Back to Journals » International Journal of General Medicine » Volume 15
Drug-Resistant Aerobic Bacterial Pathogens in Patients with Crocodile Bite Wounds Attending at Arba Minch General Hospital, Southern Ethiopia
Authors Alelign D ![]() , Tena T, Tessema M, Kidanewold A
, Tena T, Tessema M, Kidanewold A
Received 7 November 2022
Accepted for publication 15 December 2022
Published 19 December 2022 Volume 2022:15 Pages 8669—8676
DOI https://doi.org/10.2147/IJGM.S395046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Dagninet Alelign,1 Teshome Tena,2 Moges Tessema,2 Aschalew Kidanewold1
1Department of Medical Laboratory Science, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 2School of Medicine, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Dagninet Alelign, Tel +251-964-428-118, Email [email protected]
Background: A polymicrobial infection containing a diverse range of drug-resistant bacteria worsens the success of treatment for crocodile bite wound infection. However, there is a dearth of data in Ethiopia, where crocodile bite injuries are relatively common, particularly in the area around Lake Abaya and Lake Chamo in southern Ethiopia.
Methods: A hospital-based cross-sectional study was conducted from May 1st, 2021, to April 30th, 2022, at Arba Minch General Hospital. Eleven consenting patients with crocodile bite wounds were enrolled in this study. Wound swabs were collected aseptically following microbiological procedures. The diversity and type of aerobic bacterial pathogens, and drug-resistant patterns were used to determine and characterize the nature of crocodile bite wound infections.
Results: Among 11 patients with crocodile bite wounds, 72.7% (8/11) of wound samples were found to be culture-positive, with a total of 21 aerobic bacterial isolates. Gram-negative bacterial isolates were found in 57.1% (12/21). Triple-bacterial isolates were found in 62.5% (5/8) of wound samples, followed by 37.5% (3/8) of double bacterial isolates. Pseudomonas aeruginosa (n = 5), followed by Citrobacter spp. (n = 4), and coagulase-negative Staphylococci (CoNS) (n = 4) were frequently isolated bacteria. Methicillin resistance (MR-CoNS) was found in 75% of isolated CoNS. 6.7% of the isolated Enterococcus faecalis was vancomycin-resistant (VRE), while 60% of the isolated P. aeruginosa were piperacillin-resistant. Overall, 85.7% (18/21) of the isolates were found to be multidrug-resistant (MDR), with 55.6% (10/18) of them being Gram-negative MDR bacterial isolates.
Conclusion: Numerous aerobic bacteria that are resistant to the majority of common antibiotics have been associated with infections in crocodile bite wounds. Thus, the key to providing empirical therapy for such wounds is detecting the drug-resistant pattern of bacterial isolates.
Keywords: aerobic bacteria, crocodile bite, wound infection, Arba Minch, Ethiopia
Introduction
Crocodiles are the largest true carnivore reptiles in the world, and they have a fascinating nature and exert the most powerful bite of any creature.1,2 Depending on their body size and jaw length, their bite force has been confirmed at 3700 pounds per square inch.3,4 Attacks by crocodilians cause reflexive fear in humans; however, the event is uncommon.2 People who are swimming, irrigating, or fishing close to the water are at risk of being bitten by a crocodile.1,5–7
Crocodile bite injuries are becoming more frequent across the African continent. African Nile crocodile attacks range from 65 to 91% due to their widespread geographic distribution in Africa and the reliance of adjacent communities on the same water source.8,9 About 70% of those who have been bitten by a crocodile subsequently require an amputation due to the disfigurement and long-lasting impairment.8–10 These patients also often need reconstructive surgery.10–12 Failure to adequately clean bite wounds, along with delayed medical care, often leads to infection.13–16 The severe soft tissue infection associated with the unusual normal oral flora of the crocodile creates a challenging problem in the treatment of crocodile bite wounds.9,13 Despite the fact that the microbiology of infected crocodile bite wounds originates from crocodile mouths, the oral flora of crocodiles might be affected by the flora of other animals they eat or by the quality of the water in which they live. Furthermore, the bacteria could be on the patients’ skin when the skin’s natural barrier breaks.2,9,10,14
Crocodile bite wounds typically have a polymicrobial infection containing a diverse range of aerobic and anaerobic microbes; however, the type of bacterial isolates varied depending on the nature of the wound.9,14 The victim’s tissues will also deteriorate if the infection is not treated, and an amputation may be required.8,9 Additionally, infections have the capacity to propagate via the circulatory system throughout the body, resulting in the failure of multiple organs and ultimately fatality.6,9–16
Moreover, the crocodile-sourced bacteria that infect wounds are reported to be multi-drug resistant (MDR).9,17,18 This may be due to the significant increase in bacteria that are resistant to antibiotics as a result of the widespread use of antibiotics in aquatic environments.19–21 Furthermore, in developing countries like Ethiopia, the discharge of hospital septic system wastes carrying both antibiotics and antibiotic-resistant bacteria to aquatic environments has the potential of contaminating the aquatic ecosystem with antibiotic-resistant microorganisms.19,21 Though crocodile bites are frequent among persons who labor near Lake Abaya and Lake Chamo, Arba Minch, southern Ethiopia, there is a dearth of such data in Ethiopia generally and in the research region in particular. Hence, the present study aimed to assess drug-resistant bacterial pathogens in patients with crocodile bite wounds attending Arba Minch General Hospital in Southern Ethiopia.
Materials and Methods
Study Design, Period, Setting, Population, and Sample Collection Procedures
A hospital-based cross-sectional study design was conducted at the Arba Minch General Hospital orthopedic ward from May 1st, 2021 through April 30th, 2022. All out patients with crocodile bite wounds attending the orthopedic ward of the hospital during the study period were included consecutively. The fracture wound grading system developed by Gustilo and Anderson was used to categorize the types of wounds.22 Wound swab samples were aseptically obtained from the wounds of willing patients for microbiological examination. Rotating a sterile cotton-tipped applicator deeply into the wounds with adequate pressure to discharge fluid from the wound tissue and to prevent contamination on the surface of the wounds was how the wound swab samples were collected. To improve the likelihood of finding bacterial infections and obtain enough samples, multiple (two to three) wound swabs were obtained with the same technique from each site at one point in time. The samples were then processed an hour after collection in a sterile test tube with 1–2 mL of nutritional broth or Amies transport medium (Oxoid Ltd., UK).23
Isolation and Identification of Bacterial Isolates
Standard microbiological procedures were used to inoculate samples onto 5% sheep Blood Agar Medium (HiMedia Pvt. Ltd.), Chocolate Agar (HiMedia Pvt. Ltd.), Mannitol Salt Agar (HiMedia Pvt. Ltd.), MacConkey Agar (HiMedia Pvt. Ltd.), and Bile Esculin Agar (HiMedia Laboratory Pvt. Ltd., Mumbai, India). The plates were aerobically incubated at 37°C for 24–72 hours, with the inoculated chocolate agar incubated in a candle jar for 72 hours at 35–37°C to provide a 5–10% CO2 concentration. Following a gram stain on each positive culture medium, morphologically identical 3–5 pure colonies of bacteria from overnight incubated agar media were suspended in nutrient broth using sterile wire loop with reference to 0.5 McFarland standards and incubated for up to 4 hours at 37 °C for further processing. Biochemical tests (HiMedia Laboratory Pvt. Ltd., Mumbai, India) like the indole test, methyl red/Voges Proskauer test, coagulase test, oxidase test, triple sugar iron, motility, citrate utilization, urease, gas production, and hydrogen sulfide production were done for Gram-negative bacteria species identification, while catalase and coagulase tests were used for Gram-positive bacteria species identification.23,24
Antibiotic Susceptibility Testing
Antibiotic susceptibility patterns of bacterial isolates were done on Mueller Hinton Agar (HiMedia Pvt. Ltd.) by the Kirby-Bauer disk diffusion method 25 using the following antibiotics (Oxoid Ltd., Basingstoke, Hampshire, UK):26 For Gram-positive bacteria; penicillin (10 μg), cefoxitin (30 μg), gentamicin (10 μg), erythromycin (15 μg), tetracycline (30 μg), doxycycline (30 μg), clindamycin (10 μg), cotrimoxazole (25 μg), vancomycin (30 μg), and chloramphenicol (30 μg) were used, while ampicillin (10 μg), piperacillin (100 μg), amoxycillin-clavulanic acid (30 µg, BD), cefepime (30 μg), cefoxitin (30 μg), ceftriaxone (5 μg), cefuroxime (5 μg), ceftazidime (30 μg), gentamicin (10 μg), meropenem (10 μg), tetracycline (30 μg), doxycycline (30 μg), ciprofloxacin (5 μg), and chloramphenicol (30 μg) antibiotics were used for Gram-negative isolates. Then, after overnight incubation at 37°C, the diameter of the zone of inhibition was measured by millimetres and interpreted as sensitive, intermediate, or resistant according to the CLSI 2020 guidelines.26 Multidrug-resistant (MDR) is defined as isolates that resist at least one antimicrobial drug in three or more antimicrobial categories.
Data Quality Management
Data quality was assured by strictly following standard operating procedures (SOPs), training sample collectors as needed, and closely observing their development. The sterility of the culture media was verified by overnight storage of 5% of the prepared culture media at 35–37 °C. The medium batches that showed positive growth were discarded. To evaluate the effectiveness of the produced media and antibiotic discs, Escherichia coli ATCC 25922, Staphylococcus aureus ATCC 25923, and Enterococcus faecalis ATCC 29212 were utilized.23,26
Data Analysis
The Statistical Package for Social Sciences (SPSS) Version 22 was used to calculate descriptive statistics such as frequency, mean, and percentage.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board of Arba Minch University, College of Medicine and Health Sciences (Ref. No. IRB/1021/22). In addition, a formal authorization letter from the hospital was received. Each study subject gave their written informed consent before to the interview in accordance with the Helsinki Declaration. Orthopedic doctors received notice of significant test findings together with the patient’s card number.
Results
Bacterial Profile of Crocodile Bite Wounds
Of the 11 patients with crocodile bite wounds recruited in this study, the bacteriological analysis showed that 72.7% (8/11) of wound samples were found to be culture-positive, with a total of 21 total aerobic bacterial isolates grouped under eight distinct genera. Gram-negative and Gram-positive bacterial isolates constituted 57.1% (12/21) and 42.9% (9/21) of the total. Pseudomonas aeruginosa, Citrobacter spp., coagulase-negative Staphylococci (CoNS), and Enterococcus faecalis were the four most predominant isolates (Figure 1).
 |
Figure 1 Frequency of Bacterial Isolates in Patients with Crocodile Bite Wounds at Arba Minch General Hospital, Southern Ethiopia. |
There were no wound infections caused by a single aerobic bacterial isolate; rather, 62.5% (5/8) of wound infections were caused by triple bacterial isolates, followed by 37.5% (3/8) of double bacterial isolates. 37.5% (3/8) of the polymicrobial infections were caused by P. aeruginosa, Citrobacter spp., and CoNS (Table 1).
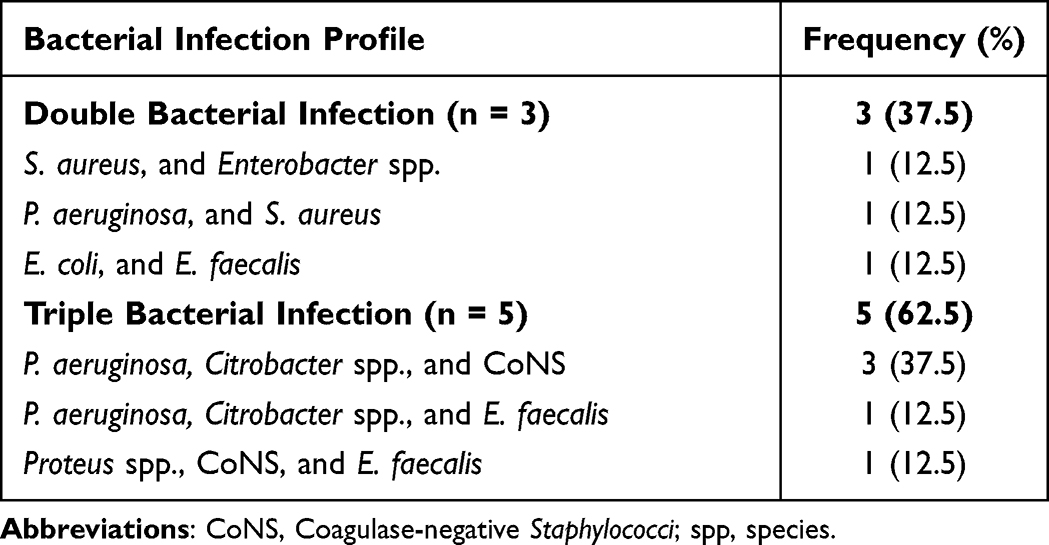 |
Table 1 Profile of Bacterial Infections (n = 8) in Patients with Crocodile Bite Wounds at Arba Minch General Hospital, Southern Ethiopia |
Antimicrobial Resistance Patterns of Bacterial Isolates
About 83.3% of Gram-negative bacterial isolates were resistant to ciprofloxacin, whereas 50% of isolated Gram-negative bacterial isolates were found to be resistant to ampicillin, tetracycline, and doxycycline. Furthermore, the most common isolates of P. aeruginosa demonstrated 80% resistance to ceftazidime and ciprofloxacin, as well as 60% resistance to piperacillin (Table 2).
 |
Table 2 Antimicrobial-Resistant Pattern of Gram-Negative Bacterial Isolates from Patients with Crocodile Bite Wounds at Arba Minch General Hospital, Southern Ethiopia |
Gram-positive bacterial isolates were found to be 88.9% resistant to penicillin and tetracycline, while 77.8% of isolates were resistant to doxycycline and chloramphenicol. About 75% of isolated CoNS were methicillin-resistant (MR-CoNS), while one isolate of S. aureus was methicillin-resistant (MRSA). Similarly, two-thirds of isolated E. faecalis were found to be resistant to vancomycin (VRE) (Table 3).
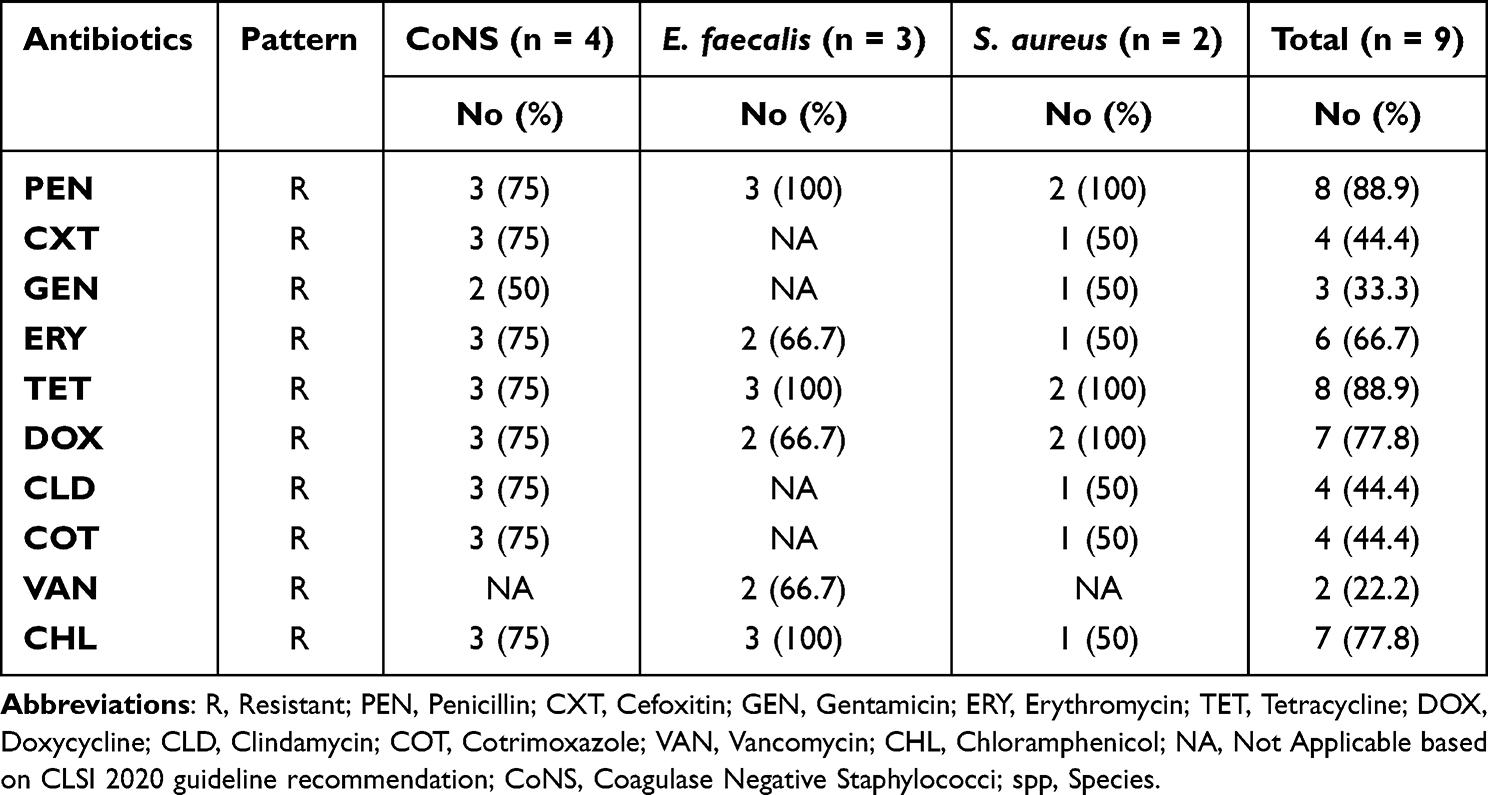 |
Table 3 Antimicrobial-Resistant Pattern of Gram-Positive Bacterial Isolates from Patients with Crocodile Bite Wounds at Arba Minch General Hospital, Southern Ethiopia |
Multidrug-Resistant Patterns of Bacterial Isolates
Among the overall bacterial isolates, 85.7% (18/21) were multidrug-resistant (MDR). 83.3% (10/12) and 88.9% (8/9) of isolated Gram-negative and Gram-positive bacteria were found to be MDR, respectively. One hundred percent of isolated E. faecalis and S. aureus were MDR, while 80% of isolated P. aeruginosa and 75% of Citrobacter spp. and CoNS were found to be MDR (Table 4).
 |
Table 4 Multidrug Resistance Pattern of Bacterial Isolates from Patients with Crocodile Bite Wounds at Arba Minch General Hospital, Southern Ethiopia |
Discussion
The prevalence of aerobic bacterial isolates from crocodile bite wounds overall in this study was 72.7% (95% CI: 45.5–90.9). The diversity of aerobic bacterial isolates (P. aeruginosa, Citrobacter spp., Enterobacter spp., E. coli, Proteus spp., and CoNS, E. faecalis, and S. aureus) observed in the present study was in consistent with the previous studies conducted in Malawi,9 California,14 Australia,15 and Tanzania.10 The majority of Gram-negative bacilli were isolated; this may indicate that the source of the infection is crocodile oral flora, which may originate from the intestinal flora of the other species that crocodiles consume, or it may indicate that faecal contamination of the wound is the result of poor personal hygiene.9,14
In this study, a wound infection caused by a single aerobic bacterial isolate was not identified. Rather, polymicrobial infections were observed with 62.5% of triple bacterial isolates and 37.5% of double bacterial isolates, of which 37.5% of the polymicrobial infections were caused by P. aeruginosa, Citrobacter spp., and CoNS, which is in line with the finding of previous studies.9,10,14,15 The combination of recipient skin flora, ambient organisms, and animal oral flora may be the cause of the wound’s polymicrobial character.9,14,16
In this study, ciprofloxacin resistance was found in 83.3% of isolated Gram-negative bacterial isolates. The predominant isolate, P. aeruginosa, showed more than 60% resistance to the tested antibiotics. Specifically, P. aeruginosa isolates showed high resistance to ceftazidime (80%), ciprofloxacin (80%), and piperacillin (60%), whereas the second predominant Citrobacter spp. isolates showed 75% resistance to ampicillin, cefuroxime, tetracycline, doxycycline, and ciprofloxacin. Likewise, more than 66.7% of isolated Gram-positive bacteria were found to be resistant to penicillin, tetracycline, doxycycline, chloramphenicol, and erythromycin. Moreover, penicillin and tetracycline resistance was identified in 88.9% of isolated Gram-positive bacteria. More than 50% of isolated CoNS and S. aureus and 66.7% of isolated E. faecalis were found to be resistant to all the antibiotics tested. Furthermore, 75% and 50% of isolated CoNS and S. aureus were methicillin-resistant, whereas vancomycin resistance was found in 66.7% of isolated E. faecalis (VRE). The reason for the variations in drug resistance patterns across bacterial isolates may be related to the source and drug-resistant ability of the isolates, or it may be related to their previous drug exposure.
The overall multidrug-resistant levels of bacterial isolates in this study were 85.7% (18/21), where Gram-negative and Gram-positive bacteria accounted for 55.6% and 44.4% of MDR, respectively. The predominate isolates P. aeruginosa (80%), Citrobacter spp. (75%), CoNS (75%) and E. faecalis (100%) were found to be MDR, which is in agreement with previous studies.9,14 This high prevalence of MDR bacteria could be due to the widespread use of antibiotics in aquatic environments or the extensive hospital septic system waste discharge, which introduces both antibiotic- and antibiotic-resistant bacteria to aquatic habitats.27,28
Limitation of the Study
The limitations of the present study include the cross-sectional study design with a small sample size in a hospital-based study, and it is difficult to determine where the isolated bacteria came from because the study only used a patient wound sample and conventional culture techniques. Studies on strictly anaerobic bacteria and fungi are completely confined due to funding and laboratory setup restrictions and no experiments to calculate the antimicrobial MIC were carried out. Additionally, this study did not take the patients’ prognoses into account.
Conclusion
In this study, significant numbers of aerobic polybacterial isolates were identified in crocodile bite wounds, and the most frequent isolated bacteria were P. aeruginosa, Citrobacter spp., and CoNS. Antibiotics that are often provided to patients have greater rates of resistance in the majority of bacterial isolates. The overall MDR among isolates was 85.7%, particularly with 75% of MR-CoNS, 50% of MRSA, 66.7% of VRE, and 60% of piperacillin resistance in P. aeruginosa. Therefore, the results of culture and sensitivity testing should be used to guide the treatment of crocodile bite wounds, and precautions should be taken to limit the emergence and spread of MDR bacteria, especially in aquatic settings. Finally, more thorough research about the molecular characterization and origin of bacterial isolates, including fungal agents, is necessary.
Data Sharing Statement
The primary author must be contacted with a valid request in order to provide the data sets used in this study.
Acknowledgment
We thank the medical staff at Arba Minch General Hospital for their assistance in gathering data, as well as the Arba Minch University Research Directorate Office for their material and financial support. Finally, we would like to express our gratitude to the study participants for their permission to participate.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the Arba Minch University College of Medicine and Health Sciences.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ryan C. Saltwater crocodiles as tourist attractions. J Sustain Tour. 1998;6(4):314–327. doi:10.1080/09669589808667319
2. Caldicott DG, Croser D, Manolis C, Webb G, Britton A. Crocodile attack in Australia: an analysis of its incidence and review of the pathology and management of crocodilian attacks in general. Wilderness Environ Med. 2005;16(3):143–159. doi:10.1580/1080-6032(2005)16[143:CAIAAA]2.0.CO;2
3. Saber AS, Hassanin A. Some morphological studies on the jaw joint of the Australian saltwater crocodile (Crocodylus porosus). J Vet Anat. 2014;7(2):55–74. doi:10.21608/jva.2014.44742
4. Erickson GM, Lappin AK, Vliet KA. The ontogeny of bite-force performance in American alligator (Alligator mississippiensis). J Zool. 2003;260(3):317–327. doi:10.1017/S0952836903003819
5. Gani MI, Hassan R, Tisen OB, Ahmad R. Human-crocodile conflicts in Sarawak, Malaysian Borneo: an analysis of crocodile attacks from 2000 until; 2020.
6. Fukuda Y, Manolis C, Appel K. Featured article: management of human‐crocodile conflict in the Northern Territory, Australia: review of crocodile attacks and removal of problem crocodiles. J Wildl Manage. 2014;78(7):1239–1249. doi:10.1002/jwmg.767
7. Mekisic AP, Wardill JR. Crocodile attacks in the Northern Territory of Australia. Med J Aust. 1992;157(11):751–754. doi:10.5694/j.1326-5377.1992.tb141275.x
8. Venter M, Kelly A, Boffard K, Pretorius R, Younus A. African Nile crocodile bite of the forearm: a case report. East Afr Orthop. 2020;14(2):102–107.
9. Wamisho BL, Bates J, Tompkins M, et al. Ward round-crocodile bites in Malawi: microbiology and surgical management. Malawi Medical Journal. 2009;21(1):29–31. doi:10.4314/mmj.v21i1.10986
10. Chalya PL, Mchembe M, Gilyoma JM, Mabula JB, Chandika AB, Mshana SE. Bite injuries at Bugando Medical Centre, Mwanza, Tanzania: a five year experience. East Cent Afr J Surg. 2011;16:1.
11. Weber DJ, Hansen AR. Infections resulting from animal bites. Infect Dis Clin North Am. 1991;5(3):663–680. doi:10.1016/S0891-5520(20)30413-X
12. Vanwersch K. Crocodile bite injury in southern Malawi. Trop Doct. 1998;28(4):221–222. doi:10.1177/004947559802800411
13. Noon Burg GE. Management of extremity trauma and related infections occurring in the aquatic environment. JAAOS. 2005;13(4):243–253. doi:10.5435/00124635-200507000-00004
14. Abrahamian FM, Goldstein EJ. Microbiology of animal bite wound infections. Clin Microbiol Rev. 2011;24(2):231–246.
15. Gruen RL. Crocodile attacks in Australia: challenges for injury prevention and trauma care. World J Surg. 2009;33(8):1554–1561. doi:10.1007/s00268-009-0103-6
16. Thomas N, Brook I. Animal bite-associated infections: microbiology and treatment. Expert Rev Anti Infect Ther. 2011;9(2):215–226. doi:10.1586/eri.10.162
17. Brook I. Microbiology and management of human and animal bite wound infections. Primary Care. 2003;30(1):25–39. doi:10.1016/S0095-4543(02)00056-8
18. Costanzo SD, Murby J, Bates J. Ecosystem response to antibiotics entering the aquatic environment. Mar Pollut Bull. 2005;51(1–4):218–223. doi:10.1016/j.marpolbul.2004.10.038
19. Baquero F, Martínez JL, Cantón R. Antibiotics and antibiotic resistance in water environments. Curr Opin Biotechnol. 2008;19(3):260–265. doi:10.1016/j.copbio.2008.05.006
20. Carvalho IT, Santos L. Antibiotics in the aquatic environments: a review of the European scenario. Environ Int. 2016;94:736–757. doi:10.1016/j.envint.2016.06.025
21. Serwecińska L. Antimicrobials and antibiotic-resistant bacteria: a risk to the environment and to public health. Water. 2020;12(12):3313. doi:10.3390/w12123313
22. Abraham Y, Wamisho BL. Microbial susceptibility of bacteria isolated from open fracture wounds presenting to the err of black-lion hospital, Addis Ababa University, Ethiopia. Afr J Microbiol Res. 2009;3(12):939–951.
23. Cheesbrough M. District laboratory practice in tropical countries, part 2. Cambridge university press; 2006. Available from: https://www.medbox.org/preview/5255d6e1-05d4-41a9-beb2-02b60e695ecc/doc.pdf.
24. Bergey S. Manual of Systematic Bacteriology. W Whitman Springer; 2010. Available from: https://link.springer.com/chapter/10.1007/978-0-387-21609-6_13.
25. Hudzicki J. Kirby-Bauer disk diffusion susceptibility test protocol. Am Soc Microbiol. 2009;8(15):55–63.
26. Wayne PA; CLSI. Performance standards for antimicrobial susceptibility testing. CLSI supplements M100. Clinical and Laboratory Standards Institute; 2020. Available from: https://www.nih.org.pk/wp-content/uploads/2021/02/CLSI-2020.pdf.
27. Korzeniewska E, Korzeniewska A, Harnisz M. Antibiotic resistant Escherichia coli in hospital and municipal sewage and their emission to the environment. Ecotoxicol Environ Saf. 2013;91:96–102. doi:10.1016/j.ecoenv.2013.01.014
28. Nnadozie CF, Odume ON. Freshwater environments as reservoirs of antibiotic resistant bacteria and their role in the dissemination of antibiotic resistance genes. Environ Pollut. 2019;254:113067. doi:10.1016/j.envpol.2019.113067
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.