Back to Journals » International Medical Case Reports Journal » Volume 19
Dupilumab for Atopic Dermatitis–Associated Nail Dystrophy: A Case Report
Authors Zhao Z, Li H, Luo D, Guan L, Yang F
Received 27 September 2025
Accepted for publication 28 January 2026
Published 20 February 2026 Volume 2026:19 568733
DOI https://doi.org/10.2147/IMCRJ.S568733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Zexin Zhao, Hongxia Li, Deping Luo, Liancheng Guan, Fan Yang
Department of Dermatology, The Second Affiliated Hospital, Guizhou University of Traditional Chinese Medicine, Guiyang, 550000, People’s Republic of China
Correspondence: Fan Yang, Department of Dermatology, The Second Affiliated Hospital, Guizhou University of Traditional Chinese Medicine, Guiyang, 550000, People’s Republic of China, Tel +86-137-6505-3270, Email [email protected]
Background: Nail dystrophy is a frequently overlooked manifestation of atopic dermatitis (AD). Although studies suggest a pooled prevalence of up to 11%, nail changes—particularly in the absence of active eczema—are often misdiagnosed as onychomycosis, leading to ineffective antifungal therapy. Evidence regarding targeted biologic treatment for this isolated phenotype remains scarce.
Case Presentation: We report a 57-year-old woman with a 10-year history of AD who developed progressive dystrophy of five fingernails over 2 years. She was repeatedly diagnosed with onychomycosis and treated with several courses of topical naftifine–ketoconazole and systemic itraconazole, without clinical benefit. Physical examination revealed markedly thickened, yellow–brown nail plates with periungual erythema and edema, but no active generalized eczema. Serial direct microscopy and fungal cultures after adequate antifungal washout were consistently negative, while total serum IgE was markedly elevated and a strong family history of atopy was present. After exclusion of other causes of nail dystrophy, a diagnosis of AD-associated nail dystrophy was established. Dupilumab was initiated with a 600 mg loading dose followed by 300 mg subcutaneously every 2 weeks, resulting in gradual improvement, complete resolution of periungual inflammation by week 12, and full nail plate reconstruction by week 28. At the 52-week follow-up, the nail plates remained largely normal with only mild roughness, without recurrence or new adverse events, while maintenance therapy with dupilumab was continued.
Conclusion: This case illustrates that AD-related nail dystrophy should be considered in patients with chronic nail changes, negative mycological studies, elevated total serum IgE, and a personal or family history of atopy. Dupilumab achieved complete and durable resolution of nail dystrophy in this patient, supporting IL-4/IL-13 pathway inhibition as a rational therapeutic option for this challenging phenotype of AD.
Keywords: dupilumab, atopic dermatitis, nail dystrophy, IL-4Rα, periungual inflammation, biologic therapy, Th2 inflammation
Introduction
Atopic dermatitis (AD) is a chronic, relapsing inflammatory dermatosis that affects adults worldwide and substantially impairs quality of life.1 Its pathogenesis reflects epidermal barrier dysfunction and type 2 immune activation, with IL-4/IL-13 signaling as a central driver.2,3 Although AD predominantly affects the skin, its clinical spectrum is heterogeneous and may include site-specific phenotypes such as chronic hand eczema and nail involvement.3
Nail changes are well recognized in psoriasis and alopecia areata, but they have received far less attention in AD and are likely underdiagnosed. Nail dystrophy in AD can present with thickening, discoloration, surface roughness, and periungual erythema or edema.4 In the absence of concurrent eczematous lesions, these findings may closely mimic onychomycosis, resulting in misdiagnosis and prolonged, ineffective antifungal therapy.
Dupilumab, a fully human monoclonal antibody that blocks signaling of IL-4 and IL-13 through binding to the IL-4 receptor alpha (IL-4Rα), has shown robust efficacy and a favorable safety profile in moderate-to-severe AD.5 However, data specifically addressing AD-related nail dystrophy are limited to small case series and individual reports. We describe a patient with long-standing AD who subsequently developed isolated nail dystrophy and experienced complete resolution after treatment with dupilumab, highlighting important diagnostic and therapeutic considerations.
Case Presentation
A 57-year-old woman with a 10-year history of AD presented with a 2-year history of progressive nail changes involving the left middle and ring fingers and the right thumb, middle, and ring fingers. She reported gradual nail thickening and deformation accompanied by periungual erythema and swelling, but denied pain, exudation, or systemic symptoms.
The patient’s AD had manifested 3 years prior to the onset of nail changes as generalized eczematous eruptions on the extremities, which completely resolved after treatment with systemic corticosteroids and topical emollients. Since then, only mild xerosis persisted. Her brother and son had allergic rhinitis, indicating a strong familial atopic background. Before presentation to our clinic, she had been clinically diagnosed with onychomycosis at several hospitals based on the morphological appearance, despite a negative result on fungal immunofluorescence microscopy. Consequently, an empirical antifungal regimen was initiated, consisting of topical naftifine–ketoconazole cream applied twice daily for 2 months combined with two courses of oral itraconazole pulse therapy (200 mg twice daily for 1 week per course, with a 3-week drug-free interval), which yielded no objective improvement after 1 month of therapy.
Clinical examination: On examination, the affected fingernails were markedly thickened with irregular rough surfaces and yellow–brown turbid discoloration. The nail plates were distorted but firmly attached to the nail beds. Diffuse periungual erythema and soft-tissue edema extended to the distal interphalangeal joints, without warmth, tenderness, or purulent discharge. No nail pitting, oil spots, or onycholysis suggestive of psoriasis were observed. The toenails and interdigital spaces were normal. Apart from generalized skin dryness with fine desquamation, no active eczematous lesions were noted. Baseline clinical photographs of the affected fingernails are shown in Figure 1.
 |
Figure 1 Baseline clinical presentation. Dorsal view of both hands showing marked nail dystrophy with rough surface texture and yellow–brown discoloration, accompanied by periungual erythema and swelling around the affected nails. |
Investigations: Initial potassium hydroxide (KOH) direct microscopy and fungal culture of nail clippings were negative. Because ongoing antifungal therapy might have contributed to false-negative results, all antifungal agents were discontinued for 1 month, during which only emollients were used. Repeat KOH examination and culture after this washout period again yielded negative findings.
Additional laboratory testing revealed a markedly elevated total serum IgE level of 1210 IU/mL (reference <100 IU/mL). Complete blood count, hepatic and renal function, electrolytes, and lipid profile were within normal ranges. Autoantibody screens showed no evidence of connective tissue disease. Serologic tests for hepatitis viruses and HIV were negative, and electrocardiography was unremarkable.
Diagnosis: Taking into account the patient’s chronic AD, strong familial atopy, markedly elevated serum IgE, and the absence of fungal organisms on repeated mycological examinations, AD-associated nail dystrophy was diagnosed. Other potential causes of nail dystrophy, including psoriasis, lichen planus, trauma, and connective tissue disease, were considered unlikely based on clinical and laboratory findings.
Treatment and Outcomes
Given the refractory nature of the condition, lack of response to appropriate antifungal therapy, and substantial impact on hand function and appearance, targeted biologic therapy was considered. After detailed discussion of potential benefits and risks, dupilumab was initiated with a 600 mg loading dose followed by 300 mg subcutaneous injections every 2 weeks in accordance with the approved regimen for adult AD.
Clinical Response Timeline
Baseline (Figure 1): Severe dystrophy of five fingernails was observed, characterized by rough surface texture, yellow–brown turbid discoloration, marked nail thickening, and periungual erythema and swelling.
Week 4: Periungual edema and erythema had clearly decreased, and the affected nails appeared slightly thinner.
Week 12 (Figure 2A–C): Periungual inflammation had almost completely resolved and finger edema had subsided, leaving only mild periungual erythema; the affected nail plates continued to thin and appeared less opaque.
 |
Figure 2 Week 12 of dupilumab therapy. (A) Dorsal view of both hands showing marked improvement in periungual erythema and swelling. (B) Close-up view demonstrating thinning of the affected nail plates and reduced opacity. (C) Close-up view of another affected hand showing similar improvement with only mild residual periungual erythema. |
Week 16 (Figure 3A–B): Periungual erythema had fully resolved, and newly grown proximal nail plates appeared smoother and more translucent.
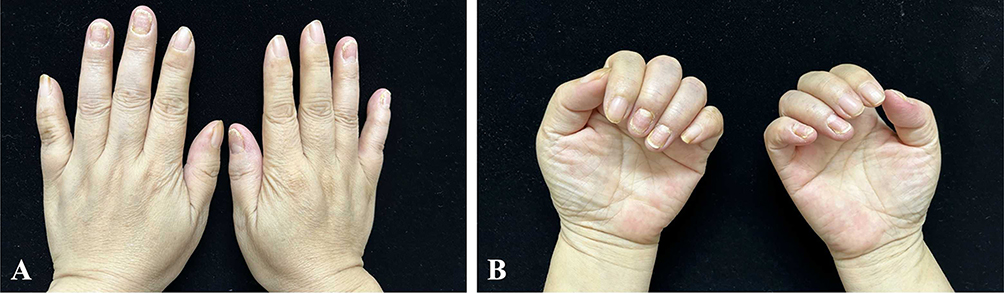 |
Figure 3 Week 16 of dupilumab therapy. (A) Representative view showing complete resolution of periungual erythema. (B) Close-up view showing smoother, more translucent newly grown proximal nail plates. |
Week 28 (Figure 4A–C): Complete nail plate reconstruction was achieved, with restoration of near-normal nail architecture, thickness, and color.
 |
Figure 4 Week 28 of dupilumab therapy. (A) Representative view showing substantial nail plate reconstruction. (B) Close-up view demonstrating restoration of near-normal nail thickness and color. (C) Additional view confirming recovery of nail plate architecture. |
Week 52 (Figure 5A–C): During maintenance dupilumab therapy, nail plate morphology remained largely normal; the left middle and ring fingernails and the right little fingernail showed only mild residual surface roughness, without recurrence of periungual inflammation. No new adverse events were reported at this visit.
 |
Figure 5 Week 52 of dupilumab therapy (maintenance phase). (A) Representative view showing largely normal nail plate morphology. (B) Close-up view of the left middle and ring fingernails showing mild residual surface roughness. (C) Close-up view of the right little fingernail showing mild residual surface roughness, without recurrence of periungual inflammation. |
The patient tolerated treatment well throughout the 52-week period and continues on regular dupilumab maintenance therapy with sustained clinical benefit.
Discussion
This case highlights the diagnostic challenge of distinguishing AD-related nail dystrophy from onychomycosis.4 Thickened, discolored nails with periungual inflammation are easily attributed to fungal infection, particularly when obvious eczematous lesions are absent. In our patient, repeated negative mycological examinations after an adequate antifungal washout period were pivotal in questioning the initial diagnosis and redirecting the diagnostic workup. Furthermore, the observed progressive decline in total serum IgE levels during dupilumab treatment—from 1210 IU/mL at baseline to 641 IU/mL at week 12, 480 IU/mL at week 28, and 336 IU/mL at week 52—provided objective laboratory corroboration for the suppression of underlying Th2 inflammation,2 paralleling the clinical improvement of the nail dystrophy.
The phenotypic presentation in our case—characterized by marked nail thickening, yellow–brown discoloration, and prominent periungual edema—diverges from the more common and often subtler nail changes in AD, such as pitting or superficial ridges.4 This pronounced dystrophy suggests a particularly intense and localized Th2-mediated inflammatory process within the nail apparatus. Furthermore, the parallel decline in serum IgE levels with clinical improvement underscores the role of systemic atopic diathesis. This case exemplifies the broad phenotypic spectrum of AD-related nail involvement and highlights how a Th2-dominant pathology can manifest as a clinical picture that closely mimics other disorders, such as onychomycosis.
The patient’s long-standing history of AD, markedly elevated serum IgE level, and strong family history of atopy supported the interpretation of the nail changes as part of the atopic disease spectrum rather than a primary fungal or autoimmune process. Similar to other AD manifestations, local Th2-driven inflammation in the nail matrix and periungual tissues may be sufficient to produce chronic nail dystrophy, even when generalized eczema is quiescent.2
Evidence on nail involvement in AD remains limited. Several studies have demonstrated substantial efficacy of dupilumab in chronic hand eczema, with improvement or resolution of concurrent nail changes in many patients.6 Individual case reports have described normalization of nail plates after several months of dupilumab therapy in patients with AD affecting the hands and nails.4,7,8 Our patient’s course, with gradual yet complete restoration of normal nail architecture over 28 weeks and sustained remission through 52 weeks, is consistent with these observations.4,7–9
The rapid improvement in periungual inflammation followed by slow but steady normalization of the nail plates suggests that IL-4/IL-13 blockade effectively suppresses local Th2-mediated inflammation while allowing physiological nail growth. The absence of systemic adverse events in our patient also reinforces the favorable safety profile of dupilumab in this context.5
The selection of dupilumab was guided by its targeted mechanism against the IL-4/IL-13 pathway, which is central to AD pathogenesis. While conventional systemic therapies, including disease-modifying antirheumatic drugs (DMARDs) such as methotrexate or cyclosporine, are established for moderate-to-severe generalized AD, their efficacy evidence primarily pertains to cutaneous lesions. Robust data supporting the use of DMARDs for isolated, refractory nail dystrophy—a less common and understudied manifestation—remain limited.4 In this context, dupilumab emerged as a rational therapeutic choice due to its high specificity for the implicated Th2 pathway and its well-established favorable safety profile.
From a practical perspective, clinicians should consider AD-associated nail dystrophy in adults presenting with chronic nail changes, negative mycological studies, elevated IgE, and a personal or family history of atopy. Early recognition may avoid unnecessary antifungal exposure and facilitate timely initiation of targeted biologic therapy for this underrecognized phenotype.
Conclusion
This case report demonstrates that dupilumab can induce complete and sustained resolution of AD-associated nail dystrophy in an adult patient with long-standing atopy and isolated nail involvement. Clinical and laboratory features, together with repeated negative mycological studies, were essential for establishing the diagnosis and selecting appropriate therapy. Further observational studies and prospective cohorts are needed to clarify the prevalence of nail involvement in AD, identify clinical or biologic markers that predict response to dupilumab, and determine the optimal treatment duration and follow-up strategies in this subgroup of patients.
Patient Perspective
“For two years my nails were thick, discolored, and embarrassing. I tried many antifungal treatments without change. After starting dupilumab, swelling subsided within weeks and my nails gradually returned to normal. By about six months I felt confident using my hands again.”
Reporting guideline: This case report is presented in accordance with the CAse REport (CARE) guidelines.10
Ethical Approval
This study was approved by the Ethics Committee of Guizhou University of Traditional Chinese Medicine (Approval No. Zw20240618).
Informed Consent
Written informed consent for publication of anonymized clinical information and images was obtained from the patient.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284–6. doi:10.1111/all.13401
2. Werfel T, Allam JP, Biedermann T, et al. Cellular and molecular immunologic mechanisms in atopic dermatitis. J Allergy Clin Immunol. 2016;138(2):336–349. doi:10.1016/j.jaci.2016.06.010
3. Cf S 4th, Billi AC, Maverakis E, et al. Novel insights into atopic dermatitis. J Allergy Clin Immunol. 2023;151(5):1145–1154. doi:10.1016/j.jaci.2022.10.023
4. Chng WQ, Yew YW. Nail manifestations in atopic dermatitis: a systematic review. Int J Dermatol. 2020;59(6):670–676. doi:10.1111/ijd.14726
5. Olbrich H, Sadik CD, Ludwig RJ, Thaçi D, Boch K. Dupilumab in inflammatory skin diseases: a systematic review. Biomolecules. 2023;13(4):634. doi:10.3390/biom13040634
6. Simpson EL, Thompson MM, Hanifin JM. Prevalence and morphology of hand eczema in patients with atopic dermatitis. Dermatitis. 2006;17(3):123–127. doi:10.2310/6620.2006.06005
7. Navarro-Triviño FJ, Vega-Castillo JJ, Ruiz-Villaverde R. Nail changes successfully treated with dupilumab in severe atopic dermatitis. Australas J Dermatol. 2021;62(3):e468–e469. doi:10.1111/ajd.13633
8. Li J, Zhang D, Dong S, et al. Dupilumab for atopic dermatitis with twenty-nail dystrophy: a case report. Clin Cosmet Invest Dermatol. 2025;18:1187–1190. doi:10.2147/CCID.S524384
9. Zubek AE, Vesely MD. Onychodystrophy associated with dupilumab therapy for atopic dermatitis. JAAD Case Rep. 2020;7:20–22. doi:10.1016/j.jdcr.2020.10.024
10. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D; CARE Group. The CARE guidelines: consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013;2013:bcr2013201554. doi:10.1136/bcr-2013-201554
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Burning and Scaling Probably Associated with Dupilumab Therapy: A Case Report
Luo N, Wang Q, Lei M, Li Z, Li T, Hao P
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1659-1662
Published Date: 17 August 2022
Dupilumab in the Treatment of Cheilitis in Atopic Dermatitis Patients
Shan J, Ali K, Da J, Li M, Qiu Y, Lou H, Wu L
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2437-2443
Published Date: 11 November 2022
Pustular Psoriasis in a Patient Treated with Dupilumab for Atopic Dermatitis: A Case Report
Liu L, Chen J, Tang K, Li F, Li S, Ding X
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2217-2221
Published Date: 14 August 2023
Perception and Experience of Dupilumab in Atopic Dermatitis: A Real-Life Study
Antoine L, Puzenat E, Popescu D, Charollais R, Dresco F, Dupond AS, Salard D, Drobacheff-Thiebaut MC, Zanella A, Ducournau A, Gallais-Serezal I, Aubin F
Patient Preference and Adherence 2023, 17:2289-2293
Published Date: 15 September 2023
Dupilumab for Atopic Dermatitis with Twenty-Nail Dystrophy: A Case Report
Li J, Zhang D, Dong S, Zhu L, Li X, Han Y
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1187-1190
Published Date: 15 May 2025