Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Drug-Related Problems in Pulmonary Hypertension with Valvular Heart Disease
Authors Abdul-Ghaffar F ![]() , Md Redzuan A
, Md Redzuan A ![]() , Makmor-Bakry M
, Makmor-Bakry M ![]() , Muhamad Nor MA
, Muhamad Nor MA
Received 24 May 2022
Accepted for publication 24 October 2022
Published 2 December 2022 Volume 2022:18 Pages 1069—1079
DOI https://doi.org/10.2147/TCRM.S374291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Farizan Abdul-Ghaffar,1,2 Adyani Md Redzuan,1 Mohd Makmor-Bakry,1 Mohamad Arif Muhamad Nor3
1Faculty of Pharmacy, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia; 2Department of Pharmacy, Hospital Serdang, Kajang, Malaysia; 3Department of Cardiothoracic, Hospital Serdang, Kajang, Malaysia
Correspondence: Mohd Makmor-Bakry, Faculty of Pharmacy, Universiti Kebangsaan Malaysia Kuala Lumpur, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, 50300, Malaysia, Tel +603 9289 7244, Fax +603 2698 3271, Email [email protected]
Purpose: The occurrence of drug-related problems (DRPs) and their causes specifically among pulmonary hypertension (PH) with valvular heart disease (VHD) has not been evaluated and is unknown. Therefore, this study aimed to determine the percentage of occurrence, types, and causes of DRPs among PH with VHD patients.
Patients and Methods: An observational retrospective study was conducted at Cardiology Centre, Hospital Serdang, from 1st January to 30th April 2021. Data were collected from medication charts, medical progress notes, laboratory and operative charts through electronic Health Information System (eHIS). The types and causes of DRPs were identified and classified based on Pharmaceutical Care Network of Europe’s (PCNE) classification system V9.02. The data were analyzed using descriptive statistics.
Results: All patients (100%) experienced at least one DRP. Total number of DRPs identified was 120 encounters which were associated with 503 causes. The majority of problems were related to treatment effectiveness (59.1%) and treatment safety (33.4%). The causes of DRPs are mainly related to inappropriate monitoring including therapeutic drug monitoring (18.6%), inappropriate combination of drugs, or drugs and dietary/herbal supplement (10.3%), drug dose was too high (8.9%), drug dose was too low (8.2%) and inappropriate timing of administration or dosing intervals (7.7%).
Conclusion: The percentage of DRP occurrence was high in the studied population. Treatment effectiveness and treatment safety issues were the main DRPs identified with various preventable causes. The findings may be useful to guide the planning of measures to prevent and solve future DRPs in the population.
Keywords: pharmaceutical care, adverse drug reactions, treatment effectiveness, treatment safety
Introduction
Pulmonary hypertension (PH) with valvular heart disease (VHD) is classified as group 2 PH according to European Society of Cardiology/European Respiratory Society 2015 guidelines for the diagnosis and treatment of pulmonary hypertension.1 VHD is a common clinical problem that has gained significant attention in cardiovascular medicine.2
In managing PH with VHD, the primary goal is to relieve the symptoms, and to deliver timely intervention to reduce long-term morbidity and mortality.3 A standard goal-directed medical therapy is required for the cardiac risk factors, namely hypertension, diabetes mellitus, and hyperlipidemia.4 The percentage of patients with heart failure and other cardiovascular diseases who experienced drug-related problems (DRPs) was reported as high as 69% to 78%.5,6 DRPs are defined as “events or circumstances involving drug therapy that actually or potentially interfere with desired health outcomes”.7 The definition of DRP is comprehensive, encompassing the concepts of adverse events, which may be preventable, and medication errors, including prescription errors, drug dispensing errors, and drug administration errors.8 DRP is detected and classified as potential if they have the perspective of causing harm to the patient for either effectiveness or safety aspects.7 Adverse drug reaction (ADR) is one of the DRPs that resulted from a preventable medication error, side-effects from medication administration, or an unforeseen event such as an allergic reaction.9 The World Health Organization defines ADR as a noxious and unintended response to a drug. It occurs at doses normally used in man for prophylaxis, diagnosis or therapy of disease, and the modification of physiological function.10 In the United Kingdom, a landmark study involving 20,000 patients being admitted to hospital found that ADRs lead to an average of eight additional days of hospital stay and are associated with approximately € 706 million per year, including ADRs which were judged potentially preventable.11 Thus, preventing DRPs and optimizing drug therapy simultaneously can prevent ADRs, shorten the length of hospital stays, save lives, and enhance patient quality of life.12
The Pharmaceutical Care Network of Europe’s (PCNE) system is widely used to classify the DRPs. The system has an improved usability and internal consistency due to periodic updates and revisions. It is essential to document and understand the nature of DRPs in the pharmaceutical care process.13 Currently, no published data is available on the percentage of DRP occurrence and its related causes among PH with VHD patients, especially in low- to middle-income countries. Thus, this study aimed to determine the percentage of occurrence, types, and causes of DRPs among PH with VHD patients in a single tertiary centre.
Materials and Methods
Setting and Study Population
This observational retrospective study was conducted at a Cardiology Centre of Hospital Serdang, a tertiary hospital with 633 beds. The study inclusion criteria were patients aged ≥18 years with confirmed diagnosis of group 2 PH with VHD either left-sided heart or/and right-sided heart, mPAP ≥25 mmHg as measured by invasive or non-invasive method who are eligible for valve surgery, admitted to cardiothoracic wards, underwent follow-up before and after valve surgery, from 1st January 2014 to 31st December 2020. Patients were excluded from the study if they underwent valve surgery with coronary artery bypass graft procedures, valve surgery redo and defaulter for follow-up before and after surgery. Consent to review the patient medical record was obtained prior to data collection. The Malaysian Medical Research Ethical Committee [NMRR-20-2396-55935 (IIR.)] and Universiti Kebangsaan Malaysia Ethical Committee (UKM PPI/111/8/JEP-2021-525) approved this study. The study complied with the Declaration of Helsinki and patient confidentiality.
Study Protocol
Patient characteristics, prescription data, medical progress notes, laboratory and operative data were extracted from hospital’s electronic Health Information System (eHIS). Drug-related variables were number of medications prescribed, number of drug-related problems identified, presence of any drug–drug interaction, drug–food interaction and drug incompatibility, adverse events, and monitoring of therapy outcome. All patients were followed-up from last clinic visit pre-surgery to first clinic visit post-surgery. All medications taken pre- and post-surgery, either oral or intravenous were traced from medication chart and documented.
DRPs were categorized using the PCNE classification V9.02.7 The PCNE DRP is divided into five domains: problem type (P), cause (C), intervention (I), acceptance of intervention (A), and outcome (O). Based on the study aim, only the DRP types (P) and causes (C) were investigated. Each DRP causality assessment was classified independently by two clinical pharmacists with at least five years’ experience. In cases of uncertainties in the classification’s accuracy, it will be further discussed with the other co-investigators (AMR & MMB). “Manifested DRP” was defined as drug problems that actually occurred or patient experienced harm. The percentage of patients with DRPs was calculated by dividing the number of patients who experienced at least one DRP by the total number of patients who used the drugs; and multiplying with 100%. A patient may encounter more than one DRP with multiple causes. Any identified adverse drug reactions were assessed utilizing the Naranjo scoring tool for causality assessment.14 The incidence of DRPs was calculated by dividing the number of patients who manifested the DRP with the number of patients receive the medications. DRP classifications were identified and determined through objectively and subjectively measured parameters found in the patient progress reports. For example, a patient was discharged with oral warfarin 33.5mg per week. During the follow-up clinic visit, the clinician found that INR reading was 1.3, below the target range (INR 2–3). Thus, the dose was increased from 33.5 mg/week to 35 mg/week. DRP was classified as a treatment effectiveness issue in this scenario, P1 and subcategory P1.2, “effect of drug treatment not optimal”.
Established references were used to compare drug indications and drug dosage regimen in the identification and confirmation of DRPs. These references include the 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: a practical chronicle of progress,1 2017 ESC/EACTS Guidelines for the management of valvular heart disease15 and Clinical Practice Guidelines Atrial fibrillation 2012.16 Additional references such as 3rd edition of National Antimicrobial Guideline Third Edition 2019,17 A Guide to Antimicrobial Therapy in the Adult ICU 201718 and 2nd edition of Clinical Pharmacokinetics Pharmacy Handbook19 were referred to confirm the appropriateness of non-cardiovascular drugs for indications and dosage regimen.
Data Collection
Figure 1 explains the process of drug-related problem identification during data collection period. Patient demographic and clinical data, including age, gender, and type of surgery were extracted from medical records. All patients were follow-up starting from their most recent pre-operative assessment clinic visit, admission to the hospital, at discharge, and post-operative assessment for follow-up as second visit. Database was created using SPSS and each of identified DRP including problem types (P) and causes (C) were recorded.
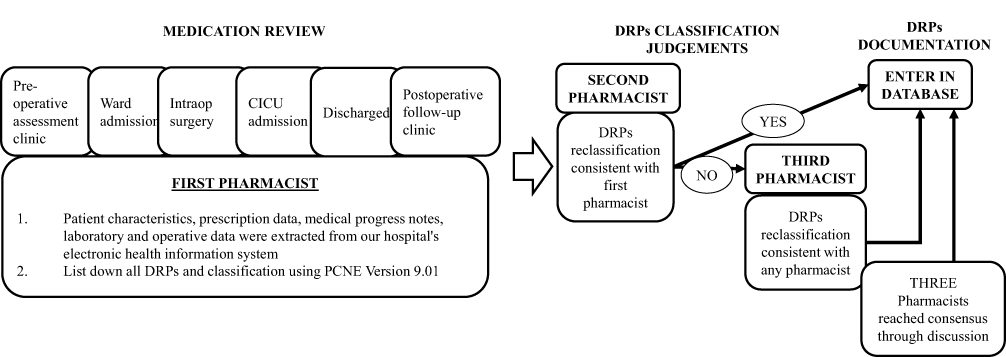 |
Figure 1 The process of drug-related problems identification. Abbreviations: DRP, drug related problem; CICU, cardiac intensive care unit, PCNE, Pharmaceutical Care Network Europe. |
Statistical Analysis
Availability of specific PH with VHD patients is limited with a total population of 61 patients. Thus, all patients were recruited as study subjects. SPSS (Version 25) was utilized to descriptively summarize the demographic and clinical characteristics of the patients. Categorical data were expressed using numbers and percentages.
Results
Demographic Characteristics
The demographic characteristics of study population with drug-related problem summarized in Table 1. The characteristics of patients (n = 61) with drug-related problems included mean age of 47 (±14.2) years old, 57% (n = 35) were female, 70% were diagnosed with severe PH, 62% with mitral valve regurgitation and 61% patients were diagnosed with mitral stenosis. Most of the patients (82%) had undergone repair and replacement procedures. Significant co-morbidities identified were atrial fibrillation (46%), systemic hypertension (33%) and asthma (15%). Overall, patients were prescribed with an average of 4.62 (±1.16) types of drugs.
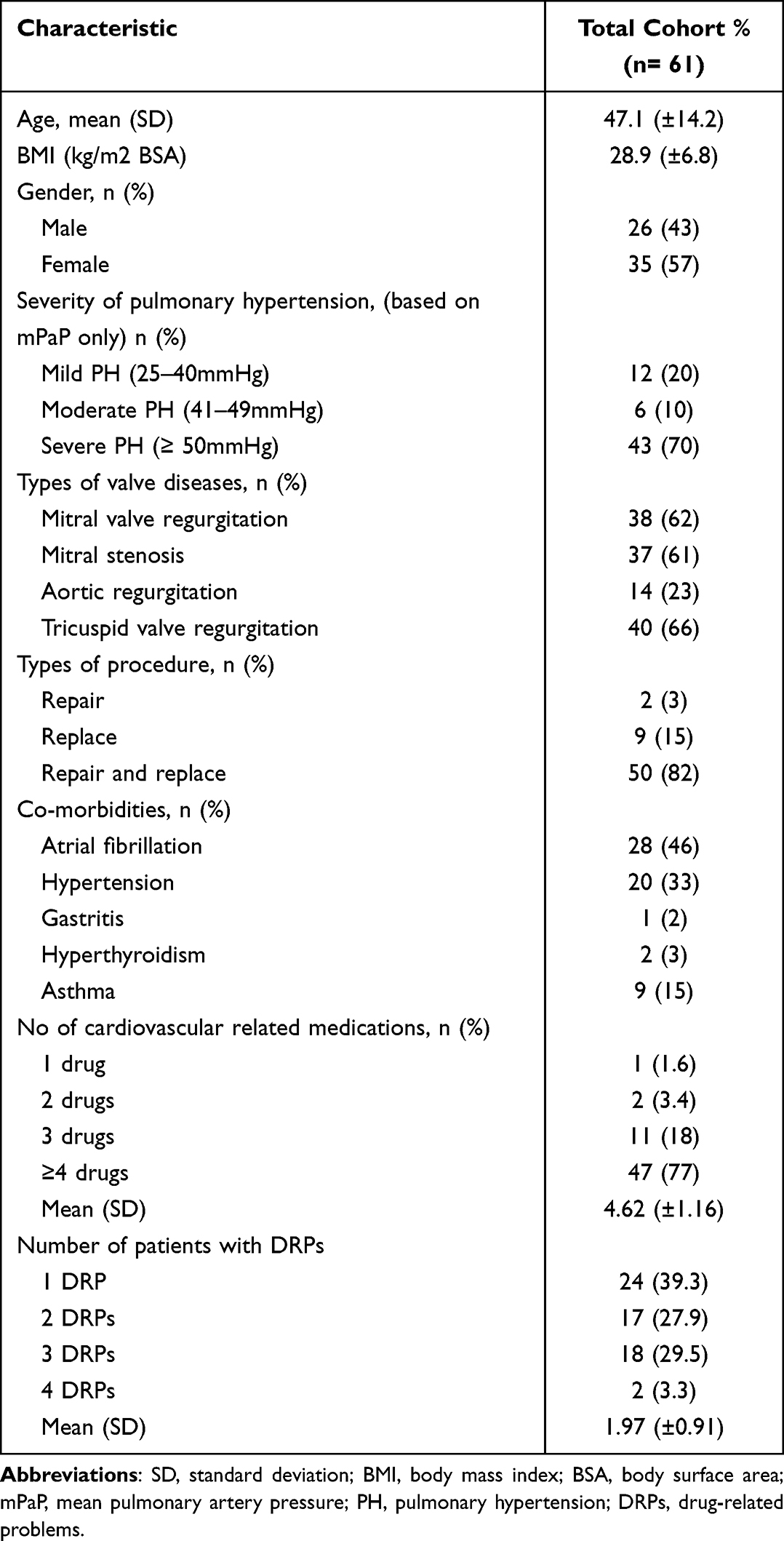 |
Table 1 Demographic Characteristics of Study Population with Drug-Related Problems |
Percentage of DRP and Types of Causes
The percentage of patients with DRPs was identified at 100% (n = 61 patients). The studied population recorded 120 DRPs with 503 associated causes (Supplementary Table 1). On average, each patient encountered 1.97 (±0.91) DRPs during the study period. Majority of the patients (60.7%) experienced two or more DRPs. The distribution of DRP’s problem domains is presented in Table 2. The primary problem domains were the treatment effectiveness issue (P1; 59.1%) and treatment safety (P2; 33.4%). Among the sub-domain of problems, “effect of drug treatment not optimal” (P1.2) was the most common issue (50.8%). The distribution of DRP’s cause domains is presented in Table 3. Generally, the causes of DRPs were related to no or inappropriate outcome monitoring (including therapeutic drug monitoring) (C9.1; 18.6%), inappropriate combination of drugs, or drugs and dietary/herbal supplement (C1.4; 10.3%), drug dose was too high (C3.2; 8.9%), drug dose was too low (C3.1; 8.2%) and inappropriate timing of administration or dosing intervals (C6.1; 7.7%).
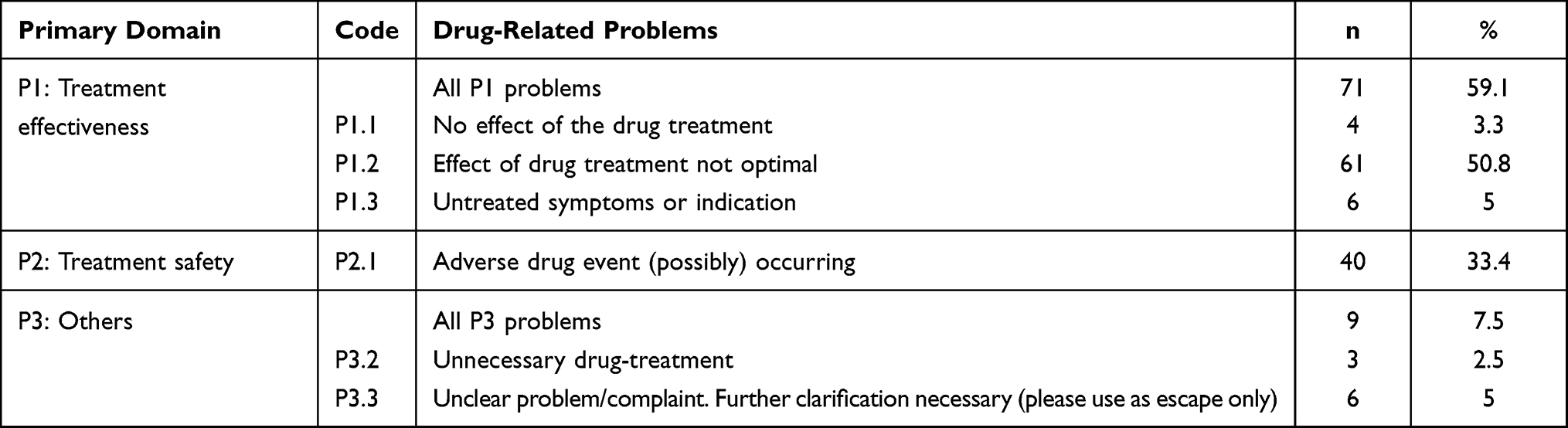 |
Table 2 Types of Drug-Related Problems Identified Among Pulmonary Hypertension with Valvular Heart Disease |
 |
Table 3 Types of Causes of Drug-Related Problems in Pulmonary Hypertension with Valvular Heart Disease |
Incidence of DRPs
The incidence of DRPs based on specific drug usage is shown in Table 4. Thirty-four patients experienced manifested DRPs. Twenty-one patients had experienced ADRs with total 24 episodes (Table 5). Three patients had encountered more than one ADR episodes. According to the Naranjo causality assessment,14 8 ADR episodes were classified as definite (8/24, 33%), 11 episodes as probable (11/24, 46%), and 5 episodes as possible (5/24, 21%). The ADRs were associated with the usage of catecholamine group drugs (n = 1/1, 100%), antiarrhythmic class III (n = 7/10, 70%), phosphodiesterase-5 inhibitors (n = 1/3, 33.3%), antihypertensive (n =1/3, 33.3%), antithrombotic agents (n = 8/25, 32%) and antibiotics (n = 3/28, 11%).
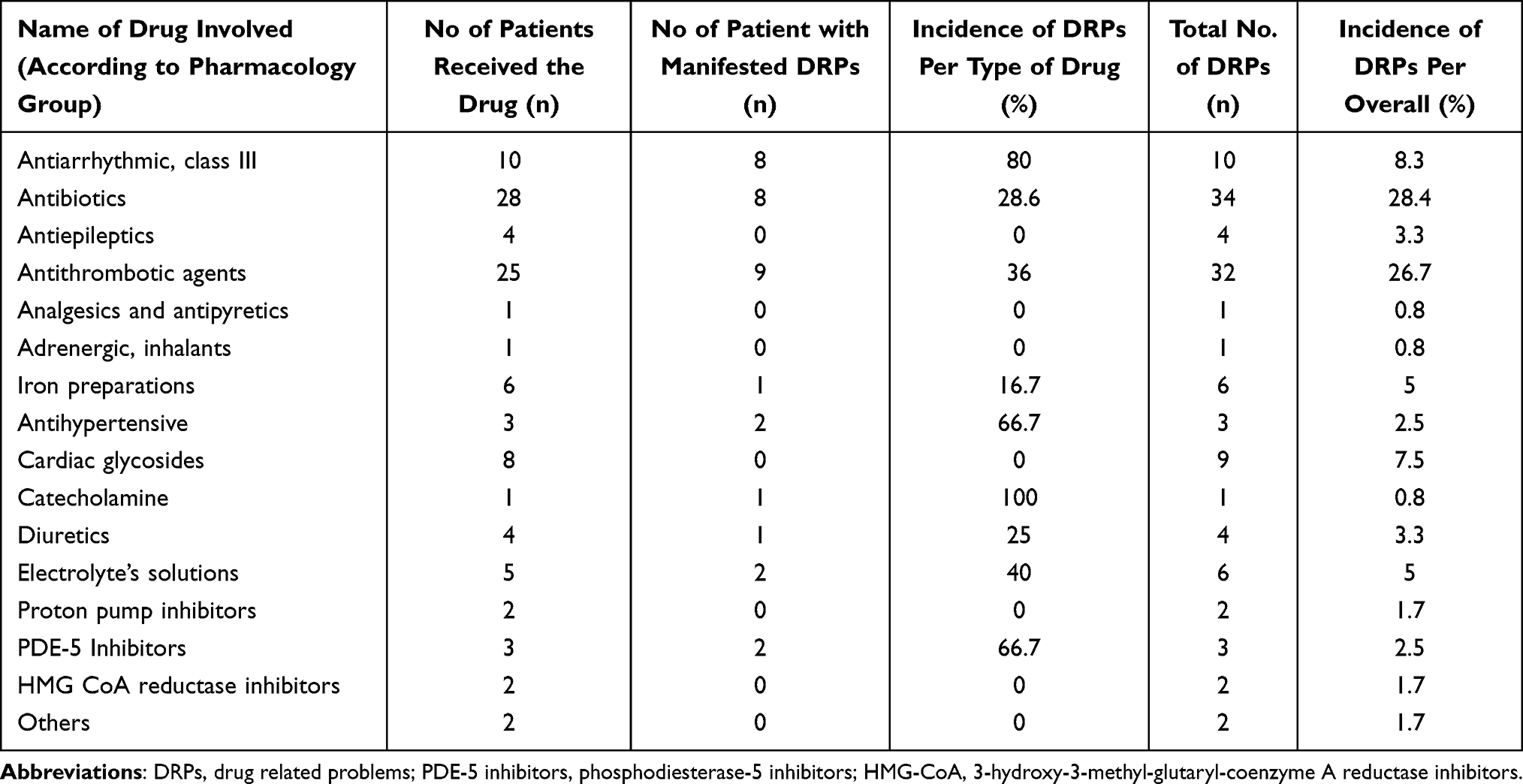 |
Table 4 The Incidence of Drug-Related Problems in Pulmonary Hypertension with Valvular Heart Disease |
 |
Table 5 The Incidence of Adverse Drug Reactions in Pulmonary Hypertension with Valvular Heart Disease |
Relationship Between DRPs and the Types of Causes
Figure 2 depicts the simplified network that explains the relationship between DRPs and causes. The thickness of the line showed the frequency of causes to each DRP. Effect of drug treatment not optimal (sub-domain P1.2; n = 259) and adverse drug reactions (sub-domain P2.1; n = 195) were the highest number of DRPs identified. The common causes for sub-domain P1.2 were no or inappropriate outcome monitoring (C9.1, n = 51), drug dose too low (C3.1, n = 36), and patient uses/takes less drug than prescribed or does not take the drug at all (C7.1, n = 22). The identified causes for sub-domain P2.1 were drug dose too high (C3.2, n = 40), no or inappropriate outcome monitoring (C9.1, n = 30), and inappropriate combination of drugs, or drugs and herbal medications, or drugs and dietary supplements (C1.4, n = 28).
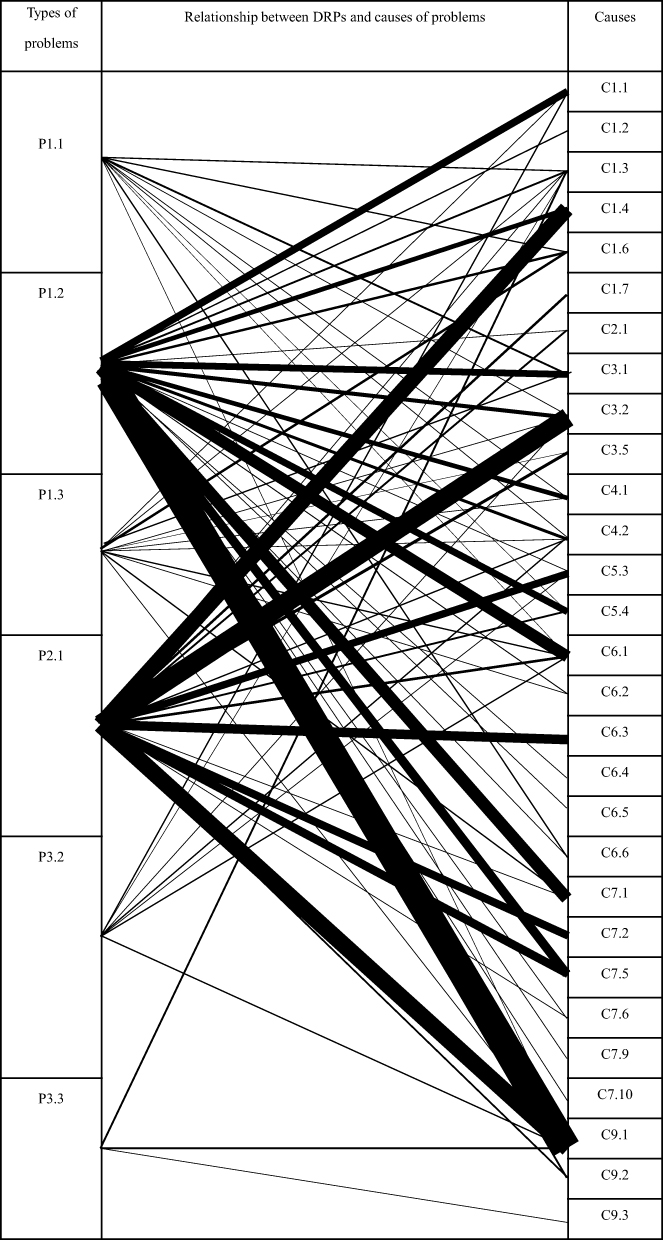 |
Figure 2 Simplified network diagram between the types and causes of drug related problems (DRPs). |
Discussion
The percentage of patients with DRPs identified in this study is high and comparable with the studies reported for other populations related to cardiovascular diseases.5 Hospital admission due to DRPs was estimated at 5–10%, in which more than half of them is preventable.20 Common causes of the DRPs identified may also serve as a guide to enhance pharmacotherapeutic management of patients in PH with VHD.
The disease’s complexity has aided the emergence of treatment complications and led to DRPs among patients. PH with VHD is commonly underdiagnosed and strongly associated with increased mortality and morbidity.1 Post-surgery and potential risks contributing to DRPs include valve-related complications such as thromboembolism, bleeding complications, prosthetic valve endocarditis, and prosthetic valve dysfunctions.21 In addition, common co-morbidities such as AF, hypertension, and chronic rheumatic heart disease and the number of drugs taken by the patient also contributed to the development of DRPs.22 Drugs such as antibiotics, amiodarone, digoxin, iron sucrose and warfarin that are commonly used as part of the medical management after VHD surgery were categorized as high-risk medications and some were narrow therapeutic index (NTI).23,24 This explains the reasons that lead to the high percentage of inappropriate monitoring in this study. An increasing number of drugs taken by the patients exponentially elevated the risk of harm.25 This risk has been quantified at 13% with two medications, 58% with five medications and 82% with seven or more medications.26 Thus, the current study supported this notion as most of the study participants also received three or more medications. Available medications such as beta-blockers, diuretics, amiodarone and digoxin may be used at suboptimal doses to reduce the cost of therapy, which ultimately contributes to DRPs and can exacerbate the patient’s condition.
This study identified issues related to treatment effectiveness as the primary DRPs. It was associated with the drug treatment not being optimal, which resulted in the progression of PH with VHD. Inappropriate monitoring of treatment outcome, usage of lower doses, drug–drug interactions, improper timing of drug administration and patient’s adherence contributed to the problem. INR readings and digoxin levels among patients who received warfarin and digoxin were subtherapeutic after valve surgery. The subtherapeutic INR maybe due to interruptions of procedures that necessitate warfarin discontinuation, which frequently occurs before surgery.4,5 Thus, patients may experience prolonged hospital stay after surgery while waiting for appropriate warfarin effect.5 Other contributing causes to subtherapeutic INR include recent administration of vitamin K, non-adherence to treatment, diarrhea, vomiting, changes in concomitant drug therapy, dietary and lifestyle, and disease status.5 The effectiveness of warfarin in patients with mechanical heart valves requires continuous antithrombotic with an INR reading within the target range.4 Therefore, patient educational program and close surveillance by an experienced health-care professional is necessary. Patient monitoring through dedicated anticoagulation clinics resulted in lower complication rates than those seen with standard care and was more cost-effective.5 Digoxin has become a part of postoperative AF management to maintain hemodynamic stability, control the symptoms, and prevent thromboembolism. Digoxin dose should be adjusted to achieve therapeutic level of 0.8–2 mcg/L.19 Thus, dose optimization is crucial, and this can be achieved with appropriate monitoring of digoxin levels, renal function status, electrolytes, and concomitant medications. All patients received antibiotic prophylaxis either cefazolin or cefuroxime; these antibiotics were prolonged after valve surgery between 48 and 72 hours. Some patients were switched to a broader spectrum antibiotic such as piperacillin/tazobactam or meropenem. However, patients tend to receive lower doses for certain antibiotics, which contributed to suboptimal treatment. For example, the cefazolin was frequently prescribed with lower dose than recommendation. Local guidelines recommended that cefazolin dose should be adjusted according to the patient’s body weight.17 These DRPs are preventable through collaboration between clinicians, clinical pharmacists, and microbiologists.
More than half of patients experienced DRPs, resulting in clinical manifestation like ADRs throughout the treatment in this study. Antiarrhythmics class III, catecholamines, antihypertensive, phosphodiesterase-5 inhibitor, electrolyte’s solutions and antithrombotic agents were among the drugs that caused DRPs and led to ADRs. Abu Ebsa (2021) reported ADRs caused 1.6% resulted in hospital admission, 1.4% required intensive medical care and 0.3% of the reported ADRs caused permanent harm.27 The occurrence of ADRs required early cessation of the causal drug, which worsened the disease condition. Factors such as dose-related and drug-related ADR are usually predictable but sometimes unavoidable.28 It is highly dependent on the patient’s sensitivity to the drug and the drug’s combination.29 In addition, antiarrhythmics such as amiodarone often cause drug-induced liver injury, which was highly associated with a high drug dose, and inappropriate monitoring worsens the patient’s clinical conditions.30 The majority of ADRs occur due to the extension of the desired pharmacologic effects of a drug, often due to the substantial variability in the pharmacokinetics and pharmacodynamics seen among patients, including genetic factors.30
Patients who received intravenous (IV) amiodarone developed elevation of total bilirubin and alanine transaminase reading after 24–48 hours throughout the study period, which was similarly reported earlier.30 Solubilizers such as polysorbate 80 in the IV amiodarone preparation may trigger immune-mediated alteration of the hepatocellular membrane.31 Hepatobiliary ADRs were the top reported ADRs by pharmacists, manifested mainly by increased liver enzymes, jaundice, or cholestasis. Thus, appropriate dosing and close monitoring of liver profiles may help in preventing ADRs.
Therapy optimization is crucial, and the responses towards drugs with NTI depend on appropriate doses and close monitoring. Preventing ADR is critical, therefore identification of patient-specific factors such as liver and kidney function, history of drug allergies and ADRs may reduce the ADR risk and provide possible alternatives. For instance, three patients encountered the same ADRs throughout the treatment, which may be preventable if the history of ADRs and drug allergies were well taken and documented. Additionally, drug interaction checkers are available on handheld devices may be utilized with the help of mobile information technology. Every health institution should support and maintain an active ADR team that responsible to evaluate incidents, monitor trends, and identify opportunities to improve medication and patient safety.
Understanding the type of DRPs and their causes among patients with PH and VHD helps health-care providers, namely doctors and pharmacists, to plan strategies to identify, resolve and prevent the DRPs. The results presented are helpful for optimization of collaborative patient management. Nevertheless, the study may have some limitations. The retrospective nature of the study is known to be associated with possible missing or misinterpretation of data. The diagnosis of confirmed PH with VHD was solely based on documented in progress notes. The pharmacists who performed the data collection may be associated with information bias and under/overestimating the DRPs percentage. Effort was taken to reduce this issue through reconfirmation of the DRP classification by another two researchers (AMR and MMB). The short duration of followed up may affect the number of DRPs. Longer exposure to multiple medications may increase the number of DRPs. The data were also gathered from a single institution, which may also limit the generalizability of the findings.
Conclusion
The percentage of DRPs among patients with PH and VHD was high. Treatment effectiveness and safety issues were the main DRPs identified with various preventable causes. The findings may be useful to guide the planning of measures to identify, solve and prevent future DRPs in the population.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
The Malaysian Medical Research Ethical Committee [NMRR-20-2396-55935 (IIR.)] and Universiti Kebangsaan Malaysia Ethical Committee (UKM PPI/111/8/JEP-2021-525) approved this study.
Acknowledgments
We thank all the staff of Pharmacy department, Cardiothoracic anesthesia and perfusion department and Cardiothoracic department of Hospital Serdang.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Galiè N, Chairperson E, Humbert M, et al. ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2015;2015(46):903–975. doi:10.1183/13993003.01032-2015
2. Wang X, Xu B, Liang H, et al. Distribution characteristics and factors influencing oral warfarin adherence in patients after heart valve replacement. Patient Prefer Adherence. 2018;12:1641–1648. doi:10.2147/ppa.s172223
3. Baumgartner H, Iung B, Otto CM. Timing of intervention in asymptomatic patients with valvular heart disease. Eur Heart J. 2020;41(45):4349–4356. doi:10.1093/eurheartj/ehaa485
4. Otto CM, Nishimura RA, Bonow RO, et al. ACC/AHA guideline for the management of patients with valvular heart disease a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2020;2021(143):e72–e227. doi:10.1161/cir.0000000000000923
5. Gastelurrutia P, Benrimoj SI, Jos E, Tuneu L, Mangues MA, Bayes-Genis A. Negative clinical outcomes associated with drug-related problems in Heart Failure (HF.) out-patients: impact of a pharmacist in a multidisciplinary HF clinic. J of Cardiac Fail. 2011;17(3):217–223. doi:10.1016/j.cardfail.2010.10.009
6. Niquille A, Bugnon O. Relationship between drug-related problems and health outcomes: a cross-sectional study among cardiovascular patients. Pharm World Sci. 2010;32:512–519. doi:10.1007/s11096-010-9401-1
7. Van Mil JWF, Horvat N, Westerlund T. Classification for Drug Related Problems V 9.00. PCNE Classification; 2019:1–10.
8. Nebeker JR, Barach P, Samore MH. Clarifying adverse drug events: a clinician’s guide to terminology, documentation, and reporting. Ann Intern Med. 2004;140(10):795–801. doi:10.7326/0003-4819-140-10-200405180-00009
9. Jokanovic N, Wang KN, Dooley MJ, et al. Prioritizing interventions to manage polypharmacy in Australian aged care facilities. Res Soc Adm Pharm. 2017;13(3):564–574. doi:10.1016/j.sapharm.2016.06.003
10. Hadi MA, Neoh CF, Zin RM, et al. Pharmacovigilance: pharmacists’ perspective on spontaneous adverse drug reaction reporting. Integrated Pharmacy Res Pract. 2017;6:91–98. doi:10.2147/iprp.s105881
11. Pirmohamed M, James S, Meakin S. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. British Med J. 2004;329(7456):15–19. doi:10.1136/bmj.329.7456.15
12. Al-Azzam SI, Alzoubi KH, AbuRuz S, et al. Drug-related problems in a sample of outpatients with chronic diseases: a cross-sectional study from Jordan. Ther Clin Risk Manag. 2016;12:233–239. doi:10.2147/tcrm.s98165
13. Van Mil JW, Westerlund LO, Hersberger KE, Schaefer MA. Drug-related problem classification systems. Ann Pharmacother. 2004;38(5):859–867. doi:10.1345/aph.1D182
14. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/clpt.1981.154
15. Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739–2791. doi:10.1093/eurheartj/ehx391
16. Ministry of Health. Malaysian CPG of atrial fibrillation; 2012. Available from: https://www.malaysianheart.org.
17. Ministry of Health M. National antibiotic guidelines 3rd edition; 2019. Available from: https://www.pharmacy.gov.my.
18. Malaysia Society of Intensive Care. Guide to antimicrobial therapy in the adult ICU 2017; 2017. Available from: https://www.msic.org.my.
19. Pharmaceutical Services Division Ministry of Health Malaysia. Clinical pharmacokinetics pharmacy handbook 2nd edition. Pharm Pract Dev Div. 2019;2019:171.
20. Niriayo YL, Kumela K, Kassa TD, Angamo MT. Drug therapy problems and contributing factors in the management of heart failure patients in Jimma University Specialized Hospital, Southwest Ethiopia. PLoS One. 2018;13(10):e0206120. doi:10.1371/journal.pone.0206120
21. Misawa Y. Valve-related complications after mechanical heart valve implantation. Surg Today. 2015;45(10):1205–1209. doi:10.1007/s00595-014-1104-0
22. Gelchu T, Abdela J. Drug therapy problems among patients with cardiovascular disease admitted to the medical ward and had a follow-up at the ambulatory clinic of Hiwot Fana Specialized University Hospital: the case of a tertiary hospital in eastern Ethiopia. SAGE Open Med. 2019;7:1–9. doi:10.1177/2050312119860401
23. Saedder EA, Brock B, Nielsen LP, Bonnerup DK, Lisby M. Identifying high-risk medication: a systematic literature review. Eur J Clin Pharmacol. 2014;70(6):637–645. doi:10.1007/s00228-014-1668-z
24. Iyer K, Dilipkumar N, Vasaya S, Pawar S, Diwan A. Comparison of drug related problems associated with use of narrow therapeutic index drugs and other drugs in hospitalized patients. J Young Pharm. 2018;10(3):318–321. doi:10.5530/jyp.2018.10.70
25. Carbonin P, Pahor M, Bernabei R, Sgadari A. Is age an independent risk factor of adverse drug reactions in hospitalized medical patients? J Am Geriatr Soc. 1991;39(11):1093–1099. doi:10.1111/j.1532-5415.1991.tb02875.x
26. Patterson SM, Cadogan CA, Kerse N, et al. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst Rev. 2014;7(10):CD008165. doi:10.1002/14651858.cd008165.pub3
27. Abu Esba LC, Al Mardawi G, AlJasser MI, Aljohani B, Abu Alburak A. Adverse drug reactions spontaneously reported at a tertiary care hospital and preventable measures implemented. J Clin Pharm Ther. 2021;46(2):460–469. doi:10.1111/jcpt.13306
28. Coxon J, Rees J. Avoiding medical errors in general practice. Trends Urol Mens Heal. 2015;6(4):13–17. doi:10.1002/tre.467
29. Khalil H, Huang C. Adverse drug reactions in primary care: a scoping review. BMC Health Serv Res. 2020;20(1):1–13. doi:10.1186/s12913-019-4651-7
30. Diab OA, Kamel J, Abd-Elhamid AA. Predictors of intravenous amiodarone induced liver injury. Egypt Hear J. 2017;69(1):45–54. doi:10.1016/j.ehj.2016.05.001
31. Stratton A, Fenderson J, Kenny P, Helman DL. Severe acute hepatitis following intravenous amiodarone: a case report and review of the literature. Acta Gastroenterol Belg. 2015;78(2):233–239.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.