Back to Journals » Research and Reports in Urology » Volume 17
Dumbbell-Shaped Giant Vesical Calculus Extending into the Urethra in a Female
Authors Wen X ![]()
Received 14 May 2025
Accepted for publication 2 August 2025
Published 11 August 2025 Volume 2025:17 Pages 287—291
DOI https://doi.org/10.2147/RRU.S523179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Xin Wen
Urology Division, The Second Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China
Correspondence: Xin Wen, The Second Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, 563000, People’s Republic of China, Email [email protected]
Abstract: Bladder calculi occur predominantly in men, and their incidence is very low in females. Female urethral calculi are even rarer and are usually associated with anatomical or pathological abnormalities. This case report describes a female patient with a giant calculus extending from the urinary bladder into the urethra, crossing the bladder neck. The patient had a three-year history of lower urinary tract symptoms before diagnosis. She was presented with acute pyelonephritis on the left side, bilateral hydronephrosis due to reflux, and recurrent urinary tract infections. An emergency cystostomy was performed at our medical center for urinary drainage, followed by open cystolithotomy. Urethroscopy revealed a urethral diverticulum near the bladder neck; however, the patient declined diverticulum resection. A five-year follow-up was conducted. This case report provides valuable insights into diagnosing and treating rare lower urinary tract calculi in females, accompanied by a literature review.
Keywords: bladder calculi, urethral calculi, urethral diverticula, female
Introduction
Urolithiasis is a common disease worldwide, and its incidence continues to rise.1,2 In China, the incidence rates of bladder calculi and urethral calculi are approximately 3.2% and 0.5%, respectively. Bladder calculi in females are rare, while urethral calculi are even rarer.2 This report presents a case of a lower urinary tract stone in female, which extended across the bladder neck into the urethra. This case may serve as a reference for the treatment of similar diseases.
Case Presentation
A 21-years-old female presented with frequent and painful urination lasting three years. She was initially misdiagnosed as having urinary tract infection and treated with antibiotics at two rural hospitals, but symptoms recurred. The patient was admitted to our medical center on April 4, 2020, with fever (maximum temperature: 104℉). Ultrasonography of the urinary system revealed bilateral hydronephrosis, bilateral ureteral dilation, trabeculated bladder, and bladder stones. Abdominal computed tomography (CT) showed a bladder stone with bladder wall thickening, urethral stone, bilateral hydronephrosis, and endometrial thickening (Figure 1). Immediate urethral catheterization failed. Due to persistent high fever despite antibiotic therapy, emergency surgery was performed for urine drainage and symptom relief. Intraoperative cystoscopy confirmed that the urethral stone was fixed and could not be repositioned into the bladder (Figure 2). Therefore, an emergency cystostomy was performed. One week later, open cystolithotomy was conducted. The stone crossed the bladder neck, extending from the bladder into the urethra. The bladder neck opening was gently dilated, and the stone was slowly pulled back into the bladder and completely removed (Figure 3). There were differences between the two groups (Table 1). Significant edema prevented simultaneous removal of a urethral diverticulum located near the bladder neck at the 6 o’clock position. Multiple polypoid tissues were found in the stone retention area and collected for pathological examination. The bladder mucosa showed chronic inflammatory changes with the formation of brown nests, partial fragmentation, and calcified components. At discharge, the patient urinated normally. Follow-up examination revealed a diverticulum measuring 2.0 cm × 1.5 cm (Figure 4), and the polypoid tissue had disappeared. The patient refused surgical removal of the diverticulum. After urination, residual urine in the diverticulum was drained by urethral squeezing, without further flow from the urethral orifice. We recommended against vaginal delivery to prevent urethrovaginal fistula formation. During the five-year follow-up, the patient experienced mild stress incontinence and one missed abortion. Behavioral therapy was administered to manage mild stress incontinence.
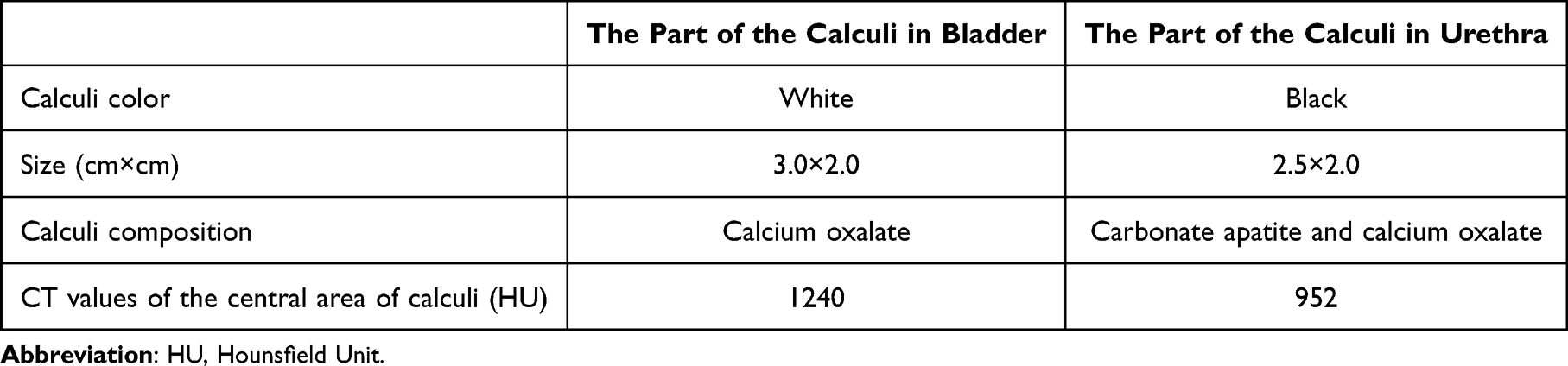 |
Table 1 Stone Test Results |
 |
Figure 1 (A) The arrow indicates bilateral hydronephrosis. (B) The arrow indicates the calculus crossing the bladder neck and extending into the urethra. |
 |
Figure 2 The arrow indicates the appearance of the calculus as observed through cystoscopy in the urethra. |
 |
Figure 3 The calculus after removal, with (A) located in the bladder and (B) in the urethra. |
 |
Figure 4 Postoperative follow-up. (A) Bladder neck opening. (B) Urethral diverticulum. |
Discussion
Lower urinary tract calculi commonly occur in males, but bladder calculi are rare in females, and urethral calculi are even rarer.3 Female calculi often develop secondary to retained upper urinary tract stones. Primary calculi typically result from pathological or anatomical abnormalities, such as infection and diverticulum in the bladder or urethra.4 In this case, the misdiagnosis may have resulted from limited clinical experience and inadequate diagnostic resources. Stones in the bladder had higher density and CT values (Table 1), suggesting earlier formation. The calculus traversed the bladder neck, grew into the urethra, and caused obstruction of the lower urinary tract. Consequently, urinary retention, bilateral hydronephrosis, secondary infections, and acute pyelonephritis of the left kidney occurred. As the urethral calculus grew, it compressed the urethra and led to urethral diverticulum formation, making the case even rarer.
The bladder calculus was composed of calcium oxalate, while the urethral calculus contained carbonate apatite and calcium oxalate (Table 1). Previous studies indicate calcium oxalate is a major component of bladder stones. The formation of carbonate apatite is associated with urinary tract infections.5 Therefore, calculus formation in this patient was likely related to dietary habits and chronic urinary tract infections.
Typically, urethral calculi are pushed back into the bladder and treated transurethrally like bladder stones.3,6 However, in this patient, the calculus was fixed and could not be repositioned into the bladder. Furthermore, the limited space of the female urethra made lithotripsy difficult, potentially causing tissue injury with low effectiveness.7 Therefore, an emergency cystostomy was performed to drain urine and relieve symptoms. Subsequently, open cystolithotomy was performed to avoid urethral and sphincter damage.3,6 The patient experienced mild stress incontinence, possibly related to multiple pregnancies and uterine curettages.8 Behavioral therapy, such as Kegel exercises, was recommended. During the five-year follow-up, the patient’s urinary incontinence symptoms improved significantly.
In this case, the bladder mucosa exhibited chronic inflammatory changes with Brunn nest formation. Brunn nests occur when transitional epithelium is exposed to chronic irritation and are commonly observed in glandular cystitis.9 After stone removal, follow-up examination showed the bladder mucosa became smooth.
Periurethral fascia protrusion can lead to urethral diverticula formation.10 In this patient, the diverticulum likely developed due to the growing calculus compressing the urethra. Because of severe local edema, the diverticulum was not removed concurrently. Three months postoperatively, the diverticulum remained, with residual urine draining upon urethral squeezing after urination.
This report aims to provide a reference for similar cases.
Consent
The study complies with the Declaration of Helsinki. Publication of this case has obtained patient consent. The manuscript contains no identifying information, the case details and accompanying images have been approved by the patient. Ethical clearance from the Second Affiliated Hospital of Zunyi Medical University.
Funding
This work was supported by The Science and Technology Department of Zunyi city (Grant Number: HZ2025139).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Knoll T. Epidemiology, pathogenesis, and pathophysiology of urolithiasis. Eur Urol Suppl. 2010;9(12):802–806. doi:10.1016/j.eursup.2010.11.006
2. Tan S, Yuan D, Su H, et al. Prevalence of urolithiasis in China: a systematic review and meta-analysis. BJU Int. 2024;133(1):34–43. doi:10.1111/bju.16179
3. Leslie SW, Sajjad H, Murphy PB. Bladder Stones. StatPearls; 2023.
4. Morton A, Tariq A, Dunglison N, Esler R, Roberts MJ. Etiology and management of urethral calculi: a systematic review of contemporary series. Asian J Urol. 2024;11(1):10–18. doi:10.1016/j.ajur.2021.12.011
5. Carpentier X, Daudon M, Traxer O, et al. Relationships between carbonation rate of carbapatite and morphologic characteristics of calcium phosphate stones and etiology. Urology. 2009;73(5):968–975. doi:10.1016/j.urology.2008.12.049
6. Hu J, Phan AT, Craig D. A rare case of a giant bladder stone associated with post-obstructive renal failure managed by open cystolithotomy. Cureus. 2023;15(5):e39718. doi:10.7759/cureus.39718
7. Naqvi SAA, Khaliq M, Zafar MN, Rizvi SAH. Treatment of ureteric stones. Comparison of laser and pneumatic lithotripsy. Br J Urol. 2010;74(6):694–698. doi:10.1111/j.1464-410X.1994.tb07108.x
8. Gao L, Wang S, Zhang D, et al. Pelvic floor muscle strength in the first trimester of primipara: across-sectional study. Int J Environ Res Public Health. 2022;19(6):3568. doi:10.3390/ijerph19063568
9. Gupta S, Adiga KP, Raj KK, Bhat N. A case report of usual presentation of unusual bladder mass-polypoid cystitis in a young Indian female. Int J Surg Case Rep. 2024;125:110640. doi:10.1016/j.ijscr.2024.110640
10. El-Nashar SA, Bacon MM, Kim-Fine S, et al. Incidence of female urethral diverticulum: a population-based analysis and literature review. Int Urogynecol J. 2014;25(1):73–79. doi:10.1007/s00192-013-2155-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.