Back to Journals » Drug Design, Development and Therapy » Volume 19
Drug Delivery Systems Targeting the Knee Microenvironment: A Prospective Strategy for Knee Osteoarthritis Treatment
Authors Xia Y ![]() , Zhou Y, Liang B, Guo Y, Dai R, Ruan Z, Wang W, Zhou X, Li X, Wang T
, Zhou Y, Liang B, Guo Y, Dai R, Ruan Z, Wang W, Zhou X, Li X, Wang T
Received 3 September 2025
Accepted for publication 21 November 2025
Published 11 December 2025 Volume 2025:19 Pages 10909—10935
DOI https://doi.org/10.2147/DDDT.S564907
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas D. Panos
Yubo Xia,1,* Yang Zhou,2,3,* Boshen Liang,4,* Ying Guo,1,* Rong Dai,5 Ziliang Ruan,1 Wei Wang,6 Xiaohan Zhou,1 Xiufang Li,5 Tao Wang1
1Third Affiliated Hospital, Yunnan University of Chinese Medicine, Kunming, People’s Republic of China; 2First Clinical Medical College,Yunnan University of Chinese Medicine, Kunming, People’s Republic of China; 3Joint Graduate School of Traditional Chinese Medicine of China, Suzhou, People’s Republic of China; 4Guang zhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 5College of Traditional Chinese Materia Medica,Yunnan University of Chinese Medicine, Kunming, People’s Republic of China; 6Department of Cardiology, The Second People’s Hospital of Kunming, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiufang Li, College of Traditional Chinese Materia Medica,Yunnan University of Chinese Medicine, Kunming, People’s Republic of China, Tel +86-13908856005, Email [email protected] Tao Wang, Third Affiliated Hospital,Yunnan University of Chinese Medicine, Kunming, People’s Republic of China, Tel +86-13648800064, Email [email protected]
Abstract: Knee osteoarthritis (KOA) is a degenerative condition of the joints marked by the gradual deterioration of cartilage, inflammation, and pain, impacting millions globally. Treatment approaches for KOA encompass both surgical and non-surgical methods aimed at alleviating symptoms and enhancing functionality rather than providing a cure. Recent research into the mechanisms of osteoarthritis (OA) has highlighted the significance of the knee joint’s microenvironment in the success of drug delivery, particularly with intra-articular therapies. A notable approach involves intra-articular (IA) injections, which allow for the targeted administration of medications directly into the joint area. Nevertheless, traditional treatments often fall short in effectiveness due to the limited bioavailability of drugs within the joint, quick clearance rates, and potential systemic side effects. Consequently, innovative drug delivery systems (DDS) that focus on the knee joint’s microenvironment have emerged as a viable method to enhance treatment efficacy and improve patient outcomes. Additionally, drug delivery systems utilizing nanotechnology have shown advantages such as precise targeting, minimized systemic toxicity, and extended therapeutic effects in treating diseases. Gaining insight into these interactions is crucial for developing optimized drug delivery systems that can improve treatment results for individuals with knee disorders. This article examines the latest developments in nanotechnology-based therapies for KOA and explores future directions for enhancing and refining treatment strategies for this condition.
Keywords: knee osteoarthritis, drug delivery systems, nanotechnology, hydrogel, microspheres, exosomes, NF-κB, extracellular matrix degradation
Introduction
Osteoarthritis1 (OA) is a progressive condition linked to factors like age and excess weight. It primarily involves the deterioration of joint cartilage and the enlargement of joint edges, often accompanied by hardening of the bone beneath the cartilage, inflammation of the synovial membrane, and damage to nearby soft tissues. Recent data indicates a swift increase in the aging population globally.2 Around 10–20% of individuals over the age of 60 are affected by osteoarthritis, making it a significant public health concern that results in pain and reduced mobility. KOA represents a substantial part of the overall OA burden, with its incidence rising annually. Currently, the global rate stands at 203 cases per 10,000 person-years for those aged 20 and above.3 As the aging population grows,4 the occurrence of KOA escalates with age, positioning it as the 11th leading cause of disability worldwide. This highlights the urgent need for effective strategies for management and prevention to tackle this escalating health issue.5
KOA is a complex degenerative disorder marked by deterioration of the articular cartilage and involving all components of the joint. It typically affects the entire knee joint, including the articular cartilage, synovial membrane, subchondral bone, menisci, ligaments, as well as the infrapatellar fat pad, with contributions from metabolic factors, abnormal mechanical stress, and oxidative damage.6–9 Treating KOA poses significant challenges due to the limited ability of articular cartilage to heal itself.10 Recent advancements in imaging techniques have uncovered that changes within the joint’s biostructure in KOA patients can alter the microarchitecture of the subchondral bone,11 leading to disrupted normal connections and abnormal interactions among sensory neurons.12 Therefore, preserving the microenvironment of articular cartilage may be crucial for preventing and managing KOA.13 Current management strategies for KOA include patient education, nonsteroidal anti-inflammatory medications, physical rehabilitation, and surgical interventions for advanced cases, with intra-articular injections being a common treatment option. However, research indicates that while these injections may provide temporary relief, their effectiveness is limited due to the rapid clearance of therapeutic agents from synovial fluid and their difficulty in penetrating the dense cartilage matrix. The avascular nature and low metabolic rate of articular cartilage, combined with its dense extracellular matrix, not only heighten its vulnerability to degeneration but also hinder drug absorption and retention. Additionally, the cartilage’s structure, characterized by a dense network of type II collagen and proteoglycans, creates a mechanical barrier that restricts the effectiveness of conventional medications. Given the pathological features of the joint microenvironment in osteoarthritis, drug delivery systems utilizing nanotechnology present a promising avenue with innovative design approaches.14,15 Nanomaterials exhibit excellent biocompatibility and biodegradability, causing minimal side effects, and can replicate the structure and function of bone tissues,16–18 promoting the proliferation and differentiation of osteoblasts to enhance bone regeneration and repair. By adjusting the size, shape, and surface characteristics of nanomaterials, including the incorporation of therapeutic agents, drugs can be effectively targeted to the affected area, improving their bioavailability and therapeutic impact while minimizing toxicity.19 This paper reviews the pathological features of the knee OA microenvironment and recent drug delivery strategies tailored to this context, such as passive and active targeting, as well as physicochemical-assisted methods. We summarize the latest developments in these strategies, evaluate their safety and effectiveness, and address the current challenges related to targeting, delivery efficiency, biocompatibility, and immune responses. Finally, we explore future directions for drug delivery systems aimed at knee OA, aiming to provide new insights and innovative strategies for disease-modifying therapies.
Methods: A comprehensive literature search was performed in PubMed, Web of Science, and Scopus (through March 2025) for English-language articles related to KOA and intra-articular drug delivery systems. Search terms included combinations of “knee osteoarthritis”, “osteoarthritis”and keywords such as “intra-articular”, “drug delivery”, “nanoparticle”, “microsphere”, “hydrogel” and “exosome”. No date restrictions were applied, but emphasis was placed on recent studies (2010–2025) and seminal earlier works. Titles and abstracts were screened to identify relevant articles, and full texts of potentially eligible studies were assessed for inclusion. We included original research and review articles focusing on targeted or sustained delivery systems to the knee joint or its microenvironment. Excluded were non-English publications and studies not related to knee OA drug delivery (eg systemic therapies or other joints). Two authors independently conducted the screening and selection; disagreements were resolved by discussion. Because this is a narrative review, no formal quality assessment or meta-analysis was performed.
The Role of Knee Microenvironment in KOA
Knee osteoarthritis (KOA) is increasingly understood as a disease affecting the entire joint rather than merely a result of cartilage degradation.20 It encompasses various elements of the knee joint, including cartilage, synovium, subchondral bone, and their intricate interactions within the microenvironment. Typically, the cells within the joint, along with the matrix and immunometabolic elements, work together to sustain a stable environment. However, when this balance is disturbed, it can lead to an excess of catabolic processes over synthesis, as well as an imbalance between pro-inflammatory and anti-inflammatory responses, initiating the pathological progression of KOA. Recent research highlights that factors within the microenvironment, such as inflammation, metabolic issues, and mechanical stress, play a crucial role in the onset of KOA.21
The knee microenvironment plays a crucial role in KOA pathology, with its intricate biophysical and biochemical characteristics significantly influencing essential pathological features like cartilage deterioration, inflammation of the synovial membrane, and changes in subchondral bone structure. This environment is made up of various cell types, matrix elements, and active signaling molecules, where notable imbalances in these components are observed during the progression of KOA, highlighting an important opportunity for targeted treatment (refer to Figure 1).
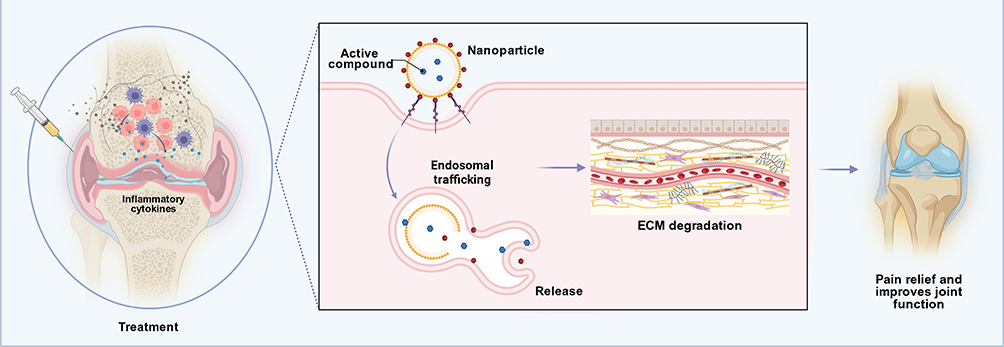 |
Figure 1 Nanoparticle-Based Targeted Therapeutic Strategies and Mechanistic Insights in Knee Osteoarthritis. Schematic representation of a nanoparticle-based targeted therapy strategy for knee osteoarthritis. Intra-articular injection of therapeutic nanoparticles into the osteoarthritic knee ensures localized delivery within the inflamed joint. Created with BioRender. Within this inflammatory microenvironment (rich in pro-inflammatory cytokines), the nanoparticles are internalized by resident cells via endosomal trafficking pathways and subsequently release their active compound intracellularly. The released therapeutic agent attenuates inflammation and inhibits cartilage extracellular matrix (ECM) degradation, thereby protecting joint tissues from further degenerative changes. This targeted intervention ultimately provides pain relief and improves joint function, leading to significant symptomatic improvement in the osteoarthritic knee. |
Pathological Interactions Between Cellular Components and Signaling Networks
The microenvironment of the knee consists primarily of chondrocytes, synovial fibroblasts (FLS), macrophages, mesenchymal stem cells (MSCs), and a rich extracellular matrix (ECM). Chondrocytes, which are the key functional cells in cartilage, play a crucial role in maintaining ECM balance, with their metabolic activity heavily influenced by mechanical stress and local signaling factors.22 Synovial fibroblasts are involved in inflammatory processes by releasing cytokines and proteases into the synovial space.23 Additionally, in KOA, macrophages display different polarization states: the pro-inflammatory M1 macrophages produce high levels of inflammatory mediators that lead to tissue damage, while the anti-inflammatory M2 macrophages facilitate tissue repair and remodeling.24 The interactions among these components are interdependent, working together through paracrine signaling and direct contact. The ECM supports chondrocyte growth, and in turn, chondrocytes secrete matrix components to uphold structural integrity, creating a feedback loop between chondrocytes and the ECM.25,26 Furthermore, exosomal miRNAs released by MSCs can encourage macrophages to adopt an M2 phenotype, establishing an anti-inflammatory repair feedback mechanism between MSCs and macrophages.27–29 Nutrients such as ascorbic acid (vitamin C) and IGF-I present in synovial fluid support cartilage health by diffusing to enhance metabolic efficiency during exercise, thereby forming a trophic chain system between synovial fluid and cartilage.30,31
The pathological mechanism underlying KOA involves a detrimental cycle initiated by disrupted interactions between synovial fluid and cartilage. This leads to synovial tissue proliferation and inflammation, characterized by neovascularization, macrophage and fibroblast-like synoviocyte infiltration, and the release of pro-inflammatory mediators32 These changes promote cartilage degradation and sustain inflammation. Additionally, synovial fluid becomes acidic due to accumulated metabolites like lactic acid, exacerbating joint pain and reducing the efficacy of pH-sensitive drugs.33 Meanwhile, the collagen–proteoglycan framework of articular cartilage undergoes progressive breakdown, leading to surface fissures. The altered microenvironment causes chondrocytes in deeper layers to undergo hypertrophy and apoptosis, and even alters the biomechanical phenotype of chondrocytes (eg, their mechanotransduction responses become abnormal), further accelerating KOA progression.32
Beyond the interactions between synovial fluid and cartilage, the pathological relationship between cartilage and the underlying subchondral bone plays a crucial role in the microenvironment of knee osteoarthritis (KOA). In osteoarthritis, the cells within the subchondral bone, including osteoblasts and osteoclasts, experience both functional and phenotypic alterations, leading to the release of bioactive substances that can affect cartilage metabolism.33 Research by Lajeunesse and associates revealed that substances such as prostaglandins, leukotrienes, and growth factors generated by osteoblasts in the subchondral bone can penetrate the calcified layer of the articular cartilage.34 Additionally, exosomes from these osteoblasts are capable of traversing the osteochondral boundary to interact with chondrocytes. Furthermore, the degradation products of the cartilage matrix and various stressors can influence the remodeling of subchondral bone. When cartilage sustains significant damage, mechanical stress is increasingly transferred to the subchondral bone, which can lead to the proliferation of osteoclasts and bone sclerosis, as well as the activation of abnormal bone remodeling mediated by osteoblasts.32 Consequently, a complex signaling network is established among the subchondral bone, cartilage, and synovium, with the “bone-cartilage unit” playing a pivotal role in the progression of KOA through the integration of biochemical and mechanical signals.
Numerous disrupted signaling pathways underlie these interactions (refer to Figure 2). NF-κB signaling is a key driver of inflammation in KOA, closely linked to chondrocyte catabolism and synovitis. Persistent NF-κB activation induces synoviocytes and chondrocytes to express inflammatory genes and cartilage-degrading enzymes (such as MMP-1 and MMP-13) in response to IL-1β and TNF-α,35–37 promoting matrix breakdown. Similarly, activation of the MAPK cascade (including JNK, ERK, and p38) generates TNF-α, IL-6, and IL-1β, which further stimulate MMP production and chondrocyte apoptosis.38 Tight control of Wnt/β-catenin signaling is required for joint homeostasis, but excessive Wnt activation in KOA drives chondrocyte hypertrophy and matrix degradation. In particular, synovial fibroblasts and M1 macrophages secrete high levels of the Wnt-activator R-spondin-2, exacerbating cartilage degeneration and aberrant bone formation.39 Finally, inflammatory cytokines such as IL-6 and TNF-α activate the JAK/STAT3 pathway in synoviocytes and macrophages, upregulating MMP-9 and other catabolic mediators, thereby worsening ECM degradation.40
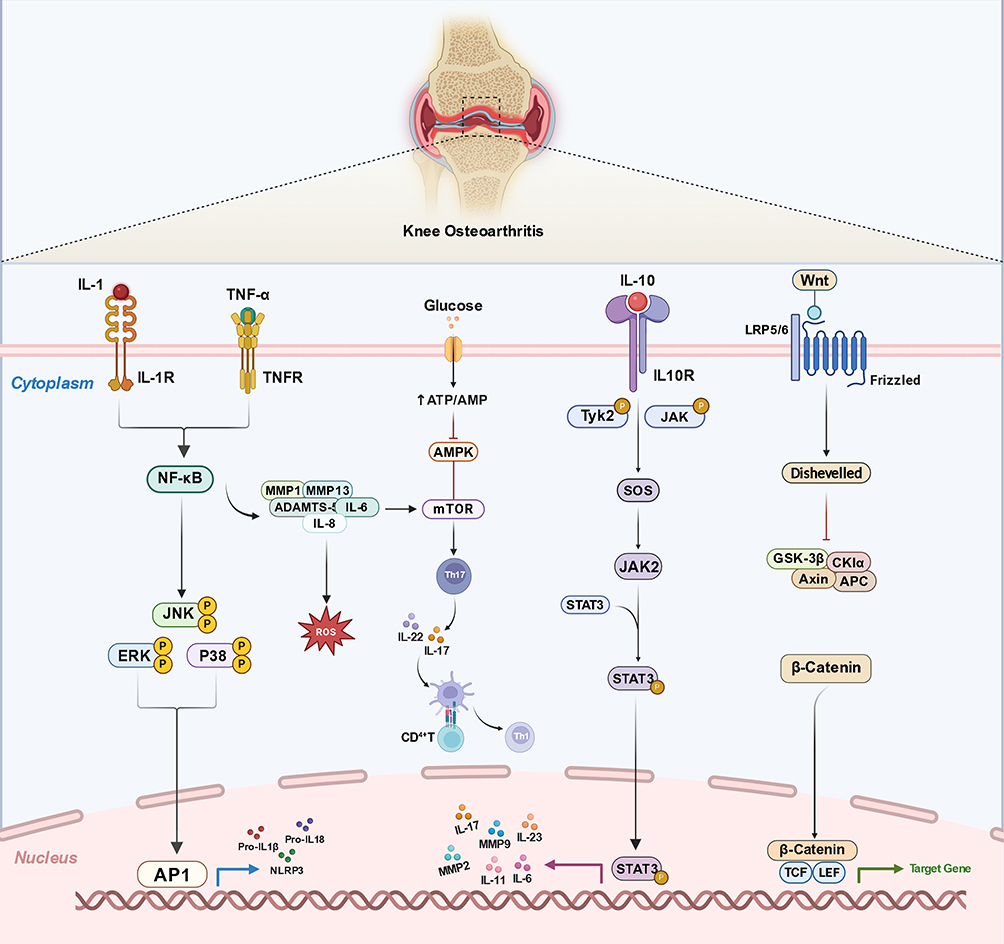 |
Figure 2 Targeted Nanotherapeutic Modulation of the Osteoarthritic Joint Microenvironment: Mechanisms and Delivery Platforms. Core inflammatory, metabolic, and developmental signaling axes that shape the osteoarthritic (OA) joint microenvironment. Created with BioRender. Pro-inflammatory cytokines IL-1 and TNF-α activate IL-1R and TNFR, respectively, converging on NF-κB and the MAPK cascades (ERK, JNK, p38), which drive nuclear AP-1 activation. These pathways induce catabolic enzymes and mediators—including MMP-1, MMP-13, ADAMTS-5, MMP-2/-9, IL-6, IL-8, and the priming of NLRP3 with pro-IL-1β/-IL-18—and amplify oxidative stress (ROS), collectively promoting extracellular matrix (ECM) degradation. Altered glucose metabolism modulates the AMPK–mTOR axis, favoring CD4⁺ T-cell polarization toward Th17 and the production of IL-17 and IL-22, further reinforcing local inflammation. In contrast, the anti-inflammatory cytokine IL-10 engages IL-10R to activate TYK2/JAK–JAK2/STAT3 signaling, culminating in STAT3-dependent transcription of genes that restrain inflammatory responses. The Wnt pathway signals through Frizzled/LRP5/6 and Dishevelled, inhibiting the β-catenin destruction complex (GSK-3β/CKIα/Axin/APC) and allowing β-catenin nuclear translocation to partner with TCF/LEF, thereby regulating context-dependent target genes involved in cartilage homeostasis and remodeling. Together, these pathways orchestrate the balance between catabolic inflammation and reparative programs that determine OA progression. (Arrows depict pathway flow; molecule lists are representative, not exhaustive.). |
The development and advancement of KOA involve a complex pathological network that includes synoviocytes, chondrocytes, subchondral osteoblasts, and immune cells and adipocytes, which communicate through various signaling molecules like cytokines, chemokines, proteases, and exosomes. This interaction disrupts the local immune response and tissue balance within the joint.41 The irregular communication among these elements intensifies the inflammatory and degenerative processes in the joints, which correlates closely with the severity of symptoms and disease progression. Notably, the infrapatellar fat pad (IFP), which functions as an anatomo-functional unit together with the synovium, has now been recognized in our review. In KOA, the IFP becomes inflamed and fibrotic, and it contributes to pain, it secretes pro-inflammatory cytokines that exacerbate joint inflammation, and fibrotic changes in the IFP alter its biomechanical properties, further affecting joint function.42
Dynamic Imbalances in Matrix Components
The extracellular matrix (ECM) found in articular cartilage mainly consists of a framework of type II collagen fibers along with proteoglycans, such as the aggregated proteoglycan Aggrecan. This composition provides the cartilage with essential mechanical characteristics, including tensile strength and compressive elasticity, which are crucial for load support and facilitating smooth joint movement.43 In healthy conditions, chondrocytes within the cartilage are responsible43 for maintaining the ECM’s dynamic balance by breaking down and eliminating the aged matrix while simultaneously producing and replenishing the new matrix, thereby ensuring the stability of the cartilage’s structure and function.
The equilibrium described above is disrupted in the presence of KOA, leading to an imbalance in ECM metabolism where degradation surpasses synthesis. In the initial phase of the lesion, there is a significant depletion of aggregated proteoglycans, an increase in the cartilage matrix’s water content, and a breakdown of the collagen framework, which are key indicators of cartilage deterioration in OA.44 The breakdown of the collagen structure leads to additional loss of proteoglycans that were previously anchored within the matrix, diminishing the matrix’s capacity to retain water and endure mechanical stress. Consequently, the cartilage becomes increasingly overloaded and deformed, which accelerates the damage to collagen fibers. Simultaneously, the chondrocytes’ ability to produce ECM diminishes in the context of inflammation and aging, complicating the replenishment of lost matrix components. The reduced capacity to synthesize matrix molecules like proteoglycans, the weakened anabolic response of aging chondrocytes to growth factors (such as IGF-1), and the disruption of TGF-β signaling (including the inhibition of the Smad pathway and the over-activation of alternative pathways) hinder the normal repair of the cartilage matrix. Additionally, the activity of matrix-degrading enzymes (like MMP-13 and ADAMTS-5) increases, further worsening the imbalance between matrix degradation and synthesis. Ultimately, this leads to a net loss of the cartilage matrix and a gradual decline in structural integrity and function, propelling the progression45 of osteoarthritis.
The imbalance in the extracellular matrix (ECM) is linked to various molecular processes, with the excessive production of enzymes that break down the matrix being a key factor in KOA.46 Chondrocytes and synoviocytes in the joints generate heightened amounts of different proteases that promote ECM breakdown. Among cartilage-degrading enzymes, aggrecan breakdown is mainly mediated by the aggrecanases ADAMTS-4 and ADAMTS-5 (with ADAMTS-5 dominant in mice), whereas type II collagen cleavage is primarily carried out by MMP-13 (collagenase-3).46,47 MMP-13 specifically targets the triple-helix structure of type II collagen, while ADAMTS-4 and ADAMTS-5 are recognized as the main enzymes that cleave aggregated proteoglycans, often referred to as “aggrecanases”. This disruption of proteoglycans leads to the accumulation of degradation products from cartilage matrix components, including fragments of collagen and proteoglycans. Current clinical strategies using single enzyme inhibitors have proven ineffective due to the redundancy of multiple enzymes, indicating that a more holistic approach to regulating upstream signaling is necessary to restore ECM balance effectively.48
The signaling pathways upstream that lead to the disruption of the extracellular matrix (ECM) are significantly altered, with inflammatory mediators and their associated pathways playing a crucial role49,50. The synthesis of the ECM is suppressed by inflammatory agents and the aging of cells.51 Notably high concentrations of inflammatory mediators, such as IL-1β, TNF-α, and IL-6, have been observed in both the synovium and cartilage. These cytokines originate from activated synovial macrophages, fibroblast-like synoviocytes, and chondrocytes, creating a persistent local inflammatory environment.49–51 IL-1β not only prompts chondrocytes to produce degrading enzymes like MMP-13 and ADAMTS-5 but also inhibits the production of type II collagen and aggregated proteoglycans by suppressing the transcription of SOX9 and COL2A1. Conversely, TNF-α enhances the damaging effects of IL-1β and promotes the expression of RANKL, which leads to abnormal remodeling of the subchondral bone and increases stress on the cartilage.52,53 Additionally, IL-6 is involved in cartilage metabolism through both classical and trans-signaling pathways, linking to autophagic metabolic disturbances and intersecting with pathways of autophagy and senescence, which further diminishes the cartilage’s ability to regenerate.54
Pro-inflammatory stimuli rapidly activate the NF-κB and MAPK pathways. For example, TLR2/4 or IL-1R engagement activates the IKK complex, leading to NF-κB (p65/p50) nuclear translocation. NF-κB then drives transcription of genes encoding degradative enzymes (MMP-1, −3, −13, ADAMTS-4/5) while suppressing anabolic genes (Aggrecan, COL2A1).55,56 Concurrently, inflammatory signals and mechanical stress activate MAPKs, culminating in AP-1 activation and further upregulation of degradative enzymes and cytokines.57 Dual inhibition of NF-κB and MAPK pathways has been shown to restore ECM homeostasis, improving the balance between matrix synthesis and degradation.58
In healthy cartilage, Wnt/β-catenin signaling is tightly regulated.59 In KOA, aberrant Wnt activation causes nuclear β-catenin accumulation, which upregulates Runx2, MMP-13, and VEGF, driving chondrocytes toward hypertrophy and catabolism.59,60 By contrast, the TGF-β/SMAD pathway supports the anabolic phenotype; its downregulation or impaired SMAD3 activity reduces cartilage repair. Excess TGF-β signaling in subchondral bone can also induce pathological bone thickening.61,62 The resulting imbalance between Wnt and TGF-β pathways leads to diminished matrix synthesis alongside increased degradation.
In cases of extensive ECM breakdown, fragments of collagen and proteoglycans, along with Tenascin-C and damage-associated molecular patterns (DAMPs) like HMGB1, accumulate in the synovial fluid. These components are detected by pattern recognition receptors (PRRs) such as TLR2/4 and RAGE on synovial and chondrocyte cell surfaces. This recognition activates pathways dependent on MyD88 or the NLRP3 inflammasome, leading to the release of pro-inflammatory cytokines, including IL-1β and IL-18, thereby creating a self-perpetuating cycle of inflammation and catabolism.63,64 Furthermore, the complement system is improperly activated in the synovial fluid of osteoarthritis, resulting in the production of C3a and C5a, which not only attract additional immune cells but also directly enhance the secretion of matrix-degrading enzymes from chondrocytes and fibroblast-like synoviocytes (FLS).65 The dysregulation of innate immunity mediated by DAMPs transforms the ECM imbalance from a localized issue into a continuously escalating pathological process within the microenvironment.
In the microenvironment of KOA, combined inflammatory, mechanical, and metabolic stresses activate signaling pathways (NF-κB, MAPK, Wnt/β-catenin, and senescence-associated routes) that disrupt the ECM balance. Concurrently, ECM fragments and DAMPs trigger innate immunity in a self-perpetuating loop. Understanding this complex signaling network informs multi-targeted therapeutic strategies to restore ECM homeostasis. The link between matrix degradation and metabolic-immune dysregulation will be explored in Synergistic Deterioration of the Metabolic and Immune Microenvironment.
Synergistic Deterioration of the Metabolic and Immune Microenvironment
In the pathological context of KOA, the local metabolic conditions are intricately linked to the immune response, resulting in a detrimental feedback loop. Research indicates that the metabolite composition of synovial fluid in KOA is notably altered, with a marked increase in glycolytic byproducts like lactic acid.66 Factors such as ischemia and hypoxia in cartilage, along with inflammatory triggers, cause chondrocyte metabolism to transition from a balanced state to a “hyperglycolytic state”, leading to excessive lactate production and accumulation in the joint space, which subsequently lowers the pH. In this acidic metabolic environment, lactate functions as a signaling molecule that activates synoviocytes and immune cells, stabilizes pro-inflammatory transcription factors like HIF-1α, and promotes increased glucose uptake and glycolysis. This cycle encourages cells to persistently generate lactate, intensifying the inflammatory response.67 Furthermore, the dysregulation of glucose metabolism and the buildup of lipid metabolites in synovial fluid also influence the immune microenvironment. Elevated glucose levels and advanced glycation end products (AGEs) can stimulate synoviocytes to release inflammatory mediators such as IL-6 and IL-8 through RAGE receptors, triggering localized inflammatory reactions. Additionally, pro-inflammatory signals from hypertrophied subsynovial fat pads and systemic metabolic issues (like obesity and type 2 diabetes) can activate and recruit monocyte-macrophages.68,69 The chronic low-grade inflammation associated with obesity, often referred to as “metabolic inflammation”, results in a higher ratio of M1-type macrophages in the synovium, which produce excessive cytokines, including TNF-α, IL-1β, and IL-6.70 These inflammatory mediators not only inflict direct damage to the cartilage matrix but also stimulate synovial fibroblasts and immune cells to release additional inflammatory factors, leading to increased oxidative stress and compromised mitochondrial function, thereby worsening tissue damage and perpetuating a cycle of metabolic stress and inflammation.71
In KOA chondrocytes, inflammatory cytokines (IL-1β, TNF-α) and hypoxia induce metabolic reprogramming. Activation of mTOR and impaired mitochondrial function shift energy production toward aerobic glycolysis. This increased glycolysis generates high lactate levels,72 lowering extracellular pH and inhibiting collagen II and proteoglycan synthesis. The acidic environment also promotes matrix-degrading enzyme activity, aggravating cartilage breakdown. Concurrently, signs of mitochondrial dysfunction become more pronounced, including structural abnormalities, decreased electron transport chain activity, and an overabundance of reactive oxygen species (ROS). Such mitochondrial impairment hinders chondrocytes’ ability to sustain normal autophagy and proliferation, pushing them towards apoptosis and senescence.73–75 Numerous studies have established a strong link between chondrocyte apoptosis and “inflammatory senescence” with the extent of cartilage damage in KOA.72 Senescent chondrocytes release factors associated with the senescence-associated secretory phenotype (SASP), such as IL-1, IL-6, and MMPs, which further intensify local inflammation and contribute to the degradation of the cartilage matrix.76
Chondrocyte metabolic dysfunctions play a dual role in inflammation, acting as both contributors and victims. Alterations in glucose metabolism and reduced mitochondrial efficiency lead chondrocytes to release increased levels of pro-inflammatory mediators and damage-associated molecular patterns (DAMPs). This process activates nearby synoviocytes and macrophages, which in turn produce inflammatory substances that heighten the metabolic strain on cartilage, establishing a continuous cycle of damage.77 The metabolic environment is crucial in influencing the immune cell types within the joint; in knee osteoarthritis (KOA), synovial macrophages can shift between pro-inflammatory M1 and anti-inflammatory M2 phenotypes, with local metabolic conditions affecting this balance. Environments rich in lactate and low in oxygen favor M1 macrophages, which rely heavily on glycolysis for energy, thus reinforcing their inflammatory characteristics. Conversely, M2 macrophages require fatty acid oxidation and functional mitochondrial oxidative phosphorylation for their activity, and their anti-inflammatory capabilities diminish under energy-limited conditions.76,78 The nutrient-deficient microenvironment in KOA supports the persistence of the pro-inflammatory M1 macrophage phenotype, leading to ongoing release of inflammatory mediators like TNF-α and IL-1β, as well as reactive oxygen species (ROS), which further aggravate cartilage breakdown.79 Additionally, metabolic byproducts from macrophages can serve as immunomodulatory signals. For instance, succinate, an intermediate in the tricarboxylic acid cycle, accumulates in M1 macrophages and enhances inflammatory responses by activating its receptor, SUCNR1, or stabilizing HIF-1α, which prompts increased IL-1β secretion and cartilage damage.80 In contrast, itaconate, produced by macrophages, exerts an anti-inflammatory feedback effect; its external application in arthritis models has been shown to reduce synovial inflammation and cartilage deterioration, highlighting its protective role.81 Nevertheless, in joints with severe degeneration, the generation of anti-inflammatory metabolites like itaconate often fails to offset the strong pro-inflammatory signals driven by “immune metabolites” such as succinate, resulting in sustained inflammation.
Alongside macrophages, the subsets of T-lymphocytes present in the joint are also affected by the surrounding metabolic conditions. In the synovium of individuals with KOA, CD4⁺ T cells can transform into either proinflammatory Th17 cells or anti-inflammatory regulatory T cells (Treg). The low oxygen and elevated glucose levels in the microenvironment trigger the mTOR/HIF-1α signaling pathway in T cells, shifting their metabolism towards glycolysis, which enhances Th17 differentiation and boosts IL-17 production. Concurrently, this metabolic shift hampers the functionality of Treg cells, which rely on oxidative metabolism.82 Research has shown that following joint injury, local IL-17 concentrations rise swiftly, primarily produced by γδ T cells and Th17 cells. Moreover, administering an antibody that neutralizes IL-17 leads to a reduction in the expression of the cell cycle inhibitor Cdkn1a (p21) within the joint, indicating that excessive IL-17 may cause a premature aging phenotype in the cells of the tissue.83 Further investigations have indicated that IL-17 released by Th17 cells can trigger premature senescence in synovial fibroblasts. These senescent cells then secrete increased amounts of proinflammatory factors (such as IL-6 and IL-8) through their senescence-associated secretory phenotypes (SASPs) and emit signals like TGF-β, which encourage the initial CD4⁺ T cells to differentiate into Th17/Th1 instead of Treg.83 Consequently, in the joints of older KOA patients, the abnormal growth of Th17 cells, driven by metabolic imbalances and hypoxic conditions, along with the inflammatory senescence of chondrocytes and synoviocytes, creates a self-perpetuating cycle. In this cycle, proinflammatory substances released by immune cells hasten cellular decline in tissues, which in turn produces SASP factors and damage-associated molecules that further activate immune cells towards an inflammatory state.83 This combined effect of inflammaging and metaflammation in KOA significantly speeds up the degenerative processes occurring in the joints.84
Research in epidemiology indicates that conditions like obesity, classified as metabolic syndromes, greatly elevate the likelihood of developing knee osteoarthritis (KOA). This condition can affect even joints that do not bear weight. Additionally, the aging process diminishes the body’s anti-inflammatory and antioxidant defenses, which together accelerate the onset and progression of KOA.70
In conclusion, the interplay between metabolic dysfunction and immune irregularities within the knee joint significantly contributes to the advancement of KOA. This interplay indicates that when creating a “drug delivery system aimed at the knee joint’s microenvironment”, it is essential to address both metabolic and immune factors concurrently. This approach aims to disrupt the reinforcing cycle of deterioration between the two, allowing for targeted intervention in the specific joint area via an advanced drug delivery system, which is anticipated to effectively interrupt the harmful cycle of metabolism and immunity in KOA.85
Targeted Drug Delivery Strategies and Design Principles
This study aims to methodically illustrate the design principles and potential applications of different targeted drug delivery systems for treating knee osteoarthritis (KOA). The strategies are categorized into four primary types: passive targeting, active targeting, endogenous stimulus-responsive targeting, and exogenous physically-assisted targeting. Additionally, the paper outlines the features, benefits, and drawbacks of each approach (see Table 1 and Figure 3).
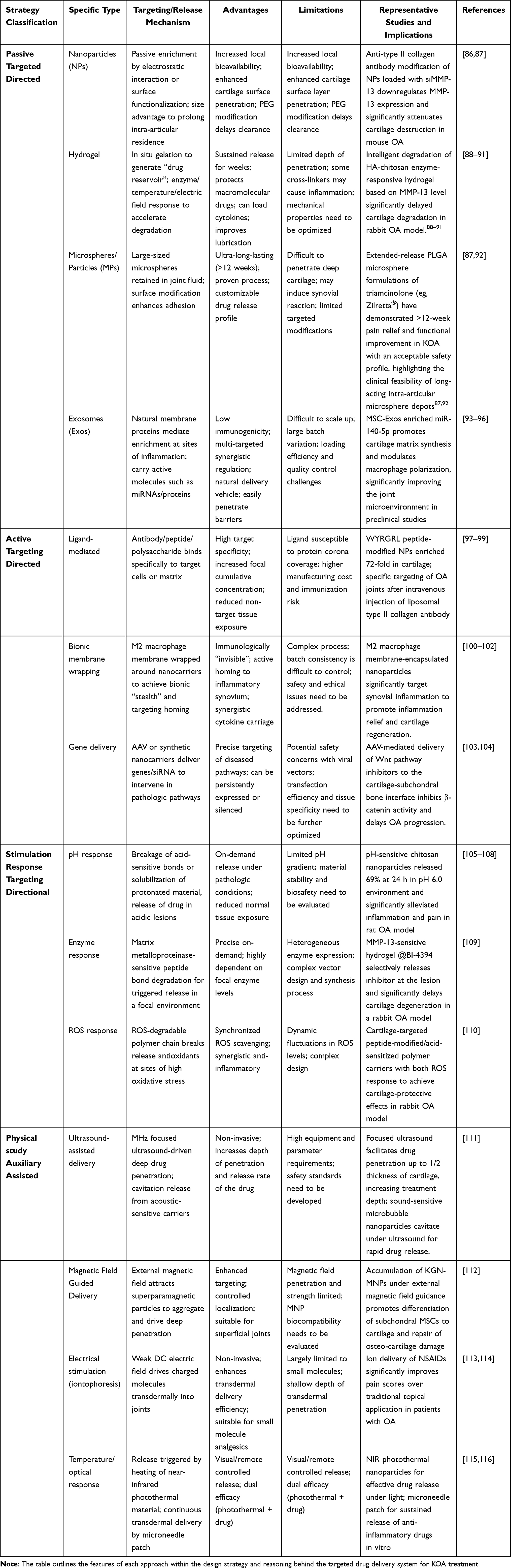 |
Table 1 Classification and Characteristics of Strategies for Targeted Drug Delivery Systems for Knee Osteoarthritis |
 |
Figure 3 Integrated Framework of Microenvironmental Signaling and Nanomedicine-Based Interventions in Osteoarthritis. Landscape of nanotherapeutic platforms and delivery strategies for osteoarthritis (OA). Created with BioRender. The schematic summarizes representative carrier platforms, stimuli‐responsive designs, and targeting paradigms used to enhance intra-articular therapy. Carrier/material platforms include polymeric and lipid systems—liposomes, micelles, PLGA and chitosan nanoparticles—together with inorganic/metal (including superparamagnetic) nanoparticles, nucleic-acid nanostructures (siRNA/mRNA/miRNA carriers and DNAzyme nanoflowers), and biogenic vesicles (exosomes). Hydrogel-based systems (often hybridized with nanoparticles) provide local depot formation and sustained release following intra-articular injection (eg, MMP-13–responsive injectable hydrogels). Stimuli-responsive/exogenous-field–assisted strategies leverage the OA microenvironment or external cues to trigger on-demand release and penetration, including enzyme-responsive and pH-responsive formulations as well as magnetic/photothermal/electrical assistance. Targeting strategies address key joint compartments and cell types: cartilage matrix and chondrocytes, synovial/inflammatory cells (eg, hyaluronic acid–modified liposomes engaging CD44 on macrophages to deliver siRNA), and endothelial cells involved in synovial angiogenesis. Collectively, these platforms aim to concentrate therapeutics within the diseased joint, modulate inflammation, and protect cartilage by improving specificity, retention, and controlled release. (Examples shown are illustrative rather than exhaustive.). |
Passive Targeting Strategy
Passive targeting utilizes the “retention effect” along with the gradual release characteristics of drug carriers within the knee joint. This is achieved by fine-tuning the particle dimensions, configuration, surface charge, and material attributes, enabling the medication to stay in the joint space for an extended period and to be released gradually without the need for a specific ligand.
Nanoparticle-Targeted Delivery Systems
In recent years, nanoparticles (NPs) have emerged as a focal point in the research of drug delivery for knee osteoarthritis (KOA) due to their diminutive size (ranging from 1 to 1000 nm) and extensive surface area. These characteristics allow them to move freely within the joint space and potentially infiltrate tissues like cartilage.117 Various types of nanocarriers are commonly utilized, including polymer-based nanoparticles (such as PLGA, chitosan, and PEG), liposomes, micelles, inorganic nanoparticles (like superparamagnetic iron oxides and silicate nanoparticles), and dendritic macromolecules.118 The primary objective in their design is to achieve targeted delivery and controlled release of therapeutics to knee lesions through functionalization of the materials. For instance, nanoparticles with a positive charge can be attracted to the negatively charged cartilage matrix, enhancing retention in the joint and targeting of the cartilage.97 Research has also explored the addition of specific ligands to the NP surface for active targeting; for example, attaching an anti-type II collagen antibody or a collagen-binding peptide like WYRGRL enables the nanoparticles to selectively attach to exposed collagen in the cartilage,86 facilitating targeted drug release. Similarly, strategies aimed at synovial membranes involve modifying antibodies or peptides that target receptors on inflammatory cells, such as macrophage markers, to deliver anti-inflammatory agents directly to the synovial membrane. Beyond targeting, many nanocarriers are engineered to respond to stimuli, using pathological signals from the OA joint to initiate drug release. For example, pH-sensitive nanoparticles can enhance the release of anti-inflammatory drugs in the acidic environment of the synovium, while reactive oxygen species (ROS)-responsive carriers can break down to release antioxidants in high radical conditions, allowing for on-demand drug delivery at inflammation sites.119 The effectiveness of nano-delivery systems is primarily seen in their ability to enhance local drug bioavailability and tissue penetration. NPs can remain dispersed in joint fluid for extended periods due to their size, which helps prolong the intra-articular half-life of the drug compared to free forms.87 Particularly, when NPs are modified with “stealth” agents like polyethylene glycol, they can evade phagocytosis by synovial macrophages, leading to more sustained drug release. Additionally, nanoparticles sized in the tens to hundreds of nanometers may partially penetrate the cartilage barrier by accessing superficial clefts or diffusing through the cartilage-synovium interface. In animal studies, the delivery of anti-inflammatory drugs or genetic materials via nanocarriers has shown greater efficacy than direct injections. For instance, a study involving antibody-modified NPs targeting type II collagen and carrying siRNA for MMP-13 demonstrated a significant reduction in MMP-13 expression in cartilage, decreased cartilage damage, and outperformed intra-articular hormone injections in a mouse model.120 This “nano+gene therapy” approach highlights the potential for effective delivery of biologics to affected tissues using nanoparticles. Likewise, polymer nanoparticle formulations loaded with anti-inflammatory drugs (such as triamcinolone acetonide and celecoxib) have shown enhanced relief from joint inflammation and better cartilage protection in various animal studies. However, challenges remain, including the rapid clearance of small nanoparticles (especially unmodified hydrophilic ones), limited drug loading capacity per nanocarrier, complex manufacturing processes, and difficulties in ensuring stability and reproducibility. Currently, most nanodrug delivery systems are still in experimental or preclinical phases, with no specific nanoformulations for KOA having been officially marketed. Nevertheless, the dynamic development in this field has generated numerous innovative therapeutic strategies for KOA, with expectations that some will be validated in clinical trials soon.
Hydrogel-Targeted Delivery System
Hydrogels are a type of three-dimensional polymer network capable of absorbing significant amounts of water, resulting in a gel-like substance. Upon injection, these hydrogels can occupy the joint cavity and form a gel on-site, serving as a “drug reservoir” that gradually releases medication, which is an effective strategy for enhancing drug retention in the joint.121 Common materials used for hydrogels in joint applications include both natural polymers, such as hyaluronic acid, gelatin, alginate, and chitosan, as well as synthetic options like PEG, PLGA-PEG, and polyacrylamide, many of which are designed to be biocompatible and biodegradable.88 When creating a hydrogel delivery system, it is essential to manage its gelation characteristics and the behavior of degradation and drug release. For instance, a heat-sensitive hydrogel remains liquid at room temperature but quickly solidifies upon injection due to body heat, adhering to the joint cavity surface to create a depot. Another example is an enzyme-degradable hydrogel that targets the elevated MMP cleavage sites in osteoarthritis joints to regulate its degradation rate and facilitate faster drug release in the affected area.89,90 Additionally, the drug’s diffusion rate can be fine-tuned by modifying the network density, allowing for precise control over the release profile.
The way hydrogels function for delivering treatment to the knee joint primarily involves a localized, gradual release mechanism.122 When injected, the gel occupies the joint space or coats the articular cartilage, which helps to retain the medication and prevents it from being swiftly washed away by joint fluid, thereby sustaining its effective concentration for several days to weeks. Compared to conventional drugs that only last a few hours, hydrogels can be administered less frequently.123 Additionally, these carriers shield the drug from being broken down or rendered inactive by enzymes. For instance, encapsulating proteins or growth factors within a hydrogel enhances their stability and prolonged efficacy in the joint. Recently, various innovative hydrogels have been developed for treating knee osteoarthritis (KOA), such as adhesive hydrogels that enhance retention by incorporating viscoelastic macromolecules or dopamine groups, allowing the gel to adhere more securely to cartilage or synovial surfaces and preventing displacement during joint movement.124 Furthermore, multiple-responsive hydrogels are designed to react to various stimuli like temperature, pH, enzymes, magnetic fields, and reactive oxygen species, enabling them to intelligently modulate drug release based on the inflammatory state of the joint.125 Super-lubricating hydrogels also play a crucial role by significantly lowering friction coefficients, mimicking the lubricating properties of joint fluid through polymer brushes or phospholipid molecules, which not only facilitate drug delivery but also minimize cartilage damage and help slow inflammation progression.126 Notably, the integration of nanoparticles with hydrogels to create nanocomposite hydrogels has gained popularity. These systems leverage the hydrogel for prolonged retention while the nanoparticles enable deeper penetration and targeted release, thus merging the benefits of both approaches.127 For example, research has shown that incorporating cartilage-targeting lipid nanoparticles into an injectable hydrogel can form a composite carrier that effectively delivers drugs aimed at regulating cholesterol metabolism, leading to significant improvements in cartilage damage in osteoarthritis model.128
Hydrogel delivery systems offer notable benefits, including their remarkable slow-release capabilities and favorable biocompatibility. Many natural polymer-based hydrogels possess inherent biological properties that aid in cartilage repair and joint lubrication. For instance, hyaluronic acid gels enhance joint lubrication and alleviate discomfort, making them popular as viscoelastic supplements in clinical settings. Additionally, hydrogels can be infused with a variety of therapeutic agents, such as small molecules, proteins, peptides, nucleic acids, and cellular exosomes, allowing for customized release profiles by adjusting the gel’s characteristics. However, a drawback of standard hydrogels is their lack of active targeting, leading to passive drug diffusion into the target tissue primarily driven by concentration gradients; this can result in inadequate drug penetration for deeper cartilage injuries. Furthermore, some degradation products or cross-linking agents from synthetic gels may trigger inflammatory responses, necessitating further optimization. In summary, hydrogel technology is under extensive investigation in the realm of knee osteoarthritis (KOA), with several products progressing to clinical validation or application. For example, a new injectable polyacrylamide hydrogel, known as Arthrosamid, underwent clinical trials in KOA patients, where a single 6 mL injection led to a significant and lasting reduction in joint pain, enhanced functionality, and a positive safety profile after one year of follow-up.91 This indicates that hydrogel delivery could emerge as a promising long-term and safe treatment alternative for KOA.
Microsphere/Particle-Targeted Delivery Systems
Microspheres, typically defined as spherical carriers ranging from 1 μm to 250 μm in diameter, are commonly constructed from biodegradable polymers like PLGA, gelatin, and chitosan. These carriers can encapsulate small drug molecules or proteins, facilitating a sustained release over time.129 In contrast to nanoparticles, microspheres are larger and tend to persist in joint fluid for extended durations, as they are less prone to entering systemic circulation via synovial microvessels.130,131 Research indicates that particles of suitable size, particularly those a few micrometers in diameter that align with synovial pore dimensions, can significantly prolong joint clearance, thereby extending the drug release period from weeks to months.87 The development of microsphere delivery systems emphasizes the choice of materials and the methods of preparation. For instance, in PLGA microspheres, varying the ratios of lactic acid and glycolic acid copolymers can influence the rate of degradation. Additionally, the size and porosity of the microspheres can be adjusted through emulsification and solvent evaporation techniques to tailor the drug release profile. To enhance targeting capabilities, some microspheres may undergo surface modifications with binding agents, such as collagen-binding peptides or hyaluronic acid, which promote adherence to cartilage defects or synovial surfaces post-injection, thereby improving local drug concentration. Nevertheless, microspheres are predominantly utilized as passive slow-release129 systems rather than as active targeting vehicles, with their primary function being the extended retention and gradual degradation of the drug through size-related mechanisms.
One of the key benefits of microsphere systems in treating KOA is their capacity for sustained effectiveness, a feat that other delivery methods struggle to match. A notable instance is the slow-release formulation of triamcinolone (Zilretta®, which contains 32 mg of triamcinolone within PLGA microspheres) that is available in the United States.92 Clinical studies indicate that Zilretta can release the medication gradually into the joint for over 12 weeks, leading to a significant decrease in average pain levels over a 24-week timeframe, along with enhancements in joint stiffness and functionality. This contrasts sharply with a single injection of traditional triamcinolone crystals, which only alleviates pain for a few weeks.92 The underlying mechanism involves the injection of PLGA microspheres creating a “depot” that steadily releases hormones into the joint fluid, thereby avoiding the peak systemic concentrations that can occur with a large single dose, which in turn minimizes systemic side effects like increased blood glucose levels. This combination of “extended release and reduced systemic exposure” positions microspheres as an optimal method for delivering hormones and analgesics intra-articularly. Similar approaches have been applied to the delivery of other medications, including NSAIDs and inhibitors of inflammatory cytokines. Animal research has consistently shown that microspheres can significantly extend the duration of drug effects and enhance markers of joint inflammation.132–135 However, a drawback of this microsphere approach is their larger size, which limits their ability to penetrate deep into cartilage, primarily affecting the synovial cavity and cartilage surface, with minimal impact on deeper cartilage injuries. Additionally, larger particles may provoke acute inflammatory or foreign body responses, although studies have demonstrated that microspheres of suitable sizes (approximately 10 μm) and made from biodegradable materials are generally well accepted. Overall, microsphere technology has advanced considerably, particularly with PLGA microspheres being available in various FDA-approved formulations. In the KOA domain, alongside Zilretta, several other products are in development, including microspheres containing IL-1 receptor antagonists and small-molecule drugs aimed at cartilage regeneration, currently undergoing clinical trials, which are anticipated to enhance long-acting treatment options.136,137
Exosome Delivery System
Exosomes derived from mesenchymal stem cells (MSC-Exos)–commonly from bone marrow, adipose tissue, synovium, or umbilical cord MSCs, which are tiny extracellular vesicles ranging from 30 to 150 nm in size and released by cells, have emerged as innovative biogenic drug carriers, particularly in the context of degenerative conditions like osteoarthritis, where they offer distinct benefits.138 Unlike artificial nanoparticles, exosomes are naturally synthesized by cells and transport a diverse array of bioactive substances, including proteins, mRNAs, miRNAs, and lipids, facilitating natural cellular interactions. Exosomes derived from mesenchymal stem cells (MSC-Exos) have garnered significant interest in the treatment of knee osteoarthritis (KOA).139 Research indicates that MSC-Exos exert multi-faceted regulatory effects: they influence immune responses in the joint, prevent chondrocyte cell death, and enhance the synthesis of cartilage matrix, thereby improving the overall joint microenvironment.140–142 These beneficial effects are partly due to the active components, such as miRNAs and growth factors,143 found within exosomes, which can alter gene expression and the characteristics of recipient cells. Furthermore, adhesion molecules on the exosome membrane enable their accumulation at inflammation sites and facilitate uptake by target cells, acting as natural “targeted delivery” systems. For instance, synovial macrophages absorb MSC-Exos and shift towards an anti-inflammatory state, while chondrocytes utilize exosomes to boost collagen production and decrease matrix metalloproteinase levels.93–95 Consequently, exosomes hold significant promise for use as therapeutic agents or as carriers for specific drug molecules.
Exosome delivery methods offer several benefits, primarily due to their excellent biocompatibility and minimal immunogenic response. Being derived from autologous or syngeneic cells, exosomes typically integrate into the body without provoking significant immune reactions, ensuring their safety. Additionally, their size, which is in the range of hundreds of nanometers, allows for effective diffusion within joints, aided by specific surface proteins that facilitate their passage through the cartilage-synovial membrane barrier. Furthermore, exosomes inherently carry biological signals that can enhance the treatment of knee osteoarthritis (KOA). For instance, mesenchymal stem cell (MSC) exosomes are abundant in anti-inflammatory microRNA-140-5p and TGF-β, contributing to the remodeling of the joint microenvironment. This intrinsic “self-carrying” characteristic enables them to provide therapeutic benefits without the need for external loading.144 However, exosome delivery faces challenges, such as the efficient extraction and preparation of sufficient exosome quantities, maintaining the stability of their contents, and the need for drug loading or surface modification when necessary. Current techniques for drug loading include incubating the drug within secretory cells or directly incorporating it into purified exosomes via electroporation, though the efficiency and control of these methods are still under refinement. Additionally, variations in the therapeutic outcomes of different exosome preparation batches highlight the need for improved quality control as we move towards clinical applications.
Preliminary clinical research has underscored the potential of exosomes in addressing KOA, despite existing obstacles. A trial involving a bone marrow MSC exosome product (ExoFlo) indicated notable pain reduction, enhanced joint functionality, and an absence of serious side effects in patients six months post intra-articular exosome injections into the knee.96 This suggests that MSC-Exos could serve as a viable cell replacement therapy regarding both safety and effectiveness. Furthermore, researchers are investigating engineered exosomes, including the genetic modification of donor cells to boost specific miRNA content (aimed at the cartilage degradation pathway) or incorporating targeted peptides on the exosome membrane to improve cartilage affinity. These methods have shown promise in animal studies. In summary, exosomes present a novel “extracellular” therapeutic strategy for KOA, merging the properties of nanocarriers and biologics: they act as both natural delivery systems and therapeutic agents.138 With improvements in production and modification techniques, exosomes are anticipated to play a crucial role in future therapies aimed at KOA. Building on the initial outcomes of passive targeting, active targeting methods could further refine delivery specificity.
Active Targeting Strategies
Active targeting enhances the capabilities of drug delivery systems by equipping them with specialized recognition features or responsive mechanisms that facilitate the precise delivery of medications to the knee’s microenvironment or allow for drug release under specific conditions. This approach encompasses two primary elements: the first involves leveraging ligand-receptor interactions to direct the delivery to particular cells or matrix elements (such as nanocarriers modified with ligands); the second involves utilizing pathophysiological signals (like pH levels, enzymes, and redox states) present in the joint to initiate the controlled release of the drug from the carrier.
Ligand-Mediated Biological Targeting
Cell- or Cartilage Matrix-Targeted Delivery Strategies
By attaching ligand molecules, such as peptides, antibodies, or sugars, to the recognition sites on the carrier’s surface, it becomes feasible to target specific cells or structures within the knee joint, thus enhancing the delivery of the drug to the desired location. In the context of knee osteoarthritis (KOA), the primary targets are the cartilage matrix (including type II collagen and aggregated proteoglycans), chondrocytes, synovial macrophages and fibroblasts, as well as neovascular endothelium.145 For targeting the cartilage matrix, ligands like the WYRGRL pentapeptide have been identified for their strong affinity to type II collagen in cartilage. When WYRGRL is incorporated onto the surface of nanoparticles, it leads to a preferential attachment of these particles to the cartilage and facilitates their infiltration into the matrix, resulting in a significant rise in drug concentration within the cartilage in animal studies. The accumulation of WYRGRL-modified carriers in cartilage tissue was found to be approximately 72 times greater than that of unmodified nanoparticles.98
A different cartilage-targeting ligand is a monoclonal antibody that specifically recognizes denatured collagen, such as one that binds to the relaxation site of the triple helix in type II collagen. This antibody has been modified to attach to lipid nanoparticles, leading to increased presence in injured joints following intravenous delivery, while showing minimal accumulation in healthy joints.99 These antibody-conjugated nanoparticles have also been effective in transporting siRNA into chondrocytes, decreasing the expression of inflammatory genes in cartilage, and significantly impeding the progression of osteoarthritis in animal studies.103,104 Additionally, small molecule ligands, including peptides that bind to cartilage adhesion proteins and cohesin, have been utilized to target cartilage proteoglycans, yielding positive outcomes.
Synovial and Inflammatory Cell-Targeted Delivery Strategies
To target synovial and inflammatory cells, a common approach involves leveraging receptors found on macrophages or synovial cells as binding sites. For instance, activated macrophages exhibit a high expression of folate receptors, prompting some research to incorporate folate modifications into liposomes for the delivery of anti-inflammatory medications.145 This strategy allows for selective uptake by synovial macrophages, thereby amplifying the anti-inflammatory response. Another notable receptor is CD44, present on synovial fibroblast-like cells and chondrocytes, which interacts with its natural ligand, hyaluronic acid (HA). In a particular study, polymer nanoparticles modified with HA (HA-NP) were developed to specifically bind to CD44-positive cells in damaged cartilage and synovium, inhibiting the inflammatory NF-κB pathway. Additionally, the HA coating enhanced the nanoparticles’ resistance to degradation by intra-articular hyaluronidase.146,147 In a mouse model of osteoarthritis, HA-NP showed remarkable ability to penetrate and protect cartilage, significantly reducing cartilage damage and subchondral osteosclerosis with treatments administered every four weeks.147
Emerging Bionic-Targeted Delivery Strategies
Furthermore, innovative biomimetic targeting methods are gaining interest, including the application of nanoparticles encapsulated in cell membranes that possess natural cell surface receptors for precise targeting of specific tissues. In a particular investigation, the membrane of anti-inflammatory M2 macrophages was utilized to encase collagenase-responsive colloidal particles, creating a nanocarrier resembling an “artificial macrophage”. This construct demonstrated the ability to actively move towards inflamed synovial areas and deliver chondroprotective medications, resulting in a notable reduction of inflammation and enhancement of cartilage regeneration in a mouse model of osteoarthritis.100–102
Active targeting through ligands holds significant promise for enhancing the precision of drug delivery; however, it encounters several obstacles. These include the risk of immune reactions caused by external macromolecular ligands and the potential for ligands to become “invisible” in living organisms due to the formation of a protein corona, which can diminish targeting effectiveness.148 Consequently, future efforts should focus on refining the selection and design of ligands or exploring alternatives like small molecules and camouflaged peptides to boost their stability and compatibility with biological systems.
Endogenous Stimulus Response Targeting Strategies
PH Response Delivery Strategy
The unique features of the knee osteoarthritis (OA) microenvironment, such as its acidic nature, presence of specific enzymes, and elevated oxidative stress, create opportunities for the creation of delivery systems that respond to stimuli. Among these, pH-responsive carriers have been extensively researched. As previously noted, the pH of OA joint fluid can decrease to nearly neutral or slightly acidic levels during inflammation. These carriers are typically constructed with acid-sensitive linkages or materials that can accept protons: the medication remains securely encapsulated under neutral or alkaline conditions, but the carrier’s structure breaks down or expands when it comes into contact with the acidic OA joint fluids, leading to the release of the drug. For instance, one study105 developed pH-sensitive nanoparticles made from chitosan that encapsulated triamcinolone, achieving a drug release rate of 69% at pH 6.0 over 24 hours, a significant increase compared to the 22% release at the normal pH of 7.4. This system demonstrated effectiveness in alleviating inflammation and pain in a rat model of knee OA, highlighting the benefits of enhanced drug release in acidic conditions. Additionally, certain amphiphilic polymeric micelles remain stable at neutral pH but undergo depolymerization when the pH drops, allowing for rapid drug release to address local inflammation.106–108
Enzyme-Responsive Delivery Strategies
Delivery systems that respond to enzymes have garnered significant interest. The high levels of matrix metalloproteinases (MMP-1, −3, −13, etc.) and ADAMTS proteases found in osteoarthritis (OA) joints play a crucial role in the breakdown of cartilage.9,149 By utilizing these enzymes, it becomes feasible to create carriers that either degrade or alter their structure in the presence of these enzymes, facilitating a release mechanism that is activated as needed. For instance, scientists have engineered an injectable hydrogel that responds to MMP-13, incorporating a peptide bond sensitive to this enzyme within its network, along with a specific inhibitor, BI-4394. When MMP-13 concentration rise in OA-affected joints, the hydrogel is cleaved by the enzyme, allowing for the timely release of the inhibitor to prevent further cartilage damage, while the gel remains stable when enzyme levels decrease, thus minimizing unnecessary drug release.109 This enzyme-activated release mechanism has effectively reduced cartilage deterioration in a rabbit model of OA and is considered an innovative approach to drug delivery with significant potential for future applications.
Redox Delivery Strategies
Elevated oxidative stress in inflammatory conditions has been leveraged to create redox-sensitive delivery systems. This involves utilizing macromolecules that degrade in the presence of reactive oxygen species (ROS) to encapsulate therapeutic agents. When ROS levels rise at the site of inflammation, the carrier disintegrates, releasing the antioxidant medication and effectively neutralizing ROS in that localized area, thus safeguarding the joints. Notably, these intelligent delivery systems are frequently paired with ligand-targeting strategies to facilitate “dual targeting”. The ligand directs the carrier to accumulate in the intended tissue, and subsequently, a local pathological signal initiates the release of the drug, enhancing the treatment’s spatial and temporal accuracy. For instance, research has integrated cartilage-targeting peptides with pH-sensitive polymers to create bifunctional nanoparticles that respond to pH changes, enabling the targeted delivery of anti-inflammatory drugs to injured cartilage, resulting in considerable protection of the cartilage in a rabbit model.110
In summary, the strategy of active targeting facilitates the precise delivery of medications to the knee’s microenvironment by utilizing biorecognition and adaptive responses. Despite the intricate nature of these systems, numerous animal studies have shown their effectiveness in enhancing drug performance and minimizing adverse effects.
Exogenous Physically Assisted Targeting Strategies
Beyond enhancements related to the carrier, external physical methods and chemical penetration strategies have been employed to improve the distribution and infiltration of drugs within the knee joint. These approaches modify the microenvironment of the joint or the behavior of the carrier by applying physical energy, which aids in delivering the medication more efficiently to its target area.
Ultrasound Delivery Strategies
Low-intensity ultrasound, particularly in the form of low-intensity pulsed ultrasound (LIPUS), has been utilized for treating joint disorders, aiding in the regeneration of cartilage. Conversely, higher intensity ultrasound serves as a targeted mechanism for drug delivery. Research by Nieminen et al explored the effects of MHz-frequency focused ultrasound on isolated cartilage and an in vitro model, revealing that this method could effectively drive drug mimics into cartilage to approximately half its thickness without causing damage. This approach significantly enhances both the depth and speed of penetration compared to traditional passive diffusion.111 These findings indicate that ultrasound-mediated drug delivery holds great potential for bypassing the cartilage matrix barrier and achieving targeted drug or carrier delivery to deeper cartilage layers. Furthermore, ultrasound can activate the release of drugs from specific acoustically responsive carriers, such as those containing microbubbles that experience cavitation under ultrasound, leading to a temporary release of the drug into adjacent tissues. In summary, ultrasound technology offers a non-invasive and precise method for improving intra-articular drug delivery, enabling deeper penetration when necessary, such as at the onset of treatment, while minimizing tissue disruption after the ultrasound application ends.
Magnetic Field-Guided Delivery Strategies
Utilizing magnetic field guidance represents a compelling strategy for enhancing localized drug delivery. When drug carriers are equipped with superparamagnetic nanoparticles (MNPs), the application of a magnetic field can concentrate and stabilize these carriers at the desired site, facilitating their deeper penetration into tissues through magnetic attraction. The development of MNP-based carriers requires careful consideration of factors such as particle size, selection of biocompatible linkers or ligands, adjustment of magnetic characteristics, and the establishment of optimal parameters for magnetic field application to ensure functionality.150 Jiang et al created degradable magnetic nanocarriers (KGN-MNP) that encapsulated the chondrogenic small molecule Kartogenin, demonstrating their effectiveness in a rabbit model of knee osteoarthritis (OA). Their findings indicated that KGN-MNP, when directed by an external magnetic field, achieved superior penetration into cartilage tissue and retention in the joint compared to controls without magnetic guidance. Additionally, these carriers promoted the differentiation of subchondral stem cells into cartilage and aided in the repair of damaged cartilage and subchondral bone.112 This evidence implies that magnetically targeted delivery can significantly improve both the concentration and duration of drug action at joint lesions, thereby enhancing therapeutic outcomes. Magnetic field guidance is particularly advantageous for superficial joints like the knee, as external magnets are easily positioned and can effectively influence the joint area. Looking ahead, advancements in superparamagnetic materials and magnetic field control technologies may enable the application of this approach in the treatment of human knee OA, allowing for precise, field-controlled drug delivery.
Delivery Strategy of Electrical Stimulation and Other Osmotic Techniques
Electrical stimulation and various pro-osmotic methods utilize electrical currents to improve the transdermal absorption of drugs into joints, a process referred to as iontophoresis. This technique operates on the concept of applying a mild direct current to the skin, facilitating the movement of charged drug molecules through the skin barrier into targeted tissues.113 Iontophoresis serves as a non-invasive approach for administering anti-inflammatory and pain-relieving medications directly into the joint spaces of superficial areas, like the knee, thereby alleviating symptoms. Research has indicated that using iontophoresis in conjunction with topical treatments can result in greater pain relief compared to topical treatments alone for individuals suffering from knee osteoarthritis.114 Currently, iontophoresis is primarily explored for the delivery of local analgesics and anti-inflammatory agents, such as NSAIDs and hormones. While its effectiveness for larger molecules aimed at repairing articular cartilage remains limited, it shows promising potential as a complementary physical therapy.
Temperature and Optical Delivery Strategies
Research has investigated the use of temperature and optical techniques for targeted drug delivery to joints.115 By applying heat to the joint area, it is possible to enhance local circulation and increase the permeability of tissues, which facilitates the movement and absorption of medications. Additionally, certain nanomaterials that convert light into heat can be activated by near-infrared radiation, prompting the release of drugs from their carriers, thereby enabling “on-demand drug delivery” within the joint. Furthermore, microneedle technology,116 typically associated with transdermal applications, has been utilized in experiments where microneedle patches are placed on the skin surrounding the knee joint to provide a sustained release of anti-inflammatory medications into the joint fluid.
In summary, the use of these physical and chemical methods adds another layer of regulation to the delivery of drugs to the knee. They can be integrated with both passive and active targeting systems, creating a multimodal approach that aims to enhance the effectiveness and accuracy of localized knee treatments. Nevertheless, choosing the right assays, fine-tuning their sensitivity and specificity, and implementing them effectively continue to pose significant challenges.
To facilitate direct comparison of the diverse intra-articular delivery platforms discussed above, Table 2 summarizes their key physicochemical properties, targeting mechanisms, developmental stages, and functional advantages and drawbacks. By systematically contrasting passive, active, stimuli-responsive, and physically assisted strategies, this overview provides an integrated framework to evaluate current technologies and identify promising directions for future clinical translation.
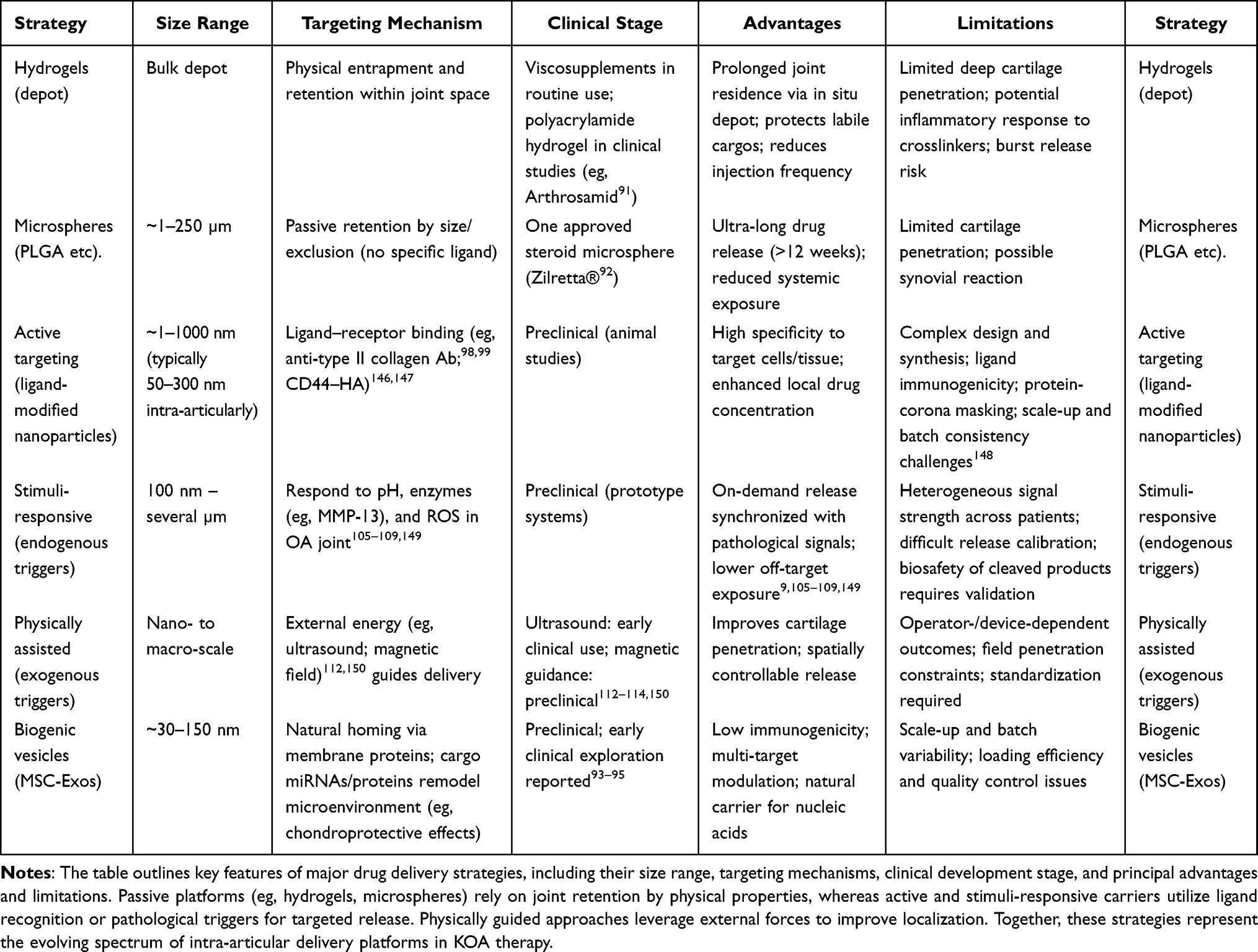 |
Table 2 Comparative Characteristics of Representative Intra-Articular Drug Delivery Strategies for KOA |
Challenges and Future Perspectives
Despite significant progress in drug delivery systems targeting the knee micro environment, many challenges remain in clinical translation. To translate the preclinical advances outlined above into clinical practice, Table 3 provides a concise overview of ongoing and completed clinical trials of intra-articular drug delivery systems for KOA. These findings underscore the rapid advancement of intra-articular drug delivery from experimental models to human application and naturally lead into the discussion of remaining challenges and future directions in Challenges and Future Perspectives.
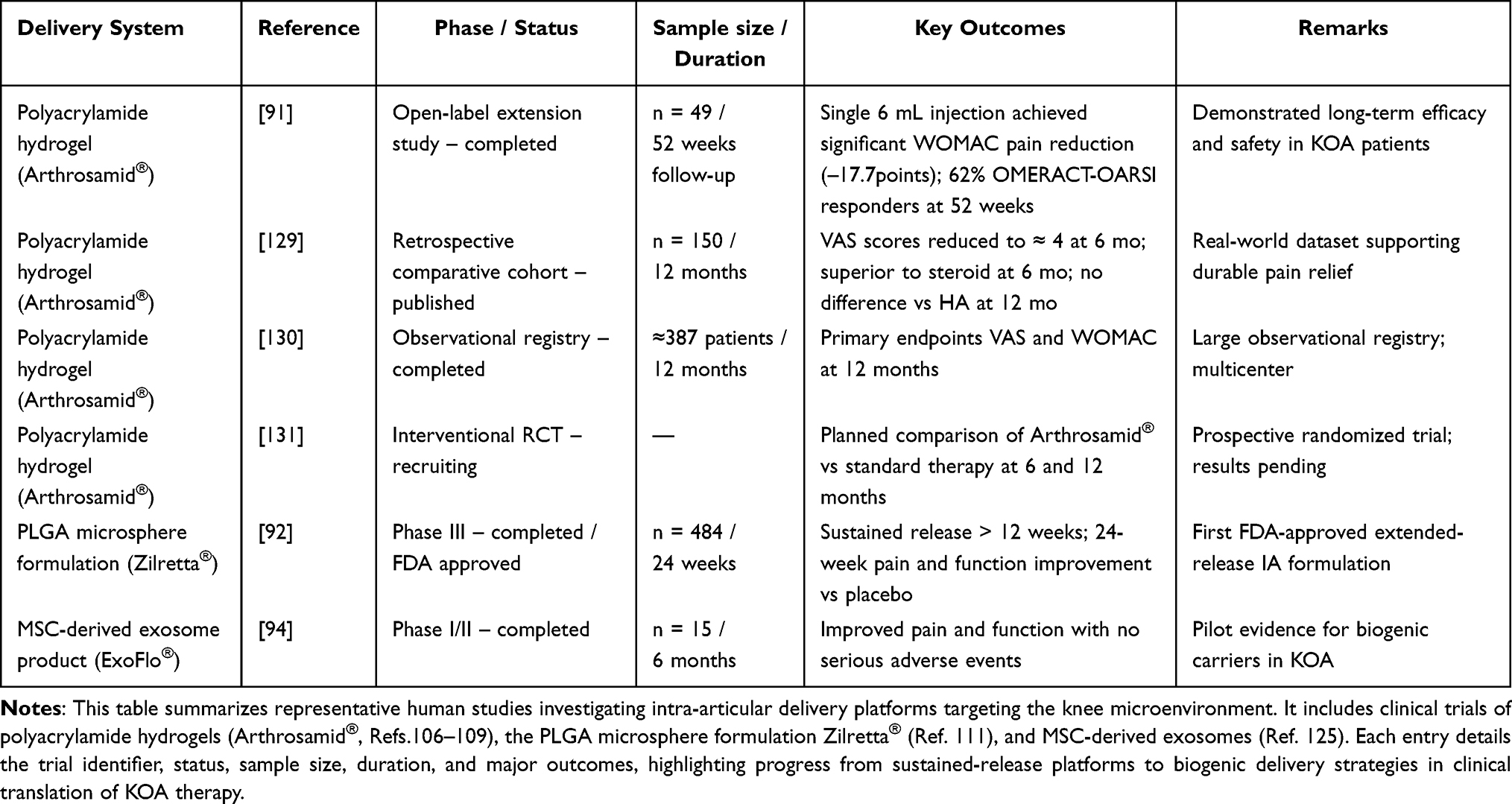 |
Table 3 Ongoing and Published Clinical Trials of Intra-Articular Drug Delivery Systems for Knee Osteoarthritis (KOA) |
The contradiction between targeting precision and heterogeneity of the knee microenvironment remains prominent. Knee joint lesions involve various tissues and cells such as cartilage, synovium, bone, etc., and the microenvironment components are complex and diverse. A single-target strategy is often difficult to cover the whole disease process, so it is necessary to develop multi-target identification strategies, integrate multiple ligands (eg, targeting both cartilage matrix and inflammatory cells) into the same carrier, or construct a stage-targeted regimen: targeting different predominant pathologies at different stages of the disease (focusing on anti-inflammation in the early stage and promoting cartilage regeneration in the late stage). This idea is similar to personalized therapy, which takes into account the heterogeneous characteristics of OA patients with the aim of achieving a more comprehensive intervention.148 In the future, the design concept of “multi-acting as one” can also be used to develop artificial multifunctional nanocarriers to achieve synergistic targeting of cartilage and synovium at multiple levels. The multi-targeting design should avoid the interference between different actions, and the rational design of the ratio and the timing of the action is the key. Overall, improving the ability of the delivery system to adapt to the heterogeneity of the knee microenvironment will help to balance the comprehensiveness and precision of the therapeutic effect.
The problem of non-uniformity in the standards of nanomedicine biocompatibility and toxicity assessment needs to be solved. Currently, different studies have focused on the safety evaluation of nanocarriers and lacked unified standardization. Some studies only observed acute inflammation or weight change of animals, which is difficult to comprehensively reflect the long-term response of the joints, and the limited volume of joint cavity in small animal models has a large physiological difference with human body, resulting in limited extrapolation of the results,151 to address these problems, it is recommended to establish a specialized toxicological evaluation system for intra-articular delivery of nanomedicines, which should include histological changes of local cartilage and synovium, biochemical indicators of joint fluid, and indicators of systemic immune response. To address these problems, it is recommended to establish a specialized toxicological evaluation system for intra-articular delivery of nanomedicines, including histological changes of local cartilage and synovium, biochemical indexes of joint fluid, and systemic immune response, and to repeat the validation in rodent and large animal models, Synovial fluid flow and other joint conditions can be reproduced to evaluate the biocompatibility and efficacy of nanocarriers in the laboratory. This in vitro model is expected to screen safer and more effective candidates and reduce the blinding of animal experiments. Overall, by unifying the evaluation criteria and novel models, the screening and optimization of nanomedicine delivery systems can be accelerated to ensure that they are adequately validated for safety before entering the clinic. Research units and regulatory agencies should collaborate to develop guidelines to institutionalize and standardize the safety evaluation of nanomedicine intra-articular delivery.
The contradiction between long-lasting residency and deep cartilage penetration poses a challenge to the design of drug delivery systems. Traditional intra-articular therapeutic drugs can hardly take into account both “staying long” and “going deep”: increasing carrier size or constructing depots (eg, hydrogels, microspheres) can prolong joint retention, but it is difficult for the drug to penetrate through the dense cartilage matrix, whereas the small molecules or small particle size carriers are easy to diffuse and penetrate, but are also difficult to penetrate through the dense cartilage matrix. Small molecules or small particle size carriers are easy to diffuse and penetrate, but are often rapidly removed. The avascular structure of cartilage and the tight type II collagen-proteoglycan network form a significant barrier effect, making it difficult for the drug to reach the deep chondrocytes. To address this dilemma, researchers are exploring new approaches for structural transformation and hierarchical delivery. For example, designing “size-variable” carriers that are initially larger in size to minimize clearance, and then responsively disassemble into smaller units upon entry into the joint to penetrate deeper into the cartilage. It has been demonstrated that positively charged multivalent molecules (eg, modified anti-biotin proteins) injected into a joint can penetrate the entire cartilage within a few hours and become firmly bound to its negatively charged matrix, allowing them to remain in the cartilage for more than a week. The application of this principle to cationic nanoparticles is expected to significantly improve the residence time and penetration depth of drugs in cartilage. Meanwhile, the development of smart-responsive carriers that undergo property transformation upon exposure to the cartilage environment is also one of the possible paths. For example, some studies have coated the surface of nanoparticles with a layer of peelable shielding, so as to maintain a large size in the synovial fluid for stable retention, and then enter the cartilage surface by the action of enzymes to remove the shielding and reduce the size, so as to release the drug deep into the cartilage fissure. Other scholars have used chondrocyte membrane-encapsulated nanoparticles, endowed with high affinity for cartilage and adaptability to the joint environment, to achieve efficient drug enrichment and cartilage protection in rat and canine osteoarthritis models. The results showed that this biomimetic nanocarrier prolonged joint retention and slowed down the cartilage damage process. These strategies suggest that long-lasting residency and deep delivery are not completely contradictory and are expected to be balanced through dynamic regulation of structure/size. In the future, we should further optimize the distribution of the carriers in different regions of the joints to achieve full delivery from the joint cavity to the deep cartilage layer. At the same time, the design of such complex carriers needs to balance the stability and decomposability to ensure that they can be safely degraded and discharged after delivery to avoid the risk of long-term residues. In conclusion, innovative design around the contradiction between “long-lasting” and “penetration” will help break through the cartilage barrier and improve drug utilization.
Large-scale production and clinical translation are still challenges for targeted delivery systems. Many laboratory-developed nanocarriers have delicate structures and remarkable therapeutic effects, but their complex compositions and cumbersome processes make it difficult to meet the scale-up requirements of industrialization. Slight changes in the preparation process can affect the physicochemical properties and therapeutic efficacy of the carriers, making it difficult to ensure batch-to-batch consistency. This problem is particularly prominent in clinical submissions: regulatory agencies require strict quality control, and quality characterization and stability verification of complex nanosystems is far more difficult than that of small molecule drugs. Therefore, the concept of “Quality by Design (QbD)” should be introduced at the design stage, and the optimization of manufacturability and controllability should be one of the goals. Specifically, on the one hand, biocompatible materials (eg, PLGA, hyaluronic acid, etc.) that have been used in clinical applications should be selected as much as possible, and simple assembly methods should be used in order to reduce the difficulty of regulatory review; on the other hand, modular and automated manufacturing processes (eg, microfluidic nanoparticles) should be developed to improve the reproducibility and yield.
The matching of delivery strategies and response mechanisms under dynamic changes in the microenvironment is also a concern. The pathological environment within the knee OA joint is not constant: the synovial fluid is pH-decreased, rich in inflammatory enzymes and ROS during inflammatory episodes, and partially normalized during remission. Such dynamic changes require an “intelligent response” from the delivery system. If the carrier response threshold is not properly set, two extreme situations may occur: either the drug cannot be released in time when the signal from the lesion is insufficient, thus missing the optimal time for intervention, or it is over-released when the signal fluctuates transiently, resulting in waste or side effects. Therefore, the amplitude and duration of pathological signals need to be fully considered in the design to ensure that the delivery strategy is synchronized with the microenvironmental changes. In the future, with the deepening of the understanding of the changing law of microenvironment in the course of OA, the delivery system can be smarter: through adjustable sensitive components, it can realize the integrated sensing of various signals, such as pH, enzyme, stress, etc., and even add biosensing module to realize the feedback-controlled drug delivery. Through the fine tuning of microenvironment responsiveness, it is expected to ensure that drugs work at the right time and place, maximizing efficacy and reducing side effects.
Finally, the synergy of active and passive targeting strategies will be an important development direction for next-generation drug delivery systems. Single strategies often have limitations, such as passive targeting that relies on carrier retention but lacks selectivity, and active targeting that is specific but may have limited coverage. Combining the advantages of the two to build a multilevel targeted delivery platform is expected to achieve more efficient drug utilization.
It can be seen that the future delivery system will be more multi-targeting strategy, through the materials, surface modification, external energy field and other means of synergy, so that the selectivity and effectiveness of drug delivery to the lesion multiply. It should be emphasized that the compatibility between modules should be taken care of when constructing a multilevel targeting platform to avoid introducing new adverse reactions or complexities due to design overlay. By optimizing the integration of active and passive strategies, we are expected to develop a precise and efficient knee-targeted drug delivery system, which will provide a breakthrough solution for the treatment of osteoarthritis of the knee, a persistent disease.
In conclusion, future-oriented targeted drug delivery strategies for the knee microenvironment should be innovative and balanced in terms of multi-targeting, evaluation criteria, tissue penetration, scale-up, dynamic response and synergistic targeting. Only by overcoming the above difficulties can the novel carriers in the laboratory be truly transformed into clinically available therapeutic tools for the benefit of the growing osteoarthritis patient population.
This article is a narrative review; therefore, no formal risk-of-bias assessment was conducted. As a result, the conclusions may be influenced by publication bias, underscoring the need for future systematic reviews and meta-analyses to validate these findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Glinkowski WM, Tomaszewski W. Intra-articular hyaluronic acid for knee osteoarthritis: a systematic umbrella review. J Clin Med. 2025;14(4):1272. PMID: 40004802. doi:10.3390/jcm14041272
2. Liu Z, Song S, Zhang Q, Wang D. Research progress on treatment measures for joint function in non-surgical patients with knee osteoarthritis. J Orthop. 2025;64(64):64–67. doi:10.1016/j.jor.2024.11.023
3. Cui A, Li H, Wang D, et al. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClin Med. 2020;29-30:100587. doi:10.1016/j.eclinm.2020.100587
4. Li J, Han X, Zhang X, et al. Spatiotemporal evolution of global population ageing from 1960 to 2017. BMC Public Health. 2019;19(1):127. doi:10.1186/s12889-019-6465-2
5. Long H, Liu Q, Yin H, et al. Prevalence Trends of Site-Specific Osteoarthritis From 1990 to 2019: findings From the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022;74(7):1172–1183. doi:10.1002/art.42089
6. Chen L, Zhang Z, Liu X. Role and mechanism of mechanical load in the homeostasis of the subchondral bone in knee osteoarthritis: a comprehensive review. J Inflamm Res. 2024;17:9359–9378. doi:10.2147/JIR.S492415
7. Martel-Pelletier J, Barr AJ, Cicuttini FM, et al. Osteoarthritis. Nat Rev Dis Primers. 2016;2(1):16072. doi:10.1038/nrdp.2016.72
8. Abramoff B, Caldera FE. Osteoarthritis: pathology, diagnosis, and treatment options. Med Clin North Am. 2020;104(2):293–311. doi:10.1016/j.mcna.2019.10.007
9. Glyn-Jones S, Palmer AJ, Agricola R, et al. Osteoarthritis. Lancet. 2015;386(9991):376–387. doi:10.1016/S0140-6736(14)60802-3
10. Liu Y, Shah KM, Luo J. Strategies for articular cartilage repair and regeneration. Front Bioeng Biotechnol. 2021;9:770655. doi:10.3389/fbioe.2021.770655
11. Li G, Yin J, Gao J, et al. Subchondral bone in osteoarthritis: insight into risk factors and microstructural changes. Arthritis Res Ther. 2013;15(6):223. doi:10.1186/ar4405
12. Henrotin Y, Pesesse L, Sanchez C. Subchondral bone and osteoarthritis: biological and cellular aspects. Osteoporos Int. 2012;23(Suppl 8):S847–51. doi:10.1007/s00198-012-2162-z
13. Xing W, Cai M, Li C, Nie Z, Tang W. Computed tomography image analysis of neuromuscular electrical stimulation in the treatment of knee osteoarthritis with different radiologic characteristics based on iterative reconstruction algorithm. World Neurosurg. 2021;149:372–379. doi:10.1016/j.wneu.2020.10.032
14. Wang D, Pan Y, Chen W, et al. Nanodrugs targeting key factors of ferroptosis regulation for enhanced treatment of osteoarthritis. Adv Sci. 2025;12(3):e202412817. doi:10.1002/advs.202412817
15. Deng R, Zhao R, Zhang Z, et al. Chondrocyte membrane-coated nanoparticles promote drug retention and halt cartilage damage in rat and canine osteoarthritis. Sci Transl Med. 2024;16(735):eadh9751. doi:10.1126/scitranslmed.adh9751
16. Hou Y, Mengmeng J, Liu Y, et al. Biomimetic construction of a lubricious hydrogel with robust mechanics via polymer chains interpenetration and entanglement for TMJ disc replacement. Chem Eng J. 2023;460:141731. doi:10.1016/j.cej.2023.141731
17. Jin Z, Zhan Y, Zheng L, Wei Q, Xu S, Qin Z. Cannabidiol-loaded poly lactic-co-glycolic acid nanoparticles with improved bioavailability as a potential for osteoarthritis therapeutic. Chembiochem. 2023;24(9):e202200698. doi:10.1002/cbic.202200698
18. Liang H, Yan Y, Sun W, et al. Preparation of melatonin-loaded nanoparticles with targeting and sustained release function and their application in osteoarthritis. Int J Mol Sci. 2023;24(10):8740. doi:10.3390/ijms24108740
19. Shu C, Yin X, Zhong Q, Cheng M. Unveiling the future: bibliometric analysis on the application of nanomaterials in osteoarthritis (2006-2023). Heliyon. 2024;10(17):e36541. doi:10.1016/j.heliyon.2024.e36541
20. Tang S, Zhang C, Oo WM, et al. Osteoarthritis. Nat Rev Dis Primers. 2025;11(1):10. doi:10.1038/s41572-025-00594-6
21. Tong L, Yu H, Huang X, et al. Current understanding of osteoarthritis pathogenesis and relevant new approaches. Bone Res. 2022;10(1):60. doi:10.1038/s41413-022-00226-9
22. Silvestrini da Silva A, Hertel FC, Valente FL, et al. Characterization of the joint microenvironment in osteoarthritic joints for in vitro strategies for MSC-based therapies: a systematic review. Appl Biosci. 2024;3(4):450–467. doi:10.3390/applbiosci3040029
23. Liu-Bryan R, Terkeltaub R. Emerging regulators of the inflammatory process in osteoarthritis. Nat Rev Rheumatol. 2015;11(1):35–44. doi:10.1038/nrrheum.2014.162
24. Yuan Z, Jiang D, Yang M, et al. Emerging roles of macrophage polarization in osteoarthritis: mechanisms and therapeutic strategies. Orthop Surg. 2024;16(3):532–550. doi:10.1111/os.13993
25. Liu M, Zeng X, Ma C, et al. Injectable hydrogels for cartilage and bone tissue engineering. Bone Res. 2017;5(1):17014. doi:10.1038/boneres.2017.14
26. Li J, Chen G, Xu X, et al. Advances of injectable hydrogel-based scaffolds for cartilage regeneration. Regen Biomater. 2019;6(3):129–140. doi:10.1093/rb/rbz022
27. PHINNEY DG, PITTENGER MF. Concise review:MSC-derived exosomes for cell-free therapy[J]. Stem Cells. 2017;35(4):851–858. doi:10.1093/rb/rbz022
28. Rani S, Ryan AE, Griffin MD, et al. Mesenchymal stem cell-derived extracellular vesicles: toward cell-free therapeutic applications[J]. Mol Ther. 2015;23(5):812–823. doi:10.1038/mt.2015.44
29. LI N, ZHAO L, YK WEI, et al. Recent advances of exosomes in immune-mediated eye diseases[J]. Stem Cell Res Ther. 2019;10(1):278. doi:10.1186/s13287-019-1372-0
30. Del Río E, Castañeda S, Timón R, et al. Synergistic effects of chronoexercise, circadian rhythm, and chondroprotective pharmacokinetics on osteoarthritis management. Biomedicines. 2025;13(3):598. doi:10.3390/biomedicines13030598
31. Zhang H, Jiang X, Bai L, et al. Vitamin C intake and osteoarthritis: findings of NHANES 2003-2018 and Mendelian randomization study. Front Nutr. 2024;11:1409578. doi:10.3389/fnut.2024.1409578
32. Hu Y, Chen X, Wang S, Jing Y, Su J. Subchondral bone microenvironment in osteoarthritis and pain. Bone Res. 2021;9(1):20. doi:10.1038/s41413-021-00147-z
33. Semenistaja S, Skuja S, Kadisa A, Groma V. Healthy and osteoarthritis-affected joints facing the cellular crosstalk. Int J Mol Sci. 2023;24(4):4120. doi:10.3390/ijms24044120
34. Roelofs AJ, De Bari C. Osteoarthritis year in review 2023: biology. Osteoarthritis Cartilage. 2024;32(2):148–158. doi:10.1016/j.joca.2023.11.002
35. Song J, Kim D, Chun CH, Jin EJ. MicroRNA-9 regulates survival of chondroblasts and cartilage integrity by targeting protogenin. Cell Commun Signal. 2013;11:66. doi:10.1186/1478-811X-11-66
36. Wan HY, Guo LM, Liu T, Liu M, Li X, Tang H. Regulation of the transcription factor NF-kappaB1 by microRNA-9 in human gastric adenocarcinoma. Mol Cancer. 2010;9:16. doi:10.1186/1476-4598-9-16
37. Zhang Q, Lenardo MJ, Baltimore D. 30 years of NF-κB: A blossoming of relevance to human pathobiology. Cell. 2017;168(1–2):37–57. doi:10.1016/j.cell.2016.12.012
38. Fan Q, Zhao M, Zhang XD, Chu TY, Kou ZX, Zhao Q. Research progress and prospect of MAPK signaling pathway in knee osteoarthritis. Eur J Orthop Surg Traumatol. 2025;35(1):134. doi:10.1007/s00590-025-04261-0
39. Samman WA, Mosalam EM, Saif DS, et al. Deciphering the role of Wnt/β-catenin and miR-214 in knee osteoarthritis: molecular and clinical insights. Front Pharmacol. 2025;16:1507693. doi:10.3389/fphar.2025.1507693
40. Chen B, Ning K, Sun ML, Zhang XA. Regulation and therapy, the role of JAK2/STAT3 signaling pathway in OA: A systematic review. Cell Commun Signal. 2023;21(1):67. doi:10.1186/s12964-023-01094-4
41. Wang MG, Seale P, Furman D. The infrapatellar fat pad in inflammaging, knee joint health, and osteoarthritis. NPJ Aging. 2024;10(1):34. doi:10.1038/s41514-024-00159-z
42. Emmi A, Stocco E, Boscolo-Berto R, et al. Infrapatellar fat pad-synovial membrane anatomo-fuctional unit: Microscopic basis for Piezo1/2 mechanosensors involvement in osteoarthritis pain. Front Cell Dev Biol. 2022;10:886604. doi:10.3389/fcell.2022.886604
43. Vincent TL, McClurg O, Troeberg L. The extracellular matrix of articular cartilage controls the bioavailability of pericellular matrix-bound growth factors to drive tissue homeostasis and repair. Int J Mol Sci. 2022;23(11):6003. doi:10.3390/ijms23116003
44. Wiegertjes R, Thielen NGM, van Caam APM, et al. Increased IL-6 receptor expression and signaling in ageing cartilage can be explained by loss of TGF-β-mediated IL-6 receptor suppression. Osteoarthritis Cartilage. 2021;29(5):773–782. doi:10.1016/j.joca.2021.01.008
45. Stassen RHMJ, van den Akker GGH, Caron MMJ, et al. TGF-β enhances phosphate-driven calcification of human OA articular chondrocytes. Calcif Tissue Int. 2025;116(1):57. doi:10.1007/s00223-025-01365-x
46. Glasson SS, Askew R, Sheppard B, et al. Deletion of active ADAMTS5 prevents cartilage degradation in a murine model of osteoarthritis. Nature. 2005;434(7033):644–648. doi:10.1038/nature03369
47. Troeberg L, Nagase H. Proteases involved in cartilage matrix degradation in osteoarthritis. Biochim Biophys Acta. 2012;1824(1):133–145. doi:10.1016/j.bbapap.2011.06.020
48. Mobasheri A, Rayman MP, Gualillo O, Sellam J, van der Kraan P, Fearon U. The role of metabolism in the pathogenesis of osteoarthritis. Nat Rev Rheumatol. 2017;13(5):302–311. doi:10.1038/nrrheum.2017.50
49. Scanzello CR, Goldring SR. The role of synovitis in osteoarthritis pathogenesis. Bone. 2012;51(2):249–257. doi:10.1016/j.bone.2012.02.012
50. Sellam J, Berenbaum F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nat Rev Rheumatol. 2010;6(11):625–635. doi:10.1038/nrrheum
51. Sokolove J, Lepus CM. Role of inflammation in the pathogenesis of osteoarthritis: latest findings and interpretations. Ther Adv Musculoskelet Dis. 2013;5(2):77–94. doi:10.1177/1759720X12467868
52. Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP, Fahmi H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat Rev Rheumatol. 2011;7(1):33–42. doi:10.1038/nrrheum
53. Muratovic D, Atkins GJ, Findlay DM. Is RANKL a potential molecular target in osteoarthritis? Osteoarthritis Cartilage. 2024;32(5):493–500. doi:10.1016/j.joca.2023.10.010
54. Zhou Y, Liang C. Il-6 in osteoarthritis: expression and research progress. BioRes Scientia. 2024;7(4):1–7. doi:10.59657/2837-2565.brs.24.195
55. Marcu KB, Otero M, Olivotto E, Borzi RM, B. Goldring M. NF-κB signaling: multiple angles to target OA. Curr Drug Targets. 2010;11(5):599–613. doi:10.2174/138945010791011938
56. Ye Y, Zhou J. The protective activity of natural flavonoids against osteoarthritis by targeting NF-κB signaling pathway. Front Endocrinol. 2023;14:1117489. doi:10.3389/fendo.2023.1117489
57. Li Z, Dai A, Yang M, Chen S, Deng Z, Li L. p38MAPK signaling pathway in osteoarthritis: Pathological and therapeutic aspects. J Inflamm Res. 2022;15:723–734. doi:10.2147/JIR.S348491
58. Lin S, Lu J, Chen Q, et al. Plantamajoside suppresses the activation of NF-κB and MAPK and ameliorates the development of osteoarthritis. Int Immunopharmacol. 2023;115:109582. doi:10.1016/j.intimp.2022.109582
59. Fazio A, Di Martino A, Brunello M, et al. The involvement of signaling pathways in the pathogenesis of osteoarthritis: an update. J Orthop Translat. 2024;47:116–124. doi:10.1016/j.jot.2024.06.002
60. Gill AK, McCormick PJ, Sochart D, Nalesso G. Wnt signalling in the articular cartilage: A matter of balance. Int J Exp Pathol. 2023;104(2):56–63. doi:10.1111/iep.12472
61. Baugé C, Girard N, Lhuissier E, Bazille C, Boumediene K. Regulation and role of TGFβ signaling pathway in aging and osteoarthritis joints. Aging Dis. 2013;5(6):394–405. doi:10.14336/AD.2014.0500394
62. Zhen G, Wen C, Jia X, et al. Inhibition of TGF-β signaling in mesenchymal stem cells of subchondral bone attenuates osteoarthritis. Nat Med. 2013;19(6):704–712. doi:10.1038/nm.3143
63. Yao Q, Wu X, Tao C, et al. Osteoarthritis: pathogenic signaling pathways and therapeutic targets. Signal Transduct Target Ther. 2023;8(1):56. doi:10.1038/s41392-023-01330-w
64. Lambert C, Zappia J, Sanchez C, Florin A, Dubuc JE, Henrotin Y. The Damage-Associated Molecular Patterns (DAMPs) as potential targets to treat osteoarthritis: perspectives from a review of the literature. Front Med Lausanne. 2021;7:607186. doi:10.3389/fmed.2020.607186
65. Wang Q, Rozelle AL, Lepus CM, et al. Identification of a central role for complement in osteoarthritis. Nat Med. 2011;17(12):1674–1679. doi:10.1038/nm.2543
66. Li HM, Guo HL, Xu C, et al. Inhibition of glycolysis by targeting lactate dehydrogenase A facilitates hyaluronan synthase 2 synthesis in synovial fibroblasts of temporomandibular joint osteoarthritis. Bone. 2020;141:115584. doi:10.1016/j.bone.2020.115584
67. Jiang D, Guo J, Liu Y, Li W, Lu D. Glycolysis: an emerging regulator of osteoarthritis. Front Immunol. 2024;14:1327852. doi:10.3389/fimmu.2023.1327852
68. Sanchez-Lopez E, Coras R, Torres A, Lane NE, Guma M. Synovial inflammation in osteoarthritis progression. Nat Rev Rheumatol. 2022;18(5):258–275. doi:10.1038/s41584-022-00749-9
69. Li Q, Wen Y, Wang L, et al. Author correction: Hyperglycemia-induced accumulation of advanced glycosylation end products in fibroblast-like synoviocytes promotes knee osteoarthritis. Exp Mol Med. 2022;54(6):862–865. doi:10.1038/s12276-022-00788-y
70. Wei G, Lu K, Umar M, et al. Risk of metabolic abnormalities in osteoarthritis: a new perspective to understand its pathological mechanisms. Bone Res. 2023;11(1):63. doi:10.1038/s41413-023-00301-9
71. Zhang M, Wu J, Cai K, et al. From dysfunction to healing: advances in mitochondrial therapy for Osteoarthritis. J Transl Med. 2024;22(1):1013. doi:10.1186/s12967-024-05799-z
72. Henry ÓC, O’Neill LAJ. Metabolic reprogramming in stromal and immune cells in rheumatoid arthritis and osteoarthritis: therapeutic possibilities. Eur J Immunol. 2025;55(4):e202451381. doi:10.1002/eji.202451381
73. Loeser RF, Collins JA, Diekman BO. Ageing and the pathogenesis of osteoarthritis. Nat Rev Rheumatol. 2016;12(7):412–420. doi:10.1038/nrrheum.2016.65
74. Wang Y, Zhao X, Lotz M, Terkeltaub R, Liu-Bryan R. Mitochondrial biogenesis is impaired in osteoarthritis chondrocytes but reversible via peroxisome proliferator-activated receptor γ coactivator 1α. Arthritis Rheumatol. 2015;67(8):2141–2153. doi:10.1002/art.39182
75. Blanco FJ, Rego I, Ruiz-Romero C. The role of mitochondria in osteoarthritis. Nat Rev Rheumatol. 2011;7(3):161–169. doi:10.1038/nrrheum.2010.213
76. Han Z, Wang K, Ding S, Zhang M. Cross-talk of inflammation and cellular senescence: a new insight into the occurrence and progression of osteoarthritis. Bone Res. 2024;12(1):69. doi:10.1038/s41413-024-00375-z
77. He XX, Huang YJ, Hu CL, Xu QQ, Wei QJ. Songorine modulates macrophage polarization and metabolic reprogramming to alleviate inflammation in osteoarthritis. Front Immunol. 2024;15:1344949. doi:10.3389/fimmu.2024.1344949
78. Batista-Gonzalez A, Vidal R, Criollo A, Carreño LJ. New insights on the role of lipid metabolism in the metabolic reprogramming of macrophages. Front Immunol. 2020;10:2993. doi:10.3389/fimmu.2019.02993
79. Zhao K, Ruan J, Nie L, Ye X, Li J. Effects of synovial macrophages in osteoarthritis. Front Immunol. 2023;14:1164137. doi:10.3389/fimmu.2023.1164137
80. Saraiva AL, Veras FP, Peres RS, et al. Succinate receptor deficiency attenuates arthritis by reducing dendritic cell traffic and expansion of Th17 cells in the lymph nodes. FASEB J. 2018;12:fj201800285. doi:10.1096/fj.201800285
81. Pan X, Shan H, Bai J, et al. F our-octyl itaconate improves osteoarthritis by enhancing autophagy in chondrocytes via PI3K/AKT/mTOR signalling pathway inhibition. Commun Biol. 2022;5(1):641. doi:10.1038/s42003-022-03592-6
82. Dang EV, Barbi J, Yang HY, et al. Control of TH17/Treg balance by hypoxia-inducible factor 1. Cell. 2011;146(5):772–784. doi:10.1016/j.cell.2011.07.033
83. Faust HJ, Zhang H, Han J, et al. IL-17 and immunologically induced senescence regulate response to injury in osteoarthritis. J Clin Invest. 2020;130(10):5493–5507. doi:10.1172/JCI134091
84. Motta F, Barone E, Sica A, Selmi C. Inflammaging and osteoarthritis. Clin Rev Allergy Immunol. 2023;64(2):222–238. doi:10.1007/s12016-022-08941-1
85. Jeon OH, Kim C, Laberge RM, et al. Local clearance of senescent cells attenuates the development of post-traumatic osteoarthritis and creates a pro-regenerative environment. Nat Med. 2017;23(6):775–781. doi:10.1038/nm.4324
86. Rao C, Shi S. Development of nanomaterials to target articular cartilage for osteoarthritis therapy. Front Mol Biosci. 2022;9:900344. doi:10.3389/fmolb.2022.900344
87. Kou L, Xiao S, Sun R, Bao S, Yao Q, Chen R. Biomaterial-engineered intra-articular drug delivery systems for osteoarthritis therapy. Drug Deliv. 2019;26:870–885. doi:10.1080/10717544.2019.1660434
88. Jiang Y, Wang Y, Li Q, Yu C, Chu W. Natural polymer-based stimuli-responsive hydrogels. Curr Med Chem. 2020;27:2631–2657. doi:10.2174/0929867326666191122144916
89. Koland M, Narayanan Vadakkepushpakath A, John A, Tharamelveliyil RA, Raghunath I. Thermosensitive in situ gels for joint disorders: pharmaceutical considerations in intra-articular delivery. Gels. 2022;8(11):723. doi:10.3390/gels8110723
90. Yi YH, Chen G, Gong S, et al. Injectable temperature-sensitive hydrogel loaded with IL-36Ra for the relief of osteoarthritis. ACS Biomater Sci Eng. 2023;9(3):1672–1681. doi:10.1021/acsbiomaterials.2c01144
91. Bliddal H, Beier J, Hartkopp A, Conaghan PG, Henriksen M. Effectiveness and safety of polyacrylamide hydrogel injection for knee osteoarthritis: results from a 12-month follow up of an open-label study. J Orthop Surg Res. 2024;19(1):274. doi:10.1186/s13018-024-04756-2
92. Paik J, Duggan ST, Keam SJ. Triamcinolone acetonide extended-release:a review in osteoarthritis pain of the knee. Drugs. 2019;79(4):455–462. doi:10.1007/s40265-019-01083-3
93. Zheng L, Wang Y, Qiu P, et al. Primary chondrocyte exosomes mediate osteoarthritis progression by regulating mitochondrion and immune reactivity. Nanomedicine. 2019;14(24):3193–3212. doi:10.2217/nnm-2018-0498
94. Ni Z, Kuang L, Chen H, et al. The exosome-like vesicles from osteoarthritic chondrocyte enhanced mature IL-1β production of macrophages and aggravated synovitis in osteoarthritis. Cell Death Dis. 2019;10(7):522. doi:10.1038/s41419-019-1739-2
95. Chen Y, Xue K, Zhang X, Zheng Z, Liu K. Exosomes derived from mature chondrocytes facilitate subcutaneous stable ectopic chondrogenesis of cartilage progenitor cells. Stem Cell Res Ther. 2018;9(1):318. doi:10.1186/s13287-018-1047-2
96. East J, Alexander T, Dordevic M. IRB approved pilot safety study of an extracellular vesicle isolate product evaluating the treatment of osteoarthritis in combat-related injuries. Stem Cell Res. 2020;1(2):1–10. doi:10.52793/JSCR.2020.1(2)-09
97. He T, Zhang C, Colombani T, Bencherif SA, Porter RM, Bajpayee AG. Intra-articular kinetics of a cartilage targeting cationic PEGylated protein for applications in drug delivery. Osteoarthritis Cartilage. 2023;31(2):187–198. doi:10.1016/j.joca.2022.09.010
98. Pontes AP, Kim C-M, Kim T-H, et al. Polymeric Nanoparticles for Drug Delivery in Osteoarthritis. Pharmaceutics. 2022;14(11):2345. doi:10.3390/pharmaceutics14112345
99. Li J, Zhang H, Han Y, Hu Y, Geng Z, Su J. Targeted and responsive biomaterials in osteoarthritis. Theranostics. 2023;13(3):931–954. doi:10.7150/thno.78639
100. Zhou F, Mei J, Yang S, et al. Modified ZIF-8 nanoparticles attenuate osteoarthritis by reprogramming the metabolic pathway of synovial macrophages. ACS Appl Mater Interfaces. 2020;12(2):2009–2022. doi:10.1021/acsami.9b16327
101. Chen X, He C, Sheng TP, et al. A magnesium-based coordination container as a multi-drugs co-loaded system for boosting anti-inflammatory therapy in joints. Chem Eng J. 2021;415:129–147. doi:10.1016/j.cej.2021.128939
102. Yang G, Fan M, Zhu J, et al. A multifunctional anti-inflammatory drug that can specifically target activated macrophages, massively deplete intracellular H2O2, and produce large amounts CO for a highly efficient treatment of osteoarthritis. Biomaterials. 2020;255:120155. doi:10.1016/j.biomaterials.2020.120155
103. Cho H, Kim BJ, Park SH, Hasty KA, Min BH. Noninvasive visualization of early osteoarthritic cartilage using targeted nanosomes in a destabilization of the medial meniscus mouse model. Int J Nanomed. 2018;13:1215–1224. doi:10.2147/IJN.S149375
104. Bedingfield SK, Yu F, Liu DD, et al. Matrix-targeted nanoparticles for MMP13 RNA interference blocks post-traumatic osteoarthritis. bioRxiv. 2020;01(30):925321.
105. T WD, Liu XM, Xu JT, et al. Intra-articular delivery of celastrol by hollow mesoporous silica nanoparticles for pH-sensitive anti-inflammatory therapy against knee osteoarthritis. J Nanobiotechnology. 2020;18(1):94. doi:10.1186/s12951-020-00651-0
106. Zerrillo L, Que I, Vepris O, et al. pH-responsive poly(lactide-co-glycolide) nanoparticles containing near-infrared dye for visualization and hyaluronic acid for treatment of osteoarthritis. J Control Release. 2019;309:265–276. doi:10.1016/j.jconrel.2019.07.031
107. Zhang M, Hu W, Cai C, Wu Y, Li J, Dong S. Advanced application of stimuli-responsive drug delivery system for inflammatory arthritis treatment. Mater Today Bio. 2022;14:100223. doi:10.1016/j.mtbio.2022.100223
108. Zhang M, Peng X, Ding Y, et al. A cyclic brush zwitterionic polymer based pH-responsive nanocarrier-mediated dual drug delivery system with lubrication maintenance for osteoarthritis treatment. Mater Horiz. 2023;10(7):2554–2567. doi:10.1039/d3mh00218g
109. Roy HS, Murugesan P, Kulkarni C, et al. On-demand release of a selective MMP-13 blocker from an enzyme-responsive injectable hydrogel protects cartilage from degenerative progression in osteoarthritis. J Mater Chem B. 2024;12(22):5325–5338. doi:10.1039/d3tb02871b
110. Chen H, Qin Z, Zhao J, et al. Cartilage-targeting and dual MMP-13/pH responsive theranostic nanoprobes for osteoarthritis imaging and precision therapy. Biomaterials. 2019;225:119520. doi:10.1016/j.biomaterials
111. Nieminen HJ, Ylitalo T, Suuronen JP, et al. Delivering agents locally into articular cartilage by intense MHz ultrasound. Ultrasound Med Biol. 2015;41(8):2259–2265. doi:10.1016/j.ultrasmedbio.2015.03.025
112. Jiang Z, Zhang Z, Li S, Lin S, Yuan H. Magnetically guided intracartilaginous delivery of kartogenin improves stem cell-targeted degenerative arthritis therapy. Int J Nanomed. 2022;21(17):5511–5524. doi:10.2147/IJN.S381815
113. Kalia YN, Naik A, Garrison J, Guy RH. Iontophoretic drug delivery. Adv Drug Delive Rev. 2004;56:619–658. doi:10.1016/j.addr.2003.10.026
114. Shentu CY, Yan G, Xu DC, Chen Y, Peng LH. Emerging pharmaceutical therapeutics and delivery technologies for osteoarthritis therapy. Front Pharmacol. 2022;13:945876. doi:10.3389/fphar.2022.945876
115. Choi S, Park J, Hyun W, et al. Stretchable heater using ligand-exchanged silver nanowire nanocomposite for wearable articular thermotherapy. ACS Nano. 2015;9:6626–6633. doi:10.1021/acsnano.5b02790
116. Kennedy J, Larrañeta E, McCrudden MTC. In vivo studies investigating biodistribution of nanoparticle-encapsulated rhodamine B delivered via dissolving microneedles. J Control Release. 2017;265:57–65. doi:10.1016/j.jconrel.2017.04.022
117. Gambaro FM, Ummarino A, Torres Andón F, Ronzoni F, Di Matteo B, Kon E. Drug delivery systems for the treatment of knee osteoarthritis: a systematic review of in vivo studies. Int J Mol Sci. 2021;22(17):9137. doi:10.3390/ijms22179137
118. Liang Q, Cheng Z, Qin L. Advanced nanoparticles in osteoarthritis treatment. Biomater Transl. 2024;5(2):95–113. doi:10.12336/biomatertransl
119. Gan X, Wang X, Huang Y, Li G, Kang H. Applications of Hydrogels in Osteoarthritis Treatment. Biomedicines. 2024;12(4):923. doi:10.3390/biomedicines12040923
120. Young IC, Chuang S-T, Gefen A, et al. A novel compressive stress-based osteoarthritis-like chondrocyte system. Exp Biol Med. 2017;242:1062–1071. doi:10.1177/1535370217699534
121. Huang H, Lou Z, Zheng S, et al. Intra-articular drug delivery systems for osteoarthritis therapy: shifting from sustained release to enhancing penetration into cartilage. Drug Deliv. 2022;29(1):767–791. doi:10.1080/10717544.2022.2048130
122. Zhu M, Zhu Y, Zhang L, Shi J. Preparation of chitosan/mesoporous silica nanoparticle composite hydrogels for sustained co-delivery of biomacromolecules and small chemical drugs. Sci Technol Adv Mater. 2013;14(4):045005. doi:10.1088/1468-6996/14/4/045005
123. Liu W, Mengsi M, Lei Z, et al. Intra-articular injectable hydroxypropyl chitin/hyaluronic acid hydrogel as bio-lubricant to attenuate osteoarthritis progression. Mater Des. 2022;217(217):110579. doi:10.1016/j.matdes.2022.110579
124. Duan WL, Zhang LN, Bohara R, et al. Adhesive hydrogels in osteoarthritis: from design to application. Mil Med Res. 2023;10(1):4. doi:10.1186/s40779-022-00439-3
125. Zhu C, Han S, Zeng X, Zhu C, Pu Y, Sun Y. Multifunctional thermo-sensitive hydrogel for modulating the microenvironment in osteoarthritis by polarizing macrophages and scavenging RONS. J Nanobiotechnol. 2022;20:221. doi:10.1186/s12951-022-01422-9
126. Lei Y, Wang Y, Shen J, et al. Injectable hydrogel microspheres with self-renewable hydration layers alleviate osteoarthritis. Sci Adv. 2022;8(5):eabl6449. doi:10.1126/sciadv.abl6449
127. Mamidi N, Velasco R, Barrera E, Ramakrishna S, Annabi N. Carbonaceous nanomaterials incorporated biomaterials: the present and future of the flourishing field. Compos Part B Eng. 2022;243:110150. doi:10.1016/j.compositesb.2022.110150
128. Zhao Z, Wang P, Li Z, et al. Targeted lipid nanoparticles distributed in hydrogel treat osteoarthritis by modulating cholesterol metabolism and promoting endogenous cartilage regeneration. J Nanobiotechnology. 2024;22(1):786. doi:10.1186/s12951-024-02965-9
129. Ding H, Tan P, Fu S, et al. Preparation and application of pH-responsive drug delivery systems. J Control Release. 2022;348:206–238. doi:10.1016/j.jconrel.2022.05.056
130. Kumar MN, Muzzarelli RA, Muzzarelli C, et al. Chitosan chemistry and pharmaceutical per-spectives[J]. Chem Rev. 2004;104(12):6017–6084. doi:10.1021/cr030441b
131. Shariatinia Z. Pharmaceutical applications of chitosan. Adv Colloid Interface Sci. 2019;263:131–194. doi:10.1016/j.cis.2018.11.008
132. Conaghan PG, Cohen SB, Berenbaum F, Lufkin J, Johnson JR, Bodick N. Brief report: a phase IIb trial of a novel extended-release microsphere formulation of triamcinolone acetonide for intraarticular injection in knee osteoarthritis. Arthritis Rheumatol. 2018;70:204–211. doi:10.1002/art.40364
133. Conaghan PG, Hunter DJ, Cohen SB, et al. Effects of a single intra-articular injection of a microsphere formulation of triamcinolone acetonide on knee osteoarthritis pain. J Bone Jt Surg Am. 2018;100:666–677. doi:10.2106/JBJS.17.00154
134. Kraus VB, Conaghan PG, Aazami HA, et al. Synovial and Systemic Pharmacokinetics (PK) of Triamcinolone Acetonide (TA) Following Intra-Articular (IA) injection of an extended-release microsphere-based formulation (FX006) or standard crystalline suspension in patients with knee osteoarthritis (OA) osteoarthr. Cartil. 2018;26:34–42. doi:10.1016/j.joca.2017.10.003
135. Russell SJ, Sala R, Conaghan PG, et al. Triamcinolone acetonide extended-release in patients with osteoarthritis and type 2 diabetes: A randomized, phase 2 study. Rheumatology. 2018;57:2235–2241. doi:10.1093/rheumatology/key265
136. Ho MJ, Jeong HT, Im SH, et al. Design and in vivo pharmacokinetic evaluation of triamcinolone acetonide microcrystals-loaded PLGA microsphere for increased drug retention in knees after intra-articular injection. Pharmaceutics. 2019;11(8):419. doi:10.3390/pharmaceutics11080419
137. Qiu S, Shi Y, Zang H, et al. Multifunctional injectable microspheres for osteoarthritis therapy via spatiotemporally modulating macrophage polarization and inflammation. NPJ Regen Med. 2024;9(1):22. doi:10.1038/s41536-024-00368-w
138. Wen S, Huang X, Ma J, et al. Exosomes derived from MSC as drug system in osteoarthritis therapy. Front Bioeng Biotechnol. 2024;12:1331218. doi:10.3389/fbioe.2024.1331218
139. Balaraman AK, Arockia Babu M, Afzal M, et al. Exosome-based miRNA delivery: transforming cancer treatment with mesenchymal stem cells. Regen Ther. 2025;28:558–572. doi:10.1016/j.reth.2025.01.019
140. Tao SC, Yuan T, Zhang YL, Yin WJ, Guo SC, Zhang CQ. Exosomes derived from miR-140-5p-overexpressing human synovial mesenchymal stem cells enhance cartilage tissue regeneration and prevent osteoarthritis of the knee in a rat model. Theranostics. 2017;7(1):180–195. doi:10.7150/thno.17133
141. Zhang S, Chu W, Lai R, Lim S, Hui J, Toh W. Exosomes derived from human embryonic mesenchymal stem cells promote osteochondral regeneration. Osteoarthr Cartil. 2016;24:2135–2140. doi:10.1016/j.joca.2016.06.022
142. Zhu Y, Wang Y, Zhao B, et al. Comparison of exosomes secreted by induced pluripotent stem cell-derived mesenchymal stem cells and synovial membrane-derived mesenchymal stem cells for the treatment of osteoarthritis. Stem Cell Res Ther. 2017;8:1–11. doi:10.1186/s13287-017-0510-9
143. Ni Z, Zhou S, Li S, et al. Exosomes: roles and therapeutic potential in osteoarthritis. Bone Res. 2020;25. doi:10.1038/s41413-020-0100-9
144. Fan WJ, Liu D, Pan LY, et al. Exosomes in osteoarthritis: updated insights on pathogenesis, diagnosis, and treatment. Front Cell Dev Biol. 2022;10:949690. doi:10.3389/fcell.2022.949690
145. Mehta S, He T, Bajpayee AG. Recent advances in targeted drug delivery for treatment of osteoarthritis. Curr Opin Rheumatol. 2021;33(1):94–109. doi:10.1097/BOR.0000000000000761
146. Liu H, Zhang Q, Wang S, Weng W, Jing Y, Su J. Bacterial extracellular vesicles as bioactive nanocarriers for drug delivery: advances and perspectives. Bioact Mater. 2021;14:169–181. doi:10.1016/j.bioactmat.2021
147. Kang LJ, Yoon J, Rho JG, et al. Self-assembled hyaluronic acid nanoparticles for osteoarthritis treatment. Biomaterials. 2021;275:120967. doi:10.1016/j.biomaterials.2021.120967
148. Gao J, Xia Z, Mary HB, Joseph J, Luo JN, Joshi N. Overcoming barriers for intra-articular delivery of disease-modifying osteoarthritis drugs. Trends Pharmacol Sci. 2022;43(3):171–187. doi:10.1016/j.tips.2021.12.004
149. Mitragotri S, Lahann J. Physical approaches to biomaterial design. Nat Mater. 2009;8(1):15–23. doi:10.1038/nmat2344
150. Patel P, Nandi A, Jha E, et al. Magnetic Nanoparticle-Based Hybrid Materials. London: Elsevier; 2021:33–64.
151. Kuyinu EL, Narayanan G, Nair LS, Laurencin CT. Animal models of osteoarthritis: classification, update, and measurement of outcomes. J Orthop Surg Res. 2016;11:19. doi:10.1186/s13018-016-0346-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.