Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Drug-Induced Movement Disorders and Its Associated Factors Among Patients Attending Treatment at Public Hospitals in Eastern Ethiopia
Authors Misgana T ![]() , Yigzaw N, Asfaw G
, Yigzaw N, Asfaw G ![]()
Received 20 May 2020
Accepted for publication 1 August 2020
Published 17 August 2020 Volume 2020:16 Pages 1987—1995
DOI https://doi.org/10.2147/NDT.S261272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Tadesse Misgana,1 Niguse Yigzaw,2 Getachew Asfaw3
1Department of Psychiatry, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Psychiatry, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia; 3Research and Training Department, Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia
Correspondence: Tadesse Misgana Tel +251 923 100 463
Email [email protected]
Background: Antipsychotic medications have both beneficial and undesired effects at a dose used for treatment purposes. Among undesired effects caused by antipsychotics, movement disorders are prevalent. However, there is no study done to determine the prevalence of movement disorders that occurred due to antipsychotics and their determinants in eastern Ethiopia.
Objective: This study aimed to find out the prevalence of drug-induced movement disorders and its determinants among patients who had been on follow-up at public hospitals in eastern Ethiopia.
Methods: A cross-sectional study was conducted from May to June 2018 at HFSUH and Jugal hospital. Extrapyramidal symptom rating scale (ESRS) was used to identify patients with drug-induced movement disorders in a sample of 411 outpatients. A systematic random sampling method was used to select the sample. Logistic regression was done to identify factors associated.
Results: A drug-induced movement disorder was found in 44% of the participants: Of this, 27.3% had drug-induced pseudo-Parkinsonism, 21.2% had drug-induced akathisia, 9.5% had drug-induced tardive dyskinesia, and 3.4% had drug-induced tardive dystonia. Being female was associated with pseudo-Parkinsonism (AOR=3.6, 95% CI: 2.03, 6.35), akathisia (AOR=4.9, 95% CI: 2.73, 8.78), and tardive dyskinesia (AOR=2.51, 95% CI: 1.08, 5.86) and being male with tardive dystonia (AOR=4.6, 95% CI: 1.8, 18.5). Alcohol use was associated with tardive dyskinesia (AOR= 5.89, 95% CI: 2.20, 15.69).
Conclusion: Drug-induced movement disorder in this study was high and nearly half of patients on antipsychotic treatment were experiencing it. Age, sex, and doses of antipsychotics were factors associated with all of the types of drug-induced movement disorders.
Keywords: akathisia, pseudo-parkinsonism, tardive dyskinesia, tardive dystonia, movement disorders, Ethiopia
Introduction
Drug-induced movement disorders constitute a worldwide problem in the treatment of schizophrenia because of the limited affordability of atypical antipsychotic drugs and because even the atypical antipsychotics can cause extrapyramidal symptoms.1,2 Antipsychotic-related movement disorders are classified as acute like akathisia and pseudo Parkinsonism which developed shortly after taking the medication, or titrating the amount and chronic, like tardive dyskinesia and tardive dystonia, that occurs after taking the antipsychotics for a long period of time.3
The prevalence of antipsychotic-induced movement disorders among patients treated by first-generation antipsychotics (FGAs) for long periods was ranged from 50% to 75%.4 The newer antipsychotics, the serotonin-dopamine antagonists (SDAs), block binding to dopamine receptors to a much lesser degree and thereby are presumed to be less likely to produce such movement disorders. Nevertheless, this risk remains and vigilance is still required when these drugs are prescribed.5
In one reviewed study involving 30,139 patients, 9.4% of the patients were developed tardive dyskinesia.6 Another reviewed medical literature showed that the prevalence of drug-induced akathisia was 25.9%.7 The retrospective study conducted at a medical center in southern Taiwan showed that one-third of the patient had at least one type of chronic movement disorders; 21.1%, 12.5%, 2.4% and 2.4% for tardive dystonia, tardive tremor, TD and tardive akathisia, respectively.8 TD prevalence rates varied substantially between studies, with an estimated prevalence of around 20% in patients using SGAs. The risk of TD is lower SGAs than with FGAs but remains a problem because SGAs are increasingly being prescribed.9
Factors contributing to the development of antipsychotic-related movement disorders were different for each specific movement disorders. Numerous articles are reporting on risk factors for TD. This includes tardive dystonia,10 treatment non-responders,11 worse premorbid functioning,12 motor sequencing factor from the Neurological Evaluation Scale,13 the percentage change in negative symptoms,14 poor prognosis, and long treatment duration15 and worsening of psychosis.16
Although the factors contributed to the developments of akathisia were not well known, it is hypothesized due to taking large doses of neuroleptic and being in middle age.17 Being treated by a large dose of the drug, using high potent medications, advanced age, being female, having a family history of movement disorders and occurrence with other types of movement disorders were factors leading the patients to psuodoparkinsonism.18 Younger age, being male, taking the highly potent drug and high dose were risk factors for tardive dystonia.19,20
The treatment gap for mental disorders is high all over the world. The earlier these conditions are recognized and addressed, the greater the chances of minimizing their impact. Therefore, early identification of drug-induced movement disorders can be useful to prevent several complications. Despite mounting evidence of the impact of antipsychotic-induced movement disorders, prevention and treatment have been slow and there is a shortage of information related to drug-induced movement disorders and its associated factors among psychiatric outpatients in Ethiopia. So, the current study is aimed to determine the prevalence of drug-induced movement disorders and to identify factors associated with it.
Methods and Materials
Study Design and Period
A cross-sectional study was conducted from May 8 to June 15, 2018.
Study Setting
The study was done in Harar town, located 525 km towards the east of Addis Ababa, the capital of Ethiopia. HFSUH is located in Harar town and is one of the specialized university hospitals in Ethiopia. The hospital had an estimated average psychiatric patient flow of 7000 annually. Jugal hospital is the first hospital founded in Harar town and the estimated average patients served are 320 per month.
Source Population
All patients diagnosed with mental illness who had been treated by antipsychotic medications at HFSUH and Jugal Hospital.
Study Population
Patients diagnosed with mental illness that fulfilled the inclusion criteria and were on follow-up at HFSUH and Jugal Hospital.
Inclusion Criteria
All patients with mental illness who had been on antipsychotic medications at the psychiatric OPDs.
Exclusion Criteria
Patients with severe illness and cannot communicate (unable to give the required information) and who had the previous history of primary movement disorders were excluded.
Sample Size Determination and Sampling Technique
The sample size was calculated using the formula for estimation of single population proportion with the assumption of the prevalence taken from a study conducted previously, which was 56%19 with a 95% confidence level, and 5% margin of error. The final estimated sample size was 416. The participants were allocated with the two hospitals proportional to their monthly client flow and then systematic random sampling was used to determine the sampling interval. Therefore, participants were selected from patients every two intervals (ie we took every other patient when they came for their follow-ups).
Study Variables
Dependent variable: Drug-induced movement disorders (presence/absence)
Independent variables:
- Socio-demographic variables: includes sex, age, marital status, level of education, residence, and occupation.
- Clinical: diagnosis of the patient, duration of treatment, co-morbid psychiatric and chronic medical illness, and having a family history of primary movement disorders were assessed by reviewing the patient’s medical chart and interviewing.
- Medication-related variables: information about the class of antipsychotics, a dose of antipsychotics (the dose was calculated and changed to chlorpromazine equivalent dose),21 concomitant medication use, and medication for movement disorders were extracted from patients chart.
- Substance-related: alcohol, tobacco and Khat use.
Operational Definitions
- Antipsychotic-induced movement disorders – defined as if the patient has at least one movement disorder among the four including akathisia, pseudo parkinsonism, tardive dystonia, and tardive dyskinesia in extrapyramidal symptom rating scale (ESRS).22
- Pseudo Parkinsonism – “a score of 2 on 2 items or a score of 3 or greater on one item indicates the presence of pseudo-Parkinsonism in ESRS.”22
- Akathisia – “score of 3 or greater on the 2 items is required for presence in ESRS.”22
- Tardive dystonia –“When establishing presence versus absence of dystonia, a score of 3 or greater on at least one item, or a score of 2 on 2 items is required to indicate the presence of dystonia in ESRS.”22
- Tardive dyskinesia- “When scoring presence versus absence of TD, a score of 3 or greater on at least one item or a score of 2 on 2 items is required to indicate the presence of TD in ESRS.”22
- Dual psychiatric diagnosis – if the patients diagnosed with two or more psychiatric disorders based on DSM IV.
- Co-morbid chronic medical illness – if the patients had any chronic medical illness in addition to psychotic illness.
Data Collectors and Data Collection Tools
Data were collected by five experienced psychiatric nurses recruited from HFSUH and Jugal Hospital and the training was given about sampling procedures.
The questionnaire has five sections: a socio-demographic questionnaire to assess the patients’ background information. Alcohol, tobacco, and chat use were measured by “Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST)”23 Clinical factors were assessed by yes/no answers of respondents and chart review. Medication-related factors were obtained from the patient medical record. The four types of antipsychotic-induced movement disorders were assessed using the “Extrapyramidal Symptom Rating Scale (ESRS)”22
Data Quality Control
Semi-structured questionnaires were used to collect the information. A standardized questionnaire containing six sections was translated into local language Amharic and Afaan Oromo and back to English, and the differences were modified accordingly. The questionnaire was checked for its reliability, clarity, simplicity, and understandability by doing pretest on 5% of the sample size.
Data Processing and Analysis
The data were edited, coded, and entered into Epi-data version 3.1 then it was exported to Statistical Package for Social science (SPSS) version 20 for analysis. Logistic regression was carried out to explain the association between explanatory and outcome variables and “ENTER” was the method of entering the independent variable. Variables with a p-value <0.05 were considered as significantly associated with drug-induced movement disorders.
Results
Socio-Demographic Characteristics of the Study Participants
Among 416 of the total study sample, 411 agreed to participate resulting in a response rate of 98.8%. The mean age of the participants was 44.73 years with SD ±14.89 years. About 243 (59.1%) of the study participants were male as shown in Table 1.
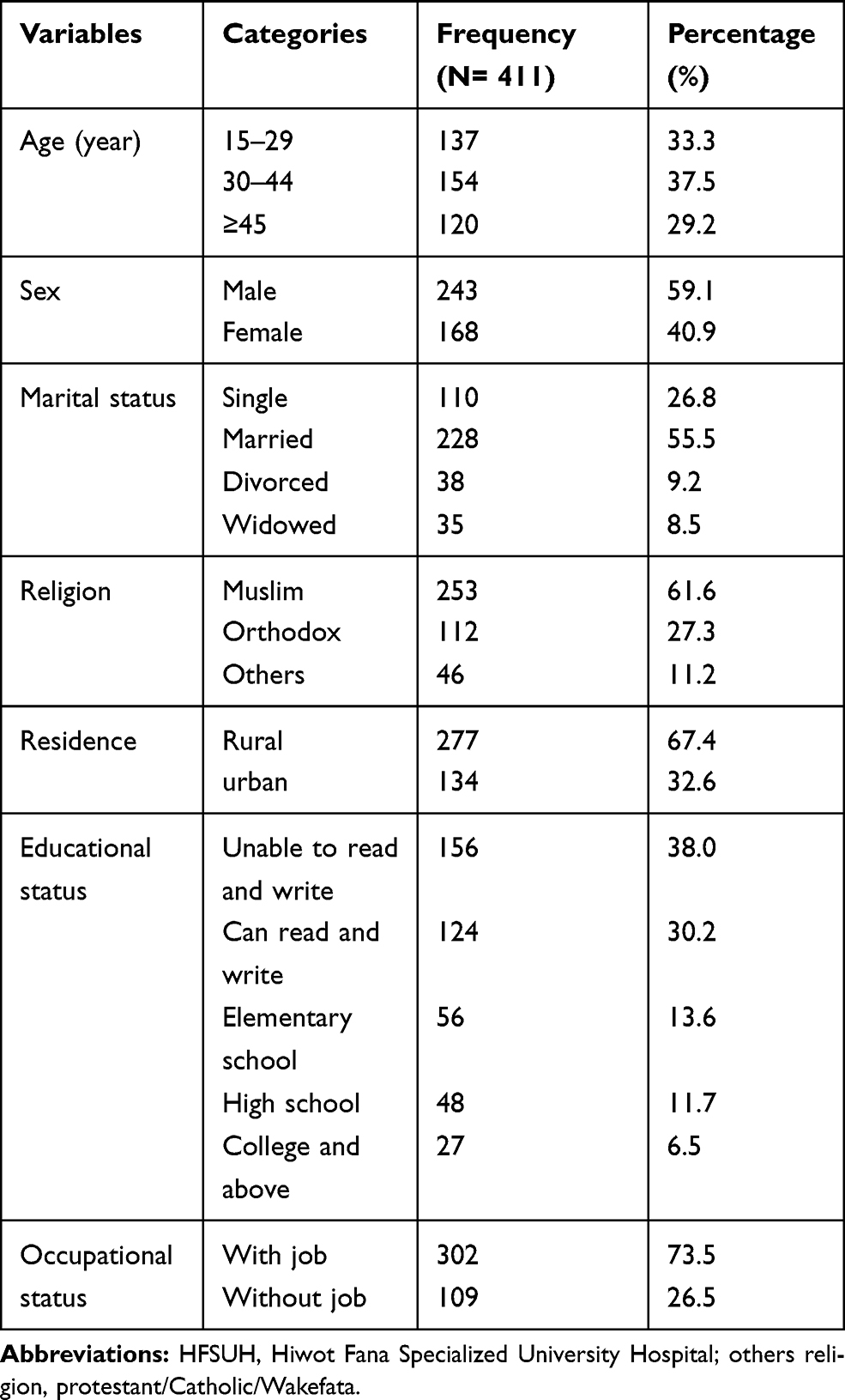 |
Table 1 Socio-Demographic Characteristic of Participants Who Were on Follow-Up at HFSUH and Jugal Hospital, 2018 |
Clinical Characteristics of the Respondents
Among the respondents, 174 (42.3%) had a diagnosis of schizophrenia. Almost half of the study participants 215 (52.3%) had received treatment within the range of 1–5 years with a mean length of 4.1 years (SD=3.2) (Table 2).
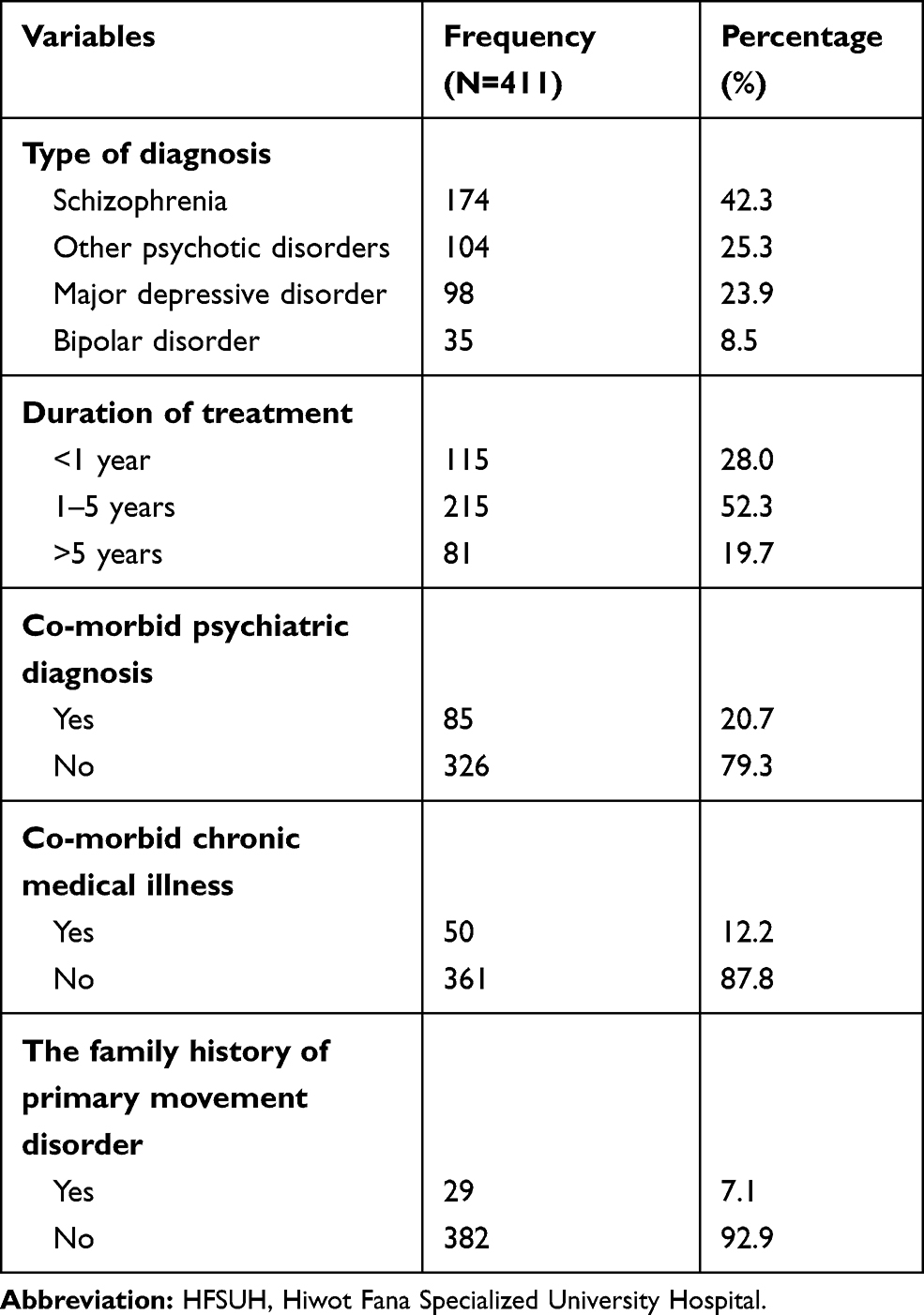 |
Table 2 Clinical Characteristics of Participants Who Were on Follow-Up at HFSUH and Jugal Hospital, 2018 |
Medication-Related Characteristics of Participants
Of study participants, 334 (81.3%) patients were receiving FGAs, 59 (14.4%) patients were receiving more than one FGAs and 21 (5.1%) were receiving both first and second-generation antipsychotics simultaneously. The average daily dose was 454 mg (+-274mg). One hundred twelve (27.3%) of patients received antidepressants, 30 (7.3%) received mood stabilizers, 13 (3.2%) received benzodiazepines and 91 (22.1%) patients received anticholinergic drug trihexyphenidyl with antipsychotics (Table 3).
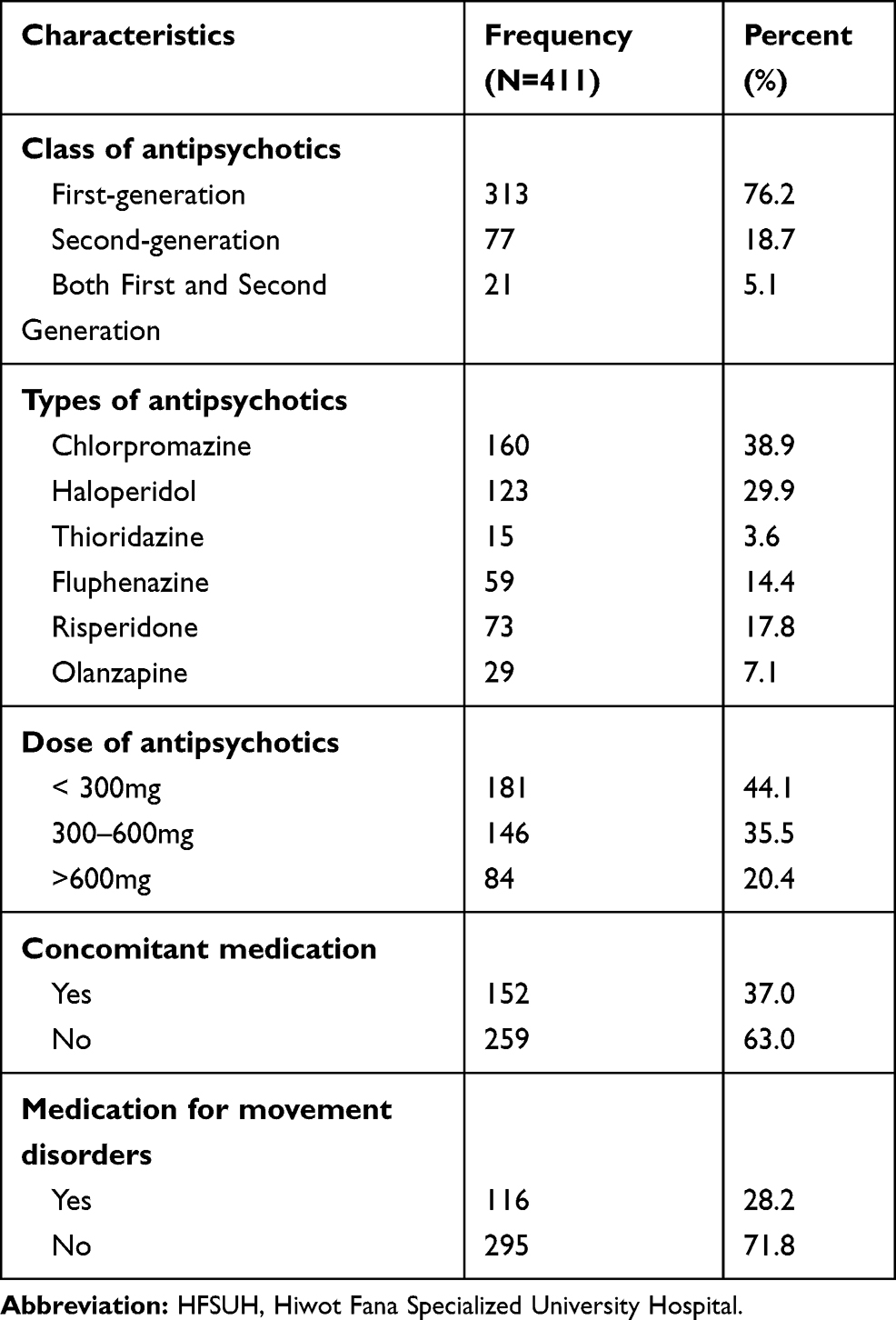 |
Table 3 Medication-Related Characteristics of Participants Who Were on Follow-Up at HFSUH and Jugal Hospital, 2018 |
Substance-Related Characteristics of Participants
From the total study participants, 242 (58.9%) had used the substance at least once during their lifetime and 168 (40.8%) were taking substances in the last 3 months before the study.
Prevalence of Drug-Induced Movement Disorders
The prevalence of drug-induced movement disorders was 44% (CI 95%: 39.2, 48.7) – of this, drug-induced Parkinsonism 112 (27.3%) (CI 95%: 23.1, 31.4), drug-induced akathisia 87 (21.2%) (CI 95%: 17.3, 25.3), drug-induced tardive dyskinesia 39 (9.5%) (CI 95%: 6.8, 12.4) and drug-induced tardive dystonia 14 (3.4%) (CI 95%: 1.7, 5.4), respectively
Clinical Global Impression of Severity of Drug-Induced Movement Disorders
Among patients having pseudo-Parkinsonism, 37.5% (n= 42) of the patients had a CGI-S score of 4 or 5 (moderate to moderately severe), whereas 29.9% (n = 26) of those with Akathisia had a sign with this degree of severity as shown in Table 4.
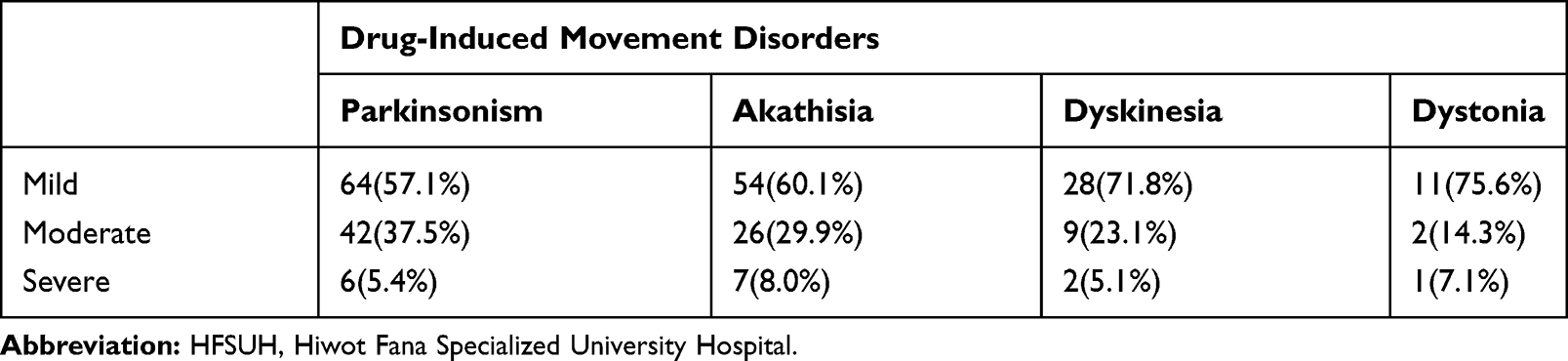 |
Table 4 Severity of Extrapyramidal Signs Related to Antipsychotic Exposure Among Patients Treated at HFSUH and Jugal Hospital, 2018 |
Factors Associated with Drug-Induced Movement Disorders
Multivariate analysis of drug-induced pseudo-Parkinsonism revealed that female patients (AOR=3.6, 95% CI: 2.03, 6.35), age range between 30 and 44 yr (AOR=2.91, 95% CI: 1.41, 5.9) and age ≥ 45 yr (AOR=5.1, 95% CI: 2.48, 10.41), being treated by FGAs (AOR=2.8, 95% CI: 1.8, 5.0), long duration of treatment (AOR=2.2, 95% CI: 1.97, 5.13), high chlorpromazine equivalent dose (AOR=2.0, 95% CI: 1.05, 4.0) and having a family history of primary movement disorders (AOR= 2.43, 95% CI: 1.86, 6.2) were factors statistically significant.
Multivariate analysis of drug-induced akathisia revealed that female patients (AOR=4.9, 95% CI: 2.73, 8.78), age range between 30 and 44 yrs (AOR=1.96, 95% CI: 1.03, 3.71) having a diagnosis of major depressive disorder (AOR= 2.66, 95% CI: 1.2, 5.7), being treated with FGAs (AOR=2.67, 95% CI: 1.1, 6.5) and high chlorpromazine equivalent dose (AOR= 2.6, 95% CI: 1.7, 4.9) were factors remained to be associated with akathisia.
Multivariate analysis of drug-induced tardive dyskinesia revealed that; patients with age ≥45 yrs (AOR=2.39, 95% CI: 1.07, 6.38), female patients (AOR=2.51, 95% CI: 1.08, 5.86), having a diagnosis of major depressive disorder (AOR= 2.71, 95% CI: 1.81, 9.02) and bipolar disorder (AOR=5.54, 95% CI: 1.39, 22.0), high chlorpromazine equivalent dose (AOR= 2.69, 95% CI: 1.05, 6.87), long duration of treatment (AOR= 5.7, 95% CI: 1.40, 23.14) and using alcohol (AOR= 5.89, 95% CI: 2.20, 15.69) were factors remained to be statistically significant.
During the multivariate analysis of drug-induced tardive dystonia, male patients (AOR=4.6, 95% CI: 1.8, 18.5), between15–29 (AOR=5.2, 95% CI: 1.4, 8.8) and high chlorpromazine equivalent dose (AOR= 5.2, 95% CI: 1.05, 25.7) were factors remained to be statistically significant as summarized in Table 5.
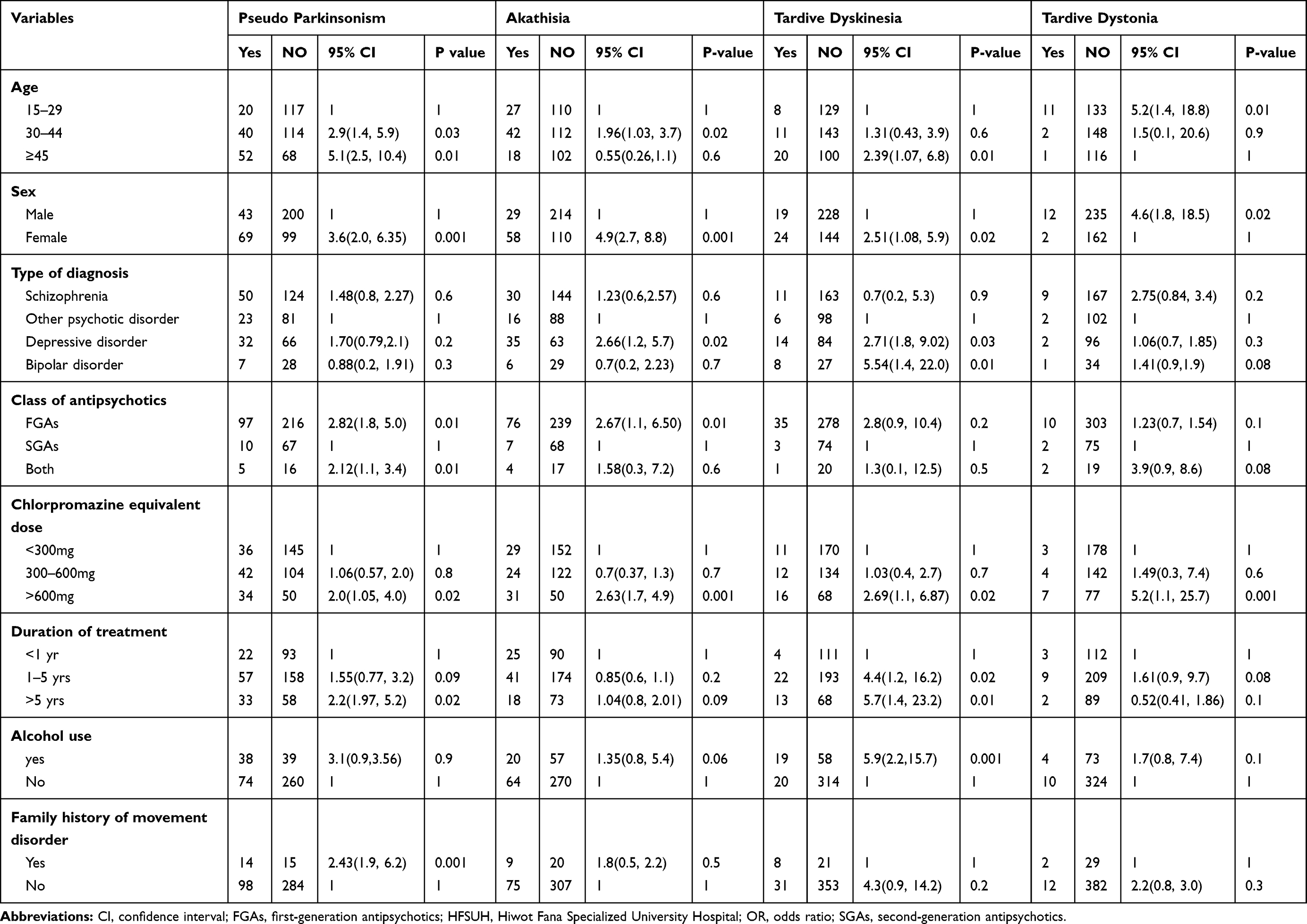 |
Table 5 Factors Associated with Drug-Induced Movement Disorders During Multivariate Analysis Among Patients Taking Antipsychotics at HFSUH and Jugal Hospital, 2018 |
Discussion
The prevalence of drug-induced movement disorders in this study was 44% (CI 95%: 39.2, 48.7) which not surprising us because mostly, it is noted by the clinicians and nurses before the study started. Most of the patients feel those movement disorders as odd and complained that they do not want to take any psychotropic medication. The result was lower than previous studies done in the United Kingdom (65%),24 Netherlands,17 Estonian (61.6%)25 and Ethiopia (56%)19 and it was higher than the study done in 11 countries (30.4%).26 This discrepancy might be due to the difference in the study setting, clinical rating scale, the variability of the disorders, types of antipsychotic exposure, and daily drug dosage. But it was in line with the study done in Netherland (43.3%).27
Female patients were significantly associated with drug-induced Parkinsonism (AOR=3.6, 95% CI: 2.03, 6.35). This was supported by a study done in Europe28 and Estonia.3 The possible reason for the association could result from the fact that the striatal dopaminergic and possibly cholinergic systems are under regulatory control by estrogen and that in females the balance between these two neurotransmitter systems in the striatum may be shifted toward higher cholinergic activity, a state that favors the development of EPS in women”.29 Patients with an age range between 30 and 44 yrs were 2.9 times and ages ≥45 yrs were 5 times more likely to develop pseudo-Parkinsonism as compared to those patients age range between15–29. This was in line with other studies done in Europe28 and brazil.30
Those patients who treated by FGAs were significantly associated with pseudo-Parkinsonism. The possible explanation could be due to the high binding of FGAs on D2 receptors and the rapid dissociation of SGAs from D2 receptors. Being treated for ≥5 yrs (AOR=2.23, 95% CI: 1.97, 5.13) was a significant association with pseudo-Parkinsonism. This was in line with a study done in Canada.31 Chlorpromazine equivalent dose >600mg/day was significantly associated with pseudo Parkinsonism (AOR= 2.05, 95% CI: 1.05, 4.00). This was consistent with other studies done.19,32
The existence of primary movement disorders in the family especially in first degree relatives was also associated with pseudo-Parkinsonism (AOR= 2.43, 95% CI: 1.86, 6.17). It may be due to the hereditary transmission of Parkinsonism. This was in agreement with a study done in the USA33 and Austria.34
Patients with an age range between 30 and 44 yrs were significantly associated with drug-induced akathisia. The possible reason could result from hormonal deregulation during middle age. This was consistent with other studies done in Netherland.35 The odds of developing akathisia among female patients were 4.9 times higher as compared to male patients. This was consistent with the study done in the UK.36 The odds of developing akathisia among patients with a diagnosis of major depressive disorder were 2.7 times higher as compared to those patients having a diagnosis of other psychotic disorders. The possible reasons could be results from the fact that the rates of EPS would increase when some antidepressants are combined with SGAs. This was supported by other studies done.37,38
Those patients who treated with FGAs were 2.7 times more likely to develop akathisia as compared to those patients treated with SGAs. This was consistent with other studies.39 Patients treated by dose >600 mg daily were significantly associated with akathisia. This was consistent with another study done in Ethiopia.19
Patients age ≥45 yrs were 2.4 times more likely to develop TD as compared to those patients age range between 15 and 29. This was supported by other studies.28,40 The odds of developing TD among female patients were 2.5 times higher as compared to male patients. This was consistent with the study done in India.41
Having the diagnosis of major depressive disorder and bipolar disorder was significantly associated with TD. This was supported by a study done in South Africa.42 Drinking alcohol was also significantly associated with the development of TD. The possible reason could be due to the “diffuse and subclinical neurotoxic effects of alcohol exposure in neuroleptic-treated patients may increase vulnerability to TD”43 This was consistent with previous studies done in the Netherlands28 and Ethiopia.19
Male patients were significantly associated with drug-induced tardive dystonia. This was consistent with other studies done in 14 European countries.44 Those patients aged between15–29 were 5.2 times more likely to develop tardive dystonia as compared to those aged ≥45 yrs. Being on chlorpromazine equivalent dose ≥ 600 mg per day was also significantly associated with tardive dystonia. This was supported by other studies done in Netherland44 and Korea.8
Conclusions
In this study, drug-induced movement disorder was high and nearly half of patients on antipsychotic treatment were experiencing antipsychotics-induced movement disorders. Age, sex, and chlorpromazine equivalent doses were associated with all of the types of drug-induced movement disorders. Older age and female sex were associated with pseudo-Parkinsonism and TD. Middle age and females were associated with akathisia, whereas being younger and a male was associated with tardive dystonia. Current alcohol use was significantly associated with TD.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; ESRS, extrapyramidal symptom rating scale; FGAs, first-generation antipsychotics; HFSUH, Hiwot Fana Specialized University Hospital; OPD, outpatient department; SGAs, second-generation antipsychotics; TD, tardive dyskinesia.
Ethical Consideration
The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical clearance was obtained from the Ethical Review Committee 15 of Amanuel Mental Specialized Hospital with the approval number of Am/14614/214. Written consent was obtained from the participants after they were informed about the importance of their participation and all procedures were explained. The informed assent was obtained from adolescents aged below 18 and consent from the caregiver of the adolescent. Privacy and confidentiality of information given by each respondent were kept properly. Those study participants suffering from side effects were referred to OPD for treatment.
Acknowledgments
We thank the University of Gondar and Amanuel Mental Specialized Hospital for financial support.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspect of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Owens DC. A guide to the extrapyramidal side effects of antipsychotic drugs. Cambridge University Press; 1999.
2. Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS drugs. 2002;16(1):23–45. doi:10.2165/00023210-200216010-00003
3. Factor SA, Lang AE, Weiner WJ. Drug-induced movement disorders. Wiley Online Library; 2005.
4. Janno S, Holi MM, Tuisku K, Wahlbeck K. Neuroleptic-induced movement disorders in a naturalistic schizophrenia population: diagnostic value of actometric movement patterns. BMC Neurol. 2008;8(1):10. doi:10.1186/1471-2377-8-10
5. Janno S, Holi MM, Tuisku K, Actometry WK. Barnes Akathisia Rating Scale in neuroleptic-induced akathisia. Eur neuropsychopharmacol. 2005;15(1):39–41. doi:10.1016/j.euroneuro.2004.05.003
6. Correll CU, Schenk EM. Tardive dyskinesia and new antipsychotics. Curr Opin Psychiatry. 2008;21(2):151–156. doi:10.1097/YCO.0b013e3282f53132
7. Chen J, Gao K, Kemp DE. Second-generation antipsychotics in major depressive disorder: update and clinical perspective. Curr Opin Psychiatry. 2011;24(1):10–17. doi:10.1097/YCO.0b013e3283413505
8. Lee M-J, Lin P-Y, Chang -Y-Y, Chong M-Y, Lee Y. Antipsychotics-induced tardive syndrome: a retrospective epidemiological study. Clin Neuropharmacol. 2014;37(4):111–115. doi:10.1097/WNF.0000000000000040
9. Stegmayer K, Walther S, van Harten P. Tardive dyskinesia associated with atypical antipsychotics: prevalence, mechanisms, and management strategies. CNS drugs. 2018;32(2):135–147. doi:10.1007/s40263-018-0494-8
10. Tenback DE, Van Harten PN, Slooff CJ, Van Os J, Group SS. Evidence that early extrapyramidal symptoms predict later tardive dyskinesia: a prospective analysis of 10,000 patients in the European Schizophrenia Outpatient Health Outcomes (SOHO) study. Am J Psychiatry. 2006;163(8):1438–1440. doi:10.1176/ajp.2006.163.8.1438
11. Chakos MH, Alvir JMJ, Woerner MG, et al. Incidence and correlates of tardive dyskinesia in the first episode of schizophrenia. Arch Gen Psychiatry. 1996;53(4):313–319. doi:10.1001/archpsyc.1996.01830040049009
12. Strous RD, Alvir JMJ, Robinson D, et al. Premorbid functioning in schizophrenia: relation to baseline symptoms, treatment response, and medication side effects. Schizophr Bull. 2004;30(2):265–278. doi:10.1093/oxfordjournals.schbul.a007077
13. de Araújo AA, de Araújo Dantas D, Do Nascimento GG, et al. Quality of life in patients with schizophrenia: the impact of socio-economic factors and adverse effects of atypical antipsychotics drugs. Psychiatric Quarterly. 2014;85(3):357–367. doi:10.1007/s11126-014-9290-x
14. Oosthuizen PP, Emsley RA, Maritz JS, Turner JA, Keyter N. Incidence of tardive dyskinesia in first-episode psychosis patients treated with low-dose haloperidol. J Clin Psychiatry. 2003;64(9):1075–1080. doi:10.4088/JCP.v64n0913
15. Chouinard G, Annable L, Ross-Chouinard A, Mercier P. A 5-year prospective longitudinal study of tardive dyskinesia: factors predicting the appearance of new cases. J Clin Psychopharmacol. 1988;8(4 Suppl):21S–26S. doi:10.1097/00004714-198808001-00005
16. Tenback DE, van Harten PN, Slooff CJ, van Os J, Group SS. Worsening of psychosis in schizophrenia is longitudinally associated with tardive dyskinesia in the European Schizophrenia Outpatient Health Outcomes Study. Compr Psychiatry. 2007;48(5):436–440. doi:10.1016/j.comppsych.2007.05.003
17. van Harten PN, Matroos GE, Hoek HW, Kahn RS. The prevalence of tardive dystonia, tardive dyskinesia, parkinsonism, and akathisia The Curacao Extrapyramidal Syndromes Study: I. Schizophr Res. 1996;19(2–3):195–203. doi:10.1016/0920-9964(95)00096-8
18. Bakker PR, de Groot IW, van Os J, van Harten PN. Long-stay psychiatric patients: a prospective study revealing persistent antipsychotic-induced movement disorder. PLoS One. 2011;6(10):10. doi:10.1371/journal.pone.0025588
19. Taye H, Awoke T, Ebrahim J. Antipsychotic medication-induced movement disorders: the case of Amanuel specialized mental hospital, Addis Ababa, Ethiopia. Am J Psychiatry Neurosci. 2014;2(5):76–82. doi:10.11648/j.ajpn.20140205.12
20. Vanasse A, Blais L, Courteau J, et al. Comparative effectiveness and safety of antipsychotic drugs in schizophrenia treatment: a real‐world observational study. Acta Psychiatr Scand. 2016;134(5):374–384. doi:10.1111/acps.12621
21. Andreasen NC, Pressler M, Nopoulos P, Miller D, Ho B-C. Antipsychotic dose equivalents and dose-years: a standardized method for comparing exposure to different drugs. Biol Psychiatry. 2010;67(3):255–262. doi:10.1016/j.biopsych.2009.08.040
22. Chouinard G, Margolese HC. Manual for the extrapyramidal symptom rating scale (ESRS). Schizophr Res. 2005;76(2–3):247–265. doi:10.1016/j.schres.2005.02.013
23. Humeniuk R, Ali R, Babor TF, et al. Validation of the alcohol, smoking, and substance involvement screening test (ASSIST). Addiction. 2008;103(6):1039–1047. doi:10.1111/j.1360-0443.2007.02114.x
24. Hansen LK, Nausheen B, Hart D, Kingdon D. Movement disorders in patients with schizophrenia and a history of substance abuse. Human Psychopharmacol. 2013;28(2):192–197. doi:10.1002/hup.2305
25. Janno S, Holi M, Tuisku K, Wahlbeck K. Prevalence of neuroleptic-induced movement disorders in chronic schizophrenia inpatients. Am J Psychiatry. 2004;161(1):160–163. doi:10.1176/appi.ajp.161.1.160
26. Honer WG, Kopala LC, Rabinowitz J. Extrapyramidal symptoms and signs in first-episode, antipsychotic exposed and non-exposed patients with schizophrenia or related psychotic illness. J Psychopharmacol. 2005;19(3):277–285. doi:10.1177/0269881105051539
27. Bakker PR. Drug-induced movement disorders in long-stay psychiatric patients. 2012.
28. Novick D, Haro JM, Bertsch J, Haddad PM. Incidence of extrapyramidal symptoms and tardive dyskinesia in schizophrenia: thirty-six-month results from the European schizophrenia outpatient health outcomes study. J Clin Psychopharmacol. 2010;30(5):531–540. doi:10.1097/JCP.0b013e3181f14098
29. Miller JC. Sex differences in dopaminergic and cholinergic activity and function in the nigrostriatal system of the rat. Psychoneuroendocrinology. 1983;8(2):225–236. doi:10.1016/0306-4530(83)90059-8
30. Barbosa MT, Caramelli P, Maia DP, et al. Parkinsonism and Parkinson’s disease in the elderly: a community‐based survey in Brazil (the Bambuí study). Mov Disord. 2006;21(6):800–808. doi:10.1002/mds.20806
31. Rochon PA, Stukel TA, Sykora K, et al. Atypical antipsychotics and parkinsonism. Arch Intern Med. 2005;165(16):1882–1888. doi:10.1001/archinte.165.16.1882
32. Estevez-Fraga C, Zeun P, Moreno JLL-S. Current methods for the treatment and prevention of drug-induced parkinsonism and tardive dyskinesia in the elderly. Drugs Aging. 2018;35(11):959–971. doi:10.1007/s40266-018-0590-y
33. Rocca WA, McDonnell SK, Strain KJ, et al. Familial aggregation of Parkinson’s disease: the Mayo Clinic family study. Ann Neurol. 2004;56(4):495–502. doi:10.1002/ana.20228
34. Wenning GK, Kiechl S, Seppi K, et al. Prevalence of movement disorders in men and women aged 50–89 years (Bruneck Study cohort): a population-based study. Lancet neurol. 2005;4(12):815–820. doi:10.1016/S1474-4422(05)70226-X
35. Halliday J, Farrington S, Macdonald S, MacEwan T, Sharkey V, McCreadie R. Nithsdale Schizophrenia Surveys 23: movement disorders: a 20-year review. Br J Psychiatry. 2002;181(5):422–427. doi:10.1192/bjp.181.5.422
36. Sachdev P. The epidemiology of drug-induced akathisia: part II. Chronic, tardive, and withdrawal akathisias. Schizophr Bull. 1995;21(3):451–461. doi:10.1093/schbul/21.3.451
37. Go CL, Rosales RL, Caraos RJ, Fernandez HH. The current prevalence and factors associated with tardive dyskinesia among Filipino schizophrenic patients. Parkinsonism Relat Disord. 2009;15(9):655–659. doi:10.1016/j.parkreldis.2009.02.015
38. Potvin S, Pampoulova T, Mancini-Marie A, Lipp O, Bouchard R, Stip E. Increased extrapyramidal symptoms in patients with schizophrenia and a comorbid substance use disorder. J Neurol Neurosurg Psychiatry. 2006;77(6):796–798. doi:10.1136/jnnp.2005.079228
39. Hunt N, Silverstone T. Tardive dyskinesia in bipolar affective disorder: a catchment area study. Int Clin Psychopharmacol. 1991;6(1):45–50. doi:10.1097/00004850-199100610-00006
40. Bakker P, Van Harten P, Van Os J. Antipsychotic-induced tardive dyskinesia and polymorphic variations in COMT, DRD2, CYP1A2, and MnSOD genes: a meta-analysis of pharmacogenetic interactions. Mol Psychiatry. 2008;13(5):544–556. doi:10.1038/sj.mp.4002142
41. Silpa KS, Aparna S, Pradeep P, Krishna NM. Drug safety evaluation of antipsychotics in schizophrenia: a prospective observational study in a tertiary care hospital. World J Pharm Res. 2015;4:1472–1481.
42. Patterson BD, Swingler D, Willows S. Prevalence of and risk factors for tardive dyskinesia in a Xhosa population in the Eastern Cape of South Africa. Schizophr Res. 2005;76(1):89–97. doi:10.1016/j.schres.2004.10.009
43. Dixon L, Weiden PJ, Haas G, Sweeney J, Frances AJ. Increased tardive dyskinesia in alcohol-abusing schizophrenic patients. Compr Psychiatry. 1992;33(2):121–122. doi:10.1016/0010-440X(92)90008-E
44. Van Rossum I, Tenback D, van Os J. Bipolar disorder and dopamine dysfunction: an indirect approach focusing on tardive movement syndromes in a naturalistic setting. BMC psychiatry. 2009;9(1):16. doi:10.1186/1471-244X-9-16
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.