyroid arteries simultaneously and to provide optimum cut-off values for blood flow velocities for differentiating between Graves’ disease and thyroiditis.
Patients and Methods
This is a case-control, observational study and all patients were prospectively recruited from the Endocrine Clinic of Kasr El Ainy Hospital, Cairo University during the period from January to March 2022. The study protocol was approved of by the Research Ethics Committee of Cairo University and institutional clearance was obtained (N-21-2022) in agreement with ethical principles of the Declaration of Helsinki.35 All participants willingly undertook the study and informed consent was obtained prior to enrolment.
The study included 69 patients with recently established thyrotoxicosis who did not receive treatment and 30 age- and sex-matched healthy control subjects. Diagnosis of thyroid hyperfunction was based on thyroid function tests which included TSH, free T3, and free T4. The patients were then split up into two groups according to the results of 99mTc-pertechnetate thyroid scintigraphy: 42 patients with Graves’ disease and 27 patients with thyroiditis (Figure 1). The diagnosis of Graves’ disease was determined by clinical features such as the presence of diffuse goiter with or without eye, skin, or nail changes as well as diffusely increased tracer uptake pattern in the thyroid scan studies. Thyroiditis was diagnosed by the presence of thyroid tenderness, absence of eye, skin, or nail changes, as well as reduced tracer uptake pattern in the thyroid scan studies. Patients with diffuse goiter were included in the study.
 |
Figure 1 Flow chart showing patient selection. |
Patients with a history of thyroid surgery, toxic nodule, multinodular goiter, subjects prescribed iodine-containing medicines, as well as amiodarone, previous radioiodine therapy, recent exposure to iodine-containing contrast agents, pregnancy or lactation, and patients on anti-thyroid medications were excluded from the study.
All participants underwent a detailed history taking and clinical evaluation including resting pulse rate and neck examination prior to ultrasonography.
Color Doppler Ultrasound (CDU)
Thyroid ultrasound examination was performed by an experienced clinician who was uninformed about the patient’s clinical status. The subjects were advised to rest for a short period of 10 minutes prior to the Doppler examination of the thyroid gland. Examination was performed in a supine attitude with an extended neck. A color Doppler ultrasound scanner ((ALT) HDI, Ultramark, Phillips) ultrasound machine was used for the study equipped with a 7–12 MHz broadband linear array transducer. The grey scale ultrasound examination of the thyroid gland was performed evaluating the size, shape, gland echo-texture, plus the existence or absence of nodules. The color Doppler ultrasound pattern of the gland was studied. Color Doppler parameters were F. 7.6 MHz, G.76%, pulse-repetition frequency (PRF) 2.1 KHz and the wall filter (WF) was M. The STA image was acquired by shifting the probes from the sagittal portion of the upper pole in the direction of the cranial aspect of the thyroid gland, at the same time sustaining placement of the probe in the sagittal plane.
The different blood-flow velocity waveforms were assessed at a steady position with an inclination angle of less than 60° amid the beam and the superior thyroid artery and the peak systolic and end diastolic velocities were established via the velocity waveform. Spectral Doppler evaluation of the right and left inferior thyroid arteries was obtained in the transverse section wherein the vessels posteriorly traversed the common carotid arteries, or in the longitudinal section of the ascending segments of the arteries, where the vessels are found parallel to the common carotid arteries.
The angle correction cursor was positioned in parallel to the blood flow direction and the Doppler angle was maintained at ≤60°. Doppler indices obtained were peak systolic velocity (PSV) and end diastolic velocities (EDV) of the right and left superior and inferior thyroid arteries. Doppler Resistivity index (RI) was calculated according to the following formula: RI=PSV-EDV/PSV of the corresponding artery (Figures 2 and 3).
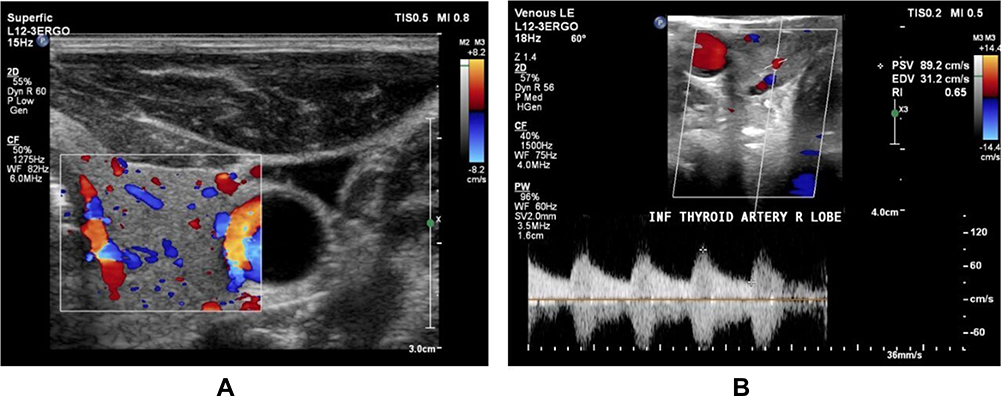 |
Figure 2 Showing images of color Doppler ultrasound and spectral Doppler flow analysis of a patient with Graves’s disease. (A) Right lobe of thyroid gland showing a diffuse increase in the thyroid gland vascularity on color Doppler. (B) Spectral Doppler flow examination of the right ITA showing an increased peak systolic velocity (89.2 cm/s) and an increased end-diastolic velocity of 31.2 cm/s. |
 |
Figure 3 Color Doppler hemodynamic parameters of the left inferior thyroid artery in a patient with thyroiditis showing a peak systolic velocity (PSV) of 17.3 cm/s, end-diastolic velocity (EDV) of 9.32 cm/s, and Resistive index (RI) of 0.46. |
Another clinician, who was oblivious to the patient’s clinical background and Doppler ultrasound examination, carried out the radioisotope scanning of the thyroid gland.
99mTechnetium (TC) Pertechnetate Thyroid Scintigraphy
It was performed according to the most updated practice guidelines for the performance of thyroid scintigraphy and uptake measurements.36 They were obtained 15 minutes after intravenous injection of 185 MBq of 99mTc pertechnetate and the static view images were attained by means of a large F-O-V dual-head gamma camera equipped with a parallel-hole collimator (Philips-Axis, Eindhoven, the Netherlands). The patients were in supine posture with an extended neck. The different static images were acquired in the anterior, and both anterior oblique projections for a minimum of 100,000 counts or 8 minutes, whichever occurs first with a 128×128 matrix size and the zooming option was adjusted to 1.0. The gamma camera was adjusted to have an energy intensity of 140 keV, together with a 20% symmetrical window. Background- and decay-corrected uptakes by the thyroid gland were estimated utilizing the software provided within the system. The parameters observed included the thyroid uptake pattern and percentage, as well as those of the salivary glands (Figure 4).
 |
Figure 4 (A) represents reduced tracer uptake in thyroiditis while (B) represents diffuse increase of radiotracer uptake in Grave’s disease. |
Statistical Analysis
Data management and analysis were accomplished using Statistical Package for Social Sciences (SPSS) version 25. Numerical data were summarized using means and standard deviations or medians and/or ranges, as appropriate. Comparisons between two groups for normally distributed numeric variables were done using the Student’s t-test while for non-normally distributed numeric variables, comparisons were done by Mann–Whitney U-test. Receiver operating characteristic (ROC) curve analysis was performed to establish the optimal cut-off point, sensitivity, specificity, and area under the curve. P-value ≤0.05 was considered statistically significant.
Results
Patients Characteristics
Sixty-nine patients who were recently diagnosed with thyrotoxicosis were split up into two groups based on the clinical findings and the results of 99mTc-pertechnetate thyroid scintigraphy: 42 patients with Graves’ disease (12 males and 30 females) and 27 patients with thyroiditis (six males and 21 females). The patients were age-matched (p-value =0.644). Clinical, biochemical characteristics, as well as thyroid scintigraphy uptake measurements and Color flow Doppler parameters of the studied groups are displayed in Table 1.
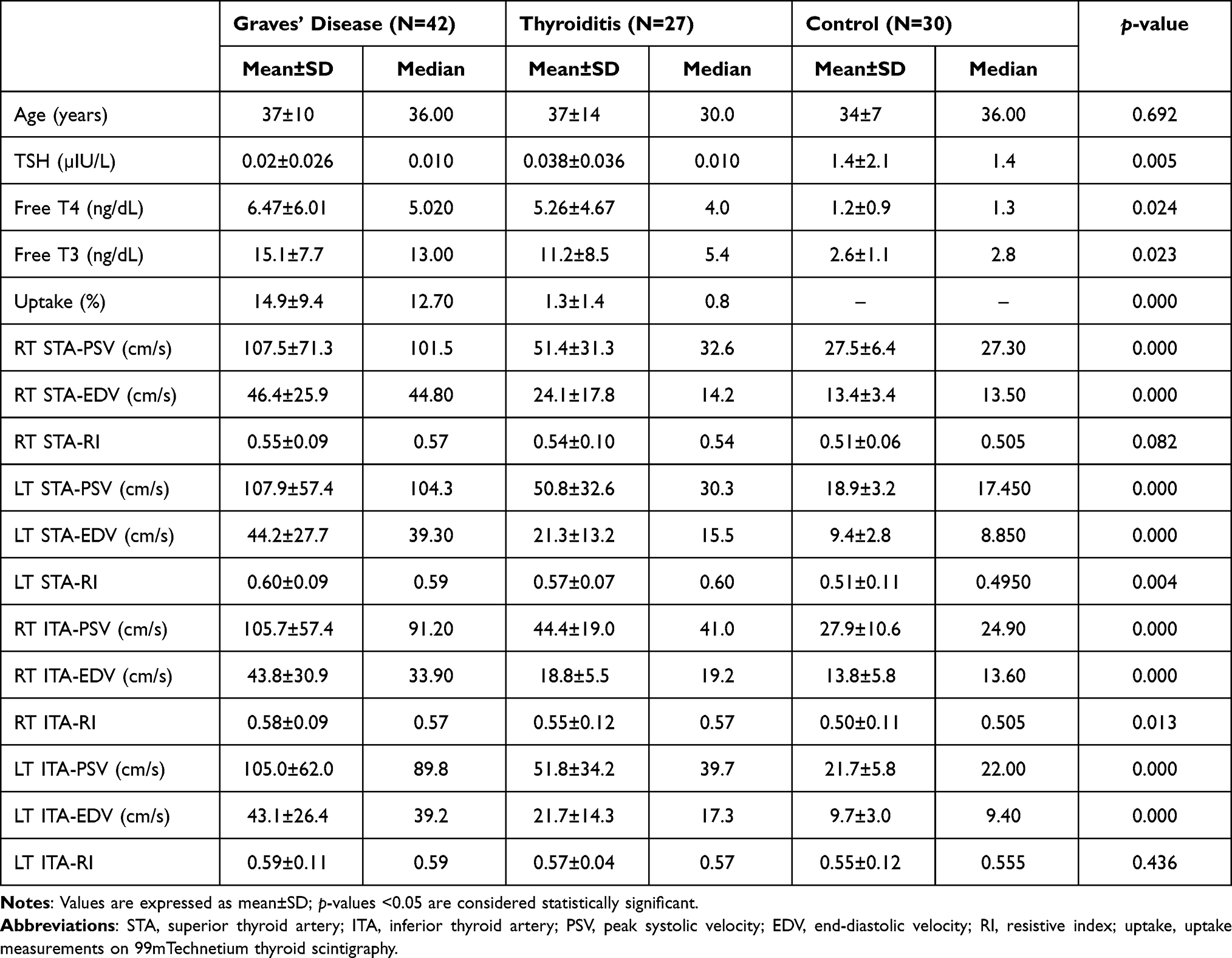 |
Table 1 Comparison of Parameters Between Studied Groups (Graves’ Disease, Thyroiditis, and the Control Group) |
Comparison of CDU Parameters Between Patients with Graves’ Disease and Thyroiditis
Evaluation of the thyroid blood flow by means of color imaging and Doppler spectral flow analysis of the superior and inferior thyroid arteries showed that the PSV and EDV of both right and left STA and ITA were significantly higher in patients with Graves’ disease as compared to patients with thyroiditis with p-values <0.001. No significant differences were, however, observed when comparing right and left STA and ITA resistivity indices between patients with Graves’ disease and thyroiditis.
Comparison of the Mean CDU Velocities of the Superior and Inferior Thyroid Arteries Between Patients with Graves’ Disease and Thyroiditis
Comparison of the mean PSV and EDV of both superior and inferior thyroid arteries among the patient groups is demonstrated in Table 2. The mean STA-PSV and EDV, as well as the mean ITA-PSV and EDV were significantly the highest among patients with Graves’ disease as compared to patients with thyroiditis, with the lowest values being observed in the euthyroid group.
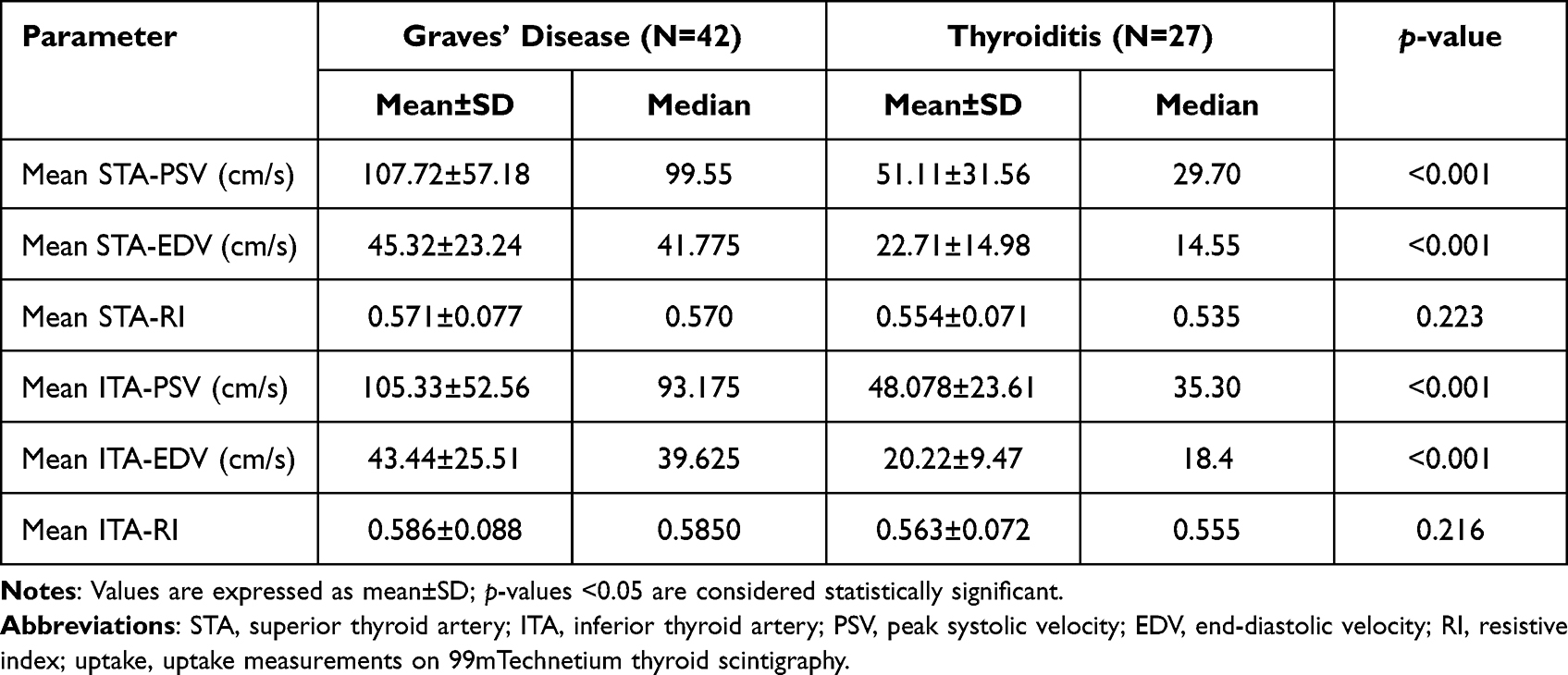 |
Table 2 Comparison Between the Patients with Graves’ Disease and Thyroiditis Regarding the Mean Systolic and Diastolic Velocities of Superior and Inferior Thyroid Arteries |
Correlation of Thyroid Scintigraphy with the Mean CDU Parameters in Patients with Thyrotoxicosis
Uptake by thyroid scintigraphy correlated significantly with CDU parameters of STA (Table 3) including mean STA PSV (r=0.629; p=0.000), STA EDV (r=0.572; p=0.000) and STA RI (r=0.283; p=0.019) in patients with thyroiditis. It also correlated significantly with CDU parameters of ITA (Table 3) including ITA-PSV (r=0.592; p=0.000) and ITA-EDV (r=0.551; p=0.000). However, CDU parameters of STA and ITA did not show a significant correlation with scintigraphy uptake in patients with Graves’ disease (Table 3).
 |
Table 3 Correlation Between Thyroid Scintigraphy Uptake and the Mean CDU Parameters of the Inferior and Superior Thyroid Arteries in the Studied Groups (Graves’ Disease, Thyroiditis) |
The Diagnostic Efficacy of the Average STA and ITA Measurements in Differentiating Between Graves’ Disease and Thyroiditis Using ROC Curve Analysis
ROC curve analysis performed to evaluate the ability of the mean STA-PSV to discriminate between Graves’ disease and thyroiditis revealed an equivalent sensitivity and specificity of 66.7%, with an area under receiver operating characteristic curve (AUC) of 0.835 (95% CI=0.735–0.934; p-value <0.001) and a cut-off value of 76.57 cm/s (Figure 5). The sensitivity and specificity significantly improved to 73.8% and 77.8%, respectively, when evaluating the ability of the mean STA-EDV in differentiating between causes of thyrotoxicosis with a similar area under ROC curve of 0.823 (95% CI=0.716–0.930; p-value <0.001) and a cut-off value of 28.22 cm/s (Figure 5). On the other hand, the mean STA-RI demonstrated a very poor sensitivity and specificity.
 |
Figure 5 ROC curve analysis for the mean STA-PSV (A) and the mean STA-EDV (B) in differentiating between Graves’ disease and thyroiditis. |
When evaluating the diagnostic performance of the inferior thyroid artery indices in differentiating between Graves’ disease and thyroiditis, the sensitivity and specificity of ITA-PSV was 76.2% and 77.8%, respectively (AUC=0.869; 95% CI=0.784–0.954; cut-off value=62.12 cm/s; p-value <0.001) (Figure 6) and this was comparable to the sensitivity and specificity of the ITA-EDV (78.6% and 77.8%, respectively) with an AUC of 0.865; 95% CI=0.788–0.952; p-value <0.001; and a cut-off value of 25.22 cm/s (Figure 6).
 |
Figure 6 ROC curve analysis for the mean ITA-PSV (A) and mean ITA-EDV (B) in differentiating between Graves’ disease and thyroiditis. |
Discussion
Color flow Doppler ultrasonography is a convenient, non-invasive, low-cost, and readily available method for evaluating blood flow and tissue vascularity. Thyroid blood flow that is diffusely augmented is a specific finding in patients with untreated Graves’ disease and an aberrant color flow Doppler pattern distinguishes most Graves’ disease patients exhibiting a normal pattern on thyroid ultrasound. Therefore, it can be used to differentiate between Graves’ disease and thyroiditis.23,24 Vascularization can be qualitatively explored by estimating the visual thyroid vascularization pattern or quantitatively studied by assessing the thyroid blood flow area. Furthermore, Doppler ultrasound permits measurement of peak systolic velocity (PSV) and end-diastolic velocity (EDV), along with other indices like the resistive index (RI) and pulsatility indices of the superior and inferior thyroid arteries as well as the intra-thyroid and intra-nodular arteries.37
These parameters, together with the B-mode ultrasound parameters, have also been integrated in a Computer-aided diagnosis (CAD) system to aid radiologists in differentiating between hot and cold thyroid nodules more accurately. Doppler indices like the resistive index (RI) and the peak systolic to the end diastolic velocity ratio (SDR) exhibited good diagnostic performance in discriminating between cold and hot nodules.17,38
Measurement of PSV is a quantitative, non-invasive, cost-effective, and readily available method that implicates the thyroid blood supply status. With the advancement in modern color Doppler technology, PSV has become a good discriminating parameter with a high reproducibility.39 The end diastolic velocity (EDV) of thyroid arteries signifies peripheral blood flow resistance.40
In this study, we assessed the role of the color Doppler flow sonography of the superior (STA) and inferior (ITA) thyroid arteries as a possible substitute of 99mTc-pertechnetate thyroid scintigraphy to differentiate between Graves’ disease and destructive thyroiditis.
Regarding the superior thyroid artery, the mean PSV and EDV of both right and left superior thyroid arteries and subsequently the average STA-PSV and STA-EDV were observed to be significantly higher in patients with Graves’ disease than in patients with thyroiditis with a p-value <0.001. This is in agreement with a study by Sundarram et al41 that also demonstrated higher mean STA-PSV among patients with untreated Graves’ disease than those with thyroiditis (54.09±4.67 cm/s vs 28.92±4.39 cm/s, respectively), however the values reported were much less than the values found in the present study (107.72±57.18 cm/s and 51.11±31.56 cm/s, respectively). As revealed in previous studies, mean STA-PSV values exceeding 100 cm/s were observed in recently diagnosed patients with Graves’ disease or those unresponsive to treatment.41
The present study exhibited an equivalent sensitivity and specificity of 66.7% for STA-PSV and a cut-off value of 76.57 cm/s, whereas the mean STA-EDV showed a sensitivity and a specificity of 73.8% and 77.8%, respectively, with a cut-off value of 28.22 cm/s. This was comparable to a study by Kumar et al,4 conducted on 65 patients with thyrotoxicosis which, however, reported a greater sensitivity of 94% and a 100% specificity of the STA-PSV in differentiating between Graves’ disease and thyroiditis at an optimal cut-off value greater than 40 cm/s. The objectivity and accuracy of STA-PSV as a quantitative measure for the etiological evaluation of hyperthyroidism was also confirmed in a former study by Erdoğan et al.25 This was also in accordance with a retrospective and a prospective analysis by Zhao et al11 on patients with untreated thyrotoxicosis that demonstrated a significantly higher mean STA-PSV in patients with Graves’ disease than those with thyroiditis, with a cut-off value of 50.5 cm/s and a high diagnostic accuracy in the differential diagnosis of thyrotoxicosis. This optimal cut-off value was further employed in hospitals where color Doppler ultrasound was done using the same standard operating procedures (SOP) but different machines and the mean STA-PSV was endorsed as a reliable test deserving promotion. The latter study also showed that the mean TRAb values were comparable to the mean STA-PSV in differentiating thyroiditis and GD. Similarly, a meta-analysis of 11 studies by Peng et al29 confirmed the eminent role of the STA-PSV in differentiating between Graves’ disease and thyroiditis, with a collective sensitivity and specificity of 86% and 93%, respectively, with an AUC of 0.94 (95% CI=0.92–0.96).
A recent study by Sarangi et al42 also reported significantly higher STA-PSV among patients with Graves’ disease than those with thyroiditis and established an optimal cut-off value of 54.3 cm/s for the mean STA-PSV with a sensitivity of 82.9% and a specificity of 86.2% in discriminating between Graves’ disease and thyroiditis. Furthermore, they concluded that values of the mean STA-PSV greater than 84.93 cm/s confirmed a 100% specificity for the diagnosis of Graves’ disease.42
The discrepant results in various studies may be attributable to numerous factors as the sample size, different ethnicity, varying modes of positioning of STA employed by the operator, or altering frequencies of ultrasound transducers.
Regarding the inferior thyroid artery, the PSV and EDV of both right and left inferior thyroid arteries and consequently the mean ITA-PSV and ITA-EDV were significantly higher in patients with Graves’ disease than in patients with thyroiditis, with p-values <0.001. The value of the mean ITA-PSV shown in the present study was 105.33±52.56 cm/s in the Graves’ disease group and this was almost comparable to the mean STA-PSV. A meta-analysis by Chiou et al31 similarly revealed a higher mean ITA-PSV value in hyperthyroid patients (41.8±21.3 cm/s compared to euthyroid patients (28.8±20 cm/s). A study by Malik et al43 also demonstrated higher mean PSV-ITA values in patients with Graves’s disease than those with thyroiditis (45.85±14.49 cm/s versus 15.83±8.15 cm/s, respectively, p<0.001). In literature, values of the mean ITA-PSV ranged widely from 42.1±14.6 cm/s to 186±38.7 cm/s, depending on the sites selected for thyroid artery sampling and factors such as racial differences, and this may, therefore, explain the higher values of ITA-PSV in Graves’ disease patients observed in our study compared to previous studies. Previous studies by Sundarram et al41 and Donkol et al1 were also consistent with the present study and demonstrated higher mean ITA-PSV in patients with Graves’ disease compared to destructive thyroiditis patients, however, no cut-off value for the mean ITA-PSV was reported by the former study.
The PSV and end diastolic velocities of the inferior thyroid artery showed a greater sensitivity and specificity compared with the superior thyroid arteries (mentioned earlier) in the present study, being 76.2% and 77.8%, respectively, for ITA-PSV with a cut-off value of 62.12 cm/s, and 78.6% and 77.8%, respectively, for the ITA-EDV with a cut-off value of 25.22 cm/s. This is an important finding because to the best of our knowledge this is the first study to compare the sensitivity and specificity and identify cut-off values for PSV and EDV of both the inferior and superior thyroid arteries concurrently. Although the superior thyroid artery is more superficially located, arising directly from the external carotid artery, it is thin and may be less notable when compared to the ITA and, hence, blood flow velocities may be better assessed using more advanced computer software and higher proficiency ultrasound equipment. The study by Donkol et al1 concluded that ITA blood flow velocity is an important parameter for discriminating between Graves’ disease and thyroiditis, with a sensitivity of 88.9% and a specificity of 87.5% for ITA-PSV (PPV of 94.1%; NPV of 77.8%; an 88.5% diagnostic accuracy) and a cut-off value of 40 cm/s.
Likewise, in a study by Bogazzi et al,10 the peak systolic, end diastolic, and mean velocities of inferior thyroid artery in patients with Graves’ disease were found to be significantly higher than patients with thyroiditis and established that a mean ITA-PSV cut-off value of 15±3 cm/s adequately diagnosed Graves’ disease. The study by Kumar et al4 conducted on 65 patients with thyrotoxicosis also demonstrated a significantly higher ITA blood flow in patients with Graves’ disease compared to those with destructive thyroiditis. Moreover, they revealed that color flow Doppler ultrasound carried a sensitivity of 96% and a specificity of 95% in distinguishing the causes of thyrotoxicosis. Another study identified a mean ITA-PSV cut-off value of 30 cm/s for differentiating between Graves’ disease and thyroiditis with a sensitivity of 91% and a specificity of 89% on ROC curve analysis.43
Several studies used other quantitative methods to assess thyroid blood flow using color pixel density (CPD) and volume flow rate (VFR) and observed that these parameters demonstrated a similar sensitivity but a lower specificity than the PSV in diagnosing Graves’ disease.21,24,44
An important finding in the present study was the significant correlation between thyroid scintigraphy uptake and the Color Doppler indices including the peak systolic and end-diastolic velocities of STA and ITA in patients with thyroiditis. This is in accordance with a study by Anjuman et al,45 which also confirmed a strong positive correlation between the peak systolic velocity of inferior thyroid artery on Color Doppler and radioactive iodine uptake in both 2 hours and 24 hours (r=0.330, p=0.003 and r=0.325, p=0.004, respectively). Considering radioactive iodine uptake as the gold standard for differentiating between Graves’ disease and subacute thyroiditis, the latter study concluded that PSV of ITA could be used as a better and more convenient alternative to scintigraphy, owing to its high sensitivity, specificity (93.7% and 83.3%, respectively), and diagnostic performance (89.7%).
Additionally, in agreement with our results, Zhao et al11 established a strong linear correlation between the mean PSV of superior thyroid artery on Color Doppler ultrasound and the 3 hours and 24 hours radioactive iodine uptake (r=0.458, p<0.001 and r=0.501, p<0.001, respectively) in patients with thyrotoxicosis and concluded that the STA-PSV is a more accurate, convenient, readily available alternative to radioactive iodine uptake (RAIU), with high reproducibility in distinguishing Graves’ disease from destructive thyroiditis.
The study by Malik et al43 also showed that 99mTC pertechnetate scanning exhibited a similar specificity and a positive predictive value (PPV) as ITA-PSV in differentiating between Graves’ disease and thyroiditis, although a greater sensitivity was encountered with scintigraphy (100% versus 91%, respectively). However, the latter study and a former study by Smith and Oates46 observed that some patients with resolving thyroiditis can display increased uptake on nuclear scanning that may be indicative of Graves’ disease and this can be potentially confusing. The latter study, thus, concluded that the mean ITA-PSV may be employed as an alternative whenever a contraindication to nuclear scanning is present, including recent iodine exposure, and additionally allows for prompt therapeutic decisions.
Previous studies have demonstrated a positive correlation between the mean PSV of the superior and inferior thyroid arteries and the mean TSH receptor antibodies (TRAb) titres. In the study by Zhao et al,11 ROC curve analysis revealed that the AUC for the mean STA-PSV (0.901; 95% CI=0.839–0.963) and the mean TRAb titres (0.902; 95% CI=0.839–0.964) was quite similar in differentiating between Graves’ disease and thyroiditis. Hiraiwa et al47 established a weak association between the peak systolic velocity of superior thyroid artery and TRAb levels and, hence, concluded that there are possibly additional unknown factors controlling the thyroid gland blood flow.
A study by Scappaticcio et al6 revealed that thyroid scintigraphy exhibited the best diagnostic accuracy in distinguishing Graves’ disease from other causes of thyrotoxicosis and that TRAb and TSI bioassays showed similar diagnostic efficacy with high sensitivity and specificity in detection of Graves’ disease. They also concluded that these assays could be used as an alternative, confining the use of scintigraphy to patients who are TRAb-negative. Moreover, the latter study6 demonstrated that thyroid ultrasound was less reliable when compared to scintigraphy and TRAb assays. A major limitation of this study, however, was that the thyroid vascularity was assessed by a qualitative method, thus underestimating the accuracy of Color Doppler ultrasound in discriminating between Graves’ disease and other causes of thyrotoxicosis.
Other studies have confirmed a high diagnostic accuracy of the TRAb levels in discriminating between the latter two conditions and showed a robust positive correlation between the mean TRAb levels and the mean ITA-PSV.42,48,49 In the current study, however, the TRAb levels were not measured owing to their high cost and financial constraints.
A recent study by Baek et al,50 employed three different Doppler techniques including Color Doppler, power Doppler, and microvascular ultrasonography (MVUS) to differentiate between Graves’ disease and thyroiditis and found them to have a comparable diagnostic accuracy with higher scores reported in patients with Graves’ than in destructive thyroiditis. In contrast to our study, they applied a semi-quantitative assessment of blood flow pattern using CD (vascularity score)51 rather than quantitative analysis of blood flow velocities, and this could explain why MVUS demonstrated a better diagnostic performance, as quantitative vascularity indices (VI) were automatically attained on MVUS images. The latter study also concluded that, although serum TSH-R-Ab assay correlated significantly with MVUS-VI, acquisition of assay results could take several days, hence limiting their use in clinical practice.
Conclusion
To the best of our knowledge this is the first study to compare and simultaneously assess the sensitivity and specificity of the mean PSV and EDV of both inferior and superior thyroid arteries and to identify cut-off values in discriminating between Graves’ disease and thyroiditis. No significant differences in the blood flow velocities were observed between the right and left thyroid arteries and, hence, Color flow Doppler ultrasound (CDU) parameters can be performed and assessed on either side. The peak diastolic and end diastolic velocities of the STA and ITA by CDU were significantly higher in patients with Graves’ diseases compared with thyroiditis, hence are effective, inexpensive parameters in differentiating between the two conditions and can be used as alternative tools whenever a contraindication to thyroid scintigraphy exists. ITA blood flow velocities showed a greater sensitivity and specificity when compared to the STA velocities in differentiating between Graves’ disease and thyroiditis, with a cut-off value of 62.12 cm/s for ITA-PSV and a cut-off value of 25.22 cm/s for ITA-EDV. However, further wide-scale studies with a greater number of patients, different ethnicity, and more advanced computer software and ultrasound equipment are required to validate the results of our study.
Data Sharing Statement
The dataset used during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Research Ethics Committee of Cairo University. An informed consent from the patients was attained before enrolment after explaining to them the value of the study.
This study complies with the Declaration of Helsinki.
Consent for Publication
All authors have read and approved the submission of the manuscript. An informed consent from the patients was attained before enrolment after explaining to them the value of the study.
Author Contributions
All authors certify that they:
- Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
- Have drafted or written, or substantially revised or critically reviewed the article.
- Have agreed to submit the article to International Journal of General Medicine.
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
- Agree to take responsibility and be accountable for the contents of the article.
Maha Assem Hussein participated in the conceptualization, study design, supervision, and writing of the manuscript; Alaa Abdel Hamid in the conceptualization, methodology and technique, acquisition, analysis and interpretation of the data; Rasha M. Abdel Samie in the study design, supervision, analysis and interpretation of the data, writing the manuscript, and is the corresponding author; Elshaymaa Hussein in the methodology and technique, analysis, and interpretation of the data; and Shereen Sadik Elsawy in the methodology, supervision, acquisition, analysis, and interpretation of the data.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
No conflict of interest to declare.
References
1. Donkol RH, Nada AM, Boughattas S. Role of color Doppler in differentiation of Graves’ disease and thyroiditis in thyrotoxicosis. World J Radiol. 2013;5(4):178–183. doi:10.4329/wjr.v5.i4.178
2. Amino N, Yabu Y, Miyai K. Differentiation of thyrotoxicosis induced by thyroid destruction from Graves’disease. Lancet. 1978;2:344–346. doi:10.1016/S0140-6736(78)92943-4
3. Lee JC. Thyroid scans. Aust Fam Physician. 2012;41(8):1–3.
4. Kumar KV, Pasupuleti V, Jayaraman M, Abhyuday V, Rayudu BR, Modi KD. Role of thyroid Doppler in differential diagnosis of thyrotoxicosis. Endocr Pract. 2009;15(1):6–9. doi:10.4158/EP.15.1.6
5. Kahaly GJ, Diana T, Kanitz M, Frommer L, Olivo PD. Prospective trial of functional thyrotropin receptor antibodies in Graves disease. J Clin Endocrinol Metab. 2020;105(4):e1006–14. doi:10.1210/clinem/dgz292
6. Scappaticcio L, Trimboli P, Keller F, Imperiali M, Piccardo A, Giovanella L. Diagnostic testing for Graves’ or non-Graves’ hyperthyroidism: a comparison of two thyrotropin receptor antibody immunoassays with thyroid scintigraphy and ultrasonography. Clin Endocrinol (Oxf). 2020;92(2):169–178. doi:10.1111/cen.14130
7. Jebreel AE, England J, Bedford K, Murphy J, Karsai L, Atkin S. Vascular endothelial growth factor (VEGF), VEGF receptors expression and microvascular density in benign and malignant thyroid diseases. Int J Exp Pathol. 2007;88(4):271–277. doi:10.1111/j.1365-2613.2007.00533.x
8. Wang JF, Milosveski V, Schramek C, Fong GH, Becks GP, Hill DJ. Presence and possible role of vascular endothelial growth factor in thyroid cell growth and function. J Endocrinol. 1998;157(1):5–12. doi:10.1677/joe.0.1570005
9. Ruchała M, Szczepanek E. Thyroid ultrasound—a piece of cake. Endokrynol Pol. 2010;61(3):330–445.
10. Bogazzi F, Bartalena L, Brogioni S, et al. Thyroid vascularity and blood flow are not dependent on serum thyroid hormone levels: studies in vivo by color flow Doppler sonography. Eur J Endocrinol. 1999;140:452–456. doi:10.1530/eje.0.1400452
11. Zhao X, Chen L, Li L, et al. Peak systolic velocity of superior thyroid artery for the differential diagnosis of thyrotoxicosis. PLoS One. 2012;7(11):e50051. doi:10.1371/journal.pone.0050051
12. Solivetti FM, Bacaro D, Cecconi P, Baldelli R, Marandino F. Small hyperechogenic nodules in thyroiditis: usefulness of cytological characterization. J Exp Clin Cancer Res. 2004;23(3):433–435.
13. Loy M, Perra E, Melis A, et al. Color-flow Doppler sonography in the differential diagnosis and management of amiodarone-induced thyrotoxicosis. Acta Radiol. 2007;48(6):628–634. doi:10.1080/02841850701342138
14. Markovic V, Eterovic D. Thyroid echogenicity predicts outcome of radioiodine therapy in patients with Graves’ disease. J Clin Endocrinol Metab. 2007;92(9):3547–3552. doi:10.1210/jc.2007-0879
15. Cappelli C, Castellano M, Pirola I, et al. The predictive value of ultrasound findings in the management of thyroid nodules. QJM. 2007;100(1):29–35. doi:10.1093/qjmed/hcl121
16. Alzahrani AS, Ceresini G, Aldasouqi SA. Role of ultrasonography in the differential diagnosis of thyrotoxicosis: a noninvasive, cost-effective, and widely available but underutilized diagnostic tool. Endocr Pract. 2012;18(4):567–578. doi:10.4158/EP11170.RA
17. Darvish L, Khezri M, Teshnizi SH, Roozbeh N, Dehkordi JG, Amraee A. Color Doppler ultrasonography diagnostic value in detection of malignant nodules in cysts with pathologically proven thyroid malignancy: a systematic review and meta-analysis. Clin Transl Oncol. 2019;21(12):1712–1729. doi:10.1007/s12094-019-02105-y
18. Yang GC, Fried KO. Most thyroid cancers detected by sonography lack intranodular vascularity on color Doppler imaging: review of the literature and sonographic-pathologic correlations for 698 thyroid neoplasms. J Ultrasound Med. 2017;36(1):89–94. doi:10.7863/ultra.16.03043
19. Chung J, Lee YJ, Choi YJ, et al.; Korean Society of Thyroid Radiology (KSThR), Korean Society of Radiology. Clinical applications of Doppler ultrasonography for thyroid disease: consensus statement by the Korean Society of Thyroid Radiology. Ultrasonography. 2020;39(4):315–330. doi:10.14366/usg.20072
20. Baek HJ, Kim DW, Lee YJ, Ahn HS, Ryu JH. Comparison of realtime and static ultrasonography diagnoses for detecting incidental diffuse thyroid disease: a multicenter study. Ultrasound Q. 2019;35(3):233–239. doi:10.1097/RUQ.0000000000000391
21. Kurita S, Sakurai M, Kita Y, et al. Measurement of thyroid blood flow area is useful for diagnosing the cause of thyrotoxicosis. Thyroid. 2005;15(11):1249–1252. doi:10.1089/thy.2005.15.1249
22. Chen L, Zhao X, Liu H, et al. Mean peak systolic velocity of the superior thyroid artery is correlated with radioactive iodine uptake in untreated thyrotoxicosis. J Int Med Res. 2012;40(2):640–647. doi:10.1177/147323001204000226
23. Vitti P, Rago T, Mazzeo S, et al. Thyroid blood flow evaluation by color-flow Doppler sonography distinguishes Graves’ disease from Hashimoto’s thyroiditis. J Endocrinol Invest. 1995;18(11):857–861. doi:10.1007/BF03349833
24. Ota H, Amino N, Morita S, et al. Quantitative measurement of thyroid blood flow for differentiation of painless thyroiditis from Graves’ Disease. Clin Endocrinol. 2007;67(1):41–45. doi:10.1111/j.1365-2265.2007.02832.x
25. Erdoğan MF, Anil C, Cesur M, Başkal N, Erdoğan G. Color flow Doppler sonography for the etiologic diagnosis of hyperthyroidism. Thyroid. 2007;17(3):223–228. doi:10.1089/thy.2006.0104
26. Ralls PW, Mayekawa DS, Lee KP, et al. Color-flow Doppler sonography in Graves’ disease: “thyroid inferno”. AJR Am J Roentgenol. 1988;150:781–784.
27. Uchida T, Takeno K, Goto M, et al. Superior thyroid artery mean peak systolic velocity for the diagnosis of thyrotoxicosis in Japanese patients. Endocr J. 2010;57(5):439–443. doi:10.1507/endocrj.K09E-263
28. Zuhur SS, Ozel A, Velet S, Bugdaci MS, Çil E, Altuntas Y. Is the measurement of inferior thyroid artery blood flow velocity by color-flow Doppler ultrasonography useful for differential diagnosis between gestational transient thyrotoxicosis and Graves’ disease? A prospective study. CLINICS. 2012;67(2):125–129. doi:10.6061/clinics/2012(02)06
29. Peng X, Wu S, Bie C, Tang H, Xiong Z, Tang S. Mean peak systolic velocity of superior thyroid artery for the differential diagnosis of thyrotoxicosis: a diagnostic meta-analysis. BMC Endocr Disord. 2019;19:56.
30. Caruso G, Attard M, Caronia A, et al. Color Doppler measurement of blood flow in the inferior thyroid artery in patients with autoimmune thyroid diseases. Eur J Radiol. 2000;36(1):5–10. doi:10.1016/S0720-048X(00)00147-9
31. Chiou S-C, Peng Y-S, Chen P-Y, et al. Color Doppler ultrasonography of inferior thyroid artery and its relation with thyroid functional state. J Med Ultrasound. 2006;14(3):51–57. doi:10.1016/S0929-6441(09)60091-6
32. Narouze S. Beware of the “serpentine” inferior thyroid artery while performing stellate ganglion block. Anesth Analg. 2009;109(1):289–290. doi:10.1213/ane.0b013e3181a20197
33. Varghese SS, Frankel SH. Numerical modeling of pulsatile turbulent flow in stenotic vessels. J Biomech Eng. 2003;125(4):445–460. doi:10.1115/1.1589774
34. Toni R, Della Casa C, Castorina S, et al. A meta-analysis of superior thyroid artery variations in different human groups and their clinical implications. Ann Anat. 2004;186(3):255–262. doi:10.1016/S0940-9602(04)80013-X
35. Association WM. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191. doi:10.1001/jama.2013.281053
36. Guidelines and Standards Committee of the Commission on Nuclear Medicine in collaboration with the SPR and SNM.ACR-SNM-SPR practice guideline for the performance of thyroid scintigraphy and uptake measurements. American College of Radiology, Society of Nuclear Medicine and Molecular Imaging, Society of Pediatric Radiology; 2009.
37. Ishay A, Pollak Y, Chervinsky L, Lavi I, Luboshitzky R. Color-flow Doppler sonography in patients with subclinical thyroid dysfunction. Endocr Pract. 2010;16(3):376–381. doi:10.4158/EP09218.OR
38. Ardakani AA, Bitarafan-Rajabi A, Mohammadi A, et al. CAD system based on B-mode and color Doppler sonographic features may predict if a thyroid nodule is hot or cold. Eur Radiol. 2019;29(8):4258–4265. doi:10.1007/s00330-018-5908-y
39. Bogazzi F, Vitti P. Could improved ultrasound and power Doppler replace thyroidal radioiodine uptake to assess thyroid disease? Nat Clin Pract Endocrinol Metab. 2008;4(2):70–71. doi:10.1038/ncpendmet0692
40. Höfling DB, Marui S, Buchpiguel CA, Cerri GG, Chammas MC. The end-diastolic velocity of thyroid arteries is strongly correlated with the peak systolic velocity and gland volume in patients with autoimmune thyroiditis. J Thyroid Res. 2017;2017:9. Article ID 1924974.
41. Sundarram KST, Sadacharan D, Ravikumar K, Kalpana S, Suresh RV. Role of color Doppler ultrasonography in differentiation of graves’ disease from thyroiditis. World J Endocr Surg. 2017;9(2):41–45. doi:10.5005/jp-journals-10002-1208
42. Sarangi PK, Parida S, Mangaraj S, Mohanty BK, Mohanty J, Sain BM. Diagnostic utility of mean peak systolic velocity of superior thyroid artery in differentiating Graves’ disease from thyroiditis. Indian J Radiol Imaging. 2021;31(02):311–317. doi:10.1055/s-0041-1734360
43. Malik SA, Choh NA, Misgar RA, et al. Comparison between peak systolic velocity of the inferior thyroid artery and technetium-99m pertechnetate thyroid uptake in differentiating Graves’ disease from thyroiditis. Arch Endocrinol Metab. 2019;63(5):495–500. doi:10.20945/2359-3997000000165
44. Saleh A, Cohnen M, Furst G, Godehardt E, Modder U, Feldkamp J. Differential diagnosis of hyperthyroidism: Doppler sonographic quantification of thyroid blood flow distinguishes between Graves’ disease and diffuse toxic goitre. Exp Clin Endocrinol Diabetes. 2002;110(1):32–36. doi:10.1055/s-2002-19992
45. Anjuman AA, Fariduddin M, Sharmin J, et al. Can color Doppler ultrasonography differentiate thyrotoxicoisis in graves’ disease from subacute thyroiditis? J Endocrinol Thyroid Res. 2017;2(5):555600.
46. Smith JR, Oates E. Radionuclide imaging of the thyroid gland: patterns, pearls and pitfalls. Clin Nucl Med. 2004;29(3):181–193. doi:10.1097/01.rlu.0000114530.12565.5b
47. Hiraiwa T, Tsujimoto N, Tanimoto K, Terasaki J, Amino N, Hanafusa T. Use of color Doppler ultrasonography to measure thyroid blood flow and differentiate Graves’ disease from painless thyroiditis. Eur Thyroid J. 2013;2(2):120–126. doi:10.1159/000350560
48. Ueda M, Inaba M, Kumeda Y, et al. The significance of thyroid blood flow at the inferior thyroid artery as a predictor for early Graves’ disease relapse. Clin Endocrinol (Oxf). 2005;63(6):657–662. doi:10.1111/j.1365-2265.2005.02397.x
49. Baldini M, Castagnone D, Rivolta R, Meroni L, Pappalettera M, Cantalamessa L. Thyroid vascularization by color Doppler ultrasonography in Graves’ disease. Changes related to different phases and to the long-term outcome of the disease. Thyroid. 1997;7(6):823–828. doi:10.1089/thy.1997.7.823
50. Baek H-S, Park J-Y, Jeong C-H, Ha J, Kang MI, Lim D-J. Usefulness of real-time quantitative microvascular ultrasonography for differentiation of Graves’ disease from destructive thyroiditis in thyrotoxic patients. Endocrinol Metab. 2022;37(2):323–332. doi:10.3803/EnM.2022.1413
51. Vita R, Di bari F, Perelli S, Capodicasa G, Benvenga S. Thyroid vascularization is an important ultrasonographic parameter in untreated Graves’ disease patients. J Clin Transl Endocrinol. 2019;15:65–69. doi:10.1016/j.jcte.2019.01.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.